

Abstract
In the face of the first wave of COVID‐19 contagion, citizens all over the world experienced concerns for their safety and health, as well as prolonged lockdowns – which brought about limitations but also unforeseen opportunities for personal growth. Broad variability in these psychological responses to such unprecedented experiences emerged. This study addresses this variability by investigating the role of personal and community resilience. Personal resilience, collective resilience, community disaster management ability, provided information by local authorities, and citizens' focus on COVID‐19‐related personal concerns and lockdown‐related opportunities for personal growth were detected through an online questionnaire. Multilevel modelling was run with data from 3,745 Italian citizens. The potential of personal resilience as a driver for individuals to overcome adverse situations with positive outcomes was confirmed. Differently, the components of community resilience showed more complex paths, highlighting the need to pay more attention to its role in the face of far‐reaching adverse events which hardly test individuals' as well as communities' adaptability and agency skills. The complexities linked to the multi‐component and system‐specific nature of resilience, as well as potential paths towards making the most out of citizens' and communities' ones, emerge. The theoretical and practical implications are discussed.
Keywords: community disaster management, community resilience, COVID‐19, multilevel modelling, pandemic, personal resilience
1. INTRODUCTION
Coronavirus disease 2019 (COVID‐19) outbreak has represented a worldwide emergency (World Health Organization, 2020a) since the first months of 2020. Italy, where the present study was carried out, was one of the most severely hit countries during the first wave of COVID‐19 infections. In the first days of March 2020, the Italian government issued a nationwide lockdown as an attempt to slow down the trend of infections (Presidenza del Consiglio dei Ministri, 2020); it was partially eased on May fourth, 2020, according to the infection rates. Despite the uniformity of stay‐at‐home orders, each Italian province – that is, each administrative district, which consists of a plurality of adjoining municipalities – suffered different severities of local infections during the first wave of contagion (Istat & Iss, 2020) and could only rely on its own local assets (e.g., healthcare structures, hospitals, healthcare professionals) to face the infections. Due to this, during this first stage of the emergency provinces represented the most relevant communities of reference in citizens' experience as to both the current concerns for their safety and health and the foreseen opportunities for personal growth. Consistently, during these months information about the incidence of COVID‐19 was spread both by National government and by Regional authorities. While National‐level communications informed about the impact of the pandemic over the National Health System and across regions, Regional‐level ones reported more detailed information about the local epidemiological and health structures status (that is, across the provinces of that Region).
As far as needed, lockdown measures – kept for a prolonged time – represented an unprecedented experience in citizens' lives and caused disruptive changes in individual and community activities, relationships, sensemaking processes and habits (e.g., De Vincenzo, Serio, Franceschi, Barbagallo, & Zamperini, 2022; Demertzis & Eyerman, 2020; Gatti & Procentese, 2021; Horton, 2020; Procentese, Gatti, & Ceglie, 2021). They brought about several psychological consequences, among which anxiety and depression stemmed (Pancani, Marinucci, Aureli, & Riva, 2021; Salari et al., 2020; Vindegaard & Benros, 2020), along with more pessimistic future perspectives and concerns for current circumstances and for the opportunities for personal growth (Procentese et al., 2021; Procentese, Gatti, & Ceglie, 2021; Torales, O'Higgins, Castaldelli‐Maia, & Ventriglio, 2020; Varga et al., 2021). However, some positive and adaptive reactions aimed at coping with these needed restrictions emerged too (Asmundson, Paluszek, & Taylor, 2021; Gattino et al., 2022; Migliorini et al., 2021; Procentese, Esposito, et al., 2021; Tamiolaki & Kalaitzaki, 2020), suggesting that COVID‐19 pandemic could have also led to post‐traumatic personal growth (e.g., Jenkins et al., 2021; Ulset & von Soest, 2022), which consists in positive psychological changes in the face of traumatic experiences (Tedeschi & Calhoun, 2004). Indeed, during the enforcement of stay‐at‐home orders individuals endeavoured to self‐distract, to engage in new activities and hobbies, and to make the most out of that unforeseen experience by relying on their own assets (e.g., Gaboardi et al., 2022; Procentese, Esposito, et al., 2021) as well as on community‐related ones (e.g., Gattino et al., 2022; Migliorini et al., 2021; Procentese, Capone, Caso, Donizzetti, & Gatti, 2020). Furthermore, the changes imposed by COVID‐19‐related experience with the social restrictions have also led to a reduction of daily stress and sensory exposure and changed family routines and relationships. In some cases, these changes seemed to reduce mental illness symptoms and even improve well‐being (Dvorsky, Breaux, & Becker, 2020) by offering different opportunities for daily positive experiences. Overall, this crisis may have provided citizens with a unique window of unforeseen opportunities.
Altogether, broad inter‐individual differences were noticed as to the psychological reactions to lockdown measures and their impact on individuals' and communities' lives, highlighting a selective effect of lockdown measures, which may have been linked to individual as well as contextual‐related factors (Gaboardi et al., 2022; Kimhi, Marciano, Eshel, & Adini, 2020; Prati & Mancini, 2021). For example, essential workers – that is, individuals having acknowledged reasons to go out of their houses at least for some hours a day during the lockdown – showed less mental health issues compared to non‐essential workers – that is, individuals being required to comply with stay‐at‐home orders with no exceptions – during strict lockdown months (Yue, Lee, Xiao, & Zhang, 2021). However, explanations for this selective effect are not available yet.
Building on this, the present study endeavours to address this gap by deepening the role resilience may have played, since it has been suggested as a possible explanation for the selective effect of lockdown experience (Lenzo et al., 2020; Mancini, 2020; Prati & Mancini, 2021). It will specifically consider the complexities linked to the psychological consequences of COVID‐19‐related lockdown – which represents a timely and worthwhile issue due to the persistent and cyclical nature of the ongoing pandemic (Gatti & Procentese, 2021) – in a twofold way. First, it focuses on both negative (COVID‐19‐related personal concerns) and positive (lockdown‐related opportunities for personal growth) perceptions stemming from lockdown experience, as an attempt to further unravel its selective effect. Second, it adopts a multilevel perspective to adequately tackle the different levels that were implied in managing these unprecedented emergency circumstances by taking into account individual, provincial and Regional characteristics at the same time. That is, it deepens personal and community resilience, as both could have been related to the above‐mentioned selective effect of lockdown measures (Kimhi et al., 2020; Prati & Mancini, 2021). Indeed, recent studies suggested that higher personal resilience might have associated to less concerns about the effect of COVID‐19 pandemic over one's health and safety (Killgore, Taylor, Cloonan, & Dailey, 2020; Megías‐Robles, Gutiérrez‐Cobo, Cabello, Gómez‐Leal, & Fernández‐Berrocal, 2022) as well as to perceived post‐traumatic growth in the face of COVID‐19 pandemic (Baños et al., 2022; Hyun et al., 2021). In the same vein, other studies showed that individuals being members of communities playing out a resilient management of the pandemic were less likely to experience higher rates of concerns with reference to the pandemic and more likely to functionally adapt to the new life circumstances brought about by it (Wang et al., 2020).
To authors' best knowledge, this is one of the first studies deepening resilience not only with reference to different systems (that is, individuals and communities) but also by considering them as characteristics which attain to different, nested levels (that is, individuals are nested into their communities, which makes the members of the same community non‐independent; Bronfenbrenner, 1979; Hox, 2010; Lewin, 1951).
2. PERSONAL AND COMMUNITY RESILIENCE
The ability of individuals and social groups to adjust and possibly progress in the aftermath of stressful events has been referred to as resilience (Norris, Stevens, Pfefferbaum, Wyche, & Pfefferbaum, 2008). Over time, the concept of resilience has enlarged its focus from single persons recovering from a trauma to different kinds of social groups – for example, families (e.g., Walsh, 2003), organizations (e.g., Kendra & Wachtendorf, 2003), local communities (e.g., Kimhi & Shamai, 2004; Norris et al., 2008; Sonn & Fisher, 1998). Indeed, resilience represents a complex construct, requiring different levels of analysis to be adequately addressed (Norris et al., 2008). For example, not everyone living in a resilient community is resilient in turn, nor a community whose members are resilient is resilient itself for sure. That is, despite their similarities, personal/psychological and community resilience represent linked yet not overlapping constructs (Berkes & Ross, 2013; Pfefferbaum, Reissman, Pfefferbaum, Klomp, & Gurwitch, 2008; Ungar, 2011).
Personal/psychological resilience refers to the intrapersonal and interpersonal attributes, abilities and competencies that enable individuals to proactively adjust to changes and even adversities (Cacioppo, Reis, & Zautra, 2011; Zautra, Hall, & Murray, 2010) by accessing and activating the needed resources (Ungar, 2011). It helps maintaining a good and adaptive functioning and achieving a successful adaptation when in need to face challenging or threatening circumstances (Callegari et al., 2016; Sheerin et al., 2018). Overall, resilient individuals show more optimism, flexibility, adaptive coping strategies and strength under adverse circumstances (Callegari et al., 2016).
Personal resilience showed its protective role under stressful circumstances even during broad emergencies (e.g., Williams & Drury, 2009) and with specific reference to COVID‐19 pandemic (Giovannini, Benczur, Campolongo, Cariboni, & Manca, 2020; Lenzo et al., 2020; Migliorini et al., 2021; Procentese, Gatti, & Ceglie, 2022a, 2022b; Roma et al., 2020). Specifically, it can be particularly important in reducing the negative effects of concerns and perceived fears, since the ability to cope with and recover from stress can shield individuals from excessively worrying about the chance to get infected or the effects of lockdown measures. Studies about the influence of personal resilience on COVID‐19‐related concerns are limited, but empirical evidence suggests that individuals with higher resilience showed decreased concerns about the contagion and lower worries about the effects of COVID‐19 pandemic, which makes them less vulnerable to pandemic‐specific distress (Killgore et al., 2020; Megías‐Robles et al., 2022). Furthermore, psychological resilience has also been linked to the process of posttraumatic growth, in which individuals experience positive transformations following adversity (Bernstein & Pfefferbaum, 2018; Levine, Laufer, Stein, Hamama‐Raz, & Solomon, 2009). Benefit finding, or the act of finding positive changes to one's life as a result of a traumatic event, is a particularly important coping strategy for personal growth (Felix et al., 2015; Folkman, 2008). Specifically, personal resilience can represent an important component in the adoption of a response to the COVID‐19 pandemic characterized by perceived post‐traumatic growth (Baños et al., 2022; Hyun et al., 2021), since those who report greater resilience and ability to recover from stressful experiences could be more likely to find positive possibilities in the context of the pandemic.
