

Abstract
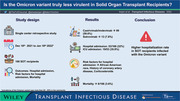
Solid organ transplant (SOT) recipients are at high risk for severe disease with severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) infection. Emerging variants of concern have disproportionately affected this population. Data on severity and outcomes with the Omicron variant in SOT recipients are limited. Thus we conducted this single‐center, retrospective cohort study of SOT recipients diagnosed with SARS‐CoV‐2 infection from December 18, 2021 to January 18, 2022, when prevalence of the Omicron variant was more than 80%‐95% in the community. Univariate and multivariate logistic regression analysis was performed to identify risk factors for hospital admission. We identified 166 SOT patients: 112 (67.5%) kidney, 22 (13.3%) liver, 10 (6.0%) lung, seven (4.2%) heart, and 15 (9.0%) combined transplants. SARS‐CoV‐2 vaccine series was completed in 59 (35.5%) recipients. Ninety‐nine (59.6%) and 13 (7.8%) recipients received casirivimab/imdevimab and sotrovimab, respectively. Fifty‐three (32%) recipients required hospital admission, of which 19 (35.8%) required intensive care unit level of care. Median follow‐up was 50 (interquartile range, 25‐59) days, with mortality reported in six (3.6%) patients. Risk factors identified for hospital admission were African American race (p < .001, odds ratio [OR] 4.00, 95% confidence interval [CI] 1.84‐8.70), history of coronary artery disease (p = .031, OR 3.50, 95% CI 1.12‐10.87), and maintenance immunosuppression with corticosteroids (p = .048, OR 2.00, 95% CI 1.01‐4.00). In conclusion, contrary to that in the general population, we found a higher hospital admission rate in SOT recipients with omicron variant infection. Further studies to investigate the efficacy of newer treatments are necessary, even as outcomes continue to improve.
Keywords: COVID‐19, omicron, SARS‐CoV‐2, solid organ transplant
Graphical abstract:
Abbreviations
- AKI
Acute kidney injury
- CDC
Centers for Disease Control and Prevention
- CI
confidence interval
- COVID‐19
Coronavirus disease of 2019
- IQR
interquartile range
- OR
odds ratio
- SARS‐CoV‐2
severe acute respiratory syndrome coronavirus 2
- SOT
solid organ transplant
- TPE
total plasma exchange
1. INTRODUCTION
Solid organ transplant (SOT) confers an increased risk for mortality from COVID‐19. 1 Since the beginning of the pandemic, the transplant community has tried to continue safe organ transplantation 2 , 3 and provide appropriate care to those living with organ transplants. However, a significant number of SOT recipients were infected and have had poor outcomes. 4
As newer treatments became available, the importance of wearing masks, social distancing, and hand hygiene remain unchanged. Even after the development and use of vaccines, SOT recipients were estimated to have an 82‐fold higher rate of breakthrough infections. 5 This led to a vaccine booster strategy being recommended. 6 , 7 However, the vaccine response in this population is still suboptimal. In 2021, several variants of concern including delta and omicron were detected. The omicron variant was first identified in South Africa and spread all over the world in a relatively short time. It is reported to be less virulent and more contagious as compared to delta in the general population, but this has not been confirmed in SOT recipients. Recently, Tixagevimab co‐packaged with cilgavimab, a monoclonal antibody for pre‐exposure prophylaxis was approved by the US Food and Drug Administration, but the clinical efficacy against new variants is still unknown. 8 Since mid‐December, the Miami‐Dade metropolitan area has seen a rise in COVID‐19 cases due to the omicron variant. 9 Currently, real‐world data on the outcomes in SOT recipients who are infected with omicron variant have not been reported. Thus, we conducted a retrospective analysis of cases, at a time when there was community spread and dominance of the omicron variant.
