

Abstract
Objectives:
The target of the current study was to evaluate and compare the shaping ability and buckling resistance of various single-file systems (TruNatomy [TRN], WaveOne gold [WOG], and XP-Endo Shaper [XPS]).
Materials and Methods:
Thirty recently extracted human first mandibular molars were chosen with severely curved mesiobuccal (MB) canals. Following access cavity preparation and determination of working length, teeth were randomly divided into three groups (n = 10) according to the instrumentation technique used, Group 1 (TRN), Group 2 (WOG), and Group 3 (XPS). Preinstrumentation and postinstrumentation, cone-beam computed tomography images were recorded at 3, 5, and 8 mm from the apex representing apical, middle, and coronal levels under the same circumstances, superimposed, and then canal transportation was determined using a particular equation. For buckling resistance calculation, files were loaded in the axial direction of the shaft and the maximum load was determined during the deflection of the file. One-way analysis of variance and Tukey test at 5% significance level were used to analyze data. Pearson's correlation between shaping ability and buckling resistance was performed.
Results:
XPS and TRN displayed significantly less canal transportation than WOG at the coronal and middle levels. While WOG recorded the highest value of buckling resistance, XPS recorded the least.
Conclusions:
XPS and TRN preserved the original curvature slightly better than WOG, while WOG reported the highest buckling resistance. There was a positive correlation between canal transportation and instrument resistance to buckle.
Clinical Relevance:
Preservation of the original shape of the canal after instrumentation is beneficial.
Keywords: Buckling resistance, cone-beam computed tomography, shaping ability, single file system, TruNatomy
Introduction
Root canal preparation comprises a crucial advance in endodontic treatment. The intricate anatomy of the canal presents challenges during instrumentation, which may hinder sufficient disinfection of the root canal system or cause procedural defects, for example, perforations, transportation, instrument separation, or ledges.[1]
Instrument development prompted single-file preparation systems, this new kinematic eliminates the need of utilizing a succession of instruments to prepare the original canal by utilizing just a single instrument.[2]
The TruNatomy System (TRN) (Dentsply Sirona) has recently been developed as a specially designed novel type of heat-treated NiTi instrument. TRN-shaping instruments are given in three distinct sizes, which are small (20/0.04 taper), prime (26/0.04 taper), and medium (36/0.03 taper). These files have an off-center parallelogram square cross-section design and a variable regressive taper.[3] These files have been gone through various heat treatments, increasing the elasticity and resistance to fatigue of the files.[3,4]
Persistent advancement of instruments and alloys prompted the improvement of more current file systems, for example, WaveOne Gold (WOG) which is a single-file system with reciprocal movement, alternating 170° counterclockwise and 50° clockwise movement.[5] The particular gold appearance of WOG instruments is due to the effect of a novel heat treatment method which applied after manufacturing. Raw metal is repeatedly heated and cooled, which not only gives it a golden color but also improves its strength and flexibility.[6]
XP-Endo Shaper (XPS) is another single-file system with continuous rotation, representing a novel snake-shaped instrument with adaptive core and innovative thermomechanically processed Ni-Ti alloy called Max-Wire (Martensite-Austenite-electropolish-fileX), which gives superelasticity and shape memory. This instrument is relatively straight in its martensitic phase (M-phase) at room temperature and changes to a curved shape when presented to intracanal temperature because of a phase transformation to austenitic phase (A-phase). Subsequently, this instrument displays a shape memory effect when embedded into the root canal (M-phase to A-phase) and has superelasticity during preparation. During its M-phase, it has an initial taper of 0.01 when cooled. While it presented to body temperature 35°C, the taper changes to 0.04.[7]
The ability of the root canal instrument to persist within the center of the root canal space without causing iatrogenic defects is one of the essential contributing elements to successful canal shaping.[8] Different methodologies have been used to evaluate the shaping ability of endodontic instrument, for example, longitudinal cleavage of the root, cross–sectioning, and radiographic imaging.[9]
Recently, cone-beam computed tomography (CBCT) has been proposed for this purpose, as it is nondestructive method that accurately determines the amount and direction of dentin removed after preparations.[10]
Buckling can be described as the elastic lateral deformation of the endodontic instrument when exposed to a compressive load in the direction of its axis.[11] In endodontic files, the low resistance to buckling can produce elastic or plastic deformation that impedes their progress in the canal apically.[12] Both the exploration of the canal orifices and the negotiation of the narrow canal walls need adequate buckling resistance.[13]
Many manufacturing approaches have been adopted to produce instrument systems for better preservation of the original canal path without deviation. Thus, the aim of this study was to evaluate and compare the canal transportation after using the recently introduced TRN with other single-file NiTi instruments (WOG and XPS) in addition to assessing the buckling resistance for each file system.
