

Abstract
Background and aim of the work.
Type 2 Diabetes Mellitus (T2DM) is a multifactorial disease, and it is considered a worldwide challenge for its increasing prevalence and its negative impact on patients’ wellbeing. Even if it is known that self-care is a key factor in reaching optimal outcomes, and males and females implement different self-care behaviors, sex-related differences in self-care of patients with T2DM have been poorly investigated. Especially, an overall view of the available evidence has not yet been done. Accordingly, this review aims to summarize, critically review, and interpret the available evidence related to the sex-related differences in self-care behaviors of patients with T2DM.
Methods.
An extensive literature review was performed with a narrative synthesis following the PRISMA statement and flowchart through four databases: PubMed, CINAHL, Scopus, and Embase.
Results.
From the 5776 identified records by the queries, only 29 articles were included, having a high-quality evaluation. Both females and males with T2DM must improve their self-care: more males reported performing better behaviors aimed at maintaining health and clinical stability (i.e., self-care maintenance) than females, but mainly in relation to physical activity. On the other hand, more females reported performing adequate behaviors aimed at monitoring their signs and symptoms (i.e., self-care monitoring) but with worse glycemic control and diabetic complications (i.e., self-care management).
Conclusions.
This review firstly provides an overall view of different self-care behaviors implemented by males and females with T2DM, showing that self-care management should be improved in both sexes. Health education must include the problems related to the diabetic pathology and the patient’s own characteristics, such as sex. (www.actabiomedica.it)
Keywords: self-care behaviors, sex-related difference, type 2 diabetes mellitus
Introduction
World Health Organization (WHO) estimates that Type II Diabetes Mellitus (T2DM) is the third-highest risk factor for premature mortality worldwide, preceded only by high blood pressure and tobacco (1). Moreover, extensive epidemiologic studies show that T2DM incidence is increasing worldwide. It affects 463 million people, with the overall figure predicted to rise to 629 million by 2045 and accounts for approximately 90% of all patients with diabetes (2). T2DM management is mainly focused on monitoring blood glucose levels, taking medication, and educating patients to maintain healthy behaviors (i.e., self-care behaviors) (3), which is fundamental to achieving good clinical outcomes and quality of life (3,4).
Self-care is a complex and natural decision-making process to maintain health, especially amongst chronic patients (4–6), such as patients with T2DM. According to Riegel’s theory, self-care behaviors could be influence actions aimed at maintaining both physiological and emotional stability (i.e., self-care maintenance), which facilitates the perception of specific signs and symptoms (i.e., self-care monitoring) and is directed at managing these upon onset (i.e., self-care management) (4,6). Overall, self-care maintenance, monitoring, and management are influenced by self-care self-efficacy, which is the level of confidence people have in their ability to perform adequate self-care, and self-care self-efficacy (4,7,8).
Since the strategic role of self-care behaviors implemented on the health outcomes of patients with chronic pathology is evident and well recognized (9–12), recently, many authors have been concentrating on the study of self-care determinants that can determine clinical outcomes, such as sex (9,10,13–17). In fact, understanding sex-related differences in self-care among chronic patients has a key role into designing evidence-based educational interventions and improving health outcomes. Also, in epidemiology, a significant difference between men and women in patients with T2DM, and other sex-related differences are highlighted in the presence of different genes and hormones, partially determined by environmental exposure (18,19). The field of sex-related differences is also studied in metabolic response to treatments (20), quality of life (21), and psychosocial variables (22). However, these differences should be considered together with the most common T2DM health determinants, which strongly influence treatment outcomes in people with T2DM (17,22), such as wellbeing, self-care and self-efficacy (23).
Therefore, to the best of our knowledge, there is a lack of synthesis regarding the sex-related differences in self-care behaviors in patients with T2DM. Indeed, the recent literature presents few empirical studies, and globally, these differences are confused and fragmented (24). This gap represents a drawback for the current need to plan strategic education interventions to support self-care in patients with T2DM.
Aims
The aim of this study was to summarize, critically review, and interpret the evidence related to sex-related differences in self-care behaviors of patients with T2DM.
Methods
Study design
It was performed an extensive literature search with a narrative synthesis (25). The articles included are published until September 2020, without an initial temporal limit, and they explored and described the sex-related differences regarding self-care behaviors in patients with T2DM.
Search method and study selection
The selection of studies for inclusion was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and flowchart (26). The PRISMA statement is an evidence-based minimum set of items to ensure the rigor of systematic searches and decrease selection bias, while the PRISMA flowchart identifies four phases (i.e., identification, screening, eligibility, and inclusion) that help guide the choice of records (26) (Figure 1). For this review, a three-stage approach was used for data synthesis because it was not possible to perform a meta-analysis due to the methodological and clinical heterogeneities among the included studies. Using keywords, such as ‘Self-care behaviors’; ‘Sex-related difference’; ‘Type 2 diabetes mellitus’ and their synonyms, the following literature databases were used: PubMed, Scopus, Embase and CINAHL. In addition, was performed an open search on Google Scholar. The main inclusion criteria were: (a) focused on sex-related differences in self-care behaviors of patients with T2DM, (b) primary research with quantitative study designs, (c) published in English. Finally, we also carried out backwards and forward citation tracking and we examined the reference lists (citation chasing) of included studies for the identification of additional studies (27). The only exclusion criterion was the low quality of papers after the appraisal of the eligible articles as requested for phase 3 of the PRISMA flow chart, as described below. The search syntax for bibliographic database searching is shown in Table 1.
Figure 1.
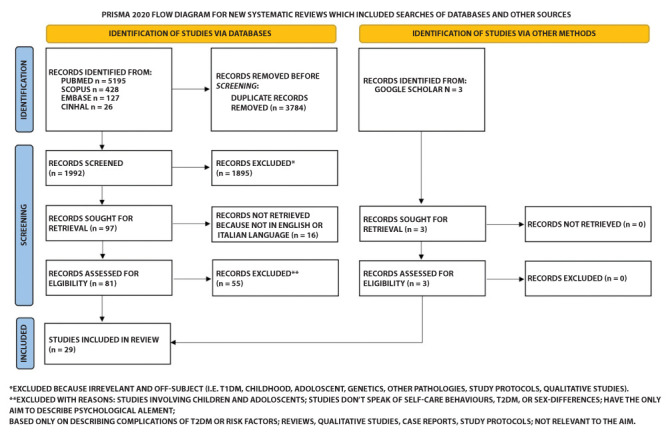
PRISMA flow chart
Table 1.
The search syntax for bibliographic database searching
| Database | Search Syntax | Search Date | Articles |
|---|---|---|---|
| PubMed | ((“diabetes mellitus, type 2”[MeSH Terms] OR “type 2 diabetes mellitus”[Text Word]) OR “diabetes type 2”[All Fields]) AND (“adult”[MeSH Terms] OR “adult”[All Fields] OR “adults”[All Fields] OR adult*[Text Word]) AND ((behavior*[Text Word] OR “self-concept”[MeSH Terms] OR “self-concept”[All Fields] OR “self-concept”[Text Word] OR “self-confidence”[Text Word] OR “self confidence”[All Fields] OR “self efficacy”[MeSH Terms] OR “self efficacy”[All Fields] OR “self efficacy”[Text Word]) OR (“Blood Glucose Self-Monitoring”[MeSH Terms] OR “self monitoring”[All Fields] OR “self monitoring”[Text Word”) OR (“self management”[MeSH Terms] OR “self management”[Text Word]) OR (“self care”[MeSH Terms] OR “self care”[All Fields] OR “self care”[MeSH Terms] OR “self-care”[Text Word]) OR (“Self Medication”[MeSH Terms] OR “self medication”[All Fields] OR “Self Administration”[MeSH Terms] OR “self administration”[All Fields])) AND (“Sex Characteristics”[MeSH Terms] OR “sex difference”[All Fields] OR “sex-related difference”[Text Word] OR “gender difference”[All Fields] OR “gender differences”[All Fields])) | 07 Sep. 2020 | 5195 |
| Scopus | TITLE-ABS-KEY ((“diabetes mellitus, type 2” OR “type 2 diabetes mellitus” OR “diabetes type 2”) AND (adult OR adults) AND (behavior OR behaviors OR “self concept” OR “self concept” OR “self-confidence” OR “self confidence” OR “self efficacy” OR “self efficacy” OR “Blood Glucose Self-Monitoring” OR “self monitoring” OR “self management” OR “self management” OR “self care” OR “self-care” OR “Self Medication” OR “Self Administration”) AND (“Sex Characteristics” OR “sex difference” OR “sex-related difference” OR “sex-related differences” OR “gender difference” OR “gender differences”)) | 07 Sep. 2020 | 428 |
| Embase | (“diabetes mellitus, type 2” OR “type 2 diabetes mellitus” OR “diabetes type 2”) AND (adult OR adults) AND (behavior OR behaviors OR “self concept” OR “self concept” OR “self-confidence” OR “self confidence” OR “self efficacy” OR “self efficacy” OR “Blood Glucose Self Monitoring” OR “self monitoring” OR “self management” OR “self management” OR “self care” OR “self-care” OR “Self Medication” OR “Self Administration”) AND (“Sex Characteristics” OR “sex difference” OR “sex-related difference” OR “sex-related differences” OR “gender difference” OR “gender differences”) | 07 Sep. 2020 | 127 |
| CINHAL | TX ((diabetes mellitus, type 2) OR (type 2 diabetes mellitus) OR (diabetes type 2)) AND (adult OR adults) AND (behavior OR behaviors OR (self concept) OR (self-concept) OR (self confidence) OR (self confidence) OR (self efficacy) OR (self-efficacy) OR (Blood Glucose Self- Monitoring) OR (self monitoring) OR (self-management) OR (self management) OR (self care) OR (self-care) OR (Self Medication) OR (Self Administration)) AND ((Sex Characteristics) OR (sex difference) OR (sex-related difference) OR (sex-related differences) OR (gender difference) OR (gender differences)) | 07 Sep. 2020 | 26 |
The selection process (Figure 1) was independently conducted by two authors (IB and FD), and, with a third researcher (CA), was conducted a discussion to reach a consensus to solve potential disagreements at each phase. During phase one (i.e., identification) were to find 5776 records, of which 97 records remain after duplicates removal and after the screening based on the title. Accordingly, in this screening phase (i.e. phase two), each screened record’s abstracts were assessed, and 55 records were excluded because their content did not meet the inclusion criteria (i.e. not written in English, were either based on qualitative research methodology or they were not related to the research question).