Diversely, community resilience is conceived as the collective ability of a social system to respond to changes and cope with significant stresses and challenges (Wilson, 2012). It is a system‐level concept (Pfefferbaum, Van Horn, & Pfefferbaum, 2017) that associates to increased local support, resources and adequate communication, and decreased traumas, as well as to the opportunities for community members to engage in collective actions and achieve positive outcomes in the face of challenging circumstances (Norris et al., 2008; Patel, Rogers, Amlôt, & Rubin, 2017; Ungar, 2011). However, community resilience is a complex and multidimensional construct (Cohen et al., 2016) encompassing several dimensions (Bonanno, Romero, & Klein, 2015; Lyons, Fletcher, & Bariola, 2016). That is, other elements should be addressed along with the shared perceptions about that community's collective ability to thrive and bounce back from challenging events: community shared representations about (a) the ability of that community to plan and play out effective measures to deal with specific disasters and (b) the adequacy and accurateness of the information provided by local authorities (Norris et al., 2008; Pfefferbaum et al., 2013; Pfefferbaum, Pfefferbaum, Nitiéma, Houston, & Van Horn, 2014). Indeed, obtaining accurate and clear information about the adverse circumstances to be faced by community leaders allows individuals to engage in critical reflexive processes (Pfefferbaum et al., 2013) and to be aware of the risks, how to reduce them, and the still available opportunities (Norris et al., 2008). Consistently, the WHO suggested people under lockdown to seek information only from trusted sources and avoid uncertain ones (WHO, 2020b). Along with an adequate communication, perceiving that one's community is concretely able to prevent specific disasters as well as prepared to face them, recover from them and mitigate their aftermaths should they happen is critical to post‐disaster community and individual health, uncertainty reduction and well‐being (Menoni & Schwarze, 2020; Norris et al., 2008).
Overall, community resilience allows to mitigate the negative impact of stressful or challenging circumstances at both individual and community levels (Chandra et al., 2010; Plough, Bristow, Fielding, Caldwell, & Khan, 2011). Its protective role has been mainly investigated with reference to far‐reaching events that trouble societies (e.g., natural disasters, terroristic attacks, war) (Ostadtaghizadeh, Ardalan, Paton, Jabbari, & Khankeh, 2015; Paton, Millar, & Johnston, 2001) whereas relatively less attention has been destined to its role in dealing with stressful circumstances whose impact is more gradual and chronic (e.g., unemployment, poverty, ageing, immigration) (Verbena, Rochira, & Mannarini, 2021) – as it was the case for COVID‐19 pandemic. With specific reference to the latter, recent studies showed that individuals obtaining accurate information about it and perceiving their community as resilient and able to manage the pandemic were less likely to experience higher rates of psychological distress and concerns with reference to it and more likely to functionally adapt to the new life circumstances brought about by the pandemic by detecting opportunities for personal growth (Brooks et al., 2020; Wang et al., 2020).
3. RATIONALE FOR THE STUDY
Building on the acknowledgment that COVID‐19‐related lockdown has had a selective impact across individuals (Prati & Mancini, 2021), this study aims at further investigating such variability in the psychological responses to this measure in terms of (a) current concerns for one's safety and health, and (b) expectations about the lockdown as a source of opportunities for personal growth. The role of both personal and province community resilience – unpacked into community collective resilience, community ability to manage that specific emergency, and Institutional provision of adequate information about the latter (Norris et al., 2008; Pfefferbaum et al., 2013, 2014) – is addressed (see Figure 1), since resilience was suggested as a possible path towards the different effects of lockdown across individuals (Lenzo et al., 2020; Prati & Mancini, 2021).
FIGURE 1.
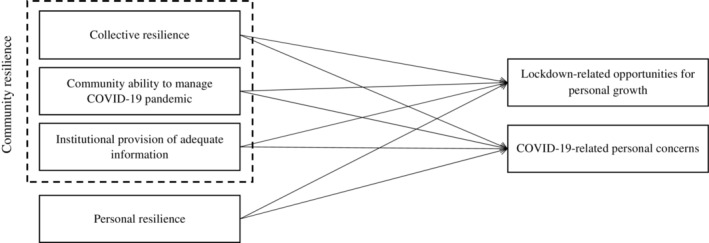
Theoretical model. The closeness to COVID‐19 was included as the individual‐level control variable, the standardized number of COVID‐19‐related deaths per province as the province‐level one.
A multilevel perspective was adopted as the most suitable due to the complexities linked to the construct of resilience (Norris et al., 2008) and to the management of the first months of pandemic in Italy. Indeed, since nationwide stay‐at‐home orders were joined by the management of the health emergency at province level and by the spread of updated information about the latter at Regional level, the inter‐individual variability in coping with COVID‐19 outbreak and the related lockdown cannot be addressed only by referring to individual attitudes, but rather requires to consider how the emergency was managed at province level and how the information campaign was run at Regional level too. That is, the different levels implied in the management of the emergency in Italy – as described in the introduction – made citizens living in the same province non‐independent as to pandemic circumstances (Bronfenbrenner, 1979; Hox, 2010; Lewin, 1951). Overall, the way citizens represented the impact of the emergency over their present and future lives may have been associated not only to their own resources but also to some contextual assets (Kimhi et al., 2020; Prati & Mancini, 2021).
As to the individual level, personal resilience already showed its buffer effect in pursuing individual successful functioning and reducing negative outcomes despite the challenging circumstances during COVID‐19 pandemic (Giovannini et al., 2020; Migliorini et al., 2021; Procentese et al., 2022a, 2022b). Furthermore, it already showed an association with individuals' focus on the opportunities for posttraumatic growth too (Bernstein & Pfefferbaum, 2018; Levine et al., 2009). Building on this, individuals being more able to functionally adapt to adverse circumstances and stressful changes – that is, more resilient (Callegari et al., 2016) – may have adapted to the new life conditions brought about by COVID‐19‐related lockdown in an easier way, mainly focusing on the opportunities for personal growth stemming from the forcibly different habits and routines (e.g., being able to make up for the lost time in family and friends relationships, being more aware of the time they spent online) rather than on safety‐ and health‐related concerns:
personal resilience negatively associates with COVID‐19‐related personal concerns (H1a) and positively associates with lockdown‐related opportunities for personal growth (H1b).
At the community level, based on the above‐mentioned characteristics of the management of the first stage of the pandemic in Italy, province communities were taken into account as the units of analysis since each Italian province suffered different severities of local infections during the first wave of contagion (Istat & Iss, 2020) and could rely on its own local assets (e.g., healthcare structures, hospitals, healthcare professionals) to face the infections. Thus, with reference to the present study, province community resilience deserves specific attention. Building on the above‐detailed literature review, it is hypothesized that in province communities represented as more resilient – that is, (a) accurate information is spread by Regional Institutions, (b) local authorities are perceived as able to manage COVID‐19 emergency, and (c) province communities are represented as able to face challenging circumstances at large – citizens may have felt less exposed to COVID‐19‐related health‐ and safety‐related threats and may have focused more on making the most out of lockdown experience. However, as mentioned above, during the first stage of COVID‐19 pandemic updated information about the epidemiological and health structures situation in each province was spread by Regional authorities, thus Regional authorities are taken into account when it comes to the solely communication provision. Overall, the following hypotheses are added:
citizens' representations about their province community collective resilience (H2a) and ability to manage COVID‐19 pandemic (H2b) and about the information provided by local Institutions (H2c) negatively associate with their COVID‐19‐related personal concerns.
citizens' representations about their province community collective resilience (H3a) and ability to manage COVID‐19 pandemic (H3b) and about the information provided by local Institutions (H3c) positively associate with their focus on lockdown‐related opportunities for personal growth.
Since community resilience relies on shared beliefs and representations (Bonanno et al., 2015; Ungar, 2011) and builds upon culturally embedded patterns of interdependence allowing the community and its members to adapt to changes and find new balance (Lyons et al., 2016; Ungar, 2011), a multiple informant approach was adopted. Indeed, it allows to collect citizens' shared representations about their community by gathering data from several members of the same community and aggregating them into a unique, community‐level, variable. This allowed to detect the shared representations about province community assets (that is, level 2 variables) without reducing them to individual perceptions (Lanz, Sorgente, & Tagliabue, 2018; van Bruggen, Lilien, & Kacker, 2002).
Lastly, the perception of susceptibility to COVID‐19 may have overwhelmed citizens, impacting their current concerns and ability to rather focus on the foreseen opportunities for personal growth (Barni et al., 2020; Fiorillo et al., 2020; Prati & Mancini, 2021; Rochira et al., 2022). Thus, the perception of susceptibility to COVID‐19 was taken into account as a control variable at both individual (i.e., knowing someone who got infected with COVID‐19) and province (i.e., the severity of local COVID‐19 impact, as reported by the Istat and Iss report, 2020) levels.
4. METHOD
4.1. Participants and procedures
A questionnaire was spread online during Italian nationwide lockdown (between March and April 2020), consistently with the National restrictions due to COVID‐19 pandemic. Word of mouth was used, since respondents were invited to contact their family and friends to ask them to complete the questionnaire. Participation was voluntary, participants received no compensation for it. The questionnaire was introduced with an explanation about confidentiality issues. Participants had to express their informed consent by putting a tick in a box to access the questionnaire. No IP addresses or identifying data were retained. Ethical approval was obtained from the Università degli Studi di Bologna Institutional Review Board for all aspects of the current research.
