

Abstract
Objectives
We investigated the effectiveness of low-level laser therapy (LLLT) in lower extremity tendinopathy and plantar fasciitis on patient-reported pain and disability.
Design
Systematic review and meta-analysis.
Data sources
Eligible articles in any language were identified through PubMed, Embase and Physiotherapy Evidence Database (PEDro) on the 20 August 2020, references, citations and experts.
Eligibility criteria for selection of studies
Only randomised controlled trials involving participants with lower extremity tendinopathy or plantar fasciitis treated with LLLT were included.
Data extraction and synthesis
Random effects meta-analyses with dose subgroups based on the World Association for Laser Therapy treatment recommendations were conducted. Risk of bias was assessed with the PEDro scale.
Results
LLLT was compared with placebo (10 trials), other interventions (5 trials) and as an add-on intervention (3 trials). The study quality was moderate to high.
Overall, pain was significantly reduced by LLLT at completed therapy (13.15 mm Visual Analogue Scale (VAS; 95% CI 7.82 to 18.48)) and 4–12 weeks later (12.56 mm VAS (95% CI 5.69 to 19.42)). Overall, disability was significantly reduced by LLLT at completed therapy (Standardised Mean Difference (SMD)=0.39 (95% CI 0.09 to 0.7) and 4–9 weeks later (SMD=0.32 (95% CI 0.05 to 0.59)). Compared with placebo control, the recommended doses significantly reduced pain at completed therapy (14.98 mm VAS (95% CI 3.74 to 26.22)) and 4–8 weeks later (14.00 mm VAS (95% CI 2.81 to 25.19)). The recommended doses significantly reduced pain as an add-on to exercise therapy versus exercise therapy alone at completed therapy (18.15 mm VAS (95% CI 10.55 to 25.76)) and 4–9 weeks later (15.90 mm VAS (95% CI 2.3 to 29.51)). No adverse events were reported.
Conclusion
LLLT significantly reduces pain and disability in lower extremity tendinopathy and plantar fasciitis in the short and medium term. Long-term data were not available. Some uncertainty about the effect size remains due to wide CIs and lack of large trials.
PROSPERO registration number
CRD42017077511.
Keywords: Laser therapy, GENERAL MEDICINE (see Internal Medicine), REHABILITATION MEDICINE
Strengths and limitations of this study
This review was performed in conformance with a prospective published protocol, which included a plan for subgrouping the trials by laser dose.
There were no language restrictions; 2 (11%) of the included trials were reported in non-English language.
The review includes results from an unpublished trial.
The review features meta-analyses with direct comparisons between low-level laser therapy and placebo, other interventions and no intervention.
Only one reviewer extracted the data from the included trials, but the extracted data were checked for correctness by another reviewer.
Introduction
Tendinopathy and plantar fasciitis are disorders associated with substantial pain and loss of function in the lower extremity, especially prevalent in the athletic population but also common in the non-athletic population.1–3 The aetiology of tendinopathy and plantar fasciitis is multifactorial and not fully understood. Risk factors for tendinopathy include overuse, acute trauma, ageing and genetic predisposition.4 5 Known risk factors for plantar fasciitis are prolonged standing and jumping, reduced ankle dorsiflexion and obesity.6–9 Disorganised and degenerating collagen fibres, increased numbers of fibroblasts, altered composition of extracellular matrix proteins, formation of new vessels and rounding of tendon cells can be found in both tendinopathy and plantar fasciitis.10 11
Conservative treatment for lower extremity tendinopathy and plantar fasciitis includes an array of modalities and approaches. The effect of exercise therapy in tendinopathy is well-established, and any exercise type is preferential to wait-and-see in the earlier stages of tendinopathy.12 However, a superiority of exercise therapy compared with other interventions has not been demonstrated. The use of non-steroidal anti-inflammatory drugs (NSAIDs) are frequently recommended in the early stages of tendinopathy and plantar fasciitis,13–15 even though the effectiveness of these drugs in lower extremity tendinopathies has only been investigated in a few placebo-controlled trials.16–20 Moreover, NSAIDs have well known potentially fatal side effects, most importantly severe cardiovascular events and gastrointestinal toxicity.21 Low-level laser therapy (LLLT), also known as photobiomodulation therapy, is a quickly administered non-invasive intervention option free from negative side effects. LLLT is an athermic photochemical modality, where red or near-infrared light is used to stimulate tissue healing and reduce pain and inflammation.22–24 The working mechanisms of LLLT are partly established. There is evidence that LLLT increases adenosine triphosphate production,25 modulates the reactive oxygen species, and the induction of transcription factors.26–29 Furthermore, it has been demonstrated that LLLT inhibits the cyclooxygenase-2 gene expression and prostaglandin E2 (PGE2) production in tendons30 31 and inhibits matrix metalloproteinase activity.31 32 In addition, under application of LLLT, macrophages are more likely to act as phagocytes.33
There are heterogeneous results from clinical trials of LLLT on tendinopathies, and this may or may not be explained by a dose–response relationship.34–36 Variation in LLLT parameters, such as wavelength, power density, pulse structure, application method and time-point of assessment may affect the treatment outcome. The World Association for Laser Therapy (WALT) has published treatment recommendations regarding the minimum LLLT doses required to reach a positive result.37 38 In a systematic review by our research group regarding the effectiveness of LLLT in knee osteoarthritis, a significant dose–response relationship was discovered when the included trials were subgrouped using the WALT treatment recommendations.39 Furthermore, in a more recent placebo-controlled trial, we found some evidence that an upper limit for the effectiveness of LLLT exists in knee osteoarthritis.40 These clinical observations are in line with the results of several in vivo and in vitro trials.41–44 Whether such biphasic laser dose–response relationship exists in tendon disorders is unclear. Prior systematic reviews have investigated LLLT in Achilles tendinopathy or plantar fasciitis.12 45–49 Unfortunately, these reviews have one or more substantial limitations, such as a lack of a dose–response analysis,12 an exclusion of relevant trials reported in non-English languages45–48 or the mistake of synthesising the results of highly heterogenious studies using the fixed effects meta-analysis model.49 Thus, the evidence regarding the effectiveness of LLLT on pain and disability in lower limb tendinopathy and plantar fasciitis is still somewhat unclear. Therefore, the objectives of the current review were to estimate the effectiveness of LLLT in tendinopathy and plantar fasciitis on patient-reported pain and disability using a dose–response analysis.
Methods
This review was conducted in adherence to a prospectively registered PROSPERO protocol and is reported in accordance with the Preferred Reporting Items of Systematic reviews and Meta-Analysis statement 2009.50
Literature search and selection of studies
We included randomised clinical trials in which the effectiveness of LLLT in tendon disorders of the lower extremity or plantar fasciitis was compared with sham (placebo) LLLT, other interventions or no intervention, in terms of patient-reported pain and/or disability. There were no restrictions regarding publication date and language.
A search for eligible reports of trials were conducted in the databases PubMed, Embase and Physiotherapy Evidence Database (PEDro) on the 20 August 2020. Furthermore, references from relevant systematic reviews46–49 and all the included trials were screened, and experts in the field were asked to provide additional published and unpublished trials. Abstracts were not included. The PubMed search string is included in the online supplemental material.
bmjopen-2021-059479supp001.pdf (1MB, pdf)
Two independent reviewers (IFN and MBS) read the titles/abstracts of the publications identified by the search. Any article judged potentially eligible by a reviewer was retrieved in full text. The same two reviewers evaluated the full texts of all the potentially eligible articles and made a careful decision to include or exclude each article, with close attention to the eligibility criteria. Any article not fulfilling the eligibility criteria was excluded and had its details listed with reason for exclusion (online supplemental material). Selection disagreements were resolved by discussion to consensus with the option of a third person’s (JJ) final decision if necessary.
Risk of bias analysis
Two reviewers (IFN and MBS) independently assessed the risk of bias of the included trials with the 0–10 points PEDro scale.51 This was done on outcome level, and since the outcomes of interest were patient-assessed pain and disability, the participants were considered the assessors. Therefore, the assessors can only be blinded in placebo-controlled trials. When risk-of-bias disagreements could not be resolved by discussion, a third reviewer (JJ) made the final consensus-based decision. The trials were labelled as being of ‘high’, ‘moderate’ or ‘poor’ methodological quality if they had a total PEDro score of ≥7, 5–6 or ≤4, respectively.52 Risk of small study bias was assessed with a funnel plot and by comparing the difference between the point effect estimates from random and fixed effects meta-analyses.
Data extraction and meta-analysis
Extraction of the following information was mandatory: number of participants allocated to laser and control groups, participant characteristics, type and duration of interventions, laser-specific application information (location of application, wavelength, energy density per treated spot, number of spots treated, mean power density per treated spot, treatment time per spot, treated area, laser sessions per week and total number of laser sessions), selected outcome measurement scales for data extraction, time-points of assessments, effect estimates and adverse events.
