

Abstract
Background
The COVID-19 pandemic led to extensive restrictions in Germany in 2020, including the postponement of elective interventions. We examined the impact on ST-elevation myocardial infarction (STEMI) as an acute and non-postponable disease.
Methods
Using German national records, all STEMI between 2017 and 2020 were identified. Using the number of STEMI cases between 2017 and 2019, we created a forecast for 2020 and compared it with the observed number of STEMI in 2020.
Results
From 2017 to 2020, 248,062 patients were treated for STEMI in Germany. Mean age was 65.21 years and 28.36% were female. When comparing forecasted and observed STEMI in 2020, a correlation can be seen: noticeable fewer STEMI were treated in those weeks respectively months with an increasing COVID-19 hospitalization rate (monthly percentage decrease in STEMI: March − 14.85%, April − 13.39%, November − 11.92%, December − 22.95%). At the same time, the crude in-hospital mortality after STEMI increased significantly at the peaks of the first and second waves (relative risk/RR of monthly in-hospital mortality: April RR = 1.11 [95% CI 1.02; 1.21], November RR = 1.13 [1.04; 1.24], December RR = 1.16 [1.06; 1.27]).
Conclusion
The COVID-19 pandemic led to a noticeable decrease in the number of STEMI interventions in Germany at the peaks of the first and second waves in 2020, corresponding to an increase in COVID-19 hospitalizations. At the same time, in-hospital mortality after STEMI increased significantly in these phases.
Graphical abstract
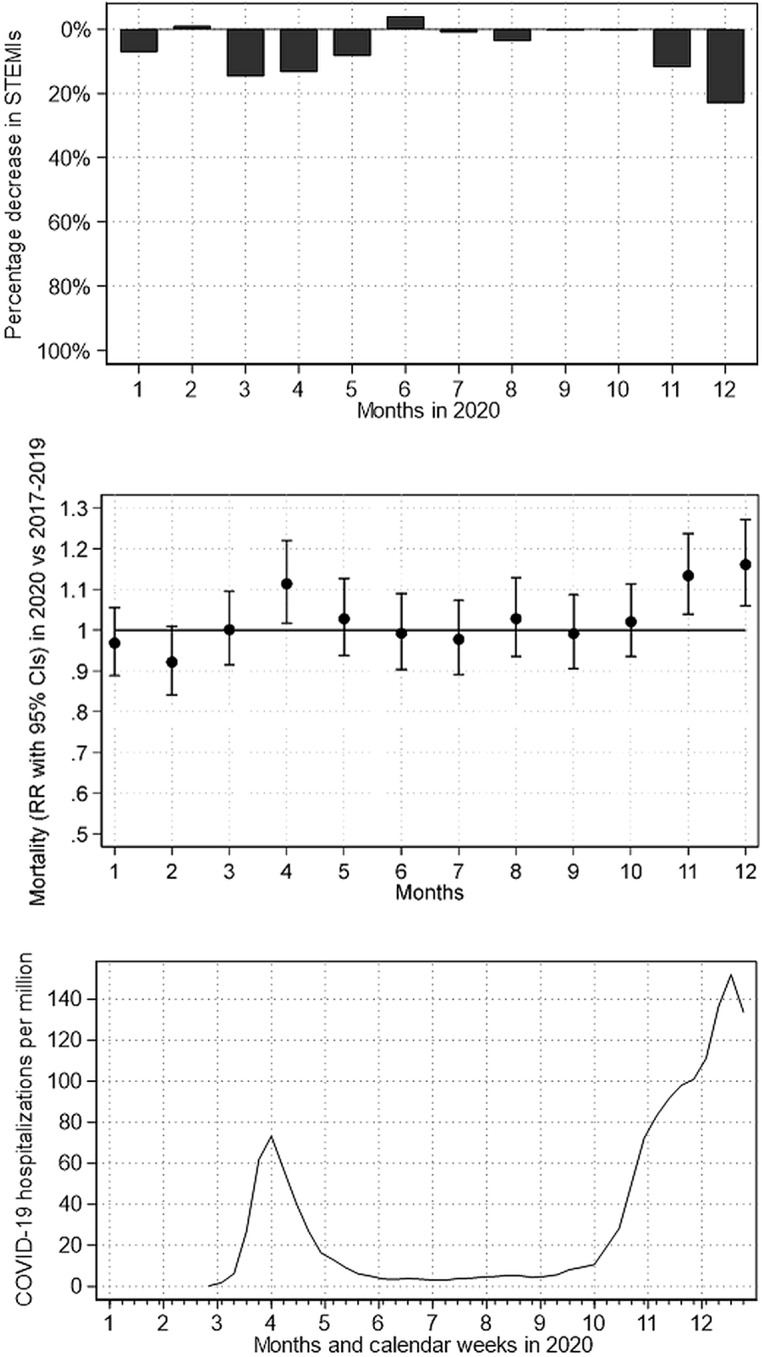
Impact of the COVID-19 pandemic on STEMI numbers and in-hospital mortality in Germany. Relative difference between forecasted and observed STEMI numbers (above figure), the relative risk of in-hospital mortality (middle figure) as well as number of new hospital admissions for COVID-19 per million inhabitants according to Roser et al.27 (bottom figure).
