

Abstract
Engaging in leisure activities promotes mental health. The effect is likely associated with resilience as the broaden‐and‐build theory suggests positive emotions elicited from leisure increase mental resources for stress coping. The present research examined whether participating in different leisure activities at a given time increases the level of resilience, which in turn reduces psychological problems. It also investigated the changes in people's leisure activities due to the COVID‐19 outbreak and the impact of these changes on their mental health. Japanese participants (N = 300) responded to two online surveys conducted before (January 2020) and after the outbreak (February 2021). They selected the leisure activities they had engaged in from 100 choices and reported their levels of resilience and depressive symptoms. An analysis of covariates revealed that the total number of selected activities significantly reduced in the second survey, but the levels of resilience and depressive symptoms remained constant. Regression analysis showed that the reduction in leisure activities did not predict depressive symptoms. However, structural equation modeling established that the relationship between leisure and depression was mediated by resilience, supporting the initial hypothesis. Importantly, this relationship slightly differed by age group, likely because popular activities and their psychological impacts vary depending on age.
Keywords: COVID‐19, leisure activities, mental health, resilience
INTRODUCTION
Leisure activities play an essential role in maintaining good mental health (Verghese et al., 2006). Leisure is defined as activities that people perform when they are free from the obligations imposed by their occupation, family, or society; thus, essential activities for a living, such as sleeping, working, and housework, are not included. The purpose of leisure activities is diverse, such as relaxing, enjoying, acquiring skills, and contributing to society (Kleiber & Nimrod, 2009). Engaging in leisure activities is likely to mitigate the negative effects of stressful experiences that threaten physical and psychological health (Iwasaki et al., 2005; Lawton et al., 2002). Several studies have shown that participating in a variety of leisure activities at a given time promotes subjective well‐being (e.g. Cummings, 2002). Moreover, a higher level of leisure engagement predicts greater life satisfaction in the next few years (Menec & Chipperfield, 1997). Leisure activities are likely to work as a buffer against stressful experiences by promoting positive emotions related to self‐fulfillment and well‐being. Consequently, they work to prevent mental illnesses, such as depression.
The mechanism of the preventive effect of leisure activities on mental illness may relate to the psychological construct of resilience. Resilience is a part of cognitive functioning that encompasses stress‐coping dynamics such as adaptation to challenging life events and adversarial situations (Nishi et al., 2010; Richardson, 2002). The definition of resilience is somewhat confusing, and literature often takes either of the two separate views, focusing on a trait‐level adaptation or a state‐level adaptation. Recently, however, Kuldas and Foody (2021) have disagreed with the trait–state dualism and suggested that resilience is a transactional or dynamic process brought by interactions between intrapersonal, interpersonal, and risk characteristics surrounding individuals. Nevertheless, a high level of resilience enables people to employ effective coping skills, promoting receptive attitudes, enhancing positive ruminations, and encouraging behavior planning that improves mental health (Kleiber et al., 2002). The direct impact of resilience on various mental disorders has been well established (Alim et al., 2008). Even severe depressive symptoms caused by extremely stressful events can be weakened by the function of resilience (Wingo et al., 2010). Leisure activities influence individuals' intrapersonal aspects (e.g. acquiring skills and becoming physically fitter) as well as interpersonal aspects (e.g. making friends); thus, they have a great potential to enhance resilience and contribute to better mental health.
Research has found that leisure activities can immediately improve subjective well‐being by eliciting positive emotions, which leads to effective stress‐coping strategies in the long term (Iwasaki, 2006). Denovan and Macaskill (2017) explained how leisure activities enhance resilience using the broaden‐and‐build theory (Fredrickson, 2001), which suggests that experiences of positive emotions enrich the quality of one's thoughts and action plans, which in turn provide personal resources to enhance coping strategies. Increased resilience then promotes subjective well‐being and coping strategies for forthcoming stressful situations (Reschly et al., 2008). The present research investigated the relationship between leisure activities, resilience, and mental health.
The research also focused on the impact of age on those variables. Generally, preferred leisure activities shift according to life stages (Janke et al., 2010; Sivan & Siu, 2021). In addition, commitments to certain activities, such as outdoor sports, shopping, and traveling, often decrease with age due to restrictions in physical mobility (Strain et al., 2002). Such a decrease in leisure for older people may have a negative impact on their resilience.
THE IMPACT OF COVID‐19 ON LEISURE ACTIVITIES AND MENTAL HEALTH
COVID‐19 has brought significant changes to our lifestyles, including leisure (e.g. Gammon & Ramshaw, 2021), marked by the huge decline in traveling and group activities. At the same time, engagement in activities at home, in open areas, or in private spaces (e.g. driving) has increased. Participation in private physical activities (e.g. walking, jogging, and weight training) has shown a similar trend. This indicates that the pandemic has brought a dynamic change to people's leisure activities rather than simply preventing them.
However, the overall impact of COVID‐19 on mental health is undoubtedly negative. The increased prevalence of psychiatric disorders has been reported worldwide (e.g. Czeisler et al., 2020; Wang et al., 2020). Therefore, it is important to address mental health issues within the context of the pandemic. The present research aimed to investigate the relationship between leisure activities and mental health and how it is affected by the pandemic. The mechanism of the negative impact of the pandemic on mental health is likely to involve heightened anxiety about the disease and increased loneliness due to isolation resulting from social distancing measures (Keller et al., 2022). Leisure participation provides people with opportunities to interact with each other. So changes in leisure may directly relate to people's quality of social interactions, which could affect mental health negatively.
This study targeted people living in Japan. Japanese have shown similar lifestyle changes to people in other countries, noted by the reduction in interpersonal contacts and traveling (Parady et al., 2020). The mental health deterioration among Japanese is also reported (e.g. Kikuchi et al., 2020). However, the impact of the pandemic on leisure and mental health can still vary across countries due to variations in governmental prevention measures (Japanese measure is, e.g., notably unrestrictive) and culture. Only a few Japanese studies on leisure activities and the pandemic have been published. Longitudinal studies directly comparing the situation before and after the spread of COVID‐19 are especially scarce. Thus, the present study attempted to fill the gaps in this research topic. It also investigated whether the impact of the pandemic was variable depending on age.
Study objectives
One difficulty in leisure research is to decide which aspect of leisure to focus on (e.g. activity types or frequency of engagement). Regarding mental illnesses, leisure activities affect them positively, but the responsive aspect is not fully determined. Frequently focused aspect is the activity types, and the impacts of physical exercises (e.g. aerobic and strength training) are often investigated. It is reported that the physical aspect of leisure significantly reduces depressive symptoms (Paluska & Schwenk, 2000). Instead of the activity types, the present research focused on the variations of activities that individuals performed in a given period. It is because diversity in daily activities should be related to resilience building. Because resilience is strongly associated with flexible thinking and multiple perspectives (Waugh et al., 2008), people with more diverse experiences would build resilience more efficiently than those with less diverse experiences. Thus, it is expected that people who engage in various leisure activities at a given time will have higher levels of resilience than those who participate in less diverse activities. Those with high resilience are also expected to withstand the psychological difficulties caused by COVID‐19.