Materials and Methods
For this study, thirty newly extracted human mandibular first molars with separate mesiobuccal (MB) canals (Vertucci's type II anatomy) were chosen. This research used only the MB canals. According to Schneider's method,[14] all root canals should accommodate file # 15 as an initial file with curvature angle ranging from 25°–35° [Figure 1]. The study plan was approved by the Research Ethics Committee of the Faculty of Dentistry, Tanta University.
Figure 1.

The lower first molar’ mesiobuccal canal with a curvature angle of 27°, determined according to Schneider methodology
Round bur size # 3 followed by Endo-Z (Dentsply, Maillefer) was used to prepare the access opening cavities. By using water-cooled diamond disc (Komet; Brasseler, Lemgo, Germany), the distal root was cut at the furcation area.
After each tooth numbered, they were haphazardly distributed into three groups (n = 10) Group I: TRN, Group II: WOG Primary, and Group III: XP-Endo Shaper (XPS).
As per the manufacturer's instructions, transparent autopolymerizing acrylic resin (Acrostone, Dental and Medical Supplies, Cairo, Egypt) was mixed and applied to a silicon mold, then the teeth were placed vertically in this custom-made mold to maintain and stabilize samples while taking CBCT images.
For each sample, three preinstrumental tomograms were chosen for evaluation.[9] The first corresponded to 3 mm from the radiographic root apex (apical third), the second to 5 mm (middle third), and the third to 8 mm (coronal third). CBCT scanning pictures were captured with Cranex three dimension unit (Soredex, Helsinki, Finland) operating at 90 kV and 8 mA. Exposure parameters were maintained constant before and after instrumentation.
The working length of each MB root canal was visually calculated by passing the hand St-St K-file size 15 (Mani, Tochigi, Japan) till it became visible at the apical foramen and subtracted 1 mm from that length. For NiTi rotary instrumentation, a particular glide path was ensured using standardized K-files sizes 10 and 15.
X-Smart Plus endodontic motor (Dentsply, Maillefer) with a 16:1 gear reduction contra-angled handpiece was used following the manufacturer's preset mode and instructions for each preparation system as follows:
Group 1: Root canals’ preparation was carried out using TRN Prime (Dentsply, Sirona, Ballaigues, Switzerland) size 26 and 4% taper operated at 500 rpm and 1.5 Ncm.
Group 2: Root canals’ preparation was carried out using primary WOG (Dentsply, Maillefer, Switzerland) size 25 and 8% taper using the preset reciprocation mode.
Group 3: Root canals’ preparation was carried out using XPS (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland) (#30/04) at speed of 800 rpm and 1 Ncm torque in gentle 3–5 strokes until the canal was prepared to the full working length. The instrumentation process was carried out inside a rubber bowel containing water and heater at a controlled temperature of 37°C.
Copious irrigation with 3 mL of 5.25% NaOCl solution using a plastic disposable syringe with 27-gauge side-ended NaviTip (Ultradent Inc., South Jordan, Utah, USA) was used after each instrument. Then, the prepared canals were flushed with 3 mL of 17% ethylenediaminetetraacetic acid for 1 min and finally rinsed with normal saline solution.
The root canals were scanned after preparation to obtain three postinstrumentation tomograms of each specimen under the same scanning parameters of preinstrumented CBCT.