Supplementary Information
The online version contains supplementary material available at 10.1007/s00392-022-02102-2.
Keywords: COVID-19 pandemic, STEMI, Myocardial infarction, In-hospital mortality, National electronic health records
Introduction
In Germany, the first lockdown restrictions due to the upcoming COVID-19 pandemic were announced on March 16, 2020. This also had a strong impact on the German healthcare system. In order to maintain hospital resources for COVID-19 patients, the postponement of elective patients was recommended [1]. However, although emergencies continued to be treated, it is discussed in the international literature that even patients with actually life-threatening diseases might have refrained from hospitalization for fear of a potential SARS-CoV-2 infection. This is also applied in particular to cardiovascular diseases such as acute coronary syndrome or myocardial infarction [2–4].
Concerning ST-elevation myocardial infarction (STEMI), several studies in Germany [5–7] as well as internationally [2, 8, 9] have already confirmed the influence of the COVID-19 pandemic in the form of declining numbers of STEMI interventions, but their results regarding in-hospital mortality after STEMI since the beginning of the COVID-19 pandemic are still unclear. In addition, nationwide analyzes are still lacking.
Therefore, this study examines the impact of the COVID-19 pandemic on the number of catheterizations due to STEMI, using nationwide healthcare data. We compare forecasted and observed numbers of STEMI in 2020 as well as in-hospital mortality throughout the first and second waves of the COVID-19 pandemic. Finally, recommendations are to be made for future handling of the pandemic with regard to emergency interventions such as STEMI.
Material and methods
The German Federal Statistical Office has been providing data on all hospital stays in Germany via its Research Data Center since 2005. The basis of these data is inpatient hospital billing under the German Diagnosis Related Groups (DRG) system, which is based on fixed charge groups—formed on the basis of diagnoses (coded according to ICD-10) and measures performed (coded according to the German Operation and Procedure Classification/OPS). Upon prespecified request, the Research Data Center may provide analysis of their data in the form of fully anonymous, aggregated results that are released by the Research Data Center. If necessary, partial results are censored. Our study did not involve direct access by the investigators to data on individual patients but only access to summary results provided by the Research Data Center. Therefore, approval by an ethics committee and informed consent were determined not to be required, in accordance with German law. All summary results were anonymized by Research Data Center. In practice, this means that any information allowing the drawing of conclusions about a single patient or a specific hospital was censored by Research Data Center to guarantee data protection. Moreover, to prevent the possibility to draw conclusions from a single hospital, the data are verified and situationally censored by Research Data Center in those cases.
This database represents a virtually complete collection of all hospitalizations in German hospitals that are reimbursed according to the DRG system. From this database, we extracted data on all STEMI (ICD-10 code I21.0, I21.1, I21.2 or I21.3) cases admitted to German hospitals between 2017 and 2020.