Respondents were 3,745 Italian citizens (69.4% female) aged between 18 and 84 (M = 39.84; SD = 14.24). They lived in 38 different provinces located in 12 Regions from the North (66.9%), Centre (4.3%), and South (28.8%) of Italy; the average province group size is 98.55 (SD = 158.75) participants per province. Most of the participants (72%) did not know someone who had been infected with COVID‐19.
4.2. Measures
The questionnaire included a socio‐demographic section, followed by these specific measures.
4.2.1. Individual dimensions
Personal resilience
The Italian version of the 14‐item Resilience Scale (Callegari et al., 2016) was used. It includes 14 items (e.g., “When I am in a difficult situation, I can usually find my way out of it.”) to be rated on a 5‐point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
COVID‐19‐related personal concerns
Five items (e.g., “The possibility of being infected”) from Rochira et al. (2022) were used to detect respondents' concerns related to COVID‐19 outbreak. Respondents were asked to rate how much each of the mentioned COVID‐19‐related aspects worried them on a 5‐point Likert scale (1 = Nothing; 5 = Completely).
Lockdown‐related opportunities for personal growth
Five items about potential enrichments and positive outcomes stemming from lockdown experience (e.g., “I will be able to use technologies more competently”) from Gattino et al. (2022) were used. Respondents had to rate their agreement with each statement on a 5‐point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
Closeness to COVID‐19
A dichotomous single‐item was used to detect whether respondents knew someone (e.g., friends, relatives) who tested positive for COVID‐19 (0 = No; 1 = Yes).
Province
Respondents were asked to indicate the Italian province where they lived. When this answer was missing, data were excluded from the analyses due to the impossibility of determining where to nest them.
4.2.2. Community dimensions
Province collective resilience
The Fletcher‐Lyons collective resilience scale (Lyons et al., 2016) was used. It includes five items (e.g., “If challenges arise for my community as a whole, we are able to actively respond to those challenges”) and respondents were asked to rate each one on a 5‐point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
Province community ability to manage COVID‐19 pandemic
The disaster management subscale of the CART – Community Advancing Resilience Toolkit (Pfefferbaum et al., 2013, 2014) was used with specific reference to COVID‐19 pandemic. It includes four items (e.g., “My community can provide adequate emergency services in times of need”) to be referred to the ongoing COVID‐19 emergency and rated on a 5‐point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
Information about COVID‐19 pandemic provided by local institutions
The institutional information and communication subscale of the CART – Community Advancing Resilience Toolkit (Pfefferbaum et al., 2013, 2014) was used with specific reference to COVID‐19 pandemic. It includes four items (e.g., “During COVID‐19 emergency, the Institutions provide clear indications on what to do”) to be rated on a 5‐point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
COVID‐19‐related deaths per province
For each province, the standardized number of COVID‐related deaths between January and May 2020 was obtained from the latest Istat and Iss report (2020).
4.3. Data analyses
4.3.1. Preliminary analyses
Several measurement models were compared using Structural Equation Modelling (SEM) to ensure that respondents discriminated among the different constructs involved in the study. Specifically, the six‐factor model – that is, the one in which all the constructs loaded on different latent variables as hypothesized (see Figure 1) – was compared to: (1) a one‐factor model (with all items loading on the same latent variable); (2) a three‐factor model (all province community resilience dimensions collapsed into a unique latent variable, personal resilience as a separate latent variable, and the items for the two outcomes loading on a unique latent variable about the psychological reactions to lockdown orders); (4) a four‐factor model (overall province community resilience as a unique latent variable, personal resilience as a separate latent variable and the two outcomes as two different latent variables). To evaluate each model fit, the Comparative Fit Index (CFI), the Tucker‐Lewis index (TLI), the Root Mean Square Error of Approximation (RMSEA) and its 90% confidence interval (CI), and the Standardized Root Mean square Residual (SRMR) were observed (MacCallum & Austin, 2000). For CFI and TLI, values equal to or greater than .90 and .95, respectively, indicate good or excellent fit; for RMSEA and SRMR, values equal to or smaller than .06 and .08, respectively, indicate good or reasonable fit. Furthermore, the Akaike information criterion (AIC) was used to determine which model best fit the data: the lower the value the better the fit. The six‐factor model was expected to be the one better fitting the data (Figure 2).
FIGURE 2.
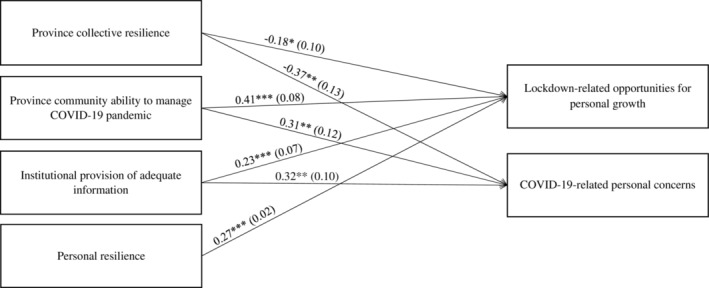
Results of the random intercept‐only model with level 2 predictors (M4). n = 3,745. ***p < .001 (2‐tailed); **p < .01 (2‐tailed); *p < .05 (2‐tailed). Unstandardized effects (B) are shown, standard errors (SE) are in brackets. Only the significant effects are shown. The closeness to COVID‐19 was included as the individual‐level control variable, the standardized number of COVID‐19‐related deaths per province as the province‐level one. For a comprehensive overview of the results see Table 3.
The reliability of each measure was checked through Cronbach's alpha (α).
4.3.2. Hypotheses testing
To test H1, a multiple regression model was run using Ordinary Least Squares (OLS) path analysis. The presence of outliers or influential cases was checked through the leverage value and Cook's D (Cousineau & Chartier, 2010). Personal resilience was used as the independent variable, COVID‐19‐related personal concerns and lockdown‐related opportunities for personal growth as the dependent ones. The closeness to COVID‐19 was included as a dummy control variable (0 = No; 1 = Yes).
As of H2 and H3, a multilevel path analysis was run following a stepwise procedure (Hox, 2010), including individual (first level, n = 3,745) and province (second level, n = 38, Maas & Hox, 2005) levels. Since a multiple informant approach was used to detect level 2 variables, level 2 scores were obtained by averaging the answers of the respondents from the same province. Furthermore, since in Italy information about the local epidemiological situation in provinces was spread at the regional level, the scores for this variable were averaged within Regions – that is, provinces belonging to the same Region had the same average score. Intra‐class Correlation (ICC) and Design Effect (DEFF) coefficients were observed as inter‐rater agreement indices (Lanz et al., 2018). Community‐level variables were grand mean centred while the individual level predictor was group mean centred (Enders & Tofighi, 2007). Maximum likelihood robust (MLR) was used as the estimator. First, a baseline model (M1) was run with no predictors to test whether the outcome variables showed differences across communities. Then, personal resilience was included as the individual‐level predictor to test its effects in addition to the clustering one (M2). The third model (M3) tested whether the effect of the individual‐level predictor on the outcomes – that is, COVID‐19‐related personal concerns and lockdown‐related opportunities for personal growth – differed across provinces – that is, whether the slopes varied across them. In the fourth model (M4), province‐level predictors – that is, province collective resilience, province ability to manage COVID‐19 pandemic and local provision of information about the pandemic – were added. To control for the perception of susceptibility to COVID‐19, the closeness to COVID‐19 was included in all the models as the individual‐level control variable and the standardized number of COVID‐19‐related deaths per province as the province‐level one.
5. RESULTS
5.1. Preliminary results
The six‐factor measurement model, where all the items loaded on their specific latent variables as hypothesized, showed a better fit, AIC = 321,650.97, CFI = 0.91, TLI = 0.90, RMSEA = 0.044, 90% CI [0.043, 0.046], SRMR = 0.04, than the above‐mentioned (1) one‐factor model, AIC = 339,592.91, CFI = 0.56, TLI = 0.53, RMSEA = 0.098, 90% CI [.097, 0.099], SRMR = 0.11, (2) three‐factor model, AIC = 328,385.45, CFI = 0.78, TLI = 0.76, RMSEA = 0.07, 90% CI [0.068, 0.071], SRMR = 0.07 and (3) four‐factor model, AIC = 327,056.28, CFI = 0.81, TLI = 0.79, RMSEA = 0.065, 90% CI [0.064, 0.067], SRMR = 0.06; thus, it was used for the subsequent analyses.
Cronbach's alphas and level 1 and 2 descriptive statistics are summarized in Table 1. Despite the low ICCs, DEFFs were always broadly higher than 2, suggesting it was worthwhile and meaningful to consider the nested structure of data (Muthen & Satorra, 1995; Snijders & Bosker, 2012). This was also consistent with the theoretical model of resilience underlying the study (Norris et al., 2008) and with the nested nature of the data (Bronfenbrenner, 1979; Lewin, 1951) – which both represent valuable, relevant and sufficient reasons to run multilevel analyses regardless of low ICC values (Nezlek, 2008). Indeed, “the fact that there is little or no between‐group variance in a measure does not mean that the relationship between this measure and another measure is the same across all groups, something that is assumed if one conducts an analysis that ignores the grouped structure of the data” (Nezlek, 2008, p.857); thus, a multilevel approach should be preferred when working with nested data. Consistently, level 1 and 2 correlations are shown in Table 2.
TABLE 1.