Assessment of canal transportation
Canal transportation was calculated for each sample at the three selected levels of MB canal after superimposing the pre- and postinstrumentation CBCT images using Adobe Photoshop software program (Adobe Systems, Mountain View, California, USA). To detect the canal wall differences between both the images, the final image was rotated over the initial image until their external contours coincided together. Then, the superimposed images were transferred to Auto-CAD software (Autodesk Inc., San Rafael, California, USA) to calculate canal transportation using a specific equation: (a1−a2)−(b1−b2) where: a1 is the shortest distance from the mesial edge of the root to the mesial edge of the uninstrumented canal, b1 is the shortest distance from the distal edge of the root to the distal edge of the uninstrumented canal, a2 is the shortest distance from the mesial edge of the root to the mesial edge of the instrumented canal, and b2 is the shortest distance from the distal edge of the root to the distal edge of the instrumented canal.[15] [Figure 2].
Figure 2.
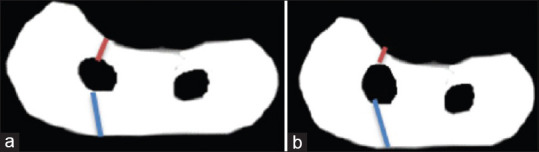
Illustration of the prepreparation (a) and postpreparation (b) measurements of the mesial and distal dentinal walls
As per this equation, a score of 0 corresponds to no canal transportation, positive value shows that the canal is transported to the furcation region (distal), while negative values illustrate transportation away from the furcation region (mesial).[15,16]
Measurement of buckling resistance
The head of the universal testing machine was connected to the handle of the instrument and the tip of the instrument was placed in a small punch cavity prepared on a stainless steel plate. A small punch hole (depth of 1 mm and width of 0.5 mm) was positioned in the center of the plate using a small round bur. The presence of this punch hole prohibits slippage of a file laterally during force application. Using a universal testing machine (Lloyd Instruments Ltd, Fareham, UK), with a speed of 1 mm/min, a gradually rising load was applied in the axial direction of each instrument from its head to the tip. The buckling resistance of the respective instrument was reported as the maximum load necessary to induce the lateral elastic displacement of 1 mm.[12]
Statistical analysis
Data were expressed as mean and standard deviation. Statistical analysis was performed using One-Way ANOVA with SPSS software program version 20 (SPSS Inc, Chicago, USA) at a significance level of P ≤ 0.05, then multiple pairwise comparisons were performed using post hoc Tuckey test. Finally, Pearson's coefficient (r) was performed to pick up a statistical correlation between shaping ability and buckling resistance of the tested instruments.
Results
Table 1 presents the descriptive statistics and comparison of the mean canal transportation at the apical, middle, and coronal levels for each group. Regarding canal transportation values, there was a statistically significant difference between the groups at the middle and coronal levels (P < 0.05). On the other hand, there were no significant differences (P = 0.1443) at the apical level.
Table 1.
Canal transportation mean and standard deviations at the three predetermined levels for the studied groups
| Groups | Apical | Middle | Coronal | P |
|---|---|---|---|---|
| Group 1 | 0.092±0.039a, A | 0.114±0.048a, B | 0.144±0.067a, D | 0.3275 |
| Group 2 | 0.090±0.022b, A | 0.250±0.047c, C | 0.286±0.023c, E | ˂0.0001 |
| Group 3 | 0.058±0.018d, A | 0.090±0.032d, e, B | 0.136±0.056e, D | 0.0239 |
Within the same raw, groups with the same lowercase were not statistically significant. Within the same column, groups with the same uppercase were not statistically significant
When comparing the root levels in each group, the coronal level recorded the highest value of canal transportation, while the apical level recorded the lowest value for all groups, with statistically significant difference except in the TRN group (P = 0.3275). The least canal transportation was recorded for the XPS group (0.095 ± 0.049), however, the highest value with the WOG group (0.209 ± 0.0933) regardless of the tested level with a statistically significant difference among groups (P < 0.0001).
Buckling resistance results revealed that the highest load to buckle was recorded by WOG, while the lowest value was recorded by XPS instruments with a statistically significant difference between the studied groups (P < 0.0001) [Table 2].
Table 2.
Buckling resistance (Newton) of tested endodontic instruments
| Groups | Buckling resistance (n) | P |
|---|---|---|
| Group 1 | 2.234a±0.197 | ˂0.0001 |
| Group 2 | 6.004b±0.379 | |
| Group 3 | 1.068c±0.124 |
Mean values with the same letters were not statistically significant
The Pearson correlation revealed a positive significant correlation between the shaping ability of the studied files at the middle and coronal levels represented by canal transportation and their buckling resistance (r = 0.853, P = 0.000 and r = 0.828, P = 0.000 respectively), while there was positive nonsignificant correlation at the apical level (r = 0.356, P = 0.192).