Using the number of STEMI cases between 2017 and 2019, we estimated the expected number of STEMI cases in 2020. In detail, this STEMI forecast was calculated by application of poisson regression models with the number of weekly (or monthly) STEMI procedures as endpoints and the calendar year and the calendar week (or month) as continuous and categorical covariates, respectively. These regression models included all procedures (2017–2019) and were then used for the prediction of the expected number of STEMI cases in 2020. Finally, the expected number of STEMI cases in 2020 is then compared to the actually observed number of STEMI cases in 2020. See Supplemental Table 1 for details of the two regression models. In the next step, crude monthly in-hospital STEMI mortality is compared between pre-pandemic (2017–2019) periods and 2020. Thereby, relative risks (RR) are calculated using poisson regression models with the application of robust standard errors.
When visualizing the results on a weekly basis, calendar weeks 53 and 1 are omitted due to problems in length. All analyses were carried out using Stata 16.0 (StataCorp, College Station, Texas, USA).
Results
Baseline characteristics and unadjusted endpoints
From 2017 to 2020, 248,062 patients were treated for a STEMI in Germany (Table 1). While 62,352–62,492 patients were treated per year from 2017 to 2019, in 2020 there were only 60,730 patients. Mean age was 65.21 years and 28.36% were female, which was comparable in all years observed. Other baseline characteristics such as logistic EuroSCORE and the extent of the coronary artery disease, i.e. 1‐, 2- or 3-vessel disease, were also comparable in all years.
Table 1.
Baseline characteristics and unadjusted endpoints of all STEMI procedures in Germany in 2017–2020
| 2017 | 2018 | 2019 | 2020 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | 62,488 | 62,352 | 62,492 | 60,730 | 248,062 | |||||
| Logistic EuroSCORE, mean/SD | 7.25 | 7.23 | 7.34 | 7.31 | 7.33 | 7.27 | 7.39 | 7.34 | 7.33 | 7.29 |
| Age in years, mean/SD | 65.04 | 13.02 | 65.21 | 13.04 | 65.26 | 12.96 | 65.32 | 12.91 | 65.21 | 12.98 |
| Female, % | 28.89% | 28.07% | 28.32% | 28.14% | 28.36% | |||||
| 1‐vessel CAD, % | 29.64% | 29.33% | 29.53% | 29.08% | 29.40% | |||||
| 2‐vessel CAD, % | 28.49% | 28.28% | 28.32% | 28.65% | 28.43% | |||||
| 3‐vessel CAD, % | 36.63% | 37.30% | 37.24% | 37.47% | 37.16% | |||||
| Left main stenosis, % | 6.10% | 6.43% | 6.18% | 6.14% | 6.21% | |||||
| Mortality, % | 10.83% | 10.96% | 10.87% | 11.09% | 10.94% | |||||
| Stent implantation, % | 86.85% | 87.63% | 88.01% | 88.48% | 87.73% | |||||
| Ventilation > 48 h, % | 8.49% | 8.32% | 8.13% | 8.42% | 8.34% |
CAD coronary artery disease, EuroSCORE European System for Cardiac Operative Risk Evaluation, N number of procedures, SD standard deviation
In-hospital mortality at 11.09% in 2020 was only slightly higher than the average at 10.94%. Regarding stent implantations, a continuous increase from 2017 to 2020 from 86.85 to 88.48% can be observed. The rate of mechanical ventilation > 48 h was comparable in all years.
Comparison of forecasted and observed STEMI in 2020
When comparing forecasted and observed STEMI numbers in 2020, a correlation can be seen (Fig. 1): noticeable fewer STEMI were treated in those weeks respectively months with an increasing COVID-19 hospitalization rate (monthly percentage decrease in STEMI: March − 14.85%, April − 13.39%, November − 11.92%, December − 22.95%).
Fig. 1.

