

Abstract
Aim
To examine the moderating effect of burnout on the relationship between nurses' competence, professional competence and professional values.
Background
There is a preponderance of burnout studies of nurses before and during the COVID‐19 pandemic. However, little is known about burnout's moderating influence on nurses' professionalism, competence and values during the ongoing pandemic.
Methods
This study used a correlational, cross‐sectional design and convenience sampling to recruit 809 Saudi nurses employed in four government hospitals. Four self‐report instruments were used to collect data from August 2021 to March 2022. Spearman Rho, structural equation modelling and multi‐group moderation analysis were used to analyse the data.
Results
Most of the participants had high burnout. There was a moderate to high correlation between the dimensions of professional competence, nurse professional values, burnout and nurse competence. Both professional competence and nurse professional values significantly affected nurse competence. Nurse professional values also had a direct effect on professional competence. Professional competence and nurse professional values on nurse competence may vary among those with low, moderate and high levels of burnout, suggesting the moderating effect of burnout.
Conclusions
The positive impacts of nurse professional values and professional competence on nursing competence were validated in this study, as was the evidence of burnout's moderating effect on the studied connections. To avoid burnout, it is necessary to increase organizational knowledge and support for nurses, their working conditions and the environment through strategies that promote well‐being and empowerment.
Implications for nursing management
Nurse managers can implement policies to help nurses minimize burnout and improve their professional values and competence. Management policies may be considered include increased staffing, opportunities to improve technical abilities through education and vocational training programs, and increased diversity of job assignments.
Keywords: burnout, moderating analysis, nurse, nurse competence, professional competence, professional values
1. INTRODUCTION
Burnout was reported by the World Health Organization (WHO, 2019) as one of the reasons that may impact why people seek medical assistance and contact health services. In the 11th Revision of the International Classification of Diseases (ICD‐11), the WHO (2019) defines burnout as a disorder when too much stress at work cannot be managed. Three dimensions measure it: emotions of tiredness or depletion of energy, increasing mental distance from one's employment, or feelings of negativism or cynicism about one's job and diminished professional efficacy. Nurse burnout is a widespread phenomenon characterized by a decline in nurses' capacity, which manifests as emotional stress, unwillingness and unhappiness, resulting in decreased workplace productivity (Mudallal et al., 2017). Stressors contributing to nurses' burnout include long work shifts, pressure to make decisions quickly and caring for patients with a poor prognosis, leading to exhaustion (Dall'Ora et al., 2020).
Burnout among nurses had been reported in the literature and published works before the COVID‐19 pandemic. Nurses' burnout was due to constant stress, even when not in the hospital, and reported symptoms of depersonalization. Their emotional exhaustion and burnout grew worse for every additional period a nurse worked (Dall'Ora et al., 2020). Burnout among nurses became more prevalent during the COVID‐19 pandemic. Polish nurses working in the cardiovascular unit report emotional exhaustion, depersonalization, job dissatisfaction and multiple assignments (Uchmanowicz et al., 2021).
Burnout is prevalent among Chinese oncology nurses (Cheng et al., 2015). The report states that nurse leaders and administrators can mitigate the negative impact of burnout on their professional values by strengthening and improving their professional value education through seminars and nursing in‐service education programs (Cheng et al., 2015). Correspondingly, the conflicting demands of patients and their care needs contribute to the cause of burnout among nurses, with the workload being the primary cause, impairing the nurses' professional conduct of duty in the delivery of care to patients (Dall'Ora et al., 2020).
While nurses experience burnout during their duty, they must maintain their professional competencies to deliver quality care (Karami et al., 2017). In 2015, Blažun et al. (2015) published ‘research literature production on nursing competencies from 1981 to 2012: a bibliometric snapshot’. They reported that there are still some issues with the meaning of the term ‘competence’ concerning performance among nurses. Bradshaw (2001) identified the necessary competencies in the conventional role of nurses today. Further, it was suggested that competence and competency definitions have yet to be resolved and agreed upon, particularly considering the urgency of other nursing fields, such as bioinformatics and the globalization of the nursing profession. On the other hand, professional values reflect the attitude of nurses towards their patients. The nurse's attitude is a critical determinant of patient‐centred care (Price, 2015). According to Schank and Weis (2009), ‘professional values are action norms that are recognized by the practitioner and professional group and provide a framework for analyzing beliefs and attitudes that impact actions and performance’ (p. 226). Since nursing is a profession and nurses are members of a professional organization, nurses must uphold professional values (Schmidt & McArthur, 2018).
Professional values have been shown to impact burnout. According to Akbarilakeh et al. (2019), stress and burnout are associated with professional values, with professional values being found to predict the occurrence of burnout in nurses. Nurses' personal and professional values are critical in the event of burnout. Compared to other people's experiences, Dall'Ora et al. (2020) found that nurses face patients' suffering, grief and death each day, compounding the burnout nurses are dealing with. Additionally, many nursing tasks were uninteresting and unsatisfying, while many other activities were appalling by usual standards. These experiences challenge the nurse's professional values (Dall'Ora et al., 2020). Therefore, this study aimed to ascertain the moderating effects of burnout on nurses' professional values and competence to establish effective nursing management strategies during future pandemics.
1.1. Background
Workplace stress caused by interpersonal interactions can lead to burnout, a psychological condition. Overwhelming fatigue, a sense of pessimism and disengagement from work, and inefficiency and productivity are symptoms of this condition (Maslach & Leiter, 2016).
Nurses' burnout became more apparent and pervasive during the COVID‐19 pandemic. The pandemic created multifaceted trauma and multidimensional anxiety for nursing students (Grande et al., 2021) and professional nurses (Ghassemi, 2021). Caring for patients during COVID‐19 exacerbates nurses' burnout (Jang et al., 2021; Sikaras et al., 2022). Burnout became more prevalent and perceptible because of risk factors such as a lack of readiness to cope with COVID‐19, a younger and inexperienced nursing staff, a lack of support from colleagues and the community, a constant threat of COVID‐19 infection, longer working hours in a COVID‐19‐infected environment, and a lack of human and logistical support and resources, among others (Ghassemi, 2021). Nurses who work with COVID‐19 patients report more significant fatigue and burnout than those who do not (Jang et al., 2021; Sikaras et al., 2022).
Published research on burnout and its relationship to professional values and competencies suggests that nurses' values and professionalism may help moderate the occurrence or cessation of burnout in the workplace (Cheng et al., 2015; Jiang et al., 2021). According to Altun (2002), nurses' values are expressed uniquely and independently, and these values play a significant role in the occurrence of burnout. Burnout is more likely to occur when nurses' values conflict with established workplace norms (Altun, 2002). Suppose policymakers engage nurses in programs and continuing education activities that help them strengthen their professional values. In that case, nurses will be able to focus more on their professional values, lowering their risk of burnout (Cheng et al., 2015). Nurse supervisors and colleagues help decrease nurses' perceived emotional exhaustion, leading to burnout (Dall'Ora et al., 2020). Moreover, Jiang et al. (2021) reported a positive relationship between older nurses' burnout and stress levels and a negative correlation between burnout and their professional identity.
The COVID‐19 pandemic has impacted how nurses view their role. Galanis et al. (2021) found that nurses experienced a high level of burnout, which was affected by and associated with numerous demographic and professional variables. It cannot be denied that the COVID‐19 pandemic presented a challenge for nurses worldwide. It was found that servant nurse leaders during COVID‐19 reduced the impact of burnout on nurses (Ma et al., 2021). The psychologically safe working environment fostered by servant leadership is one of the essential preconditions for lowering nurses' burnout (Ma et al., 2021). Burnout was prevalent among nurses during the COVID‐19 pandemic because of changes in the work environment and employment resources. Burnout occurred at all workforce levels during times of frequent job changes caused by the pandemic (Sklar et al., 2021).
