

Abstract
Decentralized clinical trials (DCTs) have the potential to improve accessibility, diversity, and retention in clinical trials by moving trial activities to participants’ homes and local surroundings. In this study, we conducted semi‐structured interviews with 20 European regulators to identify regulatory challenges and opportunities for the implementation of DCTs in the European Union. The key opportunities for DCTs that were recognized by regulators include a reduced participation burden, which could facilitate the participation of underserved patients. In addition, regulators indicated that data collected in DCTs are expected to be more representative of the real world. Key challenges recognized by regulators for DCTs include concerns regarding investigator oversight and participants’ safety when physical examinations and face‐to‐face contact are limited. To facilitate future learning, hybrid clinical trials with both on‐site and decentralized elements are proposed by the respondents.
Study Highlights.
WHAT IS THE CURRENT KNOWLEDGE ON THIS TOPIC?
☑ Decentralized clinical trials (DCTs) have the possibility to improve clinical trial conduct. However, regulatory requirements and perceived low degree of regulatory acceptance may impact the implementation of DCTs.
WHAT QUESTION DID THIS STUDY ADDRESS?
☑ What are the opportunities and challenges for the authorization and implementation of DCTs in Europe from a regulators’ perspective?
WHAT DOES THIS STUDY ADD TO OUR KNOWLEDGE?
☑ Regulators expect that DCTs will facilitate the recruitment of underserved patients. Data collected in DCTs are furthermore expected to be more representative of the real‐world. However, concerns regarding investigator oversight and safety monitoring may challenge DCT implementation. Regulators suggested that further experience with DCTs can be exerted through hybrid clinical trials, combining decentralized and on‐site activities.
HOW MIGHT THIS CHANGE CLINICAL PHARMACOLOGY OR TRANSLATIONAL SCIENCE?
☑ This research helps progress the implementation of DCTs by providing insights into the opportunities and challenges for its implementation from a European regulator’s perspective. The themes described in this research should be considered when designing a DCT and could help to educate regulators on DCTs.
Clinical trials (CTs) are essential for determining the efficacy and safety of therapeutic interventions. However, several CT processes related to operations, data collection, participant recruitment, and prevention of loss to follow‐up are suboptimal and hamper the clinical development of new interventions. 1 , 2 Current processes for participant identification, recruitment, and follow‐up are expensive and often burdensome for participants, 1 which may lead to low participation and retention. 3 Furthermore, meeting recruitment targets is challenging, 4 , 5 and this can lead to underpowered CTs, and CT discontinuation. 6 , 7 Together, these factors have scientific, ethical, and financial implications that can hinder timely access to new therapeutic interventions.
The implementation of digital technologies and other novel approaches may help to improve overall CT conduct and could enable a new operational approach known as “decentralized clinical trials” (DCTs). DCTs are CTs in which trial activities are performed at participants’ homes and/or at local health care facilities. 8 In addition to the full DCT approach, where participants do not visit the trial site at all during the trial, hybrid CTs incorporate both decentralized and site‐based elements. 8 For conceptual clarity, we use “DCTs” to refer to both full DCTs and hybrid DCTs. Examples of decentralized trial elements (also referred to as “remote elements”) include recruitment via social media, shipping study drugs directly to participants, data collection through wearables, and telemedicine visits to integrate trial participation into participants’ daily lives by reducing the need to physically attend on‐site visits. As a result, DCTs may be less disruptive to the participants’ lives, whereas allowing the recruitment of a more diverse participant population 9 and enriching datasets through more frequent or even continuous data collection in a real‐world setting. 10
The healthcare restrictions resulting from the coronavirus disease 2019 (COVID‐19) pandemic catalyzed the use of decentralized elements to ensure participant safety (by reducing the risk of infection and continuing the investigational medicinal product (IMP) treatment) and maintain data integrity. 11 , 12 Surveys have found that, post‐COVID‐19, investigators are interested in incorporating decentralized trial elements, 13 , 14 and previous initiatives have underlined the willingness of sponsors to implement DCTs. 15 , 16 Furthermore, the pandemic has compelled regulators to take a position on the implementation of decentralized elements in clinical trials, 17 and several European national competent authorities (NCAs) have recently expressed interest in DCTs, issuing guidance and conducting DCT pilot studies. 18 , 19 , 20 , 21 Nonetheless, relatively few full DCTs have been conducted in Europe thus far. Recent work has suggested that, among other factors, regulatory requirements and a perceived low degree of acceptance by NCAs and ethics committees may be limiting their implementation. 22 , 23 , 24 Hence, identifying the opportunities and challenges for DCTs from a regulatory bodies’ perspective could help enable progress. At present, these have not been formally evaluated in the European context. Therefore, this study involves interviews with European regulators—who work within different roles overseeing the authorization, conduct, or data generated in a CT—to identify those opportunities and challenges from a regulatory perspective that affect the authorization and implementation of DCTs.
METHODOLOGY
Study design and study population
Data were collected through in‐depth semi‐structured interviews with European regulators. The Consolidated Criteria for Reporting Qualitative Research (COREQ) were used to report on the methodology. 25 Representatives from 37 European Economic Area (EEA) NCAs, covering all EEA member states, were identified from the NCA and European Medicines Agency (EMA) websites and the research team’s network. Participant eligibility was restricted to regulators involved in assessing the application, implementation, and interpretation of CTs (e.g., clinical assessors and statisticians) who worked for an NCA in the EEA during the study period. Experience with assessing DCTs was not required. The respondents were asked for their personal perspectives and did not participate on behalf of their NCA. This work did not include patients and was therefore exempt from ethics review.