The data collection was handled in a two-person procedure by IFN and MBS. One reviewer entered all the data in Excel sheets, and the data were subsequently checked for correctness by another reviewer. If data extraction disagreements could not be resolved by discussion, a third reviewer (JMB) made the final consensus-based decision.
All the meta-analyses were conducted using random effects models, weighting the individual trial results relatively even when statistical heterogeneity is present.53
The pain results were synthesised using the mean difference (MD) method as this method allows for change and final scores to be combined.54 Pain scores reported on the Visual Analogue Scale (VAS) and on the Numeric Rating Scale highly correlates55 and were thus considered the same. Patient-reported disability results were synthesised with the Standardised Mean Difference (SMD) method using change scores solely.54 According to Cohen, a SMD of 0.2, 0.5 and 0.8 can be considered small, moderate and large, respectively.54
Heterogeneity was measured using I2-statistics (inconsistency).56 An inconsistency level of 25%, 50% and 75% would be considered low, moderate and high, respectively.57 Standard deviations (SDs) for meta-analysis were extracted or estimated from other variance data in the following prioritised order: SD, standard error (SE), 95% Confidence interval (CI), pvalue, interquatile range (IQR), median of correlations, visually from graph, correlation of 0.6 or mean of SDs from similar trials.
Trials were subgrouped by laser dose using the WALT treatment recommendations,58 59 as specified in the a priori protocol. WALT recommends irradiating minimum of 2–3 points on the tendon or fascia. In Achilles and patellar tendinopathy, the recommended dose with 904 nm wavelength laser is minimum 2 J/point. When using 780–860 nm wavelength laser, the minimum dose is 4 J/point. In plantar fasciitis, the recommended minimum dose is 2 J/point with a 904 nm wavelength laser or 4 J/point with 780–860 nm wavelength laser. We subgrouped the trials as recommended laser dose or non-recommended laser dose when possible. If the trial reports lacked sufficient dose parameters to be identified as recommended or non-recommended laser dose, they were categorised as unclear laser dose.
Two time-points of assessment were selected for analysis, that is, immediately after the end of LLLT and last time-point of assessment 2–12 weeks after completed LLLT (follow-up).
IFN and MBS performed the meta-analyses using Excel 2016 (Microsoft) and Review Manager V.5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Patient and public involvement
Patients or the public were not involved in the conceptualisation or carrying out of this research.
Results
A total of 870 records were identified in the search, of which 18 reports of trials (n=784) were included in review and meta-analysis (figure 1 and table 1). LLLT was applied to participants with patellar tendinopathy in 2 trials, Achilles tendinopathy in 5 trials and plantar fasciitis in 11 trials. LLLT was compared with placebo in 10 trials, other interventions in 5 trials and as an adjunct intervention in 3 trials. Two trials were reported in non-English language, and one trial was unpublished (Naterstad et al.). The excluded articles were listed with reasons for omission (online supplemental material). The mean age of the participants was 43.6 years (minimum<18, maximum 54.5, data from 14 trials), and the mean baseline pain intensity was 64.2 mm on the VAS (minimum 19.3 mm, maximum 85 mm, data from 18 trials). No adverse events were reported by any of the trial authors. None of the trial authors declared that they had received funding from the laser industry.
Figure 1.
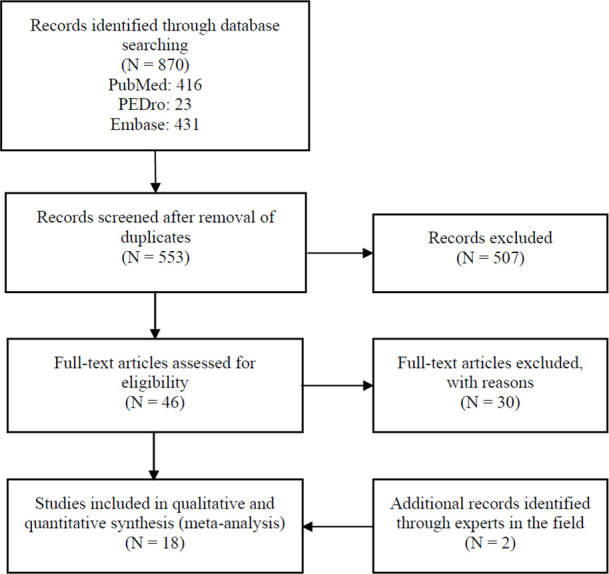
Flow chart illustrating the trial identification process. PEDro, physiotherapy evidence database.
Table 1.
Characteristics of the included trials
| First author, year | Participants at baseline (intervention) | Participants at baseline (control) | Intervention versus control | Outcome and time of reassessment after baseline (time used for analysis in bold) |
| Patellar tendinopathy | ||||
| Liu 201469, LLLT versus ET | n: 7 Age years: ≥ 18, ≤ 23 VAS pain mm: 67.9±13.2 |
n: 7 Age years: ≥ 18, ≤ 23 VAS pain mm: 65.7±15.4 |
4 weeks of LLLT versus 4 weeks of eccentric ET | Pain: VAS Disability: modified-VISA Reassessment: 4 weeks |
| Liu 201469, LLLT+ET versus ET | n: 7 Age years: ≥ 18, ≤ 23 VAS pain mm: 67.9±12.2 |
n: 7 Age years: ≥ 18, ≤ 23 VAS pain mm: 65.7±15.4 |
4 weeks of LLLT and eccentric ET versus 4 weeks of eccentric ET | Pain: VAS Disability: modified-VISA Reassessment: 4 weeks |
| Stergioulas 200360 | n: 23 Age years: 29.2±13.4 VAS pain mm: 81.7±13.4 |
n: 21 Age years: 29.8±13.8 VAS pain mm: 75.9±18.8 |
2 weeks of LLLT versus 2 weeks of sham LLLT | Pain: VAS Disability: Functional Index Questionnaire Reassessment: 2 and 6 weeks |
| Achilles tendinopathy | ||||
| Darre 199461 | n: 46 Age years: ≥ 18 VAS pain mm: 58.5±37.9 |
n: 43 Age years: ≥ 18 VAS pain mm: 72±34.3 |
2.4 weeks of LLLT versus 2.4 weeks of sham LLLT | Pain: VAS Disability: - Reassessment: 2.4 weeks |
| Naterstad† | n: 20 Age years: 45.4±14.7 VAS pain mm: 52.9±26.1 |
n: 21 Age years: 45.8±13.9 VAS pain mm: 53.8±26.7 |
4 weeks of LLLT and cryotherapy and 12 weeks of eccentric and concentric ET versus 4 weeks of sham LLLT and cryotherapy and 2 weeks of eccentric and concentric ET | Pain: THIP VAS most painful activity Disability: THIP VAS ADL Reassessment: 4 and 12 weeks |
| Stergioulas 200868 | n: 20 Age years: 30.1±4.8 VAS pain mm: 79.8±9.5 |
n: 20 Age years: 28.8±4.8 VAS pain mm: 81.8±11.6 |
8 weeks of LLLT and eccentric ET versus 8 weeks of sham LLLT and eccentric ET | Pain: VAS during activity Disability: - Reassessment: 4, 8 and 12 weeks |
| Tumilty 200862 | n: 10 Age years: 41.4±7.6 VAS pain mm: 47.8±25.9 |
n: 10 Age years: 42.5±8.5 VAS pain mm: 39±20.2 |
4 weeks of LLLT and 12 weeks of eccentric ET versus 4 weeks of sham LLLT and 12 weeks of eccentric ET | Pain: VAS in morning Disability: - Reassessment: 4 and 12 weeks |
| Tumilty 201263 | n: 20 Age years: 45.6±9.1 NRS pain mm: 21.1±1.2 |
n: 20 Age years: 46.5±6.4 NRS pain mm: 19.3±0.9 |
4 weeks of LLLT and 12 weeks of eccentric ET versus 4 weeks of sham LLLT and 12 weeks of eccentric ET | Pain: NRS Disability: - Reassessment: 4, 12 and 52 weeks |
| Plantar fasciitis | ||||
| Basford 199864 | n: 16 Age years: 42.5 (26–64)* VAS pain mm: 57.9 (22.2–97)* |
n: 15 Age years: 42 (33–51)* VAS pain mm: 46.6 (4–86)* |
4 weeks of LLLT versus 4 weeks of sham LLLT | Pain: Pain when walking in morning Disability: limping in morning Reassessment: 2, 4 and 8 weeks |