Burnout was found to have a moderating effect on the relationship between self‐efficacy and job performance in Korean nurses when it interacted with self‐efficacy. However, the study included only nurses who worked in psychiatric hospitals (Lim et al., 2022). Altun (2000) reported the personal and professional impact of burnout among Turkish nurses but did not include its impact on the nurses' competence. These two studies were conducted before the COVID‐19 pandemic. On the other hand, our study examined the moderating effect of burnout on the relationship between professional competence, which focused on nurses' professional and legal conduct, professional values centred on nurses' ethical and moral responsibilities, and nurse competence, which emphasized nurses' skills. Fukada (2018) and Matsutani et al. (2012) categorized nursing competency into seven elements, two of which are professional competence or developing professional capacity and practicing nursing ethically, which relates to a nurse's professional values. Valizadeh et al. (2019) listed 16 domains of professional competence, including nursing skills and clinical judgement that relate to nursing competence, attitude and moral action that are components of professional values, and professional independence, management and leadership correspond to professional competence. Professional competence is equated with clinical areas in which nurses practice (Halabi et al., 2021). As a result, it is attributed to nurses' clinical competence.
Additionally, our study was conducted during the COVID‐19 pandemic, a period during which frontline nurses are facing significant difficulties in carrying out their nursing roles and responsibility. Published studies on burnout during the COVID‐19 pandemic reported burnout's influence on nurses' intention to leave (de Cordova et al., 2022), burnout during the first wave of the pandemic (Galanis et al., 2021; Khan et al., 2022), burnout on quality patient care (Kakemam et al., 2021), burnout and the affective aspect of nurses (Falatah & Alhalal, 2022), burnout's burden to nurses' roles (Kishi et al., 2022) and burnout's relationship to self‐efficacy (Lim et al., 2022). None of these published studies focused on the moderating effect of burnout on nurses' professionalism, values and competence. Nurses cannot provide quality patient care without the essential ethical principles and attitudes, nursing competence and professional nursing competencies (International Council of Nurses [ICN], 2021; Oldland et al., 2020). Professional nurses should be aware of the three principles of competence: professionalism, values and skills (Fukada et al., 2018; ICN, 2021). Without a clear recognition of these essential dimensions of the nursing profession, burnout will negatively impact nurses' performance and provision of quality care (Dall'Ora et al., 2020; Kakemam et al., 2021). Thus, examining nurses' burnout experiences as a moderating variable in their professional values and competence during the COVID‐19 pandemic may improve therapeutic relationships and communication skills, guiding the development and implementation of effective nursing strategies for hospital policymakers and nursing managers dealing with similar situations in the future.
1.2. Theoretical underpinning
Maslach was the first to postulate a burnout theory and quantify it as a separate concept from stress (Maslach et al., 2008; Maslach & Leiter, 2016). Maslach Burnout Inventory (MBI) was created to measure burnout, which is still one of the most widely used scales worldwide. Maslach characterized burnout as emotional exhaustion, depersonalization, and diminished personal accomplishment (Dall'Ora et al., 2020).
Maslach expanded on her theory by stating that burnout occurs when an employed person experiences an extended and sustained mismatch with one or more of the following. These include workload issues such as having too much work but insufficient resources, control issues such as lack of autonomy in performing one's job, and reward issues such as not giving promotions to those who deserve it (Maslach & Leiter, 2016). Additionally, other situations of mismatch include community, such as when a group of coworkers lacks a sense of belonging, fairness, such as when some nurses are given an advantage over others, and values, such as when the mission and vision are unclear to employees and staff (Dall'Ora et al., 2020). Job resignation attributed to a lack of commitment to the organization, absenteeism, intention to leave the job and a high turnover rate have all been associated with burnout. Pessimism has been viewed as a crucial component of burnout in predicting turnover, and burnout mediates the association between workplace bullying and the intention to resign (Maslach & Leiter, 2016).
1.3. Research hypotheses
Considering the preceding literature on nurse competence, professional values, professional competence and burnout amidst the COVID‐19 pandemic, this study addressed the following hypotheses (Figure 1):
Professional competence influences nurse competence.
Nurse professional values influence nurse competence.
Burnout moderates the influence of professional competence and nurse professional values on nurse competence.
FIGURE 1.
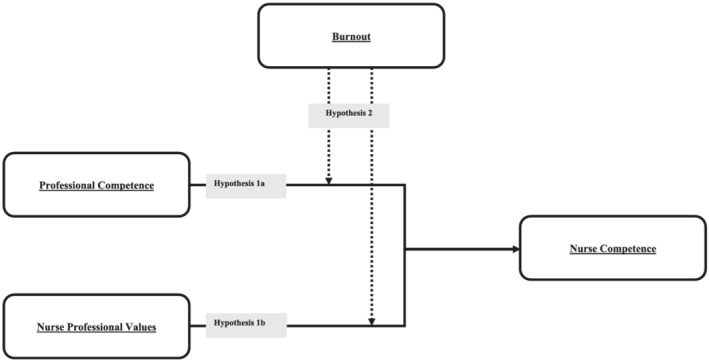
The theoretical burnout‐moderated model of the study: Professional competence and nurse professional values influence nurse competence (H1) while burnout moderates these influences on nurse competence (H2)
2. METHODS
2.1. Research design
A correlational, cross‐sectional design was used to examine the relationship between nurses' professional values and competence and the moderating role of burnout among nurses in Saudi Arabia amidst the COVID‐19 pandemic. The STROBE guideline was utilized to report this study (see Supporting Information Data S1).
2.2. Study setting
Participants were recruited from four government hospitals in Ha'il, Saudi Arabia. The first study location is a general tertiary hospital founded in 1957. It is the oldest established hospital of the four study settings, with a separate convalescent unit adjacent to the main hospital. The second study setting is a trauma centre that caters to patients with diverse health conditions. It is the only Joint Commission International‐accredited hospital in the Ha'il Region. The third study setting, established in 2018, has a capacity of 500 beds and exists to serve the Ha'il region and the entire Kingdom. There are 55 clinics on four floors, each focusing on a different medical specialty. The fourth study setting is a specialized facility that treats adult women and paediatric patients. It opened in 2018 and has already provided care for various health issues, including emergency, outpatient, medical and obstetrical and surgical care.
2.3. Sampling and participants
To recruit eligible nurses for this study, we used convenience sampling. The inclusion criteria set for our study is that the participant should be employed as staff nurses in any of the study settings during the conduct of the study. Furthermore, the participant should have given their ‘implied consent to participate in the study by returning the completed questionnaires to the researchers’ (Polit & Beck, 2017, p. 222). The completion of the questionnaire demonstrates a voluntary option to participate. No attempt was made to determine homogeneity and balance the sample's several variables, such as gender, nationality, or religion, because nurses in each study setting are naturally diverse and complex. Any attempt to balance the gender distribution or other variables could restrict or limit the number of participants (Yang et al., 2021).
Although the minimum sample size for SEM analysis is 200 (Kline, 2015), we computed the required sample size by multiplying the number of items of the instruments by five ([N = 26 + 35 + 22 + 73] * 5 = 780) (Hair et al., 2014). Excluding those who had already participated in the pre‐test, 950 online surveys were distributed, of which 850 have been completed and returned to the researchers. After extensive validation and examination, it was established that 809 questionnaires (85.16% response rate) were appropriately filled out, error‐free, and met the standards for statistical analysis.
2.4. Instrument
Four self‐report instruments were used in this investigation. The authors of these instruments gave their permission to use in this study. These instruments were administered in the original English and Arabic‐translated versions.
