

Abstract
Objective
The fixation of the coronoid fractures in terrible triad injuries is quite challenging. In this study, we introduce a minimally invasive technique using a syringe as a guide for insertion of the cannulated screw in an anterior to posterior fashion to fix the coronoid fracture in patients with terrible triad injuries.
Methods
In this retrospective study, clinical data of patients suffering from terrible triad injuries between 2012 and 2019 were analyzed. Fifteen patients with an average age of 38.2 years old (21–56 years) were enrolled in this study, of which 12 were males and three were females. The Regan–Morrey type II and type III coronoid fractures in these patients were treated with cannulated screws, inserted anteriorly using a 1 mL syringe as a guide. Outcome measures included pain, range of motion, stability and daily function using Mayo Elbow Performance scores (MEPs). The anteroposterior and lateral radiographs were used for evaluating a healing fracture.
Results
After a mean follow up of 44.2 months (range 13–80), the mean elbow flexion was 128.2°, extension was 12.3°, forearm pronation was 74.6° and supination was 73.6°. A concentric reduction was maintained without severe pain, stiffness, and radiographic evidence of instability in all patients during the follow‐up period. The mean MEPs was 89.7 points.
Conclusion
The anteroposterior cannulated screw fixation via simple syringe guide is a minimally invasive and safe option for surgical treatment of coronoid fractures in terrible triad injuries.
Keywords: Cannulated screws, Coronoid fracture, Elbow dislocation, Fixation device, Radial head fracture, Terrible triad injury
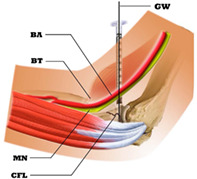
Minimally invasive anterior approach and a direct lateral approach to address the fractured coronoid. Avoiding further injury to important anterior soft tissues. Allowing adequate lateral view of the fractured coronoid and a concentric anterior fixation. BA, brachial artery; BT, biceps tendon; CFL, coronoid fracture line; MN, median nerve; GW, guide wire.
Introduction
The coronoid process is a primary bony stabilizer of the elbow, which provides an anterior buttress to prevent posterior dislocation of the ulna. 1 , 2 Although reconstruction of the coronoid fracture in the terrible triad injury can be demanding, a consensus on the best approach has not yet been established.
However, fractures of the radial head, the coronoid process, along with elbow dislocation are described as the terrible triad, a complex injury with controversies about the best surgical approaches. 1 , 2 The non‐surgical approach for these injuries is rarely used. However, the surgical treatments for these injuries have achieved good outcomes. These surgical options include: (i) fixation or excision of the coronoid; (ii) fixation, excision, or replacement of the radial head; and (iii) repair of the lateral collateral ligament (LCL) complex using standard treatment protocols. 2 , 3 , 4 , 5 Although, the radial head repair or reconstruction is technically achievable through the direct lateral approach, repair of the coronoid fracture remains a challenge due to inadequate exposure, and difficulties in fixation. Various surgical approaches with different fixation options including suture lasso technique, 6 , 7 , 8 lag screws fixation in a posteroanterior direction, 2 , 6 , 9 site‐specific plates, 4 , 8 suture anchor 10 or no treatment 8 , 11 , 12 have been reported with various outcomes for the treatment of coronoid fractures. However, the lateral approach of the elbow may be inadequate to expose both, the radial head and coronoid process, without extensive soft tissue injury. Hence, surgeons decide either a medial approach or an additional posterior approach with posteroanterior insertion of the screw, which increases the risk of instability and re‐operation. 3 Whether a global posterior approach or posteroanterior screw insertion, axial stability serves to be a major biomechanical challenge. This is because the insertion of the screw from a posterior larger fragment into an anterior smaller fragment is difficult for a firm hold of the screw in the anterior fragment.
Moreover, the current methods for fixation of the coronoid fracture with cannulated lag screws are awkward in position, and sometimes difficult to introduce the guide from an ideal entry point with designated direction in a limited space. This results in unsatisfactory outcomes.
In this study, we report a minimally invasive technique using a syringe as a guide for insertion of the cannulated screw in an anterior to posterior fashion in a free style in terms of the entry point and direction with safety to fix the coronoid fracture in patients with terrible triad injuries. The purpose of this study is to; (i) verify the reliability and safety of our technique; and (ii) investigate the outcome of this simple minimally invasive approach.