2. METHODS
2.1. Study design and patient characteristics
This was a single center, retrospective cohort study of adult SOT recipients who tested positive for severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) at Jackson Memorial Hospital‐Miami Transplant Institute, between December 18, 2021 and January 18, 2022. Of note, between December 18 and 24, 2021, around 80 percent of the randomly sampled specimens were Omicron variant. After December 25, 2021, more than 95% were Omicron variant. We included SOT recipients who were 18 years and older at the time of diagnosis of COVID‐19. We excluded all pretransplant candidates or those who had already lost their graft prior to diagnosis of COVID‐19. Testing of nasopharyngeal swab specimens using either reverse transcriptase‐polymerase chain reaction or antigen testing was done. Antibody testing targeting spike protein was performed via the VITROS test to measure IgG and total antibodies. Antibody testing was performed prior to the receipt of monoclonal antibody therapy. Data were obtained from the electronic medical record system. We collected patient demographics, immunosuppression regimen, serum creatinine at baseline, 7 days from COVID‐19 diagnosis, and at 30 days from COVID‐19 diagnosis, as well as therapies received. Clinical severity was assessed with the help of criteria suggested by the World Health Organization ordinal scale for clinical improvement. 10 The study was approved by the institutional research committee and research ethics board of the University of Miami.
2.2. Treatment strategies
At our center, all actively followed recipients were instructed to contact their transplant coordinator when symptomatic, after exposure or diagnosis of COVID‐19. Mildly symptomatic patients received casirivimab/imdevimab, which was replaced by sotrovimab once it became available in our institute. Patients who required hospital admission and no supplemental oxygen received 3 days of remdesivir. 11 Once patients required supplemental oxygen, we started remdesivir for 5 days and dexamethasone. 12 In cases where cytokine storm occurred, and/or clinical symptoms became refractory to remdesivir and dexamethasone, we gave tocilizumab, baricitinib or performed total plasma exchange (TPE). 13
2.3. Clinical outcomes
Outcomes measured include severity of disease, hospital admission, and all‐cause mortality within 1 month after diagnosis.
2.4. Statistical analysis
Demographics were analyzed with descriptive statistics. Categorical variables were reported as number and percentage. Continuous variables were reported as median and interquartile range (IQR). To analyze the trends in serum creatinine, we conducted a paired t‐test. We conducted risk factor analysis for hospital admission. For categorical variables, we used fisher's exact test or chi‐square test, whichever appropriate. We performed Mann–Whitney U test for continuous variables. After univariate analysis, we developed a logistic regression model with backward elimination to identify the risk factors for hospital admission. To develop model, we checked the correlation between risk factors and then put the variables whose p values were less than .2 into the model. All statistics were performed using SPSS (version 27.0.x). A p value of less than .05 was recognized as statistically significant. The supplementary figure was created using GraphPad Prism version 9.3.1 for Windows, GraphPad Software, San Diego, California USA, www.graphpad.com.
3. RESULTS
3.1. Patient characteristics
During the study period, we identified 166 recipients who were actively followed at our institute and diagnosed with SARS‐CoV‐2 infection. Of those, 112 (67.5%) kidney, 22 (13.3%) liver, 15 (9.0%) heart, 10 (6.0%) lung, and 15 (9.0%) combined transplants, which included two (1.2%) multivisceral transplant recipients, were found (Table 1). Eighteen (10.8%) patients had documented re‐infection. Median time of follow‐up was 50 days (IQR, 25–59) from diagnosis of COVID‐19. One hundred sixteen (69.9%) recipients and one (0.6%) recipient had 30‐day and 90‐day follow‐up, respectively. The patients were predominantly male (95, 58.4%) and of Hispanic ethnicity (99, 59.6%), with a median age of 57 (IQR 48–64) years old. The median time from transplant to diagnosis of COVID‐19 was 27 (IQR 0.6–262) months. At the time of diagnosis, tacrolimus, mycophenolate mofetil, and prednisone were used as maintenance immunosuppression in 149 (89.7%), 125 (75.3%), and 85 (51.2%) recipients, respectively. Belatacept was used as maintenance immunosuppression in eight of 125 (6.4%) of kidney transplant recipients.
TABLE 1.