The first instrument is the Nurses Professional Values Scale‐Revised (NPVS‐R), which contains 26 items with a Likert‐scale response format ranging from 1 (not important) to 5 (most important) (Weis & Schank, 2009). Each item discusses a specific section of the code and its accompanying interpretive commentary. All items are phrased positively, and none are scored negatively. The total score was calculated by adding the numeric responses to each item, with a range of possible scores of 26–130. The higher the score, the more a nurse's professional value orientation is strengthened. Caring, activism, trust, professionalism and justice are the five factors that emerged from the revised version of the NPVS. It's worth noting that the non‐revised version of the NPVS has eight factors, whereas the revised version only has five. The factors included in the current version of the NPVS‐R emphasize in a broader sense the aspect of caring, which has the most variation among professional values, followed by justice, which serves as the foundation for all professional interactions in all care settings. Duty and loyalty are the other provisions reflected in the factors of professionalism and trust. Activism protects the requirements of the nurses' code of ethics on the social nature of the profession and its accountability to the public it serves. Internal consistency reliability of the five factors ranges from 0.70 to 0.85, with a total scale alpha coefficient of .92 signifying a high level of reliability (Weis & Schank, 2009).
The second instrument used in this study is the Nurse Professional Competence Scale‐Short Form (NPC‐Scale‐SF) (Nilsson et al., 2018). A shortened version of the 88‐item Nurse Professional Competence Scale, the NPC‐Scale‐SF, measures nursing education programs' success and nurses' professional competence in response to hospital system demands. The subscales of NPC‐Scale‐SF are nursing care; value‐based nursing care; medical and technical care; care pedagogics; documentation and administration of nursing care; and development, leadership, and organization of nursing care. It has a total of 35‐items that uses a 4‐point Likert scale to assess each factor. The alpha coefficients for the 35‐item NPC Scale‐SF ranged from 0.71 to 0.86, indicating that the instrument is highly reliable (Nilsson et al., 2018).
The MBI scale is the third instrument, and it is used to assess burnout, emotional fatigue, depersonalization and decreased sense of personal accomplishment (Maslach et al., 2008; Maslach & Leiter, 2016). It consists of 22 items divided into three subscales: emotional exhaustion, depersonalization and personal accomplishment. The first subscale is emotional exhaustion, with 9‐item statements that assess feelings of being emotionally overstretched and depleted by one's job. The second subscale, depersonalization, has 5‐item statements that include five items that measure how unfeeling and impersonal one is when giving service, care, treatment or instruction to patients. Finally, the third subscale is called ‘personal accomplishment’, with 8‐item statements that measure feelings of competence and success in one's work with people. The items are scored on a 7‐point Likert scale ranging from 0 (never) to 6 (every day), with the items being answered based on how often the participants encounter each statement. The Cronbach's alpha scores for the MBI are .90 for emotional exhaustion, .79 for depersonalization and .71 for personal accomplishment.
Finally, the Nurse Competence Scale (NCS) is a generic instrument for assessing nurse competence and identifying the attributes necessary for effective nursing care (Meretoja et al., 2004). The NCS includes 73 items divided into seven competence categories: helping role (7 items), teaching–coaching (16 items), diagnostic functions (7 items), managing situations (8 items), therapeutic interventions (10 items), ensuring quality (6 items) and work role (19 items). Each competency item is evaluated using a visual analogue scale (VAS 0–100; 0 = low level of competence, 100 = high level of competence). The VAS is divided into four parts to define competence level: ≤25 for low level of competence, >25–50 for rather good, >50–75 for good, and >75–100 for very good level of competence. A 4‐point scale is used to assess the frequency of action (0 = not applicable, 1 = very seldom, 2 = occasionally and 3 = very often).
The original versions of the four instruments were translated using a methodical approach. The English to Arabic translation process was carried out by three language experts connected with a university in Hail, Saudi Arabia. To ensure that the instruments were translated efficiently and correctly, a forward‐backward translation was performed using semantic equivalence criteria and procedures throughout the process (Polit & Beck, 2017). To check for flaws and inconsistencies, we pilot tested the translated version of the instruments with a small sample (10%) of the total number of participants. The four instruments' Cronbach's alpha scores were .99 for the NPVS‐R, .97 for the MBI, .98 for the NPC‐Scale‐SF and .99 for the NCS, indicating high reliability (Taber, 2018). The English and Arabic versions of the instruments were used concurrently on the online survey form during data collection. This allowed Arabic‐speaking participants to choose what instrument versions they were comfortable using. Our Filipino and Indian participants used the English version since they are fluent in English.
2.5. Data collection
Data were collected via Google survey forms between 20 August 2021 and 15 March 2022. Due to COVID‐19 health restrictions and protocols, no face‐to‐face contacts were made during the data collection period. First, the authors paid a courtesy visit to the head of the nursing department at each study setting to secure permission to conduct the study. Following approval, the researchers distributed the online survey link to study participants with the assistance and support of nurse administrators and staff nurses, who assisted the researchers in ensuring that the online questionnaires were successfully received and completed by participants.
Our data were collected using a Google survey form. The validated instruments were formatted as a Google survey questionnaire. The link generated by this survey form was sent to the nurse administrators and then distributed to the target nurse participants' group chat (e.g., Messenger, WhatsApp, Viber). They can access the survey link via their computers or mobile phones. When they finish the survey and click the submit button, their responses are automatically saved in the Google drive repository. Only the four researchers directly involved in data collection and analysis have access to this Google drive.
Typical problems in online surveys were poor response rate, representativeness, and item‐response (Polit & Beck, 2017). To prevent these issues and improve the online survey quality, we took the following steps: used the participants' language (e.g., Arabic and English), avoided using grids or matrices to represent the Likert's scale answer and pilot tested the instruments using the Google survey form.
2.6. Validity and rigour
The survey questionnaire was initially pre‐tested among 10 eligible participants to determine its reliability. They are excluded as actual participants during data collection. Reliability analyses revealed good to excellent reliability coefficients, with Cronbach's alpha values .98, .99, .97 and .98 for the NPC‐Scale‐SF, NPVS‐R, MBI and NCS, respectively. These results support the validity and reliability of the research instruments (Taber, 2018).
2.7. Data analysis
Statistical analyses were conducted using IBM SPSS Statistics for Windows and AMOS version 20.0, Armonk, NY: IBM Corp. A p value of .05 was considered statistically significant. Descriptive statistics, which included mean and standard deviation and frequency and proportions, were employed to summarize the demographic characteristics, the professional competency scores, the nurse professional value scores, the burnout scores and categories and the nurse competence scores. Correlation analyses using Spearman Rho were initially conducted to determine the relationships between the dimension of professional competence, nurse professional values, nurse competence, and burnout.
Structural equation modelling (SEM), using maximum likelihood estimation, was also conducted to determine the influence of nurse professional values and professional competence on nurse competence (Byrne, 2013). The fit indices of the hypothesized and emerging models were evaluated using the following parameters: CMIN/df ≤ 3.00, root‐mean‐square error of approximation (RMSEA) ≤ 0.08 (Byrne, 2013), comparative‐fit‐index (CFI) ≥ 0.90, goodness‐of‐fit index (GFI) ≥ 0.90 and a higher parsimonious normal fit index (PNFI) (Huang et al., 2017). Multi‐group moderation analysis determined the moderating effect of burnout on the influence of nurse professional values and professional competence on nurse competence. It was also conducted to test the invariance or difference of the model across the levels of burnout (van Montfort et al., 2018).
2.8. Ethical considerations
After completing all the necessary paperwork, the Ethics Review Board of the University of Hail granted permission to conduct this study (reference number H‐2021‐012; approved on 8 February 2021). The data were collected online through Google survey forms that displayed the description and consent statements. Consent forms in both English and Arabic were used. The participant impliedly consented to participate by voluntarily completing the form. Throughout the study, we maintained participant anonymity and data confidentiality.
3. RESULTS
3.1. Demographic profile of participants
It can be seen in Table 1 that most participants were female (86.80%), had a bachelor's degree (86.20%), had 1–5 years of clinical experience (64.90%), were Roman Catholic (46.50%) and were assigned in a specialized unit (52.90%).
TABLE 1.