This study investigated the change in leisure activities using a survey conducted twice with the same sample: The first one was in January 2020, just before the start of the pandemic, and the second one was conducted a year later. Japanese nationals aged between 20 to over 70 were asked to select activities they had engaged in and indicate the duration and frequency of the engagement. A total of 100 activities were presented. The participants' levels of resilience and depressive symptoms were also measured. It was hypothesised that (1) the number of leisure activities participated at a time is related to the level of resilience and depressive symptoms, (2) changes in leisure participation due to the pandemic are associated with changes in mental health among people, and (3) participants with the higher level of resilience before pandemic (thus participated in larger number of leisure activities) tend to have less severe depressive symptoms during the pandemic.
METHOD
Participants and procedure
The survey was conducted online through a research company, which recruited registered members to participate in this study and reimbursed them. The survey took place twice (January 2020 and February 2021). The target number of participants for the first survey was 1200, consisting of 200 people in each of the following six age groups: 20s, 30s, 40s, 50s, 60s, and 70s or above. The number of men and women in each group was equal. The research company continued to recruit participants until the target number of responses was collected (the refusal/incomplete response rate was not disclosed to the authors). The samples were randomly chosen from all areas of Japan. The main analyses were planned to be performed by dividing participants into three age groups (young: 20–39, middle: 40–59, and older: 60–89), and a sample calculation revealed that approximately 300 participants were required (see Section 3.3). It was aimed to obtain twice as many participants as the requirement. So the target number of participants was set to 1200 with an expected dropout rate of 50 per cent. Unfortunately, the second survey yielded a much higher dropout rate, and only 300 participants responded (164 men and 136 women; mean age = 53.5, SD = 15.15). The characteristics of the 1200 respondents and a comparison of the first and second samples are reported in Supplemental S1. It was shown that the second survey sample was a fairly unbiased subset of the initial 1200 respondents.
In both surveys, the participants were asked to select the leisure activities they had engaged in. They also reported the total duration of engagement and frequency of engagement for each activity they chose. Similar questions were asked about daily activities, such as housework. Finally, the levels of resilience and depressive symptoms were assessed. The procedure of the second survey was identical to the first. All participants provided informed consent. The surveys were conducted anonymously, and participants were allowed to withdraw at any time. This study met the ethical guidelines of Kanazawa University.
Measures
Leisure activities
A hundred leisure activities (e.g. watching movies, reading, and playing golf) were listed for participants to select from (see Supplemental S2). These were taken from previous Japanese research targeting a wide range of age groups (Iwasa & Yoshida, 2018; Iwasa et al., 2019; Kozono et al., 2016) as well as from an official survey on leisure activities created by Japanese government. Participants could write down activities that were not included in the list. For each of the selected activities, participants reported the total number of years (in units of 0.5 years) that they had regularly performed it. The frequency of commitments was also measured using a 5‐point scale (1 = a few times a year to 5 = almost every day).
Mental health
Levels of resilience and depressive symptoms were measured as indicators of mental health. A Japanese version of the Resilience Scale (Nishi et al., 2010) was used. It has 25 items measuring the key components of resilience, such as determination and perseverance (e.g. “Manage one way or other”) and adaptability to adversity (e.g. “I do not dwell on things”). These items were rated on a 7‐point scale (1 = not at all agree to 7 = strongly agree). This scale's interitem reliability (Cronbach's alpha) is reported to be .90 (Nishi et al., 2010). The extent of depressive symptoms was measured using the two‐item Patient Health Questionnaire (PHQ‐2; Kroenke et al., 2003). It is often used for screening and is derived from the original nine‐item version (PHQ‐9). The PHQ‐2 asks about the presence of anhedonia and depressed mood within the last 2 weeks, using a 4‐point scale (0 = not at all to 3 = nearly every day). The Japanese version has been confirmed reliable and valid (Inagaki et al., 2013). Cronbach's alpha for this scale is reported to be .76 (Yu et al., 2011). The total score of the two questions being three or higher indicates depressive disorder. The Cronbach's alpha values in the present study was as follows: resilience at first survey = .96, second = .97; PHQ at first = .85, second = .90. These were similar to the aforementioned values in the past studies.
Other variables
Participants' demographic information included age, gender, years of education, employment status, and having children/grandchildren or not. For employment, participants were first asked to choose their status from “I am currently working,” “I have worked in the past, but not now,” and “I have never worked.” Next, the total number of jobs held and years in employment were reported. A summary of these characteristics is presented in Table 1. In addition, participants were asked to choose the daily activities they engaged in from nine choices (e.g. laundry, cooking, and cleaning) and the electronic devices they usually used. The items for electronic devices were smartphones, tablets, and PCs. The rating scales for these activities were identical to those for leisure activities. The daily activities and device usage were asked to see whether they were related to participants' leisure activities. For example, more daily activities are associated with fewer leisure activities.
TABLE 1.
A summary of demographics, the mean number of selected activities, and mean mental health scores for the participants in the three age groups
| Young (20–39 years) | Middle (40–59 years) | Older (60–89 years) | |
|---|---|---|---|
| Sample characteristics | |||
| Number of participant (% men) | 65 (54.3%) | 113 (54.9%) | 122 (55.1%) |
| Mean age (SD) | 30.9 (5.38) | 50.9 (5.44) | 67.9 (5.77) |
| Years of education (SD) | 15.2 (2.55) | 14.6 (2.55) | 14.5 (2.99) |
| Number of being employed | 56 (96.2%) | 87 (77.0%) | 41 (33.6%) |
| Number of having children/grandchildren | 19 (29.2%) | 58 (51.3%) | 91 (74.6%) |
| Mean (SD) number of selected activities and mean mental health scores | |||
| Leisure activity (range 0–98) | |||
| First survey | 31.80 (21.16) | 26.55 (20.36) | 25.03 (17.97) |
| Second survey | 9.78 (7.35) | 8.27 (7.26) | 8.60 (6.87) |
| Daily activity (range 0–9) | |||
| First survey | 3.75 (2.94) | 3.83 (3.20) | 4.07 (2.98) |
| Second survey | 2.23 (2.40) | 2.58 (2.40) | 2.92 (2.34) |
| Electronic devices (range 0–3) | |||
| First survey | 1.77 (1.14) | 1.53 (1.12) | 1.40 (1.00) |
| Second survey | 1.25 (1.08) | 1.25 (1.09) | 1.41 (0.93) |
| Resilience (range 25–175) | |||
| First survey | 101.75 (22.32) | 107.87 (21.33) | 117.61 (21.45) |
| Second survey | 104.71 (20.37) | 106.40 (21.95) | 117.21 (21.63) |
| PHQ‐2 (range 0–6) | |||
| First survey | 1.75 (1.53) | 1.25 (1.47) | 0.89 (1.09) |
| Second survey | 1.69 (1.56) | 1.40 (1.65) | 0.98 (1.33) |
Data analysis
The data from the 300 participants who answered both surveys were analyzed. Three primary analyses were conducted, using the demographic variables (gender, currently employed or not, years of education, and having children/grandchildren or not) as covariates. First, the number of selected leisure activities and mental health scores between the two surveys were compared while controlling the demographic variables by conducting analysis of covariance tests (ANCOVAs). Bonferroni multiple comparison tests were used for post hoc assessments. Second, a hierarchical multiple regression analysis was performed to examine whether a reduction in leisure activities (the number of selected activities in the first survey was subtracted from that in the second survey) and a lower level of resilience predict more severe depressive symptoms. This analysis was performed separately for each age group. For the regression model, the demographic variables and the resilience scores at the first survey were entered in Step 1. The change of leisure, daily activities, and device usage were entered in Step 2. The R 2 change from Step 1 to Step 2 was examined to see whether the change in leisure activities led to a better prediction of depression. A residual analysis (normality tests for the residuals) of the obtained model was performed to validate it. In order to verify the results of the multiple regression, a logistic regression analysis was performed with the same model after categorically converting the PHQ‐2 scores based on its clinical cutoff point (below or above the cutoff score of 3).