| Cinar 201770 | n: 29 Age years: 46.6±10.1 VAS pain mm: 61.3±19.4 |
n: 22 Age years: 44.2±9.7 VAS pain mm: 54.9±19.7 |
3 weeks of LLLT and stretching versus 3 weeks of stretching | Pain: VAS Disability: AOFAS-F activity limitations Reassessment: 3 and 12 weeks |
| Cinar 201871 | n: 24 Age years: 46.5±10.3 NRS pain mm: 6.3±1.4 |
n: 17 Age years: 44±8.6 NRS pain mm: 6.2±2.1 |
3 weeks of LLLT and 12 weeks of stretching versus 12 weeks of stretching | Pain: NRS Disability: - Reassessment: 3 and 12 weeks |
| Cinar 201871, ESWT | n: 24 Age years: 46.5±10.3 NRS pain mm: 6.3±1.4 |
n: 25 Age years: 45.4±9.7 NRS pain mm: 6.7±2.7 |
3 weeks of LLLT and 12 weeks of stretching versus 3 weeks of ESWT (2000 mJ/mm2, session once per week) and 12 weeks of stretching | Pain: NRS Disability: - Reassessment: 3 and 12 weeks |
| Elsehrawy 201872 | n: 23 Age years: 46.4±10 VAS pain: 85±8 |
n:23 Age years: 46±10.2 VAS pain: 82±15 |
3 weeks of LLLT and stretching versus 2 weeks of ESWT (2050 shocks/min, 10 Hz, 2.5 bars once per week) and stretching | Pain: VAS Disability: FFI disability subscale Reassessment: 4 weeks |
| Kiritsi 201065 | n: 15 Age years: 41±12 VAS pain mm: 67±8.3 |
n: 15 Age years: 41±12 VAS pain mm: 67±9.3 |
6 weeks of LLLT versus 6 weeks of sham LLLT | Pain: ADL VAS Disability: - Reassessment: 6 weeks |
| Koteeswaran 202075 | n: 15 Age years: 30–60 NRS pain: 74.7±11.9 |
n: 15 Age years: 30–60 NRS pain: 72.7±8 |
2 weeks of LLLT and stretching versus 2 weeks of TUS and stretching | Pain: NRS Disability: FAAM Reassessment: 2 weeks |
| Lamba 201366 | n: 40 Age years: 40.9±10.4 VAS pain mm: 57.5±10.8 |
n: 40 Age years: 40.4±9.7 VAS pain mm: 62±7.6 |
4 weeks of LLLT and stretching versus 4 weeks of sham LLLT and stretching | Pain: VAS Disability: - Reassessment: 1,2, 3 and 4 weeks |
| Macias 201567 | n: 37 Age years: ≥ 18 VAS pain mm: 69.1±12.7 |
n: 32 Age years: ≥ 18 VAS pain mm: 67.6±11.8 |
3 weeks of LLLT versus 3 weeks of sham LLLT | Pain: VAS heel pain Disability: FFI disability subscale 8 weeks Reassessment: 1, 2, 3, 6 and 8 weeks |
| Sanmak 201973 | n: 17 Age years: 53* VAS pain mm: 70* |
n: 17 Age years: 49* VAS pain mm: 80* |
4 weeks of LLLT versus 3 weeks of ESWT (2 bar with 2000 shocks/min at 10 Hz once per week) | Pain: VAS Reassessment: 4 and 8 weeks |
| Ulusoy 201774, TUS | n: 20 Age years: 53.4±14.7 VAS pain mm: 68.7±12.5 |
n: 20 Age years: 51.0±9.6 VAS pain mm: 66.6±1.1 |
3 weeks of LLLT and 7 weeks of ET and stretching versus 3 weeks of TUS (1 mHz; 2 W/cm2) and 7 weeks of ET and stretching | Pain: VAS in morning Disability: - Reassessment: 7 weeks |
| Ulusoy 201774, ESWT | n: 20 Age years: 53.4±14.7 VAS pain mm: 68.7±12.5 |
n: 20 Age years: 54.4±6.9 VAS pain mm: 66±11.2 |
3 weeks of LLLT and 7 weeks of ET and stretching versus 3 weeks of ESWT (2.5 bar with 2000 shocks/min at 10 Hz three times per week) and 7 weeks of ET and stretching | Pain: VAS in morning Disability: - Reassessment: 7 weeks |
| Yüzer 200676 | n: 24 Age years: 49.6±1.2 VAS pain mm: 80±12 |
n: 30 Age years: 51.5±11.5 VAS pain mm: 76±15 |
1.4 weeks of LLLT versus steroid injection | Pain: VAS Disability: - Reassessment: 5.4, 13.4 and 25.4 weeks |
Numbers for age and pain are means±SD, unless otherwise indicated.
*Median with or without IQR.
†Naterstad et al. Efficacy of Low-level Laser Therapy as an addition to exercise and cryotherapy in chronic Achilles tendinopathy: a double-blinded randomised controlled trial.
ADL, activity of daily living; AOFAS-F, American Orthopedic Foot and Ankle Score Function; ESWT, Extracorporeal Shockwave Therapy; ET, exercise therapy; FAAM, foot and ankle ability measurement questionnaire; FFI, Foot Function Index; LLLT, Low-Level Laser Therapy; NRS, Numeric Rating Scale; THIP, Tendinopathy Health Impact Profile; TUS, therapeutic ultrasound; VAS, Visual Analogue Scale.
LLLT was compared with placebo LLLT in 10 trials,60–68 and exercise therapy or stretching exercises was applied as a cointervention in five of these trials. LLLT was compared with exercise therapy or stretching exercises in three trials.69–71 A comparison between LLLT and Extracorporeal Shockwave Therapy (ESWT) in plantar fasciitis was performed in four trials.71–74 LLLT was compared with therapeutic ultrasound in two trials74 75 and steroid injection in one trial.76 Recommended laser doses were applied in at least 11 trials,60–62 65 66 68–71 74 and a non-recommended dose was used in at least 1 trial.63 We were unable to categorise the laser doses in the remaining six trials64 67 72 73 75 76 due to inadequately or missing descriptions of laser parameters (table 2). Two different laser doses were applied in the same session in two of the trials.65 69
Table 2.
LLLT characteristics of the included trials
| First author, year | Wave-length (nm) | Mean output power (mW) | Seconds per treatment spot (s) | Joules per treatment spot (J) | Number of spots treated | Number of sessions/Weeks | Dose recommended by WALT |
| Patellar tendinopathy | |||||||
| Liu 201469 | 810 810 |
200 200 |
600 300 |
- - |
1* 2 |
24/4 | Yes |
| Stergioulas 200360 | 904 | 50 | 300 | 1.2 | 10 | 10/2 | Yes |
| Achilles tendinopathy | |||||||
| Darre 199461 | 830 | 30 | – | 4 | 4 | 12/2.5 | Yes |
| Naterstad‡ | 904 | 60 | 50 | 3 | 6 | 12/4 | Yes |
| Stergioulas 200868 | 820 | 30 | – | 0.9 | 6 | 12/8 | Yes |
| Tumilty 200862 | 810 | 100 | 30 | 3 | 6 | 12/4 | Yes |
| Tumilty 201263 | 810 | 7 | 30 | 0.21 | 6 | 12/4 | No |
| Plantar fasciitis | |||||||
| Basford 199864 | 830 | 30 | – | – | 3 † | 12/4 | Unclear |
| Cinar 201770 | 830 | 100 | 80 | 5.6 | 5 | 10/3 | Yes |
| Cinar 201871 | 830 | 100 | 80 | 5.6 | 5 | 10/3 | Yes |
| Elsehrawy 201872 | 830 | – | – | – | 3 † | 6/3 | Unclear |
| Kiritsi 201065 | 904 904 |
60 60 |
– – |
8.4 – |
1* 2 † |
18/6 | Yes |
| Koteeswaran 202075 | 830 | – | 180 | – | 3 | 9/3 | Unclear |
| Lamba 201366 | 820 | 100 | 80 | – | 3 † | 12/4 | Yes |
| Macias 201567 | 635 | 17 | 600 | – | 3 | 6/3 | Unclear |
| Sanmak 201973 | 685 | 30 | 60 | – | 2 † | 12/4 | Unclear |
| Ulusoy 201774 | 830 | 50 | 200 | – | 3 † | 15/3 | Yes |
| Yüzer 200676 | 904 | – | 30 | – | – | 10/1.4 | Unclear |
*Two different dosages applied within the same session.
†Naterstad et al. Efficacy of Low-level Laser Therapy as an addition to exercise and cryotherapy in chronic Achilles tendinopathy: a double-blinded randomised controlled trial.
‡One or more spots/areas treated with movement of the laser probe.
LLLT, Low-Level Laser Therapy; WALT, World Association for Laser Therapy.
Overall pain and disability results — LLLT versus any control
Data allowing for a meta-analysis of an immediate pain change were available from 16 trials with recommended, non-recommended or unknown laser dosing.
