

ABSTRACT
BACKGROUND
COVID‐19‐disrupted schools, including shifts to virtual learning which may have impacted academic progress. This study assessed characteristics associated with changes in academic grades (before and during the pandemic) for different learning modalities for US students ages 13‐19.
METHODS
Students (N = 2152) completed a web survey on school‐related experiences during the 2020‐2021 school year. County social vulnerability and SARS‐CoV‐2 transmission data were merged with survey data. Multivariable logistic regression analysis for grade change was conducted with student and school characteristics for each learning modality, controlling for community characteristics.
RESULTS
Greater proportions of remote/virtual (34.4%) and hybrid (30.1%) learning students reported grade decline compared to in‐person students (19.9%). Among in‐person students, odds of reporting same/improved grades were 65% lower among non‐Hispanic black students and 66% lower among non‐Hispanic students from other races, compared to non‐Hispanic white students. Among hybrid students, odds of reporting same/improved grades for students reporting anxiety were 47% lower than students without anxiety, and odds of reporting same/improved grades among students reporting substance use were 40% lower than students not reporting substance use. Among remote/virtual students, odds of reporting same/improved grades among students with depression were 62% lower than odds of students not reporting depression symptoms. Remote/virtual students who received school‐provided educational services also had 1.55 times the odds of reporting same/improved grades, compared to remote/virtual students not receiving these services.
CONCLUSIONS
Academic grades were negatively impacted during COVID‐19 and learning mode may have contributed. Understanding these impacts is critical to student health and academic achievement.
Keywords: COVID‐19, coronavirus, adolescents, academic grades, disparities, virtual learning
In March 2020, the COVID‐19 pandemic led to an unprecedented change to traditional learning in US schools. Nearly, 93% of all students in the US engaged in some form of virtual learning in Spring 2020 1 with many school closures continuing into the following year. 2 The extent to which student learning modality (eg, attended school in‐person or virtually) affected academic progress during the pandemic is unknown. To better understand how academic progress may have been affected by the pandemic, it is useful to consider the role of learning modality as well as other student, school, and community characteristics.
The Social Ecological Model (SEM) provides a framework to understand how a student's individual characteristics (eg, mental health, academic ability) interact with social relationships (eg, peers, school, family) and environmental factors (eg, neighborhood social capital) to influence health outcomes. 3 , 4 , 5 Academic achievement has also been examined through the SEM lens. The connections between individual, family, and school characteristics and academic achievement, including standardized test scores, are well documented 6 , 7 , 8 , 9 , 10 , 11 , 12 and form the foundation for the Whole School, Whole Community, Whole Child model. This model illustrates that multiple components and systems influence a school's ability to ensure students are safe, supported, challenged, engaged, and healthy. 13 , 14
There is evidence that overall student achievement, regardless of learning modality, was impacted by the pandemic. For example, in a survey of school district administrators during the 2020‐2021 school year, 34% reported a substantial increase in the percentage of high school students receiving poor grades, with greater increases in districts serving mostly black and Hispanic students or districts with historically lower academic achievement levels. 15 Signs of learning loss and disparities are also evident in standardized test scores—one study reported drops in reading and math scores, compared to prepandemic scores of students in the same grade level (with greatest declines among black and Hispanic youth). 16 During COVID‐19, it is possible that student learning modality and community characteristics (eg, level of social vulnerability 17 and community social capital 18 ) may have interacted, contributing to or exacerbating learning disparities among US K‐12 students. For example, socially vulnerable counties 19 , 20 experienced higher COVID‐19 case counts 21 and fatality rates 22 and, as a result, may have been more likely to mandate virtual‐only instruction. Given disparities in full‐time, in‐person learning by race/ethnicity have been demonstrated during the pandemic across school levels and by geographic region and state, 23 learning modality might be a potential mechanism that contributed to grade declines.
Learning modality might have also influenced students' sense of belonging at school, emotional wellbeing, and access to school‐provided supports. Emerging research indicates that students in virtual‐only instruction were less likely to report feeling connected to school 24 and urban and large districts were less likely to provide 100% in‐person instruction than rural, suburban, and smaller jurisdictions. 25 These findings suggest potential disparities in school connectedness and academic achievement, dependent on school instruction mode and location. Further, a myriad of negative effects on adolescent mental health and well‐being related to COVID‐19 have been documented, suggesting a mental health crisis among adolescents, many of whom were already experiencing challenges. 26 These challenges may have been further exacerbated by school closures and virtual learning as schools provide important mental health services and learning supports. 27 Schools are one of the primary providers of mental health services to students 27 ; however, the extent to which schools provided such services during the pandemic is unclear. 28 , 29 School connectedness and access to health‐related supports and services can buffer the negative impact of individual risk factors on adolescent wellbeing and improve overall mental health 30 , 31 and, consequently, academic achievement. 32 , 33 Finally, service gaps might disproportionately impact students from low‐income households and racial/ethnic minority groups who are more likely than other groups to rely solely on educational settings for mental health services. 34
The purpose of this study is to use SEM principles to describe self‐reported grade change during the pandemic, and to identify individual, school, and community characteristics associated with grade change, within each of 3 learning modalities.
METHODS
Study Design and Participants
Data were collected as part of the Monitoring School COVID‐19 Mitigation Strategies Project (a CDC Foundation project, funded by donors to its' COVID‐19 Emergency Response Fund, to inform CDC's Operational Strategy for K‐12 Schools through Phased Prevention COVID‐19 recommendations). 1 , 35 Survey data on student experiences during the 2020‐2021 school year were collected May 10‐June 1, 2021, using Qualtrics (Provo, UT), an online survey platform that provides access to specific populations through double‐opt‐in market research panels. Qualtrics samples are intended to be nationally representative based on US Census estimates and include quotas for demographic characteristics.
Web panel members who identified as a parent of a teen aged 13 or older in middle or high school were asked to provide consent for their child to participate. If consent was provided, a survey invitation was emailed to the teen. Inclusion criteria were students ages 13 and above; attending a US‐based public, private or charter middle or high school; and provided assent to participate. Among the 7589 respondents initiating the survey, 5231 were screened out because they did not meet criteria, they did not finish the survey, or quotas had already been met. An additional 183 surveys were excluded for data quality issues, resulting in 2175 respondents. Twenty‐three additional surveys were dropped for students who indicated they were “transgender,” “non‐binary,” or “non‐conforming”—the small sample would not allow for reliable estimates for this population. The final analytic sample was 2152 respondents (Figure 1).
Figure 1.
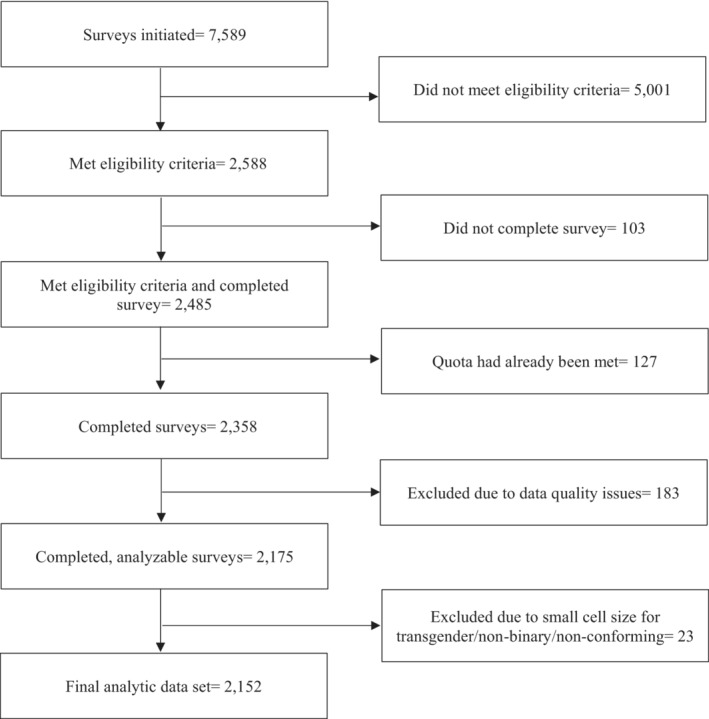
Study Inclusion Criteria for Final Analytic Sample
CDC/ATSDR Social Vulnerability Index (SVI) and SARS‐CoV‐2 transmission data were obtained from publicly available data based on the counties where students reported they attended school during the 2020‐2021 school year. The SVI ranks US Census tracts and counties on 15 social factors, with higher scores denoting higher vulnerability. 36 County‐specific data from 2018 SVI data set (most recent available) were analyzed. 36 County‐specific SARS‐CoV‐2 transmission levels (based on new positive case rate and percent positivity) were obtained from the CDC COVID Data Tracker 37 to characterize disease burden at time of data collection.