Weekly and monthly number of STEMI as well as weekly number of COVID-19 hospitalizations in Germany. Forecasted and observed weekly and monthly number of STEMI interventions (above figures in A and B), relative difference between forecasted and observed weekly and monthly number of STEMI interventions (middle figures in A and B) as well as weekly number of new hospital admissions for COVID-19 per million inhabitants according to Roser et al. [27] (bottom figure in A)
However, the observed number of STEMI interventions in those months with only small COVID-19 hospitalization rates following the first wave reached the forecasted value but did not exceed it in response to the previous lower ones. This resulted in an overall reduction of STEMI interventions in 2020 compared to 2017–2019.
When considering the forecasted and observed monthly in-hospital mortality in case of STEMI (Fig. 2), crude in-hospital mortality after STEMI increased significantly at the peaks of the first and second waves in 2020 (monthly in-hospital mortality: April RR = 1.11 [95% CI 1.02; 1.21], November RR = 1.13 [1.04; 1.24], December RR = 1.16 [1.06; 1.27]).
Fig. 2.

Monthly in-hospital mortality after STEMI intervention in Germany. Forecasted and observed monthly in-hospital mortality after STEMI (above figure) as well as the relative risk of monthly in-hospital mortality (bottom figure). RR relative risk; CI confidence interval
Discussion
Our results show that the COVID-19 pandemic resulted in a noticeable decrease in the number of STEMI interventions in Germany at the peaks of the first and second waves in 2020, corresponding to an increasing rate of COVID-19 hospitalizations. Meanwhile, in-hospital mortality after STEMI increased significantly during these phases.
Decreases in the number of STEMI procedures during the lockdown were also reported by Mesnier et al. [10] in a registry study in France. Furthermore, the authors noted that there was no catch-up phenomenon in the 4 weeks following the lockdown. But they analyzed only 8 weeks, the 4 weeks preceding and following the lockdown. However, we observed a whole year. Our study confirmed those results for the entire year 2020: No catch-up effect could be observed in those months with only small COVID-19 hospitalization rates following the first wave. This resulted in an overall reduction of STEMI in Germany in 2020. There are several possible explanations for the lower number of STEMI: The population may have moved less during the lockdown, so STEMI occurred less frequently due to a reduction of excessive physical activity. The same applies to a possible decrease of professional stress, e.g. by reducing travel times or working in a familiar environment at home [2, 10]. However, these effects are speculative since physical activity is generally also considered to be a protective factor for cardiovascular disease and all-cause mortality [11, 12]. Furthermore, previous studies suggest that the rate of depression and mental stress during the COVID-19 pandemic may even have increased [13]. In addition, less pollution may have contributed to the reduced STEMI numbers. Alternatively, patients with STEMI may not have contacted medical emergency services due to fear of a SARS-CoV-2 infection [2, 10, 14]. In the last case, a catch-up effect is not to be expected.
Similar results with declining patient numbers during the COVID-19 pandemic but higher in-hospital mortality have also been observed in other disciplines such as acute stroke care [15] or in patients undergoing cholecystectomy [16].
Furthermore, Rattka et al. [2] analyzed the topic in a meta-analysis of ten international studies with 50,123 STEMI patients. In contrast to our results, the authors found no increase in in-hospital mortality. They argue that information campaigns may have been quickly implemented and pre- as well as in-hospital procedures may have been rapidly optimized by the medical teams and cardiology professionals. However, they also point out that the observed period may have been too short to discover significant differences in mortality.
On the other hand, and in line with our results, Gluckman et al. [17] indicated an increasing in-hospital mortality after STEMI during the lockdown. They discussed a possible delay by patients, medical services or cardiac catheterization laboratories. Furthermore, Wienbergen et al. [18] showed a significantly higher rate of patients presenting with cardiogenic shock and out-of-hospital cardiac arrest. That may be associated with a delayed presentation in the case of STEMI and may also have contributed to the increased in-hospital mortality demonstrated in our study. Therefore, early hospital admission in the case of STEMI seems particularly important.
Consequently, people and especially patients with already known heart disease such as coronary artery disease must be made aware that they should report to medical emergency services in the event of acute symptoms, pointing out the high risk of mortality and morbidity in these cases.