Overall, pain was significantly reduced by LLLT over any control immediately after completed therapy (13.15 mm VAS (95% CI 7.82 to 18.48), I2=65%, n=784) (figure 2) and at follow-ups 4–12 weeks later (12.56 mm VAS (95% CI 5.69 to 19.42), I2=48%, n=556) (figure 3).
Figure 2.

Overall pain results immediately after completed therapy—LLLT versus any control. AT, Achilles tendinopathy; CT, cryotherapy; ESWT, Extracorporeal Shock Wave Therapy; ET, exercise therapy; I, insoles; LLLT, Low-Level Laser Therapy; PF, plantar fasciitis; PT, patellar tendinopathy; S, stretching; TU, Therapeutic Ultrasound.
Figure 3.

Overall pain results at follow-ups—LLLT versus any control. AT, Achilles tendinopathy; CT, cryotherapy; ESWT, Extracorporeal Shock Wave Therapy; ET, exercise therapy; I, insoles; LLLT, Low-Level Laser Therapy; PF, plantar fasciitis; PT, patellar tendinopathy; S, stretching; TU, therapeutic ultrasound.
Overall, the disability results immediately after completed therapy significantly favoured LLLT over any control (SMD=0.39 (95% CI 0.09 to 0.7), I2=30%, n=260) (figure 4). A disability reduction by LLLT remained significant at follow-ups 4–9 weeks after completed therapy (SMD=0.32 (95% CI 0.05 to 0.59), I2=4%, n=222) (figure 5).
Figure 4.

Overall disability results immediately after completed therapy—LLLT versus any control. AT, Achilles tendinopathy; CT, cryotherapy; ESWT, Extracorporeal Shock Wave Therapy; ET, exercise therapy; I, insoles; LLLT, Low-Level Laser Therapy; PF, plantar fasciitis; PT, patellar tendinopathy; S, stretching; TU, therapeutic ultrasound.
Figure 5.

Overall disability results at follow-ups—LLLT versus any control. AT, Achilles tendinopathy; CT, cryotherapy; ET, exercise therapy; I, insoles; LLLT, Low-Level Laser Therapy; PF, plantar fasciitis; PT, patellar tendinopathy; S, stretching.
Overall and subgroup pain results—LLLT versus placebo control
Overall, pain was significantly reduced by LLLT over placebo control immediately after completed therapy (11.48 mm VAS (95% CI 2.68 to 20.28), I2=73%, n=507) (figure 2) and during follow-ups 4–8 weeks after completed therapy (13.62 mm VAS (95% CI 2.18 to 25.06), I2=68%, n=277) (figure 3).
The recommended laser doses significantly reduced pain compared with placebo immediately after completed therapy (14.98 mm VAS (95% CI 3.74 to 26.22), I2=67%, n=367) (figure 6). A non-recommended laser dose from a single trial provided no significant pain reduction compared with placebo immediately after completed therapy (−3.0 mm VAS (95% CI −11.17 to 5.17), n=40) (figure 6). Trials with unknown laser doses significantly favoured LLLT over placebo control immediately after completed therapy (10.83 mm VAS (95% CI 2.44 to 19.21), I2=0%, n=100). The between-subgroup difference was significant (p=0.02) (figure 6).
Figure 6.

Subgroup pain results immediately after completed therapy—LLLT versus placebo control. AT, Achilles tendinopathy; CT, cryotherapy; ET, exercise therapy; LLLT, Low-Level Laser Therapy; PF, plantar fasciitis; PT, patellar tendinopathy; S, stretching.
At follow-ups 4–8 weeks after completed therapy, the recommended laser doses significantly reduced pain compared with placebo (14.00 mm VAS (95% CI 2.81 to 25.19), I2=5%, n=136) (online supplemental figure S1). A non-recommended laser dose provided in a single trial did not significantly reduce pain compared with placebo at follow-up 8 weeks after completed therapy (0.0 mm VAS (95% CI −7.62 to 7.62), n=40) (online supplemental figure S1). At follow-ups 4–5 weeks after completed therapy, trials with unknown laser doses demonstrated a significant pain reduction by LLLT compared with placebo (23.94 mm VAS (95% CI 14.39 to 33.48), I2=0%, n=97) (online supplemental figure S1). The between-subgroup difference was significant (p<0.001) (online supplemental figure S1).
Overall and subgroup pain results—LLLT versus other interventions
Overall, pain was significantly reduced by LLLT compared with other interventions immediately after completed therapy (13.23 mm VAS (95% CI 4.07 to 22.39), I2=66%, n=173) (figure 2). Follow-up results of pain 4–12 weeks after completed therapy favoured LLLT over other interventions, but not significantly (9.41 mm VAS (95% CI −0.44 to 19.26), I2=16%, n=193) (figure 3).
The recommended laser doses were compared with exercise therapy in one trial and ESWT in another trial immediately after completed therapy and the pain results favoured LLLT, but not significantly (13.91 mm VAS (95% CI −1.34 to 29.15), I2=65%, n=63) (online supplemental figure S4).
The pain results from three trials with unknown laser doses, in which two groups received ESWT and one group received therapeutic ultrasound, favoured LLLT immediately after completed therapy, but not significantly (12.88 mm VAS (95% CI −1.29 to 27.04), I2=77%, n=110) (online supplemental figure S4).
At follow-ups 4–12 weeks after completed therapy, pain was significantly lowered by the recommended laser doses compared with other interventions (15.90 mm VAS (95% CI 2.30 to 29.51), I2=0%, n=103) (online supplemental figure S5). Pain was not significantly lowered by unknown laser doses compared with other interventions at follow-ups 4–12 weeks after completed therapy (2.93 mm VAS (95% CI −15.8 to 21.67), I2=52%, n=87) (online supplemental figure S5).
Subgroup pain results—LLLT versus no intervention
Pain was significantly lowered by the recommended laser doses when used as an adjunct to exercise, stretching and insoles over exercise, stretching and insoles alone, both immediately after completed therapy (18.15 mm VAS (95% CI 10.55 to 25.76), I2=0%, n=104) (online supplemental figure S2) and at follow-up 9 weeks after completed therapy (19.67 mm VAS (95% CI 5.16 to 34.18), I2=0%, n=80) (online supplemental figure S3).
Overall and subgroup disability results—LLLT versus placebo control
Overall, the disability results favoured LLLT over placebo control immediately after completed therapy, but not significantly (SMD=0.24 (95% CI −0.18 to 0.58), I2=0%, n=107) (figure 4). The same applied to the follow-up results 4–8 weeks after completed therapy (SMD=0.19 (95% CI −0.11 to 0.49), I2=0%, n=173) (online supplemental figure S6).
The disability results immediately after completed therapy favoured the recommended laser doses over other interventions, but not significantly (SMD=0.25 (95% CI −0.21 to 0.7), I2=0%, n=76) (online supplemental figure S7). The same applied to unknown laser doses compared with placebo control immediately after completed therapy (SMD=0.10 (95% CI −0.61 to 0.8), n=31) (online supplemental figure S7).
At follow-ups 4–8 weeks after completed therapy, the disability results favoured the recommended laser doses over other interventions, but not significantly (SMD=0.24 (95% CI −0.21 to 0.7), I2=0%, n=76) (online supplemental figure S6). The same applied to the unknown laser doses compared with placebo-control immediately after completed therapy (SMD=0.14 (95% CI −0.26 to 0.54), I2=0%, n=107) (online supplemental figure S6).
Overall and subgroup disability results—LLLT versus other interventions
The overall disability results immediately after completed therapy favoured LLLT, but not significantly (SMD=0.58 (95% CI −0.11 to 1.27), I2=56%, n=90) (figure 4).
The recommended laser doses neither provided a significant disability reduction compared with other interventions immediately after completed therapy (SMD=0.20 (95% CI −0.85 to 1.25), n=14) (online supplemental figure S8). The same applied to unknown laser doses compared with other interventions immediately after completed therapy (SMD=0.73 (95% CI −0.26 to 1.72), n=76) (online supplemental figure S8).
Subgroup disability results—LLLT versus no intervention
The disability results of the recommended laser doses applied as an adjunct to exercise therapy or stretching immediately after completed therapy favoured LLLT, but not significantly (SMD=0.68 (95% CI −0.49 to 1.85), I2=69%, n=61) (online supplemental figure S9). At follow-up 9 weeks after completed therapy, disability was significantly lowered by the recommended laser doses as an adjunct to stretching and insoles compared with exercise therapy and insoles alone (SMD=0.82 (95% CI 0.24 to 1.41), n=49) (online supplemental figure S10).
Sensitivity analysis of laser dose categorisation
The irradiation procedure by Darre et al61 was judged as a recommended laser dose, based on the reported dose parameters in the paper. However, the dose description is somewhat sparse and could be misinterpreted. If the study by Darre et al was allocated to the unknown laser dose subgroup, the statistical heterogeneity would be eliminated in the recommended laser dose group and the estimated pain reduction would be increased to 21.12 mm VAS ((95% CI 14.94 to 27.31), I2=0%, n=278) versus placebo immediately after completed therapy (online supplemental figure S11).