Summary of reliability coefficients and level 1 and 2 descriptive statistics for all the study variables
| Variables | α | ICC | DEFF | M | SD | |
|---|---|---|---|---|---|---|
| Level 1 | Level 2 | |||||
| 1. COVID‐19‐related personal concerns | .72 | – | – | 3.28 a | 0.69 | – |
| 2. Lockdown‐related opportunities for personal growth | .68 | – | – | 3.43 a | 0.64 | – |
| 3. Personal resilience | .88 | – | – | 4.00 a | 0.52 | – |
| 4. Closeness to COVID‐19 (1 = yes) | – | – | – | 0.28 b | 0.45 | – |
| 5. Province collective resilience | .88 | .04 | 5.19 | 3.59 a | 0.71 | 0.14 |
| 6. Province community ability to manage COVID‐19 pandemic | .89 | .02 | 3.05 | 3.48 a | 0.83 | 0.15 |
| 7. Information provided by local institutions | .79 | .05 | 6.17 | 3.30 a | 0.82 | 0.18 |
| 8. COVID‐related deaths per province | – | – | – | 52.50 c | – | 54.29 |
Note: n = 3,745. Province level values for variables 1 to 4 are not included because they have been used only as individual level variables; individual level values for variable 8 are not included because this variable is a province‐level one only.
Abbreviations: α = Cronbach's alpha; DEFF = Design Effect; ICC = Intra‐class Correlation; M = mean; SD = standard deviation.
1–5 range scale.
0–1 range scale.
3.30–278.10 range scale.
TABLE 2.
Summary of level 1 and 2 correlations for all the study variables
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. COVID‐19‐related personal concerns | – | – | – | – | −.06*** a | .116*** a | .146*** a | −.093*** a |
| 2. Lockdown‐related opportunities for personal growth | .255*** | – | – | – | −.015 a | .120*** a | .110*** a | −.055*** a |
| 3. Personal resilience | .01 | .234*** | – | – | .035* a | .098*** a | .033* a | −.009 a |
| 4. Closeness to COVID‐19 (1 = yes) | −.058*** | −.026 | −.004 | – | .179*** a | −.083*** a | −.255*** a | .312*** a |
| 5. Province collective resilience | −.034* | .152*** | .269*** | .043** | – | .320*** | −.098*** | .383*** |
| 6. Province community ability to manage COVID‐19 pandemic | .058*** | .245*** | .246*** | −.011 | .526*** | – | .495*** | −.206*** |
| 7. Information provided by local institutions | −.014 | .150*** | .211*** | −.08*** | .306*** | .364*** | – | −.610*** |
| 8. COVID‐related deaths per province | – | – | – | – | – | – | – | – |
Note: N = 3,745. Individual‐level correlation coefficients are below the diagonal, while province‐level ones are above it. Province‐level correlations among variables 1 to 4 are not included because variables 1 to 4 were only used as individual level ones; individual level values for variable 8 are not included because this variable is only a province‐level one.
***p < .001 (2‐tailed); **p < .01 (2‐tailed); *p < .05 (2‐tailed).
These values refer to the correlations between individual level (rows 1–4) and province‐level (columns 5–8) variables.
5.2. Hypotheses testing
As of H1, personal resilience showed a significant, positive association with lockdown‐related opportunities for personal growth, B = 0.28, SE = 0.02, p < .001, but no association with COVID‐19‐related personal concerns, B = 0.01, SE = 0.02, p = .55, supporting H1b but not H1a. Conversely, the closeness to COVID‐19 significantly associated with COVID‐19‐related personal concerns, B = −0.09, SE = 0.02, p < .001, but not with lockdown‐related opportunities for personal growth, B = −0.04, SE = 0.02, p = .11. There were no outliers and/or influential cases affecting the analyses, with the leverage value being always lower than .009 and Cook's D always lower than .01.
Multilevel results are summarized in Table 3. The baseline model (M1) showed that the mean scores for both COVID‐19‐related personal concerns and lockdown‐related opportunities for personal growth randomly varied across provinces, even though the low ICCs suggested that only a small part of both variances was explained by level 2 clustering. However, DEFFs were higher than 2 for both variables (Muthen & Satorra, 1995). The random intercept‐only model (M2) confirmed that personal resilience had a significant, positive effect on lockdown‐related opportunities for personal growth but no relationship with COVID‐19‐related personal concerns; however, no increases in ICC and DEFF coefficients emerged for both the dependent variables, suggesting that some other variable may have played a stronger role as to their variability. Furthermore, the intercept significant random variances confirmed that both the outcomes still randomly varied across provinces. In the random slope model (M3), both the slope random variances were non‐significant, indicating that the two level 1 relationships did not randomly vary in strength across provinces; the intercept random variances were still significant for both the dependent variables. In the last model (M4), all level 2 predictors showed significant associations with both lockdown‐related opportunities for personal growth and COVID‐19‐related personal concerns. Partially unexpectedly, all these associations were positive but the ones involving province collective resilience. Thus, H2a, H3b, and H3c were supported by the results, while H2b, H2c, and H3a were not. Further, while the intercept random variance of COVID‐19‐related personal concerns kept its significance when adding level 2 predictors in the model, lockdown‐related opportunities for personal growth did not vary across communities anymore, suggesting that its random variance had been explained by level 2 predictors. Consistently with these results, in M4 ICC and DEFF values increased for both lockdown‐related opportunities for personal growth and COVID‐19‐related personal concerns, and such increases were greater for lockdown‐related opportunities for personal growth.
TABLE 3.
Multilevel modelling results
| M1 | M2 | M3 | M4 | ||
|---|---|---|---|---|---|
| B (SE) | B (SE) | B (SE) | B (SE) | ||
| Fixed effects | |||||
| Individual level | |||||
| Closeness to COVID‐19 (1 = yes) → COVID‐19‐related personal concerns | −0.01 (0.01) | −0.01 (0.03) | −0.01 (0.02) | −0.01 (0.02) | |
| Closeness to COVID‐19 (1 = yes) → lockdown‐related opportunities for personal growth | 0.01 (0.03) | 0.01 (0.03) | 0.01 (0.02) | 0.01 (0.03) | |
| Personal resilience → COVID‐19‐related personal concerns | −0.01 (0.02) | 0.004 (0.03) | −0.01 (0.03) | ||
| Personal resilience → lockdown‐related opportunities for personal growth | 0.27*** (0.02) | 0.28*** (0.03) | 0.27*** (0.02) | ||
| Province level | |||||
| COVID‐related deaths → COVID‐19‐related personal concerns | 0.001 (0.001) | 0.001 (0.001) | 0.001 (0.001) | 0.001 (0.001) | |
| COVID‐related deaths → lockdown‐related opportunities for personal growth | 0.001 (0.001) | 0.001 (0.001) | 0.001 (0.001) | 0.001 (0.001) | |
| Province community ability to manage COVID‐19 pandemic → COVID‐19‐related personal concerns | 0.31** (0.12) | ||||
| Information provided by local institutions → COVID‐19‐related personal concerns | 0.32** (0.10) | ||||
| Province collective resilience → COVID‐19‐related personal concerns | −0.37** (0.13) | ||||
| Province community ability to manage COVID‐19 pandemic → lockdown‐related opportunities for personal growth | 0.41*** (0.08) | ||||
| Information provided by local institutions → lockdown‐related opportunities for personal growth | 0.23*** (0.07) | ||||
| Province collective resilience → lockdown‐related opportunities for personal growth | −0.18* (0.10) | ||||
| Intercepts | COVID‐19‐related personal concerns | 3.24*** (0.02) | 3.24*** (0.02) | 3.24*** (0.02) | 3.24*** (0.03) |
| Lockdown‐related opportunities for personal growth | 3.42*** (0.02) | 3.42*** (0.02) | 3.42*** (0.02) | 3.41*** (0.01) | |
| Random effects | |||||
| Intercepts at province level | COVID‐19‐related personal concerns | 0.01* (0.01) | 0.01* (0.01) | 0.01* (0.01) | 0.01* (0.003) |
| Lockdown‐related opportunities for personal growth | 0.01** (0.002) | 0.01** (0.002) | 0.01** (0.002) | 0.001 (0.001) | |
| Slopes at province level | Personal resilience → COVID‐19‐related personal concerns | 0.005 (0.01) | |||
| Personal resilience → lockdown‐related opportunities for personal growth | 0.002 (0.01) | ||||
| Residual within variances | COVID‐19‐related personal concerns | 0.46*** (0.01) | 0.46*** (0.01) | 0.46*** (0.01) | 0.46*** (0.01) |
| Lockdown‐related opportunities for personal growth | 0.40*** (0.01) | 0.38*** (0.01) | 0.38*** (0.01) | 0.38*** (0.01) | |
| ICC | COVID‐19‐related personal concerns | .031 | .031 | .031 | .037 |
| Lockdown‐related opportunities for personal growth | .015 | .015 | .015 | .027 | |
| DEFF | COVID‐19‐related personal concerns | 4.02 | 4.02 | 4.02 | 4.61 |
| Lockdown‐related opportunities for personal growth | 2.46 | 2.46 | 2.46 | 3.63 | |
Note. n = 3,745.
***p < .001 (2‐tailed); **p < .01 (2‐tailed); *p < .05 (2‐tailed).
M1 = baseline model; M2 = random intercept‐only model; M3 = random slope model; M4 = random intercept‐only model with level 2 predictors. ICC = Intraclass Correlation; DEFF = Design Effect.
Both the control effects on lockdown‐related opportunities for personal growth and the effect of COVID‐19‐related deaths per province on COVID‐19‐related personal concerns were non‐significant across all the models. Differently, the effect of the closeness to COVID‐19 on COVID‐19‐related personal concerns became non‐significant when considering the clustering of the respondents in their provinces – that is, since M2 – suggesting that it may have depended on the nesting into provinces more than on the closeness to COVID‐19 itself. Even though this mismatches previous results about the negative impact of the contacts with COVID‐19 in terms of either knowing someone who got infected or fearing contracting it (Barni et al., 2020; Fiorillo et al., 2020), it seems consistent with Italian provinces having suffered different severities of local infections during the first wave of contagion (Istat & Iss, 2020), which may have implied stronger concerns for personal safety and health as well as a higher probability to know someone who got infected for individuals living in the most strongly affected provinces.