Demographic profile of the participants (n = 809)
| Characteristic | Frequency (f) | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 107 | 13.20% |
| Female | 702 | 86.80% |
| Years of experience | ||
| Below 1 year | 65 | 8.00% |
| 1–5 years | 525 | 64.90% |
| 6–10 years | 219 | 27.10% |
| More than 10 years | 0 | 0.00% |
| Religion | ||
| Islam | 353 | 43.60% |
| Roman Catholic | 376 | 46.50% |
| Hinduism | 80 | 9.90% |
| Highest educational attainment | ||
| Nursing | 89 | 11.00% |
| Bachelor | 697 | 86.20% |
| Masters | 23 | 2.80% |
| Doctorate | 0 | 0.00% |
| Unit of assignment | ||
| Regular ward | 286 | 35.40% |
| Department | 95 | 11.70% |
| Special unit | 428 | 52.90% |
3.2. Descriptive statistics of burnout and correlation of variables
As presented in Table 2, the mean overall burnout score was 84.92 (SD = 41.71), and categorization of the individual scores indicated that more participants had high burnout (63.70%). Analyses of the dimensions of burnout also showed that most of the participants had high levels of occupational exhaustion (61.60%) and depersonalization (67.40%), while 44.10% had low levels of personal accomplishment. Correlation analyses (see Supporting Information S1) also showed moderate to high correlation between the dimensions of professional competence, dimensions of nurse professional values, burnout and nurse competence.
TABLE 2.
Descriptive statistics of burnout and burnout dimensions among the participants (n = 809)
| Variables | Mean (SD) | Frequency (f) | Percentage (%) |
|---|---|---|---|
| Overall burnout levels | 84.92 (41.71) | ||
| Low burnout | 126 | 15.60% | |
| Moderate burnout | 168 | 20.80% | |
| High burnout | 515 | 63.70% | |
| Dimensions of burnout | |||
| Occupational exhaustion | 34.95 (17.19) | ||
| Low | 137 | 16.90% | |
| Moderate | 174 | 21.50% | |
| High | 498 | 61.60% | |
| Depersonalization | 19.37 (9.71) | ||
| Low | 107 | 13.20% | |
| Moderate | 157 | 19.40% | |
| High | 545 | 67.40% | |
| Personal accomplishment | 30.60 (15.25) | ||
| Low | 357 | 44.10% | |
| Moderate | 81 | 10.00% | |
| High | 371 | 45.90% |
3.3. Influence of professional competence and nurse professional values on nurse competence
Initial analyses of the hypothesized model indicated poor parameter indices (Table 3). Modification indices also suggested a path from nurse professional values to professional competence and multiple covariances between the different dimensions of professional competence and nurse professional values. Hence, the model was re‐specified and adjusted.
TABLE 3.
Goodness‐of‐fit statistics for the structural equation model analysis and moderation (multiple group) analysis (n = 809)
| Model | Chi‐square | RMSEA | GFI | CFI | PNFI | |||
|---|---|---|---|---|---|---|---|---|
| χ 2 (df) | χ 2/df (p value) | ∆χ 2 (p value) | RMSEA (p value) | 90% CI | ||||
| Structural equation models | ||||||||
| Hypothesized model | 641.49 (52) | 12.34 (0.001) | – | 0.118 (0.001) | 0.110–0.127 | 0.88 | 0.97 | 0.76 |
| Emerging model | 135.37 (47) | 2.88 (0.001) | – | 0.053 (0.304) | 0.043–0.062 | 0.97 | 0.99 | 0.79 |
| Moderation (multiple group) analysis | ||||||||
| Model with no restrictions | 626.87 (141) | 4.45 (0.001) | – | 0.065 (0.001) | 0.062–0.071 | 0.91 | 0.97 | 0.68 |
| Model with restricted structural weights | 1513.59 (165) | 9.17 (0.001) | 28.47 (0.001) | 0.101 (0.001) | 0.096–0.105 | 0.85 | 0.91 | 0.75 |
Abbreviations: CFI, comparative fit index; CI, confidence interval; df, degrees of freedom; GFI, Goodness‐of‐Fit Index; PNFI, Parsimonious Normal Fit Index; RMSEA, root‐mean‐square error of approximation; χ2, Chi‐square fit statistics.
After re‐specification, the model had better fit parameters (χ 2/df = 0.288, p = .001; RMSEA = 0.053, p = .304; CFI = 0.99; GFI = 0.97; PNFI = 0.79). In addition, both professional competence (β = .12, p = .002) and nurse professional values (β = .88, p = .002) significantly affected nurse competence, measuring 87.40% of the variance. Nurse professional values also had a direct effect on professional competence (β = .38, p = .002) and measured 14.60% of its variance (Figure 2).
FIGURE 2.
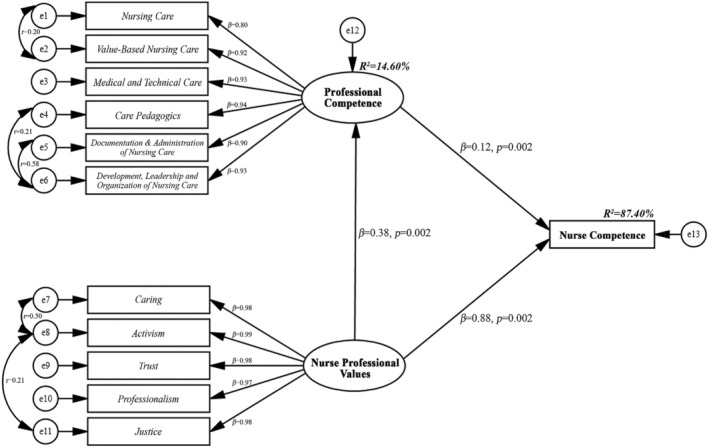
Emerging model of the influence of professional competence and nurse professional values on nurse competence (χ 2/df = 2.88, RMSEA = 0.053, CFI = 0.99, GFI = 0.97, PNFI = 0.79). Abbreviations: CFI, comparative fit index; df, degrees of freedom; GFI, Goodness‐of‐Fit Index; PNFI, Parsimonious Normal Fit Index; RMSEA, root‐mean‐square error of approximation; χ2, Chi‐square fit statistics
3.4. Moderating effect of burnout on the influence of professional competence and nurse professional values on nurse competence
Multi‐group moderation analysis revealed that the goodness‐of‐fit statistics between the unconstrained and restrained structural weights were statistically different (Table 3). This result indicates that the influence of professional competence and nurse professional values on nurse competence may vary among those with low, moderate and high levels of burnout, suggesting the moderating effect of burnout.
As illustrated in Table 4, the effects of professional competence on nurse competence decreased from low burnout (β = .23, p = .003) to moderate (β = .07, p = .047) and high burnout (β = .01, p = .806). On the other hand, the effects of nurse professional values to nurse competence initially increased from low burnout (β = .55, p = .001) to moderate burnout (β = .99, p = .001) but dropped at high burnout levels (β = .62, p = .001). A similar finding can be noted with nurse professional values' effect on professional competence, with smaller regression coefficients. Comparative analyses using critical ratios showed that the path coefficients for professional competence to nurse competence were not statistically different among the levels of burnout. Yet, as presented in Table 4, pairwise path comparisons were statistically significant on all levels of burnout for the effects of nurse professional values on both nurse competence and professional competence.
TABLE 4.
Multi‐group moderation analysis of burnout on the relationship of professional competence and nurse professional values on nurse competence (n = 809)
| Variables | Low burnout (n = 126) | Moderate burnout (n = 168) | High burnout (n = 515) | Pairwise path comparisons a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p value | β | p value | β | p value | Low versus moderate | Low versus high | Moderate versus high | |||
| Professional competence | → | Nurse competence | .23 | .003 | .07 | .047 | .01 | .806 | −1.74 (0.082) | 1.33 (0.184) | 1.90 (0.057) |
| Nurse professional values | → | Nurse competence | .55 | .001 | .99 | .001 | .62 | .001 | 29.97 (0.001) | 15.47 (0.001) | −12.29 (0.001) |
| Nurse professional values | → | Professional competence | −.23 | .003 | .22 | .004 | .13 | .004 | 4.58 (0.001) | 4.46 (0.001) | −2.59 (0.010) |
Values are represented as z value (p value).