Finally, an exploratory model proposing that resilience has a mediating effect on the relationship between leisure activities and depressive symptoms was constructed. The model was tested using structural equation modeling (SEM), which draws possible causal relationships as direct paths between variables. The hypothesised model was evaluated using the root mean‐square error of approximation (RMSEA), goodness‐of‐fit index (GFI), and the comparative fit index (CFI). RMSEA below .05 and GFI and CFI above .95 were considered good fit (Hu & Bentler, 1999). Indirect effects were examined using a mediation analysis with the bias‐corrected bootstrap 95 per cent confidence intervals (CI) procedure (Hayes, 2017). SPSS ver. 25 was used for the ANCOVAs and multiple regression, while SEM was performed using Amos ver. 27.
For using the age variable in analyses, the present research divided participants into three groups (young: 20–39, middle: 40–59, and older: 60–89) rather than treating it as a continuous variable. The literature on leisure often describes that preferred leisure activities tend to change along with life stage development, such as getting married, having children, and getting career promotions (Akar et al., 2012; Havighurst & Feigenbaum, 1959). Although people of a similar age tend to experience similar life stage development, the time to experience specific life events still varies across individuals to a great extent. Thus, incorporating age groups into analyses would be more effective in capturing those lifestyle changes than treating age as a continuous variable. Therefore, the ANCOVAs, regression, and SEM analyses in the present research used the three age groups.
Before conducting the above analyses, the authors examined whether the sample size of 300 was enough using GPower software (Erdfelder et al., 1996). For the two‐way ANCOVA, the software calculated that 158 participants would be enough to observe a medium effect size (Cohen's d = .25, α = .05, power = .80). For the multiple regression analyses, 231 participants (77 participants in each of the three age groups 1 ) would be enough to observe a small to medium effect size (Cohen's d = .12, α = .05, power = .80), which is thought to be sufficient in psychology research (see Funder & Ozer, 2019).
RESULTS
The changes in leisure activities
Some participants mentioned five activities as not being included in the list of 100. Among the total of 105 leisure activities, those selected by fewer than three participants were removed from the following analyses for data clean‐up. Seven items were removed, leaving 98 leisure activities. Next, the total number of selected leisure activities for each participant was counted. The summary of the three age groups is reported in Table 1, along with the number of selected daily activities, electronic devices, and mean mental health scores. An ANCOVA was performed to examine whether the number of selected leisure activities changed between the two surveys and whether it differed by age. A within‐subject factor was the survey (first vs. second), and a between factor was the age group (young vs. middle vs. older). Participants' demographic variables (age, years of education, currently employed or not, and having children/grandchildren or not) were included as covariates. The partial eta‐squared values ( ) were reported as effect sizes, indicating the following: .01 to .06 = small, 07 to .14 = medium, above .14 = large.
Significant main effects of the survey, F(1, 293) = 5.234, p < .05, , and age, F(2, 293) = 3.805, p < .05, , were found, showing that fewer leisure activities were selected in the second survey and participants in the young group selected more activities than those in the older group. No difference was found between the middle and young or older groups. A two‐way interaction between survey and age was significant, F(2, 293) = 3.073, p < .05, . An examination of a simple main effect revealed that the difference between the young and older groups was present only in the first survey (p < .05). Similar ANCOVAs performed on the number of selected daily activities and device usage revealed no significant main effect of the survey, Fs < 1, ps > .05. An interaction between survey and age was found for electronic device usage, F(2, 293) = 4.62, p < .05, , revealing that fewer numbers of electronic devices were selected in the second survey than the first among the young (p < .001) and middle groups (p < .05). No other effect was found.
Next, the differences between the two surveys were analyzed by individual activities. The selection of the 1200 participants in the first survey was summarized in Supplemental S2. The comparison between the first and second surveys was summarized in Supplemental S3. In almost all activities, the number of participants who chose them reduced from the first to the second survey. When the frequency of performance, measured with a 5‐point scale, was compared across the two surveys using an independent sample t‐test, 93 out of 98 leisure activities were performed significantly less frequently at the time of the second survey. Finally, the proportion of people who quit or continued each activity throughout the 1‐year period was examined. The proportions of participants who selected each activity in both surveys, in the first survey only, and in the second survey only, were calculated. The result is reported in Supplemental S4. The most common response was to select the activity in the first survey but not in the second. However, there were some exceptions. Activities taking place indoors and performed solely (e.g. watching movies, knitting, and reading) were continued at the time of the second survey. Physical exercises performed alone (e.g. jogging, yoga, walking, and muscle training) were also continued. New activities participants started by the second survey were mostly home‐based activities (e.g. gardening, playing games, and studying).
The relationship between leisure activities and mental health
The summed scores for the resilience scale and PHQ‐2 were used in subsequent analyses. Their means and standard deviations across the two surveys are presented in Table 1. The ANCOVA on the selected number of leisure activities was performed on the resilience and PHQ‐2 scores separately. For the resilience score, the main effect of survey was absent, F(1, 293) = 0.12, p = .725, , but that of age group was present, F(2, 293) = 9.155, p < .001, . The older group showed higher resilience than the others (ps < .001). No difference was found between the young and middle groups. The main effect of survey was also absent from the analysis on the PHQ‐2, but the main effect of age group was significant, F(2, 293) = 3.436, p < .05, . The older adults reported lower depression scores than the young (p < .001). No difference was found between the older and middle groups (p > .05). No other effect was observed.
Looking into the people who exceeded the PHQ‐2 cutoff (the summed score of the two items is three or more), 12.0 per cent of participants in the first survey fell into the category of being clinically depressed, and the proportion increased to 16.3 per cent in the second survey. This change was statistically significant, χ 2 = 60.02, df = 1, p < .001, with a medium effect size (φ = .447). Those who exceeded the cutoff in the first survey were the greatest in the young group (n = 19, 29.2%), followed by the middle (n = 11, 9.7%) and the older groups (n = 6, 4.9%). However, in the second survey, the number remained constant for the young (n = 18, 27.7%), whereas a noticeable increase was observed for the middle (n = 18, 15.9%) and older groups (n = 13, 10.7%).