Outcomes and interview guide development
The interview guide was designed to collect information about regulatory opportunities and challenges for DCTs (Table S1 ). To that end, it included five topics, open interview questions, and detailed probes. The interview guide topics were identified via the Trials@Home “decentralized trial process” framework 26 and using the authors’ experience, and they were as follows: (i) CT authorization of DCTs; (ii) decentralized recruitment and enrollment of participants; (iii) direct‐to‐participant (DtP) IMP supply; (iv) the acceptance of the evidence generated by decentralized means; and (v) the impact of COVID‐19 on CTs. The content of the interview guide was validated by a discussion of the preliminary guide with a clinical assessor from an NCA, expert reviews by six Trials@Home consortium members with DCT regulatory expertise, and three pilot interviews.
Data collection
Semi‐structured interviews of ~1 hour each were conducted online by a trained researcher (A.J.d.J.), with 1 to 3 respondents at a time, between May and October 2021. Data collection continued until no new themes were being identified from new data according to the saturation criterion. 27 Before the interviews, the interview guide and informed consent form were shared with the respondents. Because the interviews were conducted online, verbal consent was obtained from each participant before their interview. All topics and open interview questions detailed in Table S1 were discussed with the respondents, and the respondents were free to elaborate on the topics that suited their expertise. A summary of each interview was drafted based on field notes and shared with the respective respondent for additional clarification or correction if necessary.
The respondents’ current areas of expertise were classified by the following categories: (i) CT assessors—who are involved in the assessment of CT application dossiers before trial commencement, (ii) GCP inspectors, (iii) and clinical data assessors. The geographic region in which the interviewee’s NCA operates was determined using the geographic regions from the “standard country or area codes for statistical use (M49).” 28 The participant’s years of experience as regulator were collected from the transcripts or curricula vitae.
Data analysis
The interviews were audio‐recorded, transcribed verbatim, and pseudonymized for further analysis. Transcripts from the three pilot interviews were included in the data analysis because no changes were made to the interview guide topics based on these pilot interviews. The interview transcripts were qualitatively analyzed by thematic analysis 29 using NVivo 12 Pro, QSR International (Burlington, MA). First, two interview transcripts were independently coded by two authors (A.J.d.J. and T.I.v.R.). In the next stage, the codes were iteratively reviewed, aggregated, and categorized into (sub‐)themes to draft a codebook and a preliminary thematic map. Six of the 13 subsequent transcripts were coded in duplicate and discussed by three researchers (A.J.d.J., T.I.v.R., and Y.S.A.T.) to refine the initially identified (sub‐)themes, thus allowing for triangulation between the authors. We then classified opportunities and challenges for the identified themes.
RESULTS
Respondents’ characteristics and experience
In total, 124 representatives from all European regions 28 were invited to participate, 53 of whom responded. Twenty regulators from 11 European NCAs participated in one of the 15 interviews (Table 1 ). All European regions except Eastern Europe were represented in the interview series. The reasons for non‐participation were lack of prior experience with DCTs (n = 12), time constraints (n = 8), the project not being within the remit of the invitee or department (n = 4), or other reasons (n = 9).
Table 1.
Characteristics of the respondents (n = 20)
| Characteristic | Category | Frequency (%) |
|---|---|---|
| Years of experiencea | 0–4 years | 4 (20) |
| 5–9 years | 5 (25) | |
| >10 years | 11 (55) | |
| Expertise/role | Clinical trial assessor | 8 (40) |
| GCP inspector | 5 (25) | |
| Clinical data assessor | 6 (30) | |
| Otherb | 1 (5) | |
| European region | Northern Europe | 6 (30) |
| Southern Europe | 5 (25) | |
| Western Europe | 9 (45) | |
| Eastern Europe | 0 (0) |
GCP, good clinical practice.
Experience as a clinical regulator.
Ethicist. The European region where the interviewees’ national competent authority operates was determined using the Geographic Regions from the “standard country or area codes for statistical use (M49).” 28
All respondents had experience with individual decentralized elements, such as DtP IMP supply, electronic data collection tools, and home nurse visits. In addition, most respondents had experience of providing scientific advice for DCTs or had been involved in European‐level discussions regarding DCTs, for example, through the EMA Innovation Task Force (ITF), Good Clinical Practice Inspectors Working Group (GCP IWG), and/or Clinical Trials Facilitation and Coordination Group (CTFG). None of the respondents had assessed a full DCT.
Five major themes were identified from the interview data: (i) justification of decentralized elements, (ii) sponsor and investigator responsibilities; (iii) trial participants’ interests; (iv) data quality; and (v) future directions (Figure 1 ). In relation to these themes, both opportunities and challenges applicable to DCTs and conventional CTs were identified (Table S2 ). The key opportunities and challenges are presented in Table 2 .
Figure 1.
