

The results obtained in this study support the need to develop appropriate way of communicating and transmitting job recognition at a distance in the context of health teleworking. Among other considerations, video conferencing, virtual moments of conviviality, and telemediated job recognition official implementation and practice guides are suggested.
Keywords: absenteeism, COVID-19 pandemic, health care workers, moderated mediation analysis, new work-related stressors, organizational changes, psychological distress, recognition
Objectives
We aimed to evaluate the effects of new work-related stressors on psychological distress and absenteeism and the role of recognition in these relationships.
Methods
Moderated path analyses were carried out on a sample of 1128 health care workers.
Results
Increased workload related to COVID-19 (coronavirus disease 2019) (β = 1.511, P ≤ 0.01) and fear of COVID-19 (β = 0.844, P ≤ 0.01) were directly associated with a higher level of psychological distress and indirectly (β = 2.306, P ≤ 0.01; and β = 1.289, P ≤ 0.05, respectively) associated with a higher level of absenteeism. Recognition (β = 0.260, P ≤ 0.001) moderated the association between teleworking and psychological distress. Furthermore, this significant moderation effect had a significant impact on absenteeism (β = 0.392, P ≤ 0.05). Regardless of the workplace (on site or teleworking), high recognition was beneficial for psychological distress. This effect seems more important when working on site.
Conclusions
The results propose that specific new work-related stressors should be addressed in the context of organizational change (eg, a pandemic).
Over the past 2 years, almost every aspect of working and family lives has been dramatically impacted by the coronavirus disease 2019 (COVID-19) pandemic.1 Workplaces have had to deal with major organizational changes to adapt to the new tumultuous reality. COVID-19 has been said to have revolutionized some aspects of working life, and the way work is done may turn out to be one of the most important long-term consequences of the pandemic.1 Among these changes are the sudden shift to teleworking for some and the close contact with a virus that worsened the work conditions and increased the workload for others. While the pandemic represents a major change in the lives of people around the world, it has been and continues to be particularly persistent and omnipresent for health care workers.
Since the beginning of the pandemic, health care workers have been the ones dealing with sick people, treating them, and confronting suffering and death, which has an effect on their mental health.2 In fact, a recent systematic review concluded that health care workers were one of the most vulnerable groups as a broad spectrum of psychological problems was observed: 5.2% to 71.2% in anxiety, 1.00% to 88.3% in stress, 8.27% to 61.67% in insomnia, and 4.5% to 50.4% in depression.3 In Canada, 8 months into the pandemic, one-third (33%) of participating health care workers reported fair or poor mental health, with most (70%) of them indicating that their mental health was “a little worse now” or “much worse now” compared with before March 2020.4 In Italy, health care workers were more likely to report fatigue.5 Workers' level of absenteeism was also affected, as 12,000 of more than 290,000 employees were listed as absent at the height of the crisis in the Quebec health care system.6 Beyond absences of a few days when an employee was diagnosed with COVID-19, many of these absences were also the consequence of other factors, such as fatigue, exhaustion, and psychological distress. For nurses, 8902 were absent for diverse reasons, whereas 816 were on sick leave due to COVID-19 as of November 27, 2021 (ie, right in the middle of the data collection period of this study).7 These absences were compensated with overtime and private agencies,7 which adds a burden to colleagues who have to work more hours, along with working with agency colleagues who are less familiar with the organization of work and the specific tasks that vary from one establishment to another. Not only are these absences problematic for colleagues and difficult for the employer to manage, but most importantly, they are detrimental to the quality of care offered to the population. Absenteeism is even more worrying in the context of a global health crisis, which also involves load shedding and the reduction of certain operations to ensure hospital capacity.8
What is happening on a global scale in the world of work and in the public health services sector can be seen from the angle of change. Considering the above, it is relevant to shed additional light on the effects of the specific changes that the pandemic generated, given that many new additional changes are to come in the future. Workers in the health care sector experienced a major structural reform in 2015 (ie, Bill 10) with the merger of establishments and centralization.9 They will have to experience other changes, considering that a work reorganization is unavoidable for a more human and efficient network. This observation existed before the pandemic and was largely reaffirmed as the pandemic progressed.10 It is known that during normal times, work-related stressors can lead to employees' psychological distress and absenteeism. Of pertinent concern are the new work-related stressors that health care workers have to confront in times of stress accentuated by a global health crisis.
Further, several unions representing various professions working in the Quebec health care sector are demanding an increase in compensation for their members,11 who are now called “essential workers and guardian angels.” However, wage increases are humble and do not seem quite up to expectations.12 In the absence of being able to offer monetary compensation adjusted to the importance of the tasks that are carried out, nonmonetary compensation, such as recognition, may be even more important and a realistic way to value and support the efforts made in the short term. Therefore, in this context, we might wonder if recognition can attenuate the deleterious effect of new work-related stressors for health care workers.
Purpose of the Study
This cross-sectional study focuses on new work-related stressors emerging in the context of a pandemic for health care workers in the province of Quebec, Canada, and their effects on psychological distress and absenteeism. The study assesses the role of recognition at work in these relationships established on a sample of 1128 health care workers during the fourth and fifth waves of the COVID-19 pandemic. To this end, this study considers both job demands–resources (JD-R)13 and conservation of resources (COR)14 theories.
BACKGROUND
Psychological Distress and Absenteeism
Absenteeism refers to absences that are avoidable and unscheduled, which is a source of irritation for both employers and colleagues.15 In fact, absenteeism is disruptive to proper organizational functioning and is costly to organizations and the economy as a whole.15 The costs for the employer include direct costs (eg, salary replacement, overtime paid to colleagues) and indirect costs (eg, loss of productive time).16 For the employees themselves, it is not without consequences. Among others, they may lose opportunities for advancement and promotion, are likely to be judged negatively by their colleagues and supervisors, and are deprived of part of their salary. It is possible to imagine that this is even truer for health care workers who have the burden of dealing with a global health crisis and who might have felt guilty for leaving their colleagues behind when absent. Between 2016 and 2020, work absence statistics from Statistics Canada indicated an upward trend in the number of days of absenteeism. In terms of days lost per worker in a year, the Canadian average was 11.6 days, whereas the province of Quebec had an average of 13.9 days.17 The determinants of unplanned absenteeism pertain to psychosocial factors, work factors and stressors, personal illness, family issues, and mental health concerns.18,19 In the past few decades, psychological distress has been established as an important determinant of absenteeism at work.20,21 More recent studies22 have found that mental health problems are a mediator of the relationship between stress related to COVID-19 and absenteeism.
In the context of organizational change, researchers have indicated that the global level of psychological distress increases during the process of organizational change.23 They concluded that to reduce the negative outcomes of reorganization for health care workers, managers could, among others, increase the number of opportunities for rewards. During a reorganization or a period of important organizational changes (eg, COVID-19 pandemic), increased workloads are not generally compensated by an increase in recognition or other rewards that could attenuate the negative effects of increasingly requesting workers' effort.23 Therefore, this study attempts to examine the potential moderating effect of a nonmonetary reward in such a context, namely, recognition.