Next, the correlations between leisure activities and mental health were examined. The number of selected leisure activities at the first and the second surveys significantly correlated with resilience measured at the corresponding surveys (first, r(298) = .14; second, r(298) = .12, ps < .05), but not with the PHQ scores (first, r(298) = −.06; second, r(298) = .002). Also, a significant and moderate correlation emerged between the resilience and PHQ (first, r(298) = −.450; second, r(298) = −.395, ps < .01). Next, a hierarchical multiple regression was performed separately for each age group to investigate how reduced leisure variations affected depressive symptoms (measured with the PHQ‐2). The procedure is described in Section 3.3. The results are reported in Table 2. The R 2 change (ΔR 2) was nonsignificant for all groups, indicating that the reduction of activities alone cannot predict the severity of depression. However, the higher level of resilience was associated with lower depressive symptoms for all. When PHQ scores in the first survey were added to Step 1, the effect of resilience ceased to be significant for the young and middle groups (young: β = −.114, 95% CI [−0.023, 0.007], middle: β = −.041, 95% CI [−0.016, 0.010]), meaning that the impact of resilience is stronger for the older adults.
TABLE 2.
Results of the multiple regression analyses by three age groups
| Variables | Step 1 | Step 2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | p | 95% CI | ΔR 2 | B | SE | β | p | 95% CI | ΔR 2 | |
| Young | .188 * | .030 | ||||||||||
| Gender a | −0.008 | .369 | −.003 | .983 | [−0.747, 0.731] | −0.098 | .379 | −.032 | .797 | [−0.857, 0.661] | ||
| Employment status b | 0.604 | .551 | .135 | .277 | [−0.498, 1.707] | 0.936 | .608 | .209 | .129 | [−0.282, 2.154] | ||
| Children/grandchildren b | −0.847 | .417 | −.249 | .046 | [−1.681, −0.014] | −0.751 | .439 | −.221 | .092 | [−1.629, 0.128] | ||
| Years of education | −0.045 | .047 | −.114 | .345 | [−0.139, 0.049] | −0.049 | .048 | −.124 | .316 | [−0.145, 0.048] | ||
| Resilience | −0.022 | .008 | −.319 | .009 | [−0.039, −0.006] | −0.021 | .008 | −.297 | .017 | [−0.038, −0.004] | ||
| Leisure activity (1st–2nd) | −0.017 | .013 | −.199 | .210 | [−0.043, 0.010] | |||||||
| Daily activity (1st–2nd) | 0.106 | .086 | .201 | .224 | [−0.067, 0.279] | |||||||
| Electronic devices (1st–2nd) | −0.045 | .198 | −.034 | .820 | [−0.443, 0.352] | |||||||
| Middle | .114 * | .022 | ||||||||||
| Gender a | 0.376 | .318 | .114 | .240 | [−0.255, 1.006] | 0.345 | .320 | .104 | .283 | [−0.289, 0.978] | ||
| Employment status b | −0.325 | .377 | −.083 | .390 | [−1.072, 0.421] | −0.296 | .381 | −.076 | .440 | [−1.052, 0.460] | ||
| Children/grandchildren b | −0.426 | .304 | −.129 | .164 | [−1.028, 0.177] | −0.417 | .311 | −.127 | .184 | [−1.033, 0.200] | ||
| Years of education | −0.007 | .020 | −.034 | .714 | [−0.047, 0.032] | −0.007 | .021 | −.033 | .732 | [−0.048, 0.034] | ||
| Resilience | −0.021 | .007 | −.276 | .003 | [−0.035, −0.007] | −0.025 | .007 | −.318 | .001 | [−0.039, −0.010] | ||
| Leisure activity (1st–2nd) | 0.017 | .012 | .189 | .144 | [−0.006, 0.040] | |||||||
| Daily activity (1st–2nd) | −0.031 | .076 | −.060 | .680 | [−0.182, 0.119] | |||||||
| Electronic devices (1st–2nd) | −0.070 | .156 | −.052 | .656 | [−0.379, 0.239] | |||||||
| Older | .198 ** | .009 | ||||||||||
| Gender a | 0.123 | .232 | .046 | .596 | [−0.336, 0.582] | 0.128 | .234 | .048 | .586 | [−0.336, 0.592] | ||
| Employment status b | −0.146 | .241 | −.052 | .546 | [−0.624, 0.332] | −0.125 | .245 | −.045 | .611 | [−0.611, 0.361] | ||
| Children/grandchildren b | −0.003 | .256 | −.001 | .992 | [−0.509, 0.504] | −0.007 | .264 | −.002 | .979 | [−0.529, 0.515] | ||
| Years of education | 0.008 | .012 | .054 | .534 | [−0.016, 0.031] | 0.007 | .012 | .053 | .542 | [−0.017, 0.032] | ||
| Resilience | −0.028 | .005 | −.450 | .000 | [−0.038, −0.017] | −0.027 | .005 | −.442 | .000 | [−0.038, −0.017] | ||
| Leisure activity (1st–2nd) | −0.010 | .009 | −.118 | .289 | [−0.028, 0.008] | |||||||
| Daily activity (1st–2nd) | 0.038 | .056 | .082 | .499 | [−0.073, 0.150] | |||||||
| Electronic devices (1st–2nd) | 0.036 | .124 | .027 | .774 | [−0.210, 0.281] | |||||||
0 = men, 1 = women.
0 = absent, 1 = present.
p < .05.
p < .01.
p < .10.
A residual analysis (normality tests for the residuals) for the obtained model was performed to assess its validity. The result revealed a nonnormal distribution of the residuals of this model. It was most likely due to the strongly skewed PHQ‐2 responses. So their distribution was adjusted using logarithmic transformations, and the residual analysis was performed again, but this did not alter the residual distribution. Thus, logistic regression was performed, and the results showed a consistent pattern with the original regression for the young and older group; the reduction in leisure activities, daily activities, and use of electronic devices were not significant predictors of depression. The reduction in activities was somewhat associated with depression in the middle group (Wald = 4.196, p < .05, 95% CI [1.003, 1.124]), but this relationship disappeared when the PHQ in the first survey was included in the model.
The indirect effects of resilience
The previous correlation analyses showed that the number of selected leisure activities was not directly associated with the extent of depressive symptoms but directly related to resilience. Therefore, resilience may mediate the relationship between leisure activities and depression. The absence of a direct relationship between activity reduction and depression in the regression analyses also supports this account. To test this hypothesis, a longitudinal design model was developed in which resilience mediates the relationship between leisure activities and depression symptoms (see Figure 1). The demographic variables were included as control variables. The number of daily activities and electronic devices were omitted because the model fitness was substantially reduced when they were included due to their strong correlation with the leisure activities. The analyses were performed with all participants first, followed by separate analyses for the three age groups.
FIGURE 1.
