

Abstract
While racial/ethnic oral health inequities have been documented for many years in the United States, the potential role of racism has not been examined until recently. In fact, the common practice has been to attribute racial/ethnic disparities in oral health to low socioeconomic position and/or the lack of access to care. In contrast, racism is considered a fundamental cause of a broad range of adverse health outcomes for racial/ethnic minorities. Emerging evidence on oral health suggests that racism can affect access to oral health and clinical decision‐making by acting as a social determinant of health (SDoH). Specifically, SDoHs may affect access to quality dental care due to the lack of dental insurance, low dentist‐population ratio in racial/ethnic minority communities and the lack of diversity in the dental profession. We describe potential mechanisms through which racism can affect important SDoHs that are essential to oral health equity, outline recommendations to mitigate its existing negative effects and propose interventions to minimize pathogenic effects of racism on oral health outcomes in the population.
Keywords: oral health, race/ethnicity, racism
Oral health is essential for an individual's general health and wellbeing. Although oral health in the United States (U.S.) has improved over time, inequities associated with race/ethnicity and socioeconomic position remain pervasive [1]. For instance, recent national data show that Black or African American (these terms are used interchangeably) and Mexican American children between 6 and 9 years old are more likely to have untreated tooth decay in their primary and/or permanent dentition than their White counterparts. A similar pattern is evident for tooth decay among adults 65–74 years of age, and for moderate to severe periodontitis, among adults 45–74 years old. Mexican American and African American adults are also more likely to have untreated tooth decay and moderate–severe periodontitis than White adults. With regards to socioeconomic position, children of families with income below the poverty level are more likely to have untreated tooth decay than their peers of families with higher income. Moreover, adults 65–74 years old with less than a high school education are almost three times as likely to have untreated tooth decay and experience complete tooth loss, compared with adults with more than a high school education. Interestingly, these socioeconomic inequities are observed across racial/ethnic groups with Blacks and Mexican Americans carrying a higher burden suggesting that race and ethnicity adversely affects oral health, independent of socioeconomic indicators.
While oral health inequities have been attributed to behaviors such as tobacco use and poor dietary choices, the major driver of these inequities appears to be reduced access to quality dental health services due to limited access to a dental provider and/or a lack of dental insurance. Historic and ongoing policies of racism have created large racial/ethnic variations in income, education, employment and wealth that are strong predictors of access to health and dental insurance. To that end, racism can affect access to oral healthcare and/or appropriate clinical decision‐making by acting as a social determinant of health (SDoH) through reduced access to quality dental care via low dentist‐population ratio in minority communities, and poorer quality of care linked to the lack of diversity in the profession. A low dentist‐population ratio in minority communities contributes to reduced access to quality dental care. African Americans and Hispanics or Latinos (these terms are used interchangeably) represent 13.4% and 18.5% of the U.S. population, respectively. However, as of 2020, Blacks were 3.8% and Latinos were 5.9% of U.S. practicing dentists [2]. Interestingly, these proportions have remained virtually unchanged since 2010 (Figure 1) [3]. The lack of racial/ethnic diversity of the dental profession has serious implications for oral health inequities by creating “dental deserts” (racial/ethnic minority communities with very few or no dentists) [4]. It is estimated that 64 million Americans reside in areas with a shortage of dental professionals. These “dental deserts” are especially prevalent in rural and low‐income communities. The dentist‐population ratio in the United States was 61 dentists per 100,000 population in 2020; a ratio that has remained nearly unchanged since 2012 (60 dentists per 100,000 population) [4]. In fact, the U.S. Human Resources and Services Administration (HRSA) estimated in 2022 that the United States will need 11,181 additional dental professionals to meet the needs of shortage areas. While data on the racial/ethnic dentist‐population ratio are not available, the striking lack of diversity in the dental profession suggests that very few dentists from underrepresented minority backgrounds are present in many racial/ethnic minority communities.
FIGURE 1.