Methods
Patient Selection
After ethical board approval (SAHo WMU‐CR2018‐08‐417), all patients treated for terrible triad injury from June of 2012 to September 2019 were evaluated.
Inclusion criteria included: (i) patients with Regan–Morrey type II and III coronoid fractures; (ii) patients with Mason type II and III fractures of the radial head that were either reduced, fixed or excised; and (iii) patients who were treated using a non‐collapsible syringe guide for insertion of cannulated screws to fix the coronoid fractures. Exclusion criteria included: (i) patients treated with an old injury of the affected elbow; (ii) patients followed‐up for <12 months; and (iii) patients with diabetes or elbow arthrosis, such as gout, rheumatoid arthritis and so forth. Informed consent was obtained for all patients participating in the study.
Surgical Process
Anesthesia and Position
For brachial block or general anesthesia, the patient was placed in a supine position on the surgical table.
Approach and Exposure
The elbow was approached with a direct lateral incision through the Kocher interval between the extensor carpi ulnaris and anconeus. The radial head fracture was exposed and retracted, allowing visualization of the coronoid process (Fig. 1). The surgeon palpated and localized the biceps tendon with one finger while used a hemostat to dissect lateral to the biceps tendon through a lateral incision from deep to superficial. The anterior elevated skin was dissected where the tip of the hemostat is pointed, just one fingerbreadth distal to the elbow flexion crease medial to the midline in the antecubital region (Fig. 2). A 0.8 mm Kirschner wire was used through the lateral incision to maintain the reduced coronoid fragment temporarily when needed, and a guidewire was placed through the portal (Fig. 3).
Fig. 1.
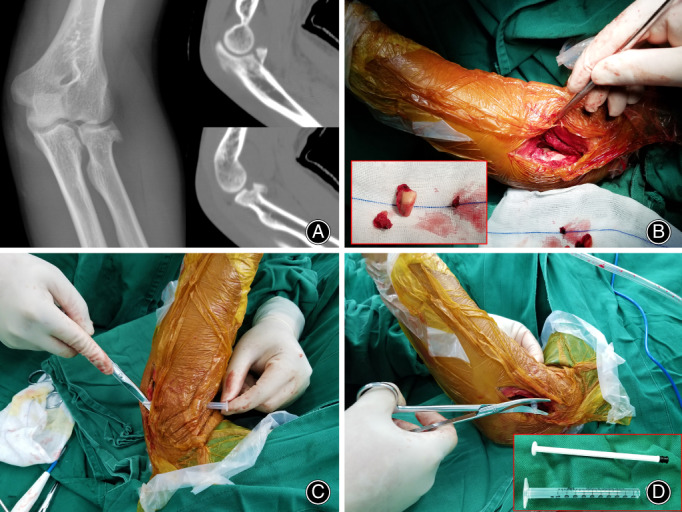
Pre‐op and intra‐op findings: Anteroposterior (AP) X‐ray of the radial head fracture and lateral CT scan of the coronoid and radial head fractures (A), view of the coronoid fracture through the lateral incision after removal of the radial head fragment shown in the inset image (B), intra‐operative insertion of the 1 mL syringe guide (C, D).
Fig. 2.
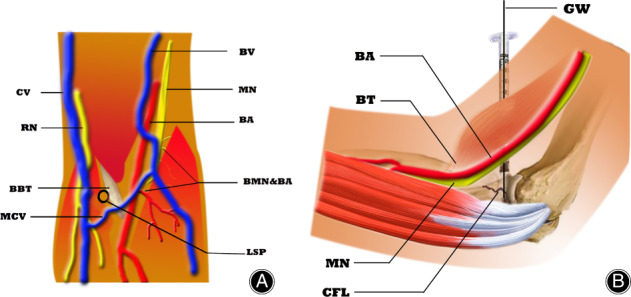
Schematic orientation of the syringe guide placement. Front view (A): BA, brachial artery; BBT, biceps brachii tendon; BMN & BA, branches of the median nerve and brachial artery; BV, basilic vein; CV, cephalic vein; LSP, location of syringe placement; MCV, median cubital vein; MN, median nerve; RN, radial nerve. Medial view (B): BA, brachial artery; BT, biceps tendon; CFL, coronoid fracture line; GW, guide wire; MN, median nerve.
Fig. 3.