The study has certain strengths and limitations, in accordance with previous analyzes [19–24]. A major strength is the use of a very large, complete national data set of all STEMI based on electronic health records, allowing us to draw conclusions with high applicability. There are also limitations beyond those typical of retrospective studies. The analysis relies on administrative data, so coding errors are almost unavoidable. Usually, however, 20% of DRG are reviewed by independent physician teams from health insurances, so overall reliability should be good. Furthermore, data is limited to the actual hospital stay as well as to the coded data that are transmitted by the hospitals. Therefore, statements about parameters before or after the stay, or a differentiation within the stay are not possible. This refers e.g. to parameters like rate of cardiogenic shocks or resuscitations before admission, time delays to hospitalization, or the door-to-balloon time. For the same reason, rates of out-of-hospital deaths or unsuccessful resuscitations before hospital admission due to STEMI could not be captured and thus the overall mortality may be even higher than the observed in-hospital mortality suggests. In addition, the use of risk scores recommended in the ESC Guidelines [25, 26], e.g. the GRACE risk score, was not suitable because it can hardly be calculated using the data sent to DESTATIS by the hospitals (e.g. no transmission of precise heart rate or blood pressure). The logistic EuroSCORE used in this study is therefore one way of at least roughly estimating the risk. Finally, no long-term follow-up is possible because the data source used does not allow a connection between different hospital stays of the same patient. Our study thus solely provides data on in-hospital outcomes, although for a very large, complete national yearly cohort of procedures.
Conclusions
In summary, the COVID-19 pandemic led to a noticeable decrease in the number of STEMI interventions in Germany at the peaks of the first and second waves in 2020. At the same time, in-hospital mortality after STEMI increased significantly in these phases.
Supplementary Information
Below is the link to the electronic supplementary material.
Author contributions
VO: conception and design as well as analysis and interpretation of the data particularly from the medical perspective, first draft, substantive revision. PS: interpretation of data, substantive revision. IH: interpretation of data, substantive revision. AH: interpretation of data, substantive revision. MZ: interpretation of data, substantive revision. DW: interpretation of data, substantive revision. KK: conception and design as well as acquisition and analysis and interpretation of the data particularly from the statistical-methodological perspective, first draft, substantive revision. CM: conception and design as well as analysis and interpretation of the data particularly from the medical perspective, first draft, substantive revision. All authors have approved the submitted version to be published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by internal funding from the University Heart Center/Medical Center – University of Freiburg.
Data availability
Data are available upon reasonable request. The patients’ data are stored on the server of the Federal Bureau of statistics and are not available due to data protection. The calculated raw data are sent anonymized to the scientist.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and informed consent
Our study did not involve direct access by the investigators to data on individual patients but only access to summary results provided by the Research Data Center of the Federal Bureau of Statistics. Therefore, approval by an ethics committee and informed consent were determined not to be required, in accordance with German law.
Footnotes
Klaus Kaier and Constantin von zur Mühlen share the last authorship.
References