Discussion
Retaining the original shape of the canal, including the apical foramen and curvature, is recommended during preparation; therefore, the root canal should be enlarged evenly in all directions.[17] However, these targets often are not easy to accomplish, leading to uneven dentin removal and subsequent canal transportation, that might jeopardize the outcome of treatment.[18] Canal transportation is attributed to several variables, including the geometric characteristics of the instrument, additional thermal treatments during the manufacturing process, and its operating mode.[9,19,20,21,22]
Heat treatment process of NiTi alloys can improve the performance of rotary endodontic instruments during root canal preparation. Therefore, various rotary endodontic instruments (TRN, WOG, and XPS) made of different NiTi alloys were selected in this study.
Three-dimension method was used to assess the morphology of the tooth externally and internally and to evaluate the extent and direction of canal transportation before and after instrumentation.[23]
The transportation of the canal during instrumentation happens most often at three different levels with different degrees of root canal curvature:[24] the apical third where the apical part of the instrument enlarges the outer wall of the canal, the middle third where the instrument attempts to cut the inner wall of the canal, and at the opening facing the outer wall of the root canal.[25] In this study, canal transportation was therefore tested at these levels to examine all potential canal transportations.
Resistance to buckling is one of the important factors that control the advancement of the instrument apically during cleaning and chapping of curved and narrow root canal.[12] Therefore, it was investigated in this study.
MB root canals of mandibular first molars were chosen with extreme curves because they comprise canals which are often narrow and curved in two planes, raising the severity of instrumentation.[26] Initial canal width is standardized by selecting only MB canals accommodating size #15 K-file as an initial apical file and exhibiting (25°–45°) curvature according to Schneider's method,[14] this canal anatomy could probably lead to preparation defects like canal transportation.[27]
In addition, crowns were retained to mimic as closely as possible the clinical endodontic procedure in which tension on files during root canal instrumentation was generated by the intervention of cervical dentin projections.[28] Furthermore, distal root sectioning was performed to facilitate the evaluation of before and after instrumentation multi-slice CBCT scan images.[29]
Higher efficiency of the XPS instrument was observable relative to TRN and WOG. In relation to WOG, XPS and TRN showed significantly less transportation in the middle and coronal root areas. These results can be due to the creative rotary shaping XPS instrument, which is made of Max-Wire alloy that made it more flexible and resistant to cyclic fatigue. These results can be due to the creative rotary shaping XPS instrument, which is made of Max-Wire alloy that made it more flexible and resistant to cyclic fatigue, besides its opportunity to expand and contract to conform to the anatomy of the root canal. The instrument has a size/taper of 30/0.01, which can reach a final canal preparation of a minimum of 30/0.04 according to the manufacturer.[7]
This finding is in accordance with Azim et al., Hassan et al. studies, and Pacheco-Yanes et al., which revealed best-centering ability which retained the original canal anatomy of XPS files in comparison with other instruments.[7,30,31] On the other hand, this result disagrees with Versani et al. and Werdina and Bahnam studies which showed that XPS significantly altered the overall geometry of the root canal or it had a lower centering ability.[32,33] However, the contradictory results were difficult to compare and may be explained by differences in systems and methodology applied.
TRN was manufactured using a NiTi alloy heat-treatment process designed to maximize the fatigue resistance and flexibility of this system during root canal treatment.[3,4] It has a regressive taper and an off-centered parallelogram cross-section, and these can clarify its results. The TRN present study results were in agreement with Pit et al. that reported more conservative preparations were obtained with TRN and VDW.ROTATE systems as they provided less removal of the tooth substance and more preservation of the original shape of the canal during the instrumentation step of the endodontic treatment[34] and Kabil et al. who showed that XPS and TRN instruments caused very small canal transportation which were in the distal direction.[35]
There is an inverse relationship between instrument tapering and canal transportation.[36] The primary WOG instrument has an 8% taper over the first 3 mm. This is greater than the other two rotary instruments in which the TRN instrument has a constant 4% taper along its entire length, while XPS possesses an initial 1% taper along its whole length, which expands to a final 4% taper and this can explain the finding of WOG.[7] The findings of WOG were contradicted by Abdullah et al. and Singh et al. who showed the superiority of the WOG system over tested systems in terms of shaping ability, lower canal aberrations, and better performance.[37,38] However, the contradictory results were difficult to compare and may be explained by differences in systems and methodology applied.