The quality appraisal of the 29 papers in the inclusion phase (i.e., phase 3) was assessed by the independent work of two authors (IB, FD), using standardized Checklist from the Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews (28). The JBI Checklist critical appraisal tool consists of 8 criteria related to qualitative research philosophy, research design, and trustworthiness (Table 2). The overall scoring, which indicates the two authors’ assessment (i.e., Yes, No, Unclear or Not/Applicable), was discussed within a consensus meeting. The authors’ agreement had to concern with their degree of credibility. Any disagreements between the authors were solved by consensus discussion or referred to a third reviewer (CA).
Table 2.
JBI Checklist - Critical appraisal
| Author, year | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|
| Caruso R., 2020 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Sahin S., 2020 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
2 3 |
1 3 |
1 1 |
3 1 |
6 6 |
| Tokunaga-Nakawatase Y., 2019 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Boonsatean W., 2018 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
1 1 |
3 1 |
7 6 |
| Alghafri T. S., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Aghili R., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
3 1 |
3 1 |
6 6 |
| Avedzi H. M., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Caruso R., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
3 1 |
1 1 |
7 8 |
| Naicker K., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
3 1 |
3 1 |
6 7 |
| Rossi MC., 2017 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
3 1 |
7 7 |
| Lipscombe C., 2016 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
3 3 |
7 7 |
| Mansyur C. L., 2016 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Vitale M., 2016 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
3 3 |
7 7 |
| Yin J., 2016 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
2 3 |
7 7 |
| Choi J. S., 2015 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
3 1 |
1 1 |
7 8 |
| Cuevas H. E., 2015 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
8 8 |
| Mansyur C. L., 2015 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
3 1 |
3 1 |
6 6 |
| Lipscombe C., 2014 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
3 1 |
1 1 |
7 7 |
| Shrestha A. D., 2013 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
3 1 |
7 7 |
| Badawi G., 2012 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
1 1 |
3 1 |
7 6 |
| Vaccaro J. A., 2012 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
1 1 |
8 7 |
| Chiu C., 2011 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
1 1 |
8 7 |
| Cherrington A., 2010 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
1 1 |
8 7 |
| Kacerovsky-Bielesz G., 2009 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
3 1 |
7 7 |
| Misra R., 2009 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
3 1 |
1 1 |
7 7 |
| Taru C., 2008 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 1 |
1 1 |
8 7 |
| Nau DP., 2007 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
2 1 |
7 6 |
| Brown SA., 2000 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
3 1 |
2 1 |
6 7 |
| Hawthorne K., 1999 | FD IB |
1 1 |
1 1 |
1 1 |
1 1 |
1 3 |
1 3 |
1 1 |
3 1 |
7 6 |
FD: Federica Dellafiore; IB: Irene Baroni
Data Extraction, Analysis and Synthesis
The included articles were analyzed according to a narrative analysis approach (25). Specifically, the authors read the full texts several times to get an overview of the content of each paper (Table 3) in accordance with the following format: (a) first author and publication’s years, (b) population/geographic area (c) study aim, (d) study methodology and design and (f) main results. After the entire research team provided an account of the main findings and seeing that a meta-analysis was not feasible for high heterogeneity, the authors, to allow better interpretation and usability of the results within the scientific literature, agreed to consider the ‘Middle-Range Theory of Self-Care of Chronic Illness’ as the framework that better represented these results (6). Therefore, the results were grouped into self-care maintenance, self-care monitoring, self-care management, and determinants of self-care (i.e. some psychosocial factors can be considered associated to self-care activities, such as social support and self-efficacy) (29) (Table 4).
Table 3.
Study characteristics and main results
| Author, Year | Aim | Sample | Design and methods | Main results |
|---|---|---|---|---|
| Caruso R. et al., 2020 | (1) To describe sex-related differences in self-care. (2) To identify determinants of self-care related to sex; (3) To investigate how sex interacts with the effect of clinical and socio-demographic variables on self-care in adults with T2DM. | The study enrolled a consecutive sample of 540 adults with T2DM. | The study is a multicenter cross-sectional study, secondary analysis. Self-care maintenance, self-care monitoring, self-care management, and self-care confidence were measured by the Self-Care of Diabetes Inventory (SCODI). | Females perform equal or better self-care than males. An increase of one point in female’s persistence self-care confidence resulted in a 3% decrease in the risk of inadequate self-care. Among females, having been diagnosed of T2DM from <10 years showed a lower risk of inadequate self-care management. |
| Sahin S. et al., 2020 | To explore the influence of self foot care behavior and illness acceptance on the risk of developing diabetic foot ulcers (DFU) in adults with T2DM. | 246 adults, males and females, with T2DM. | Cross-sectional study. Data were collected using: socio-demographic questionnaire, The Michigan Neuropathy Screening Instrument Questionnaire (MNSI-Q), Diabetes Foot Self-Care Behavior Scale (DFSBS), Acceptance of Illness Scale (AIS). | AIS scores in male patients are higher than that among female patients. Male gender is a determinant of good foot care behaviour and determinants of AIS were found to include male gender, longer duration of education, low economic status, presence of other non-infectious diseases and hospitalization in the past year. |
| Tokunaga-Nakawatase Y. et al., 2019 | To assess physical activity behavior of Japanese male and female patients with T2DM from the viewpoint of dietary intake and weight control. | Patients with T2DM were being treated at the diabetes clinic of an educational hospital. | A cross-sectional study was conducted. Physical activity self-management behavior was assessed using the valuation Scale for Self-Management Behavior Related to Physical Activity of Type 2 Diabetic Patients (ES SMBPA-2D). | Non-obese-but-overeating (NO/OE) female patients showed higher levels of HbA1c than not-overeating females. Furthermore, In female patients, unlike the males, patients in the (B) NO/OE category showed higher levels of HbA1c than patients in other groups, and there was no relationship between physical activity self-management behavior, dietary intake, and BMI. |
| Boonsatean W. et al., 2018 | 1. To investigate the illness perception and self-management among Thai women and Thai women and men with T2DM. 2. To investigate the psychometric properties of the translated instruments used. | A multistage sampling method with 220 men and women with T2DM that lived in communities. | Cross-sectional study. Data were collected with interviews, after assurancing confidentiality and giving the possibility to withdraw from the study. | Men showed higher confidence in the T2DM treatment effectiveness than women. Females reported higher mean score for glucose management and healthcare use than men. Although, women demonstrated higher mean scores for glucose management and of healthcare use than men, who showed higher mean scores of dietary control and of physical activity than women. |
| Alghafri T. S. et al., 2017 | To describe the physical activity patterns of adults with T2DM and examine the sociodemographic factors, physiological factors and perceptions of physical activity associated with recommended physical activity levels of ≥600MET-min/wk and prolonged sitting time. | 305 participants over Muscat, calculated using an estimated 15% prevalence of meeting the physical activity recommendations in patients with diabetes. | A cross-sectional study. Data were collected using the Global Physical Activity Questionnaire conducted in 17 randomly selected primary health centres in Muscat. | More males than females reported being at an “action” or “maintenance” stage of physical activity. Compared to males, females were less physically active across the three physical activity domains (work, travel and leisure). Females reported longer sitting time than males and are more likely to be obese, prefer to pray and stay at home for child care reasons, and so there were significantly more females with uncontrolled diabetes. |
| Aghili R. et al., 2017 | To determine behavioral and psychosocial differences among patients 30–65 years old, with T2DM dignosis. | 441 adults (203 women and 177 men) who had been diagnosed with T2DM at least six months prior to enrollment. | A descriptive-analytic cross-sectional, non-interventional, observational study. Data were collected using (EQ-5D-3L) questionnaire. In addition, to measure the state of health-related quality of life (HRQoL), EQ visual analogical scale (EQVAS) was used. | Significant age and gender differences were seen regarding EQ-5D-3L, with men under the age of 55 reporting the highest level of health state compared to women and men above the age of 55. In particular, women tend to have higher BMI compared to men. Behaviors toward diabetes care are different between genders, with women having worse diabetes control, with a basal insulin dose being higher in women compared to men, causing higher score on anxiety for women with diabetes. |
| Avedzi H. M. et al., 2017 | To examine self-reported dietary behaviours and actual food intakes among adultmen and women with T2DM participating in Alberta’s Caring for Diabetes (ABCD) Study. | Of the 248 eligible participants, 170 were selected for the analysis. | An observational cohort study. Participants completed 3-day food records and questions about glycemic index (GI) concept knowledge and dietary behaviours. Daily average GI and glycemic load (GL) were calculated for all carbohydrates consumed. | About 60% of men had carbohydrate intakes below the Acceptable Micronutrient Distribution Ranges (AMDR) while the 80% of women had protein and total fat intakes above the AMDR. 40% of women consumed carbohydrates below the AMDR, exceeding the AMDR for protein and total fat intakes. |