THEORETICAL MODEL
The theoretical model of this study considers both the JD-R13 and COR14 theories. The JD-R theory makes the general assumption that job demands and resources stimulate two very different processes—a health-impairment process and a motivational process, leading, respectively, to lower or higher job performance (ie, absenteeism).13 It is assumed that organizations design the job demands and job resources of their employees and that employees, in turn, might flourish (ie, motivational process) or experience strain (ie, health-impairment process) after being exposed to these work conditions.24 In this study, job demands refer to the factors related to the COVID-19 pandemic, which are work-related stressors characterized by their novelty, such as teleworking, worsened work conditions, increased workload, and fear of COVID-19. These job demands/new work-related stressors are likely to initiate a health-impairment process, leading to an increase in absenteeism via their effect on psychological distress. In such a scenario, health care workers do not have the energy to reach work goals (eg, not being absent from work). At the individual level, exposure to multiple organizational changes at baseline has been associated with mental distress at follow-up.25 In the present study, the changes refer to the new work-related stressors, which are likely to be associated with psychological distress and therefore absenteeism.
The Role of New Work-Related Stressors on Psychological Distress and Absenteeism
In the context of the present study, teleworking corresponds to working from home via the Internet and communication technologies.26 It should be noted that teleworking (ie, working from home) in the COVID-19 context was, in the case of the health care sector, precipitated and imposed by public health restrictions. Therefore, it was definitely a change for workers who teleworked during the pandemic (ie, new teleworkers), as they were not used to working from home before the pandemic. Although we were unable to locate any study on the effect of teleworking on health care workers, the literature regarding teleworking in the context of COVID-19 for workers in general is equivocal. For instance, a study conducted among workers during the first lockdown concluded that teleworking was beneficial, as it was negatively associated with stress,27 as well as positively associated with psychological well-being.28 Another study carried out among employees of small and medium organizations during the second and third waves of the pandemic found, on the contrary, that teleworking was detrimental, as it was associated with lower work engagement.29 A study reported that starting teleworking from home was associated with increased psychological distress among 15,454 Japanese workers.30 It is possible that working from home can reduce the risk of infection linked to COVID-19, particularly for health care workers. It has also been argued that by working from home, teleworkers are able to develop greater social support from some colleagues while distancing themselves from negative work relationships.31 We posit that the element of novelty is likely to surpass potential beneficial effects of teleworking. Indeed, the context in which it was set up suddenly and unprepared is likely to have been stressful. To our knowledge, no empirical studies have examined the effects of teleworking on absenteeism during the COVID-19 pandemic in a sample of health care workers in Quebec, Canada. Consequently, we intend to shed some light on the effects of teleworking in this particular context.
Worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19 are additional new work-related stressors that might have an effect on health care workers' psychological distress and absenteeism. For instance, heavy workloads, working in unsafe settings, and lack of social support were found to be predictors of posttraumatic stress symptoms among health care workers.32 Direct involvement in COVID-19 screening or treatment, workloads, uncertainties caused by the pandemic, and less psychological support in the workplace have been described as determinants of burnout among Malaysian health care workers.33 Fear of infection among health care workers has been associated with COVID stress syndrome,34 and fear of COVID-19 correlated with community nurses' work-related distress, which, in turn, impacted their intention to quit their work and the nursing profession.35 A recent study established that the threat of COVID-19 triggered employees' absenteeism.22
Therefore, considering the JD-R health-impairment process as well as the empirical evidence presented above, the following hypotheses are postulated:
H1. New work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) are directly associated with psychological distress. (Direct effect on psychological distress hypothesis)
H2. New work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) are directly associated with absenteeism. (Direct effect on absenteeism hypothesis)
The Mediating Role of Psychological Distress on Absenteeism
As mentioned previously, the JD-R theory postulates that job demands (eg, new work-related stressors) stimulate a health-impairment process leading to lower job performance (ie, absenteeism).13 Consistent with this process, new work-related stressors are expected to deplete resources and can thus lead to absenteeism via their effects on psychological distress. On the empirical side, the risk of being infected with the COVID-19 virus has been associated with higher mental health problems, which in turn increases the level of absenteeism among employees.22 Further, psychological distress is a mediator in the relationship between a stressor (ie, appraisal of economic crisis) and absenteeism.36 Teleworking was indirectly associated with lower job performance (ie, intention to quit) via its effect on work engagement.29 These empirical results seem to support the general idea that new work-related stressors lead to a stress reaction (eg, psychological distress), which leads to behavioral consequences in terms of job performance (eg, absenteeism).
Accordingly, the following hypothesis is postulated:
H3. Psychological distress mediates the relationship between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) and absenteeism. (Mediation hypothesis)
The Moderating Role of Recognition
One essential work resource is examined in this research: recognition. Recognition is an intangible compensation that refers to the received esteem from others at work (eg, colleagues, supervisors) and acknowledgment associated with achievement (eg, favorable criticism).37 As previously stated, the undesirable impact of workload on mental health can be attenuated by job resources, according to JD-R theory.38 Workers need resources to adequately deal with new work-related stressors.39 This echoes a previous work40 that argued that job demands (eg, new work-related stressors) are likely to lead to psychological distress in the context of low rewards (eg, low recognition). This proposition is consistent with COR theory,14 which fine-tunes the JD-R proposition and postulates that organizational resources could support the prevention of a cycle of loss (ie, loss spiral), ultimately preventing employees from entering into a health-impairment process characterized by psychological distress and absenteeism. Recognition is likely to weaken the loss spiral. In other words, recognition could prevent a sequel that regulates employees' ineffective adjustment to their work environments. Here, we assume that health care workers' psychological distress is the result of the interplay between new work-related stressors and recognition. Furthermore, recognition is expected to lessen the effects of new work-related stressors on health care workers' psychological distress, which would affect absenteeism. We were unable to identify empirical studies that specifically addressed the moderating role of recognition in these relationships. However, the direct effects of recognition are conspicuous in the literature, which indicates that recognition is associated with lower psychological distress41 and lower absenteeism.42
Therefore, the following hypotheses are postulated:
H4. Recognition moderates the association between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) and psychological distress. (Moderation hypothesis)
H5. The relationship between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19), psychological distress, and absenteeism is moderated by recognition. (Moderated mediation hypothesis) (Fig. 1).
FIGURE 1.
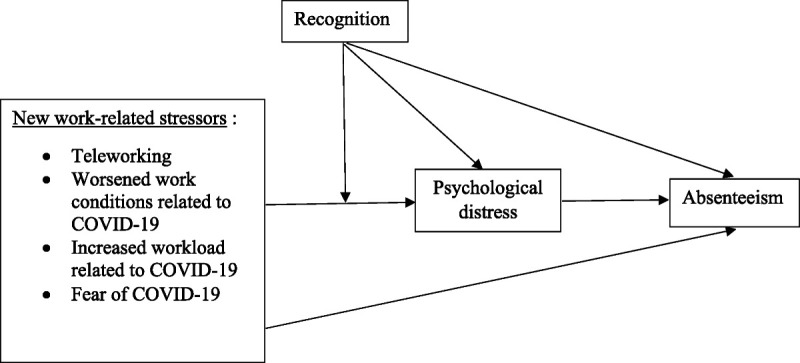
Hypothetical model.