- 1.Kapsner LA, Kampf MO, Seuchter SA, Gruendner J, Gulden C, Mate S, Mang JM, Schuttler C, Deppenwiese N, Krause L, Zoller D, Balig J, Fuchs T, Fischer P, Haverkamp C, Holderried M, Mayer G, Stenzhorn H, Stolnicu A, Storck M, Storf H, Zohner J, Kohlbacher O, Strzelczyk A, Schuttler J, Acker T, Boeker M, Kaisers UX, Kestler HA, Prokosch HU. Reduced Rate of Inpatient Hospital Admissions in 18 German University Hospitals during the COVID-19 lockdown. Front Public Health. 2020;8:594117. doi: 10.3389/fpubh.2020.594117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rattka M, Dreyhaupt J, Winsauer C, Stuhler L, Baumhardt M, Thiessen K, Rottbauer W, Imhof A. Effect of the COVID-19 pandemic on mortality of patients with STEMI: a systematic review and meta-analysis. Heart. 2021;107:482–487. doi: 10.1136/heartjnl-2020-318360. [DOI] [PubMed] [Google Scholar]
- 3.Toscano O, Cosentino N, Campodonico J, Bartorelli AL, Marenzi G. Acute myocardial infarction during the COVID-19 pandemic: an update on clinical characteristics and outcomes. Front Cardiovasc Med. 2021;8:648290. doi: 10.3389/fcvm.2021.648290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mafham MM, Spata E, Goldacre R, Gair D, Curnow P, Bray M, Hollings S, Roebuck C, Gale CP, Mamas MA, Deanfield JE, de Belder MA, Luescher TF, Denwood T, Landray MJ, Emberson JR, Collins R, Morris EJA, Casadei B, Baigent C. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet. 2020;396:381–389. doi: 10.1016/S0140-6736(20)31356-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Scholz KH, Lengenfelder B, Thilo C, Jeron A, Stefanow S, Janssens U, Bauersachs J, Schulze PC, Winter KD, Schroder J, Vom Dahl J, von Beckerath N, Seidl K, Friede T, Meyer T. Impact of COVID-19 outbreak on regional STEMI care in Germany. Clin Res Cardiol. 2020;109:1511–1521. doi: 10.1007/s00392-020-01703-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Seiffert M, Brunner FJ, Remmel M, Thomalla G, Marschall U, L'Hoest H, Acar L, Debus ES, Blankenberg S, Gerloff C, Behrendt CA. Temporal trends in the presentation of cardiovascular and cerebrovascular emergencies during the COVID-19 pandemic in Germany: an analysis of health insurance claims. Clin Res Cardiol. 2020;109:1540–1548. doi: 10.1007/s00392-020-01723-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Eckner D, Hofmann EM, Ademaj F, Martinovic K, Vogt F, Becher PM, Schrage B, Westermann D, Pauschinger M. Differences in the treatment of acute coronary syndrome in the pre-COVID and COVID Era: an analysis from two German High-Volume Centers. J Cardiovasc Dev Dis. 2021;8:145. doi: 10.3390/jcdd8110145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.De Luca G, Verdoia M, Cercek M, Jensen LO, Vavlukis M, Calmac L, Johnson T, Ferrer GR, Ganyukov V, Wojakowski W. Impact of COVID-19 pandemic on mechanical reperfusion for patients with STEMI. J Am Coll Cardiol. 2020;76:2321–2330. doi: 10.1016/j.jacc.2020.09.546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rodríguez-Leor O, Cid-Álvarez B, de Prado AP, Rossello X, Ojeda S, Serrador A, López-Palop R, Martín-Moreiras J, Rumoroso JR, Cequier Á. Impact of COVID-19 on ST-segment elevation myocardial infarction care. The Spanish experience. Revista Española de Cardiología (English Edition) 2020;73:994–1002. doi: 10.1016/j.rec.2020.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mesnier J, Cottin Y, Coste P, Ferrari E, Schiele F, Lemesle G, Thuaire C, Angoulvant D, Cayla G, Bouleti C. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: a registry study. Lancet Public Health. 2020;5:e536–e542. doi: 10.1016/S2468-2667(20)30188-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, Collet J-P, Corrado D, Drezner JA, Halle M. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: the Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC) Eur Heart J. 2021;42:17–96. doi: 10.1093/eurheartj/ehaa605. [DOI] [PubMed] [Google Scholar]