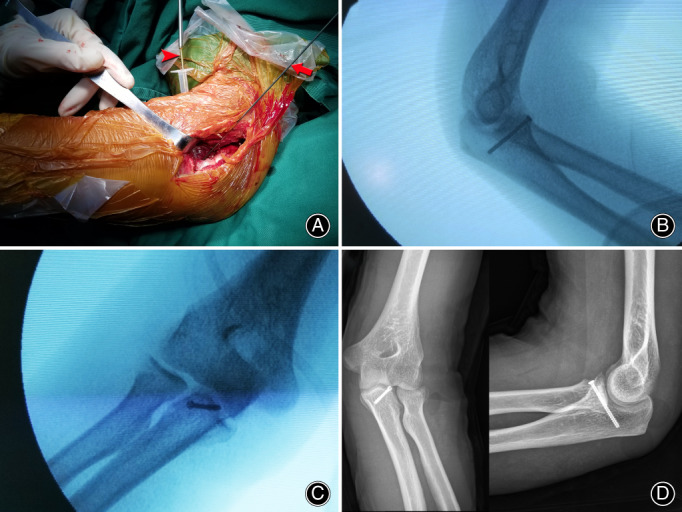
Intra‐op screw placement in a non‐comminuted fracture of the coronoid. Screw fixation of the coronoid fracture through the non‐collapsible syringe guide (red arrowhead), and lateral K‐wire (red arrow) insertion for temporary fracture fixation (A), intra‐operative fluoroscopy with both lateral (B) and AP (C) views, post‐operative day seven AP and lateral X‐rays (D).
Insertion of the Cannulated Screw(s)
The 1 mL non‐collapsible syringe guide was introduced through the portal in a two‐step procedure. First, the syringe with the small front head was kept intact and passed in the portal from the front towards the coronoid (Fig. 1C). In the second step, the small front head was cut off for inserting the guide wire (Fig. 1D). Pressure was maintained against the fragment during the placement of the cannulated screws in the coronoid's depth in an anteroposterior direction. The coronoid fracture was stabilized with two 3 mm headless cannulated screws for larger comminuted fragments (10 elbows; Fig. 4), while only one screw was used for one large fragment (five elbows). Under fluoroscopic guidance, the intra‐operative ulno‐humeral stability was checked, through an arc of flexion–extension from 30°–120°. The valgus stress test was used to assess the valgus laxity with the forearm in neutral rotation.
Fig. 4.
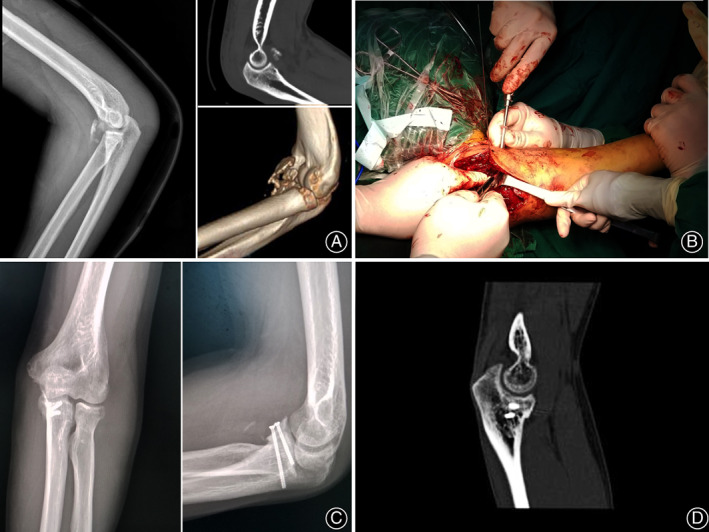
Intra‐op screw placement in a comminuted coronoid fracture. Lateral X‐ray and CT scan (sagittal view) of a comminuted coronoid fracture (A), intra‐operative screws fixation of the coronoid fracture (B), post‐operative day seven AP and lateral X‐rays of the coronoid process (C), CT scan (sagittal view) of the coronoid process 1‐month post‐op (D).
Management of Associated Injuries
For the radial head fractures, if they were in two parts as Mason type II, they were either reduced/fixed (12 elbows) or excised (two elbows). Those with three parts as in Mason type III (one elbow) were also reduced and fixed with countersunk small fragment screws, or headless compression screws through the lateral incision.