Variables
Change in academic grades (primary outcome) was constructed from 2 survey questions: “How would you describe your grades in school now?” and “How would you describe your grades in school before the COVID‐19 pandemic (before February 2020)?” Response options for each question were “mostly A's,” “mostly B's,” “mostly C's,” “mostly D's,” “mostly F's,” “none of these grades,” or “not sure.” A dichotomous variable was created to categorize grades as “declined” or “same/improved” since the pandemic began for respondents who provided letter grade information for both questions (excluding those who reported “none of these grades” or “not sure” for one or both questions). To assess learning modality, respondents were asked to characterize how they attended school most often during the 2020‐2021 school year: “in‐person 100% (coming into school),” “remote/virtual learning (staying at home) 100%,” or “hybrid (a mix of coming into school and staying at home).”
Student characteristics
Sociodemographic characteristics included gender (female, male), race/ethnicity (Hispanic, non‐Hispanic white, non‐Hispanic black, non‐Hispanic other), and school level (middle school—grades 6‐8, high school—grades 9‐12). The non‐Hispanic other race/ethnicity category includes respondents who selected “Asian,” “American Indian or Alaska Native,” “Native Hawaiian or Pacific Islander,” “some other race,” or multiple race/ethnicity categories on the survey. The non‐Hispanic other category is not disaggregated due to small cell size generating unstable estimates and, also, to protect confidentiality.
Health and behavioral characteristics were derived from mental health and substance use variables. The Patient Health Questionnaire 2 (PHQ‐2) and Generalized Anxiety Disorder (GAD‐2) were used to assess depression and anxiety, respectively. 38 These scales are abbreviated versions of the PHQ‐9 and GAD‐7 scales, respectively, which have been validated in adult primary care and extended to general samples of adolescents 39 , 40 , 41 and young adults. 42 , 43 PHQ‐2 and GAD‐2 have been demonstrated to perform similarly to the longer scales with regard to identifying young people with probable mood or anxiety disorders. 38 Respondents were asked, “Over the last 2 weeks, how often have you been bothered by the following problems?” Anxiety items were: “feeling nervous, anxious, or on edge” and “not being able to stop or control worrying.” Depression items were: “little interest or pleasure in doing things” and “feeling down, depressed, or hopeless.” Response choices for each of these 4 survey items were “never,” “rarely,” “sometimes,” “often,” or “very often.” Response choices “rarely” and “sometimes” were combined for each survey item and then the following scores were assigned (never = 0, rarely/sometimes = 1, often = 2, very often = 3). Using the GAD‐2 scale, respondents with anxiety symptoms represent those who scored ≥3 after summing both anxiety items (range = 0‐6). Using the PHQ‐2 scale, respondents with depression symptoms represented those who scored ≥3 after summing both depression items (range = 0‐6). Substance use was assessed by asking respondents, “Since the pandemic began (February 2020), have you started using or increased using substances to help you cope with stress or emotions (substance use includes tobacco, alcohol, legal or illegal drugs, or prescription drugs that are taken in a way not recommended by your doctor)?” Survey respondents responded “yes” or “no” for each of the following substances: alcohol, non‐prescription drugs, prescription drugs, tobacco products. A dichotomous variable was created to categorize substance use as any use (ie, responded “yes” to at least 1 substance) or no use (ie, responded “no” to all). Although this substance use measure was not validated prior to use in this study, similar retrospective substance use measures have been reported in other research. 44
School‐provided supports
We focused on student‐reported receipt of services to support learning and health to assess whether schools were providing these services to students as needed. Survey respondents indicated the frequency with which they received education‐related services during the 2020‐2021 school year: in‐school or after school tutoring, accommodations for assignments (eg, teacher gave them more time to complete assignments, provided additional instruction after class), academic support (changes to classroom assignments or extra help from the teacher), and individual classroom support (a second teacher or aide helped them in the classroom). Respondents also indicated how often they received health‐related services: occupational therapy, speech therapy, and behavioral/mental health support (by school counselor, classroom teacher, or other school staff member). For each service type, a separate dichotomous variable was created to categorize responses as either received any service (ie, responded “yes” to at least 1 service) or no services (ie, responded “no” to all).
Community characteristics
US Census region (Midwest, Northeast, South, West) and locality (rural, suburban, urban) of the respondent's school were obtained through the survey. Tertiles were computed to identify counties in the bottom one‐third of the SVI range (low vulnerability), middle one‐third (moderate vulnerability), and top one‐third (high vulnerability). SARS‐CoV‐2 transmission level was calculated as the number of days during the survey data collection period that the county where the school is located met criteria for high transmission level. Transmission data were available for 15 of the 22 data collection days.
Data Analysis
Analysis was conducted with Stata Version 14 (College Station, TX). Survey data were weighted to be representative of the sampled population using demographic variables (age, gender, race/ethnicity). A multipurpose Iterative Proportional Fitting procedure was used to calibrate individual‐level weights, simultaneously adjusting for population estimates from 2019 National Health Interview Survey 45 ; bloc‐level nonresponse adjustment based on calibration in the quintiles of estimated propensity to respond to surveys; and weight trimming procedures (removed 5% of extreme high/low estimates).
Pearson χ2 tests were conducted to identify unadjusted, bivariate associations between learning modality and student characteristics, school‐provided supports, and community characteristics (Table 1) to illustrate the prevalence and relationship between these variables before subpopulating the analyses for logistic regression. Bivariate analyses were also conducted between academic grade change (outcome measure) and student characteristics and school‐provided supports (Table 2) to 1) illustrate the prevalence and relationship between the variables before subpopulating the analyses for logistic regression, and 2) inform which variables should be included in the models, a part of model specification. In Table 2, we focused on student and school characteristics which may be most useful to school decision makers looking to identify students who might need more academic support.