| Caruso R. et al., 2017 | To describe T2DM patients’ gender differences related to their wellbeing, self-care and self-efficacy. | A convenience sample of 150 patients with a diagnosis of T2DM. | A secondary analysis of data from a cross-sectional study. The following instruments were used to collect data: WHO-Wellbeing questionnaire (WBQ), General self-efficacy (GSE), Diabetes specific Self-efficacy (SE_spec), Summary of Diabetes Self-Care Activities (SDSCA). | Men have a higher perception of self-efficacy than women. GSE was not significantly different among men and women (p = 0.186), while diabetes specific self-efficacy was higher in men (p = 0.023). |
| Naicker K. et al., 2017 | To determine if symptoms of depression and anxiety are differentially associated with clinical diabetes measures and self-management behaviours in individuals with T2DM, and whether these associations vary by patient sex. | 2035 individuals who were confirmed in the sub-study to have T2DM, based on results of three repeated laboratory tests (fasting plasma glucose, oral glucose tolerance, and serum HbA1c levels). | A cross-sectional analysis. Depression and anxiety symptoms were measured in HUNT 3 using a 7-item mental health index (CONOR-MHI) and anxiety symtoms with HSCL-10 and Hospital Anxiety and Depression Scales (HADS). | More women than men had either depressive or anxious symptoms only, but an association between depression/anxiety and glycemic control was found only in men. Anxious symptoms alone were associated with high serum CRP levels in women (OR = 1.57 [95% CI: 1.05, 2.34]), as well as a greater tendency to report avoiding saturated fats in women (OR = 1.17 [1.17, 1.94]). |
| Rossi M. C. et al., 2017 | To assess gender differences in T2DM in terms of diabetes-related distress, physical and psychological well-being, empowerment, perceived social support and other measures of satisfaction with treatment and care. | A random sample of 2390 patients with T2DM was selected by 26 diabetes outpatient clinics in Italy. | A cross-selectional study. Secondary analysis of the BENCH-D data. Data were collected using: SF-12 Health Survey, WHO-5 well-being index, Problem Areas in Diabetes (PAID) 5, Health Care Climate Questionnaire, Patients Assessment of Chronic Illness Care, Diabetes Empowerment Scale, Diabetes Self-care Activities, Global Satisfaction for Diabetes Treatment, Barriers to Taking Medications, Perceived Social Support. | Women had poorer scores for: physical functioning, psychological well-being, self-care activities dedicated to physical activities, diabetes-related distress, satisfaction with treatment, barriers to medication taking, satisfaction with access to chronic care and healthcare communication, and perceived social support than men. Furthermore, women showed a lower prevalence of known diabetes complications than men, higher levels of HbA1c, total and LDL-cholesterol and BMI. |
| Lipscombe C. et al., 2016 | To describe and examine the association between physical activity, smoking, and alcohol consumption according to individual DD (diabetes distress) subscales and total DD. | It was used a using mixed methods sampling, recruiting a total of 1971 patients. | A cross-selectional study. Data were collected using: e 17-item Diabetes Distress Scale (DDS-17), Alcohol Use and Disorders Identification Test (AUDIT), Canadian Community Health Survey (CCHS). | In both male and females physical inactivity was associated with a greater probability of moderate distress with moderate-severe anxiety symptoms, with an increased odds of inactivity in women only, influencing DD negatively. |
| Mansyur C. L. et al., 2016 | To compare more acculturated men and women with those who were less acculturated. | 248 Hispanic patients from 4 community health centers. | A cross-sectional, secondary analysis of baseline survey data from a RCT. Dependent and independent variables were measured by Likert scales. The dependent variable, self-efficacy (SE), was measured using the Self-Efficacy for Diabetes Scale. | Men were more discouraged than women from following a healthful diet but who ate the same foods anyway tended to have lower self-efficacy; women who received more support and who ate the same foods as their families tended to have higher self-efficacy. |
| Vitale M. et al., 2016 | To investigate, in a large, nationally representative, cohort of men and women with T2DM, the quality of diet, the adherence to the nutritional recommendations with regard to fat, fiber and added sugars and their relation with the plasma lipid profile. | 2573 people with T2DM, 1535 men and 1038 women, aged 50 e 75. | A RCT study was conducted to compare the impact of glucose lowering drugs on cardiovascular events. The dietary habits were assessed with the Italian version of the European Prospective Investigation into Cancer and Nutrition (EPIC) questionnaire. | BMI was significantly higher in women and glucose control, evaluated as HbA1c, was marginally better in women. Plasma LDL-cholesterol and HDL- cholesterol were significantly higher in women. This happened because the proportion of energy from total fat and saturated fat was significantly higher in women, consuming sugars added by the consumer, exceeding the recommended intake for saturated fat. The intake of fiber and the proportion of cohort achieving the recommend intake were generally low, and significantly higher in women; accordingly, the glycemic load of the diet was lower in women. |
| Jin J. et al., 2016 | To examine factors associated with persistent poor glycemic control in Chinese patients with T2DM. | 15 473 people with T2DM were enrolled in the study. | A Cross-sectional study. Data were collected using: standardized procedures for BMI and blood pressure (BP) and The EuroQol-5D for quality of life assessment. Student’s t-test,Mann–Whitney U-test. | Female gender was associated with more unactivity and poor glycemic control, and lower HRQoL than their men counterparts. |
| Choi J. S. et al., 2015 | To identify gender-specific factors (demographic and disease-related characteristics, barriers to diabetes self-care behaviors, social support, family support, diabetes self-efficacy, and depression) influencing diabetes self-care behaviors and health-related quality of life among older adults. | 278 older adults (77 women, 201 men) 65 or older, diagnosed with T2DM for at least 6 months, who were treated with medications, and who agreed to participate in the original research. | Cross-sectional study, a secondary analysis. Data were extracted from the original study (Chang, 2010), regarding demographic and disease-related characteristics, barriers to diabetes self-care, social support, family support, diabetes self-efficacy, depression, diabetes self-care behaviors, and health-related quality of life. | The number of diabetes-related complications (β = –0.17, p = 0.015), diabetes self-efficacy (β = 0.25, p = 0.001), and depression (β = –0.39, p < 0.001) were significant predictors of older men’s self-care behaviors. While in older women: diabetes, self-care (β = 0.50, p < 0.001), depression (β = –0.34, p = 0.006), duration of diabetes (β = 0.25, p = 0.035), and barriers to diabetes self-care behaviors (β = –0.33, p = 0.006) were significant predictors of diabetes self-care behaviors. |
| Cuevas H. E. et al., 2015 | To describe patterns of home self-monitoring of blood glucose (SMBG) in Mexican Americans with T2DM diagnosis. | In total 83 individuals of Mexican Americans diagnosed with T2DM. | It was used a randomized repeated-measures pre-test/post-test control group design. Glucometer data from an experimental group (diabetes self-management education plus nurse case management) and a comparison group (diabetes self-management education only) were analyzed. | In terms of gender, more females than males never checked their blood glucose levels, and more females than males checked blood glucose levels more than one time per week. |
| Mansyur C. L. et al., 2015 | To explore how social support, social norms and barriers are associated with self-efficacy and self-care adherence in Hispanic patients with T2DM and how these differ for men and women. | 248 Hispanic men and women with uncontrolled T2DM, who were randomized: 123 to intervention and 125 to usual care | A randomized control trial. Participants randomized to the intervention group were shown an interactive educational program for diabetes management containing culturally targeted video segments, educational modules and games. | Women had significantly lower self-care adherence than men tending to be significantly more obese than men, although both T2DM men and women tended to be obese on average. |
| Lipscombe C. et al., 2014 | To examine the association between physical inactivity and anxiety symptoms in a community-based of people with T2DM. | 1953 participants in the current study took part in the baseline evaluation of the Evaluation of Diabetes Treatment (EDIT) study in 2011. | A cross-selectional study. Data were collected using The Generalized Anxiety Disorder 7-item scale (GAD-7) to assess anxiety symptoms and the amount of days over the past month spent engaged in sports or exercise for at least 15 min for physical inactivity. | Women were more likely than men to report having mild and moderate-severe anxiety symptoms, moreover mild anxiety symptoms were associated with an increased odds of inactivity in women only, whereas moderate to severe anxiety symptoms were associated with an increase in the odds of inactivity for men only. |
| Shrestha A. D. et al., 2013 | To assess the gender differences in care, symptoms, mode of diagnosis and self-management of T2DM. | The primary purpose of this study was to assess the gender differences in care, symptoms, mode of diagnosis and self-management of T2DM. | A cross-selectional study. Data were collected using a semi-structured questionnaire, which was about personal information, symptoms of diabetes, mode of diagnosis followed by date of diagnosis and treatment, self management and self-efficacy. | Lesser women were following the recommended healthy diet practices than men, having a worse glycaemic control; women with lower self-efficacy couldn’t follow good diet. Furthermore, women tend to present more depressive somatic symptoms associated with diabetes while men were more likely to present fatigue, muscle aches and sexual dysfunction. |