The avulsed lateral collateral ligament (LCL) complex was repaired using anchor sutures to reattach the LCL back to the lateral epicondyle of the humerus. There was no mid‐substance tear of the LCL. Moreover, to confirm that the medial collateral ligament (MCL) was intact, the valgus stress test was repeated before wound closure.
Post‐operative Care
After stability was confirmed, the elbow was placed in a long arm splint at 90° flexion with the forearm in pronation to protect the repaired LCL. On post‐operative day seven, patients initiated range of motion, step by step for 4 weeks at 30° to maximum tolerated flexion in a brace. Once the healing was achieved, the maximum active range of motion exercises was started through physical posture. In 3 months, muscular rehabilitation was initiated to strengthen the particular stabilizing muscles.
Follow‐up and Functional Evaluation
Patients were followed‐up and evaluated clinically. Functional outcomes were assessed according to the Mayo Elbow Performance score (MEPs), which was based on pain, mobility, stability and functional evaluation. This MEPs is a 100‐point scale score, with maximum score of 45 points for pain relief, 25 points for function (five points each for grooming, feeding, personal hygiene, putting on a shirt, and putting on shoes), 20 points for motion and 10 points for stability. The MEPs falls into four grades: ≥ 90 indicates excellent; 75–89 indicates good; 60–74 indicates fair; and <60, indicates poor. Radiographic assessment of the elbow, based on A/P and lateral views, were also performed to evaluate joint, focusing the fracture union status and screw positioning at last follow‐up.
Results
General Outcome
In all 15 patients (three females and 12 males) age between 21 and 56 years (average age 38.2 years) were enrolled. All injuries were unilateral, closed, and posterolateral dislocation without any neuro‐vascular involvement. Of the 15 injuries, 13 were sustained due to a fall from a height, and two cases resulted from a road traffic accident. The radial head fractures were classified as Mason type II (14 elbows) and Mason type III (one elbow). They were reduced and fixed through the direct lateral approach, as well as the avulsed LCL. Fracture of the coronoid process comprised 12 Regan‐Morrey type II, and three Regan‐Morrey types III. These were reduced through the lateral incision, and fixed via the anterior portal in the antecubital region in an anteroposterior direction. All the coronoid fractures were repaired using the minimally invasive anterior portal approach. No medial collateral ligament (MCL) lesion that contributed to instability was encountered during stability assessment under fluoroscopy. All LCL were repaired using anchor sutures. There were no complications encountered such as injuries to brachial arteries, radial or median nerves or superficial veins during insertion of the cannulated screws.
Results of ROM and MEPs
At mean follow‐up at 44.2 months, the average arcs of elbow motions were 128.2° in flexion 12.3° in extension, 73.6° in supination and 74.6° in pronation.
The average MEPs was 89.7, with nine excellent outcomes and six good outcomes.
All patients maintained a concentric reduction in both, ulnotrochlear and radiocapitellar articulation, with isometric fixation of the LCL.
Radiographic Results
Radiographs of all patients were reviewed. As per the final follow‐up radiographs, fracture union was achieved for all coronoid and radial head reconstruction. The coronoid fracture showed a solid osseous union in the final follow‐up radiograph. Post‐operative radiographs at the last follow‐up showed absence of arthritis, heterotopic ossification, and instability at the elbow.
Case Report
Presentation
A 45 year‐old male at our office fell from a 2 m height, when replacing a broken bulb from an electric lamp. After 5 days, he presented complaining of persistent pain at the left elbow. The patient was diagnosed with posterior dislocation of the elbow, and associated fractures of the coronoid process and radial head. The dislocation was reduced and splinted.
Physical Examination and Investigation Findings
On examination, visible varus deformity was observed without any laceration at the elbow. Pain was elicited on palpation at the lateral elbow, with limitations in the ranges of motion for forearm. Lateral CT scan showed a transverse Regan‐Morrey type II coronoid fracture along with Mason type II anterolateral radial head fracture (Fig. 1). The patient was healthy apart from this injury.