Clinical characteristics, management, and outcomes of SOT recipients with COVID‐19
| Clinical characteristics | |
|---|---|
| Variable | All Patients N = 166 (%) # , * |
| Demographics | |
| Age, median (IQR) | 57 (48–64) |
| Gender, male | 95 (58.4%) |
| Ethnicity, Hispanic | 99 (59.6%) |
| Race | |
| White | 126 (75.9%) |
| African American | 38 (32.8%) |
| Asian | 2 (1.2%) |
| Comorbidities | |
| Hypertension | 129 (77.7%) |
| Diabetes mellitus | 54 (32.5%) |
| Chronic kidney disease | 14 (8.4%) |
| Coronary artery disease | 15 (9.0%) |
| COPD | 10 (6.0%) |
| HIV | 3 (1.8%) |
| Transplanted organ | |
| Kidney | 112 (67.5%) |
| Liver | 22 (13.3%) |
| Heart | 15 (9.0%) |
| Lung | 10 (6.0%) |
| Combined transplants | 15 (9.0%) |
| Kidney‐pancreas | 7 (4.2%) |
| Liver‐kidney | 5 (3.0%) |
| Heart‐kidney | 1 (0.6%) |
| Multi‐visceral | 2 (1.2%) |
| Maintenance immunosuppression | |
| Tacrolimus | 149 (89.7%) |
| Sirolimus | 21 (12.6%) |
| MMF | 125 (75.3%) |
| Belatacept | 8/125 (6.4%) |
| Prednisone | 85 (51.2%) |
| Time from transplant to diagnosis (months), median (range) | 27 (0.6–262) |
| Days of symptoms on presentation, median (IQR) | 3 (2–5) |
| Prior history of COVID‐19 | 18 (10.8%) |
| Vaccination status | |
| Completed primary series | 59 (35.5%) |
| Received two vaccine doses | 63 (37.9%) |
| Received one vaccine dose | 7 (4.2%) |
| Unvaccinated | 37 (22.2%) |
| COVID‐19 antibody data ** | |
| IgG tested | 95 (57.2%) |
| IgG detected | 66/95 (69.4%) |
| Management | |
| Immunosuppression | |
| No reduction in immunosuppression | 89 (53.6%) |
| MMF held | 32/125 (25.6%) |
| MMF 50% dose reduction | 42/125 (25.3%) |
| WHO ordinal clinical severity score | |
| 1. No limitation of activities | 105 (63.2%) |
| 2. Limitation of activities | 3 (1.8%) |
| 3. Hospitalized, no oxygen therapy | 21 (12.6%) |
| 4. Oxygen by mask or nasal prongs | 22 (13.2%) |
| 5. Not invasive ventilation or high flow mask | 7 (4.2%) |
| 6. Intubation and mechanical ventilation | 3 (1.8%) |
| 7. Ventilation + additional organ support (vasopressors, RRT, ECMO) | 5 (3.0%) |
| Treatment | |
| Casirivimab‐imdevimab | 99 (59.6%) |
| Sotrovimab | 13 (7.8%) |
| Remdesivir | 50 (30.12%) |
| Dexamethasone IV/PO | 36 (21.68%) |
| Tocilizumab | 3 (1.80%) |
| Therapeutic plasma exchange | 11 (6.6%) |
| Outcomes | |
| Overall mortality | 6 (3.6%) |
| 30‐day mortality | 5 (3.0%) |
| Hospitalized | 65 (39%) |
| Hospitalized due to worsening of COVID‐19 symptoms | 53 (32%) |
| ICU | 19 (35.8%) |
| COVID medical ward | 34 (64.1%) |
| Length of stay, days, median (IQR) | 5 (3–8) |
| Follow‐up, days, median (IQR) | 50 (25–59) |
Abbreviations: COPD, chronic obstructive pulmonary disease; COVID‐19, coronavirus disease of 2019; ECMO, extracorporeal membrane oxygenation; HIV, human immunodeficiency virus; ICU, intensive care unit; IgG, immunoglobulin G; IQR, interquartile range; IV, intravenous; MMF, mycophenolate mofetil; PO, oral; RRT, renal replacement therapy; SOT, solid organ transplant; WHO, World Health Organization.
Data presented as absolute number (percentage), unless specified otherwise.
Individual percentage values are rounded and might not total 100%.
Antibody testing targeting spike protein was performed via the VITROS test to measure IgG and total antibodies.
3.2. Vaccination status
There were 129 (77.7%) patients who had received at least one dose of the COVID‐19 vaccine; with 59 (35.5%), 63 (37.9%), seven (4.2%) having received 3, 2, and single dose, respectively. Of 129 who received vaccinations, 123 (95.3%) received messenger RNA (mRNA) vaccines, with only six (4.6%) adenovirus‐vector vaccine recipients. At the time of diagnosis, COVID‐19 antibody testing was performed in 95 (57.2%); 66 of 95 (69.4%) had detectable antibody levels which included 25 (37.8%) fully vaccinated patients. Of note, there were no recipients who received Tixagevimab‐cilgavimab prior to SARS‐CoV‐2 infection.