| Badawi G. et al., 2012 | To investigate the characteristics of self-rated health in a Canadian community sample of people with diabetes | 1837 adults with T2DM participating in the Montreal Diabetes Health and Well-Being Study. | A cross-selectional study. Data were collected using: the World Health Organization Disability Assessment Schedule II to assess disability and the Patient Health Questionnaire to assess depression. | Physical activity were associated with better health status in men. Furthermore, they were more likely to rate their health as excellent, while women were more likely to rate their health as good, fair or poor. |
| Vaccaro J. A. et al., 2012 | To examine gender differences in medical advice related to diet and physical activity for obese African American adults (N = 470) with and without T2DM. | A stratified cluster sampling design was performed. Of 9990 men and women, 5692 were interviewed and examined. | A cross-selectional study. Data were collected using: NHANES survey, the Canadian Community Health survey (CCHS) and especially the Behavioral Risk Factor Sur veillance System (BRFSS). | Lesser women were following the recommended healthy diet practices than men, in fact males with T2DM were five times more encouraged to reduce fat and calories as compared with females with T2DM. |
| Chiu C. et al., 2011 | To investigate gender differences in biological, behavioral, and psychosocial variables, and how these variables explain the gender–functional limitations relationship in adults with T2DM. | 1619 adults with T2DM from the Health and Retirement Study and its diabetes specific mail survey. | Data were collected from the HRS (2003, Health and Retirement Study) diabetes specific mail survey. | Women have better dietary abits but significantly higher BMI, than men, and poorer scores for physical functioning and self-care activities dedicated to physical activities were founded. Furthermore, women had higher levels of HbA1c than men, and it was found a higher incidence of diabetic complications among women. |
| Cherrington A. et al., 2010 | 1. To examine the relationship between depressive symptoms and glycemic control in patients with T2DM in a primary care setting and to assess whether self-efficacy plays a mediating role within that relationship. 2. To examine the gender influence on these relationships. | 162 patients were recruited by clinic staff during routine clinic visits and referred for possible participation if they had a previous diagnosis of T2DM. | A cross-selectional study. Data were collected by patient interview and medical chart review, fundamental for the HbA1c most recent value. Center for Epidemiologic Studies Depression (CES-D) Scale was used for assessing depression. | Between males there is strong evidence that diabetes self-efficacy mediates the effect of depressive symptoms on glycemic control, but this was not statistically significant for women. Although, the relationship between self-efficacy and glycemic control (r = -0.18) approached significance for the females (P = .07). |
| Kacerovsky-Bielesz G. et al., 2009 | To test the hypothesis that sexspecific differences exist in terms of (a) glucometabolic control and (b) social and psychological factors. | A consecutive sampling of 257 patients with T2DM. | A cross-selectional study with data collection from a metropolitan diabetes outpatient service employing clinical testing and standardised psychological questionnaires. | In women BMI tended to be higher but did not significantly differ compared with men. More women than men reported no or very rare alcohol consumption while HbA1c tended to be higher, but did not significantly differ compared with men. |
| Misra R. et al., 2009 | To examine gender and ethnic differences in diabetes outcomes, psychosocial predictors, knowledge, and perceived difficulty in self-management behaviors among T2DM patients. | A convenience sample of 180 T2DM patients from two health clinics in Bryan and College Station. | A cross-selectional study. Data were collected using: The Revised Ideas About Diabetes (IAD-R) scale, The PRQ85 scale, DQIP instrument, The Diabetes Specific Quality of Life Scale (DSQOL). | Females felt more inhibited by their disease, feeling it as a burden and restriction in their social interactions, having a less positive outlook. Females reported more difficulty with dietary adherence than men. Despite this, females reported higher social support and a lower knowledge of the disease. |
| Taru C. et al., 2008 | To establish effective dietary self-management behavior for T2DM male and female, by focusing on how dietary intake and dietary self-management affect control indices of T2DM. | 170 patients with T2DM diagnosis, 93 men and 77 women. | A cross-selectonal study. Data were collected using: clinical blood data (HbA1c, T-colesterol, HDL-cholesterol), BMI, food frequency questionnaire (FFQ), Lifecorder EX to calculate physical activity, Metavine-S to measure resting energy expenditure, the Dietary Self-management Behavior Questionnaire (DSBQ). | Reducing the amount of cooking salt may be effective for: 1. Reducing dietary intake 2. Prevention of complications such as hypertension 3. Suppression of appetite, decreasing the carbohydrate intake. It is more effective than simply emphasizing the need to reduce such intake. |
| Nau D. P. et al., 2007 | To determine the main effects, and interactive effect, of depression and gender on patients’ adherence to oral diabetes medications. | More than 6000 adults were recruited from medical and pharmacy claims data. | A cross-selectional study. Data were collected using: Patient Health Questionnaire (PHQ-8), Patient Health Questionnaire (PHQ-9), a summated scale consisting of 2 items to investigate family or friend’s support, a 5-point Likert scale to measure self-efficacy. | Findings showed a significant association of depression severity and worse medication adherence in men, while women were relatively adherent regardless of depressive symptom severity. |
| Brown S. A. et al., 2000 | To describe metabolic control, knowledge, andhealth beliefs of Mexican Americans with T2DM. | 252 people with T2DM diagnosis. 126 for the treatment group and 126 for the control group. | A randomized clinical trial study. Data were collected using: a questionnaire based on National Standards for Diabetes Patients Education Programs and other programs realized for clinic data, such as HbA1c. | Between individuals treated with diet only males exhibited higher HbA1c levels than females, conversely, individuals on insulin only, females showed a higher mean of HbA1c compared with males. |
| Hawthorne K. et al., 1999 | To study factors such as sex, educational status and place of care and study their influence on other factors, such as: knowledge and self-management of diabetes, and glycemic control. | 201 Pakistani moslem patients with T2DM attending the Manchester Diabetes Centre (MDC), and 10 general practitioner (GP). | A cross-selectional study. Interviews were conducted with closed and opened questions, which could help the patient to express their feelings. | Women had poorer glycemic control than men and their knowledge of diabetic complications was generally lower than in men. They reported that knowledge of diabetic complications was generally lower in women than in men |
Table 4.
Data Synthesis within the Middle-Range Theory of Self-Care of Chronic Illness framework
| Author, year | Self-care Maintenance | Self-care Monitoring | Self-care Management | Self-care determinants |
|---|---|---|---|---|
| Caruso R., 2020 | X | X | X | |
| Sahin S., 2020 | X | |||
| Tokunaga-Nakawatase Y., 2019 | X | |||
| Boonsatean W.,2018 | X | X | X | |
| Alghafri T. S., 2017 | X | X | ||
| Aghili R., 2017 | X | X | X | |
| Avedzi H. M., 2017 | X | |||
| Caruso R., 2017 | X | |||
| Naicker K., 2017 | X | X | ||
| Rossi M. C., 2017 | X | X | X | X |
| Lipscombe C., 2016 | X | X | ||
| Mansyur C. L., 2016 | X | |||
| Vitale M., 2016 | X | X | ||
| Yin J., 2016 | X | |||
| Choi J. S., 2015 | X | |||
| Cuevas H. E., 2015 | X | |||
| Mansyur C. L., 2015 | X | X | ||
| Lipscombe C., 2014 | X | |||
| Shrestha A. D., 2013 | X | X | X | |
| Badawi G., 2012 | X | X | ||
| Vaccaro J. A., 2012 | X | |||
| Chiu C., 2011 | X | X | X | X |
| Cherrington A., 2010 | X | |||
| Kacerovsky-Bielesz G., 2009 | X | X | X | |
| Misra R., 2009 | X | X | ||
| Taru C., 2008 | X | |||
| Nau D. P., 2007 | X | |||
| Brown S. A., 2000 | X | |||
| Hawthorne K., 1999 | X | X | ||
| Total N° 29 | 18 (62%) | 11 (38%) | 5 (17%) | 19 (65%) |
Results
Of the 29 included articles, 25 reported cross-sectional data collection (Table 3), and most of them (n=12) were conducted in American countries (USA, Canada, and Mexico). Of the other articles, eight were conducted in European countries (Italy, United Kingdom, Spain, Germany, Austria, and Norway), and nine in Middle Eastern countries (Japan, China, Nepal, Thailand, Oman, Iran, and South Korea). The included articles’ data extraction identified four main areas belonging to self-care maintenance, self-care monitoring, self-care management, and determinants of self-care (Table 4).
In general, some articles reported results on the self-care construct in general which highlight the non-homogeneity of the results that emerged from this review. Caruso et al. 2020 (17) found that females perform equal or better self-care than males, while the same authors in 2017 (30) reported that there were no significant sex-related differences related to self-care. Previous studies showed the same disagreement: Yin J. 2016 (31) reported that females were more intensively treated and had better self-care behaviors with high levels of treatments’ adherence; while Choi J.S., 2015 (32) stated that older (≥ 70 years) men scored slightly higher on diabetes self-care behaviours compared to older women but with no statistically significant difference, and, finally, Mansyur C. L. 2015 (33) reported that women had significantly lower self-care adherence than men. Additionally, a more specifical narrative analysis was performed, and four main areas describing an overall view of sex-related differences emerged from the results of 29 included articles (Table 4).
Self-care Maintenance: diet and weight control, exercise and physical activity, medications and insulin therapy
Eighteen studies reported results on self-care maintenance activities. Overall, despite substantial evidence showing that males practised more adequate physical activity than females, conflictual results were found on dietary, weight and concomitant factors (i.e. foot care, smoke and alcohol).