Risk of bias within studies
Ten of the included trials were found to be of high methodological quality, and the remaining eight included trials were found to be of moderate methodological quality (table 3). All the trials featured adequate randomisation. Allocation concealment was sufficient in 11 (61%) of the trials. The groups were similar at baseline in 15 (83%) of the trials. The participants were blinded in 9 (50%) of the trials. The therapists were blinded in 5 (28%) of the trials, all of which were placebo controlled. The assessors were blinded in 7 (39%) of the trials, all of which were placebo controlled. Outcome data were available from more than 85% of the participants in 14 (78%) of the trials. An intention-to-treat analysis was used in 10 (56%) of the trials. A between-group statistical comparison was performed in all the trials. Point measures and variability outcome data were stated in 17 (94%) of the trial reports.
Table 3.
PEDro score
| Study ID | Item number | Total | Quality | ||||||||||
| 1* | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Basford 199864 | + | + | – | + | + | – | + | + | – | + | + | 7 | High |
| Cinar 201770 | + | + | + | + | – | – | – | + | + | + | + | 7 | High |
| Cinar 201871 | + | + | + | + | – | – | – | + | + | + | + | 7 | High |
| Darre 199461 | + | + | + | – | + | + | – | – | – | + | – | 5 | Moderate |
| Elsehrawy 201872 | + | + | – | + | – | – | – | + | – | + | + | 5 | Moderate |
| Kiritsi 201065 | + | + | + | + | + | + | + | – | – | + | + | 8 | High |
| Koteeswaran 202075 | + | + | – | + | – | – | – | + | + | + | + | 6 | Moderate |
| Lamba 201366 | + | + | – | + | + | – | – | + | – | + | + | 6 | Moderate |
| Liu 201469 | + | + | – | + | – | – | – | + | + | + | + | 6 | Moderate |
| Macias 201567 | + | + | + | + | + | – | + | + | + | + | + | 9 | High |
| Naterstad | + | + | + | + | + | + | + | + | + | + | + | 10 | High |
| Sanmak 201973 | + | + | + | + | – | – | – | + | + | + | + | 7 | High |
| Stergioulas 200360 | + | + | – | + | + | – | + | – | – | + | + | 6 | Moderate |
| Stergioulas 200868 | + | + | + | + | + | – | – | – | + | + | + | 8 | High |
| Tumilty 200862 | + | + | + | + | + | + | + | + | + | + | + | 10 | High |
| Tumilty 201263 | + | + | + | + | + | + | + | + | + | + | + | 10 | High |
| Ulusoy 201774 | + | + | – | + | – | – | – | + | – | + | + | 5 | Moderate |
| Yüzer 200676 | + | + | + | + | – | – | – | – | – | + | + | 5 | Moderate |
- Eligibility criteria specified.
- Random allocation.
- Concealed allocation.
- Groups similar at baseline.
- Subject blinding.
- Therapist blinding.
- Assessor blinding.
- Less than 15% dropout.
- Intention-to-treat analysis.
- Between-group statistical comparisons.
- Point measures and variability data.
*Item not included in the mean score.
PEDro, Physiotherapy Evidence Database.;
The lack of therapist and assessor blinding were the two most obvious methodological inadequacies. However, risk-of-bias subgroup analyses performed post-hoc revealed that there was no significant interaction between the effect estimates and the lack of blinding (online supplemental figures S12 and S13).
Risk-of-bias across studies (small study bias)
In a random effects model, small and large trials are weighted relatively even when statistical heterogeneity is present. In a fixed effects model, the heterogeneity is ignored and will not influence the weights. Smaller studies in meta-analyses tend to show more positive results than larger trials.77 However, there was almost no difference between the pain results of the two meta-analysis models, indicating that no small study bias exists (online supplemental figures S14 and S15). Likewise, there was no obvious asymmetry in a funnel plot based on the same meta-analyses of pain, indicating that no small study bias was present (online supplemental figures S16).
Discussion
We investigated the effectiveness of LLLT in tendon and aponeurosis disorders of the lower extremity. Our overall meta-analysis results demonstrated that pain and disability were statistically significantly reduced by LLLT compared with any control both immediately after completed therapy and in the follow-up period, that is, 4–12 weeks after completed therapy for pain and 4–8 weeks after completed therapy for disability.
Like in our previous meta-analysis of LLLT in knee osteoarthritis,39 we subgrouped the included trials in the current review using the WALT treatment recommendations.58 59 Compared with placebo control, the recommended laser doses in the current review generally had a larger pain-relieving effect than non-recommended laser both immediately after therapy and in the follow-up period. Similarly, the recommended laser doses had a significant pain-relieving effect as an adjunct to exercise therapy, stretching and insoles both immediately after completed therapy and in the follow-up period. Compared with other treatment modalities, the recommended laser doses were significantly superior, but only at follow-up and only as a pain treatment.
The minimal clinically important improvement (MCII) for pain expressed on the VAS or NRS has not been established for tendinopathy in the lower extremity,78 even though pain is a prominent feature of this condition. In plantar fasciitis, the MCII for VAS pain has been estimated to be 8 mm for average pain,79 and our results are above this threshold in all comparisons.
As for disability, we found that LLLT overall had a small and significant effect both immediately after completed therapy and in the follow-up period. Compared with placebo, there were no significant effect of LLLT on disability immediately after completed therapy and at follow-ups. Only Cinar et al70 provided follow-up data on disability regarding LLLT as an add-on to exercise therapy. They found a large and significant positive effect on disability 12 weeks after completed therapy; however, their results are based only on 49 participants,70 and thus this meta-analysis result should be interpreted with caution.
We were unable to dose categorise the study by Macias et al,67 since they used a laser within the visible spectrum (635 nm), which is not mentioned in the WALT treatment guidelines. Light in the red wavelengths (600–700 nm) penetrates the tissue to a lesser extent than light with a wavelength of 700–1000 nm.80 Macias et al used a relatively low mean output power, but they stated that they irradiated the tissue for 600 s and achieved a significant pain reduction. The methodological quality of their trial67 was categorised as high, with a PEDro score of 9.
Sanmak et al73 also used a laser within the red spectrum, but they applied a much smaller dose. Sanmak et al73 compared LLLT with ESWT in plantar fasciitis and found no difference between the groups regarding pain immediately after treatment, but an insignificant better result for ESWT 4 weeks after completed treatment. Comparing LLLT to ESWT, we would expect different effect-time profiles for pain alleviation, as the effect of ESWT might be greater at later time-points.81 Sanmak et al73 applied LLLT in a circular motion on the insertion site of the plantar fascia for 60 s and along the fascia for another 60 s. They stated that they irradiated the tissue with 2 J/cm2, which according to our calculation (Watt*seconds) corresponds to a relatively low mean output power of 18 mW/cm2. Moving the laser probe during irradiation will yield a smaller laser dose per treated cm2, and larger movement will for instance reduce the energy delivered per treated cm2. Additionally, the skin underneath the heel is thick,82 and thus absorbs a large percentage of the laser.
We did not identify any trials focusing on trochanter tendinopathy, peroneal or tibialis posterior tendinopathy. In a double-blinded randomised trial by Lögdberg-Andersson et al,83 the effect of a 904 nm wavelength laser in participants with trochanteritis or myofascial pain was investigated. They found a significant positive effect compared with placebo on pain expressed on a VAS and with algometry, both at the end of treatment and 4 weeks after.83 This trial was not included in our review, since we were unable to isolate the participants of interest.
We were only able to identify two randomised controlled trials regarding the effect of LLLT compared with a control in patellar tendinopathy. Ashok et al84 have compared the effect of LLLT to that of therapeutic ultrasound in persons with patellar tendinopathy, and they found a statistically significant effect in favour of LLLT, both on pain reduction and function. However, it should be noted that this trial is small (n=8) and only of moderate methodological quality. Another LLLT trial by Meier et al85 included participants with both patellar tendinopathy (n=58) and Achilles tendinopathy (n=52). We omitted this trial, since it solely concerned the effects of an invisible (904 nm wavelength) laser versus a red (632 nm wavelength) laser. Meier et al85 stated that the red laser was placebo, but the laser dose applied in the sham procedure may possibly have had a photochemical effect. Both groups achieved a positive effect on a combined index of pain and function, favouring the 904 nm wavelength laser, but the report of the trial neither includes point effect estimates, nor variability data.