The higher buckling resistance of WOG may be related to its larger taper of 8% along the apical 3 mm length, this design provides a larger core diameter of the file which can resist to buckle during axial force. These results were in agreement with Lopes et al. who record higher resistance of WOG to buckling.[39] On the other hand, XPS had the lowest resistance to buckling due to that it is manufactured from Maxwire alloy with a tip diameter of 0.30 mm and a constant 1% taper along the entire shaft which expands to a final 4% taper. In addition, the lower modulus of elasticity of this alloy leads to greater flexibility and superelastic behavior of XPS. These explanations were in agreement with Kwak et al. and Patil et al. who attributed higher buckling resistance to higher taper.[40,41]
The results revealed a strong correlation between the shaping ability of the tested files and its buckling resistance where the values of both variables tend to increase together. The increase in buckling resistance plays an important role in advancement of the instrument apically during the cleaning and shaping of narrow and curved root canals,[13] which reproduce efficient performance and less canal transformation.
Conclusions
The shaping abilities of XPS and TRN instruments are better than WOG instrument particularly at the middle and coronal portions of the curved root canal. WOG demonstrated greater buckling resistance than TRN and XPS systems. A positive correlation existed between the shaping ability of the tested instruments and their buckling resistance.
Financial support and sponsorship
The study was self-funded by the authors.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Hülsmann M, Peters O, Dummer P. Mechanical preparation of root canals: Shaping goals, techniques and means. Endod Topics. 2005;10:30–76. [Google Scholar]
- 2.Caviedes-Bucheli J, Moreno JO, Carreño CP, Delgado R, Garcia DJ, Solano J, et al. The effect of single-file reciprocating systems on Substance P and Calcitonin gene-related peptide expression in human periodontal ligament. Int Endod J. 2013;46:419–26. doi: 10.1111/iej.12005. [DOI] [PubMed] [Google Scholar]
- 3.Van der Vyver P, Vorster M, Peters O. Minimally invasive endodontics using a new single-file rotary system. Int Dent Afr. 2019;9:6–20. [Google Scholar]
- 4.Dentsply Sirona. TruNatomy Brochure. Johnson (TN): Dentsply Sirona; c2019. [Last updated on 2019 Sep 18; Last accessed on 2019 May 22]. Available from: https://www.dentsplysirona.com/en/explore/endodontics/trunatomy.html . [Google Scholar]
- 5.Özyürek T. Cyclic fatigue resistance of reciproc, WaveOne, and WaveOne Gold Nickel-titanium instruments. J Endod. 2016;42:1536–9. doi: 10.1016/j.joen.2016.06.019. [DOI] [PubMed] [Google Scholar]
- 6.Webber J. Shaping canals with confidence: WaveOne GOLD single-file reciprocating system. Roots. 2015;1:34–40. [Google Scholar]
- 7.Azim A, Piasecki L, da Silva Neto U, Cruz A, Azim K. XP Shaper, a novel adaptive core rotary instrument: Micro-computed tomographic analysis of its shaping abilities. J Endod. 2017;43:1532–8. doi: 10.1016/j.joen.2017.04.022. [DOI] [PubMed] [Google Scholar]
- 8.Al-Omari M, Dummer P, Newcombe R. Comparison of six files to prepare simulated root canals. Int Endod J. 1992;25:57–25. doi: 10.1111/j.1365-2591.1992.tb00738.x. [DOI] [PubMed] [Google Scholar]
- 9.Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30:559–67. doi: 10.1097/01.don.0000129039.59003.9d. [DOI] [PubMed] [Google Scholar]