3.3. Management
Immunosuppression agents were modified by the transplant team depending on severity of symptoms. Antimetabolite agents were held in 32 of 125 (25.6%) recipients; tacrolimus was continued in the majority of the recipients (Table 1). Sotrovimab, casirivimab/imdevimab, remdesivir, and tocilizumab were given in 13 (7.8%), 99 (59.6%), 50 (30.1%), and 3 (1.8%) recipients, respectively. Dexamethasone for treatment for COVID‐19 was used in 36 (21.7%). TPE was reserved for refractory cases and performed in 11 (6.6%).
3.4. Outcomes
Hospital admission was observed in 65 (39%); with 53 (32%) admitted due to worsening COVID‐19 symptoms (Table 1). All 65 hospital admissions were seen within 30 days of SARS‐Cov‐2 diagnosis. The median length of hospital stay was 5 (IQR, 3–8) days.
Kidney function was compared among patients before COVID‐19 diagnosis, 7 days postdiagnosis of COVID‐19, and 1‐month postdiagnosis of COVID‐19. Median creatinine was 1.3 mg/dl (range 0.5–9.4), 1.3 mg/dl (range 0.6–10.7), and 1.27 mg/dl (range 0.6–10.4), respectively. Creatinine increased after COVID‐19 diagnosis (p < .001); however 1‐month posttransplant, there was no statistical difference when compared to prior to infection (p = .31) (Figure S1).
Of 53 patients hospitalized for worsening COVID‐19 symptoms, 19 (35.8%) patients required intensive care unit (ICU) level of care with eight of 19 patients (42.1%) required mechanical ventilation. During follow‐up, two (1.2%) recipients had biopsy‐proven graft rejection, and six (3.6%) died. The mortality was seen on day 4, 13, 13, 25, 27, and 31 after diagnosis of COVID‐19.
We then conducted risk factor analysis for hospital admission, summarized in supplemental table. In the univariate analysis, for hospital admission, we found that African American race was statistically significant. After that, we developed a logistic regression model with stepwise backward elimination based on the univariate analysis result. Statistically significant risk factors identified for hospital admission were African American race (p < .001, odds ratio [OR] 4.00, 95% confidence interval [CI] 1.84–8.70), history of coronary artery disease (p = .031, OR 3.50, 95% CI 1.12–10.87), and maintenance immunosuppression with corticosteroids (p = .048, OR 2.00, 95% CI 1.01–4.00) (Table 2).
TABLE 2.
Univariate and multivariate analysis of risk factors for hospital admission in patient population
| Risk factor | Univariate p value | Multivariate p value | Odds ratio | 95% confidence interval |
|---|---|---|---|---|
| Age | .52 | |||
| Gender | .63 | |||
| African American race | .001 | <.001 | 4.00 | 1.84–8.70 |
| Hypertension | .44 | |||
| Diabetes | .17 | |||
| Coronary artery disease | .16 | .031 | 3.50 | 1.12–10.87 |
| Chronic obstructive pulmonary disease | .83 | |||
| Maintenance immunosuppression | ||||
| Tacrolimus | .69 | |||
| Mycophenolate | .44 | |||
| Corticosteroids | .077 | .048 | 2.00 | 1.01–4.00 |
| Everolimus | .072 | |||
4. DISCUSSION
We present a single‐center, retrospective cohort study, describing our experience managing COVID‐19 in SOT recipients during the Omicron surge. We observed low mortality and a higher hospital and ICU admission rate compared to reports from general population. 14 African American race, history of coronary artery disease, and corticosteroid usage were identified as risk factors for hospital admission. 15 , 16
Early in the pandemic, high mortality and hospital admission rates have been reported in SARS‐CoV‐2 infected in SOT. 4 With the availability of new treatments, outcomes have significantly improved. 17 In a prospective study conducted by Solera et al., assessing outcomes in SOT patients during the omicron wave, hospitalization rate was found to be 24%, with a mortality rate of 4.4%. Use of sotrovimab early and receiving three or more doses of the vaccine significantly decreased length of hospital stay and disease severity. 18
In the United States, monoclonal antibodies and COVID‐19 vaccines were available since November 2020 and early 2021, respectively. Thus, compared to existing literature in SOT patients, our cohort is a mix of vaccinated, unvaccinated, and patients who have received monoclonal antibodies despite limited supply of sotrovimab. This contributes to the relatively lower hospital admission rate (39%) and mortality (3.6%). However, as compared to the general population, 14 we experienced a higher hospital admission rate, which affects the transplant community significantly. Similar findings were also reported by Villanego et al., in their multicenter study conducted in Spain. 19
Additionally, of the six deaths in our patient cohort, the majority (5/6, 83.3%) occurred within 30 days of COVID‐19 diagnosis—a finding in contrast with Heldman et al., 20 which reported >20% of deaths occurring between 28 and 90 days following COVID‐19 diagnosis. This difference could likely be due to the the availability of vaccines, newer COVID‐19 therapies, and difference in SARS‐CoV‐2 variants that were prevalent during the time‐periods captured by our study.