The presence and role of inflammation in chronic tendinopathy have been an ongoing debate in the last few decades. There is currently increased support that inflammation has a causal role in tendinopathy, where immune cells and molecular mediators are included as inflammatory components.86–88 PGE2 has been suggested to sustain inflammation and pain in human tendon disease.89 In Achilles tendinopathy, a reduction of PGE2 and a concurrent increased pain pressure threshold after LLLT were found in a double-blinded randomised clinical trial by Bjordal et al,90 where microdialysis of the tendon was performed in seven participants. The participants had aggravated the symptoms through a pain inducing activity immediately prior to the examination. Only the immediate (105 min) response to LLLT was investigated in the trial, but the findings support the notion that LLLT may have an anti-inflammatory effect in Achilles tendinopathy.
Several authors of the included trials failed to adequately describe the laser dose parameters used. A LLLT dose–response relationship has been established in systematic reviews of tendinopathy34–36 and osteoarthritis.39 In the current review, some of the statistical heterogeneity is plausibly due to the variation in laser doses applied. The statistical heterogeneity of the dose subgroup analyses was generally lower than in the overall (any dose) analyses and this indicates that the laser dose might be more important for the effect than the location of the tendinopathy. The only study that caused noteworthy statistical heterogeneity in the dose subgroup analysis with placebo control was the one by Darre et al.61 Most of the pain and disability analyses comparing LLLT with other interventions were based on trials of plantar fasciitis. These analyses yielded a moderate level of statistical heterogeneity, and it may be explained by the variation in control interventions.
The included trials had a moderate to high methodological quality (mean PEDro score=7.1). Although therapist and assessor blinding lacked in many of the included studies, the lack of blinding was not significantly associated with higher effect estimates (online supplemental material).
Future trials on the topic should include larger patient samples and directly compare the effectiveness of different LLLT parameters. Additionally, systematic reviews of LLLT should include dose-response investigations.
Strengths and limitations of this study
This review was conducted in conformance with a detailed a priori published protocol, which includes, for example, a plan for subgrouping the trials by laser dose. The review includes results from two studies reported in non-English language61 76 and an unpublished study. The review features meta-analyses with direct comparisons between LLLT and placebo LLLT, other interventions and no intervention. Although only one reviewer extracted data from the included trials, the extracted data were checked for correctness by another reviewer.
Implications for practice
The LLLT dose parameters were inadequately described in 6 (35%) of the trial articles. This prohibited a comprehensive laser dose–response relationship investigation using the WALT treatment recommendations.37 38 Since the laser doses identified as WALT recommended doses provided significantly positive results in most instances, we suggest adhering to these recommendations until further trials increase the precision of the analysis.
Conclusions
LLLT significantly reduces pain and disability in lower extremity tendinopathy and plantar fasciitis in the short and medium terms. Long-term data were not available. Some uncertainty about the effect size remains due to wide CIs and lack of larger trials.
Supplementary Material
Footnotes
Twitter: @INaterstad
Contributors: IFN and MBS wrote the PROSPERO protocol. IFN and MBS selected the trials, with the involvement of JJ when necessary. IFN and MBS judged the risk of bias, with the involvement of JJ when necessary. IFN and MBS extracted the data. IFN and MBS translated the non-English articles. IFN performed the analyses, under supervision by MBS. All authors participated in interpreting of the results. IFN drafted the first version of the manuscript, and subsequently revised it, based on comments by JJ, JB, CC, RABL-M and MBS. All authors read and accepted the final version of the manuscript. IFN acts as the guarantor for this study.
Funding: The Norwegian Fund for Post-Graduate Training for Physiotherapists funded this research, grant number 44 944. No other specific grant from any funding agency in the public, commercial or not-for-profit sectors was received for this work.
Disclaimer: The corresponding author had full access to all data in the study and had the final responsibility for the decision to submit for publication.
Competing interests: JMB and RABLM are former board members and prior presidents of the World Association for Laser Therapy, a non-profit research organisation from which they have never received funding, grants or fees. The other authors declared that they had no conflict of interests related to this work.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
The dataset for meta-analysis is available from the corresponding author upon reasonable request. The corresponding author affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained. The dataset for meta-analysis is available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
Not applicable.
References
- 1.Riel H, Lindstrøm CF, Rathleff MS, et al. Prevalence and incidence rate of lower-extremity tendinopathies in a Danish general practice: a registry-based study. BMC Musculoskelet Disord 2019;20:239. 10.1186/s12891-019-2629-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Albers S, Zwerver J, van den Akker-Scheek I. 7 Incidence And Prevalence Of Lower Extremity Tendinopathy In The General Population: Abstract 7 Table 1. Br J Sports Med 2014;48:A5.1–A5. 10.1136/bjsports-2014-094114.7 [DOI] [Google Scholar]
- 3.Janssen I, van der Worp H, Hensing S, et al. Investigating Achilles and Patellar tendinopathy prevalence in elite athletics. Res Sports Med 2018;26:1–12. 10.1080/15438627.2017.1393748 [DOI] [PubMed] [Google Scholar]
- 4.Wang JH-C, Iosifidis MI, Fu FH. Biomechanical basis for tendinopathy. Clin Orthop Relat Res 2006;443:320–32. 10.1097/01.blo.0000195927.81845.46 [DOI] [PubMed] [Google Scholar]
- 5.Magnusson SP, Kjaer M. The impact of loading, unloading, ageing and injury on the human tendon. J Physiol 2019;597:1283–98. 10.1113/JP275450 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Prichasuk S, Subhadrabandhu T. The relationship of pes planus and calcaneal Spur to plantar heel pain. Clin Orthop Relat Res 1994;306:192–6. [PubMed] [Google Scholar]
- 7.Rano JA, Fallat LM, Savoy-Moore RT. Correlation of heel pain with body mass index and other characteristics of heel pain. J Foot Ankle Surg 2001;40:351–6. 10.1016/S1067-2516(01)80002-8 [DOI] [PubMed] [Google Scholar]
- 8.Riddle DL, Pulisic M, Pidcoe P, et al. Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am 2003;85:872–7. 10.2106/00004623-200305000-00015 [DOI] [PubMed] [Google Scholar]
- 9.Taunton JE, Ryan MB, Clement DB, et al. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med 2002;36:95–101. 10.1136/bjsm.36.2.95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc 2003;93:234–7. 10.7547/87507315-93-3-234 [DOI] [PubMed] [Google Scholar]
- 11.Zhang J, Nie D, Rocha JL, et al. Characterization of the structure, cells, and cellular mechanobiological response of human plantar fascia. J Tissue Eng 2018;9:2041731418801103. 10.1177/2041731418801103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.van der Vlist AC, et al. Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. Br J Sports Med 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chan K-M, Fu S-C. Anti-inflammatory management for tendon injuries - friends or foes? Sports Med Arthrosc Rehabil Ther Technol 2009;1:23. 10.1186/1758-2555-1-23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Aicale R, Bisaccia RD, Oliviero A, et al. Current pharmacological approaches to the treatment of tendinopathy. Expert Opin Pharmacother 2020;21:1467–77. 10.1080/14656566.2020.1763306 [DOI] [PubMed] [Google Scholar]
- 15.Jomaa G, Kwan C-K, Fu S-C, et al. A systematic review of inflammatory cells and markers in human tendinopathy. BMC Musculoskelet Disord 2020;21:78. 10.1186/s12891-020-3094-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Duchman KR, Lemmex DB, Patel SH, et al. The effect of non-steroidal anti-inflammatory drugs on Tendon-to-Bone healing: a systematic review with subgroup meta-analysis. Iowa Orthop J 2019;39:107–19. [PMC free article] [PubMed] [Google Scholar]