Boonsatean W. et al. 2018 (34) showed that men performed higher scores of dietary control than women, similarly to Vaccaro J. A.2012 (35) and Shrestha A. D.2013 (36) that reported that lesser women were following the recommended healthy diet practices than men, and to Misra R.2009 (37) that found that females were also more likely to report difficulty with dietary adherence. Conversely, Avedzi H. M. et al. 2017 (38) and Vitale M. et al. 2016 (39) stated that women consumed more legumes, vegetables, fruits, eggs, and milk and avoided high fats/caloric foods than men, like Naicker K. et al. 2017 (40) that reported a greater tendency of avoiding saturated fats in women. In this regard, Vitale M. et al. 2016 (39) highlighted some discordant points in the eating behaviour of males and females: it seems that the proportion of energy from total fat and saturated fat was significantly higher in women than in men, but in women, the intake of fibre was significantly higher than in men with a lower global glycaemic load of the diet. And again, Chiu C. et al. 2011 (41) stated that women have better dietary habits but significantly higher BMI than men. Finally, Taru C. et al. 2008 (42) assumed that for females, “reducing the amount of cooking salt” may be more effective for reducing dietary intake than simply emphasizing the need to reduce such intake.
Specifically, on weight control, Tokunaga-Nakawatase Y. et al. 2019 (43) reported that non-obese-but-overeating female patients showed higher levels of HbA1c than not-overeating females, unlike the males. Aghili R. 2017 (44) affirm that women tend to have higher BMI compared to men. Similarly, Mansyur C. L. 2015 (33) found that women tended to be significantly more obese than men, although both T2DM men and women tended to be obese on average; and Rossi M. C. et al., 2017 (45) report that higher levels of total and LDL-cholesterol, and BMI were found in women. Badawi G. et al., 2012 (46) add that obesity was associated with poorer health status in women but not in men. Also, Vitale M. et al. 2016 (39) agree that BMI was significantly higher in women; instead, Kacerovsky-Bielesz G. et al., 2009 (22) confirm that BMI tended to be higher in women but did not significantly differ compared with men.
Considering the physical activity, Boonsatean W. et al., 2018 (34) showed that men reported practicing more physical activity than women. Alghafri T.S. et al., 2018 (47) also agree that compared to males, females were less physically active and tended to report longer sitting time. Also, Rossi M. C. 2017 (45) and Chiu C. 2011 (41) reported that women had statistically significant poorer scores for physical functioning and self-care activities dedicated to physical activities. On the same line, Shrestha A. D.et al. 2013 (36) found that women were straggling behind men in the recommended exercise for at least five days a week. But, Badawi G. et al., 2012 (46) concluded that physical activity was associated with better health status in men only, and Kacerovsky-Bielesz G. et al., 2009 (22) reported that more women than men performed regular physical exercise.
Based on medications, insulin therapy, and risk factors control, Brown S.A. et al., 2000 (48) reported that among individuals treated with diet only, males exhibited higher HbA1c levels than females; conversely, for individuals on insulin only, females showed a higher mean of HbA1c compared with males. Aghili R. et al., 2017 (44) add that the basal insulin dose was higher in women compared to men, and Chiu C. et al. 2011 (41) concluded that there were no significant sex-related differences in the medication adherence. Investigating blood pressure as a concomitant factor for diabetes, Aghili R. et al. 2017 (44) affirm that diastolic blood pressure was significantly higher in men, as well as Vitale M. et al. 2016 (39) reported that diastolic blood pressure was slightly lower in women than in men. Sahin et a., 2020 (49) reported that the male sex is a determinant of good foot care behaviour; on the contrary, Rossi M. C. et al., 2017 (45) reported that women showed higher adherence than men to self-care activities dedicated to foot care. Lastly, Rossi M. C. et al., 2017 (45) found that women were less frequently smokers than men and Kacerovsky-Bielesz G. 2009 (22) found that more women than men reported no or very rare alcohol consumption.
Self-care Monitoring: glycaemic control and blood glucose testing
Eleven studies reported results on self-care monitoring activities. Overall, despite substantial evidence showing that females practiced greater adequate blood glucose monitoring than males, these latter seem to have a higher level of glycemic control in terms of lower HbA1c.
Caruso R. et al. 2020 (17) found that self-care monitoring was lower among males when compared with females, while Lipscombe C. et al. 2016 (50) stated that more females than males never checked their blood glucose levels, but Cuevas H. E. et al. 2015 (51) specifies that more females than males checked blood glucose levels more than one time per week. Instead, Rossi M. C. et al. 2017 (45) and Chiu C. 2011 (41) reported that women showed higher adherence than men to self-care activities dedicated to self-monitoring of blood glucose even if they have significantly higher levels of HbA1c than men. Alghafri T. S. 2018 (47) too, reported that compared to males, there were significantly more females with uncontrolled diabetes, in accordance with Boonsatean W. et al. 2018 (34), Aghili R. 2017 (44), Shrestha A. D. et al. 2013 (36), and Hawthorne K. et al. 1999 (52) that reported that women had poorer glycemic control than men. On the contrary, Vitale M. et al. 2016 (39) reported that glucose control, evaluated as HbA1c, was marginally better in women, while Kacerovsky-Bielesz G. et al. 2009 (22) found that in women, HbA1c tended to be higher, but did not significantly differ compared with men.
Self-care Management
Only five studies reported results on self-care management. Studies on this topic are described in detail below.
Boonsatean W. et al. 2018 (34) and Chiu C. et al. 2011 (41) found a higher incidence of diabetic complications among women, despite a demonstrated higher mean score for glucose management and healthcare use than men. On the contrary, Rossi M. C. et al. 2017 (45) found that women had a lower prevalence of known diabetes complications than men. Meanwhile, Hawthorne K. et al. 1999 (52) reported that knowledge of diabetic complications was generally low, lower in women than in men. Finally, Caruso et al. 2020 (24) reported that males, having been diagnosed with diabetic neuropathy, were associated with inadequate self-care management; on the contrary, females, having been diagnosed with T2DM from <10 years and having diabetes retinopathy showed a lower risk of inadequate self-care management.
Self-care’s determinants: psychosocial factors associated with self-care activities
Nineteen studies investigated self-care behaviors’ determinants. Overall, a substantial amount of evidence reported more diabetes-related psychological difficulties and a lower perception of social support in females than in males. Furthermore, these studies highlighted the fundamental role of self-efficacy as a self-care determinant and mediator, but its level was found to be significantly lower in females than in males.
Aghili R. et al. 2017 (44) report that women under the age of 55 reported a higher level of distress, depression, anxiety and worse quality of life compared to men in the same age group, in accordance with Caruso et al. 2017 (30) that report that men perception of wellbeing is higher than in women, while the level of anxiety and depression are higher in women. Badawi G. et al. 2012 (46) reported that men were more likely to rate their health as excellent, while women were more likely to rate their health as good, fair or poor. Also, Naicker K. et al. 2017 (40) reported that more women than men had either depressive or anxious symptoms but was found strong associations between depression/anxiety and glycemic control in men only, while Yin J. et al. 2016 (31) found an association between poor glycemic control and depressive symptoms both in men and women but was more common in women than in men. Instead, Nau D. P. et al. 2007 (53) found a significant association between depression severity and worse medication adherence in men, while women were relatively adherent regardless of depressive symptom severity. However, Lipscombe C. et al. 2014 (54) reported that women were more likely than men to report having mild and moderate-severe anxiety symptoms; moreover, mild anxiety symptoms were associated with an increased odds of inactivity in women only, whereas moderate to severe anxiety symptoms were associated with an increase in the odds of inactivity for men only. The same authors found a similar association in 2016 with diabetes distress (50). On the same aspect, Rossi M. C. et al. 2017 (45) reported statistically significant poorer scores for psychological wellbeing, empowerment, diabetes-related distress, satisfaction with treatment, barriers to medication taking, satisfaction with access to chronic care and healthcare communication, and perceived social support in women than men. Shrestha A. D. et al. 2013 (36) found that women tend to present more depressive somatic symptoms associated with diabetes while men were more likely to present fatigue, muscle aches and sexual dysfunction. According to Chiu C. et al. 2011 (41), women had lower scores than men on diabetes coping status, perceived control, self-efficacy, and perceived family support but higher scores on depressive symptoms than men. Also, Kacerovsky-Bielesz G et al. .2009 (22) found that women tended to express a lower degree of satisfaction with social support. On the contrary, Misra R. et al. 2009 (37) reported that females reported higher social support compared to their male peers.
Caruso R et al. 2017 (30) found that men have a higher perception of self-efficacy than women. Moreover, Cherrington A. et al. 2010 (55) reported that there is strong evidence that diabetes self-efficacy mediates the effect of depressive symptoms on glycemic control for males. In the same area, Boonsatean W. et al. 2018 (34) found that men felt more confident in the treatment given by the health professionals and showed higher confidence in the treatment effectiveness than women. Deepening, Mansyur C. L. et al. 2016 (56) reported that men who were more discouraged from following a healthful diet but who ate the same foods tended to have lower Self-efficacy, while women who received more support and who ate the same foods as their families tended to have higher Self-efficacy. The same author (33) found that women had significantly lower self-efficacy (SE) and tended to perceive that they received lower levels of support. Shrestha A. D. et al. 2013 (36) reported that men who had higher self-efficacy had better dietary practice, while women with lower self-efficacy could not follow a good diet.
Caruso R. et al. 2020 (24) reported that in females, a higher level of persistence in self-care self-efficacy as a determinant of adequate self-care maintenance, while in both males and females, persistence higher level of self-care self-efficacy was associated with a decrease in the risk of inadequate self-care management. Moreover, among males, being an active worker was associated with inadequate self-care maintenance, while low income was associated with inadequate self-care maintenance only in females. On the same line, Choi J. S. et al. 2015 (32) stated that the number of diabetes-related complications, diabetes self-efficacy, and depression were significant predictors of self-care behaviors in older men; while in older women, the predictors were diabetes self-efficacy, depression, duration of diabetes, and barriers to diabetes self-care.