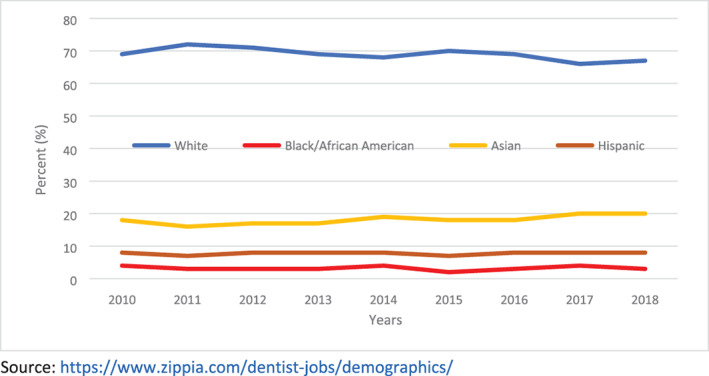
Racial/ethnic diversity of U.S. dental profession: 2010–2018 [Color figure can be viewed at wileyonlinelibrary.com]
Prior research indicates that racial/ethnic minority dentists are more likely to practice in minority and underserved communities than White dentists [5, 6]. For example, Black (81%) and Hispanic (67%) dentists are more likely to work in underserved areas than White dentists (48%). Black (63%) and Hispanic (50%) dentists are also more likely to participate in Medicaid or public insurance than their White counterparts (39%) [7]. Moreover, this lack of professional diversity has implications for minority patients' engagement with their dental providers. For instance, research has found higher levels of compliance and satisfaction with healthcare among racial/ethnic minority patients when treated by practitioners of their own cultural and racial/ethnic background compared to providers with a different background [8, 9]. In addition, limited diversity of dental professionals likely plays a role in bias related to clinical decision making when treating racial/ethnic minority patients. Research indicates that patients' race/ethnicity affects providers' clinical decisions especially when a patient is Black. For example, using the same clinical scenario with photographs and radiographs, Patel and colleagues showed that Black patients were more likely to receive a tooth extraction recommendation when presenting with a decayed tooth and symptoms of irreversible pulpitis relative to their White peers who were more likely to receive a root canal treatment recommendation for the same tooth [10]. Thus, diversification of the dental profession is likely to minimize implicit biases and improve the quality of care that racial/ethnic minority patients receive from their dental providers.
To reduce and/or avoid the ways in which racism can adversely affect oral health inequities, we need concerted efforts to acknowledge and remove the barriers affecting access to quality dental care in racial/ethnic minority communities. Specifically, we need a multi‐pronged approach to reduce and ultimately eliminate oral health inequities. First, we need to identify factors that may bias admissions to dental schools for racial/ethnic minority applicants such as standardized tests, for example, Dental Admission Test, on which many racial/ethnic minority students do not do well [11]. In tandem, we need to develop, fund and implement comprehensive plans to create sizeable cohorts of applicants from diverse racial/ethnic backgrounds that are prepared to successfully complete dental education. This would facilitate the creation of new cohorts of dental graduates that reflect the U.S. population and the communities that the profession of dentistry serves.
Moreover, increases in the racial/ethnic diversity of the student body should be one criterion considered in the accreditation of dental schools to highlight the vital importance of resolving the long‐standing racial/ethnic inequities in admission. A recent study suggests that although dental schools' enrollment for Black students increased between 2000 and 2019, Black students continue to be markedly under‐represented relative to all enrollees and their share of the U.S. population [12]. The small increase in African American students was due to the opening of new schools and increases in class size, as the rate of acceptance of Black students showed very little change. HRSA has projected a 9% increase of full‐time dentists in 2030 (207,930 vs. 190,510 in 2017) which may be adequate to meet projected growth in demand for oral health services. However, these projections did not explicitly incorporate either the racial/ethnic diversity of the U.S. population or the dental workforce [13]. Thus, the proposed increase in dentists is unlikely to address the lack of racial/ethnic diversity of the dental profession. In fact, if the increase were to be mostly in non‐Hispanic White dentists, this increase has the potential to markedly widen the existing inequities in the diversity of the workforce (and increase oral health inequities) given that the populations where the need is greatest are also the populations that are experiencing high rates of population growth.
Second, dental schools must expand their curriculum to integrate factors affecting oral health beyond individual‐level factors, using a multidisciplinary approach. Specifically, the curriculum should be expanded to include SDoHs, racism/discrimination, health equity, and public health, and how these factors can affect oral health. A recent National Academy of Sciences report outlines a similarly comprehensive and integrated agenda for the training of nurses in the United States [14]. Currently, although SDoHs appear in the pre‐doctoral dental curriculum, the training on this subject is limited and fragmented in separate courses in dental public health, community engagement and cultural competency. Thus, there is the need for comprehensive SDoHs content that is integrated throughout the curriculum with emphasis on a holistic approach rather than the current biomedical‐centric training [15, 16]. Such curriculum change can promote interdisciplinary collaboration within and outside the biomedical sciences (medicine, nursing, social workers, public health, social scientists, etc.) to expand the focus of dentists from the mouth/head to also giving greater attention to the whole person and their individual's needs as well as their social milieu. Furthermore, these curriculum changes should consider the role of risk and resilience factors that can affect oral health over the lifecourse. For example, dentistry needs to better address the needs of an aging population with a high retention of their teeth that is also challenged with the presence of chronic diseases and use of polypharmacy.