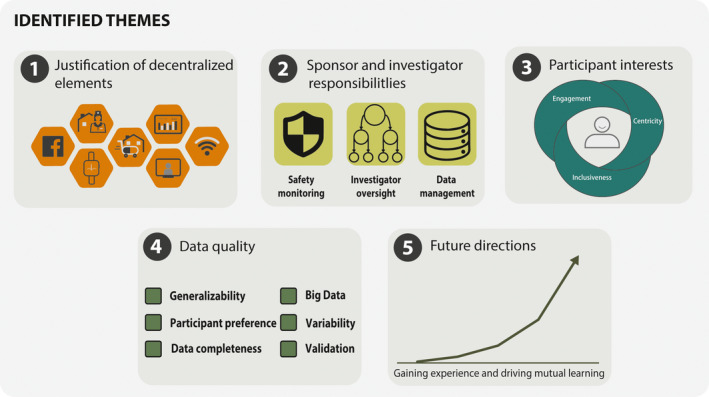
Graphical representation of the five identified themes. [Colour figure can be viewed at wileyonlinelibrary.com]
Table 2.
Key opportunities and challenges for the implementation of decentralized clinical trials as stated by the interviewees
| Theme | Opportunities | Challenges |
|---|---|---|
| Justification of decentralized elements |
|
|
| Sponsor and investigator responsibilities |
|
|
| Trial participants’ interests |
|
|
| Data quality |
|
|
| Future directions |
|
|
CT, clinical trial; CTR, Clinical Trials Regulation EU 536/2014; DCT, decentralized clinical trial; EU, European Union; IMP, investigational medicinal product.
Justification of decentralized elements
The respondents indicated that decentralized elements should suit the research question and be clearly described and justified on a case‐by‐case basis within the clinical trial protocol, owing to the novelty of these approaches. It was stated that a decrease of trial costs would not be considered sufficient justification for implementing decentralized elements. Risks associated with the implementation of decentralized elements should be anticipated and mitigated.
Late‐phase confirmatory CTs were considered more suitable for DCTs than early‐phase CTs, as the safety‐risk profile of the IMP should be sufficiently elucidated. However, the respondents indicated that they were open to all proposals from trial sponsors:
It is up to the sponsor to push the envelope and convince us that it is safe, that it is actually a good way of conducting a clinical trial. I think as a regulator you should not hinder the progress, but you are not the person who does the interventions either. And one way of hindering progress is to state certain things like ‘this would never go’ and ‘this is never acceptable,’ when in fact you don’t have the expertise to think through every scenario and what is actually acceptable (clinical trial assessor).
Opportunities to conduct DCTs for chronic diseases, low‐risk diseases (such as allergic rhinitis or smoking cessation), and rare diseases were recognized by several respondents, due to the ability to self‐manage chronic diseases; and the opportunity to recruit more participants in a CT for rare diseases due to the wider geographic reach. On the contrary, therapeutic areas (TAs) that require careful assessment or observation—such as Parkinson’s disease or those requiring more intensive care, such as oncology—were considered by several respondents to be less appropriate. It was acknowledged, however, that, in certain instances, oncology and palliative care trials could and should be conducted close to the participants’ direct surroundings to benefit the participant (Supplementary Information Quote S1 ).
Sponsor and investigator responsibilities
Investigator oversight
Several challenges regarding the use of third parties in DCTs were recognized, including the training of third parties and the hesitancy of NCAs, ethics committees, and investigators to delegate tasks to third parties. This is because of a lack of clarity regarding qualifications and the overall responsibility of the investigator, under the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) GCP guideline. One respondent explained this as follows:
The most difficult issue we have experienced is the acceptance of external staff so, home visits by home nurses, and home doctors. They are not very well accepted, either by ethics committees but, even more, by the PI (clinical data assessor).
As a solution, one respondent proposed that home visits should ideally be organized via a site’s existing infrastructure. Furthermore, there was a need for clear lines of communication among the investigator staff, local healthcare professionals, and vendors, as participants should not be responsible for communicating safety information.
Safety monitoring
Many respondents indicated that proper safety monitoring typically requires in‐person (on‐site) visits to perform physical examinations and reported challenges regarding fully decentralized safety monitoring. Namely, timely and uninterrupted access to interpretable safety data is vital, and safety data should be synchronized to the electronic medical record to ensure continuity of care. In addition, safety data should be reviewed regularly by site study staff. Opportunities to ensure timely review of safety data include (i) monitoring the investigator staff’s data review, (ii) provision of a stable data transfer connection, (iii) provision of mobile internet to trial participants if needed, and (iv) use of algorithms to assist manual review.
Data management and privacy
One potential challenge mentioned by the interviewees is that the participants’ personally identifiable data should not be available to the sponsor during a DCT. Therefore, several respondents indicated that activities during which personal data is obtained or required—including screening procedures and shipment of IMP—should be performed under the responsibility of the investigator. In addition, the data flow—including the data transfer and (temporary) data storage—should be clearly described.
Trial participants’ interests
Many respondents highlighted reducing the burden of trial participation as one of the main opportunities for DCTs. The DCTs could also enable the inclusion of patients with reduced or challenged mobility, as well as patients from larger geographic areas. However, multiple interviewees indicated that the inclusion of digitally illiterate patients (e.g., elderly people) in DCTs may be a challenge, although others indicated that elderly patients may be able to participate (Supplementary Information Quote S2 ).
The limited in‐person interaction in a DCT was considered a challenge. The respondents highlighted the importance of in‐person visits for engaging participants and building rapport, which was considered particularly helpful for recruiting and retaining participants. Furthermore, in‐person visits may be important for assessing whether patients are suitable for a CT and could help participants decide whether to participate. One respondent explained this as follows:
If you are face‐to‐face, you see the whole patient; there’s a direct contact and you can get attention to a medical health condition or characteristics which you would not have seen if you just have a video. You could miss something that may lead to exclusion or maybe an additional risk (clinical trial assessor).