- 17.Paoloni JA, Milne C, Orchard J, et al. Non-Steroidal anti-inflammatory drugs in sports medicine: guidelines for practical but sensible use. Br J Sports Med 2009;43:863–5. 10.1136/bjsm.2009.059980 [DOI] [PubMed] [Google Scholar]
- 18.Bussin ER, Cairns B, Bovard J, et al. Randomised controlled trial evaluating the short-term analgesic effect of topical diclofenac on chronic Achilles tendon pain: a pilot study. BMJ Open 2017;7:e015126. 10.1136/bmjopen-2016-015126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Heinemeier KM, Øhlenschlæger TF, Mikkelsen UR, et al. Effects of anti-inflammatory (NSAID) treatment on human tendinopathic tissue. J Appl Physiol 2017;123:1397–405. 10.1152/japplphysiol.00281.2017 [DOI] [PubMed] [Google Scholar]
- 20.Aström M, Westlin N. No effect of piroxicam on Achilles tendinopathy. A randomized study of 70 patients. Acta Orthop Scand 1992;63:631–4. 10.1080/17453679209169724 [DOI] [PubMed] [Google Scholar]
- 21., Bhala N, Emberson J, et al. , Coxib and traditional NSAID Trialists' (CNT) Collaboration . Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet 2013;382:769–79. 10.1016/S0140-6736(13)60900-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chung H, Dai T, Sharma SK, et al. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng 2012;40:516–33. 10.1007/s10439-011-0454-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mussttaf RA, Jenkins DFL, Jha AN. Assessing the impact of low level laser therapy (LLLT) on biological systems: a review. Int J Radiat Biol 2019;95:120–43. 10.1080/09553002.2019.1524944 [DOI] [PubMed] [Google Scholar]
- 24.Bjordal JM, Lopes-Martins RAB, Joensen J, et al. The anti-inflammatory mechanism of low level laser therapy and its relevance for clinical use in physiotherapy. Physical Therapy Reviews 2010;15:286–93. 10.1179/1743288X10Y.0000000001 [DOI] [Google Scholar]
- 25.Silveira PCL, Silva LAda, Fraga DB, et al. Evaluation of mitochondrial respiratory chain activity in muscle healing by low-level laser therapy. J Photochem Photobiol B 2009;95:89–92. 10.1016/j.jphotobiol.2009.01.004 [DOI] [PubMed] [Google Scholar]
- 26.Moriyama Y, Moriyama EH, Blackmore K, et al. In vivo study of the inflammatory modulating effects of low-level laser therapy on iNOS expression using bioluminescence imaging. Photochem Photobiol 2005;81:1351–5. 10.1562/2005-02-28-RA-450 [DOI] [PubMed] [Google Scholar]
- 27.Fillipin LI, Mauriz JL, Vedovelli K, et al. Low-Level laser therapy (LLLT) prevents oxidative stress and reduces fibrosis in rat traumatized Achilles tendon. Lasers Surg Med 2005;37:293–300. 10.1002/lsm.20225 [DOI] [PubMed] [Google Scholar]
- 28.Chen AC-H, Arany PR, Huang Y-Y, et al. Low-Level laser therapy activates NF-kB via generation of reactive oxygen species in mouse embryonic fibroblasts. PLoS One 2011;6:e22453. 10.1371/journal.pone.0022453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Luo L, Sun Z, Zhang L, et al. Effects of low-level laser therapy on ROS homeostasis and expression of IGF-1 and TGF-β1 in skeletal muscle during the repair process. Lasers Med Sci 2013;28:725–34. 10.1007/s10103-012-1133-0 [DOI] [PubMed] [Google Scholar]
- 30.de Jesus JF, Spadacci-Morena DD, dos Anjos Rabelo ND, et al. Low-Level laser therapy in IL-1β, COX-2, and PGE2 modulation in partially injured Achilles tendon. Lasers Med Sci 2015;30:153–8. 10.1007/s10103-014-1636-y [DOI] [PubMed] [Google Scholar]
- 31.Marcos RL, Leal Junior ECP, Messias FdeM, et al. Infrared (810 nm) low-level laser therapy in rat Achilles tendinitis: a consistent alternative to drugs. Photochem Photobiol 2011;87:1447–52. 10.1111/j.1751-1097.2011.00999.x [DOI] [PubMed] [Google Scholar]
- 32.Marcos RL, Leal-Junior ECP, Arnold G, et al. Low-Level laser therapy in collagenase-induced Achilles tendinitis in rats: analyses of biochemical and biomechanical aspects. J Orthop Res 2012;30:1945–51. 10.1002/jor.22156 [DOI] [PubMed] [Google Scholar]
- 33.Frigo L, Fávero GM, Lima HJC, et al. Low-Level Laser Irradiation (InGaAlP-660 nm) Increases Fibroblast Cell Proliferation and Reduces Cell Death in a Dose-Dependent Manner. Photomed Laser Surg 2010;28:S-151–S-156. 10.1089/pho.2008.2475 [DOI] [PubMed] [Google Scholar]
- 34.Bjordal JM, Couppe C, Ljunggren AE. Low level laser therapy for tendinopathy. Evidence of a Dose–Response pattern. Physical Therapy Reviews 2001;6:91–9. 10.1179/ptr.2001.6.2.91 [DOI] [Google Scholar]
- 35.Haslerud S, Magnussen LH, Joensen J, et al. The efficacy of low-level laser therapy for shoulder tendinopathy: a systematic review and meta-analysis of randomized controlled trials. Physiother Res Int 2015;20:108–25. 10.1002/pri.1606 [DOI] [PubMed] [Google Scholar]
- 36.Tumilty S, Munn J, McDonough S, et al. Low level laser treatment of tendinopathy: a systematic review with meta-analysis. Photomed Laser Surg 2010;28:3–16. 10.1089/pho.2008.2470 [DOI] [PubMed] [Google Scholar]
- 37.WALT . Recommended treatment doses for low level laser therapy 780-860 nm wavelength, 2010a. Available: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_780-860nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
- 38.WALT . Recommended treatment doses for Low Level Laser Therapy 904 nm wavelength., 2010b. Available: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_904nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
- 39.Stausholm MB, Naterstad IF, Joensen J, et al. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open 2019;9:e031142. 10.1136/bmjopen-2019-031142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Stausholm MB, Naterstad IF, Alfredo PP, et al. Short- and long-term effectiveness of low-level laser therapy combined with strength training in knee osteoarthritis: a randomized placebo-controlled trial. J Clin Med 2022;11:3446. 10.3390/jcm11123446 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Huang Y-Y, Chen AC-H, Carroll JD, et al. Biphasic dose response in low level light therapy. Dose Response 2009;7:dose-response.0–383. 10.2203/dose-response.09-027.Hamblin [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Huang Y-Y, Sharma SK, Carroll J, et al. Biphasic dose response in low level light therapy - an update. Dose Response 2011;9:dose-response.1. 10.2203/dose-response.11-009.Hamblin [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zein R, Selting W, Hamblin MR. Review of light parameters and photobiomodulation efficacy: dive into complexity. J Biomed Opt 2018;23:1–17. 10.1117/1.JBO.23.12.120901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys 2017;4:337–61. 10.3934/biophy.2017.3.337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rhim HC, Kim MS, Choi S, et al. Comparative efficacy and tolerability of nonsurgical therapies for the treatment of Midportion Achilles tendinopathy: a systematic review with network meta-analysis. Orthop J Sports Med 2020;8:2325967120930567:232596712093056. 10.1177/2325967120930567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Martimbianco ALC, Ferreira RES, Latorraca CdeOC, et al. Photobiomodulation with low-level laser therapy for treating Achilles tendinopathy: a systematic review and meta-analysis. Clin Rehabil 2020;34:713–22. 10.1177/0269215520912820 [DOI] [PubMed] [Google Scholar]
- 47.Wang W, Jiang W, Tang C, et al. Clinical efficacy of low-level laser therapy in plantar fasciitis: a systematic review and meta-analysis. Medicine 2019;98:e14088. 10.1097/MD.0000000000014088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dos Santos SA, Sampaio LM, Caires JR, et al. Parameters and effects of Photobiomodulation in plantar fasciitis: a meta-analysis and systematic review. Photobiomodul Photomed Laser Surg 2019;37:327–35. 10.1089/photob.2018.4588 [DOI] [PubMed] [Google Scholar]
- 49.Salvioli S, Guidi M, Marcotulli G. The effectiveness of conservative, non-pharmacological treatment, of plantar heel pain: a systematic review with meta-analysis. Foot 2017;33:57–67. 10.1016/j.foot.2017.05.004 [DOI] [PubMed] [Google Scholar]
- 50.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535. 10.1136/bmj.b2535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother 2009;55:129–33. 10.1016/S0004-9514(09)70043-1 [DOI] [PubMed] [Google Scholar]
- 52.Moseley AM, Herbert RD, Maher CG, et al. Reported quality of randomized controlled trials of physiotherapy interventions has improved over time. J Clin Epidemiol 2011;64:594–601. 10.1016/j.jclinepi.2010.08.009 [DOI] [PubMed] [Google Scholar]
- 53.Higgins JPT, Green S. Cochrane Handbook for systematic reviews of interventions, 2011. Available: http://handbook.cochrane.org/
- 54.Higgins JP, Green S. Cochrane Handbook for systematic reviews of interventions, 2011. Available: http://handbook.cochrane.org/