Table 1.
Characteristics of Students, School‐Provided Supports, and Community Characteristics of Survey Respondents Ages 13‐19 Attending K‐12 Schools by Learning Modality (In‐Person, Hybrid, or Remote/Virtual) for the SY 2020‐2021
| Student Learning Modality, N, % (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall, N, % (95% CI) | In‐person | Hybrid | Remote/Virtual | p‐Value | |||||
| Total | 2152 | 425 (19.8%) | 884 (41.1%) | 843 (39.2%) | |||||
| Academic grade change* | <.001 | ||||||||
| Declined | 632 | 29.8 (27.8, 31.9) | 83 | 19.9 (16.2, 24.3) | 267 | 30.1 (27.1, 33.4) | 282 | 34.4 (31.1, 37.9) | |
| Same/improved | 1496 | 70.2 (68.1, 72.2) | 338 | 80.1 (75.7, 83.8) | 608 | 69.9 (66.6, 72.9) | 550 | 65.6 (62.1, 68.9) | |
| Student sociodemographic characteristics | |||||||||
| Gender | .02 | ||||||||
| Female | 1071 | 49.0 (46.7, 51.2) | 205 | 46.2 (41.3, 51.2) | 412 | 46.6 (43.2, 50.0) | 454 | 52.8 (49.2, 56.3) | |
| Male | 1081 | 51.0 (48.8, 53.3) | 220 | 53.8 (48.8, 58.7) | 472 | 53.4 (50.0, 56.8) | 389 | 47.2 (43.7, 50.8) | |
| Race/ethnicity | <.001 | ||||||||
| Non‐Hispanic white | 1117 | 52.8 (50.6, 55.0) | 264 | 62.7 (57.8, 67.4) | 527 | 61.3 (57.9, 64.6) | 326 | 39.1 (35.7, 42.6) | |
| Non‐Hispanic black | 272 | 13.0 (11.6, 14.6) | 44 | 11.4 (8.5, 15.2) | 87 | 9.6 (7.8, 11.9) | 141 | 17.2 (14.7, 20.1) | |
| Hispanic | 530 | 25.6 (23.7, 27.6) | 83 | 19.9 (16.1, 24.2) | 187 | 21.3 (18.6, 24.3) | 260 | 32.9 (29.6, 36.3) | |
| Non‐Hispanic other † | 233 | 8.6 (7.6, 9.8) | 34 | 6.0 (4.2, 8.4) | 83 | 7.7 (6.2, 9.6) | 116 | 10.8 (9.0, 13.0) | |
| School level | .6 | ||||||||
| High school (grades 9‐12) | 1367 | 67.7 (65.6, 69.6) | 261 | 65.7 (60.9, 70.1) | 559 | 67.7 (64.5, 70.7) | 547 | 68.6 (65.4, 71.7) | |
| Middle school (grades 6‐8) | 785 | 32.3 (30.4, 34.4) | 164 | 34.4 (29.9, 39.1) | 325 | 32.3 (29.3, 35.5) | 296 | 31.4 (28.3, 34.6) | |
| Student health/behavioral characteristics | |||||||||
| Mental health ‡ | |||||||||
| Has anxiety symptoms | 478 | 22.3 (20.5, 24.2) | 88 | 20.8 (17.0, 25.1) | 215 | 24.1 (21.3, 27.2) | 175 | 21.2 (18.4, 24.3) | .3 |
| Has depression symptoms | 422 | 19.5 (17.8, 21.3) | 78 | 18.8 (15.1, 23.0) | 174 | 19.0 (16.5, 21.9) | 170 | 20.4 (17.7, 23.4) | .7 |
| Substance use since pandemic began § | 348 | 15.9 (14.3, 17.6) | 79 | 19.2 (15.5, 23.5) | 152 | 16.5 (14.2, 19.3) | 117 | 13.5 (11.3, 16.1) | .04 |
| School‐provided supports | |||||||||
| Received education‐related services ‖ | 1515 | 70.1 (68.0, 72.1) | 285 | 66.1 (61.2, 70.7) | 633 | 71.9 (68.7, 74.8) | 597 | 70.3 (67.0, 73.5) | .1 |
| Received health‐related services ¶ | 288 | 13.1 (11.7, 14.7) | 75 | 17.1 (13.7, 21.2) | 111 | 12.8 (10.7, 15.4) | 102 | 11.5 (9.4, 13.9) | .02 |
| Community characteristics | |||||||||
| US Census region # | <.001 | ||||||||
| Midwest | 411 | 20.8 (19.0, 22.8) | 96 | 25.0 (20.9, 29.7) | 198 | 25.2 (22.2, 28.4) | 117 | 14.3 (12.0, 17.0) | |
| Northeast | 385 | 16.5 (15.0, 18.1) | 46 | 9.5 (7.1, 12.7) | 190 | 19.9 (17.3, 22.6) | 149 | 16.6 (14.2, 19.3) | |
| South | 873 | 38.6 (36.4, 40.7) | 230 | 51.4 (46.4, 56.4) | 314 | 33.2 (30.0, 36.4) | 329 | 37.7 (34.3, 41.1) | |
| West | 483 | 24.1 (22.2, 26.1) | 53 | 14.0 (10.7, 18.1) | 182 | 21.9 (19.1, 24.9) | 248 | 31.5 (28.2, 34.9) | |
| Locality** | <.001 | ||||||||
| Rural | 425 | 14.1 (12.8, 15.4) | 106 | 18.5 (15.3, 22.3) | 199 | 16.3 (14.2, 18.7) | 120 | 9.5 (7.9, 11.4) | |
| Suburban | 1085 | 56.4 (54.2, 58.5) | 220 | 58.5 (53.6, 63.2) | 433 | 55.7 (52.2, 59.0) | 432 | 56.0 (52.5, 59.4) | |
| Urban | 642 | 29.6 (27.6, 31.7) | 99 | 23.0 (19.1, 27.4) | 252 | 28.1 (25.1, 31.2) | 291 | 34.5 (31.3, 37.9) | |
| Social vulnerability index †† , ‡‡ | <0.001 | ||||||||
| Low | 750 | 35.7 (33.6, 37.9) | 163 | 39.8 (35.0, 44.8) | 331 | 38.9 (35.5, 42.3) | 256 | 30.5 (27.3, 33.9) | |
| Moderate | 687 | 31.6 (29.6, 33.7) | 138 | 33.2 (28.7, 38.1) | 290 | 32.0 (28.9, 35.3) | 259 | 30.5 (27.4, 33.9) | |
| High | 715 | 32.6 (30.6, 34.7) | 124 | 27.0 (22.9, 31.6) | 263 | 29.1 (26.1, 32.4) | 328 | 39.0 (35.6, 42.5) | |
| High days of SARS‐CoV‐2 transmission ‡‡ , §§ | .05 | ||||||||
| 0 days | 1249 | 62.0 (59.8, 64.2) | 254 | 64.0 (59.0, 68.7) | 494 | 59.2 (55.6, 62.6) | 501 | 64.0 (60.5, 67.4) | |
| 1‐7 days | 472 | 22.3 (20.5, 24.3) | 85 | 19.7 (16.0, 24.0) | 200 | 22.9 (20.1, 26.0) | 187 | 23.1 (20.1, 26.2) | |
| 8‐14 days | 315 | 15.7 (14.1, 17.4) | 187 | 16.4 (13.0, 20.5) | 145 | 17.9 (15.3, 20.9) | 102 | 12.9 (10.7, 15.6) | |
Table shows unweighted counts (N), weighted overall and column percentages (%), and weighted 95% confidence intervals (CIs). p‐Value represents associations between the groups of learning modalities by each variable of interest. p‐Values <.05 were considered statistically significant.
SY, school year.
Represents change in letter grades since before the start of the COVID‐19 pandemic (before February 2020). Grade change could not be computed for n = 24 survey respondents because they reported “none of these grades” or “not sure” for one or both questions about academic grades.
Non‐Hispanic other race/ethnicity category includes Asian, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, some other race, or selected more than one race category. The Non‐Hispanic other category is not disaggregated due to small cell size generating unstable estimates and to protect confidentiality.
Using the GAD‐2 scale (Generalized Anxiety Disorder), respondents with anxiety symptoms represent those who scored ≥3 for anxiety, indicating a need for follow‐up screening for anxiety. Using the PHQ‐2 scale (Patient Health Questionnaire), respondents with depression symptoms represent those who scored ≥3 for depression, indicating a need for follow‐up screening for depression.
Started or increased use of at least 1 substance (alcohol, tobacco, prescription drug, or non‐prescription drug) to help cope with stress or emotions, taken in a way not recommended by a doctor.
Education‐related services received during SY 2020‐2021 (tutoring, accommodations for assignments, academic support, and/or individual classroom support).
Health‐related services received during SY 2020‐2021 (occupational therapy, speech therapy, and/or behavioral/mental health support).
Based on survey respondent's self‐reported state of residence.
Based on survey respondent's self‐reported location of school. This information was missing for n = 188 respondents.
2018 CDC/ATSDR Social Vulnerability Index (SVI) for the county where respondent school is located. Low = counties in bottom one‐third, or tertile, of SVI scores (lowest vulnerability). Moderate = counties in middle tertile of SVI scores. High = counties in top tertile of SVI scores (highest vulnerability).
Could not be computed for n = 188 survey respondents due to missing school location.
Number of days that the county where the school is located was designated as having a high SARS‐CoV‐2 transmission level (8‐14 days).
Table 2.