It was recognized that there is an opportunity to introduce a “personal contact moment” in DCTs with the incorporation of home visits, which could also facilitate certain study activities, such as complex IMP administration.
Data quality
A recurrent theme in the interviews was the regulatory acceptance of data generated by decentralized means. Six aspects were identified relating to this theme (Figure 2 ).
Figure 2.
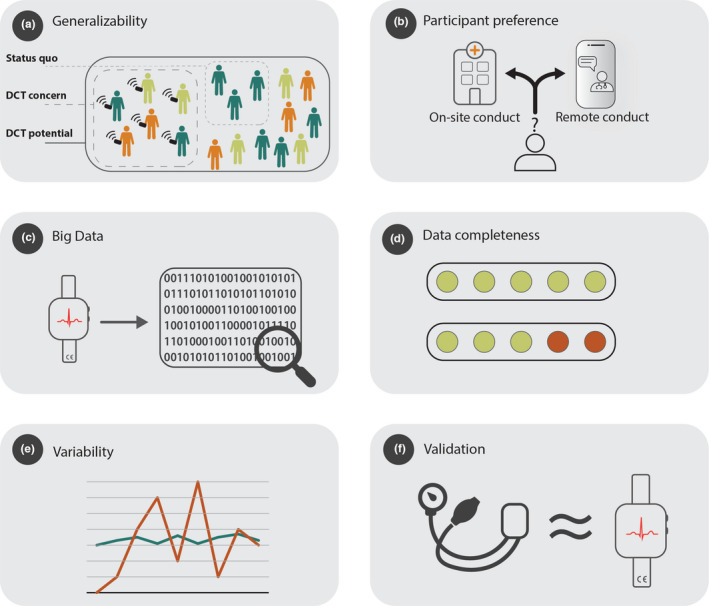
Graphical representation of the data quality sub‐themes identified from the interview data. (a) Generalizability; the current inability to recruit a diverse and representative trial population for a clinical trial, the concern that DCT recruitment is limited to participants with digital skills, and the potential of DCTs to recruit a representative sample generalizable to the target population. (b) Participant preference; the opportunity to incorporate participant preferences and the potential impact of different data collection methods on the outcomes. (c) Big Data; the challenge to interpret large datasets generated through, for example, wearables. (d) Data completeness; the opportunity to generate more complete data through passive data collection, and the challenge of more missing data because of poor technology adherence. (e) variability; the potential increase in variability in DCTs, because more data collection methods are utilized. (f) Validation; the challenge to validate novel digital outcomes. DCT, decentralized clinical trial. [Colour figure can be viewed at wileyonlinelibrary.com]
Generalizability
There was a diversity of views regarding generalizability in the context of a DCT. Several respondents were concerned about enrolling a “skewed population,” as both online recruitment and digital illiteracy in relation to the digital tools were considered potential challenges. However, other respondents indicated that conventional CTs are subject to similar challenges and remarked that DCTs may attract populations who are not included in conventional CTs, making them more generalizable. Furthermore, respondents mentioned that DCTs offer the possibility to test IMP closer to a real‐world setting (Supplementary Information Quote S3 ).
Participant preference
The option to introduce decentralized or on‐site activities according to a participant’s preference or need, was considered an opportunity for DCTs. However, other respondents were concerned about these optional approaches, as different methods of data collection could differently affect the outcomes (Supplementary Information Quote S4 ). As a solution, one clinical data assessor indicated that the optional approach should be incorporated in both the interventional and control arms, and proper randomization should be ensured.
Big data
Incorporating digital technologies in DCTs may provide further opportunities for continuous data collection, thereby generating large data sets. However, the respondents indicated that the generation of “Big Data” through digital technology could unnecessarily burden participants and the dataset could be challenging to interpret (Supplementary Information Quote S5 ).
Data completeness
Missing data and the reasons for these gaps could create challenges for data interpretation and were considered by several respondents to be a challenge for DCTs:
If, remotely, something is missing, it may be very unclear what is happening. […] If, for instance, you think about a diary where the patient enters a score every day. If you do this for a year and let’s say 50% of the entries are missing, it will be very difficult to interpret because you cannot just simply assume that he forgot to answer or that it's not related to the outcome (clinical data assessor).
However, other respondents argued that DCTs provide the opportunity to reduce missing data by improving protocol compliance, training stakeholders, passively collecting data, implementing monitoring and reminder systems, considering device practicalities, and enabling visits through the use of home nurses.
Variability
Interviewees also mentioned that variability of measurements may increase in DCTs, due to self‐measurement, the inclusion of local healthcare professionals and laboratories, and more diverse populations. This potential increase in variability was considered a challenge by the respondents, as it could hinder the inference of drug effects. Therefore, it was suggested that DCTs may need to enroll larger samples and must limit the amount of missing data. It should also be ensured that the participant‐reported data are entered and generated by the trial participants themselves—for example, using adequate identification systems.
Validation
The respondents indicated that the validation of novel digital outcome measures might be challenging because sponsors may not know what is expected of them when validating a new outcome and may be unwilling to invest in novel outcome measures when conventional and accepted alternatives are available. The respondents agreed that accepted outcome measures could be adopted for at‐home situations, albeit dependent on the context of the CT, as one interviewee explained:
[Adopting an accepted measurement to an at‐home situation] would be acceptable, but what we would like to know is: how do you do it? And if you do, what study population do you have? Are they used to taking their blood pressure at home? Does everyone in the study population have the same wearables? Are they trained? Is there a helpdesk they can call if they have issues? (clinical trial assessor).