In the risk factor analysis, African American race, coronary artery disease, and steroid usage were identified as risk factors for hospital admission. 15 Disparities in access to and utilization of monoclonal antibodies have been reported, with the African American population having low uptake. 21 , 22 We also have checked the distribution of monoclonal antibody usage among races at our center. There was no statistically significant difference; however, African American race was identified as an independent risk factor. The reason might be not only a biological mechanism but also other unmeasurable variables, such as accessibility to other medical care. These social and cultural factors need to be better studied in transplant patients.
To our knowledge, this is the first report identifying risk factors for hospital admission in SOT recipients infected with SARS‐CoV‐2 albeit limited to the omicron variant. COVID‐19 is disproportionately affecting African American communities, including SOT recipients. Of note, at least one dose of the vaccine was given in 28/38 (73.6%) and 101/126 (80.1%) for African American and Caucasian, respectively, which is not statistically different (p > .05). Ensuring equitable access to newer treatment modalities, and prevention education should be prioritized in SOT patients.
The current study has several limitations. First, whole genome sequencing data were not done routinely to identify the Omicron variant. With this knowledge, the study period was cautiously selected and limited to a time when more than 80% of the cases in the community were due to Omicron. Second, we have a relatively short follow‐up period to identify other complications such as rejection, secondary fungal infection, or even death. Finally, given the small sample size, we could not conduct risk factor analysis for mortality. Even for risk factor analysis for hospital admission, we should take into consideration that type 2 error might exist.
In conclusion, we found a low mortality but a high hospital and ICU admission rate in our cohort during the Omicron surge. While the Omicron variant is reported to be less virulent, and more transmissible, the hospital admission rate is higher in SOT patients compared to that reported in national data, 14 which continues to burden transplant centers. Further studies are needed to assess the effectiveness of early treatment with sotrovimab, and 3 days of remdesivir in preventing hospitalization in this population. Also, studying different variants is needed for a better understanding of SARS‐CoV‐2 infection in SOT recipients, to prepare for emerging variants of concern.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
SA, GG, and YN conceived and designed the study. YN analyzed the data. All the authors participated in the generation of the data and interpretation of results. SA, GG, and YN wrote the first version of the article. All the authors approved the final version of the manuscript.
FUNDING INFORMATION
The authors received no specific funding for this work.
Supporting information
Supporting Information
Graphical Abstract
Anjan S, Khatri A, Viotti JB, et al. Is the Omicron variant truly less virulent in solid organ transplant recipients? Transpl Infect Dis. 2022;e13923. 10.1111/tid.13923
Giselle Guerra and Yoichiro Natori share co‐senior authorship.
Contributor Information
Giselle Guerra, Email: gguerra@med.miami.edu.
Yoichiro Natori, Email: yxn138@med.miami.edu.