METHODS
Procedures and Participants
The data were collected during the fourth and fifth waves of the COVID-19 pandemic in the province of Quebec, Canada (from October 18, 2021 to January 27, 2022). The sample recruited comprised 1128 health care workers. Given the public health restrictions imposed by the pandemic, we designed an online survey and favored a network sampling to bypass in-person interactions and respect social distancing. The participants had to occupy a paid work within the Quebec health care sector. The questionnaire link was shared on social networks, such as Facebook and LinkedIn. Quebec's health care sector workers were targeted, so the questionnaire link was sent to administrators of Facebook health care sector workers' unions and professional associations' pages by email. These requests were honored by some of the groups, as the link was shared on a few Facebook pages, namely, the Alliance du personnel professionnel et technique de la santé et des services sociaux, Fédération interprofessionnelle de la santé du Québec, Confédération des syndicats nationaux (CSN), and the Ordre des infirmières et infirmiers auxiliaires du Québec. The Ordre des infirmières et infirmiers auxiliaires du Québec sent the questionnaire link to its members via their newsletter with an email, whereas the Ordre des ergothérapeutes du Québec sent the questionnaire link to its members via email. The participants of this research declared that they read the consent form by clicking on the checkbox to that effect in the survey. No monetary compensation was given. Ethical approval was granted by the institutional review board of the University of Quebec in Trois-Rivières (protocol code: CER-21-280-07.13; date of approval: October 5, 2021). The collected sample comprised 1128 health care workers, of which 92.38% were female (note that this proportion is similar to the actual proportion of women working in the health care system in Canada (ie, 82%)43), with an average age of 41.2 years. It is worth noting that 36.84% were nurses, 12.94% were social workers, 1.42% were personal care attendants, 22.16% were occupational therapists, 1.51% were physiotherapists, and 36.97% were other health-related professionals (eg, nutritionist, specialized educator, psychologist, laboratory technician, medical secretary).
Measures
Absenteeism
Absenteeism was measured with a single item (ie, “In the past 12 months, how many days have you been absent from work due to personal health problems or injury?”), which was coded in number of days.
Psychological Distress
Psychological distress was evaluated with six items (eg, “During the past month, about how often did you feel hopeless?” α = 0.87) based on the Kessler Psychological Distress Scale (K6).44 This variable was measured on a five-point additive scale, with responses ranging from 0 (none of the time) to 4 (all of the time).
Teleworking
Teleworking was measured with a single item (ie, “Have you done any teleworking during the COVID-19 crisis?”), which was coded either as 0 (no) or 1 (yes).
Worsened Work Conditions Related to COVID-19
Worsened work conditions related to COVID-19 were measured with a single item (ie, “How has the COVID-19 crisis affected your work conditions?”) and were coded as 0 (The COVID-19 crisis improved or did not change work conditions) or 1 (The COVID-19 crisis worsened work conditions).
Increased Workload Related to COVID-19
Increased workload related to COVID-19 was measured with a single item (ie, “How has the COVID-19 crisis affected your workload?”) and was coded on a five-point Likert scale (0 = decrease, large decrease, or same as before, and 1 = increase or large increase). Workload was treated as dichotomous in the analysis (0 = decrease or same as before and 1 = increase).
Fear of COVID-19
Fear of COVID-19 was measured with a single item (ie, “Have you been afraid for your own health while performing your duties since the start of the COVID-19 pandemic?”), which was coded either as 0 (no) or 1 (yes).
Recognition
The Effort-Reward Imbalance Questionnaire40 was used to assess recognition with five items (eg, “Considering all my efforts and achievements, I receive the respect and prestige I deserve at work”; α = 0.84). This variable was measured on a four-point additive scale, with responses ranging from 1 (strongly agree) to 4 (strongly disagree).
Control Variables
Previous studies have identified variables associated with psychological health and/or absenteeism. These variables are gender,27,45–47 age,48–51 educational level,52,53 household income,28,54 marital status,55–57 parental status,55,58,59 work schedule (full-time),58,60 number of hours worked,61,62 and work zone (hot).63 In this study, gender was coded as either 0 (male) or 1 (female). Age was coded in number of years. Marital status was coded as 0 (single) or 1 (living as a couple). Educational level was coded using the highest degree attained by the participant on a 10-category scale with ranks ordered according to the number of years needed to complete each degree from lowest to highest (1 = none, 2 = high school, 3 = professional school, 4 = college [general], 5 = college [technical], 6 = university [undergraduate certificate], 7 = university [bachelor's degree], 8 = university [graduate diploma], 9 = university [master's degree], 10 = university doctorate). Household income was coded using pretax household income for the preceding 12 months on a 12-category scale (1 = less than $20,000, 12 = $120,000 or more). Marital status was coded as 0 (single) or 1 (living as a couple). Parental status was coded as 0 (no) or 1 (dependent children living with the participant). Work schedule was coded as 0 (part-time) or 1 (full-time). The number of hours worked was coded as the number of hours. Work zone (hot) was measured with a single item (ie, “Have you worked in a hot zone [more at risk of contagion of the virus])?” and was coded 0 (no) or 1 (yes). Negative impact related to COVID-19 was measured with a single item (ie, “Has COVID-19 had an impact on your work life?”) and was coded as 0 (positive impact or no impact) or 1 (negative impact).
Data Analysis
Moderated path analyses were conducted with MPlus software, version 8,64 with a robust maximum likelihood estimator to estimate all models. The goodness of fit was evaluated using the Tucker-Lewis index and the comparative fit index. Values greater than 0.90 and 0.95 are considered indicative of satisfactory and excellent fit, respectively.65 Those analyses fall under the rubric of conditional indirect effects; that is, the effect of interest here is an indirect (mediation) effect that could be conditioned by the values of a moderator.66,67 We used a previously described modeling method for conditional indirect effects.68 First, our analytical procedure was to evaluate a model that comprised recognition and new work-related stressors so that we could estimate the main effects they exert on absenteeism and psychological distress. Second, recognition and new work-related stressors were entered into a second model to test whether they indirectly influenced absenteeism via psychological distress. Third, we verified whether recognition had a moderating effect on the relationship between new work-related stressors and psychological distress. Thus, we introduced, one by one, interactions between recognition and new work-related stressors. In total, four interaction effects were verified—one for each new work-related stressors. Given the number of interactions to be evaluated separately, we applied a Bonferroni correction to the estimated interactions and set the significance level at P < 0.01. Furthermore, it should be noted that the controlled variables were included in all models tested.
RESULTS
Descriptive Analysis
Table 1 presents the main variables' descriptive results (mean/proportion, SD) and correlations. Notably, the average number of days of absenteeism was 18.08 days for the last 12 months, which is largely above the Canadian average established at 11.6 days for 2020, as previously stated. The mean level of psychological distress was 9.25, which corresponds to a moderate level of psychological distress, according to one interpretation suggested by the Public Health Expertise and Reference Centre.69
TABLE 1.
Descriptive and Correlational Statistics
| M/% | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
|---|---|---|---|---|---|---|---|---|---|
| 1. | 18.08 | 39.00 | 1 | ||||||
| 2. | 9.25 | 4.85 | 0.24** | 1 | |||||
| 3. | 13.61 | 3.37 | −0.16** | −0.48** | 1 | ||||
| 4. | 42.11 | −0.07* | −0.15** | 0.23** | 1 | ||||
| 5. | 82.36 | 0.09** | 0.18** | −0.20** | −0.10** | 1 | |||
| 6. | 86.88 | 0.04 | 0.22** | −0.16** | −0.10** | 0.25** | 1 | ||
| 7. | 69.15 | 0.08** | 0.18** | −0.11** | −0.10** | 0.11** | 0.10** | 1 |
1, Absenteeism; 2, psychological distress; 3, recognition; 4, teleworking; 5, worsened work conditions related to COVID-19; 6., increased workload related to COVID-19; 7, fear of COVID-19; M, mean or percentage.