4. DISCUSSION
This study determined the influence of nurse professional values and professional competence on nurse competence. In addition, this study ascertained the moderating effect of burnout on the influence of nurse professional values and professional competence on nurse competence. By and large, results indicated that both nurse professional values and professional competence positively affected nurse competence. Furthermore, analyses suggested that burnout among nurses moderated the direct effects of nurse professional values and professional competence on nurse competence, with an inversed U‐shaped effect for nurse professional values and a constant decrease in effect for professional competence.
During the COVID‐19 pandemic, nurses reported higher burnout than before the pandemic. Falatah and Alhalal (2021) explored the role of work‐related stress on nurses in Saudi Arabia during the COVID‐19 pandemic. They reported that work‐related stress implicitly or explicitly affected nurses' affective responses, well‐being and compassion. Similarly, Lim et al. (2022) examined the moderating effect of burnout on the connection between self‐efficacy and job performance during the COVID‐19 pandemic. They found that burnout moderates the impact of self‐efficacy in reducing work performance. During the COVID‐19 pandemic, Kakemam et al. (2021) observed that an increase in adverse hospital events was associated with nurse burnout. This high burnout resulted in substandard patient care and an increased likelihood of adverse events in the clinical setting. Correspondingly, an increase in psychological and physical stress has been associated with increased burnout among Japanese nurses, resulting in a higher incidence of burnout. These nurses provide direct care to patients hospitalized for observation suspected of having COVID‐19 infection (Kishi et al., 2022).
It is interesting to note that nurse professional values significantly and positively influenced professional competence among the participants. ICN (2021) posited that nurse professional values refer to the culmination of the socialization in the nursing profession from code of ethics, experiences, mentors and peers. In contrast, professional competency reflects the nurses' attitudes, knowledge, and psycho‐social and psychomotor elements (Oldland et al., 2020). Literature has emphasized the importance of professional values in directing a nurse's professional actions, ensuring quality patient care, maintaining patient safety and improving decision‐making skills, actions and ethical judgement (Altun, 2002; Poreddi et al., 2021; Weis & Schank, 2009). This notion is further supported by Skela‐Savič et al. (2017). They accentuated that a dimension of the content structure of professional competence is the ‘competency expected in practice’, which involves the nurse's professional values of helping, teaching‐coaching and work roles. It has also been shown that the different dimensions of nurse professional values—caring, activism, trust, professionalism and justice—are imperative in developing a nurse's professional competence, particularly those focused on clinical care (Prosen et al., 2021).
Results also showed the moderate and positive influence of nurse professional values on nurse competence, a finding consistent with previous theoretical assertions. Nursing competency is the nurse's ability to effectively demonstrate attributes including personal characteristics, professional attitude, values, knowledge and skills to fulfil their professional responsibilities (Pueyo‐Garrigues et al., 2022). Fukada (2018) even divided the elements of nursing competence into three (personal traits, professional attitude and behaviours and ability to provide cases based on professional knowledge and skills), with two categories focusing on professional values. Professional attitudes and behaviours encompass a nurse's responsibility for professional development, assuming professional responsibilities (Fukada, 2018) and autonomy which is encapsulated in the six constructs of the NPVS‐R (caring, activism, trust, professionalism and justice) (Weis & Schank, 2009). These theoretical underpinnings support the importance of nurse professional values in developing nurse competence; hence, nurses should always endeavour to enhance their professional values. Nurse administrators should continuously provide opportunities and avenues for nurses to build this critical attribute. In this light, Mlambo et al. (2021) posited that nurses should participate in continuing education to develop competency and professionalism. Administrators are urged to provide and support continuing education and provide nurses adequate access to such education with appropriate education incentives and provisions.
The model can also glean that professional competence positively affected nurse competence, which has been noted in previous literature. Heydari et al. (2016) purported that professional competency is integral in rendering nursing care according to professional standards. Nursing competency has been extensively defined as providing efficient, effective, safe and quality nursing care. Therefore, nurses must establish excellent professional competence to fulfil their nursing roles and responsibilities of delivering quality nursing care professionally. Karami et al. (2017) even emphasized that professional competence is a fundamental concept in nursing, and it is necessary for the delivery and improvement of quality patient care. In a similar vein, studies have posited that clinical nursing competence is an accumulation of different general and specific competencies, which include professional skills, and these are important in facilitating better‐quality patient care (Faraji et al., 2019; Heydari et al., 2016; Immonen et al., 2019). Afshar et al. (2020) even accentuated that the lack of professional competency or professional insufficiency can negatively affect nurses' development of clinical competencies. As such, nurse administrators should explore and implement programs and approaches to enhance professional competence among nurses. Mlambo et al. (2021) suggested establishing appropriate programs and interventions to improve the work environment and provide continuing education opportunities.
It is also worth noting that the results of the moderation analysis confirmed that burnout had a significant moderating effect. For professional competence, burnout has a decreasing impact suggesting that the influence of professional competence on nurse competence decreased with increasing levels of burnout. On the other hand, burnout had an inversed U‐shaped effect on the relationship between nurse professional values and nurse competence. This result denotes that the influence of nurse professional values was amplified as burnout increased from mild to moderate, but it decreased when burnout level was high. The negative effect of burnout on professional competence and nurse competence may be attributed to the physical, emotional, and psychological burden on a nurse. Burnout is defined as a psychological syndrome due to a prolonged response to chronic interpersonal stressors of a person's job. It has three dimensions: occupational exhaustion, depersonalization, and personal accomplishment (Maslach & Leiter, 2016). Across the literature, six domains of burnout have been identified: workload, control, reward, community, fairness and values (Maslach et al., 2016; Mukherjee et al., 2020). Therefore, increasing levels of burnout may denote higher levels of workload, lower sense of control, inadequate rewards, poor community relationships, and increased inequities and social injustice. These factors can negatively affect a nurse's physical, emotional, and psychological capacity to provide quality nursing care, regardless of their professional competence, due to high levels of exhaustion, loss of energy, fatigue, negative emotions, low morale and inability to cope with current stressors (Dall'Ora et al., 2020; Galanis et al., 2021). As a result of these burnout experiences, the ability of nurses to function competently in the clinical setting decreases and may compromise patient care (Ali Zakeri et al., 2020; Kakemam et al., 2021; Ma et al., 2021).
In a different light, the results showed that burnout had an inversed U‐shaped effect on the relationship between nurse professional values and nurse competence. This finding indicates that the influence of nurse professional values on nurse competence was highest when burnout was at a moderate level. This result may be due to the nature of the profession, which allows nurses to function and even refine their competency under constant occupational pressure and stress. Studies on burnout levels of nurses have shown that this population of health care professionals constantly has moderate levels of burnout due to the complex nature of their occupation (Ali Zakeri et al., 2020; de Cordova et al., 2022; Jose et al., 2020). With such a level of burnout, workload and other factors may be manageable and even provide an avenue for nurses to enhance their decision‐making skills and clinical skills, thus, their overall nurse competence (Afshar et al., 2020; Mudallal et al., 2017).