Surgical Procedure and Rehabilitation
A direct lateral incision was made through the Kocher interval. The radial head was exposed and retracted for adequate visualization of the coronoid fracture. A blunt dissection from deep to superficial through the lateral incision was made just lateral to the biceps tendon. The coronoid fracture was reduced and held temporarily by a 0.8 mm Kirshner wire through the lateral incision. A 1 ml non‐collapsible syringe guide was used to hold the fragment, while the 3.0 mm cannulated screws were introduced in the depth of the coronoid process, about one fingerbreadth distal to elbow flexion crease. After fixation of the coronoid fracture, the valgus stress was performed to confirm an intact MCL and to rule out valgus laxity. The radial head fragment was excised, and the LCL was reattached back to the lateral epicondyle isometric point with an anchor suture. The wound was closed in layers, and a post‐operative dressing that incorporated a posterior plaster splint with ulno‐humeral joint, held at 90° flexion and forearm in pronation was applied. At 28 months of follow‐up a flexion arc of 129°, extension arc of 11.2°, pronation of 70°, and supination of 70° were achieved (Fig. 5).
Fig. 5.
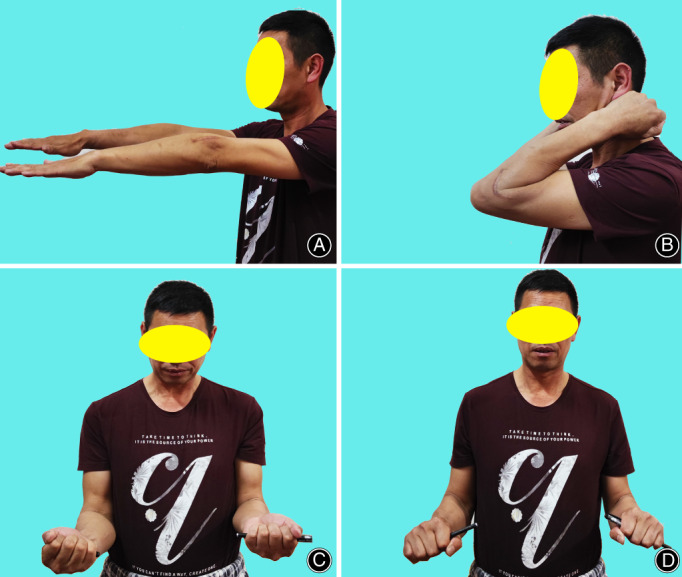
Range of motions at 28 months follow‐up: extension (A), flexion (B), supination (C), pronation (D).
Discussion
Advantages of This Technique
Treatment of the coronoid fracture in the terrible triad injury has been reported in different studies with different exposure and fixation techniques. 2 , 3 , 4 , 6 , 7 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 However, these approaches present different surgical demands for exposure of the coronoid process, but the fixation technique remains crucial for the stability of the elbow. Our technique to the coronoid fracture is simple, minimally invasive and resulted in a satisfactory outcome. Using a simple lateral incision the coronoid fracture was exposed, reduced and fixed through an anterior portal. This fixation method bypasses the major neuro‐vascular structures such as brachial artery and median nerve of the anterior surface of the elbow. This allows access to the anterior plane of the elbow in a minimal space.
Open reduction and internal fixation of the coronoid fracture, with a posterior to anterior screw fixation has been reported as an effective fixation method. 3 , 20 However, instability and re‐operation remain as significant problems. Moreover, this fixation approach poses a biomechanical disadvantage to axial stability because the insertion of the screw from a posterior larger fragment into an anterior smaller fragment is difficult for a firm hold of the screw into the anterior fragment. Additionally, the proper placement of the screw in a posteroanterior fashion with considerable inclination concerning the plane of the fracture is always challenging. Garrigues et al., 13 reported in a recent comparative study of surgical fixation techniques for coronoid fixation that higher stability and fewer complications were achieved with the suture lasso technique than posterior to anterior lag screws. These findings indicate the traditional fixation of coronoid fracture using screw inserted posteroanteriorly is not reliable. In this paper, we present a minimally invasive anterior to posterior screw fixation of the coronoid process through an anterior portal. Our approach has technical advantages in terms of accessibility, correct reduction of the fracture, and fixation/placement of the screw(s) via the anterior route in a plane that is perpendicular to the fracture.
In general, the need for rigid internal fixation increases with the size of the coronoid fracture fragment, but the fixation technique is critical, 19 especially when the coronoid fracture is small in size, and happens anteriorly or anterolaterally in posterolateral rotatory injury of the elbow. 20 , 21 Under such circumstances, fixation of coronoid process fracture with small or even comminuted fragments using cannulated screws placed posteroanteriorly is difficult and even contraindicated. However, satisfactory results can be obtained when screw fixation is carried out in anteroposterior fashion. In this study, a single small fragment was fixed with one screw and even two cannulated screws were used successfully for comminuted fragments.