*P ≤ 0.05 (coefficients ≥ 0.05).
**P ≤ 0.01 (coefficients ≥ 0.05).
Multiple Regression Analyses
Table 2 provides results on the main effects of recognition and new work-related stressors on absenteeism and psychological distress. The results showed that psychological distress was associated with higher absenteeism. Furthermore, recognition was associated with lower levels of psychological distress, whereas increased workload related to COVID-19 and fear of COVID-19 were associated with higher levels of psychological distress.
TABLE 2.
Direct Effects of Recognition and New Work-Related Stressors on Psychological Distress and Absenteeism
| Psychological Distress | Absenteeism | |
|---|---|---|
| Constant | 13.67** | 11.09** |
| Psychological distress | 1.527** | |
| Recognition | −0.577** | −0.343 |
| New work-related stressors | ||
| Teleworking | 0.359 | −0.163 |
| Worsened work conditions related to COVID-19 | 0.503 | 4.057 |
| Increased workload related to COVID-19 | 1.511** | −3.846 |
| Fear of COVID-19 | 0.844** | 2.527 |
| Adjustments | ||
| CFI | 1.00 | |
| TLI | 1.00 | |
| χ2 (df) | 533.811 (31) | |
CFI, comparative fit index; df, degrees of freedom; TLI, Tucker-Lewis index.
*P ≤ 0.01.
The following variables were controlled for in all models: gender, age, educational level, household income, marital status, parental status, work schedule (full-time), number of hours worked, work zone (hot), and negative impact related to COVID-19 (unstandardized coefficients).
Mediation Analyses
The results provided in Table 3 show variables that indirectly influenced absenteeism via psychological distress. Recognition was indirectly associated with lower absenteeism via its effect on psychological distress. Increased workload related to COVID-19 and fear of COVID-19 were indirectly associated with higher absenteeism via their effects on psychological distress.
TABLE 3.
Indirect Effects of Recognition and New Work-Related Stressors on Absenteeism
| Estimation | P | |
|---|---|---|
| Recognition | −0.881 | 0.000 |
| New work-related stressors | ||
| Teleworking | 0.549 | 0.186 |
| Worsened work conditions related to COVID-19 | 0.767 | 0.147 |
| Increased workload related to COVID-19 | 2.306 | 0.002 |
| Fear of COVID-19 | 1.289 | 0.011 |
| Moderated mediation | ||
| Interaction recognition—teleworking | 0.392 | 0.011 |
The following variables were controlled for in all models: gender, age, educational level, household income, marital status, parental status, work schedule (full-time), number of hours worked, work zone (hot), and negative impact related to COVID-19 (unstandardized coefficients).
Moderation Analysis
As shown in Fig. 2, recognition (β = 0.260, P ≤ 0.001) played a moderating role between teleworking and psychological distress. A low level of recognition was associated with a higher level of psychological distress, regardless of the workplace (ie, on site or teleworking), during COVID-19. A high level of recognition attenuated the effect of the workplace (ie, on site or teleworking) on psychological distress during COVID-19. This effect seems more important in the context of on-site work.
FIGURE 2.
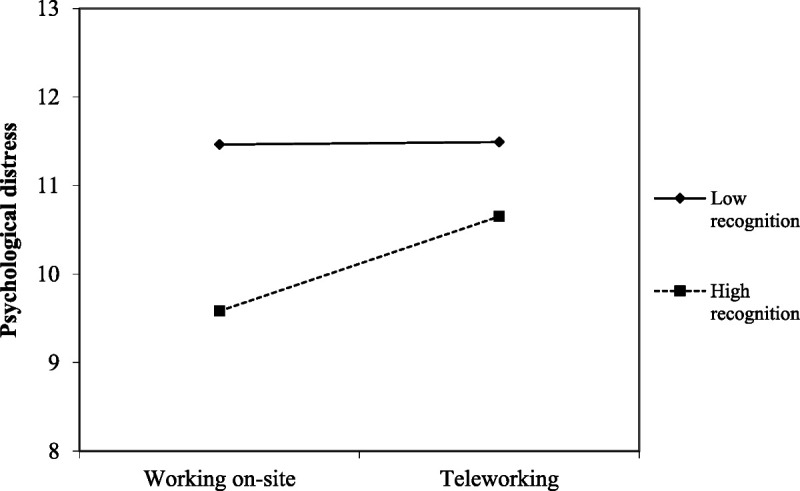
Significant interaction.
Moderated Mediation Analyses
The significant interaction between recognition and teleworking also demonstrated a significant moderated mediation effect (Table 3). Indeed, the interaction between recognition and workplace (ie, on site or teleworking) on psychological distress was positively associated with absenteeism. In other words, recognition moderated the effect of the workplace (ie, on site or teleworking) on psychological distress, and this influenced absenteeism.
DISCUSSION
This research aimed to investigate the direct and indirect effects of new work-related stressors on psychological distress and absenteeism, as well as the moderating role of recognition on the relationship between new work-related stressors, psychological distress, and absenteeism during the fourth and fifth waves of the COVID-19 pandemic based on a sample of 1128 health care workers in the province of Quebec, Canada.
The first hypothesis (H1), which postulated that new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) were directly associated with psychological distress, was partially supported. Indeed, increased workload related to COVID-19 and fear of COVID-19 were both significantly and positively associated with psychological distress, whereas teleworking and worsened work conditions related to COVID-19 were not. Note that we also found that recognition was negatively associated with psychological distress, even if we had not formulated a specific hypothesis for the direct effect of recognition. These results are consistent with previous empirical studies regarding the effect of increased workload related to COVID-1932,33 and fear of COVID-1934,35 on health care workers' mental health. These results are also consistent with the JD-R theory,13 which postulates that job demands (eg, new work-related stressors) are likely to initiate a health-impairment process leading to psychological distress. Surprisingly, teleworking and worsened work conditions related to COVID-19, both new work-related stressors, were not significantly associated with psychological distress. This is in contradiction with the health-impairment process of the JD-R theory,13 as well as the empirical background for worsened work conditions related to COVID-19.32,35 Regarding the effect of teleworking, we had previously noted that the literature is rather equivocal. Some studies found that teleworking was somewhat beneficial for stress and psychological well-being,27,28 whereas others found the opposite for work engagement and psychological distress.29,30 It has also been argued that by working from home, teleworkers are able to develop greater social support from some colleagues while distancing themselves from negative work relationships.31 Thus, we expected that the element of novelty, specifically for new health care teleworkers, would be detrimental instead of insignificant.
The second hypothesis (H2) postulated that new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) were directly associated with absenteeism. This hypothesis was rejected. In fact, none of the new work-related stressors were directly associated with absenteeism. Even if we had not formulated a specific hypothesis as to the direct effect of recognition, we found that recognition was not significantly or directly associated with absenteeism. These results are surprising considering the evidence from empirical studies as well as JD-R theory.13 According to the JD-R theory, job demands (eg, new work-related stressors) could initiate a health-impairment process leading to lower job performance (ie, absenteeism). Although we could not locate any study pertaining to the direct effect of new work-related stressors on absenteeism, we found a study that established that the threat of COVID-19 triggered employees' absenteeism.22 It is possible to argue that the effects of new work-related stressors on absenteeism can be explained by a mediation mechanism instead of a direct effect. Hence, new work-related stressors are more likely to be associated with absenteeism via their effects on mental health (eg, psychological distress). In fact, we formulated a specific hypothesis for this effect (see H3).