Focusing on the burnout‐moderated model of the influence of nurse professional values and professional competence on nurse competence, the current results have theoretical and applied significance. Theoretically, this model contributes to the growing knowledge on the interaction of nurse professional values, professional competence, nurse competence, and burnout. From a clinical perspective, the knowledge culled from the model can be utilized by nurse practitioners and nurse administrators to develop appropriate policies, programs and interventions to promote nurse professional values, professional competence and nurse competence and maintain burnout within a manageable level. Programs and interventions to address burnout may be customized according to the dynamics of the institution and may be implemented at an individual, departmental and organizational level (Maslach et al., 2008; Maslach & Leiter, 2016). Organizational understanding and support are also imperative in improving the working environment and in implementing approaches that can enhance nurses' general well‐being to empower them in addressing burnout (Ali Zakeri et al., 2020; Falatah & Alhalal, 2021). The study results also accentuate the need to constantly assess and evaluate the nurse's professional values, professional competence, and nurse competence and provide opportunities to enhance these attributes through training, workshops, and continuing education (Karami et al., 2017; Mlambo et al., 2021).
We conducted our study during the COVID‐19 pandemic. Professionalism and competence unquestionably remain regardless of the presence or absence of a pandemic, as it is necessary for nurses. Nonetheless, the pandemic affirms nurses' inherent professionalism and competence for various reasons. One explanation is that an overwhelming number of patients exhibit COVID‐19 symptoms unknown to the medical community (WHO, 2020). Despite this, nurses sustain the same degree of care, professionalism and competence despite their concern and lack of knowledge regarding the severity of the novel coronavirus (Fernandez et al., 2020; Sun et al., 2020).
The fact that nurses are working relentlessly during the pandemic, which could affect their morale, empathy and compassion and lead to a loss of professionalism and competence, is another reason why professionalism and competence are emphasized more than usual during the pandemic (Fernandez et al., 2020; Ruiz‐Fernández et al., 2021). Nevertheless, our results demonstrated that these two essential characteristics of nurses were not affected negatively by the pandemic and, in contrast, were reinforced more.
Finally, during the pandemic, nurses revealed to the world that, in addition to their professionalism and competence, they possess the courage to confront the COVID‐19 virus head‐on (Khodaveisi et al., 2021). Despite the risk of COVID‐19 to themselves and their family, their service and sacrifice exemplify professionalism and competence.
4.1. Limitations and recommendations
This study presented several limitations that may affect the findings' generalizability. First, the study employed a cross‐sectional design, which may not have allowed researchers to determine the causation among study variables. Second, we used self‐reported survey instruments, leading to overestimating and underestimating the results. Third, convenience sampling was utilized, which may not represent the total population. This study included only four hospitals in a particular region of Saudi Arabia. Therefore, the outcomes of this study must be regarded with caution.
We recommend evaluating the emerging model developed from this study with bigger sample size and across many sites (e.g., nationwide or multi‐country). An experimental or longitudinal design may be necessary to determine causation between variables and produce accurate results. Finally, qualitative research will increase the depth of narratives regarding nurses' professional values and competencies.
5. CONCLUSION
This study confirmed the positive effects of nurse professional values and professional competence on nurse competence and provided evidence on the moderating effect of burnout on the analysed associations. Although higher nurse professional values and professional competence enhance nurse competence, higher levels of burnout may limit the impact of nurse professional values and professional competence on nurse competence. The burnout‐moderated model of the influence of nurse professional values and professional competence on nurse competence emphasizes three critical points. First, nurse professional values and professional competence should be assessed and enhanced through training, workshops, continuing education and appropriate incentives. Second, nurse administrators may consider implementing appropriate policies and programs to mitigate the development and aggravation of burnout among nurses. These programs must be individualized to the institution's setting and may be implemented across the different levels of the institution. Lastly, there is a need to boost organizational understanding and support for the nurses and improve their working conditions and the environment through approaches that promote well‐being and empowerment to prevent burnout.
6. IMPLICATIONS FOR NURSING MANAGEMENT
Our findings highlight the need for nurse managers to be aware of burnout among their nursing staff. According to our results, burnout moderates nurses' competence, professional values and professional competence. Burnout being the underlying source of the problem, it should be managed initially. Nurse managers should plan activities to help decrease nurse burnout by establishing a conducive and healthy working environment with rest periods between tasks. While hospitals are always occupied with patients, there are periods when nurses can take breaks when the occupancy is low. In particular, burnout can be reduced if activities at least once or twice each month allow nurses to take a vacation, contingent on staff availability and the number of patients.
Additionally, the sources of burnout may be from the hospital or personal. Nurses can suffer from burnout while working in the hospital if they are experiencing stress at home attributable to a range of issues, including family problems, marital concerns and other matters. As a response, nurse managers should be able to evaluate whether burnout is caused by personal factors, hospital factors or both. Direct communication with the nurse can assist in reducing the impact of burnout.
Nurses' burnout increased during the COVID‐19 pandemic and will continue to do so due to factors such as longer work hours, additional tasks related to COVID‐19 protocols, and fear and anxiety of possibly bringing the infection home are some of the reasons why it became more difficult for nurses to experience burnout compared to pre‐pandemic. Nurse managers' responsibilities did not change throughout the pandemic. They were rather strengthened and structured to make them more adaptable to the pandemic demands concerning their nurses' burnout experiences.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest.
ETHICS STATEMENT
University of Ha'il Research Ethics Committee (REC) approval number H‐2021‐012 (approved on 2 August 2021).
Supporting information
Data S1. STROBE Statement—Checklist of items that should be included in reports of cross‐sectional studies
Table S1. Correlation Coefficients among the Dimensions of Professional Competence, Dimensions of Nurse Professional Values, Burnout, and Nurse Competence (n = 809)
ACKNOWLEDGEMENTS
We would like to express our gratitude to the nurse participants from the four hospitals in Ha'il region, Saudi Arabia.
Grande, R. A. N. , Berdida, D. J. E. , Villagracia, H. N. , Raguindin, S. M. , Cornejo, L. T. O. , Al Reshidi, N. M. , Alshammari, A. T. , Aljebari, B. J. , & AlAbd, A. M. A. (2022). The moderating effect of burnout on professionalism, values and competence of nurses in Saudi Arabia amidst the COVID‐19 pandemic: A structural equation modelling approach. Journal of Nursing Management, 1–14. 10.1111/jonm.13754