Characteristics of Students and School‐Provided Supports of Survey Respondents Ages 13‐19 Attending K‐12 Schools by Academic Grade Change (Declined or Same/Improved) for the SY 2020‐2021
| Academic Grade Change*, N, % (95% CI) | |||||||
|---|---|---|---|---|---|---|---|
| Overall, N, % (95% CI) | Declined | Same/Improved | p‐Value | ||||
| Total | 2128 | 632 (29.4%) | 1496 (69.5%) | ||||
| Student learning modality | <.001 | ||||||
| In‐person | 421 | 19.8 (18.1, 21.7) | 83 | 13.3 (10.7, 16.3) | 338 | 22.6 (20.5, 24.9) | |
| Hybrid | 875 | 40.6 (38.5, 42.8) | 267 | 41.1 (37.2, 45.2) | 608 | 40.4 (37.9, 43.1) | |
| Remote/virtual | 832 | 39.5 (37.4, 41.8) | 282 | 45.6 (41.6, 49.7) | 550 | 37.0 (34.4, 39.6) | |
| Student sociodemographic characteristics | |||||||
| Gender | .4 | ||||||
| Female | 1059 | 48.9 (46.8, 51.2) | 300 | 47.5 (43.4, 51.6) | 759 | 49.6 (47.0, 52.3) | |
| Male | 1069 | 51.0 (48.8, 53.3) | 332 | 52.5 (48.4,56.6) | 737 | 50.4 (47.7, 53.1) | |
| Race/ethnicity | .01 | ||||||
| Non‐Hispanic white | 1105 | 52.9 (50.7, 55.1) | 294 | 48.4 (44.3, 52.5) | 811 | 54.8 (52.1, 57.4) | |
| Non‐Hispanic black | 267 | 12.9 (11.4, 14.4) | 90 | 14.2 (11.6, 17.3) | 177 | 12.3 (10.6, 14.2) | |
| Hispanic | 525 | 25.7 (23.7, 27.7) | 186 | 29.9 (26.3, 33.8) | 339 | 23.8 (21.6, 26.2) | |
| Non‐Hispanic other † | 231 | 8.6 (7.6, 9.8) | 62 | 7.4 (5.8, 9.6) | 169 | 9.1 (7.8, 10.6) | |
| School level | .8 | ||||||
| High school (grades 9‐12) | 1354 | 67.8 (65.7, 69.7) | 400 | 67.5 (63.6, 71.0) | 954 | 67.9 (65.5, 70.3) | |
| Middle school (grades 6‐8) | 774 | 32.2 (30.3, 34.3) | 232 | 32.6 (29.0, 36.4) | 542 | 32.1 (29.8, 34.5) | |
| Student health/behavioral characteristics | |||||||
| Mental health ‡ | |||||||
| Has anxiety symptoms | 472 | 22.3 (20.5, 24.2) | 196 | 31.7 (28.01, 35.7) | 276 | 18.3 (16.3, 20.4) | <.001 |
| Has depression symptoms | 419 | 19.6 (17.9, 21.4) | 183 | 29.5 (25.9, 33.4) | 236 | 15.4 (13.6, 17.4) | <.001 |
| Substance use since pandemic began § | 344 | 15.9 (14.3, 17.6) | 135 | 21.0 (17.8, 24.5) | 209 | 13.7 (12.0, 15.6) | <.001 |
| School‐provided supports | |||||||
| Received education‐related services ‖ | 1502 | 70.3 (68.2, 72.3) | 436 | 68.5 (64.5, 72.2) | 1066 | 71.0 (68.6, 73.4) | .3 |
| Received health‐related services ¶ | 286 | 13.2 (11.8, 14.8) | 80 | 11.9 (9.6, 14.7) | 206 | 13.7 (12.0, 15.6) | .3 |
Table shows unweighted counts (N), weighted overall and column percentages (%), and weighted 95% confidence intervals (CIs). Academic grade change represents change in letter grades since before the start of the COVID‐19 pandemic (before February 2020). Grade change could not be computed for n = 24 survey respondents because they reported “none of these grades” or “not sure” for one or both questions about academic grades. p‐Values <0.05 considered statistically significant.
SY, school year.
Academic grade change represents change in letter grades since before the start of the COVID‐19 pandemic (before Feb. 2020). Grade change could not be computed for n = 24 survey respondents because they reported “none of these grades” or “not sure” for one or both questions about academic grades (overall sample size (2152) minus surveys without grade change information (24) = 2128).
Non‐Hispanic other race/ethnicity category includes Asian, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, some other race, or selected more than one race category. The Non‐Hispanic other category is not disaggregated due to small cell size generating unstable estimates and to protect confidentiality.
Using the GAD‐2 scale (Generalized Anxiety Disorder), respondents with anxiety symptoms represent those who scored ≥3 for anxiety, indicating a need for follow‐up screening for anxiety. Using the PHQ‐2 scale (Patient Health Questionnaire), respondents with depression symptoms represent those who scored ≥3 for depression, indicating a need for follow‐up screening for depression.
Started or increased use of at least one substance (alcohol, tobacco, prescription drug, or non‐prescription drug) to help cope with stress or emotions, taken in a way not recommended by a doctor.
Education‐related services received during SY 2020‐2021 (tutoring, accommodations for assignments, academic support, and/or individual classroom support).
Health‐related services received during SY 2020‐2021 (occupational therapy, speech therapy, and/or behavioral/mental health support).
Multivariable logistic regression models were then conducted (Table 3). Regression analysis was first conducted with the entire sample. Then models were subpopulated by learning modality to assess the relationships between grade change and student and school characteristics for each learning group, controlling for community characteristics. Because county‐level SVI and SARS‐CoV‐2 transmission data were merged with survey data, we calculated the intraclass coefficient (ICC = 0.02) to determine any clustering effects. Because there were no clustering effects, we did not use hierarchical models.
Table 3.
Multivariable Logistic Regression for Having Same or Improved Academic Grades (Compared to Prepandemic) and Characteristics of Students and School‐Provided Supports, Subpopulated by Student Learning Modality (In‐Person, Hybrid, or Remote/Virtual) in SY 2020‐2021
| Student Learning Modality | ||||||||
|---|---|---|---|---|---|---|---|---|
| Overall (N = 2012) | In‐person (N = 403) | Hybrid (N = 830) | Remote/Virtual (N = 779) | |||||
| OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | |
| Student learning modality | ‐ | ‐ | ‐ | |||||
| In‐person | Ref. | |||||||
| Hybrid | 0.58 (0.42, 0.80) | .001 | ||||||
| Remote/virtual | 0.50 (0.36, 0.69) | <.001 | ||||||
| Student sociodemographic characteristics | ||||||||
| Gender | ||||||||
| Female | Ref. | Ref. | Ref. | Ref. | ||||
| Male | 0.85 (0.69, 1.05) | .132 | 1.04 (0.60, 1.80) | .902 | 0.74 (0.54, 1.03) | .071 | 0.90 (0.64, 1.26) | .537 |
| Race/ethnicity | ||||||||
| Non‐Hispanic white | Ref. | Ref. | Ref. | Ref. | ||||
| Non‐Hispanic black | 0.80 (0.57, 1.12) | .196 | 0.35 (0.15, 0.80) | .013 | 1.27 (0.72, 2.25) | .404 | 0.72 (0.43, 1.19) | .200 |
| Hispanic | 0.78 (0.60, 1.02) | .068 | 1.27 (0.61, 2.61) | .523 | 0.78 (0.51, 1.19) | .245 | 0.68 (0.45, 1.02) | .061 |
| Non‐Hispanic other* | 1.22 (0.83, 1.77) | .309 | 0.34 (0.13, 0.87) | .025 | 1.50 (0.81, 2.77) | .197 | 1.50 (0.85, 2.65) | .159 |
| School level | ||||||||
| High school (grades 9‐12) | Ref. | Ref. | Ref. | Ref. | ||||
| Middle school (grades 6‐8) | 0.91 (0.73, 1.12) | .368 | 1.19 (0.66, 2.14) | .560 | 0.82 (0.59, 1.14) | .240 | 0.96 (0.68, 1.36) | .825 |
| Student health/behavioral characteristics | ||||||||
| Mental health † | ||||||||
| Has anxiety symptoms | 0.60 (0.44, 0.81) | .001 | 0.67 (0.27, 1.7) | .396 | 0.53 (0.33, 0.84) | .007 | 0.66 (0.41, 1.06) | .082 |
| Has depression symptoms | 0.61 (0.44, 0.85) | .003 | 0.73 (0.27, 2.0) | .547 | 0.92 (0.54, 1.60) | .754 | 0.38 (0.23, 0.60) | <.001 |
| Substance use since pandemic began ‡ | 0.71 (0.53, 0.95) | .022 | 0.60 (0.29, 1.2) | .163 | 0.60 (0.39, 0.92) | .021 | 0.84 (0.53, 1.34) | .459 |
| School‐provided supports | ||||||||
| Received education‐related services § | 1.31 (1.04, 1.65) | .024 | 0.91 (0.48, 1.74) | .783 | 1.33 (0.93, 1.92) | .120 | 1.55 (1.08, 2.22) | .018 |
| Received health‐related services ‖ | 1.36 (0.98, 1.89) | .069 | 1.02 (0.44, 2.33) | .967 | 1.28 (0.77, 2.10) | .340 | 1.47 (0.84, 2.56) | .174 |
Overall model was not subpopulated by learning mode. All models controlled for community characteristics (Census region, locality, Social Vulnerability Index, and SARS‐CoV‐2 transmission level). Significant findings (p < .05) are bolded. Referent group for each mental health measure is “no” (did not report symptoms at level that warranted additional screening). Referent group for the outcome variable, academic grade change, is declined. Referent group for substance use is “no” (did not report any substance use). Referent group for each school‐provided support measure is “no” (did not receive any services of that type).
CI, confidence interval; OR, odds ratio; SY, school year.
Non‐Hispanic other race/ethnicity category includes Asian, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, some other race, or selected more than 1 race category. The Non‐Hispanic other category is not disaggregated due to small cell size generating unstable estimates and to protect confidentiality.