Safety and Technical Feasibility
The key step for this procedure is the placement of the guide syringe from the cubital fossa anteriorly. As known, the cubital fossa is located in a depression on the anterior surface of the elbow joint with three borders along with an apex which is directed inferiorly. 22 It contains four main vertical deep structures from lateral to medial: radial nerve, biceps tendon, brachial artery and median nerve. 23 Our portal goes through just lateral to the biceps tendon, which safely avoids the medial brachial artery and median nerve. The radial nerve is at the outermost side of the cubital fossa and there is sufficient space between the radial nerve and biceps tendon for placement of the guide syringe. Anatomically the superficial veins of the cubital fossa are classified into four types according to the presence of the median cubital vein (MCV), which is close to the exit of the portal. 24 Therefore, the portal is prepared just lateral to the biceps tendon using a blunt hemostat to dissect slowly direct to the skin from deep to superficial. The anterior elevated skin is dissected where the tip of the hemostat is pointed and the guide syringe is then inserted through this portal. In this way, the medial brachial artery and median nerve are well protected by the biceps tendon and superficial MCV if present, is pushed away bluntly by the hemostat and secured. In this series, such complications as the injuries of deep structures and superficial veins were not encountered.
Limitations
There are certain limitations of this study: (i) the study population was relatively small; (ii) the fracture characteristics were limited to Regan–Morrey types II and type III; and (iii) all operations were all performed under the supervision of one surgeon at a single institute. Thus, the results obtained may not be reproducible by other surgeons or at other institutes. However, the use of this technique in a large study population with different fracture characteristics of the coronoid process will verify the potential of this surgical technique.
Conclusion
An anteroposterior reduction and maintenance of the coronoid fragment via a syringe guided screw fixation is a simple, minimally invasive approach for the surgical treatment of terrible triad injuries of the elbow, allowing concentric stability, and limiting soft tissue injury.
Author Contributions
Feiya Zhou, Hede Yan and Tokai B. Cooper carried out the conception and designing of the study, acquisitioned interpretation of data, and drafting the article; Xiaobin Luo, Xinglong Chen and Yiheng Chen conducted final drafting and English editing. All authors have reviewed, read and approved the manuscript. All authors listed meet the authorship criteria according to the latest guidelines of International Committee of Medical Journal Editors. All authors are in agreement with the manuscript.
Acknowledgement
This study was funded by Clinical Research Foundation of the 2nd Affiliated Hospital Wenzhou Medical University (SAHoWMU‐CR2018‐08‐417).
Contributor Information
Hede Yan, Email: yanhede@hotmail.com.
Feiya Zhou, Email: feiyazhou@yeah.net.
References
- 1. Hotchkiss RN. Fracture and dislocation of the elbow. In: Rockwood CA, Green DP, Bucholz RW, Heckman JD, editors. 4th ed. Philadelphia, PA: Lippincott‐Raven; 1996. p. 929–1024. [Google Scholar]
- 2. Pugh DM, Wld LM, Schemitsch EH, King GJ, McKee MD. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am. 2004;86(6):1122–30. [DOI] [PubMed] [Google Scholar]
- 3. Zhang C, Zhong B, Luo CF. Treatment strategy of terrible triad injury of the elbow: experience in Shanghai 6th hospital. Injury. 2014;45(6):942–8. [DOI] [PubMed] [Google Scholar]
- 4. Forthman C, Henket M, Ring DC. Elbow dislocation with intra‐articular fracture: the results of operative treatment without repair of the medial collateral ligament. J Hand Surg Am. 2007;32(8):1200–9. [DOI] [PubMed] [Google Scholar]