Funding information This research did not receive any specific grant from funding agencies in the public, commercial or not‐for‐profit sectors.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Afshar, M. , Sadeghi‐Gandomani, H. , & Alavi, N. M. (2020). A study on improving nursing clinical competencies in a surgical department: A participatory action research. Nursing Open, 7(4), 1052–1059. 10.1002/nop2.485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbarilakeh, M. , Goodarzi, F. , & Oroei, M. (2019). The association between professional value and occupational burnout among nurses working in the emergency department. Social Determinants of Health, 5(1), 36–47. 10.22037/sdh.v5i1.26947 [DOI] [Google Scholar]
- Ali Zakeri, M. , Bazmandegan, G. , Ganjeh, H. , Zakeri, M. , Mollaahmadi, S. , Anbariyan, A. , & Kamiab, Z. (2020). Is nurses' clinical competence associated with their compassion satisfaction, burnout and secondary traumatic stress? A cross‐sectional study. Nursing Open, 8(1), 354–363. 10.1002/nop2.636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Altun, İ. (2002). Burnout and nurses' personal and professional values. Nursing Ethics, 9(3), 269–278. 10.1191/0969733002ne509oa [DOI] [PubMed] [Google Scholar]
- Blažun, H. , Kokol, P. , & Vošner, J. (2015). Research literature production on nursing competences from 1981 till 2012: A bibliometric snapshot. Nurse Education Today, 35(5), 673–679. 10.1016/j.nedt.2015.01.002 [DOI] [PubMed] [Google Scholar]
- Bradshaw, A. (2001). Competence and British nursing: A view from history. Journal of Clinical Nursing, 9(3), 321–329. 10.1046/j.1365-2702.2000.00399.x [DOI] [PubMed] [Google Scholar]
- Byrne, B. M. (2013). Structural equation modeling with Mplus: Basic concepts, applications, and programming. Routledge. 10.4324/9780203807644 [DOI] [Google Scholar]
- Cheng, F. , Meng, A. , & Jin, T. (2015). Correlation between burnout and professional value in Chinese oncology nurses: A questionnaire survey. International Journal of Nursing Sciences, 2(2), 153–157. 10.1016/j.ijnss.2015.04.004 [DOI] [Google Scholar]
- Dall'Ora, C. , Ball, J. , Reinius, M. , & Griffiths, P. (2020). Burnout in nursing: A theoretical review. Human Resources for Health, 18(1), 41. 10.1186/s12960-020-00469-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Cordova, P. B. , Johansen, M. L. , Grafova, I. B. , Crincoli, S. , Prado, J. , & Pogorzelska‐Maziarz, M. (2022). Burnout and intent to leave during COVID‐19: A cross‐sectional study of New Jersey hospital nurses. Journal of Nursing Management, 1–9. 10.1111/jonm.13647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Falatah, R. , & Alhalal, E. (2022). A structural equation model analysis of the association between work‐related stress, burnout and job‐related affective well‐being among nurses in Saudi Arabia during the COVID‐19 pandemic. Journal of Nursing Management, 30(4), 892–900. 10.1111/jonm.13587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faraji, A. , Karimi, M. , Azizi, S. M. , Janatolmakan, M. , & Khatony, A. (2019). Evaluation of clinical competence and its related factors among ICU nurses in Kermanshah‐Iran: A cross‐sectional study. International Journal of Nursing Sciences, 6(4), 421–425. 10.1016/j.ijnss.2019.09.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernandez, R. , Lord, H. , Halcomb, E. , Moxham, L. , Middleton, R. , Alananzeh, I. , & Ellwood, L. (2020). Implications for COVID‐19: A systematic review of nurses' experiences of working in acute care hospital settings during a respiratory pandemic. International Journal of Nursing Studies, 111, 103637. 10.1016/j.ijnurstu.2020.103637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fukada, M. (2018). Nursing competency: Definition, structure and development. Yonago Acta Medica, 61(1), 001–007. 10.33160/yam.2018.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galanis, P. , Vraka, I. , Fragkou, D. , Bilali, A. , & Kaitelidou, D. (2021). Nurses' burnout and associated risk factors during the COVID‐19 pandemic: A systematic review and meta‐analysis. Journal of Advanced Nursing, 77(8), 3286–3302. 10.1111/jan.14839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghassemi A. E. (2021). Burnout in nurses during the COVID‐19 pandemic: The rising need for development of evidence‐based risk assessment and supportive interventions. Evidence‐based nursing, ebnurs‐2021‐103438. Advance online publication. 10.1136/ebnurs-2021-103438 [DOI] [PubMed]
- Grande, R. A. N. , Berdida, D. J. E. , Paulino, R. R. J. C. , Anies, E. A. , Ebol, R. R. T. , & Molina, R. R. (2021). The multidimensionality of anxiety among nursing students during COVID‐19 pandemic: A cross‐sectional study. Nursing Forum, 57(2), 267–276. 10.1111/nuf.12675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hair, J. F. , Sarstedt, M. , Hopkins, L. , & Kuppelwieser, G. V. (2014). Partial least squares structural equation modeling (PLS‐SEM): An emerging tool in business research. European Business Review, 26(2), 106–121. 10.1108/EBR-10-2013-0128 [DOI] [Google Scholar]
- Halabi, J. O. , Nilsson, J. , & Lepp, M. (2021). Professional competence among registered nurses working in hospitals in Saudi Arabia and their experiences of quality of nursing care and patient safety. Journal of Transcultural Nursing, 32(4), 425–433. 10.1177/1043659621992845 [DOI] [PubMed] [Google Scholar]
- Heydari, A. , Kareshki, H. , & Armat, M. R. (2016). Is nurses' professional competence related to their personality and emotional intelligence? A cross‐sectional study. Journal of Caring Science, 5(2), 121–132. 10.15171/jcs.2016.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, P.‐H. , Chen, H. , & Weng, L.‐J. (2017). A penalized likelihood method for structural equation modeling. Psychometrika, 82, 329–354. 10.1007/s11336-017-9566-9 [DOI] [PubMed] [Google Scholar]
- Immonen, K. , Oikarainen, A. , Tomietto, M. , Kääriäinen, M. , Tuomikoski, A. M. , Kaučič, B. M. , Filej, B. , Riklikiene, O. , Vizcaya‐Morena, M. , Perez‐Cañaveras, R. M. , De Raeve, P. , & Mikkonen, K. (2019). Assessment of nursing students' competence in clinical practice: A systematic review of reviews. International Journal of Nursing Studies, 100, 103414. 10.1016/j.ijnurstu.2019.103414 [DOI] [PubMed] [Google Scholar]
- International Council of Nurses . (2021). The ICN code of ethics. Switzerland. Retrieved from. https://www.icn.ch/system/files/2021-10/ICN_Code-of-Ethics_EN_Web_0.pdf [Google Scholar]
- Jang, Y. , You, M. , Lee, H. , Lee, M. , Lee, Y. , Han, J.‐O. , & Oh, J. H. (2021). Burnout and peritraumatic distress of healthcare workers in the COVID‐19 pandemic. BMC Public Health, 21(1), 2075. 10.1186/s12889-021-11978-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jiang, H. , Huang, N. , Jiang, X. , Yu, J. , Zhou, Y. , & Pu, H. (2021). Factors related to job burnout among older nurses in Guizhou province, China. PeerJ, 9, e12333. 10.7717/peerj.12333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jose, S. , Dhandapani, M. , & Cyriac, M. C. (2020). Burnout and resilience among frontline nurses during COVID‐19 pandemic: A cross‐sectional study in the emergency department of a tertiary care center, North India. Indian Journal of Critical Care Medicine, 24(11), 1081–1088. 10.5005/jp-journals-10071-23667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kakemam, E. , Chegini, Z. , Rouhi, A. , Ahmadi, F. , & Majidi, S. (2021). Burnout and its relationship to self‐reported quality of patient care and adverse events during COVID‐19: A cross‐sectional online survey among nurses. Journal of Nursing Management, 29(7), 1974–1982. 10.1111/jonm.13359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karami, A. , Farokhzadian, J. , & Foroughameri, G. (2017). Nurses' professional competency and organizational commitment: Is it important for human resource management? PLoS ONE, 12(11), e0187863. 10.1371/journal.pone.0187863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan, Y. , Bruyneel, A. , & Smith, P. (2022). Determinants of the risk of burnout among nurses during the first wave of the COVID‐19 pandemic in Belgium: A cross‐sectional study. Journal of Nursing Management, 30, 1–11. 10.1111/jonm.13624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khodaveisi, M. , Oshvandi, K. , Bashirian, S. , Khazaei, S. , Gillespie, M. , Masoumi, S. Z. , & Mohammadi, F. (2021). Moral courage, moral sensitivity and safe nursing care in nurses caring of patients with COVID‐19. Nursing Open, 8(6), 3538–3546. 10.1002/nop2.903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kishi, H. , Watanabe, K. , Nakamura, S. , Taguchi, H. , & Narimatsu, H. (2022). Impact of nurses' roles and burden on burnout during the COVID‐19 pandemic: Multicentre cross‐sectional survey. Journal of Nursing Management, 1–9. 10.1111/jonm.13648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline, R. B. (2015). Principles and practice of structural equation modeling. Guilford publications. [Google Scholar]