REFERENCES
- 1. Raja MA, Mendoza MA, Villavicencio A, et al. COVID‐19 in solid organ transplant recipients: a systematic review and meta‐analysis of current literature. Transplant Rev (Orlando). 2020;35(1):100588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Kumar D, Manuel O, Natori Y, et al. COVID‐19: a global transplant perspective on successfully navigating a pandemic. Am J Transplant. 2020;20(7):1773‐1779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Chandorkar A, Coro A, Natori Y, et al. Kidney transplantation during coronavirus 2019 pandemic at a large hospital in Miami. Transpl Infect Dis. 2020;22(6):e13416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kates OS, Haydel BM, Florman SS, et al. COVID‐19 in solid organ transplant: a multi‐center cohort study. Clin Infect Dis. 2020;. 73(11):e4090‐e4099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Qin CX, Moore LW, Anjan S, et al. Risk of breakthrough SARS‐CoV‐2 infections in adult transplant recipients. Transplantation. 2021;105(11):e265‐e266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hall VG, Ferreira VH, Ku T, et al. Randomized trial of a third dose of mRNA‐1273 vaccine in transplant recipients. N Engl J Med. 2021;385(13):1244‐1246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kamar N, Abravanel F, Marion O, et al. Assessment of 4 doses of SARS‐CoV‐2 messenger RNA‐based vaccine in recipients of a solid organ transplant. JAMA Netw Open. 2021;4(11):e2136030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Tixagevimab and cilgavimab (Evusheld) for pre‐exposure prophylaxis of COVID‐19. JAMA. 2022;327(4):384‐385. [DOI] [PubMed] [Google Scholar]
- 9. This is unprecedented: Omicron causes 80% of coronavirus cases in Miami‐Dade in 2 weeks. 2021. Accessed July 5, 2022. https://www.local10.com/news/local/2021/12/17/this-is-unprecedented-omicron-causes-80-of-coronavirus-cases-in-miami-dade-in-2-weeks/
- 10. WHO R&D Blueprint . COVID‐19 therapeutic trial synopsis. Accessed December 16, 2020. https://www.who.int/publications‐detail/covid‐19‐therapeutic‐trial‐synopsis
- 11. Gottlieb RL, Vaca CE, Paredes R, et al. Early Remdesivir to prevent progression to severe Covid‐19 in outpatients. N Engl J Med. 2022;386(4):305‐315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Group RC, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid‐19. N Engl J Med. 2021;384(8):693‐704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Faqihi F, Alharthy A, Abdulaziz S, et al. Therapeutic plasma exchange in patients with life‐threatening COVID‐19: a randomised controlled clinical trial. Int J Antimicrob Agents. 2021;57(5):106334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Iuliano AD, Boehmer JM, Boehmer TK, et al. Trends in disease severity and health care utilization during the early Omicron variant period compared with previous SARS‐CoV‐2 high transmission periods — United States, December 2020–January 2022. MMWR Morb Mortal Wkly Rep 2022;71:146‐152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Acosta AM, Garg S, Pham H, et al. Racial and ethnic disparities in rates of COVID‐19‐associated hospitalization, intensive care unit admission, and in‐hospital death in the United States from March 2020 to February 2021. JAMA Netw Open. 2021;4(10):e2130479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Ko JY, Danielson ML, Town M, et al. Risk factors for Coronavirus Disease 2019 (COVID‐19)‐associated hospitalization: COVID‐19‐associated hospitalization surveillance network and behavioral risk factor surveillance system. Clin Infect Dis. 2021;72(11):e695‐e703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Heldman MR, Kates OS, Safa K, et al. Changing trends in mortality among solid organ transplant recipients hospitalized for COVID‐19 during the course of the pandemic. Am J Transplant. 2022;22(1):279‐288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Solera JT, Arbol BG, Alshahrani A, et al. Impact of vaccination and early monoclonal antibody therapy on COVID‐19 outcomes in organ transplant recipients during the Omicron wave. Clin Infect Dis. 2022. doi: 10.1093/cid/ciac324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Villanego F, Vigara LA, Alonso M, et al. Trends in COVID‐19 outcomes in kidney transplant recipients during the period of Omicron variant predominance. Transplantation. 2022;106(6):e304‐e305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Heldman MR, Kates OS, Safa K, et al. Delayed mortality among solid organ transplant recipients hospitalized for COVID‐19. Clin Infect Dis. 2022. doi: 10.1093/cid/ciac159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Behr CL, Joynt Maddox KE, Meara E, Epstein AM, Orav EJ, Barnett ML. Anti‐SARS‐CoV‐2 monoclonal antibody distribution to high‐risk medicare beneficiaries, 2020–2021. JAMA. 2022;327(10):980983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Bierle DM, Ganesh R, Wilker CG, et al. Influence of social and cultural factors on the decision to consent for monoclonal antibody treatment among high‐risk patients with mild‐moderate COVID‐19. J Prim Care Community Health. 2021;12:21501327211019282. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information
Graphical Abstract