Using the GAD‐2 scale (Generalized Anxiety Disorder), respondents with anxiety symptoms represent those who scored ≥3 for anxiety, indicating a need for follow‐up screening for anxiety. Using the PHQ‐2 scale (Patient Health Questionnaire), respondents with depression symptoms represent those who scored ≥3 for depression, indicating a need for follow‐up screening for depression.
Started or increased use of at least 1 substance (alcohol, tobacco, prescription drug, or non‐prescription drug) to help cope with stress or emotions, taken in a way not recommended by a doctor.
Education‐related services received during SY 2020‐2021 (tutoring, accommodations for assignments, academic support, and/or individual classroom support).
Health‐related services received during SY 2020‐2021 (occupational therapy, speech therapy, and/or behavioral/mental health support).
All findings were considered statistically significant if p‐value <.05.
RESULTS
Table 1 depicts descriptive characteristics of respondents for overall sample and by learning modality (unweighted counts and weighted percentages), including corresponding bivariate associations. Learning modality was significantly associated with academic grade change, gender, race/ethnicity, substance use, receiving school‐provided health‐related services, Census region, locality, and SVI. Among in‐person students, about one‐fifth (19.9%) reported their grades declined compared to prepandemic while 34.4% of remote/virtual students reported their grades declined. Non‐Hispanic white students represented 62.7% of in‐person students but only 39.1% of remote/virtual students. For all other race/ethnic groups, there were greater proportions of students from those groups attending school remotely/virtually, compared to in‐person. Greater proportions of in‐person (19.2%) and hybrid (16.5%) students reported substance use, compared to remote/virtual students (13.5%). Additionally, while 17.1% of in‐person students reported they received health‐related services from school, only 12.8% of hybrid students and 11.5% of remote/virtual students received these services. Students from the South represented the largest group in each learning modality and the distribution of different localities (rural, suburban, urban) was similar for all modalities. Overall, about a third of students (32.6%) were from high SVI counties and county SVI varied across learning modality. In‐person students were primarily from low SVI counties (39.8%) and remote/virtual students were primarily from high SVI counties (39.0%).
Table 2 depicts prevalence estimates of student characteristics and school‐provided supports and academic grade change (unweighted counts and weighted percentages), including corresponding bivariate associations. Learning modality, race/ethnicity, anxiety symptoms, depression symptoms, and substance use were significantly associated with grade change. Among students whose grades declined, 45.6% were remote/virtual students, 41.1% were hybrid students, and 13.3% were in‐person students. With regard to race/ethnicity, non‐Hispanic white students comprised 54.8% of students whose grades stayed the same or improved but only 48.4% of students whose grades declined. The opposite pattern was true for non‐Hispanic black and Hispanic students—there were greater proportions of non‐Hispanic black (14.2%) and Hispanic (29.9%) students in the declined grades group, compared to the same/improved grades group (non‐Hispanic black = 12.3%; Hispanic = 23.8%). For each mental health measure, a greater proportion of students in the group that reported their grades declined reported experiencing anxiety or depression symptoms, compared to those in the same/improved grades group. Finally, 21% of the declined grades group reported substance use compared to only 13.7% of the same/improved grades group.
Results from the multivariable logistic regression models, subpopulated by learning modality, are shown in Table 3. Controlling for community characteristics, significant associations with academic grade change were observed for student characteristics and school‐provided supports. Associations varied depending on learning modality. Regression results for each learning modality are described below. Prevalence estimates and regression results for the community characteristics are provided in Appendix Tables A1 and A2.
In‐Person Learning
Among in‐person students, race/ethnicity was the only measure significantly associated with grade change. When compared to non‐Hispanic white students, the odds of reporting same/improved grades compared to prepandemic were 65% lower among non‐Hispanic black students and 66% lower among non‐Hispanic other race students (p < .05).
Hybrid Learning
Among hybrid students, anxiety symptoms and substance use were the only measures significantly associated with grade change. The odds of reporting same/improved grades among students who reported anxiety symptoms were 47% less than students not reporting anxiety symptoms (p < .01). The odds of reporting same/improved grades among students who reported substance use were 40% less than students who did not report substance use (p < .05).
Remote/Virtual Learning
Having depression symptoms and receiving school‐provided educational services were the only measures significantly associated with grade change. The odds of reporting same/improved grades among students who reported depression symptoms were 62% less than the odds of students did not report depression symptoms (p < .001). Those who received educational services from school had 1.55 times the odds of reporting same/improved grades, compared to students not receiving these services (p < .05).
DISCUSSION
Approximately 20% of students attending school in‐person reported their grades declined since the start of the pandemic, with more students in the hybrid (about 30%) and remote/virtual (34%) groups reporting a decline. These findings are concerning given teachers might have been more lenient with grading during the 2020‐2021 school year, especially with virtual‐only students, 46 , 47 suggesting actual learning loss could be greater.
Public health experts have noted the potential for the pandemic to exacerbate existing racial/ethnic disparities in education and health. 23 Learning modality may be a contributing factor. In a study of 12 US states, large reductions in test scores for the 2020‐2021 school year were observed compared to previous years, and this decline was significantly larger in districts with less access to in‐person schooling. 47 US districts serving mostly black and Hispanic students and districts with high concentrations of limited English learners were less likely to provide primarily in‐person instruction and provided less instruction time in general than schools with lower proportions of minorities and English language learners. 25 In this study, non‐Hispanic white students comprised 53% of the sample but only 39% of virtual/remote learners. The finding that full‐time virtual learning was more prevalent among black and Hispanic students is consistent with other studies. 23 , 48
While grade change was significantly associated with race/ethnicity in bivariate models, adjusted models showed this was only the case for in‐person students, with black and non‐Hispanic students of other races having lower odds of reporting same/improved grades (compared to prepandemic) than white students. One potential explanation that warrants further research is the role of teacher implicit bias to determine if implicit bias played a greater role for in‐person 49 compared to virtual instruction during the pandemic, possibly influencing how much race/ethnicity minority students attending school in‐person felt connected to school. Research indicates that students who feel connected to school and perceive teachers and school rules/policies as fair, have higher academic achievement. 33 These biases might be more likely to emerge when interacting face‐to‐face, and there is some evidence that counties where teachers hold higher levels of implicit and explicit racial bias have larger adjusted white/black test score inequalities. 49
Results consistently reflect that virtual learning (full‐ or part‐time) was challenging for students in all racial/ethnic groups but was disproportionately experienced by racial/ethnic minority students. Among remote/virtual learners, students receiving educational services from school had higher odds of maintaining or improving grades, indicating virtually delivered academic support did help students keep up during the pandemic. However, it is unclear whether students had equitable access to these supports which involves both school‐provision of services and individual capacity to receive (eg, highspeed internet, WiFi‐enabled device, private/dedicated space). Receipt of school‐provided, health‐related services (eg, occupational therapy, speech therapy) was not related to grade change. One possible explanation is that tutoring supports may have been supplemental in some districts and not legally required whereas occupational and speech therapy may have been a part of required Individual Education Plans. We are not aware of other studies addressing the provision of virtual school‐provided learning supports and academic outcomes, although successes and challenges with remote learning for K‐12 schools have been documented. 50 , 51 These results point to the importance of including strategies for continuity in academic support services in school emergency operations plans.
Roughly 1 in 5 students reported currently experiencing symptoms of depression or anxiety, corroborating results from the COVID Experiences Study (COVEX). 24 , 48 The learning experience of students with symptoms of mental health conditions varied by learning modality. Efforts to improve and sustain school connectedness, which has been shown to be protective for adolescent mental health, might help attenuate impacts of learning modality on mental health. 52 Additionally, protective factors not included in our survey (eg, parental supervision, family support/connectedness) may have buffered potentially deleterious effects of disruptions to in‐person schooling on academic achievement.
IMPLICATIONS FOR SCHOOL HEALTH
The COVID‐19 pandemic has resulted in unprecedented disruptions to K‐12 education. This study provides evidence that many students may have been struggling to maintain their academic grades while also grappling with their mental health. As many as 20% of students reported symptoms of anxiety and/or depression and roughly 30% reported their grades had worsened compared to prepandemic, with higher proportions of decline among remote/virtual learners. Helping students to develop positive coping skills and address nonacademic barriers to learning may be important for successful return to in‐person learning. K‐12 schools may find that some student populations have fallen behind academically because of the pandemic, particularly among students who engaged in virtual learning, suggesting additional support and accommodations are needed.
These findings highlight the importance of keeping schools open for in‐person learning, when feasible. However, if schools need to pivot to virtual instruction in response to an emergency, it is critical that K‐12 school administrators have plans in place to lessen detrimental effects on student mental health and academic progress. Ensuring that schools are prepared to offer educational services and learning accommodations virtually might help students at least maintain their grades during such disruptions.