- Lim, S. , Song, Y. , Nam, Y. , Lee, Y. , & Kim, D. (2022). Moderating effect of burnout on the relationship between self‐efficacy and job performance among psychiatric nurses for COVID‐19 in national hospitals. Medicina, 58(2), 171. 10.3390/medicina58020171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma, Y. , Faraz, N. A. , Ahmed, F. , Iqbal, M. K. , Saeed, U. , Mughal, M. F. , & Raza, A. (2021). Curbing nurses' burnout during COVID‐19: The roles of servant leadership and psychological safety. Journal of Nursing Management, 29(8), 2383–2391. 10.1111/jonm.13414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maslach, C. , Leiter, M. , & Schaufeli, W. (2008). Measuring burnout. In Cartwright S. & Cooper C. L. (Eds.), The Oxford handbook of organizational well‐being. Oxford University Press. 10.1093/oxfordhb/9780199211913.003.0005 [DOI] [Google Scholar]
- Maslach, C. , & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. 10.1002/wps.20311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matsutani, M. , Sakyo, Y. , Oku, H. , Hori, N. , Takaya, T. , & Miura, Y. (2012). New baccalaureate nursing graduates' perceptions of required nursing competency: An analysis of interview data from nurses in their first year of work. Seiroka Kango Gakkaishi, 16, 9–19. [Google Scholar]
- Meretoja, R. , Isoaho, H. , & Leino‐Kilpi, H. (2004). Nurse competence scale: Development and psychometric testing. Journal of Advanced Nursing, 47(2), 124–133. 10.1111/j.1365-2648.2004.03071.x [DOI] [PubMed] [Google Scholar]
- Mlambo, M. , Silén, C. , & McGrath, C. (2021). Lifelong learning and nurses' continuing professional development, a metasynthesis of the literature. BMC Nursing, 20(1), 62. 10.1186/s12912-021-00579-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mudallal, R. H. , Othman, W. M. , & Al Hassan, N. F. (2017). Nurses' burnout: The influence of leader empowering behaviors, work conditions, and demographic traits. Inquiry : A Journal of Medical Care Organization, Provision and Financing, 54, 0046958017724944. 10.1177/0046958017724944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mukherjee, S. , Tennant, A. , & Beresford, B. (2020). Measuring burnout in pediatric oncology staff: Should we be using the Maslach Burnout Inventory? Journal of Pediatric Oncology Nursing, 37(1), 55–64. 10.1177/1043454219873638 [DOI] [PubMed] [Google Scholar]
- Nilsson, J. , Engström, M. , Florin, J. , Gardulf, A. , & Carlsson, M. (2018). A short version of the nurse professional competence scale for measuring nurses' self‐reported competence. Nurse Education Today, 71, 233–239. 10.1016/j.nedt.2018.09.028 [DOI] [PubMed] [Google Scholar]
- Oldland, E. , Botti, M. , Hutchinson, A. M. , & Redley, B. (2020). A framework of nurses' responsibilities for quality healthcare — Exploration of content validity. Collegian, 27(2), 150–163. 10.1016/j.colegn.2019.07.007 [DOI] [Google Scholar]
- Polit, D. F. , & Beck, C. T. (2017). Nursing research: Generating and assessing evidence for nursing practice (10th ed.). Wolters Kluwer Health. [Google Scholar]
- Poreddi, V. , Narayanan, A. , Thankachan, A. , Joy, B. , Awungshi, C. , & Reddy, S. S. (2021). Professional and ethical values in nursing practice: An Indian perspective. Investigacion Y Educacion en Enfermeria, 39(2), e12. 10.17533/udea.iee.v39n2e12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price, B. (2015). Understanding attitudes and their effects on nursing practice. Nursing Standard, 30(15), 50–60. 10.7748/ns.30.15.50.s51 [DOI] [PubMed] [Google Scholar]
- Prosen, M. , Kvas, A. , Bošković, S. , & Ličen, S. (2021). Cross‐cultural adaptation and psychometric evaluation of the Slovenian version of the nurse professional competence scale. BMC Nursing, 20(1), 142. 10.1186/s12912-021-00664-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pueyo‐Garrigues, M. , Pardavila‐Belio, M. I. , Canga‐Armayor, A. , Esandi, N. , Alfaro‐Díaz, C. , & Canga‐Armayor, N. (2022). Nurses' knowledge, skills and personal attributes for providing competent health education practice, and its influencing factors: A cross‐sectional study. Nurse Education in Practice, 58, 103277. 10.1016/j.nepr.2021.103277 [DOI] [PubMed] [Google Scholar]
- Ruiz‐Fernández, M. D. , Ramos‐Pichardo, J. D. , Ibáñez‐Masero, O. , Carmona‐Rega, M. I. , Sánchez‐Ruiz, M. J. , & Ortega‐Galán, Á. M. (2021). Professional quality of life, self‐compassion, resilience, and empathy in healthcare professionals during COVID‐19 crisis in Spain. Research in Nursing & Health, 44(4), 620–632. 10.1002/nur.22158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt, B. J. , & McArthur, E. C. (2018). Professional nursing values: A concept analysis. Nursing Forum, 53(1), 69–75. 10.1111/nuf.12211 [DOI] [PubMed] [Google Scholar]
- Sikaras, C. , Ilias, I. , Tselebis, A. , Pachi, A. , Zyga, S. , Tsironi, M. , Gil, A. P. R. , & Panagiotou, A. (2022). Nursing staff fatigue and burnout during the COVID‐19 pandemic in Greece. AIMS Public Health, 9(1), 94–105. 10.3934/publichealth.2022008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skela‐Savič, B. , Hvalič‐Touzery, S. , & Pesjak, K. (2017). Professional values and competencies as explanatory factors for the use of evidence‐based practice in nursing. Journal of Advanced Nursing, 73(8), 1910–1923. 10.1111/jan.13280 [DOI] [PubMed] [Google Scholar]
- Sklar, M. , Ehrhart, M. G. , & Aarons, G. A. (2021). COVID‐related work changes, burnout, and turnover intentions in mental health providers: A moderated mediation analysis. Psychiatric Rehabilitation Journal, 44(3), 219–228. 10.1037/prj0000480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun, N. , Wei, L. , Shi, S. , Jiao, D. , Song, R. , Ma, L. , Wang, H. , Wang, C. , Wang, Z. , You, Y. , Liu, S. , & Wang, H. (2020). A qualitative study on the psychological experience of caregivers of COVID‐19 patients. American Journal of Infection Control, 48(6), 592–598. 10.1016/j.ajic.2020.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taber, K. S. (2018). The use of Cronbach's alpha when developing and reporting research instruments in science education. Research in Science Education, 48(6), 1273–1296. 10.1007/s11165-016-9602-2 [DOI] [Google Scholar]
- Uchmanowicz, I. , Kubielas, G. , Serzysko, B. , Kołcz, A. , Gurowiec, P. , & Kolarczyk, E. (2021). Rationing of nursing care and professional burnout among nurses working in cardiovascular settings. Frontiers in Psychology, 12, 726318. 10.3389/fpsyg.2021.72631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valizadeh, L. , Zamanzadeh, V. , Eskandari, M. , & Alizadeh, S. (2019). Professional competence in nursing: A hybrid concept analysis. Medical‐Surgical Nursing Journal, 8(2), 1–8. 10.5812/msnj.90580 [DOI] [Google Scholar]
- van Montfort, K. , Oud, J. H. L. , & Voelkle, M. C. (2018). Continuous time modeling in the behavioral and related sciences. Springer. 10.1007/978-3-319-77219-6 [DOI] [Google Scholar]
- Weis, D. , & Schank, M. J. (2009). Development and psychometric evaluation of the nurses professional values scale‐revised. Journal of Nursing Measurement, 17(3), 221–231. 10.1891/1061-3749.17.3.221 [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2019). Burn‐out an "occupational phenomenon": International Classification of Diseases. Accessed from: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases
- Yang, J. Y. , Wang, J. D. , Zhang, Y. F. , Cheng, W. J. , & Li, L. (2021). A heuristic sampling method for maintaining the probability distribution. Journal of Computer Science and Technology, 36(4), 896–909. 10.1007/s11390-020-0065-6 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. STROBE Statement—Checklist of items that should be included in reports of cross‐sectional studies
Table S1. Correlation Coefficients among the Dimensions of Professional Competence, Dimensions of Nurse Professional Values, Burnout, and Nurse Competence (n = 809)
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.