6. DISCUSSION
COVID‐19 pandemic and the measures adopted to contain the spread of the virus had huge psychological repercussions in terms of both self‐concerns for the harmful consequences of the pandemic and perceived opportunities for personal growth due to the unforeseen and unprecedented lockdown experience (e.g., Asmundson et al., 2021; Gattino et al., 2022; Migliorini et al., 2021; Pancani et al., 2021; Procentese, Esposito, et al., 2021; Salari et al., 2020; Tamiolaki & Kalaitzaki, 2020; Torales et al., 2020; Varga et al., 2021; Vindegaard & Benros, 2020). However, although lockdown measures were enforced in almost every region of the world, their impact over individuals and their psychological responses was heterogeneous (Prati & Mancini, 2021). Building on this, the present study aimed at further investigating such variability, by addressing the buffer role resilience may have played – as suggested by Lenzo et al. (2020) and by Prati and Mancini (2021). It specifically unravelled the effect of resilience at both individual and community levels, consistently with the acknowledgment about resilience being a complex construct requiring several levels of analysis to be adequately addressed (Norris et al., 2008). Provinces were taken into account as the community of reference – that is, the level 2 units of analysis – due to the characteristics of the management of the first stage of the pandemic in Italy.
Overall, the results dovetail with previous evidence (Kimhi et al., 2020; Lenzo et al., 2020; Prati & Mancini, 2021) as to three main aspects: (a) the responses to COVID‐19‐related lockdown in terms of both concerns for personal safety and health and foreseen opportunities for personal growth varied across individuals as well as across communities; (b) both individual‐ and province‐level resilience accounted for such variability in individual responses to COVID‐19‐related lockdown – up to explaining the whole variability across provinces when it came to the foreseen opportunities for personal growth; (c) both individual and community resilience associated with both the concerns for personal safety and health and the foreseen opportunities for personal growth, even though different patterns emerged. Furthermore, these results stand regardless of the perception of personal and local exposure to COVID‐19‐related risks, supporting previous acknowledgments about individual and province community resilience accounting for a part of individual attentiveness for major negative and positive self‐impacts due to the pandemic (Tamiolaki & Kalaitzaki, 2020). However, the patterns of relationships which emerged for individual and community resilience were sometimes inconsistent with the proposed hypotheses.
First, as to personal resilience, the results suggest that the more individuals perceive themselves as able to engage in successful adaptation processes in the face of adverse circumstances, the more they focus on the elements of that challenging experience which can enrich them and their future lives despite the current hard times. Therefore, the more they are able to look at those troubling circumstances as opportunities for personal growth. Differently, no significant relationship emerged between personal resilience and COVID‐19‐related personal concerns, suggesting that such self‐perception could not be able to reduce the concrete adversity‐related concerns.
The emerged relationship is consistent with the existing literature considering personal resilience as an effective mechanism for overcoming adverse situations with positive outcomes (Fergus & Zimmerman, 2005) – such as personal growth. Moreover, with specific reference to the ongoing pandemic, it corroborates recent research showing significant relationships between personal resilience and the ability to cope with it (Giovannini et al., 2020; Lenzo et al., 2020; Migliorini et al., 2021). However, building on this, the lack of relationship between personal resilience and COVID‐19‐related concerns for one's safety and health rather represents an unexpected result. It may depend on the concerns for one's safety and health being here detected not as the negative impact of the pandemic on individual mental health, well‐being and social domain – which are the most investigated dimensions in previous research (Giovannini et al., 2020; Lenzo et al., 2020; Migliorini et al., 2021) – but rather as the concrete risks of getting infected, not living in a safe environment, not receiving adequate treatments when in need due to the COVID‐19‐related overload of requests in hospitals. However, due to the peculiarities of COVID‐19 pandemic, this result may also be due to the far‐reaching nature of this specific adverse event, which was acknowledged as requiring measures issued at different levels to be faced. That is, individuals might also have felt that their own ability to adapt to the lockdown circumstances might have not be enough to reduce the concrete threats to their health and safety – which might have still represented a risk when they had to go out of their house for the allowed needs and reasons (e.g., for groceries, to go to the pharmacy); conversely, other community members' behaviours and attitudes might have played a more relevant role in reducing such threats.
Furthermore, as to community resilience, more complex patterns emerged, echoing previous findings about community resilience as a complex and multidimensional construct encompassing several aspects, which differently associate with individual responses to adverse circumstances (Cohen et al., 2016). Overall, the results suggest that the more a community is able and prepared to manage a specific emergency – in this case, COVID‐19 pandemic – and local authorities provide adequate information about it, the more its members focus on both emergency‐related self‐concerns and opportunities for personal growth. Conversely – and unexpectedly – the more a community is broadly able to bounce back from adversities with positive outcomes, the less its members focus on both emergency‐related personal concerns and opportunities for personal growth.
On the one hand, these results suggest that shared representations about one's community as able to face a specific threat – in this case, COVID‐19 pandemic – and to keep its members updated about the latter associate with citizens' thoughtful attitude towards the stressor to be faced – which promotes their attention to both health‐related risks and the opportunities for personal growth – which is consistent with previous studies (Norris et al., 2008; Pfefferbaum et al., 2013). That is, such representations might work as buffers and – conversely to the expectations – as stressful factors at the same time. Indeed, a thoughtful attitude towards the pandemic might have made citizens more aware about both the risks the emergency brought about and the potential enrichments which may stem from those forcibly different life circumstances (Gattino et al., 2022), increasing their inner strength despite the personal costs (Migliorini et al., 2021). However, these results partially mismatch the hypotheses and previous studies showing the reduction of negative outcomes when citizens received accurate information about COVID‐19 (Wang et al., 2020) and perceived local Institutions as competent and trustworthy as to the management of the pandemic (Gattino et al., 2022). Such inconsistencies may depend on the different levels on analysis taken into account since both the mentioned studies tackled the considered community features only through citizens' individual perceptions about them.
On the other hand, these results also suggest that shared representations about one's community being broadly able to face troubling circumstances pursuing positive outcomes rather associate to a more passive attitude towards a specific stressor – such as COVID‐19 pandemic. That is, such representations make citizens focus less on both the threats for themselves and the potential learnings stemming from that stressful circumstance. Overall, this suggests that community broad collective resilience may work as a disengagement trigger rather than as a protective factor when it comes to a concrete emergency to be faced, differently from the hypotheses. It is hard to propose a unique explanation for this unexpected result. On the one hand, it is possible that in this kind of communities citizens delegate to others (e.g., local Institutions) the management of the emergency in terms of both taking care of reducing risks for community members and being ready to catch the available opportunities for individual and community progress and growth. However, on the other hand it may also be the case for citizens to trust their community's ability to overcome challenging circumstances at large and get the best out of them both in terms of risks reduction and individual and community enhancement. In either case, it seems like citizens sharing this representation of their community may assume that the latter will take care of itself and of its members throughout the emergency; consistently, they may rely on this significant group to get through it (Mannarini et al., 2021) – hence showing lower levels of attention to what is happening and to its implications both as risks and opportunities for themselves. Altogether, these results are consistent with previous studies showing that community collective resilience can act as a buffer against the negative impact of adverse events (Patel et al., 2017), yet they add that such representation may also associate with community members thinking less about their own experience of coping and adaptation, henceforth acknowledging fewer space and opportunities for nurturing self‐enhancement too.
Taken together, these findings highlight the centrality not only of personal resilience but also of the representations of one's community as prepared for managing a concrete emergency, providing adequate information about it, and broadly able to bounce back from adverse circumstances in shaping community members' psychological responses to an emergency. The emerged patterns bring about several implications, which can provide directions for both future studies and interventions aimed at facing broad emergencies. As to the latter, the present results suggest that keeping the levels of confidence in one's community's resilience high through an emergency‐focused informative campaign – aimed at stressing its ability to face that specific and concrete adversity – may represent an effective strategy to support an adaptive response in community members. Indeed, this could make the latter careful about the possible personal losses and risks, but also foster their positive re‐appraisal of their own resources and possibilities. This might reduce citizens' risky behaviours while allowing them to make the most out of those challenging circumstances too.
As to the theoretical implications, several aspects deserve attention. First, as to personal resilience, these results suggest that further studies are needed to look deeper into disentangling whether resilience could be able to reduce threat‐related concerns even when they refer to concrete risks during far‐reaching disasters and emergencies. Furthermore, when it comes to community resilience, these results support the need to address it as a multi‐component construct (Bonanno et al., 2015; Cohen et al., 2016; Norris et al., 2008; Pfefferbaum et al., 2013, 2014) and tackle its components separately, since they might show different patterns of relationships with the other considered variables – as it happened in the present study. Specifically, these results suggest that community broad collective resilience may actually work as a buffer as to the concrete threat‐related concerns, while reducing the attention paid to the opportunities for self‐enhancement too; conversely, its ability to manage a specific emergency and provide adequate information about it may work as factors prompting community members attitude to catching the emergency‐related opportunity for personal growth, while making them more careful also to the emergency‐related threats to themselves. Building on these results, future studies should further deepen whether they represent emergency‐specific patterns – for example, due to the specific peculiarities of COVID‐19 pandemic and of its management in Italy – or more general patterns of functioning of the different components of community resilience. It is also to consider that these patterns may be specific of community resilience components when they are addressed in a multilevel perspective. Furthermore, these findings suggest that future investigations should further explore community resilience as a contextualized process that might highly vary across different types of adversities, places and populations (Verbena et al., 2021). An in‐depth comprehension of the resilience process at community level requires to take into account that community resilience can be enacted in multiple ways depending on the nature of stressors and the people who cope with them (Matarrita‐Cascante, Trejos, Qin, Joo, & Debner, 2017). As regards to the latter point, future inquiries could further explore the perspective of community members on community resilience as a valuable source of knowledge (Faulkner, Brown, & Quinn, 2018).
6.1. Limitations and future directions
Some limitations of the present study require to be addressed too and open further research questions. First, a snowball sampling procedure was adopted, providing a non‐representative sample, and implying a self‐selection bias. Thus, the present results cannot be generalized to the overall Italian population. Nevertheless, the online distribution of the questionnaire and word of mouth allowed to reach a broad and heterogeneous group of participants while complying with all the restrictions due to COVID‐19 pandemic, providing validity to the results.