Schools may need to increase their capacity to provide educational supports to students struggling academically, including effective means to identify those with the greatest need. Likewise, additional resources to support and promote mental health and well‐being may be useful, especially for those students who have engaged in remote/virtual learning during the pandemic. The American Rescue Plan and Elementary and Secondary School Emergency Relief Fund 53 presents an opportunity to more equitably strengthen the capacity of educational systems to recover from disruptions related to COVID‐19 and other emergencies. More equitable policies and practices in US schools related to educational and mental health support will further address students disproportionately impacted by the pandemic and continue to strengthen teaching and learning.
Limitations
The following limitations are noted. First, survey data were self‐reported and could reflect social desirability bias. Second, a convenience survey sample was used and may not be representative of all middle and high school students attending K‐12 schools in the US. Third, because the survey was related to COVID‐19 and there was a need to collect data rapidly, some survey items had not been previously evaluated in terms of reliability and validity (we note in the methods any previous validations or use of measures in other research). Fourth, the survey was conducted online so the experiences of students without reliable internet and computer access are not represented. Fifth, this was a cross‐sectional study design and conclusions about causality of associations cannot be drawn. Sixth, grades are subjective measures of performance and teachers could have adjusted their grading methods for students in different learning modalities (as documented elsewhere 24 , 54 ). Seventh, school district‐level SVI data were not available and social vulnerability characteristics may vary throughout a given county (and level of resources available to private schools could also vary). Additionally, since data were collected solely at the student level, results might not fully characterize the extent to which schools provided academic and health support services. Finally, absenteeism, COVID‐19 illness (for students, family members, caregivers), and COVID‐19 deaths (for family members, caregivers) were not collected but could have affected grades.
Conclusions
Overall, larger proportions of students who attended school in‐person full‐time during the 2020‐2021 school year maintained or improved their grades, compared to students attending remotely/virtually (part‐time or full‐time). This finding is concerning as only about 20% of students attended school in‐person full‐time in 2020‐2021. Since virtual learning has been shown to be more prevalent among lower‐income and racial/ethnic minority students, 55 widening disparities in academic achievement following long stretches of remote instruction remains essential to address. 23 , 25
Models examined by learning modality provide tailored insights and have the potential to inform preparedness planning in anticipation of future shifts to virtual learning. School districts with plans to operate virtually in emergency situations in the future may need to be prepared to offer students additional academic support. Furthermore, school administrators, teachers, and other staff may need to be prepared to recognize if students who experience academic grade declines are also experiencing symptoms of depression or anxiety.
While a shift to virtual learning may have been protective against SARS‐CoV‐2 transmission among K‐12 student populations, it has been linked with lower school connectedness 24 which might contribute to academic disengagement. Reduced access to in‐person learning has also been associated with poorer learning and negative mental health and behavioral outcomes in children. 48 , 54 While online teaching and learning has been shown to be effective with trained faculty and high‐quality instructional design (eg, online college/university courses), emergency remote teaching stemming from a crisis can diminish instruction quality. 50
Human Subjects Approval Statement
This activity was determined to meet the definition of research involving human subjects and Institutional Review Board approval was provided by the Advarra Institutional Review Board (See 45 C.F.R. part 46; 21 C.F.R. part 56).
Conflict of Interest
All authors of this article declare they have no conflicts of interest. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Table A1.
Community Characteristics Corresponding to the Geographic Location of Students Ages 13‐19 Attending K‐12 Schools and Academic Grade Change (Declined or Same/Improved) in SY 2020‐2021
| Academic Grade Change*, N, % (95% CI) | |||||||
| Overall, N, % (95% CI) | Declined | Same/Improved | p‐Value | ||||
| Total | 2128 | 632 (29.4%) | 1496 (69.5%) | ||||
| Community characteristics | |||||||
| Census region † | .14 | ||||||
| Midwest | 406 | 20.8 (19.0, 22.8) | 130 | 22.2 (18.9, 25.8) | 276 | 20.3 (18.1, 22.6) | |
| Northeast | 381 | 16.5 (15.0, 18.1) | 116 | 17.1 (14.3, 20.2) | 265 | 16.3 (14.5, 18.2) | |
| South | 863 | 38.5 (36.4, 40.7) | 231 | 34.6 (30.9, 38.5) | 632 | 40.2 (37.6, 42.8) | |
| West | 478 | 24.2 (22.3, 26.2) | 155 | 26.2 (22.7, 30.0) | 323 | 23.3 (21.1, 25.7) | |
| Locality ‡ | .95 | ||||||
| Rural | 421 | 14.1 (12.8, 15.5) | 121 | 13.1 (10.9, 15.6) | 300 | 14.5 (13.0, 16.3) | |
| Suburban | 1075 | 56.4 (54.2, 58.6) | 303 | 54.3 (50.2, 58.3) | 772 | 57.4 (54.7, 60.0) | |
| Urban | 632 | 29.5 (27.5, 31.5) | 208 | 32.7 (29.0, 36.6) | 424 | 28.1 (25.8, 30.6) | |
| Social vulnerability index § , ‖ | .019 | ||||||
| Low | 745 | 35.9 (33.8, 38.1) | 193 | 31.2 (27.5, 35.1) | 552 | 37.9 (35.3, 40.5) | |
| Moderate | 678 | 31.6 (29.6, 33.7) | 213 | 33.8 (30.0, 37.7) | 465 | 30.7 (28.3, 33.2) | |
| High | 705 | 32.5 (30.5, 34.6) | 226 | 35.1 (31.3, 39.1) | 479 | 31.4 (29.0, 34.0) | |
| High days of SARS‐CoV‐2 transmission ¶ , ,‖ | .46 | ||||||
| 0 days | 1238 | 62.2 (60.0, 64.4) | 352 | 60.2 (56.0, 64.3) | 886 | 63.1 (60.4, 65.7) | |
| 1‐7 days | 464 | 22.1 (20.3, 24.1) | 143 | 23.8 (20.4, 27.6) | 321 | 12.4 (19.3, 23.7) | |
| 8‐14 days | 310 | 15.6 (14.0, 17.4) | 95 | 6.0 (13.1, 19.4) | 215 | 15.5 (13.6, 17.6) | |
Table shows unweighted counts (N), weighted overall and column percentages (%), and weighted 95% confidence intervals (CI). Academic grade change represents change in letter grades since before the start of the COVID‐19 pandemic (before February 2020). p‐Values <.05 were considered statistically significant.
SY, school year.
Academic grade change represents change in letter grades since before the start of the COVID‐19 pandemic (before Feb. 2020). Grade change could not be computed for n = 24 survey respondents because they reported “none of these grades” or “not sure” for 1 or both questions about academic grades (overall sample size (2152) minus surveys without grade change information (24) = 2128).
Based on survey respondent's self‐reported state of residence.
Based on survey respondent's self‐reported location of school. This information was missing for n = 188 respondents.
2018 CDC/ATSDR Social Vulnerability Index (SVI) for the county where school is located. Low = counties in bottom one‐third, or tertile, of SVI scores (lowest vulnerability). Moderate = counties in middle tertile of SVI scores. High = counties in top tertile of SVI scores (highest vulnerability).
Could not be computed for n = 188 survey respondents due to missing school location information.
Number of days that the county where the school is located was designated as having a high SARS‐CoV‐2 transmission level (8‐14 days).
Table A2.