- 10.Jain D, Medha A, Patil N, Kadam N, Yadav V, Jagadale H. Shaping ability of the fifth generation Ni-Ti rotary systems for root canal preparation in curved root canals using cone-beam computed tomographic: An in vitro study. J Int Oral Health. 2015;7:57–61. [PMC free article] [PubMed] [Google Scholar]
- 11.Beer FP, Johnston ER. Mechanics of Materials. 3rd ed. New York: McGraw-Hill; 1992. [Google Scholar]
- 12.Lopes HP, Elias CN, Mangelli M, Lopes WS, Amaral G, Souza LC, et al. Buckling resistance of pathfinding endodontic instruments. J Endod. 2012;38:402–4. doi: 10.1016/j.joen.2011.10.029. [DOI] [PubMed] [Google Scholar]
- 13.Jafarzadeh H, Abbott PV. Ledge formation: Review of a great challenge in endodontics. J Endod. 2007;33:1155–62. doi: 10.1016/j.joen.2007.07.015. [DOI] [PubMed] [Google Scholar]
- 14.Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 15.Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 16.Yamamura B, Cox TC, Heddaya B, Flake NM, Johnson JD, Paranjpe A. Comparing canal transportation and centering ability of endosequence and vortex rotary files by using micro-computed tomography. J Endod. 2012;38:1121–5. doi: 10.1016/j.joen.2012.04.019. [DOI] [PubMed] [Google Scholar]
- 17.Gonzalez-Rodrıguez M, Ferrer-Luque C. A comparison of Profile, Hero 642, and K3 instrumentation systems in teeth using digital imaging analysis. Oral Surg Oral Med Oral Pathol. 2004;97:112–5. doi: 10.1016/j.tripleo.2003.08.019. [DOI] [PubMed] [Google Scholar]
- 18.Weine FS, Kelly RF, Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975;1:255–62. doi: 10.1016/S0099-2399(75)80037-9. [DOI] [PubMed] [Google Scholar]
- 19.Ajuz N, Armada L, Goncalves L, Debelian G, Siqueira JF., Jr Glide path preparation in S-shaped canals with rotary pathfinding nickel titanium instruments. J Endod. 2013;39:534–7. doi: 10.1016/j.joen.2012.12.025. [DOI] [PubMed] [Google Scholar]
- 20.Short JA, Morgan LA, Baumgartner JC. A comparison of canal centering ability of four instrumentation techniques. J Endod. 1997;23:503–7. doi: 10.1016/S0099-2399(97)80310-X. [DOI] [PubMed] [Google Scholar]
- 21.Silva EJ, Tameirão MD, Belladonna FG, Neves AA, Souza EM, De-Deus G. Quantitative transportation assessment in simulated curved canals prepared with an adaptive movement system. J Endod. 2015;41:1125–9. doi: 10.1016/j.joen.2015.02.028. [DOI] [PubMed] [Google Scholar]
- 22.Hartmann MS, Barletta FB, Camargo Fontanella VR, Vanni JR. Canal transportation after root canal instrumentation: A comparative study with computed tomography. J Endod. 2007;33:962–5. doi: 10.1016/j.joen.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 23.Aguiar C, Donida F, Câmara A, Frazão M. Changes in root canal anatomy using three nickel-titanium rotary system: A cone beam computed tomography analysis. Braz J Oral Sci. 2013;12:307–12. [Google Scholar]
- 24.Gergi R, Arbab-Chirani R, Osta N, Naaman A. Microcomputed tomographic evaluation of canal transportation instrumented by different kinematics rotary nickel-titanium Instruments. J Endod. 2014;40:1223–7. doi: 10.1016/j.joen.2014.01.039. [DOI] [PubMed] [Google Scholar]
- 25.Freire LG, Gavini G, Cunha RS, Santos MD. Assessing apical transportation in curved canals: Comparison between cross-sections and micro-computed tomography. Braz Oral Res. 2012;26:222–7. doi: 10.1590/s1806-83242012000300007. [DOI] [PubMed] [Google Scholar]
- 26.Paqué F, Zehnder M, De-Deus G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J Endod. 2011;37:1394–7. doi: 10.1016/j.joen.2011.06.031. [DOI] [PubMed] [Google Scholar]