Furthermore, the items detecting level 2 variables refer to respondents' local community, yet they do not specify which community they should think about (e.g., provinces, Regions, etc.). While these items refer to assets, aspects of the management of the emergency and other dimensions which were all played out by provinces during the first wave of COVID‐19 pandemic outbreak – which makes it likely that respondents thought to those communities while rating those items – it should also be reckoned that some participants may have thought to different local communities while answering.
Last, the cross‐sectional design of the study cannot allow inferences about the direction of causality in the tested relationships. That is, it is not possible to exclude bi‐directional and circular relationships. However, it was not possible to plan a second wave of data collection due to the unavailability of information about the duration of COVID‐19‐related pandemic and to the consistently continuous changes in the needed measures. Nevertheless, longitudinal designs could provide a better understanding of the short‐term and long‐term effects of COVID‐19 pandemic and of the protective measures it has required, as well as of the buffering factors reducing citizens' concerns and sustaining their focus on the unexpected opportunities for personal growth and self‐enhancement stemming from COVID‐19‐related changes as to daily lives and habits. In addition, deepening how the relationships among these elements have shaped over time would be worthwhile too, due to the persistent and cyclical nature of the pandemic and taken into account to the continuously evolving protective measures in light of the progresses with the vaccines.
7. CONCLUSION
This study deepens citizens' safety‐ and health‐related concerns brought about by COVID‐19 pandemic and foreseen opportunities for personal growth in the first months of the ongoing pandemic – which represented unexpected and unprecedented adverse event for individuals and communities all over the world. It specifically deepens the role that personal and province community resilience may have played with reference to them. Overall, three main results emerged. First, the responses to COVID‐19‐related lockdown in terms of both concerns for personal safety and health and foreseen opportunities for personal growth varied across individuals as well as across province communities, supporting the need to consider both for a deeper understanding of such issues. Consistently, both individual‐ and province‐level resilience accounted for the variability in individual responses to COVID‐19‐related lockdown – up to explaining the whole variability across provinces when it came to the foreseen opportunities for personal growth. Last, personal resilience only showed a positive association with citizens' focus on lockdown‐related opportunities for personal growth, supporting its potential as a driver for individuals to overcome adverse situations with positive outcomes (Fergus & Zimmerman, 2005; Giovannini et al., 2020; Lenzo et al., 2020; Migliorini et al., 2021). Differently, the components of community resilience showed more complex paths to both lockdown‐related opportunities for personal growth and COVID‐19‐related personal concerns. Specifically, while community ability to manage the pandemic and the provision of adequate information by local institutions associated with a more thoughtful attitude towards the pandemic – in terms of attention to both the related risks and opportunities – collective resilience rather associated to a more passive attitude, characterized by lower levels of attention to the emergency to be faced. These results highlight the need to pay more attention to the role of resilience in the face of far‐reaching, unexpected adverse events – which hardly test individuals' as well as communities' adaptability and agency skills due to their magnitude. They highlight the complexities linked to the multi‐component and system‐specific nature of resilience (Bonanno et al., 2015; Cohen et al., 2016; Norris et al., 2008; Pfefferbaum et al., 2013, 2014), as well as potential paths towards making the most out of citizens' and communities' resilience.
Altogether, the need for interventions aimed at (1) sustaining individuals' personal resilience and (2) supporting the spread of adequate and emergency‐specific information and management plans by local authorities clearly emerges. This could allow citizens to be more aware of both the emergency‐related risks which arise for themselves and the opportunities for personal growth and self‐enhancement due to emergency‐related circumstances. Indeed, as the present results suggest, community's ability to plan an adequate use of these available resources to face the ongoing emergency, reduce the losses in its aftermath, answer its members' emergency‐related needs, and restore its own functioning represent critical skills to rely on in order for communities to sustain their members' functional adaptation and positive re‐appraisal of troubling circumstances during an adverse event (Norris et al., 2008; Pfefferbaum et al., 2013, 2017).
CONFLICT OF INTEREST
The authors declare that there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
ETHICS STATEMENT
The authors declare that the research is conducted ethically, responsibly and legally; the results are reported honestly; the submitted work is original and not (self‐)plagiarized; funding sources and conflicts of interest are disclosed. Ethical approval was obtained from the Università degli Studi di Bologna Institutional Review Board for all aspects of the current research.
ACKNOWLEDGMENT
Open Access Funding provided by Universita degli Studi di Napoli Federico II within the CRUI‐CARE Agreement.
Procentese, F. , Gatti, F. , Rochira, A. , Tzankova, I. , Di Napoli, I. , Albanesi, C. , Aresi, G. , Compare, C. , Fedi, A. , Gattino, S. , Guarino, A. , Marta, E. , & Marzana, D. (2022). The selective effect of lockdown experience on citizens' perspectives: A multilevel, multiple informant approach to personal and community resilience during COVID‐19 pandemic. Journal of Community & Applied Social Psychology, 1–22. 10.1002/casp.2651
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available in Dataset COVID‐19 (April‐May 2020) at http://doi.org/10.6092/unibo/amsacta/6634.
REFERENCES
- Asmundson, G. J. G. , Paluszek, M. M. , & Taylor, S. (2021). Real versus illusory personal growth in response to COVID‐19 pandemic stressors. Journal of Anxiety Disorders, 81, 102418. 10.1016/j.janxdis.2021.102418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baños, R. M. , Garcés, J. J. , Miragall, M. , Herrero, R. , Vara, M. , & Soria‐Olivas, E. (2022). Exploring the heterogeneity and trajectories of positive functioning variables, emotional distress, and post‐traumatic growth during strict confinement due to COVID‐19. Journal of Happiness Studies, 23(4), 1683–1708. 10.1007/s10902-021-00469-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barni, D. , Danioni, F. , Canzi, E. , Ferrari, L. , Ranieri, S. , Lanz, M. , … Rosnati, R. (2020). Facing the COVID‐19 pandemic: The role of sense of coherence. Frontiers in Psychology, 3027, 1. 10.3389/fpsyg.2020.578440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkes, F. , & Ross, H. (2013). Community resilience: Toward an integrated approach. Society & Natural Resources, 26(1), 5–20. 10.1080/08941920.2012.736605 [DOI] [Google Scholar]
- Bernstein, M. , & Pfefferbaum, B. (2018). Posttraumatic growth as a response to natural disasters in children and adolescents. Current Psychiatry Reports, 20(5), 37. 10.1007/s11920-018-0900-4 [DOI] [PubMed] [Google Scholar]
- Bonanno, G. A. , Romero, S. A. , & Klein, S. I. (2015). The temporal elements of psychological resilience: An integrative framework for the study of individuals, families, and communities. Psychological Inquiry, 26(2), 139–169. 10.1080/1047840X.2015.992677 [DOI] [Google Scholar]
- Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press. [Google Scholar]
- Brooks, S. K. , Webster, R. K. , Smith, L. E. , Woodland, L. , Wessely, S. , Greenberg, N. , & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–992. 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo, J. T. , Reis, H. T. , & Zautra, A. J. (2011). Social resilience: The value of social fitness with an application to the military. American Psychologist, 66(1), 43–51. 10.1037/a0021419 [DOI] [PubMed] [Google Scholar]
- Callegari, C. , Bertù, L. , Lucano, M. , Ielmini, M. , Braggio, E. , & Vender, S. (2016). Reliability and validity of the Italian version of the 14‐item resilience scale. Psychology Research and Behavior Management, 9, 277–284. 10.2147/PRBM.S115657 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandra, A. , Acosta, J. D. , Meredith, L. S. , Sanches, K. , Howard, S. , Uscher‐Pines, L. , … Yeung, D. (2010). Understanding community resilience in the context of national health security: A literature review. Santa Monica, CA: RAND Corporation. 10.7249/WR737 [DOI] [Google Scholar]
- Cohen, O. , Geva, D. , Lahad, M. , Bolotin, A. , Leykin, D. , Goldberg, A. , & Aharonson‐Daniel, L. (2016). Community resilience throughout the lifespan the potential contribution of healthy elders. PLoS One, 11(2), e0148125. 10.1371/journal.pone.0148125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cousineau, D. , & Chartier, S. (2010). Outliers detection and treatment: A review. International Journal of Psychological Research, 3(1), 58–67. 10.21500/20112084.844 [DOI] [Google Scholar]