The third hypothesis (H3), which postulated that psychological distress mediated the relationship between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) and absenteeism, was partially supported. Increased workload related to COVID-19 and fear of COVID-19 were associated with higher absenteeism via their effects on psychological distress. For their part, teleworking and worsened work conditions related to COVID-19 were not indirectly associated with absenteeism via psychological distress. In accordance with the JD-R theory,13 we postulated that these job demands/new work-related stressors were likely to initiate a health-impairment process, leading to an increase in absenteeism via their effect on psychological distress. In coherence with this process, new work-related stressors are expected to deplete resources and thus lead to absenteeism via their effect on psychological distress. On the empirical side, previous studies have found that the risk of being infected with the COVID-19 virus was associated with higher mental health problems, which in turn increased the level of absenteeism among employees.22 Psychological distress has been indicated as a mediator in the relationship between a stressor (ie, appraisal of economic crisis) and absenteeism,36 and teleworking was indirectly associated with lower job performance (ie, intention to quit) via its effect on work engagement.29 These empirical results seem to support the general idea that new work-related stressors lead to a stress reaction (eg, psychological distress), which results in behavioral consequences in terms of job performance (eg, absenteeism). However, teleworking and worsened work conditions related to COVID-19 did not have a direct effect on psychological distress in the present study. Therefore, it is obvious that the explanatory mechanism (ie, indirect effect) that is the subject of the present hypothesis does not operate in our context. Furthermore, it is possible to argue that the nonsignificant result of teleworking might be partially explained by the possibility that, in the context of working from home, the rate of absenteeism is less declared and monitored. We surmise that teleworkers may be present at home instead of considering themselves absent.
The fourth hypothesis (H4), which postulated that recognition moderated the association between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19) and psychological distress, was partially supported. We found that recognition played a moderating role in the relationship between teleworking and psychological distress. For their part, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19 were not significantly moderated by recognition. Therefore, it seems that recognition alone is not enough to mitigate the effects of these specific new work-related stressors on psychological distress. Thus, it will be necessary to attempt to identify alternative organizational resources for promoting adaptation to new work-related stressors. As previously stated, the undesirable impact of workload on mental health can be attenuated by job resources, according to the JD-R theory.38 Workers need resources to adequately deal with new work-related stressors.39 This idea is consistent with a previous study,40 which argued that job demands (eg, new work-related stressors) are likely to lead to psychological distress in the context of low rewards (eg, low recognition). Even though we were not able to identify any empirical studies that specifically addressed the moderating role of recognition on these relations, our results regarding the moderating effect of recognition on teleworking are coherent with theories that postulate these concepts. Regardless of the workplace (on site or teleworking), high recognition was beneficial for psychological distress. In other words, in the context of high recognition, the workplace (on site or teleworking) is less detrimental to psychological distress. This effect seems more important in the context of on-site work. We argue that this is probably because recognition is transmitted or perceived more easily in person than from a distance.
The fifth hypothesis (H5) postulated that the relationship between new work-related stressors (ie, teleworking, worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19), psychological distress, and absenteeism was moderated by recognition. This hypothesis was partially supported. In fact, we observed that the moderation effect of recognition on the relationship between teleworking and psychological distress (see H4) was significantly associated with absenteeism. This proposition is consistent with COR theory,14 which fine-tunes the JD-R proposition and postulates that organizational resources could support the prevention of a cycle of loss (ie, loss spiral), ultimately preventing employees' from entering into a health-impairment process characterized by psychological distress and absenteeism. Recognition was expected to weaken the loss spiral and prevent a sequel that regulates employees' ineffective adjustment to their work environments. In other words, recognition was expected to lessen the effects of new work-related stressors on health care workers' psychological distress, which would affect absenteeism. Overall, it appears that teleworking does not significantly influence psychological distress on its own. However, when interacting with recognition, it acts on psychological distress. This effect has repercussions on absenteeism. The nonsignificant results regarding worsened work conditions related to COVID-19, increased workload related to COVID-19, and fear of COVID-19 are not surprising, considering that these new work-related stressors were not moderated by recognition (see H4).
In total, we established that psychological distress played a mediating role between new work-related stressors and absenteeism. Increased workload related to COVID-19 and fear of COVID-19 were directly associated with a higher level of psychological distress and indirectly associated with a higher level of absenteeism. We also observed that recognition played a moderating role in the relationship between teleworking and psychological distress. Furthermore, this significant moderation effect had a significant impact on absenteeism (moderated mediation effect). Regardless of the workplace (on site or teleworking), high recognition was beneficial for psychological distress. This effect seems more important when working on site. The findings highlight that recognition at work can alter the relationship between new work-related stressors and psychological distress, resulting in lower absenteeism. Therefore, increased workload related to COVID-19, fear of COVID-19, and recognition emerged as crucial determinants that should be given due consideration by organizations in the public health services sector that wish to lower psychological distress and absenteeism in the context of organizational change (eg, a pandemic).
Practical Implications
The results obtained in this study suggest that line managers and human resource (HR) professionals in the public health services sector should pay special attention to the increased workload related to COVID-19, fear of COVID-19, recognition in general, and recognition when teleworking. First, the increased workload related to COVID-19 (or workload in general) could be reduced, for example, through work reorganization and the optimization of schedule management. Consistent with this, a previous study suggested focusing on stabilizing replacements in targeting employees' workload.70 This is certainly not an easy task for public health services sector line managers and HR professionals, especially in the situation of an acute insufficiency of candidates for employment that team up with a pandemic. The actual context brings a lot of increased workload for workers, as well as little room for maneuvering for the employer by force of circumstances. Perhaps one possible avenue would be to try to attract more workers to this sector to distribute the workload. Improved HR marketing campaigns and the development of the employer brand in this sector could be helpful. Inevitably, it will also be necessary to improve the work conditions as well as the direct remuneration in this sector to achieve this goal of attraction. Second, fear of COVID-19 should also be the target of specific interventions. Among others, it was suggested that online and electronic media broadcasts provide advice on how to prevent the risk of transmission between patients and health care workers in medical settings to reduce fear of COVID-19.71 Providing protection equipment also seems essential. A prior study identified that health care workers had a greater need for personal protective equipment than for psychological help, as they feared the virus.72 Two literature reviews also pointed to the importance of providing health care workers with adequate protective equipment.73,74 Nevertheless, we posit that the most realistic and promising course of action is based on optimizing recognition at work, which corresponds to our third practical implication proposition. Accordingly, workplace recognition programs, such as line managers and HR professionals highlighting workers' positive behaviors as well as their fundamental role in the COVID-19 context, are crucial. Recognition should be precise and legitimate, with colleagues and supervisors who authentically prioritize occasions to chat with workers.75 With regard to the recognition offered at a distance, few studies have identified the best practices to adopt. Others have suggested, among others, favoring video conferencing or the telephone rather than emails to organize virtual moments of conviviality and devote time to resolving issues quickly.76 Another suggestion is to reach out to workers regularly, to preserve a social connection.77 In this way, workers are likely to feel considered important. The studied context has given priority to the design of telemediated HR management practices, because it is essential to provide similar job resources even at a distance. Accordingly, telemediated job recognition official implementation and practice guides are suggested.