Discussion
Our literature review provided an overall perspective on the evidence related to sex-related differences in self-care behaviors of patients with T2DM. We discovered 29 primary studies emerging by databases search, showing a growing interest in this topic by researchers; accordingly, the literature is extensive, but results are often fragmented and contradictory, undermining the effective possibility for nurses and clinicians to establish interventions to support the lacking areas of diversity between males and females with T2DM in the implementation of their self-care behaviors. So, we wanted to summarize and interpret evidence about sex-related differences in self-care among this population. For this aim, our study can be considered innovative and very useful in clinical practice, as it will allow combining each individual research effort into a global vision.
As already highlighted, self-care has a crucial role in determining a positive clinical trajectory among patients with chronic diseases (57). Sex-related differences are an important feature of the real world, as men and females perform many aspects of biology, physiopathology, and clinical issues in a specific way. It is possible to recognise males’ and females’ peculiarities in self-care behaviors. Indeed, it was found that males and females with T2DM performed self-care differently; more males reported performing better behaviors aimed at maintaining health and clinical stability (i.e., self-care maintenance) than females, but mainly concerning physical activity. On the other hand, more females reported performing adequate behaviors aimed at monitoring their signs and symptoms (i.e., self-care monitoring) but with worse glycemic control and diabetic complications (i.e., self-care management). These results are relevant because they clarify what is known about this aspect, which is fundamental for designing future research and implementing evidence-based personalized educational interventions for both sexes.
Self-care maintenance refers to those behaviors performed to improve wellbeing, preserve health, or maintain physical and emotional stability (5,58), and it represents the first step to staying healthy. Specifically, most of the included studies explored self-care maintenance behaviors, focusing on physical activity, diet, weight control behaviors, and treatment adherence of patients with T2DM. Many available studies argued that males practiced greater physical activity than females, thus highlighting the need to develop women tailored educational interventions to support physical activity. Even if regular physical activity provides an important benefit to the health of women, in general, women are often more sedentary than men (59), and participation in physical activity decreases as women age (60), increasing the risk for cardiovascular disease, diabetes, hypertension, colon cancer, and depression (61). For women with T2DM, physical activity is more important because empirical evidence shows that increasing physical activity, along with dietary changes, can dramatically decrease the risk of developing type 2 diabetes (62). However, the current evidence of sex-related differences in diet, weight, foot care, smoke and alcohol need to be improved to settle doubts coming from contradictory results.
Meanwhile, females reported more adequate self-monitoring behaviors (i.e., blood glycemic control) than males, but our results show also that females with T2DM generally report more inadequate glycemic control (i.e. higher level of HbA1c) than males. This result is comparable to what is reported by adults with T1DM (9). These findings may suggest that other inadequate behaviors, such as self-care maintenance behaviors, often reported by females with diabetes, could negatively influence glycemic control so much that the positive influence of reported adequate levels of self-care monitoring seems exceeded. However, this hypothesis needs to be empirically tested. Future empirical studies would be useful to understand the previous research that showed worse glycemic control among females who performed better blood glucose monitoring than males and vice-versa. These results are contrary to those of studies showing that adequate self-monitoring of blood glucose leads to better glycemic control (lower HbA1c) in patients with diabetes (63,64). This other contradiction can also be explained by the findings of other studies showing the leading role of self-efficacy in determining adequate behaviors e better outcomes (65,66) and that man reports a higher perception of self-efficacy than women (30,33). Therefore, considering these results, the influence of sex in modulating the association between self-monitoring and glycaemic control should be further investigated with empirical research designed to control selection bias for sex and psychosocial variables. Furthermore, these findings suggest that more specific educational interventions should be included in the clinical practice for both sexes.
Considering self-care management (i.e., the ability to respond to signs and symptoms when they occur), only five studies reported results on this topic. Two main components could be referred to as self-care management: autonomous and consultative behaviours, that patients need to perform as the result of their decision-making on specific observed signs and/or symptoms (4). In line with previous research in T2DM and T1DM populations (29), this review shows that patients with T2DM generally have difficulties in performing adequate self-care management, especially females that seem to report worse glycemic control e diabetic complications than males. However, this aspect is clearly under-investigated and showed conflictual results, with few studies aimed at investigating sex-related differences in self-care management.
Self-efficacy is one of the most important factors (i.e. self-care determinants) that affect the successfulness of self-care behaviors in patients with T2DM (67), explaining the 11.4% of variance regarding diabetes self-care and 31.3% variance of diabetes self-care behavioral intention (68). Additionally, the self-efficacy of patients with T2DM is strongly associated with the perceived quality of life (69), eating habits (70) and predicted the patients’ glycemic control (71). Therefore, it is emerging the strategic role of self-efficacy in determining self-care behaviors of patients with T2DM, and for this reason, clarifying the peculiarities of males and females is essential. In the general population, males have significantly higher self-efficacy strength than their female peers (72), and our results confirmed this result for women with T2DM. In this regard, it is possible hypnotizing different factors causing these differences. Firstly, the role division and social resources disadvantage for women, gendered family division, and social division of labor. This disadvantage will accumulate the old age, with the increase in chronic illness. Secondly, it has been described that often males overestimate their abilities and performance, with a relatively high level of confidence in facing challenges. Thirdly, the influence of social desirability, with the traditional thinking of “men are more able” is still deeply rooted (72). Accordingly, all these factors need to be deeply studied in patients with T2DM.
So, the under-investigated areas require empirical investigation to better understand sex-specific patterns of self-care behaviors and self-care determinants. Specifically, researchers need to deeply understand the relationships between each component of self-care and males’ and females’ specific outcomes. Also, this kind of knowledge could be important to improve clinical practice because the awareness of sex-specific patterns in self-care behaviors might create tailored interventions for providing self-care to both sexes.
Conclusions
Understanding sex-related differences in adults with T2DM is important for addressing future research and clinical practice because males and females with T2DM have reported performing self-care differently. Our results showed conflictual results: more males reported performing better behaviors aimed at maintaining health and clinical stability (i.e., self-care maintenance) than females, but mainly in relation to physical activity; On the other hand, more females reported performing adequate behaviors aimed at monitoring their signs and symptoms (i.e., self-care monitoring), but with worse glycemic control and diabetic complications (i.e., self-care management). However, more empirical research is recommended to obtain optimal knowledge for addressing clinical practice.
Considering that the available evidence on this topic is still fragmented, this literature review had some limitations. First, it was not possible to perform a meta-analysis because of the degree of methodological and clinical heterogeneity among the included studies. Second, although a large number of included articles to summarize the evidence related to sex-related differences in patients’ self-care behaviors with T2DM, the search terms and databases we used might not have found all relevant studies because of the numerous behaviors that are referred to as self-care. Third, we have to acknowledge that the majority of the included studies do not have performed statistical analysis stratified by sex, which could have led to biased results.
We suggest that healthcare providers involved in the care management of adults with T2DM give particular attention to supporting females with T2DM to enhance their behaviors aimed at maintaining adequate health and glycemic control, such as regular physical activity, and improved management of the diabetes-related psychological issue and weight-control behaviors. Considering the care management of males with T2DM, we recommend that clinicians pay particular attention to sustaining patients to monitor changes in their signs and symptoms, such as better blood glucose monitoring and dietary intake. We recommend educational interventions for both sexes to enhance patients’ ability in self-care management, such as responding to signs and symptoms when they occur.