- 55.Thong ISK, Jensen MP, Miró J, et al. The validity of pain intensity measures: what do the NRS, vas, VRS, and FPS-R measure? Scand J Pain 2018;18:99–107. 10.1515/sjpain-2018-0012 [DOI] [PubMed] [Google Scholar]
- 56.Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. 10.1002/sim.1186 [DOI] [PubMed] [Google Scholar]
- 57.Higgins JPT, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. 10.1136/bmj.327.7414.557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.WALT . Recommended treatment doses for low level laser therapy 780-860 nm wavelength: world association for laser therapy, 2010. Available: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_780-860nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
- 59.WALT . Recommended treatment doses for low level laser therapy 904 nm wavelength: world association for laser therapy, 2010. Available: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_904nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf
- 60.Stergioulas A. Effects of a 904 nm GaAs laser versus placebo in the treatment of Patellar tendonitis. Laser & Tecnology 2003;13:21–6. [Google Scholar]
- 61.Darre EM, Klokker M, Lund P, et al. [Laser therapy of Achilles tendinitis]. Ugeskr Laeger 1994;156:6680–3. [PubMed] [Google Scholar]
- 62.Tumilty S, Munn J, Abbott JH, et al. Laser therapy in the treatment of Achilles tendinopathy: a pilot study. Photomed Laser Surg 2008;26:25–30. 10.1089/pho.2007.2126 [DOI] [PubMed] [Google Scholar]
- 63.Tumilty S, McDonough S, Hurley DA, et al. Clinical effectiveness of low-level laser therapy as an adjunct to eccentric exercise for the treatment of Achilles' tendinopathy: a randomized controlled trial. Arch Phys Med Rehabil 2012;93:733–9. 10.1016/j.apmr.2011.08.049 [DOI] [PubMed] [Google Scholar]
- 64.Basford JR, Malanga GA, Krause DA, et al. A randomized controlled evaluation of low-intensity laser therapy: plantar fasciitis. Arch Phys Med Rehabil 1998;79:249–54. 10.1016/S0003-9993(98)90002-8 [DOI] [PubMed] [Google Scholar]
- 65.Kiritsi O, Tsitas K, Malliaropoulos N, et al. Ultrasonographic evaluation of plantar fasciitis after low-level laser therapy: results of a double-blind, randomized, placebo-controlled trial. Lasers Med Sci 2010;25:275–81. 10.1007/s10103-009-0737-5 [DOI] [PubMed] [Google Scholar]
- 66.Lamba D, Tiwari M, Singh P, M.; Pankaj S. To study the characteristics and efficacy of 820 nm GA-Al-As diode laser for the treatment of plantar fasciitis among Porters/Coolies in Kumaun region, India: a randomized clinical trial. Indian Journal of Physiotherapy and Occupational Therapy - An International Journal 2013;7:34–9. 10.5958/j.0973-5674.7.4.118 [DOI] [Google Scholar]
- 67.Macias DM, Coughlin MJ, Zang K, et al. Low-Level Laser Therapy at 635 nm for Treatment of Chronic Plantar Fasciitis: A Placebo-Controlled, Randomized Study. J Foot Ankle Surg 2015;54:768–72. 10.1053/j.jfas.2014.12.014 [DOI] [PubMed] [Google Scholar]
- 68.Stergioulas A, Stergioula M, Aarskog R, et al. Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic Achilles tendinopathy. Am J Sports Med 2008;36:881–7. 10.1177/0363546507312165 [DOI] [PubMed] [Google Scholar]
- 69.Liu X-G, Cheng L, Song J-M. Effects of low-level laser therapy and eccentric exercises in the treatment of Patellar tendinopathy. International Journal of Photoenergy 2014;2014:1–6. 10.1155/2014/785386 [DOI] [Google Scholar]
- 70.Cinar E, Saxena S, Uygur F. Low-Level laser therapy in the management of plantar fasciitis: a randomized controlled trial. Lasers Med Sci 2018;33:949–58. 10.1007/s10103-017-2423-3 [DOI] [PubMed] [Google Scholar]
- 71.Cinar E, Saxena S, Uygur F. Combination therapy versus exercise and orthotic support in the management of pain in plantar fasciitis: a randomized controlled trial. Foot Ankle Int 2018;39:406–14. 10.1177/1071100717747590 [DOI] [PubMed] [Google Scholar]
- 72.ELsehrawy G, Nasef S, Ibrahim M, et al. Extracorporeal shock wave therapy versus low-level laser therapy in the management of chronic plantar fasciitis. Suez Canal University Medical Journal 2018;21:71–81. 10.21608/scumj.2018.42935 [DOI] [Google Scholar]
- 73.Yinilmez Sanmak Ömür Damla, Geler Külcü D, Mesci N, et al. Comparison of effects of low-level laser therapy and extracorporeal shock wave therapy in plantar fasciitis treatment: a randomized, prospective, single-blind clinical study. Turk J Phys Med Rehabil 2019;65:184–90. 10.5606/tftrd.2019.3528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Ulusoy A, Cerrahoglu L, Orguc S. Magnetic resonance imaging and clinical outcomes of laser therapy, ultrasound therapy, and extracorporeal shock wave therapy for treatment of plantar fasciitis: a randomized controlled trial. J Foot Ankle Surg 2017;56:762–7. 10.1053/j.jfas.2017.02.013 [DOI] [PubMed] [Google Scholar]
- 75.Koteeswaran K, Ramya K, Rajeshwari A, et al. Effectiveness of low level laser therapy versus ultrasound therapy with plantar fascia streching in subjects with plantar fasciitis. Indian J Public Health Res Dev 2020;11:92–6. 10.37506/v11/i1/2020/ijphrd/193792 [DOI] [Google Scholar]
- 76.Yüzer S SS, Gürçay E, Ünlü E. Comparison of the effectiveness of laser therapy and steroid ınjection in epin calcanei. Turk J Phys Med Rehabil 2006;52:68–71. [Google Scholar]
- 77.IntHout J, Ioannidis JPA, Borm GF, et al. Small studies are more heterogeneous than large ones: a meta-meta-analysis. J Clin Epidemiol 2015;68:860–9. 10.1016/j.jclinepi.2015.03.017 [DOI] [PubMed] [Google Scholar]
- 78.Murphy M, Rio E, Debenham J, et al. Evaluating the progress of mid-portion Achilles tendinopathy during rehabilitation: a review of outcome measures for self- reported pain and function. Int J Sports Phys Ther 2018;13:283–92. 10.26603/ijspt20180283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Landorf KB, Radford JA, Hudson S. Mid of two commonly used outcome measures for foot problems. Journal of Foot and Ankle Research 2010;3:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kwon K, Son T, Lee K-J, et al. Enhancement of light propagation depth in skin: cross-validation of mathematical modeling methods. Lasers Med Sci 2009;24:605–15. 10.1007/s10103-008-0625-4 [DOI] [PubMed] [Google Scholar]
- 81.Vulpiani MC, Trischitta D, Trovato P, et al. Extracorporeal shockwave therapy (ESWT) in Achilles tendinopathy. A long-term follow-up observational study. J Sports Med Phys Fitness 2009;49:171–6. [PubMed] [Google Scholar]
- 82.Oltulu P, Ince B, Kokbudak N, et al. Measurement of epidermis, dermis, and total skin thicknesses from six different body regions with a new ethical histometric technique. Turkish Journal of Plastic Surgery 2018;26:56–61. 10.4103/tjps.TJPS_2_17 [DOI] [Google Scholar]
- 83.Lögdberg-Andersson M, Mützell S, Hazel Åke. LOW LEVEL LASER THERAPY (LLLT) OF TENDINITIS AND MYOFASCIAL PAINS - A RANDOMIZED, DOUBLE-BLIND, CONTROLLED STUDY. Laser Therapy 1997;9:79–85. 10.5978/islsm.9.79 [DOI] [Google Scholar]
- 84.Ashok N, Raghul S, Sivakumar VPR. Compare The Effects of Low-Level Laser and Ultrasonic Therapy in Subjects with Jumper’s Knee. International Journal of Research and Scientific Innovation 2018;5. [Google Scholar]
- 85.Meier JK, Kerkour K. Traitement laser de la tendinite. Médecine et hygiène 1988;46:907–11. [Google Scholar]
- 86.Millar NL, Dean BJ, Dakin SG. Inflammation and the continuum model: time to acknowledge the molecular era of tendinopathy. Br J Sports Med 2016;50:1486. 10.1136/bjsports-2016-096419 [DOI] [PubMed] [Google Scholar]
- 87.Dean BJF, Gettings P, Dakin SG, et al. Are inflammatory cells increased in painful human tendinopathy? A systematic review. Br J Sports Med 2016;50:216–20. 10.1136/bjsports-2015-094754 [DOI] [PubMed] [Google Scholar]
- 88.Mosca MJ, Rashid MS, Snelling SJ, et al. Trends in the theory that inflammation plays a causal role in tendinopathy: a systematic review and quantitative analysis of published reviews. BMJ Open Sport Exerc Med 2018;4:e000332. 10.1136/bmjsem-2017-000332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Bergqvist F, Carr AJ, Wheway K, et al. Divergent roles of prostacyclin and PGE2 in human tendinopathy. Arthritis Res Ther 2019;21:74. 10.1186/s13075-019-1855-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Bjordal JM, Lopes-Martins RAB, Iversen VV. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. Br J Sports Med 2006;40:76–80. 10.1136/bjsm.2005.020842 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-059479supp001.pdf (1MB, pdf)
Data Availability Statement
The dataset for meta-analysis is available from the corresponding author upon reasonable request. The corresponding author affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained. The dataset for meta-analysis is available from the corresponding author upon reasonable request.