Limitations and Recommendations for Future Research
This study is not without limitations. First, a snowball strategy sampling method was used to recruit health care workers. It is possible that this sampling method introduced bias; consequently, our sample is probably not representative of the entire health care workers' population. Despite that, it was previously demonstrated that this sampling approach is legitimate and grants for indiscernible results in comparison with a standard sample.78 It also allowed us to survey health care workers in the context of a pandemic in which in-person communications were unrealistic. Consequently, the nonprobabilistic sample that served to provide this study's conclusions should be interpreted with prudence. Further, the response rate was difficult to evaluate, considering that we used a snowball sampling method. Second, our sample was composed of 92.38% women. Although this proportion is similar to the actual proportion of women working in the health care system in Canada (ie, 82%),43 the results of this research should still be interpreted with vigilance. The results obtained are probably more representative of women and are therefore not necessarily generalizable to both genders. Third, this study is cross-sectional, making it impossible to confirm causality. Fourth, this study evaluated workers' perceptions; for this reason, the variables were at the individual level, and responses were garnered from one source (ie, health care workers). Therefore, future studies should also collect data from line managers to avoid common method variance bias. Fifth, it is worth mentioning that being aware of the high workload of health care workers in the context of the COVID-19 pandemic, a short questionnaire format was used. For example, we did not address alternative work-related stressors (eg, low decision authority, low skill utilization) that may accentuate health care workers' psychological distress and absenteeism rates. Nor did we assess the individual resources (eg, emotional intelligence, self-efficacy) that these health care workers were able to mobilize to filter their perception of new work-related stressors. In relation to that, we assume that emotional quotient or alternative competences should be investigated in association to new work-related stressors' adjustment in any context of organizational change. It is possible that unobserved variables could have influenced the relationships evaluated in this study. For instance, it could be relevant to verify the additional effect that alternative rewards (eg, monetary rewards) offered to health care workers might have on psychological distress and absenteeism. Future studies should be carried out using longitudinal data and diverse samples in terms of sectors of activity and countries and should occur after the pandemic context to confirm and extend our research. Future research should also evaluate whether different patterns of association exist according to gender and/or sex. Further, work-family integration versus segmentation preferences are worth examining,79 together with basic psychological needs for autonomy, competence, and relatedness80 in terms of possible differential effects on psychological distress and absenteeism. Future studies should also investigate the effects of recognition when teleworking. Particular attention should be paid to the ability to transmit and receive colleagues' and supervisors' recognition in a teleworking context. Attempts to identify ways to better transmit and ensure that recognition is equally efficient at a distance could be an interesting avenue for research. In doing so, researchers will contribute to the advancement of knowledge to facilitate the transition to the new normal. This includes, but is not limited to, the study of work organization conditions in the context of telework, which will probably become a new standard in the world of future work. Although its implementation might be limited to specific contexts, the movement toward teleworking is expected to become a new way of working,81 even for some health care workers. To that effect, a report from Statistic Canada showed that the majority (79.4%) of new health care and social assistance teleworkers would prefer to work mostly from home once the COVID-19 pandemic is over (47.5%, half of hours at home; 31.9%, most of hours at home), against 20.6% who would prefer to do most or all hours outside the home.82 Accordingly, it is necessary to adjust to this new reality and preferences, and researchers could offer an important contribution in this regard.
CONCLUSIONS
The main objectives of this research were to examine the direct and indirect effects of new work-related stressors on psychological distress and absenteeism, as well as the moderating role of recognition on the relationship between new work-related stressors, psychological distress, and absenteeism during the fourth and fifth waves of the COVID-19 pandemic based on a sample of 1128 health care workers in the province of Quebec, Canada. The results indicated that increased workload related to COVID-19 and fear of COVID-19 were directly associated with a higher level of psychological distress and indirectly associated with a higher level of absenteeism. We also observed that recognition played a moderating role in the relationship between teleworking and psychological distress. Furthermore, this significant moderation effect had a significant impact on absenteeism (moderated mediation effect). Regardless of the workplace (on site or teleworking), high recognition was beneficial for psychological distress. This effect seems more important when working on site. Importantly, we found that recognition alone was not sufficient to mitigate the effects of all new work-related stressors. Hence, it seems that although recognition is an important resource, it is not necessarily the cure of all ills or the ultimate cure to prevent the fall in the battle faced by essential workers/“guardian angels.” Consequently, alternative rewards, work arrangements, and HR management practices should be further investigated. Despite the limitations of our study, we hope to contribute to a myriad of reflections on work-related stressors in the context of COVID-19 pandemic. The conclusions of this research lengthen the literature by demonstrating the moderated pathways through which new work-related stressors are linked to the psychological distress and absenteeism of health care workers and by suggesting specific practical recommendations to address these issues. Beyond any doubt, health care workers will have to face additional changes in the future. Moreover, there is a possibility that other pandemics and/or any other major change are ahead of us that will prolong or possibly bring new work-related stressors. At the time of writing, the sixth wave of COVID-19 was confirmed by the Public Health Expertise and Reference Centre.83 Even if this research indicates that recognition seems beneficial in the context of changes associated with new work-related stressors, it will still be crucial to make sure that it is equally positive for both on-site and working from home. Given that recognition seems more easily transmitted on site should not be a license to avoid teleworking. Instead, it supports the need to better organize this resource and develop an optimal and appropriate way of transmitting recognition at a distance. As new health care teleworkers seem to prefer teleworking, at least for a few days a week, it is critical to adjust to it in the finest possible manner. Accordingly, video conferencing, virtual moments of conviviality, and telemediated job recognition official implementation and practice guides are suggested.
Footnotes
Funding sources: None to disclose.
Conflict of interest: None declared.
Contributor Information
Annick Parent-Lamarche, Email: annickparentlamarche@hotmail.com.
Sonia Laforce, Email: sonia.laforce@uqtr.ca.
REFERENCES
- 1.Eurofound . COVID-19: a changed Europe 2021. Available at: https://www.eurofound.europa.eu/fr/news/news-articles/covid-19-a-changed-europe. Accessed April 18, 2022.
- 2.Eurofound . COVID-19 intensifies emotional demands on healthcare workers. 2020. Available at: https://www.eurofound.europa.eu/fr/publications/blog/covid-19-intensifies-emotional-demands-on-healthcare-workers. Accessed March 28, 2022.
- 3.Yaghoubi M, Salimi M, Meskarpour-Amiri M. Systematic review of productivity loss among healthcare workers due to COVID-19. Int J Health Plann Manage. 2022;37:94–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Statistics Canada . Mental Health Among Health Care Workers in Canada During the COVID-19 Pandemic. 2021. Available at: https://www150.statcan.gc.ca/n1/daily-quotidien/210202/dq210202a-eng.htm. Accessed March 29, 2022.
- 5.Mansueto G Lopes FL Grassi L, et al. Impact of COVID-19 outbreak on Italian healthcare workers versus general population: results from an online survey. Clin Psychol Psychother. 2021;28:1334–1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Leduc L. L'absentéisme loin du sommet enregistré en 2020. La Presse. 2021. Available at: https://www.lapresse.ca/covid-19/2021-12-21/reseau-de-la-sante/l-absenteisme-loin-du-sommet-enregistre-en-2020.php. Accessed March 29, 2022. [Google Scholar]
- 7.Archambault H, Duchaine H. Près de 9000 infirmières absentes du réseau, in Journal de Montréal. Montreal, Quebec, Canada; 2021. Available at: https://www.journaldemontreal.com/2021/11/27/plus-de-8600-infirmieres-absentes-du-reseau. Accessed March 29, 2022. [Google Scholar]
- 8.Gerbet T.À peine enclenché, le niveau maximal de délestage est déjà insuffisant au Québec, in Radio-Canada. 2022.