Conflict of Interest:
Each author declares that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangement) that might pose a conflict of interest in connection with the submitted article
References
- WHO. Diabetes. World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes . [Google Scholar]
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019 Nov;157:107843. doi: 10.1016/j.diabres.2019.107843. [DOI] [PubMed] [Google Scholar]
- American Association of Diabetes Educators. An Effective Model of Diabetes Care and Education: Revising the AADE7 Self-Care Behaviors¯. Diabetes Educ. 2020 Apr;46(2):139–60. doi: 10.1177/0145721719894903. [DOI] [PubMed] [Google Scholar]
- Riegel B, Jaarsma T, Strömberg A. A middle-range theory of self-care of chronic illness. ANS Adv Nurs Sci. 2012 Sep;35(3):194–204. doi: 10.1097/ANS.0b013e318261b1ba. [DOI] [PubMed] [Google Scholar]
- Riegel B, Dickson VV. A situation-specific theory of heart failure self-care. J Cardiovasc Nurs. 2008 Jun;23(3):190–6. doi: 10.1097/01.JCN.0000305091.35259.85. [DOI] [PubMed] [Google Scholar]
- Riegel B, Dickson VV, Faulkner KM. The Situation-Specific Theory of Heart Failure Self-Care: Revised and Updated. J Cardiovasc Nurs. 2016 Jun;31(3):226–35. doi: 10.1097/JCN.0000000000000244. [DOI] [PubMed] [Google Scholar]
- Ausili D, Rossi E, Rebora P, et al. Socio-demographic and clinical determinants of self-care in adults with type 2 diabetes: a multicentre observational study. Acta Diabetol. 2018 Jul;55(7):691–702. doi: 10.1007/s00592-018-1135-x. [DOI] [PubMed] [Google Scholar]
- Yu DS-F, De Maria M, Barbaranelli C, et al. Cross-cultural applicability of the Self-Care Self-Efficacy Scale in a multi-national study. J Adv Nurs. 2021 Feb;77(2):681–92. doi: 10.1111/jan.14617. [DOI] [PubMed] [Google Scholar]
- Baroni I, Arrigoni C, Caruso R, Magon A, Villa G, Manara DF, et al. Self-care and type 1 diabetes mellitus: systematic review of sex-related differences. Panminerva Med. 2021 Jan 25 doi: 10.23736/S0031-0808.21.04134-3. [DOI] [PubMed] [Google Scholar]
- Dellafiore F, Arrigoni C, Pittella F, Conte G, Magon A, Caruso R. Paradox of self-care gender differences among Italian patients with chronic heart failure: findings from a real-world cross-sectional study. BMJ Open. 2018 Sep 28;8(9):e021966. doi: 10.1136/bmjopen-2018-021966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riegel B, Jaarsma T. Recognizing the Complexity of Self-Care. Int J Nurs Stud. 2021 Apr;116:103908. doi: 10.1016/j.ijnurstu.2021.103908. [DOI] [PubMed] [Google Scholar]
- Riegel B, Dunbar SB, Fitzsimons D, et al. Self-care research: Where are we now? Where are we going? Int J Nurs Stud. 2021 Apr;116:103402. doi: 10.1016/j.ijnurstu.2019.103402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamis-Holland JE, Lu J, Korytkowski M, et al. Sex differences in presentation and outcome among patients with type 2 diabetes and coronary artery disease treated with contemporary medical therapy with or without prompt revascularization: a report from the BARI 2D Trial (Bypass Angioplasty Revascularization Investigation 2 Diabetes) J Am Coll Cardiol. 2013 Apr 30;61(17):1767–76. doi: 10.1016/j.jacc.2013.01.062. [DOI] [PubMed] [Google Scholar]
- Hendriks SH, van Hateren KJJ, Groenier KH, et al. Sex Differences in the Quality of Diabetes Care in the Netherlands (ZODIAC-45) PloS One. 2015;10(12):e0145907. doi: 10.1371/journal.pone.0145907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee CS, Riegel B, Driscoll A, et al. Gender differences in heart failure self-care: a multinational cross-sectional study. Int J Nurs Stud. 2009 Nov;46(11):1485–95. doi: 10.1016/j.ijnurstu.2009.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brera AS, Arrigoni C, Dellafiore F, et al. Burnout syndrome and its determinants among healthcare workers during the first wave of the Covid-19 outbreak in Italy: a cross-sectional study to identify sex-related differences. Med Lav. 2021 Aug 26;112(4):306–19. doi: 10.23749/mdl.v112i4.11316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caruso R, Rebora P, Luciani M, Di Mauro S, Ausili D. Sex-related differences in self-care behaviors of adults with type 2 diabetes mellitus. Endocrine. 2020 Feb;67(2):354–62. doi: 10.1007/s12020-020-02189-5. [DOI] [PubMed] [Google Scholar]
- Kautzky-Willer A, Harreiter J, Pacini G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr Rev. 2016 Jun;37(3):278–316. doi: 10.1210/er.2015-1137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gale EA, Gillespie KM. Diabetes and gender. Diabetologia. 2001 Jan;44(1):3–15. doi: 10.1007/s001250051573. [DOI] [PubMed] [Google Scholar]
- Lyons MR, Peterson LR, McGill JB, et al. Impact of sex on the heart’s metabolic and functional responses to diabetic therapies. Am J Physiol Heart Circ Physiol. 2013 Dec 1;305(11):H1584–1591. doi: 10.1152/ajpheart.00420.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schunk M, Reitmeir P, Schipf S, et al. Health-related quality of life in women and men with type 2 diabetes: a comparison across treatment groups. J Diabetes Complications. 2015 Mar;29(2):203–11. doi: 10.1016/j.jdiacomp.2014.11.010. [DOI] [PubMed] [Google Scholar]
- Kacerovsky-Bielesz G, Lienhardt S, Hagenhofer M, et al. Sex-related psychological effects on metabolic control in type 2 diabetes mellitus. Diabetologia. 2009 May;52(5):781–8. doi: 10.1007/s00125-009-1318-7. [DOI] [PubMed] [Google Scholar]
- Caruso R, Rebora P, Dellafiore F, et al. Clinical and socio-demographic determinants of inadequate self-care in adults with type 1 diabetes mellitus: the leading role of self-care confidence. Acta Diabetol. 2019 Feb;56(2):151–61. doi: 10.1007/s00592-018-1259-z. [DOI] [PubMed] [Google Scholar]
- Caruso R, Rebora P, Luciani M, Di Mauro S, Ausili D. Sex-related differences in self-care behaviors of adults with type 2 diabetes mellitus. Endocrine. 2020 Feb;67(2):354–62. doi: 10.1007/s12020-020-02189-5. [DOI] [PubMed] [Google Scholar]
- Popay J, Roberts H, Sowden A, et al. Guidance on the conduct of narrative synthesis in systematic reviews: A product from the ESRC Methods Programme. 2006 [Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71) doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kacem A, Mayr P. Analysis of Footnote Chasing and Citation Searching in an Academic Search Engine. ArXiv170702494 Cs [Internet] 2017 Sep 23 [Google Scholar]
- Moola S, Munn Z, Tufanaru C, et al. Chapter 7: Systematic reviews of etiology and risk. JBI Man Evid Synth [Internet] 2020 [Google Scholar]
- Ausili D, Barbaranelli C, Rossi E, et al. Development and psychometric testing of a theory-based tool to measure self-care in diabetes patients: the Self-Care of Diabetes Inventory. BMC Endocr Disord. 2017 Oct 16;17(1):66. doi: 10.1186/s12902-017-0218-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caruso R, Arrigoni C, Magon A, et al. Health Determinants in Italian Type 2 diabetes mellitus (T2DM) patients: a critical gender differences analysis. J Res Gend Stud. 2017;7(2):93. [Google Scholar]
- Yin J, Yeung R, Luk A, et al. Gender, diabetes education, and psychosocial factors are associated with persistent poor glycemic control in patients with type 2 diabetes in the Joint Asia Diabetes Evaluation (JADE) J Diabetes. 2016 Jan;8(1):109–19. doi: 10.1111/1753-0407.12262. [DOI] [PubMed] [Google Scholar]
- Choi JS, Kim BH, Chang SJ. Gender-Specific Factors Influencing Diabetes Self-Care Behaviors and Health-Related Quality of Life Among Older Adults With Type 2 Diabetes in South Korea. Res Gerontol Nurs. 2015 Aug;8(5):231–9. doi: 10.3928/19404921-20150331-01. [DOI] [PubMed] [Google Scholar]
- Mansyur CL, Rustveld LO, Nash SG, Jibaja-Weiss ML. Social factors and barriers to self-care adherence in Hispanic men and women with diabetes. Patient Educ Couns. 2015 Jun;98(6):805–10. doi: 10.1016/j.pec.2015.03.001. [DOI] [PubMed] [Google Scholar]
- Boonsatean W, Carlsson A, Dychawy Rosner I, Östman M. Sex-related illness perception and self-management of a Thai type 2 diabetes population: a cross-sectional descriptive design. BMC Endocr Disord. 2018 Dec;18(1):5. doi: 10.1186/s12902-017-0229-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaccaro JA, Huffman FG. Gender Differences in Medical Advice and Health Behavior of Obese African Americans With and Without Type 2 Diabetes. Am J Mens Health. 2012 Sep;6(5):383–94. doi: 10.1177/1557988312449853. [DOI] [PubMed] [Google Scholar]
- Shrestha AD, Kosalram K, Gopichandran V. Gender difference in care of type 2 diabetes. JNMA J Nepal Med Assoc. 2013 Mar;52(189):245–50. [PubMed] [Google Scholar]
- Misra R, Lager J. Ethnic and gender differences in psychosocial factors, glycemic control, and quality of life among adult type 2 diabetic patients. J Diabetes Complications. 2009 Jan;23(1):54–64. doi: 10.1016/j.jdiacomp.2007.11.003. [DOI] [PubMed] [Google Scholar]
- Avedzi HM, Mathe N, Storey K, Johnson JA, Johnson ST. Examining sex differences in glycemic index knowledge and intake among individuals with type 2 diabetes. Prim Care Diabetes. 2018 Feb;12(1):71–9. doi: 10.1016/j.pcd.2017.07.005. [DOI] [PubMed] [Google Scholar]