Multivariable Logistic Regression Results for Having Same or Improved Academic Grades (Compared to Prepandemic) and Community Characteristics, Subpopulated by Student Learning Modality (In‐Person, Hybrid, or Remote/Virtual) in SY 2020‐2021
| Student Learning Modality | ||||||||
|---|---|---|---|---|---|---|---|---|
| Overall (N = 2012) | In‐person (n = 403) | Hybrid (n = 830) | Remote/virtual (n = 779) | |||||
| OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | OR (95% CI) | p‐Value | |
| Community characteristics | ||||||||
| Census region* | ||||||||
| Midwest | Ref. | Ref. | Ref. | Ref. | ||||
| Northeast | 1.14 (0.81, 1.61) | .440 | 1.56 (0.52, 4.70) | .427 | 1.18 (0.74, 1.88) | .490 | 1.10 (0.59, 2.05) | .755 |
| South | 1.43 (1.06, 1.93) | .021 | 1.56 (0.72, 3.36) | .260 | 1.58 (1.01, 2.46) | 0.045 | 1.42 (0.82, 2.47) | .215 |
| West | 1.30 (0.92, 1.85) | .141 | 1.35 (0.51, 3.59) | .550 | 1.48 (0.88, 2.50) | .144 | 1.23 (0.67, 2.31) | .486 |
| Locality † | ||||||||
| Rural | Ref. | Ref. | Ref. | Ref. | ||||
| Suburban | 0.96 (0.72, 1.28) | .793 | 0.60 (0.29, 1.24) | .167 | 0.91 (0.60, 1.36) | .632 | 1.38 (0.82, 2.31) | .226 |
| Urban | 0.95 (0.69, 1.31) | .760 | 0.56 (0.24, 1.28) | .168 | 1.02 (0.64, 1.64) | .929 | 1.23 (0.71, 2.11) | .461 |
| Social vulnerability index ‡ , § | ||||||||
| Low | Ref. | Ref. | Ref. | Ref. | ||||
| Moderate | 0.75 (0.57, 0.98) | .032 | 1.17 (0.60, 2.32) | .640 | 0.65 (0.44, 0.96) | .031 | 0.79 (0.51, 1.24) | .305 |
| High | 0.72 (0.54, 0.96) | .023 | 0.66 (0.32, 1.35) | .253 | 0.74 (0.48, 1.16) | .193 | 0.74 (0.47, 1.14) | .171 |
| High days of SARS‐CoV‐2 transmission § , ‖ | ||||||||
| 0 days | Ref. | Ref. | Ref. | Ref. | ||||
| 1‐7 days | 0.89 (0.68, 1.17) | .400 | 0.57 (0.28, 1.18) | .130 | 0.72 (0.48, 1.09) | .113 | 1.23 (0.79, 1.92) | .358 |
| 8‐14 days | 0.94 (0.70, 1.25) | .659 | 1.17 (0.51, 2.68) | .705 | 0.82 (0.54, 1.26) | .368 | 0.92 (0.55, 1.53) | .753 |
Overall model was not subpopulated by learning mode. Significant findings (p < .05) are bolded. Models also included student and school characteristics listed in Table 3. Referent group for the outcome variable, academic grade change, is declined.
CI, confidence interval; SY, school year.
Based on survey respondent's self‐reported state of residence.
Based on survey respondent's self‐reported location of school. This information was missing for n = 188 respondents.
2018 CDC/ATSDR Social Vulnerability Index (SVI) for the county where school is located. Low = counties in bottom one‐third, or tertile, of SVI scores (lowest vulnerability). Moderate = counties in middle tertile of SVI scores. High = counties in top tertile of SVI scores (highest vulnerability).
Could not be computed for n = 188 survey respondents due to missing school location information.
Number of days that the county where the school is located was designated as having a high SARS‐CoV‐2 transmission level (8‐14 days).
Fisher HH, Hawkins GT, Hertz M, Sliwa S, Beresovsky V. Student and school characteristics associated with COVID‐19‐Related learning decline among middle and high school students in K‐12 schools. J Sch Health. 2022; 92: 1027‐1039. DOI: 10.1111/josh.13243
Indicates that continuing education hours are available. Visit www.ashaweb.org and click on Continuing Education for more information.
Contributor Information
Holly H. Fisher, Email: hfisher@cdc.gov.
Georgianne T. Hawkins, Email: mtx7@cdc.gov.
Marci Hertz, Email: mvf4@cdc.gov.
Sarah Sliwa, Email: xxh8@cdc.gov.
Vladislav Beresovsky, Email: hvy4@cdc.gov.
REFERENCES
- 1. U.S. Census Bureau . Week 5 Household Pulse Survey: May 28–June 2. Table 2. COVID‐19 Pandemic Impact on How Children Received Education, by Select Characteristics; 2020. Available at: https://www.census.gov/data/tables/2020/demo/hhp/hhp5.html. Accessed July 15, 2022.
- 2. MCH Strategic Data . COVID‐19 IMPACT: School District Operational Status Updates for Spring 2021, current as of 4/12/2021; 2021. Available at: https://www.mchdata.com/covid19/schoolclosings. Accessed July 15, 2022.
- 3. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion program. Health Educ Behav. 1988;15(4):351‐377. [DOI] [PubMed] [Google Scholar]
- 4. Agnafors S, Barmark M, Sydsjö G. Mental health and academic performance: a study on selection and causation effects from childhood to early adulthood. Soc Psychiatry Epidemiol. 2021;56:857‐866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Lounsbury DW, Mitchell SG. Introduction to special issue on social ecological approaches to community health research and action. Am J Community Psychol. 2009;44(3–4):213‐220. [DOI] [PubMed] [Google Scholar]
- 6. Stewart EB. School structural characteristics, student effort, peer associations, and parental involvement: the influence of school‐ and individual‐level factors on academic achievement. Educ Urban Soc. 2008;40(2):179‐204. [Google Scholar]
- 7. Rivkin SG, Schiman JC. Instruction time, classroom quality, and academic achievement. Econ J. 2015;125(588):F425‐F448. [Google Scholar]
- 8. Nelson JR, Benner GJ, Lane K, Smith BW. Academic achievement of K‐12 students with emotional and behavioral disorders. J Except Child. 2004;71(1):59‐73. [Google Scholar]
- 9. Bradley BJ, Greene AC. Do health and education agencies in the United States share responsibility for academic achievement and health? A review of 25 years of evidence about the relationship of adolescents' academic achievement and health behaviors. J Adolesc Health. 2013;52(5):523‐532. [DOI] [PubMed] [Google Scholar]
- 10. Busch V, Loyen A, Lodder M, Schrijvers AJP, van Yperen TA, de Leeuw JRJ. The effects of adolescent health‐related behavior on academic performance: A systematic review of the longitudinal evidence. Rev Educ Res. 2014;84(2):245‐274. [Google Scholar]
- 11. Hawkins GT, Lee SH, Michael SL, et al. Individual and collective positive health behaviors and academic achievement among US high school students, Youth Risk Behavior Survey 2017. Am J Health Promot. 2022;36(4):651‐661. 10.1177/08901171211064496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rasberry CN, Tiu GF, Kann L, et al. Health‐related behaviors and academic achievement among high school students—United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(35):921‐927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Lewallen TC, Hunt H, Potts‐Datema W, Zaza S, Giles W. The whole school, whole community, whole child model: A new approach for improving educational attainment and healthy development for students. J Sch Health. 2015;85(11):729‐739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Michael SL, Merlo AL, Basch CE, Wentzel KR, Wechsler H. Critical connections: health and academics. J Sch Health. 2015;85(11):740‐758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Carminucci J, Hodgman S, Rickles J, Garet M. Student Attendance and Enrollment Loss in 2020–2021. 2021. Available at: https://www.air.org/sites/default/files/2021‐07/research‐brief‐covid‐survey‐student‐attendance‐june‐2021_0.pdf. Accessed November 4, 2021.
- 16. Lewis K, Kuhfeld M, Ruzek E, McEachinet A. Learning During COVID‐19: Reading and Math Achievement in the 2020–21 School Year. Portland, OR: NWEA; 2021. Available at: https://www.nwea.org/content/uploads/2021/07/Learning‐during‐COVID‐19‐Reading‐and‐math‐achievement‐in‐the‐2020‐2021‐school‐year.research‐brief‐1.pdf. Accessed August 15, 2021. [Google Scholar]
- 17. Wodtke GT, Harding DJ, Elwert F. Neighborhood effects in temporal perspective: the impact of long‐term exposure to concentrated disadvantage on high school graduation. Am Sociol Rev. 2011;76(5):713‐736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Woolley ME, Grogan‐Kaylor A, Gilster ME, et al. Neighborhood social capital, poor physical conditions, and school achievement. Child Sch. 2008;30(3):133‐145. [Google Scholar]
- 19. Flanagan BE, Gregory EW, Hallisey EJ, Heitgerd JL, Lewis B. A social vulnerability index for disaster management. J Homel Secur Emer Manage. 2011;8(1):3. [Google Scholar]
- 20. Flanagan BE, Hallisey EJ, Adams E, Lavery A. Measuring community vulnerability to natural and anthropogenic hazards: the Centers for Disease Control and Prevention's social vulnerability index. J Environ Health. 2018;80(10):34‐36. [PMC free article] [PubMed] [Google Scholar]
- 21. Karaye IM, Horney JA. The impact of social vulnerability on COVID‐19 in the U.S.: an analysis of spatially varying relationships. Am J Prev Med. 2020;59(3):317‐325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Nayak A, Islam SJ, Mehta A, et al. Impact of social vulnerability on COVID‐19 incidence and outcomes in the United States. 2020. Available at: https://www.medrxiv.org/content/10.1101/2020.04.10.20060962v2.full.pdf. Accessed August 10, 2022.