- 9.Loi modifiant l'organisation et la gouvernance du réseau de la santé et des services sociaux notamment par l'abolition des agences régionales. 2015. Available at: http://www2.publicationsduquebec.gouv.qc.ca/dynamicSearch/telecharge.php?type=5&file=2015C1F.PDF. Accessed March 29, 2022.
- 10.Cousineau ME. Québec promet une vaste réforme du système de santé. Le Devoir. 2022. [Google Scholar]
- 11.QMI Agency . Le rattrapage salarial au cœur des négociations en santé. J Montreal. 2021. Available at: https://www.ledevoir.com/politique/quebec/692538/presentation-plan-reorganisation-soins-de-sante. Accessed March 29, 2022. [Google Scholar]
- 12.Radio-Canada . La nouvelle offre de Québec au secteur public ne satisfait pas les syndicats. 2021. Available at: https://ici.radio-canada.ca/nouvelle/1781330/quebec-fonction-public-depot-offre-lebel--manifeste-montreal. Accessed April 22, 2022.
- 13.Demerouti E Bakker AB Nachreiner F, et al. The job demands–resources model of burnout. J Appl Psychol. 2001;86:499–512. [PubMed] [Google Scholar]
- 14.Hobfoll SE. Conservation of resources: a new attempt at conceptualizing stress. Am Psychol. 1989;44:513–524. [DOI] [PubMed] [Google Scholar]
- 15.Statistics Canada . Work Absence Rates: Data Quality, Concepts and Methodology. 2020. Available at: https://www.statcan.gc.ca/en/statistical-programs/document/3701_D68_T25. Accessed March 28, 2022.
- 16.Nunes AP, et al. The effect of employee assistance services on reductions in employee absenteeism. J Bus Psychol. 2018;33:699–709. [Google Scholar]
- 17.Statistics Canada . . Table 14-10-0190-01 Work Absence of Full-Time Employees by Geography, Annual, Inactive. 2021. 10.25318/1410019001-eng. [DOI]
- 18.Kocakulah MC, et al. Absenteeism problems and costs: causes, effects and cures. Int Bus Econ Res J. 2016;15:89–96. [Google Scholar]
- 19.Niedhammer I Chastang JF Sultan-Taïeb H, et al. Psychosocial work factors and sickness absence in 31 countries in Europe. Eur J Public Health. 2013;23:622–9. [DOI] [PubMed] [Google Scholar]
- 20.Hardy GE, Woods D, Wall TD. The impact of psychological distress on absence from work. J Appl Psychol. 2003;88:306–314. [DOI] [PubMed] [Google Scholar]
- 21.Siu OL. Predictors of job satisfaction and absenteeism in two samples of Hong Kong nurses. J Adv Nurs. 2002;40:218–229. [DOI] [PubMed] [Google Scholar]
- 22.Karatepe OM, Saydam MB, Okumus F. COVID-19, mental health problems, and their detrimental effects on hotel employees' propensity to be late for work, absenteeism, and life satisfaction. Curr Issue Tour. 2021;24:934–951. [Google Scholar]
- 23.Lavoie-Tremblay M Bonin JP Lesage AD, et al. Contribution of the psychosocial work environment to psychological distress among health care professionals before and during a major organizational change. Health Care Manag. 2010;29:293–304. [DOI] [PubMed] [Google Scholar]
- 24.Bakker AB, Demerouti E. Job demands–resources theory: taking stock and looking forward. J Occup Health Psychol. 2017;22:273–285. [DOI] [PubMed] [Google Scholar]
- 25.Fløvik L, Knardahl S, Christensen JO. Organizational change and employee mental health. Scand J Work Environ Health. 2019;45:134–145. [DOI] [PubMed] [Google Scholar]
- 26.Tremblay DG, Paquet R, Najem E. Telework: a way to balance work and family or an increase in work—family conflict? Can J Commun. 2006;31:715–731. [Google Scholar]
- 27.Parent-Lamarche A, Boulet M. Workers' stress during the first lockdown: consequences on job performance analyzed with a mediation model. J Occup Environ Med. 2021;63:469–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Parent-Lamarche A, Boulet M. Employee well-being in the COVID-19 pandemic: the moderating role of teleworking during the first lockdown in the province of Quebec, Canada. Work. 2021;70:763–775. [DOI] [PubMed] [Google Scholar]
- 29.Parent-Lamarche A. Teleworking, work engagement, and intention to quit during the COVID-19 pandemic: same storm, different boats? Int J Environ Res Public Health. 2022;19:1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shiota N Ishimaru T Okawara M, et al. Association between work-related changes caused by the COVID-19 pandemic and severe psychological distress among Japanese workers. Ind Health. 2021;60:216–223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Collins AM, Hislop D, Cartwright S. Social support in the workplace between teleworkers, office-based colleagues and supervisors. New Technol Work Employ. 2016;31:161–175. [Google Scholar]
- 32.d'Ettorre G Ceccarelli G Santinelli L, et al. Post-traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: a systematic review. Int J Environ Res Public Health. 2021;18:601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Roslan NS Yusoff MSB Razak AA, et al. Burnout prevalence and its associated factors among Malaysian healthcare workers during COVID-19 pandemic: an embedded mixed-method study. Healthcare (Basel). 2021;9:90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Taylor S Landry CA Rachor GS, et al. Fear and avoidance of healthcare workers: an important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord. 2020;75:102289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.JAA SantosDe los, Labrague LJ, The impact of fear of COVID-19 on job stress, and turnover intentions of frontline nurses in the community: a cross-sectional study in the Philippines. Dent Traumatol, 2021; 27: 52–59. [Google Scholar]
- 36.Montani F, et al. Appraisal of economic crisis, psychological distress, and work-unit absenteeism: a 1-1-2 model. J Bus Psychol. 2020;35:609–620. [Google Scholar]
- 37.Siegrist J, Wahrendorf M. Work Stress and Health in a Globalized Economy: The Model of Effort-Reward Imbalance. Cham, Switzerland: Springer; 2016. [Google Scholar]
- 38.Bakker AB, Demerouti E, Euwema MC. Job resources buffer the impact of job demands on burnout. J Occup Health Psychol. 2005;10:170–180. [DOI] [PubMed] [Google Scholar]
- 39.Kniffin KM, et al. COVID-19 and the workplace: implications, issues, and insights for future research and action. Am Psychol. 2021;76:63–77. [DOI] [PubMed] [Google Scholar]
- 40.Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. 1996;1:27–41. [DOI] [PubMed] [Google Scholar]
- 41.Parent-Lamarche A, Marchand A, Saade S. A multilevel analysis of the role personality play between work organization conditions and psychological distress. BMC Psychol. 2021;9:1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Allisey A, Rodwell J, Noblet A. An application of an extended effort-reward imbalance model to police absenteeism behaviour. Pers Rev. 2016;45:663–80. [Google Scholar]
- 43.Bourgeault IL. Le travail des femmes est largement invisible dans tous les domaines des soins de santé. Hoffpost Quebec. 2018. Available at: https://www.huffpost.com/archive/qc/entry/travail-femmes-largement-invisible_a_23429998. Accessed April 11, 2022. [Google Scholar]
- 44.Kessler RC Barker PR Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60:184–189. [DOI] [PubMed] [Google Scholar]