- 12.Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, George SM, Olson RD. The physical activity guidelines for Americans. JAMA. 2018;320:2020–2028. doi: 10.1001/jama.2018.14854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, Dörrie N, Schweda A, Skoda E-M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health. 2020;42:672–678. doi: 10.1093/pubmed/fdaa106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hannan EL, Wu Y, Cozzens K, Friedrich M, Tamis-Holland J, Jacobs AK, Ling FS, King SB, III, Venditti FJ, Walford G. Percutaneous coronary intervention for ST-elevation myocardial infarction before and during COVID in New York. Am J Cardiol. 2021;142:25–34. doi: 10.1016/j.amjcard.2020.11.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Richter D, Eyding J, Weber R, Bartig D, Grau A, Hacke W, Krogias C. Analysis of nationwide stroke patient care in times of COVID-19 pandemic in Germany. Stroke. 2021;52:716–721. doi: 10.1161/STROKEAHA.120.033160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Koch F, Hohenstein S, Bollmann A, Meier-Hellmann A, Kuhlen R, Ritz J-P. Cholecystectomies in the COVID-19 pandemic during and after the first lockdown in Germany: an analysis of 8561 patients. J Gastrointest Surg. 2022;26:408–413. doi: 10.1007/s11605-021-05157-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gluckman TJ, Wilson MA, Chiu ST, Penny BW, Chepuri VB, Waggoner JW, Spinelli KJ. Case rates, treatment approaches, and outcomes in acute myocardial infarction during the coronavirus disease 2019 pandemic. JAMA Cardiol. 2020;5:1419–1424. doi: 10.1001/jamacardio.2020.3629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wienbergen H, Retzlaff T, Schmucker J, Marin LAM, Rühle S, Garstka D, Osteresch R, Fach A, Hambrecht R. Impact of COVID-19 pandemic on presentation and outcome of consecutive patients admitted to hospital due to ST-elevation myocardial infarction. Am J Cardiol. 2021;151:10–14. doi: 10.1016/j.amjcard.2021.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Oettinger V, Kaier K, Heidt T, Hortmann M, Wolf D, Zirlik A, Zehender M, Bode C, von zur Mühlen C, Stachon P. Outcomes of transcatheter aortic valve implantations in high-volume or low-volume centres in Germany. Heart. 2020;106:1604–1608. doi: 10.1136/heartjnl-2019-316058. [DOI] [PubMed] [Google Scholar]
- 20.Kaier K, Oettinger V, Reinecke H, Schmoor C, Frankenstein L, Vach W, Hehn P, von zur Mühlen C, Bode C, Zehender M, Reinöhl J. Volume–outcome relationship in transcatheter aortic valve implantations in Germany 2008–2014: a secondary data analysis of electronic health records. BMJ Open. 2018;8:e020204. doi: 10.1136/bmjopen-2017-020204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stachon P, Hehn P, Wolf D, Heidt T, Oettinger V, Zehender M, Bode C, von zur Mühlen C, Kaier K. In-hospital outcomes of self-expanding and balloon-expandable transcatheter heart valves in Germany. Clin Res Cardiol. 2021;110:1977–1982. doi: 10.1007/s00392-021-01928-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schrage B, Becher PM, Goßling A, Savarese G, Dabboura S, Yan I, Beer B, Söffker G, Seiffert M, Kluge S, Kirchhof P, Blankenberg S, Westermann D. Temporal trends in incidence, causes, use of mechanical circulatory support and mortality in cardiogenic shock. ESC Heart Failure. 2021;8:1295–1303. doi: 10.1002/ehf2.13202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Neumann JT, Goßling A, Sörensen NA, Blankenberg S, Magnussen C, Westermann D. Temporal trends in incidence and outcome of acute coronary syndrome. Clin Res Cardiol. 2020;109:1186–1192. doi: 10.1007/s00392-020-01612-1. [DOI] [PubMed] [Google Scholar]
- 24.Freisinger E, Fuerstenberg T, Malyar NM, Wellmann J, Keil U, Breithardt G, Reinecke H. German nationwide data on current trends and management of acute myocardial infarction: discrepancies between trials and real-life. Eur Heart J. 2014;35:979–988. doi: 10.1093/eurheartj/ehu043. [DOI] [PubMed] [Google Scholar]
- 25.Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio AL, Crea F, Goudevenos JA, Halvorsen S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. [DOI] [PubMed] [Google Scholar]
- 26.Collet J-P, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2021;42:1289–1367. doi: 10.1093/eurheartj/ehaa575. [DOI] [PubMed] [Google Scholar]
- 27.Roser M, Ritchie H, Ortiz-Ospina E, Hasell J (2020) Coronavirus Pandemic (COVID-19), Published Online at OurWorldInData.org. https://ourworldindata.org/COVID-hospitalizations
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available upon reasonable request. The patients’ data are stored on the server of the Federal Bureau of statistics and are not available due to data protection. The calculated raw data are sent anonymized to the scientist.