In the context of digital data‐collection technologies, CT assessors in particular highlighted that the devices used to collect the data should have a Conformité Européenne marking to show they are used in line with their intended use.
Future directions
According to the respondents, the COVID‐19 pandemic and associated restrictions have been a catalyst for the implementation of decentralized elements in CTs. To ensure further mutual learning, the respondents emphasized that DCT approaches should be discussed with regulators—for example, through scientific advice. In addition, the use of hybrid CTs was advocated by the respondents to gain more experience with a combination of decentralized elements, whereas allowing for the incorporation of on‐site visits.
Currently, the acceptance of individual decentralized elements—such as electronic consent and DtP IMP supply—differs between NCAs, due to variation in national legislation. In addition, the respondents explained that ethics committees may have different views regarding the implementation of decentralized elements. To harmonize the evaluation of DCTs, the respondents described the need for a consolidated opinion on DCTs, which is being drafted by the CTFG is (at the time of the interviews). The application of the 536/2014 EU Clinical Trials Regulation (CTR) could further lead to a more harmonized evaluation of DCTs. One respondent explained this as follows:
When it comes to an individual clinical trial under the CTR, there will be this common assessment as well. So, I suppose that that will facilitate the discussion as well, and hopefully, at some point, we will have a common view in Europe (clinical trial assessor).
DISCUSSION
In this study, we investigated the perspectives of European regulators regarding the implementation of DCTs for benefit‐risk assessments. Opportunities and challenges for implementing DCTs were identified. Of note, several identified challenges may also be relevant for conventional CTs, such as challenges related to the validation of data collection tools, investigator oversight, and generalizability of trial results—although some may be more evident for DCTs.
Justification of decentralized elements
In this study, we found that DCT approaches may be considered for a diverse set of TAs and target populations, as was also illustrated by a pilot project conducted in Sweden in which DCTs were used for all phases throughout clinical development, covering a diverse set of TAs (including diabetes, COVID‐19, and breast cancer). 19 Clinical development for rare diseases may, however, especially benefit from a DCT approach, as participant recruitment may be difficult, requiring continued evidence generation after marketing authorization has been granted. 30
Data quality of data generated by decentralized means
It has been suggested that digital technologies could lead to more clinically meaningful end points than conventional end points, as data could be collected more frequently, and more objectively due to the reduced impact of observer and recall bias. 31 , 32 Although the opportunity to collect richer data via digital technologies was recognized by the regulators, they were cautious about the impact of large data sets on end points. In addition, missing data due to technical defects or poor technology adherence were found to be a potential challenge. Solutions to limit missing data are context‐specific but could include training, sending reminders, minimizing participation burden, making user support available (e.g., helpdesks), backing‐up operating systems, and validating the technology. 33 , 34
Challenges associated with the validation of digital technologies have been said to impede their uptake. 35 , 36 In agreement with our findings, a recent study found that the main concerns of the Committee for Medicinal Products for Human Use of the EMA regarding digital data collection technologies include the relevance and validation of the novel technology. 37 A discussion of the requirements for the qualification of digital technology is beyond the scope of this paper, but these have been previously described. 38 , 39
Investigator oversight
Although the involvement of third parties, such as home nurse services, may be necessary to manage DCTs, the respondents suggested that investigators may be hesitant to delegate specific tasks, as they may be held responsible for any noncompliance by third parties, as stated in ICH E6 R2 4.2.5 and 4.2.6. 40 Furthermore, previous research has found that training third parties, obtaining data from third parties, and obtaining ethics approval can all create additional challenges for the involvement of third parties in a DCT. 41 Home nursing services provided through a site’s existing infrastructure can address these issues. The use of external home nurse services could also be considered, provided the qualifications are clear.
Participants’ interests and generalizability
The reduction in the burden on participants was considered by the regulators to be a key opportunity for DCTs. However, there is also a need to avoid overburdening participants with digital technology. 42 In addition, the (perceived) need for in‐person visits—for physical examinations and to build a relationship—could limit the implementation of full DCTs. A trusting relationship between the investigator and (potential) trial participants has been shown in trials to aid the recruitment and retention of trial participants. 43 However, other studies have shown that recruiting participants through online means can accelerate and improve recruitment rates, compared with traditional on‐site participant recruitment. 44 , 45 In DCTs, safety of participants and relationships with investigator staff should be ensured and maintained through regular contact via decentralized means or home visits.