- 45.Matud MP, García MC. Psychological distress and social functioning in elderly Spanish people: a gender analysis. Int J Environ Res Public Health. 2019;16:341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Antczak E, Miszczyńska KM. Causes of sickness absenteeism in Europe—analysis from an intercountry and gender perspective. Int J Environ Res Public Health. 2021;18:11823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Thorsen SV Pedersen J Flyvholm MA, et al. Perceived stress and sickness absence: a prospective study of 17,795 employees in Denmark. Int Arch Occup Environ Health. 2019;92:821–828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Burmeister EA Kalisch BJ Xie B, et al. Determinants of nurse absenteeism and intent to leave: an international study. J Nurs Manag. 2019;27:143–153. [DOI] [PubMed] [Google Scholar]
- 49.Horesh D, Kapel Lev-Ari R, Hasson-Ohayon I. Risk factors for psychological distress during the COVID-19 pandemic in Israel: loneliness, age, gender, and health status play an important role. Br J Health Psychol. 2020;25:925–933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Løkke Nielsen AK. Determinants of absenteeism in public organizations: a unit-level analysis of work absence in a large Danish municipality. Int J Hum Resour Manag. 2008;19:1330–1348. [Google Scholar]
- 51.Wang Y, Kala MP, Jafar TH. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: a systematic review and meta-analysis. PLoS One. 2020;15:e0244630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Fu W Wang C Zou L, et al. Psychological health, sleep quality, and coping styles to stress facing the COVID-19 in Wuhan, China. Transl Psychiatry. 2020;10:225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Jamaludin II, You HW. Burnout in relation to gender, teaching experience, and educational level among educators. Educ Res Int. 2019;2019:1–5. [Google Scholar]
- 54.Wee LH Yeap LLL Chan CMH, et al. Anteceding factors predicting absenteeism and presenteeism in urban area in Malaysia. BMC Public Health. 2019;19:540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Becker C, Kirchmaier I, Trautmann ST. Marriage, parenthood and social network: subjective well-being and mental health in old age. PLoS One. 2019;14:e0218704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Marchand A, Demers A, Durand P. Does work really cause distress? The contribution of occupational structure and work organization to the experience of psychological distress. Soc Sci Med. 2005;61:1–14. [DOI] [PubMed] [Google Scholar]
- 57.Saruan NAM, Yusoff HM, Fauzi MFM. Family responsibilities and involuntary job absenteeism among nurses in teaching hospital. Malay J Public Health Med. 2019;19:38–46. [Google Scholar]
- 58.Bernstrøm VH, Houkes I. A systematic literature review of the relationship between work hours and sickness absence. Work Stress. 2018;32:84–104. [Google Scholar]
- 59.Klersy C Callegari A Martinelli V, et al. Burnout in health care providers of dialysis service in northern Italy—a multicentre study. Nephrol Dial Transplant. 2007;22:2283–2290. [DOI] [PubMed] [Google Scholar]
- 60.Mousteri V, Daly M, Delaney L. Underemployment and psychological distress: propensity score and fixed effects estimates from two large UK samples. Soc Sci Med. 2020;244:112641. [DOI] [PubMed] [Google Scholar]
- 61.Bowers A, et al. Loneliness influences avoidable absenteeism and turnover intention reported by adult workers in the United States. J Org Effect People Perform. 2022;9:312–335. [Google Scholar]
- 62.Sparks K, et al. The effects of hours of work on health: a meta-analytic review. In: Managerial, Occupational and Organizational Stress Research. London: Routledge; 2018:451–468. [Google Scholar]
- 63.Simard K, Parent-Lamarche A. Abusive leadership, psychological well-being, and intention to quit during the COVID-19 pandemic: a moderated mediation analysis among Quebec's healthcare system workers. Int Arch Occup Environ Health. 2022;95:437–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Muthén LK, Muthén B. MPlus User's Guide: Statistical Analysis With Latent Variables, User's Guide. Los Angeles: Muthén & Muthén; 2017. [Google Scholar]
- 65.Hoyle RH. Structural Equation Modeling: Concepts, Issues, and Applications. Newbury Park, CA: Sage; 1995. [Google Scholar]
- 66.Hayes AF. Partial, conditional, and moderated moderated mediation: quantification, inference, and interpretation. Community Monogr. 2018;85:4–40. [Google Scholar]
- 67.Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36:717–731. [DOI] [PubMed] [Google Scholar]
- 68.Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivar Behav Res. 2007;42:185–227. [DOI] [PubMed] [Google Scholar]
- 69.INSPQ . Détresse psychologique. Fiche 11—Kessler Psychological Distress Scale—6 items (K6). 2019. Available at: https://www.inspq.qc.ca/boite-outils-pour-la-surveillance-post-sinistre-des-impacts-sur-la-sante-mentale/instruments-de-mesure-standardises/questionnaires/detresse-psychologique. Accessed March 30, 2022.
- 70.Bambra C Egan M Thomas S, et al. The psychosocial and health effects of workplace reorganisation. 2. A systematic review of task restructuring interventions. J Epidemiol Community Health. 2007;61:1028–1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Rana W, Mukhtar S, Mukhtar S. Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J Psychiatr. 2020;51:102080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Chung JP, Yeung WS. Staff mental health self-assessment during the COVID-19 outbreak. East Asian Arch Psychiatry. 2020;30:34. [DOI] [PubMed] [Google Scholar]
- 73.De Brier N Stroobants S Vandekerckhove P, et al. Factors affecting mental health of health care workers during coronavirus disease outbreaks (SARS, MERS & COVID-19): a rapid systematic review. PLoS One. 2020;15:e0244052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Kisely S Warren N McMahon L, et al. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. BMJ. 2020;369:m1642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Gibson KR, O'Leary K, Weintraub JR. The little things that make employees feel appreciated. Harv Bus Rev. 2020. [Google Scholar]
- 76.Brun J-P, Laval C. Le pouvoir de la reconnaissance au travail: 30 fiches pratiques pour allier santé, engagement et performance. Paris, France: Eyrolles; 2018. [Google Scholar]
- 77.Galea S, Merchant RM, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med. 2020;180:817–818. [DOI] [PubMed] [Google Scholar]
- 78.Casler K, Bickel L, Hackett E. Separate but equal? A comparison of participants and data gathered via Amazon's MTurk, social media, and face-to-face behavioral testing. Comput Hum Behav. 2013;29:2156–2160. [Google Scholar]
- 79.Desrochers S, Sargent LD. Boundary/border theory and work-family Integration1. Org Manage J. 2004;11:40–48. [Google Scholar]
- 80.Ryan RM, Deci EL. Self-determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York: Guilford Publications; 2017. [Google Scholar]
- 81.Galanti T Guidetti G Mazzei E, et al. Work from home during the COVID-19 outbreak: the impact on employees' remote work productivity, engagement, and stress. J Occup Environ Med. 2021;63:e426–e432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Mehdi T., Morissette R., Working from home: productivity and preferences. 2021. Available at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2021001/article/00012-eng.htm. Accessed March 30, 2022.
- 83.INSPQ . Ligne du temps COVID-19 au Québec. Public Health Expertise and Reference Centre. 2022. Available at: https://www.inspq.qc.ca/covid-19/donnees/ligne-du-temps. Accessed April 22, 2022.