- 27.Peters OA, Boessler C, Paqué F. Root canal preparation with a novel nickel-titanium instrument evaluated with micro-computed tomography: Canal surface preparation over time. J Endod. 2010;36:1068–72. doi: 10.1016/j.joen.2010.02.023. [DOI] [PubMed] [Google Scholar]
- 28.Hashem AA, Ghoneim AG, Lutfy RA, Foda MY, Omar GA. Geometric analysis of root canals prepared by four rotary NiTi shaping systems. J Endod. 2012;38:996–1000. doi: 10.1016/j.joen.2012.03.018. [DOI] [PubMed] [Google Scholar]
- 29.Marzouk AM, Ghoneim AG. Computed tomographic evaluation of canal shape instrumented by different kinematics rotary nickel-titanium systems. J Endod. 2013;39:906–9. doi: 10.1016/j.joen.2013.04.023. [DOI] [PubMed] [Google Scholar]
- 30.Hassan R, Roshdy N, Issa N. Comparison of canal transportation and centering ability of Xp Shaper, WaveOne and Oneshape: A cone beam computed tomography study of curved root canals. Acta Odontol Latinoam. 2018;31:67–74. [PubMed] [Google Scholar]
- 31.Pacheco-Yanes J, Gazzaneo I, Pérez A, Armada L, Neves M. Transportation assessment in artificial curved canals after instrumentation with reciproc, reciproc blue, and XP-endo shaper systems. J Invest Clin Dent. 2019;10:e12417. doi: 10.1111/jicd.12417. [DOI] [PubMed] [Google Scholar]
- 32.Versani MA, Versiani MA, Carvalho K, Mazzi-Chaves J, Sousa-Neto M. Micro – Computed Tomographic evaluation of the shaping ability of XP-endo shaper, iRaCe, and EdgeFile systems in long oval-shaped canals. J Endod. 2018;44:489–95. doi: 10.1016/j.joen.2017.09.008. [DOI] [PubMed] [Google Scholar]
- 33.Werdina V, Bahnam I. Evaluation of centering ability of XP endo shaper, Edge Evolve and Hyflex CM in simulated curved canals (A comparative study) Irbil Den J. 2019;2:130–40. [Google Scholar]
- 34.Piţ A, Borcean I, Vărgatu I, Mai A, Shyblak M, Samir Mokdad S, et al. Evaluation of the time and efficiency of TruNatomy, VDW.ROTATE, Protaper gold and Reciproc blue in shaping root canals-an in vitro study. Romanian J Oral Rehab. 2020;3:250–8. [Google Scholar]
- 35.Kabil E, Katić M, Anić I, Bago I. Micro-computed evaluation of canal transportation and centering ability of 5 rotary and reciprocating systems with different metallurgical properties and surface treatments in curved root canals. J Endod. 2021;47:477–84. doi: 10.1016/j.joen.2020.11.003. [DOI] [PubMed] [Google Scholar]
- 36.Pique F, Ganahl D, Peters OA. Effects of root canal preparation on apical geometry assessed by microcomputed tomography. J Endod. 2009;35:1056–9. doi: 10.1016/j.joen.2009.04.020. [DOI] [PubMed] [Google Scholar]
- 37.Abdullah A, Mohammad A, Thomas S, Abdul M. Shaping ability of ProTaper Gold and WaveOne Gold nickel - titanium rotary file in different canal configurations. Saudi Endod J. 2018;8:202–7. [Google Scholar]
- 38.Singh S, Mirdha N, Shilpa PH, Tiwari RV, Abdul MS, Sainudeen S. Shaping ability of 2Shape and WaveOne gold files using cone-beam computed tomography. J Int Soc Prev Community Dent. 2019;9:245–9. doi: 10.4103/jispcd.JISPCD_411_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lopes W, Lopes H, Elias C, Vieira M, Batista M, Cunha R. Resistance to bending and buckling of WaveOne and Reciproc instruments. Endo-Endod Pract Tod. 2014;8:153–6. [Google Scholar]
- 40.Kwak SW, Ha JH, Lee W, Kim SK, Kim HC. Buckling resistance, bending stiffness, and torsional resistance of various instruments for canal exploration and glide path preparation. Restor Dent Endod. 2014;39:270–5. doi: 10.5395/rde.2014.39.4.270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Patil P, Gulve M, Kolhe S. Comparative evaluation of buckling resistance of Proglider and One-G file: An in vitro study. Endod. 2018;30:21–4. [Google Scholar]