The risk of excluding digitally illiterate participants was considered a potential challenge for DCTs, with elderly participants considered to be more often digitally illiterate. Whereas digital recruitment strategies have recruited younger participants in some studies, 44 , 46 another study found no differences between traditional and digital recruitment strategies in terms of age. 47 In addition, DCTs can use recruitment strategies similar to conventional CTs, such as physicians’ networks and registries. Although recruitment of demographically skewed samples may limit the generalizability of trial results, it should be noted that conventional CTs suffer from similar issues because of strict eligibility criteria or sampling in specific clinical settings. 48
Future directions
In this study, regulators said they were open to DCT proposals but indicated that their experiences with full DCTs were limited. The Danish Medicines Agency’s and Swissmedic/Swissethics DCT guidance emphasize that experience is needed “to identify the weaknesses and strengths […], including the impact of the reduced face‐to‐face visits” 18 and to show if “new standards are needed to approve DCTs”. 20 The respondents in this study suggested that regulators should be approached with proposals for (hybrid) DCTs, for example, through EMA scientific advice. This process of learning‐by‐doing can be supplemented by providing training for regulators to support the evaluation of DCTs, complex datasets, and novel end points through initiatives such as Trials@Home (https://trialsathome.com/), Mobilise‐D (https://www.mobilise‐d.eu/), RADAR‐AD (https://www.radar‐ad.org/), and the United States‐based Clinical Trials Transformation Initiative (https://ctti‐clinicaltrials.org/). In addition, changes in CT conduct engendered by the COVID‐19 pandemic provide the opportunity to identify learnings relevant for DCTs. For example, the US Food and Drug Administration Oncology Center of Excellence has launched an initiative to evaluate the effect of decentralized assessments on data quality and to identify mitigation strategies from trial data affected by the COVID‐19 pandemic. 49
Endeavors to harmonize guidance and regulations regarding decentralized elements on a European level may further facilitate the uptake of DCTs and could overcome the need for country‐specific adjustments. For example, there is currently no consensus in the European Union regarding the acceptability and validity of using decentralized elements, such as electronic signatures to obtain informed consent via decentralized means, and the shipment of IMPs directly to trial participants. 50
Strengths, limitations, and suggestions for future research
This study provides a list of important opportunities and challenges for the implementation of DCTs in Europe from a regulatory perspective. This study incorporated complementary perspectives of regulators from different European regions involved in assessing the authorization, conduct, and clinical data of CTs. However, their representativeness may be restricted, as the perspectives of regulators who are less familiar with—or more critical of—DCT approaches may have been limited. Although no prior experience with DCTs was required to participate in this project, we found that some potential interviewees chose not to participate in this research due to lack of experience. As such, the perspective of regulators who are less supportive of DCTs may not have been fully captured in this research. Furthermore, the individual perspectives captured in this research may not fully reflect the NCAs’ standpoints.
Currently, it is not clear whether decentralized elements and recruitment approaches allow for the inclusion of a more representative and diverse trial population. In addition, data on the comparability of DCTs and conventional CTs are needed. Finally, the development of a regulatory framework for DCT assessment and educational activities could facilitate mutual learning by sponsors and regulators. Future studies on these topics are therefore recommended.
CONCLUSION
Regulators agree that DCT approaches can be considered for various types of trials, provided that the decentralized elements are justified considering the research question and trial characteristics. The key opportunities of DCTs recognized by European regulators include exerting a lower participation burden, allowing underserved groups to participate in CTs, and capturing data from the “real world.” However, from a regulatory perspective, reducing face‐to‐face contact, and the maintenance of investigator oversight when involving third parties are considered challenges to implementation of DCTs. The possible impact of decentralization on data quality should also be addressed when designing a DCT. The factors identified in this study indicate that the EU regulatory network is ready to gain experience with DCTs to ensure participant‐centered trials.
FUNDING
This work has received support from the EU/EFPA Innovative Medicines Initiative Joint Undertaking Trials@Home (grant No. 831458). The Innovative Medicines Initiative (IMI) website can be accessed through the following link: www.imi.europa.eu.
CONFLICT OF INTEREST
The authors declared no competing interests for this work.
AUTHOR CONTRIBUTIONS
A.J.d.J., T.I.v.R., M.G.P.Z., G.J.M.W.v.T., S.A., J.F.M., T.D.S., A.d.B., Y.S.A.T., and H.G wrote the manuscript. A.J.d.J., Y.S.A.T., M.G.P.Z., and H.G. designed the research. A.J.d.J. performed the research. A.J.d.J, T.I.v.R., and Y.S.A.T. analyzed the data.
DISCLAIMER
This paper reflects the views of the Trials@Home consortium and neither IMI nor the European Union and EFPIA are liable for any use that may be made of the information contained herein.
Supporting information
Table S1
Table S2
Supplementary Material
ACKNOWLEDGMENTS
The authors thank the respondents for their time and willingness to participate in this research project.
DATA AVAILABILITY STATEMENT
Interview transcript data was used in this study. Participants did not consent to make the transcripts publicly available. Supporting quotes are available in the results section of this paper. Excerpts from anonymized transcripts can be made available upon request. Please contact the corresponding author for more information.
- 1. Fogel, D.B. Factors associated with clinical trials that fail and opportunities for improving the likelihood of success: a review. Contemp. Clin. Trials Commun. 11, 156–164 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Gross, D. & Fogg, L. Clinical trials in the 21st century: the case for participant‐centered research. Res. Nurs. Health 24, 530–539 (2001). [DOI] [PubMed] [Google Scholar]
- 3. Gul, R.B. & Ali, P.A. Clinical trials: the challenge of recruitment and retention of participants. J. Clin. Nurs. 19, 227–233 (2010). [DOI] [PubMed] [Google Scholar]
- 4. Walters, S.J. et al. Recruitment and retention of participants in randomised controlled trials: a review of trials funded and published by the United Kingdom Health Technology Assessment Programme. BMJ Open 7, e015276 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Carlisle, B. , Kimmelman, J. , Ramsay, T. & MacKinnon, N. Unsuccessful trial accrual and human subjects protections: an empirical analysis of recently closed trials. Clin. Trials 12, 77–83 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Amstutz, A. et al. Discontinuation and non‐publication of randomised clinical trials supported by the main public funding body in Switzerland: a retrospective cohort study. BMJ Open 7, e016216 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kasenda, B. et al. Prevalence, characteristics, and publication of discontinued randomized trials. JAMA 311, 1045–1051 (2014). [DOI] [PubMed] [Google Scholar]
- 8. Trials@Home . Trials@Home glossary <https://trialsathome.com/trialshome‐glossary/> (2020). Accessed January 18, 2022.