- De Vincenzo, C. , Serio, F. , Franceschi, A. , Barbagallo, S. , & Zamperini, A. (2022). A “viral epistolary” and psychosocial spirituality: Restoring transcendental meaning during COVID‐19 through a digital community letter‐writing project. Pastoral Psychology, 71, 153–171. 10.1007/s11089-021-00991-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Demertzis, N. , & Eyerman, R. (2020). Covid‐19 as cultural trauma. American Journal of Cultural Sociology, 8(3), 428–450. 10.1057/s41290-020-00112-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dvorsky, M. R. , Breaux, R. , & Becker, S. P. (2020). Finding ordinary magic in extraordinary times: Child and adolescent resilience during the COVID‐19 pandemic. European Child & Adolescent Psychiatry, 30(11), 1829–1831. 10.1007/s00787-020-01583-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders, C. K. , & Tofighi, D. (2007). Centering predictor variables in cross‐sectional multilevel models: A new look at an old issue. Psychological Methods, 12(2), 121–138. 10.1037/1082-989X.12.2.121 [DOI] [PubMed] [Google Scholar]
- Faulkner, L. , Brown, K. , & Quinn, T. (2018). Analyzing community resilience as an emergent property of dynamic social‐ecological systems. Ecology and Society, 23(1), 24–34. [Google Scholar]
- Felix, E. , Afifi, T. , Kia‐Keating, M. , Brown, L. , Afifi, W. , & Reyes, G. (2015). Family functioning and posttraumatic growth among parents and youth following wildfire disasters. American Journal of Orthopsychiatry, 85(2), 191–200. 10.1037/ort0000054 [DOI] [PubMed] [Google Scholar]
- Fergus, S. , & Zimmerman, M. A. (2005). Adolescent resilience: A framework for. Annual Review of Public Health, 26, 399–419. 10.1146/annurev.publhealth.26.021304.144357 [DOI] [PubMed] [Google Scholar]
- Fiorillo, A. , Sampogna, G. , Giallonardo, V. , Del Vecchio, V. , Luciano, M. , Albert, U. , … Volpe, U. (2020). Effects of the lockdown on the mental health of the general population during the COVID‐19 pandemic in Italy: Results from the COMET collaborative network. European Psychiatry, 63(1), e87. 10.1192/j.eurpsy.2020.89 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Folkman, S. (2008). The case for positive emotions in the stress process. Anxiety, Stress, and Coping, 21(1), 3–14. 10.1080/10615800701740457 [DOI] [PubMed] [Google Scholar]
- Gaboardi, M. , Gatti, F. , Santinello, M. , Gandino, G. , Guazzini, A. , Guidi, E. , … Procentese, F. (2022). The photo diaries method to catch the daily experience of Italian university students during COVID‐19 lockdown. Community Psychology in Global Perspective, 8(2), 59–80. 10.1285/i24212113v8i2p59 [DOI] [Google Scholar]
- Gatti, F. , & Procentese, F. (2021). Local community experience as an anchor sustaining reorientation processes during COVID‐19 pandemic. Sustainability, 13(8), 4385. 10.3390/su13084385 [DOI] [Google Scholar]
- Gattino, S. , Rizzo, M. , Gatti, F. , Compare, C. , Procentese, F. , Guarino, A. , … Albanesi, C. (2022). COVID‐19 in our lives: Sense of community, sense of community responsibility, and reflexivity in present concerns and perception of the future. Journal of Community Psychology, 50(5), 2344–2365. 10.1002/jcop.22780 [DOI] [PubMed] [Google Scholar]
- Giovannini, E. , Benczur, P. , Campolongo, F. , Cariboni, J. , & Manca, A. (2020). Time for transformative resilience: The COVID‐19 emergency. Luxembourg: Publications Office of the European Union. 10.2760/062495 [DOI] [Google Scholar]
- Horton, R. (2020). Offline: COVID‐19 is not a pandemic. The Lancet, 396(10255), 874. 10.1016/S0140-6736(20)32000-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hox, J. J. (2010). Multilevel analysis: Techniques and applications. New York, NY: Routledge. [Google Scholar]
- Hyun, S. , Wong, G. T. F. , Levy‐Carrick, N. C. , Charmaraman, L. , Cozier, Y. , Yip, T. , & Liu, C. H. (2021). Psychosocial correlates of posttraumatic growth among US young adults during the COVID‐19 pandemic. Psychiatry Research, 302, 114035. 10.1016/j.psychres.2021.114035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Istat [Istituto Nazionale di Statistica], & Iss [Istituto Superiore di Sanità] (2020). Impatto dell'epidemia COVID‐19 sulla mortalità totale della popolazione residente periodo gennaio‐maggio 2020 . Retrieved from https://www.istat.it/it/files/2020/07/Rapp_Istat_Iss_9luglio.pdf (last accessed on Sept. 29th, 2020).
- Jenkins, M. , Hoek, J. , Jenkin, G. , Gendall, P. , Stanley, J. , Beaglehole, B. , … Every‐Palmer, S. (2021). Silver linings of the COVID‐19 lockdown in New Zealand. PLoS One, 16(4), e0249678. 10.1371/journal.pone.0249678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendra, J. M. , & Wachtendorf, T. (2003). Elements of resilience after the world trade center disaster: Reconstituting new York City's emergency operations Centre. Disasters, 27(1), 37–53. 10.1111/1467-7717.00218 [DOI] [PubMed] [Google Scholar]
- Killgore, W. D. , Taylor, E. C. , Cloonan, S. A. , & Dailey, N. S. (2020). Psychological resilience during the COVID‐19 lockdown. Psychiatry Research, 291, 113216. 10.1016/j.psychres.2020.113216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimhi, S. , Marciano, H. , Eshel, Y. , & Adini, B. (2020). Recovery from the COVID‐19 pandemic: Distress and resilience. International Journal of Disaster Risk Reduction, 50, 101843. 10.1016/j.ijdrr.2020.101843 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimhi, S. , & Shamai, M. (2004). Community resilience and the impact of stress: Adult response to Israel's withdrawal from Lebanon. Journal of Community Psychology, 32(4), 439–451. 10.1002/jcop.20012 [DOI] [Google Scholar]
- Lanz, M. , Sorgente, A. , & Tagliabue, S. (2018). Inter‐rater agreement indices for multiple informant methodology. Marriage & Family Review, 54(2), 148–182. 10.1080/01494929.2017.1340919 [DOI] [Google Scholar]
- Lenzo, V. , Quattropani, M. C. , Musetti, A. , Zenesini, C. , Freda, M. F. , Lemmo, D. , … Franceschini, C. (2020). Resilience contributes to low emotional impact of the COVID‐19 outbreak among the general population in Italy. Frontiers in Psychology, 11, 3062. 10.3389/fpsyg.2020.576485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine, S. Z. , Laufer, A. , Stein, E. , Hamama‐Raz, Y. , & Solomon, Z. (2009). Examining the relationship between resilience and posttraumatic growth. Journal of Traumatic Stress, 22(4), 282–286. 10.1002/jts.20409 [DOI] [PubMed] [Google Scholar]
- Lewin, K. (1951). Field theory in social science: Selected theoretical papers. New York: Harpers. [Google Scholar]
- Lyons, A. , Fletcher, G. , & Bariola, E. (2016). Assessing the well‐being benefits of belonging to resilient groups and communities: Development and testing of the Fletcher‐Lyons collective resilience scale (FLCRS). Group Dynamics: Theory, Research, and Practice, 20(2), 65–77. 10.1037/gdn0000041 [DOI] [Google Scholar]
- Maas, C. J. , & Hox, J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology, 1(3), 86–92. 10.1027/1614-2241.1.3.86 [DOI] [Google Scholar]
- MacCallum, R. C. , & Austin, J. T. (2000). Applications of structural equation modeling in psychological research. Annual Review of Psychology, 51(1), 201–226. 10.1146/annurev.psych.51.1.201 [DOI] [PubMed] [Google Scholar]
- Mancini, A. D. (2020). Heterogeneous mental health consequences of COVID‐19: Costs and benefits. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S15–S16. 10.1037/tra0000894 [DOI] [PubMed] [Google Scholar]
- Mannarini, T. , Rizzo, M. , Brodsky, A. , Buckingham, S. , Zhao, J. , Rochira, A. , & Fedi, A. (2021). The potential of psychological connectedness: Mitigating the impacts of COVID‐19 through sense of community and community resilience. Journal of Community Psychology, 50, 2273–2289. 10.1002/jcop.22775 [DOI] [PubMed] [Google Scholar]
- Matarrita‐Cascante, D. , Trejos, B. , Qin, H. , Joo, D. , & Debner, S. (2017). Conceptualizing community resilience: Revisiting conceptual distinctions. Community Development, 48(1), 105–123. 10.1080/15575330.2016.1248458 [DOI] [Google Scholar]
- Megías‐Robles, A. , Gutiérrez‐Cobo, M. J. , Cabello, R. , Gómez‐Leal, R. , & Fernández‐Berrocal, P. (2022). A longitudinal study of the influence of concerns about contagion on negative affect during the COVID‐19 lockdown in adults: The moderating effect of gender and resilience. Journal of Health Psychology, 27(5), 1165–1175. 10.1177/1359105321990794 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menoni, S. , & Schwarze, R. (2020). Recovery during a crisis: Facing the challenges of risk assessment and resilience management of COVID‐19. Environment Systems & Decisions, 40, 189–198. 10.1007/s10669-020-09775-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Migliorini, L. , De Piccoli, N. , Cardinali, P. , Rollero, C. , Marzana, D. , Arcidiacono, C. , … Di Napoli, I. (2021). Contextual influences on Italian university students during the COVID‐19 lockdown: Emotional responses, coping strategies and resilience. Community Psychology in Global Perspective, 7(1), 71–87. 10.1285/i24212113v7i1p71 [DOI] [Google Scholar]
- Muthen, B. O. , & Satorra, A. (1995). Complex sample data in structural equation modeling. Sociological Methodology, 25, 267–316. 10.2307/271070 [DOI] [Google Scholar]
- Nezlek, J. B. (2008). An introduction to multilevel modeling for social and personality psychology. Social and Personality Psychology Compass, 2(2), 842–860. 10.1111/j.1751-9004.2007.00059.x [DOI] [Google Scholar]
- Norris, F. H. , Stevens, S. P. , Pfefferbaum, B. , Wyche, K. F. , & Pfefferbaum, R. L. (2008). Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. American Journal of Community Psychology, 41(1), 127–150. 10.1007/s10464-007-9156-6 [DOI] [PubMed] [Google Scholar]
- Ostadtaghizadeh, A. , Ardalan, A. , Paton, D. , Jabbari, H. , & Khankeh, H. R. (2015). Community disaster resilience: A systematic review on assessment models and tools. PLoS Currents, 7, PMC4395373. 10.1371/CURRENTS.DIS.F224EF8EFBDFCF1D508DD0DE4D8210ED [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pancani, L. , Marinucci, M. , Aureli, N. , & Riva, P. (2021). Forced social isolation and mental health: A study on 1,006 Italians under COVID‐19 lockdown. Frontiers in Psychology, 12, 1540. 10.3389/fpsyg.2021.663799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel, S. S. , Rogers, M. B. , Amlôt, R. , & Rubin, G. J. (2017). What do we mean by “community resilience”? A systematic literature review of how it is defined in the literature. PLoS Currents, 9, PMC5693357. 10.1371/currents.dis.db775aff25efc5ac4f0660ad9c9f7db2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paton, D. , Millar, M. , & Johnston, D. (2001). Community resilience to volcanic hazard consequences. Natural Hazards, 24(2), 157–169. 10.1023/A:1011882106373 [DOI] [Google Scholar]