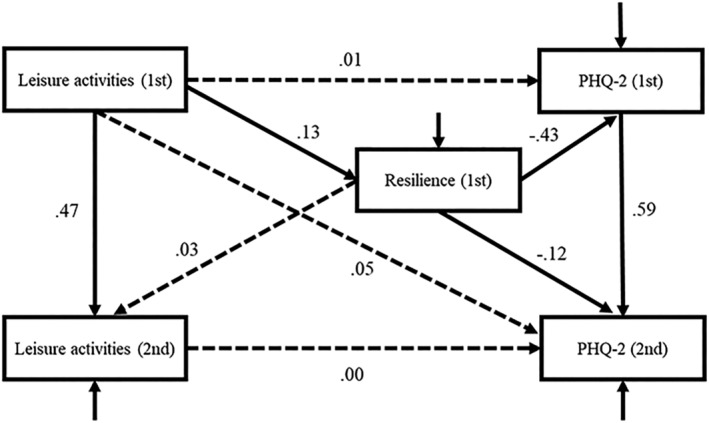
Path analysis examining the mediating role of resilience on depression symptoms (N = 300). Note: Covariates are gender, currently employed or not, having children/grandchildren, and years of education at the first survey. All paths from these covariates to dependent variables are omitted for visual clarity. The solid black lines indicate significant paths, and the dashed lines indicate nonsignificant paths. The reported values are β.
The goodness‐of‐fit indices of the model with all participants were reasonable, χ 2(13) = 20.60, p = .081, GFI = .99, CFI = .98, RMSEA = .04. As shown in Figure 1, the leisure activities at both surveys had no direct effect on either of the PHQ scores, but resilience at first survey had significant effects on both PHQs. A mediation analysis revealed that the first leisure activity indirectly related to second PHQ score (mediated by resilience, indirect effect = −.001, 95% CI = −0.003 to 0.000; mediated by resilience and PHQ in first survey, indirect effect = −.003, 95% CI = −0.005 to −0.001). This model was superior to other models with reversed variable positions and path directions. Because this study was a longitudinal design, leisure activities, resilience, and depression scores had two measurements each. The level of fit for the alternative models using all these measurements was assessed by adding the cross‐lagged paths or synchronous paths to the model. None of those models showed a better fit than the hypothesised model.
Next, the hypothesised model was assessed by the age groups. The fit indices for the young group were good (χ 2(13) = 15.46, p > .05, GFI = .95, CFI = .96, RMSEA = .05), and those for the middle age group were acceptable (χ 2(13) = 13.27, p > .05, GFI = .98, CFI = .99, RMSEA = .01). Both models showed almost identical paths to the overall model except one. In the young‐ and middle‐group model, the first resilience did not have a direct effect on the second PHQ. The path from the first resilience to the first PHQ was significant for both models (young, β = −.342, p < .01; middle, β = −.342, p < .01). The leisure activity in the first survey indirectly related to second PHQ score for both groups (young, indirect effect = −.003, 95% CI = −0.011 to 0.000; middle, indirect effect = −.006, 95% CI = −0.014 to −0.002). The model also fitted adequately to the older group (χ 2(13) = 14.95, p > .05, GFI = .97, CFI = .98, RMSEA = .04). The significant paths were identical to the overall model except the one between the leisure activity at the first survey and the first resilience score, which was not significant in the older model. In this model, the first resilience score had direct impacts on both PHQs (first: β = −.436, p < .001, second: β = −.186, p < .05), but no indication that resilience is heightened by leisure activities. Thus, the mediating effect of resilience was not supported for the older group.
DISCUSSION
This study investigated the relationship between leisure activity and mental health, as well as how it was influenced by COVID‐19. The hypotheses were that (1) the number of leisure activities participated at a time is related to the level of resilience and depressive symptoms, (2) changes in leisure participation due to the pandemic are associated with changes in mental health among people, and (3) participants with the higher level of resilience before pandemic (thus participated in larger number of leisure activities) tend to have less severe depressive symptoms during the pandemic.
Over the course of 1 year during the pandemic, the number of leisure activities people engaged in decreased regardless of age. The nonstrict policy for COVID‐19 prevention in Japan did not stop people from restricting their leisure activities. At the same time, however, the current data found some evidence for people being keen to find new activities to replace the ones they had to give up, which is consistent with other international studies (e.g. Balanzá‐Martínez et al., 2020).
Although the activity reduction was noticeable, the results of regression analyses showed that the reduction of activities alone could not predict the increase in depressive symptoms. Instead, the direct effect of resilience on depressive symptoms was robust across generations, which is consistent with previous studies (Alim et al., 2008). Importantly, the model that resilience mediated the relationship between leisure activity and depression symptoms was confirmed, suggesting that performing a wide variety of leisure activities in a given time is related to a higher level of resilience, which likely to contribute to reducing the current and future depressive symptoms. It might be the case that highly resilient people have actively looked for alternative activities to substitute the ones they had to give up. The present study focused only on the number of engaged activities, which showed a simple reduction after the COVID‐19 outbreak. However, if alternative activities are good and satisfactory, they might make up for the reduction of the total number in terms of people's resilience building and subjective well‐being. A qualitative investigation of how people alter their leisure activities and how they feel about it may be useful to reveal the leisure‐related coping strategies taken by people with high and low levels of resilience.
The results showed that younger people had lower levels of resilience than older people and reported more severe depressive symptoms. This finding is consistent with previous research demonstrating that resilience increases with age (Nygren et al., 2005). The accumulation of rich life experiences among older generations is most likely to help increase resilience. Kuldas and Foody (2021) defined resilience as a dynamic interaction of intrapersonal, interpersonal, and risk factors. If that is the case, leisure activities, which influence people intrapersonally and interpersonally, would contribute to one's resilience building throughout the lifetime. There is, however, a possible sampling bias in the present study. The participants were registered members of the online survey company, and thus, they must be very familiar with computers or other electronic devices. Considering that the usage of such devices among older generations is not as common as in younger generations, the older participants in the present research might have been particularly adaptable to new technologies. Such adaptable older adults may have higher levels of resilience than others who do not use those devices.
Recent Japanese culture may also contribute to the lower levels of resilience among young people. Japanese culture is traditionally collectivistic that prioritizes group harmony, but it seems to be shifting towards individualism, which emphasizes the autonomy and responsibility of individuals (Ogihara, 2017). In recent Japan, due to the increased individualism, societies require people to take responsibility for themselves rather than relying on others' support. However, the traditional collectivistic value is still strong; thus, belonging to social groups and behaving as expected by other group members are still very important. In this complex cultural trend, many young Japanese people have failed to find a comfortable place in society (Norasakkunkit & Uchida, 2011). This cultural trend can prevent young Japanese from building resilience, and consequently, they become more vulnerable to the negative psychological impacts of the pandemic.