- 5. Papatheodorou LK, Rubright JH, Heim KA, Weiser RW, Sotereanos DG. Terrible triad injuries of the elbow:Does the coronoid need to fixed? Clin Orthop Relat Res. 2014;472(7):2084–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. McKee MD, Pugh DM, Wild LM, Schemitsch EH, King GJ. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique. J Bone Joint Surg Am. 2005;87(1):22–32. [DOI] [PubMed] [Google Scholar]
- 7. Zeiders GJ, Patel MK. Management of unstable elbows following complex elbow dislocation, the terrible triad injury. J Bone Joint Surg Am. 2008;90(4):75–84. [DOI] [PubMed] [Google Scholar]
- 8. Doornberg JN, Ring D. Coronoid fracture patterns. J Hand Surg Am. 2006;31(1):45–52. [DOI] [PubMed] [Google Scholar]
- 9. Doornberg JN, van Duijin J, Ring D. Coronoid fracture height in terrible triad injuries. J Hand Surg Am. 2006;31(5):794–7. [DOI] [PubMed] [Google Scholar]
- 10. Pai V, Pai V. Use of suture anchor for coronoid fracture in the terrible triad of the elbow. J Orthop Surg(Hong Kong). 2009;17(1):31–5. [DOI] [PubMed] [Google Scholar]
- 11. Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am. 2002;84(4):547–51. [DOI] [PubMed] [Google Scholar]
- 12. Jeon IH, Sanchez‐Sotelo J, Zhao K, An KN, Morrey BM. The contribution of the coronoid and radial head to the stability of the elbow. J Bone Joint Surg Br. 2012;94(1):86–92. [DOI] [PubMed] [Google Scholar]
- 13. Garrigues GE, Wray WH, Lindenhovius AL, Ring DC, Ruch DS. Fixation of the coronoid process in elbow fracture dislocation. J Bone Joint Surg Am. 2011;93(20):1873–81. [DOI] [PubMed] [Google Scholar]
- 14. Liu G, Hu J, Ma W, Li M, Xu R, Pan Z. Surgical treatment for terrible triad injury of the elbow with anteromedial coronoid fracture through combined surgical approach. J Int Med Res. 2018;46(8):3053–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Reichel LM, Milam GS, Reitman CA. Anterior approach for operative fixation of coronoid fractures in complex elbow instability. Tech Hand Up Extrem Surg. 2012;16(2):98–104. [DOI] [PubMed] [Google Scholar]
- 16. Josefsson JO, Gentz CF, Johnell O, Wendeberg B. Dislocations of the elbow and intra‐articular fractures. Clin Orthop Relat Res. 1989;246:126–30. [PubMed] [Google Scholar]
- 17. Egol KA, Immerman I, Paksima N, Tejwani N, Koval KJ. Fracture‐dislocation of the elbow functional outcome following treatment with a standardized protocol. Bull NYU Hosp Jt Dis. 2007;65(4):263–70. [PubMed] [Google Scholar]
- 18. Mathew PK, Athwal GS. King GJ (2009) terrible triad injury of the elbow: current concepts. J Am Acad Orthop Surg. 2009;17(3):137–51. [DOI] [PubMed] [Google Scholar]
- 19. O'Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD. Difficult elbow fractures: pearls and pitfalls. AAOS Instr Course Lect. 2003;52:113–34. [PubMed] [Google Scholar]
- 20. Ballesteros‐Betancourt JR, Garcia‐Tarrino R, García‐Elvira R, Muñoz‐Mahamud E, Fernández‐Valencia JA, Llusá‐Pérez M, et al. The anterior limited approach of the elbow for the treatment of capitellum and trochlea fractures. Surgical technique and clinical experience in 8 cases. Injury. 2020;22:1–11. [DOI] [PubMed] [Google Scholar]
- 21. Wu H, Liao Q, Zhu Y, Liu H. Surgical reconstruction of comminuted coronoid fracture in terrible triad of the elbow. Eur J Orthop Surg Traumatol. 2012;22(8):667–71. [DOI] [PubMed] [Google Scholar]
- 22. Ma CX, Pan WR, Liu ZA, Zeng FQ, Qiu ZQ, Liu MY. Deep lymphatic anatomy of the upper limb: an anatomical study and clinical implications. Ann Anat. 2019;223:32–42. [DOI] [PubMed] [Google Scholar]
- 23. Haładaj R, Wysiadecki G, Dudkiewicz Z, Polguj M, Topol M. The high origin of the radial artery (Brachioradial artery): its anatomical variations, clinical significance, and contribution to the blood supply of the hand. Biomed Res Int. 2018;2018:1520929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lee H, Lee SH, Kim SJ, Choi WI, Lee JH, Choi IJ. Variations of the cubital superficial vein investigated by using the intravenous illuminator. Anat Cell Biol. 2015;48(1):62–5. [DOI] [PMC free article] [PubMed] [Google Scholar]