- Pfefferbaum, B. , Van Horn, R. L. , & Pfefferbaum, R. L. (2017). A conceptual framework to enhance community resilience using social capital. Clinical Social Work Journal, 45(2), 102–110. 10.1007/s10615-015-0556-z [DOI] [Google Scholar]
- Pfefferbaum, B. J. , Reissman, D. B. , Pfefferbaum, R. L. , Klomp, R. W. , & Gurwitch, R. H. (2008). Building resilience to mass trauma events. In Sleet D., Mercy J., Bonzo S., & Doll L. (Eds.), Handbook of injury and violence prevention (pp. 347–358). Boston: Springer. 10.1007/978-0-387-29457-5_19 [DOI] [Google Scholar]
- Pfefferbaum, R. L. , Pfefferbaum, B. , Nitiéma, P. , Houston, J. B. , & Van Horn, R. L. (2014). Assessing community resilience: An application of the expanded CART survey instrument with affiliated volunteer responders. American Behavioral Scientist, 59(2), 181–199. 10.1177/0002764214550295 [DOI] [Google Scholar]
- Pfefferbaum, R. L. , Pfefferbaum, B. , Van Horn, R. L. , Klomp, R. W. , Norris, F. H. , & Reissman, D. B. (2013). The communities advancing resilience toolkit (CART): An intervention to build community resilience to disasters. Journal of Public Health Management and Practice, 19(3), 250–258. 10.1097/PHH.0b013e318268aed8 [DOI] [PubMed] [Google Scholar]
- Plough, A. , Bristow, B. , Fielding, J. , Caldwell, S. , & Khan, S. (2011). Pandemics and health equity: Lessons learned from the H1N1 response in Los Angeles County. Journal of Public Health Management and Practice, 17(1), 20–27. 10.1097/phh.0b013e3181ff2ad7 [DOI] [PubMed] [Google Scholar]
- Prati, G. , & Mancini, A. D. (2021). The psychological impact of COVID‐19 pandemic lockdowns: A review and meta‐analysis of longitudinal studies and natural experiments. Psychological Medicine, 51(2), 201–211. 10.1017/S0033291721000015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Presidenza del Consiglio dei Ministri . (2020). Gazzetta Ufficiale della Repubblica Italiana (p. 62). https://www.gazzettaufficiale.it/eli/gu/2020/03/09/62/sg/pdf [Google Scholar]
- Procentese, F. , Capone, V. , Caso, D. , Donizzetti, A. R. , & Gatti, F. (2020). Academic Community in the Face of emergency situations: Sense of responsible togetherness and sense of belonging as protective factors against academic stress during COVID‐19 outbreak. Sustainability, 12(22), 9718. 10.3390/su12229718 [DOI] [Google Scholar]
- Procentese, F. , Esposito, C. , Gonzalez Leone, F. , Agueli, B. , Arcidiacono, C. , Freda, M. F. , & Di Napoli, I. (2021). Psychological lockdown experiences: Downtime or an unexpected time for being? Frontiers in Psychology, 12, 1159. 10.3389/fpsyg.2021.577089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Procentese, F. , Gatti, F. , & Ceglie, E. (2021). Sensemaking processes during the first months of COVID‐19 pandemic: Using diaries to deepen how Italian youths experienced lockdown measures. International Journal of Environmental Research and Public Health, 18(23), 12569. 10.3390/ijerph182312569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Procentese, F. , Gatti, F. , & Ceglie, E. (2022a). Protective and risk social dimensions of emergency remote teaching during COVID‐19 pandemic: A multiple mediation study. Journal of Community Psychology, 1‐17. 10.1002/jcop.22879 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Procentese, F. , Gatti, F. , & Ceglie, E. (2022b). Teachers' efficacy in the face of emergency remote teaching during COVID‐19 pandemic: The protective role of personal resilience and sense of responsible togetherness. Psicologia Sociale, 17(1), 79–92. 10.1482/103778 [DOI] [Google Scholar]
- Rochira, A. , Gatti, F. , Prati, G. , Mannarini, T. , Fedi, A. , Procentese, F. , … Aresi, G. (2022). An integrated model of compliance with COVID‐19 prescriptions: Instrumental, normative, and affective factors associated with health‐protective behaviors. International Journal of Behavioral Medicine, 1–13. 10.1007/s12529-021-10052-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roma, P. , Monaro, M. , Colasanti, M. , Ricci, E. , Biondi, S. , Di Domenico, A. , … Mazza, C. (2020). A 2‐month follow‐up study of psychological distress among Italian people during the COVID‐19 lockdown. International Journal of Environmental Research and Public Health, 17(21), 8180. 10.3390/ijerph17218180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salari, N. , Hosseinian‐Far, A. , Jalali, R. , Vaisi‐Raygani, A. , Rasoulpoor, S. , Mohammadi, M. , … Khaledi‐Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID‐19 pandemic: A systematic review and meta‐analysis. Globalization and Health, 16(1), 57. 10.1186/s12992-020-00589-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheerin, C. M. , Lind, M. J. , Brown, E. A. , Gardner, C. O. , Kendler, K. S. , & Amstadter, A. B. (2018). The impact of resilience and subsequent stressful life events on MDD and GAD. Depression and Anxiety, 35, 140–147. 10.1002/da.22700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snijders, T. A. , & Bosker, R. J. (2012). Multilevel analysis: An introduction to basic and advanced multilevel modeling. Beverly Hills, CA: Sage. [Google Scholar]
- Sonn, C. , & Fisher, A. (1998). Sense of community: Community resilient responses to oppression and change. Journal of Community Psychology, 26, 457–472. 10.1002/(SICI)1520-6629(199809)26:5<457::AID-JCOP5>3.0.CO;2-O [DOI] [Google Scholar]
- Tamiolaki, A. , & Kalaitzaki, A. E. (2020). “That which does not kill us, makes us stronger”: COVID‐19 and posttraumatic growth. Psychiatry Research, 289, 113044. 10.1016/j.psychres.2020.113044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tedeschi, R. G. , & Calhoun, L. G. (2004). Posttraumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15, 1–18. 10.1207/s15327965pli1501_01 [DOI] [Google Scholar]
- Torales, J. , O'Higgins, M. , Castaldelli‐Maia, J. M. , & Ventriglio, A. (2020). The outbreak of COVID‐19 coronavirus and its impact on global mental health. International Journal of Social Psychiatry, 66(4), 317–320. 10.1177/0020764020915212 [DOI] [PubMed] [Google Scholar]
- Ulset, V. S. , & von Soest, T. (2022). Posttraumatic growth during the COVID‐19 lockdown: A large‐scale population‐based study among Norwegian adolescents. Journal of Traumatic Stress, 35, 941–954. 10.1002/jts.22801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ungar, M. (2011). Community resilience for youth and families: Facilitative physical and social capital in contexts of adversity. Children and Youth Services Review, 33(9), 1742–1748. 10.1016/j.childyouth.2011.04.027 [DOI] [Google Scholar]
- van Bruggen, G. H. , Lilien, G. L. , & Kacker, M. (2002). Informants in organizational marketing research: Why use multiple informants and how to aggregate responses. Journal of Marketing Research, 39(4), 469–478. 10.1509/jmkr.39.4.469.19117 [DOI] [Google Scholar]
- Varga, T. V. , Bu, F. , Dissing, A. S. , Elsenburg, L. K. , Bustamante, J. J. H. , Matta, J. , … Rod, N. H. (2021). Loneliness, worries, anxiety, and precautionary behaviours in response to the COVID‐19 pandemic: A longitudinal analysis of 200,000 Western and northern Europeans. The Lancet Regional Health ‐ Europe, 2, 100020. 10.1016/j.lanepe.2020.100020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verbena, S. , Rochira, A. , & Mannarini, T. (2021). Community resilience and the acculturation expectations of the receiving community. Journal of Community Psychology, 49(2), 390–405. 10.1002/jcop.22466 [DOI] [PubMed] [Google Scholar]
- Vindegaard, N. , & Benros, M. E. (2020). COVID‐19 pandemic and mental health consequences: Systematic review of the current evidence. Brain, Behavior, and Immunity, 89, 531–542. 10.1016/j.bbi.2020.05.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh, F. (2003). Family resilience: A framework for clinical practice. Family Process, 42(1), 1–18. 10.1111/j.1545-5300.2003.00001.x [DOI] [PubMed] [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , Ho, C. S. , & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID‐19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. 10.3390/ijerph17051729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, R. , & Drury, J. (2009). Psychosocial resilience and its influence on managing mass emergencies and disasters. Psychiatry, 8(8), 293–296. 10.1016/j.mppsy.2009.04.019 [DOI] [Google Scholar]
- Wilson, G. A. (2012). Community resilience, globalization, and transitional pathways of decision‐making. Geoforum, 43(6), 1218–1231. 10.1016/j.geoforum.2012.03.008 [DOI] [Google Scholar]
- World Health Organization (2020a). Director‐General's opening remarks at the media briefing on COVID‐19 . https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020
- World Health Organization (2020b). Mental Health and Psychosocial Considerations during the COVID‐19 Outbreak . https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf
- Yue, Z. , Lee, D. S. , Xiao, J. , & Zhang, R. (2021). Social media use, psychological well‐being and physical health during lockdown. Information, Communication & Society, 1‐18, 1–18. 10.1080/1369118X.2021.2013917 [DOI] [Google Scholar]
- Zautra, A. J. , Hall, J. S. , & Murray, K. E. (2010). Resilience: A new definition of health for people and communities. In Reich J. R., Zautra A. J., & Hall J. S. (Eds.), Handbook of adult resilience (pp. 3–30). NY: Guilford Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are openly available in Dataset COVID‐19 (April‐May 2020) at http://doi.org/10.6092/unibo/amsacta/6634.