Examination of the hypothesised model generally supported the account that engaging in a higher number of leisure activities in a given time increases resilience, which could work for mental health. This is consistent with the notion that resilience is related to flexible thinking and multiple perspectives (Waugh et al., 2008). However, the mediating effect of resilience varied by age. Specifically, the results indicated that the variations mattered for resilience among younger people but not older ones. This may be because popular activities differ depending on age, resulting in different psychological impacts. The present data (see Supplemental S2) showed a tendency for younger people to choose activities for momentary entertainment and relaxation. Performing various relaxing activities may help younger people recover from daily labor and obligations, and this may elicit positive emotions, which is essential for resilience building. On the contrary, popular activities among the older adults are more social and involve skill building. Past studies have also found that the activities popular among older people are more strongly related to cognitive functioning, life satisfaction, and well‐being (Iwasa et al., 2012; Menec, 2003; Wang et al., 2012), compared with the activities simply for short‐term entertainment (e.g. playing games alone). Engaging in a small number of cognitively taxing activities might be more important for resilience building than engaging in various activities, especially for older people. The extent of positive emotion elicited by leisure is most likely to vary across different activities. So further investigations considering types of activities are necessary (see the limitations below).
Regarding the mediator between depression and leisure, something other than resilience might have been involved. Keller et al. (2022) recently investigated the relationship between the distress caused by COVID‐19, depression, anxiety, and loneliness. They found that symptoms of anxiety and loneliness mediated the positive association between post‐COVID‐19 distress and depression. In the context of the present research, people who participate in many leisure activities are likely to have various social communities that reduce loneliness. The lower level of loneliness before the pandemic may predict the lower level of depression before and during the pandemic. Therefore, loneliness may mediate the relationship between leisure and depression.
Strengths, limitations, and future scope
This study had three unique points. First, it was a longitudinal study that compared the participants' status before and after the spread of COVID‐19. This is significant because most studies examining COVID‐related behavioral changes do not have actual data representing the “before” status (a common procedure is to ask participants to recall the past). The first survey of the present study was conducted before the outbreak. Second, the current research emphasized the adaptable side of human nature rather than finding a simple increase in mental health problems due to the pandemic, as in most published studies on this topic. People utilized resilience and sought new leisure activities to combat the pandemic's negative influence. Finally, a large set of leisure activities were presented to the participants. Using the large number of choices, which were carefully selected based on previous research, was essential to grasp an accurate picture of the participants' situations while avoiding time‐consuming data analysis often associated with a free‐response method. Important to note that the list included culturally specific activities (e.g. Japanese dancing), and the inclusion of such activities is important when a similar study is conducted elsewhere.
The limitations of this study are as follows. First, it did not measure the actual amount of leisure time people lost (or gained) due to the pandemic. The reported reduction in the number of committed activities does not necessarily imply a decreased time spent on leisure activities. Furthermore, the results did not identify whether the decline in activities was a consequence of external factors (such as the cancelation of events) or the voluntary restrictions of participants. Varying consequences may impact mental health differently.
Second, this study did not consider the types of activities (e.g. physical or non‐physical). The psychological impact should vary across activities; for example, physical activities have superior effects on depressive symptoms (Paluska & Schwenk, 2000). Karp et al. (2006) claim that all leisure activities contain three components: mental, physical, and social, and the interactions of these components affect multiple cognitive domains. Therefore, it is important to focus on the functions of each type of activity and examine the combined effect of participating in a variety of activities.
Third, the scale used to measure depressive symptoms was insufficient. The PHQ‐2 is a screening instrument designed to reduce the burden on participants and contains only two items. Recent mental health studies targeting Japanese people using the PHQ‐9 (Ueda et al., 2020) and the Generic Depression Score (Fujita et al., 2021) have shown increased levels of depression due to the pandemic. Therefore, the absence of an increase in this study may be related to the insufficient measuring power of the PHQ‐2. Although it is well validated, it would be preferable to use a scale with a broader distribution of scores for more precise measurements. In addition, the direct relationship between leisure activities and resilience was not fully established. The results showed a significant correlation between the number of leisure activities and the level of resilience, but causal relationships between the two variables need to be empirically tested. Other psychological variables such as level of anxiety may need to be measured and controlled to do so.
Finally, the present findings may have limited generalizability due to the sample characteristics. Although the sample size of the second survey was sufficient for the analyses, the dropout rate from the first survey was very high. Thus, the remaining participants may not represent the general population of Japan. For example, people who were severely affected by the pandemic may not have responded to the second survey. There is also a possibility that the older people in the present study were particularly adaptable. A study with a larger sample is necessary to confirm the current findings, and a method other than online surveys may be essential to recruit varieties of older adults. Repeating the study in different countries must also be beneficial to reveal the influence of national prevention measures and culture.
In conclusion, this study found that engaging in a larger number of leisure activities reduces depressive symptoms through resilience. Engaging in a variety of leisure activities can be a very effective and entertaining process of resilience building (Caldwell, 2005), and such resilience can work to protect people from stress even in an appalling disaster such as the COVID‐19 pandemic (Kimhi et al., 2020).
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest with this work.
ETHICS STATEMENT
The study met the ethical guidelines of Kanazawa University.
Supporting information
Table S1.1.The demographic characteristics of samples at 1st and 2nd survey.
Table S1.2. The characteristics of respondents by six age groups at first survey (N = 1200)
Table S2. The number of participants for leisure, daily, and device using activities at 1st survey
Table S3. The number of participants and frequency of all activity at 1st and 2nd surveys
Table S4. The number of participants in each type of change for all leisure activities
Table S5. Intercorrelations of demographic, activities, mental health variables by survey
ACKNOWLEDGMENTS
This work was supported by JSPS KAKENHI through a Grant‐in‐Aid for Scientific Research (B) Number 19H01761 and Grant‐in‐Aid for Transformative Research Areas (A) Number 20H05803 and 2020 Collaborative Research Support Program of Kanazawa University.
Takiguchi, Y. , Matsui, M. , Kikutani, M. , & Ebina, K. (2022). The relationship between leisure activities and mental health: The impact of resilience and COVID‐19. Applied Psychology: Health and Well‐Being, 1–19. 10.1111/aphw.12394
ENDNOTE
The current sample size of the young group was slightly smaller than 77. Therefore, we calculated the post hoc statistical power for the regression analysis and confirmed that it was sufficient (see Hoenig & Heisey, 2001 for the importance of the post hoc power approach).
DATA AVAILABILITY STATEMENT
The data supporting this study's findings are available from the corresponding author upon reasonable request.