- 9. Khozin, S. & Coravos, A. Decentralized trials in the age of real‐world evidence and inclusivity in clinical investigations. Clin. Pharmacol. Ther. 106, 25–27 (2019). [DOI] [PubMed] [Google Scholar]
- 10. Izmailova, E.S. , Wagner, J.A. & Perakslis, E.D. Wearable devices in clinical trials: hype and hypothesis. Clin. Pharmacol. Ther. 104, 42–52 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Li, G. et al. Digitalized adaptation of oncology trials during and after COVID‐19. Cancer Cell 38, 148–149 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gaba, P. & Bhatt, D.L. The COVID‐19 pandemic: a catalyst to improve clinical trials. Nat. Rev. Cardiol. 17, 673–675 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Xue, J.Z. et al. Clinical trial recovery from COVID‐19 disruption. Nat. Rev. Drug Discov. 19, 662–663 (2020). [DOI] [PubMed] [Google Scholar]
- 14. Waterhouse, D.M. et al. Early impact of COVID‐19 on the conduct of oncology clinical trials and long‐term opportunities for transformation: findings from an American Society of Clinical Oncology Survey. JCO Oncol. Pract. 16, 417–421 (2020). [DOI] [PubMed] [Google Scholar]
- 15. TransCelerate Biopharma Inc . Beyond COVID‐19: modernizing clinical trial conduct <https://www.transceleratebiopharmainc.com/wp‐content/uploads/2020/07/TransCelerate_Beyond‐COVID19_Modernizing‐Clinical‐Trial‐Conduct_July‐2020.pdf> (2020). Accessed January 18, 2022.
- 16. National Academies of Sciences, Engineering, and Medicine . Virtual Clinical Trials: Challenges and Opportunities: Proceedings of a Workshop (The National Academies Press, Washington, DC, 2019). [PubMed] [Google Scholar]
- 17. de Jong, A.J. et al. COVID‐19 and the emerging regulatory guidance for ongoing clinical trials in the European Union. Clin. Pharmacol. Ther. 109, 1517–1527 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Danish Medicines Agency . The Danish Medicines Agency’s guidance on the implementation of decentralised elements in clinical trials with medicinal products <https://laegemiddelstyrelsen.dk/en/news/2021/guidance‐on‐the‐implementation‐of‐decentralised‐elements‐in‐clinical‐trials‐with‐medicinal‐products‐is‐now‐available/~/media/5A96356760ED408CBFA9F85784543B53.ashx> (2021). Accessed October 20, 2021.
- 19. Swedish Medical Products Agency . Decentralised and virtual interventional clinical trials <https://www.lakemedelsverket.se/en/permission‐approval‐and‐control/clinical‐trials/medicinal‐products‐for‐human‐use/decentralised‐and‐virtual‐interventional‐clinical‐trials> (2021). Accessed November 26, 2021.
- 20. Swissmedic and Swissethics . Position paper by Swissmedic and swissethics on decentralized clinical trials (DCTs) with medicinal products <https://www.swissmedic.ch/swissmedic/en/home/humanarzneimittel/clinical‐trials/clinical‐trials‐on‐medicinal‐products/publikationen.html> (2021). Accessed March 9, 2021.
- 21. BfArM . BfArM im dialog: decentralised clinical trials (DCT) <https://www.bfarm.de/DE/Aktuelles/Veranstaltungen/Termine/2021‐06‐30‐dezentrale_klinische_pruefungen.html> (2021). Accessed October 27, 2021.
- 22. Coert, R.M.H. , Timmis, J.K. , Boorsma, A. & Pasman, W.J. Stakeholder perspectives on barriers and facilitators for the adoption of virtual clinical trials: qualitative study. J. Med. Internet Res. 23, e26813 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Polhemus, A.M. et al. Accelerating adoption of patient‐facing technologies in clinical trials: a pharmaceutical industry perspective on opportunities and challenges. Ther. Innov. Regul. Sci. 53, 8–24 (2019). [DOI] [PubMed] [Google Scholar]
- 24. Cox, S.M. , Lane, A. & Volchenboum, S.L. Use of wearable, mobile, and sensor technology in cancer clinical trials. JCO Clin. Cancer Informatics 2, 1–11 (2018). [DOI] [PubMed] [Google Scholar]
- 25. Tong, A. , Sainsbury, P. & Craig, J. Consolidated criteria for reporting qualitative research (COREQ): a 32‐item checklist for interviews and focus groups. Int. J. Qual. Health Care 19, 349–357 (2007). [DOI] [PubMed] [Google Scholar]
- 26. Trials@Home (Work Package 2 – TECH) . Deliverable 2.3 – technology scan <https://trialsathome.com/wp‐content/uploads/2020/10/D2.3‐Scanning‐results_Master.pdf> (2020). Accessed March 1, 2021.