- 23. Oster E, Jack R, Halloran C, et al. Disparities in learning mode access among K–12 students during the COVID‐19 pandemic, by race/ethnicity, geography, and grade level—United States, September 2020–April 2021. MMWR Morb Mortal Wkly Rep. 2021;70(11):953‐958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Hertz MF, Kilmer G, Verlenden J, et al. Adolescent mental health, connectedness, and mode of school instruction during COVID‐19. J Adolesc Health. 2022;70(1):57‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Hodgman S, Rickles J, Carminucci J, Garet M. District Approaches to Instruction in 2020–21: Differences in Instructional Modes and Instruction Time Across Contexts. Arlington, VA: American Institutes for Research; 2021. Available at: https://www.air.org/sites/default/files/2021‐07/research‐brief‐covid‐survey‐differences‐instructional‐modes‐june‐2021_0.pdf. Accessed October 29, 2021. [Google Scholar]
- 26. Office of the U.S. surgeon general. In: Protecting Youth Mental Health: The U.S. Surgeon General's Advisory. Washington, DC: U.S. Department of Health and Human Services; 2021. Available at: surgeon‐general‐youth‐mental‐health‐advisory.pdf (hhs.gov). [Google Scholar]
- 27. Substance Abuse and Mental Health Services Administration . Key Substance Use and Mental Health Indicators in the United States: Results From the 2018 National Survey on Drug Use and Health (HHS Publication No. PEP19‐5068, NSDUH Series H‐54). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2019. Available at https://www.samhsa.gov/data. Accessed January 14, 2022. [Google Scholar]
- 28. Breslau J, Lane M, Sampson N, Kessler RC. Mental disorders and subsequent educational attainment in a US national sample. J Psychiatr Res. 2008;42(9):708‐716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Eide ER, Showalter MH, Goldhaber DD. The relation between children's health and academic achievement. Child Youth Serv Rev. 2010;32(2):231‐238. [Google Scholar]
- 30. Olubiyi O, Futterer A, Kang‐Yi CD. Mental health care provided through community school models. J Ment Health Train Educ Pract. 2019;14(5):297‐314. [Google Scholar]
- 31. U.S. Centers for Disease Control and Prevention . Research Brief: Chronic Health Conditions and Academic Achievement; 2017. Available at: https://www.cdc.gov/healthyschools/chronic_conditions/pdfs/2017_02_15‐CHC‐and‐Academic‐Achievement_Final_508.pdf. Accessed January 17, 2022.
- 32. Larson S, Chapman S, Spetz J, Brindis CD. Chronic childhood trauma, mental health, academic achievement, and school‐based health center mental health services. J Sch Health. 2007;87(9):675‐686. 10.1111/josh.12541. [DOI] [PubMed] [Google Scholar]
- 33. Niehaus K, Rudasill KM, Rakes CR. A Longitudinal study of school connectedness and academic outcomes across sixth grade. J Sch Psychol. 2012;50(4):443‐460. 10.1016/j.jsp.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 34. Ali MM, West K, Teich JL, Lynch S, Mutter R, Dubenitz J. Utilization of mental health services in educational setting by adolescents in the United States. J Sch Health. 2019;89(5):393‐401. [DOI] [PubMed] [Google Scholar]
- 35. CDC Foundation . Monitoring School COVID‐19 Prevention Strategies; 2021. Available at: https://www.cdcfoundation.org/monitoring‐school‐covid‐19‐prevention‐strategies. Accessed August 10, 2021.
- 36. U.S. Centers for Disease Control and Prevention . CDC/ATSDR Social Vulnerability Index; 2021. Available at: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html. Accessed November 1, 2021.
- 37. U.S. Centers for Disease Control and Prevention . COVID Data Tracker; 2021. Available at: https://covid.cdc.gov/covid‐data‐tracker/#datatracker‐home. Accessed August 10, 2021.
- 38. Bentley KH, Sakurai H, Lowman KL, et al. Validation of brief screening measures for depression and anxiety in young people with substance use disorders. J Affect Disord. 2021;282:1021‐1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Allgaier A, Pietsch K, Frühe B, Sigl‐Glöckner J, Schulte‐Körne G. Screening for depression in adolescents: validity of the patient health questionnaire in pediatric care. Depress Anxiety. 2012;29(10):906‐913. [DOI] [PubMed] [Google Scholar]
- 40. Richardson LP, McCauley E, Grossman DC, et al. Evaluation of the patient health Questionnaire‐9 item for detecting major depression among adolescents. Pediatrics. 2010;126(6):1117‐1123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Tiirikainen K, Haravuori H, Ranta K, Kaltiala‐Heino R, Marttunen M. Psychometric properties of the 7‐item generalized anxiety disorder scale (GAD‐7) in a large representative sample of Finnish adolescents. Psychiatry Res. 2019;272:30‐35. [DOI] [PubMed] [Google Scholar]
- 42. Keum BT, Miller MJ, Inkelas KK. Testing the factor structure and measurement invariance of the PHQ‐9 across racially diverse U.S. college students. Psychol Assess. 2018;30(8):1096‐1106. [DOI] [PubMed] [Google Scholar]
- 43. Parkerson HA, Thibodeau MA, Brandt CP, Zvolensky MJ, Asmundson GJG. Cultural‐based biases of the GAD‐7. J Anxiety Disord. 2015;31:38‐42. [DOI] [PubMed] [Google Scholar]
- 44. Dumas M, Ellis W, Litt DM. What does adolescent substance use look like during the COVID‐19 pandemic? Examining changes in frequency, social contexts, and pandemic‐related predictors. J Adolesc Health. 2020;67(3):354‐361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. U.S. Centers for Disease Control and Prevention . National Health Interview Survey; 2019. Available at NHIS ‐ 2019 NHIS (cdc.gov). Accessed July 10, 2021.
- 46. Sawchuk, S. Grading students during the coronavirus crisis: What's the right call? Education Week; 2020. Available at: Grading Students During the Coronavirus Crisis: What's the Right Call? (edweek.org). Accessed January 17, 2022.
- 47. Townsley M. Grading principles in pandemic‐era learning: recommendations and implications for secondary school leaders. J Sch Admin Res Develop. 2020;5(S1):8‐14. [Google Scholar]
- 48. Verlenden JV, Pampati S, Rasberry CN, et al. Association of children's mode of school instruction with child and parent experiences and well‐being during the COVID‐19 pandemic — COVID experiences survey, United States, October 8–November 13, 2020. MMWR Morb Mortal Wkly Rep. 2021;70(11):369‐376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Chin MJ, Quinn DM, Dhaliwal TK, Lovison VS. Bias in the air: A nationwide exploration of teachers' implicit racial attitudes, aggregate bias, and student outcomes. Educ Res. 2020;49(8):566‐578. [Google Scholar]
- 50. Hodges C, Moore S, Lockee B, Altruist T, Bond A. The difference between emergency remote teaching and online learning. EDUCAUSE Review; 2020. Available at: https://er.educause.edu/articles/2020/3/the‐difference‐between‐emergency‐remote‐teaching‐and‐online‐learning. Accessed December 1, 2021.
- 51. Halloran C, Jack R, Okun JC, Oster E. Pandemic Schooling Mode and Student Test Scores: Evidence From U.S. States. Cambridge, MA: National Bureau of Economic Research; 2021. 10.3386/w29497. [DOI] [Google Scholar]
- 52. U.S. Centers for Disease Control and Prevention . School Connectedness: Strategies for Increasing Protective Factors among Youth. Atlanta, GA: U.S. Department of Health and Human Services; 2009. [Google Scholar]
- 53. U.S. Department of Education . American Rescue Plan of 2021 Elementary and Secondary School Emergency Relief. Washington, DC: Office of Elementary & Secondary Education; 2021. Available at:. https://oese.ed.gov/offices/american‐rescue‐plan/american‐rescue‐plan‐elementary‐and‐secondary‐school‐emergency‐relief/ Accessed January 16, 2022. [Google Scholar]
- 54. Johnson S. California Teachers Grapple With Grading Nearly a Year After Initial School Closures. February 9; 2021. EdSource: Highlighting Strategies for Student Success. Available at: https://edsource.org/2021/california‐teachers‐grapple‐with‐grading‐nearly‐a‐year‐after‐initial‐school‐closures/648376.
- 55. Loades ME, Chatburn E, Higson‐Sweeney N, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID‐19. J Am Acad Child Adolesc Psychiatry. 2020;59(11):1218‐1239. [DOI] [PMC free article] [PubMed] [Google Scholar]