REFERENCES
- Akar, G. , Clifton, K. J. , & Doherty, S. T. (2012). Redefining activity types: Who participates in which leisure activity? Transportation Research Part A: Policy and Practice, 46(8), 1194–1204. 10.1016/j.tra.2012.05.007 [DOI] [Google Scholar]
- Alim, T. N. , Feder, A. , Graves, R. E. , Wang, Y. , Weaver, J. , & Westphal, M. (2008). Trauma, resilience, and recovery in a high risk African‐American population. American Journal of Psychiatry, 165, 1566–1575. 10.1176/appi.ajp.2008.07121939 [DOI] [PubMed] [Google Scholar]
- Balanzá‐Martínez, V. , Atienza‐Carbonell, B. , Kapczinski, F. , & De Boni, R. B. (2020). Lifestyle behaviours during the COVID‐19—Time to connect. Acta Psychiatrica Scandinavica, 141(5), 399–400. 10.1111/acps.13177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldwell, L. (2005). Leisure and health: Why is leisure therapeutic? British Journal of Guidance and Counselling, 33(1), 7–26. 10.1080/03069880412331335939 [DOI] [Google Scholar]
- Cummings, S. M. (2002). Predictors of psychological well‐being among assisted‐living residents. Health & Social Work, 27, 293–302. 10.1093/hsw/27.4.293 [DOI] [PubMed] [Google Scholar]
- Czeisler, M. É. , Lane, R. I. , Petrosky, E. , Wiley, J. F. , Christensen, A. , Njai, R. , … Rajaratnam, S. M. W. (2020). Mental health, substance use, and suicidal ideation during the COVID‐19 pandemic—United States, June 24‐30, 2020. Morbidity and Mortality Weekly Report, 69, 1049–1057. 10.15585/mmwr.mm6932a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denovan, A. , & Macaskill, A. (2017). Stress, resilience and leisure coping among university students: Applying the broaden‐and‐build theory. Leisure Studies, 36(6), 852–865. 10.1080/02614367.2016.1240220 [DOI] [Google Scholar]
- Erdfelder, E. , Faul, F. , & Buchner, A. (1996). GPOWER: A general power analysis program. Behavior Research Methods, Instruments, & Computers, 28, 1–11. 10.3758/BF03203630 [DOI] [Google Scholar]
- Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden‐and‐build theory of positive emotions. American Psychologist, 56, 218–226. 10.1037/0003-066x.56.3.218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fujita, K. , Inoue, A. , Kuzuya, M. , Uno, C. , Huang, C. H. , Umegaki, H. , & Onishi, J. (2021). Mental health status of the older adults in Japan during the COVID‐19 pandemic. Journal of the American Medical Directors Association, 22(1), 220–221. 10.1016/j.jamda.2020.11.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Funder, D. C. , & Ozer, D. J. (2019). Evaluating effect size in psychological research: Sense and nonsense. Advances in Methods and Practices in Psychological Science, 2(2), 156–168. 10.1177/2515245920979282 [DOI] [Google Scholar]
- Gammon, S. , & Ramshaw, G. (2021). Distancing from the present: Nostalgia and leisure in lockdown. Leisure Sciences, 43, 131–137. 10.1080/01490400.2020.1773993 [DOI] [Google Scholar]
- Havighurst, R. J. , & Feigenbaum, K. (1959). Leisure and lifestyle. American Journal of Sociology, 64(4), 396–404. 10.1086/222500 [DOI] [Google Scholar]
- Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. Guilford Publications. [Google Scholar]
- Hoenig, J. M. , & Heisey, D. M. (2001). The abuse of power: The pervasive fallacy of power calculations for data analysis. The American Statistician, 55(1), 19–24. 10.1198/000313001300339897 [DOI] [Google Scholar]
- Hu, L. T. , & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Inagaki, M. , Ohtsuki, T. , Yonemoto, N. , Kawashima, Y. , Saitoh, A. , Oikawa, Y. , Kurosawa, M. , Muramatsu, K. , Furukawa, T. A. , & Yamada, M. (2013). Validity of the Patient Health Questionnaire (PHQ)‐9 and PHQ‐2 in general internal medicine primary care at a Japanese rural hospital: A cross‐sectional study. General Hospital Psychiatry, 35(6), 592–597. 10.1016/j.genhosppsych.2013.08.001 [DOI] [PubMed] [Google Scholar]
- Iwasa, H. , Kai, I. , Kim, H. , Suzuki, T. , Yoshida, H. , & Yoshida, Y. (2012). Leisure activities and cognitive function in elderly community‐dwelling individuals in Japan: A 5‐year prospective cohort study. Journal of Psychosomatic Research, 72(2), 159–164. 10.1016/j.jpsychores.2011.10.002 [DOI] [PubMed] [Google Scholar]
- Iwasa, H. , & Yoshida, Y. (2018). Actual conditions of leisure activity among older community‐dwelling Japanese adults. Gerontology and Geriatric Medicine, 4, 23372141878167. 10.1177/2333721418781677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwasa, H. , Yoshida, Y. , Ishioka, Y. , & Suzukamo, Y. (2019). Development of a leisure activity scale for contemporary older adults: Examination of its association with cognitive function. Japanese Journal of Public Health, 66(10), 617–628. 10.11236/jph.66.10_617 [DOI] [PubMed] [Google Scholar]
- Iwasaki, Y. (2006). Counteracting stress through leisure coping: A prospective health study. Psychology Health and Medicine, 11(2), 209–220. 10.1080/13548500500155941 [DOI] [PubMed] [Google Scholar]
- Iwasaki, Y. , MacKay, K. , & Mactavish, J. (2005). Gender‐based analyses of coping with stress among professional managers: Leisure coping and non‐leisure coping. Journal of Leisure Research, 37(1), 1–28. 10.1080/00222216.2005.11950038 [DOI] [Google Scholar]
- Janke, M. C. , Carpenter, G. , Payne, L. L. , & Stockard, J. (2010). The role of life experiences on perceptions of leisure during adulthood: A longitudinal analysis. Leisure Sciences, 33(1), 52–69. 10.1080/01490400.2011.533108 [DOI] [Google Scholar]
- Karp, A. , Paillard‐Borg, S. , Wang, H. X. , Silverstein, M. , Winblad, B. , & Fratiglioni, L. (2006). Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dementia and Geriatric Cognitive Disorders, 21(2), 65–73. 10.1159/000089919 [DOI] [PubMed] [Google Scholar]
- Keller, F. M. , Derksen, C. , Kötting, L. , Dahmen, A. , & Lippke, S. (2022). Distress, loneliness, and mental health during the COVID‐19 pandemic: Test of the extension of the evolutionary theory of loneliness. Applied Psychology: Health and Well‐Being. 10.1111/aphw.12352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kikuchi, H. , Machida, M. , Nakamura, I. , Saito, R. , Odagiri, Y. , Kojima, T. , Watanabe, H. , Fukui, K. , & Inoue, S. (2020). Changes in psychological distress during the COVID‐19 pandemic in Japan: A longitudinal study. Journal of Epidemiology, 30(11), 522–528. 10.2188/jea.JE20200271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimhi, S. , Marciano, H. , Eshel, Y. , & Adini, B. (2020). Resilience and demographic characteristics predicting distress during the COVID‐19 crisis. Social Science & Medicine, 265, 113389. 10.1016/j.socscimed.2020.113389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleiber, D. A. , Hutchinson, S. L. , & Williams, R. (2002). Leisure as a resource in coping with negative life events: Self‐protection, self‐restoration, and personal transformation. Leisure Sciences, 24(2), 219–235. 10.1080/01490400252900167 [DOI] [Google Scholar]