- 27. Saunders, B. et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual. Quant. 52, 1893–1907 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. United Nations (Statistics Division) . Geographic regions <https://unstats.un.org/unsd/methodology/m49/> (2021). Accessed July 13, 2021.
- 29. Braun, V. & Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101 (2006). [Google Scholar]
- 30. Pontes, C. et al. Evidence supporting regulatory‐decision making on orphan medicinal products authorisation in Europe: methodological uncertainties. Orphanet J. Rare Dis. 13, 206 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Boehme, P. et al. How soon will digital endpoints become a cornerstone for future drug development? Drug Discov. Today 24, 16–19 (2019). [DOI] [PubMed] [Google Scholar]
- 32. Stephenson, D. , Badawy, R. , Mathur, S. , Tome, M. & Rochester, L. Digital progression biomarkers as novel endpoints in clinical trials: a multistakeholder perspective. J. Parkinsons Dis. 11, S103–S109 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Marquis‐Gravel, G. et al. Technology‐enabled clinical trials: transforming medical evidence generation. Circulation 140, 14261436 (2019). [DOI] [PubMed] [Google Scholar]
- 34. European Medicines Agency . Guideline on computerised systems and electronic data in clinical trials (draft) <https://www.ema.europa.eu/en/documents/regulatory‐procedural‐guideline/draft‐guideline‐computerised‐systems‐electronic‐data‐clinical‐trials_en.pdf> (2021). Accessed October 27, 2021.
- 35. Coravos, A. et al. Modernizing and designing evaluation frameworks for connected sensor technologies in medicine. NPJ Digit. Med. 3, 37 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Mantua, V. , Arango, C. , Balabanov, P. & Butlen‐Ducuing, F. Digital health technologies in clinical trials for central nervous system drugs: an EU regulatory perspective. Nat. Rev. Drug Discov. 20, 83–84 (2021). [DOI] [PubMed] [Google Scholar]
- 37. Dekker, M.J.H.J. , Stolk, P. & Pasmooij, A.M.G. The use of remote monitoring technologies: a review of recent regulatory scientific advices, qualification opinions, and qualification advices issued by the European Medicines agency. Front. Med. 8, 619513 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Goldsack, J.C. et al. Verification, analytical validation, and clinical validation (V3): the foundation of determining fit‐for‐purpose for Biometric Monitoring Technologies (BioMeTs). NPJ Digit. Med. 3, 55 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. European Medicines Agency . Questions and answers: qualification of digital technology‐based methodologies to support approval of medicinal products <https://www.ema.europa.eu/en/documents/other/questions‐answers‐qualification‐digital‐technology‐based‐methodologies‐support‐approval‐medicinal_en.pdf> (2020). Accessed December 21, 2021.
- 40. International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use . Guideline for good clinical practice ICH E6 (R2) <https://www.ich.org/page/efficacy‐guidelines> (2016).
- 41. Apostolaros, M. et al. Legal, regulatory, and practical issues to consider when adopting decentralized clinical trials: recommendations from the clinical trials transformation initiative. Ther. Innov. Regul. Sci. 54, 779–787 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Coyle, J. et al. Learning from remote decentralised clinical trial experiences: A qualitative analysis of interviews with trial personnel, patient representatives and other stakeholders. Br. J. Pharmacol. 88, 1031–1042 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Chhatre, S. et al. Patient‐centered recruitment and retention for a randomized controlled study. Trials 19, 205 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Moseson, H. , Kumar, S. & Juusola, J.L. Comparison of study samples recruited with virtual versus traditional recruitment methods. Contemp. Clin. Trials Commun. 19, 100590 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Brøgger‐Mikkelsen, M. , Ali, Z. , Zibert, J.R. , Andersen, A.D. & Thomsen, S.F. Online patient recruitment in clinical trials: systematic review and meta analysis. J. Med. Internet Res. 22, e22179 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Frandsen, M. , Thow, M. & Ferguson, S.G. The effectiveness of social media (Facebook) compared with more traditional advertising methods for recruiting eligible participants to health research studies: a randomized, Controlled Clinical Trial. JMIR Res. Protoc. 5, e161 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Reuter, K. , Liu, C. , Le, N. , Angyan, P. & Finley, J.M. General practice and digital methods to recruit stroke survivors to a clinical mobility study: comparative analysis. J. Med. Internet Res. 23, e28923 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Kennedy‐Martin, T. , Curtis, S. , Faries, D. , Robinson, S. & Johnston, J. A literature review on the representativeness of randomized controlled trial samples and implications for the external validity of trial results. Trials 16, 495 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. FDA Oncology Center of Excellence . Advancing oncology decentralized trials <https://www.fda.gov/about‐fda/oncology‐center‐excellence/advancing‐oncology‐decentralized‐trials> (2021). Accessed March 9, 2021.
- 50. Trials@Home work package 4 (EAGLE) . Deliverable 4.1: mapping and analysis of the EU legislation on remote decentralised clinical trials including legal, regulatory, ethical and stakeholder recommendations for the conduct of the pan‐EU pilot <https://trialsathome.com/mapping‐and‐analysis‐of‐the‐eu‐legislation‐on‐remote‐decentralised‐clinical‐trials‐d4‐1/> (2021). Accessed March 9, 2021.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1
Table S2
Supplementary Material
Data Availability Statement
Interview transcript data was used in this study. Participants did not consent to make the transcripts publicly available. Supporting quotes are available in the results section of this paper. Excerpts from anonymized transcripts can be made available upon request. Please contact the corresponding author for more information.