- Vitale M, Masulli M, Cocozza S, et al. Sex differences in food choices, adherence to dietary recommendations and plasma lipid profile in type 2 diabetes – The TOSCA.IT study. Nutr Metab Cardiovasc Dis. 2016 Oct;26(10):879–85. doi: 10.1016/j.numecd.2016.04.006. [DOI] [PubMed] [Google Scholar]
- Naicker K, Øverland S, Johnson JA, et al. Symptoms of anxiety and depression in type 2 diabetes: Associations with clinical diabetes measures and self-management outcomes in the Norwegian HUNT study. Psychoneuroendocrinology. 2017 Oct;84:116–23. doi: 10.1016/j.psyneuen.2017.07.002. [DOI] [PubMed] [Google Scholar]
- Chiu C-J, Wray LA. Gender Differences in Functional Limitations in Adults Living with Type 2 Diabetes: Biobehavioral and Psychosocial Mediators. Ann Behav Med. 2011 Feb;41(1):71–82. doi: 10.1007/s12160-010-9226-0. [DOI] [PubMed] [Google Scholar]
- Taru C, Tsutou A, Nakawatase Y, Usami M, Miyawaki I. Gender Differences of Dietary Self-Management Behavior Affecting Control Indices in Type II Diabetes. :15. [PubMed] [Google Scholar]
- Tokunaga-Nakawatase Y, Taru C, Tsutou A, Nishigaki M, Miyawaki I. Self-management behavior concerning physical activity of Japanese type 2 diabetes patients, characterized by sex, daily energy intake and body mass index. Diabetol Int. 2019 Jul;10(3):206–12. doi: 10.1007/s13340-018-0381-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aghili R, Ridderstråle M, Kia M, et al. The challenge of living with diabetes in women and younger adults: A structural equation model. Prim Care Diabetes. 2017 Oct;11(5):467–73. doi: 10.1016/j.pcd.2017.05.001. [DOI] [PubMed] [Google Scholar]
- Rossi MC, Lucisano G, Pintaudi B, et al. The complex interplay between clinical and person-centered diabetes outcomes in the two genders. Health Qual Life Outcomes. 2017 Jan;15(1):41. doi: 10.1186/s12955-017-0613-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Badawi G, Gariépy G, Pagé V, Schmitz N. Indicators of self-rated health in the Canadian population with diabetes: Self-rated health, depression and disability in people with diabetes. Diabet Med. 2012 Aug;29(8):1021–8. doi: 10.1111/j.1464-5491.2012.03571.x. [DOI] [PubMed] [Google Scholar]
- Alghafri TS, Alharthi SM, Al-farsi Y, Bannerman E, Craigie AM, Anderson AS. Correlates of physical activity and sitting time in adults with type 2 diabetes attending primary health care in Oman. BMC Public Health. 2018 Dec;18(1):85. doi: 10.1186/s12889-017-4643-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown SA, Harrist RB, Villagomez ET, Segura M, Barton SA, Hanis CL. Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes. Diabetes Educ. 2000 Jun;26(3):425–38. doi: 10.1177/014572170002600310. [DOI] [PubMed] [Google Scholar]
- Şahin S, Cingil D. Evaluation of the relationship among foot wound risk, foot self-care behaviors, and illness acceptance in patients with type 2 diabetes mellitus. Prim Care Diabetes. 2020 Oct;14(5):469–75. doi: 10.1016/j.pcd.2020.02.005. [DOI] [PubMed] [Google Scholar]
- Lipscombe C, Smith KJ, Gariepy G, Schmitz N. Gender differences in the association between lifestyle behaviors and diabetes distress in a community sample of adults with type 2 diabetes. J Diabetes. 2016 Mar;8(2):269–78. doi: 10.1111/1753-0407.12298. [DOI] [PubMed] [Google Scholar]
- Cuevas HE, Brown SA, García AA, Winter M, Brown A, Hanis CL. Blood Glucose Self-Monitoring Patterns in Mexican Americans: Further Lessons from the Starr County Border Health Initiative. Diabetes Technol Ther. 2015 Feb;17(2):105–11. doi: 10.1089/dia.2014.0147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawthorne K, Tomlinson S. Pakistani moslems with Type 2 diabetes mellitus: effect of sex, literacy skills, known diabetic complications and place of care on diabetic knowledge, reported self-monitoring management and glycaemic control. Diabet Med J Br Diabet Assoc. 1999 Jul;16(7):591–7. doi: 10.1046/j.1464-5491.1999.00102.x. [DOI] [PubMed] [Google Scholar]
- Nau DP, Aikens JE, Pacholski AM. Effects of gender and depression on oral medication adherence in persons with type 2 diabetes mellitus. Gend Med. 2007 Sep;4(3):205–13. doi: 10.1016/s1550-8579(07)80041-6. [DOI] [PubMed] [Google Scholar]
- Lipscombe C, Smith KJ, Gariépy G, Schmitz N. Gender Differences in the Relationship between Anxiety Symptoms and Physical Inactivity in a Community-Based Sample of Adults with Type 2 Diabetes. Can J Diabetes. 2014 Dec;38(6):444–50. doi: 10.1016/j.jcjd.2013.12.002. [DOI] [PubMed] [Google Scholar]
- Cherrington A, Wallston KA, Rothman RL. Exploring the relationship between diabetes self-efficacy, depressive symptoms, and glycemic control among men and women with type 2 diabetes. J Behav Med. 2010 Feb;33(1):81–9. doi: 10.1007/s10865-009-9233-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mansyur CL, Rustveld LO, Nash SG, Jibaja-Weiss ML. Hispanic Acculturation and Gender Differences in Support and Self-Efficacy for Managing Diabetes. Diabetes Educ. 2016 Jun;42(3):315–24. doi: 10.1177/0145721716640905. [DOI] [PubMed] [Google Scholar]
- Riegel B, Barbaranelli C, Sethares KA, et al. Development and initial testing of the self-care of chronic illness inventory. J Adv Nurs. 2018 Oct;74(10):2465–76. doi: 10.1111/jan.13775. [DOI] [PubMed] [Google Scholar]
- Riegel B, Lee CS, Dickson VV, Carlson B. An update on the self-care of heart failure index. J Cardiovasc Nurs. 2009 Dec;24(6):485–97. doi: 10.1097/JCN.0b013e3181b4baa0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) Surgeon General’s report on physical activity and health. From the Centers for Disease Control and Prevention. JAMA. 1996 Aug 21;276(7):522. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) Prevalence of sedentary lifestyle--Behavioral Risk Factor Surveillance System, United States, 1991. MMWR Morb Mortal Wkly Rep. 1993 Jul 30;42(29):576–9. [PubMed] [Google Scholar]
- Segar M, Jayaratne T, Hanlon J, Richardson CR. Fitting fitness into women’s lives: effects of a gender-tailored physical activity intervention. Womens Health Issues Off Publ Jacobs Inst Womens Health. 2002 Dec;12(6):338–47. doi: 10.1016/s1049-3867(02)00156-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuomilehto J, Lindström J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001 May 3;344(18):1343–50. doi: 10.1056/NEJM200105033441801. [DOI] [PubMed] [Google Scholar]
- Machry RV, Rados DV, Gregório GR de, Rodrigues TC. Self-monitoring blood glucose improves glycemic control in type 2 diabetes without intensive treatment: A systematic review and meta-analysis. Diabetes Res Clin Pract. 2018 Aug;142:173–87. doi: 10.1016/j.diabres.2018.05.037. [DOI] [PubMed] [Google Scholar]
- Dunn TC, Xu Y, Hayter G, Ajjan RA. Real-world flash glucose monitoring patterns and associations between self-monitoring frequency and glycaemic measures: A European analysis of over 60 million glucose tests. Diabetes Res Clin Pract. 2018 Mar;137:37–46. doi: 10.1016/j.diabres.2017.12.015. [DOI] [PubMed] [Google Scholar]
- Chan CKY, Cockshaw W, Smith K, Holmes-Truscott E, Pouwer F, Speight J. Social support and self-care outcomes in adults with diabetes: The mediating effects of self-efficacy and diabetes distress. Results of the second diabetes MILES - Australia (MILES-2) study. Diabetes Res Clin Pract. 2020 Aug;166:108314. doi: 10.1016/j.diabres.2020.108314. [DOI] [PubMed] [Google Scholar]
- Caruso R, Rebora P, Dellafiore F, et al. Clinical and socio-demographic determinants of inadequate self-care in adults with type 1 diabetes mellitus: the leading role of self-care confidence. Acta Diabetol. 2019 Feb;56(2):151–61. doi: 10.1007/s00592-018-1259-z. [DOI] [PubMed] [Google Scholar]
- Dehghan H, Charkazi A, Kouchaki GM, et al. General self-efficacy and diabetes management self-efficacy of diabetic patients referred to diabetes clinic of Aq Qala, North of Iran. J Diabetes Metab Disord. 2017;16:8. doi: 10.1186/s40200-016-0285-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Didarloo AR, Shojaeizadeh D, Gharaaghaji Asl R, Habibzadeh H, Niknami S, Pourali R. Prediction of Self-Management Behavior among Iranian Women with Type 2 Diabetes: Application of the Theory of Reasoned Action along with Self-Efficacy (ETRA) Iran Red Crescent Med J. 2012 Feb;14(2):86–95. [PMC free article] [PubMed] [Google Scholar]
- Jahanlou AS, Alishan Karami N. The effect of literacy level on health related-quality of life, self-efficacy and self-management behaviors in diabetic patients. Acta Med Iran. 2011;49(3):153–8. [PubMed] [Google Scholar]
- O’Hea EL, Moon S, Grothe KB, et al. The interaction of locus of control, self-efficacy, and outcome expectancy in relation to HbA1c in medically underserved individuals with type 2 diabetes. J Behav Med. 2009 Feb;32(1):106–17. doi: 10.1007/s10865-008-9188-x. [DOI] [PubMed] [Google Scholar]
- Cosansu G, Erdogan S. Influence of Psychosocial Factors on Self-Care Behaviors and Glycemic Control in Turkish Patients With Type 2 Diabetes Mellitus. J Transcult Nurs. 2014 Jan;25(1):51–9. doi: 10.1177/1043659613504112. [DOI] [PubMed] [Google Scholar]
- Wang Y, Xu L, Qin W, et al. Gender Difference in General Self-Efficacy among Young-Old Elderly Aged 60-74 in Rural Shandong China: A Cross-Sectional Survey. Int J Environ Res Public Health. 2019 Dec 12;16(24):E5070. doi: 10.3390/ijerph16245070. [DOI] [PMC free article] [PubMed] [Google Scholar]