- Kleiber, D. A. , & Nimrod, G. (2009). “I can't be very sad”: Constraint and adaptation in the leisure of a “learning in retirement” group. Leisure Studies, 68, 67–83. 10.1080/02614360802260820 [DOI] [Google Scholar]
- Kozono, M. , Gondo, Y. , Ogawa, M. , Ishioka, Y. , Masui, Y. , Nakagawa, T. , … Takahashi, R. (2016). The relationship between leisure activities and cognitive function in community‐dwelling older adults. Japanese Journal of Gerontology, 38, 32–44. [Google Scholar]
- Kroenke, K. , Spitzer, R. L. , & Williams, J. B. (2003). The patient health questionnaire‐2: Validity of a two‐item depression screener. Medical Care, 41, 1284–1292. 10.1097/01.MLR.0000093487.78664.3C [DOI] [PubMed] [Google Scholar]
- Kuldas, S. , & Foody, M. (2021). Neither resiliency‐trait nor resilience‐state: Transactional resiliency/e. Youth & Society. 10.1177/0044118X211029309 [DOI] [Google Scholar]
- Lawton, M. P. , Moss, M. S. , Winter, L. , & Hoffman, C. (2002). Motivation in later life: Personal projects and well‐being. Psychology and Aging, 17(4), 539–547. 10.1037/0882-7974.17.4.539 [DOI] [PubMed] [Google Scholar]
- Menec, V. H. (2003). The relation between everyday activities and successful aging: A 6‐year longitudinal study. Journal of Gerontology, 58, 74–82. 10.1093/geronb/58.2.S74 [DOI] [PubMed] [Google Scholar]
- Menec, V. H. , & Chipperfield, J. G. (1997). Remaining active in later life: The role of locus of control in seniors' leisure activity participation, health, and life satisfaction. Journal of Aging and Health, 9(1), 105–125. 10.1177/089826439700900106 [DOI] [PubMed] [Google Scholar]
- Nishi, D. , Uehara, R. , Kondo, M. , & Matsuoka, Y. (2010). Reliability and validity of the Japanese version of the Resilience Scale and its short version. BioMedical Central Research Notes, 3, 310. 10.1186/1756-0500-3-310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norasakkunkit, V. , & Uchida, Y. (2011). Psychological consequences of postindustrial anomie on self and motivation among Japanese youth. Journal of Social Issues, 67(4), 774–786. 10.1111/j.1540-4560.2011.01727.x [DOI] [Google Scholar]
- Nygren, B. , Aléx, L. , Jonsén, E. , Gustafson, Y. , Norberg, A. , & Lundman, B. (2005). Resilience, sense of coherence, purpose in life and self‐transcendence in relation to perceived physical and mental health among the oldest old. Aging & Mental Health, 9, 354–362. 10.1080/1360500114415 [DOI] [PubMed] [Google Scholar]
- Ogihara, Y. (2017). Temporal changes in individualism and their ramification in Japan: Rising individualism and conflicts with persisting collectivism. Frontiers in Psychology, 8, 695. 10.3389/fpsyg.2017.00695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paluska, S. A. , & Schwenk, T. (2000). Physical activity and mental health: Current concepts. Sports Medicine, 29, 167–180. 10.2165/00007256-200029030-00003 [DOI] [PubMed] [Google Scholar]
- Parady, G. , Taniguchi, A. , & Takami, K. (2020). Travel behavior changes during the COVID‐19 pandemic in Japan: Analyzing the effects of risk perception and social influence on going‐out self‐restriction. Transportation Research Interdisciplinary Perspectives, 7, 100181. 10.1016/j.trip.2020.1000181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reschly, A. L. , Huebner, E. S. , Appleton, J. J. , & Antaramian, S. (2008). Engagement as flourishing: The contribution of positive emotions and coping to adolescents' engagement at school and with learning. Psychology in the Schools, 45, 419–431. 10.1002/pits.20306 [DOI] [Google Scholar]
- Richardson, G. E. (2002). The metatheory of resilience and resiliency. Journal of Clinical Psychology, 58(3), 307–321. 10.1002/jclp.10020 [DOI] [PubMed] [Google Scholar]
- Sivan, A. , & Siu, G. P. S. (2021). A longitudinal study on leisure of Hong Kong adolescents. Leisure Studies, 40, 306–320. 10.1080/02614367.2020.1858329 [DOI] [Google Scholar]
- Strain, L. A. , Grabusic, C. C. , Searle, M. S. , & Dunn, N. J. (2002). Continuing and ceasing leisure activities in later life: A longitudinal study. The Gerontologist, 42(2), 217–223. 10.1093/geront/42.2.217 [DOI] [PubMed] [Google Scholar]
- Ueda, M. , Stickley, A. , Sueki, H. , & Matsubayashi, T. (2020). Mental health status of the general population in Japan during the COVID‐19 pandemic. Psychiatry and Clinical Neurosciences, 74(9), 505–506. Portico. 10.1111/pcn.13105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verghese, J. , LeValley, A. , Derby, C. , Kuslansky, G. , Katz, M. , Hall, C. , Buschke, H. , & Lipton, R. B. (2006). Leisure activities and the risk of amnestic mild cognitive impairment in the elderly. Neurology, 66, 821–827. 10.1212/01.wnl.0000202520.68987.48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , McIntyre, R. S. , Choo, F. N. , Tran, B. , Ho, R. , Sharma, V. K. , & Ho, C. (2020). A longitudinal study on the mental health of general population during the COVID‐19 epidemic in China. Brain, Behavior, and Immunity, 87, 40–48. 10.1016/j.bbi.2020.04.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, H. X. , Xu, W. , & Pei, J. J. (2012). Leisure activities, cognition and dementia. Biochimica et Biophysica Acta, 1822, 482–491. 10.1016/j.bbadis.2011.09.002 [DOI] [PubMed] [Google Scholar]
- Waugh, C. E. , Fredrickson, B. L. , & Taylor, S. F. (2008). Adapting to life's slings and arrows: Individual differences in resilience when recovering from an anticipated threat. Journal of Research in Personality, 42, 1031–1046. 10.1016/j.jrp.2008.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wingo, A. P. , Wrenn, G. , Pelletier, T. , Gutman, A. R. , Bradley, B. , & Ressler, K. J. (2010). Moderating effects of resilience on depression in individuals with a history of childhood abuse or trauma exposure. Journal of Affective Disorders, 126, 411–414. 10.1016/j.jad.2010.04.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu, X. , Stewart, S. M. , Wong, P. T. , & Lam, T. H. (2011). Screening for depression with the Patient Health Questionnaire‐2 (PHQ‐2) among the general population in Hong Kong. Journal of Affective Disorders, 134(1–3), 444–447. 10.1016/j.jad.2011.05.007 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1.1.The demographic characteristics of samples at 1st and 2nd survey.
Table S1.2. The characteristics of respondents by six age groups at first survey (N = 1200)
Table S2. The number of participants for leisure, daily, and device using activities at 1st survey
Table S3. The number of participants and frequency of all activity at 1st and 2nd surveys
Table S4. The number of participants in each type of change for all leisure activities
Table S5. Intercorrelations of demographic, activities, mental health variables by survey
Data Availability Statement
The data supporting this study's findings are available from the corresponding author upon reasonable request.