Third, there should be incentives in place to recruit and retain racial/ethnic minority dentists to work in underserved communities. For instance, current loan repayment programs should explicitly seek to recruit applicants during their senior year of dental schools from racial/ethnic diverse backgrounds, as well as others who would be interested in working in underserved areas. Moreover, future employers such as hospitals and local clinics, as well as federal agencies should create financial incentives for dentists, especially racial/ethnic minority dentists, to work in underserved and vulnerable communities (i.e., National Institutes of Health Loan Repayment Program for dentists without research training or careers) and/or retain these dentists to serve these communities. Finally, scholarship opportunities for dentists should be developed to obtain public health training. The latter will enhance the oral health research infrastructure by developing a cadre of scientists who can document, understand and effectively address racial/ethnic inequities in oral health in the U.S. population.
While the use of racial/ethnic categories has helped to document and track oral health inequities, racial and ethnic categories are the products of racism, and as such, merely documenting racial/ethnic inequities will not address racism. In fact, racism has been identified as a public health crisis [17] and as a serious threat to the nation's health [18]. Recent calls have also been made to acknowledge and address systemic racism as a commitment to health equity in medicine [19, 20, 21]. For example, the U.S. Preventive Services Task Force has outlined strategies to mitigate health inequities and other effects of systemic racism [21]. Similarly, mental health professionals are documenting how the social injustice of structural racism is adversely affecting the mental health of stigmatized racial/ethnic populations [20]. Finally, the President of the American Dental Association recently called for the elevation of dentistry through increased diversity at all levels of the profession [2]. The time has come for the profession of dentistry to support policy changes designed to reduce oral health inequities. This will require sustained attention by the dental profession not only to document the ways in which racism adversely affects oral health but also to have unquestioned leadership in designing, implementing and supporting interventions to eliminate the legacy of racism in oral health and oral care in the United States.
Borrell LN, Williams DR. Racism and oral health equity in the United States: Identifying its effects and providing future directions. J Public Health Dent. 2022;82(Suppl. 1):8–11. 10.1111/jphd.12501
REFERENCES
- 1. Office of Disease Prevention and Health promotion . Healthy People 2020. Oral Health. Objectives and National Snapshots Washington, DC. https://www.healthypeople.gov/2020/topics-objectives/topic/oral-health/national-snapshot.
- 2. Wright JT, Vujicic M, Frazier‐Bowers S. Elevating dentistry through diversity. J Am Dent Assoc. 2021;152(4):253–5. [DOI] [PubMed] [Google Scholar]
- 3. Zippia Careers. Healthcare Practitioner and Technical Industry. Dentist. Demographics and Statistics in the U.S. https://www.zippia.com/dentist-jobs/demographics/.
- 4. U.S. Health Resources & Services Administration. Health workforce. Shortage areas. January 4, 2022: HRSA; 2022. https://data.hrsa.gov/topics/health-workforce/shortage-areas.
- 5. Mertz E, Calvo J, Wides C, Gates P. The black dentist workforce in the United States. J Public Health Dent. 2017;77(2):136–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Mertz E, Wides C, Calvo J, Gates P. The Hispanic and Latino dentist workforce in the United States. J Public Health Dent. 2017;77(2):163–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. American Dental Association . ADA News. HPI publishes findings into racial disparities in oral health. https://www.ada.org/en/publications/ada-news/2021-archive/april/hpi-publishes-findings-into-racial-disparities-in-oral-health.
- 8. Blair IV, Havranek EP, Price DW, Hanratty R, Fairclough DL, Farley T, et al. Assessment of biases against Latinos and African Americans among primary care providers and community members. Am J Public Health. 2013;103(1):92–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cooper LA, Roter DL, Carson KA, Beach MC, Sabin JA, Greenwald AG, et al. The associations of clinicians' implicit attitudes about race with medical visit communication and patient ratings of interpersonal care. Am J Public Health. 2012;102(5):979–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Patel N, Patel S, Cotti E, Bardini G, Mannocci F. Unconscious racial bias may affect dentists' clinical decisions on tooth restorability: a randomized clinical trial. JDR Clin Trans Res. 2019;4(1):19–28. [DOI] [PubMed] [Google Scholar]
- 11. Rosales J, Walker T. The racist beginnings of standarized testing. Washington, DC: National Education Association; 2021. [cited 2021 November 19]. https://www.nea.org/advocating-for-change/new-from-nea/racist-beginnings-standardized-testing [Google Scholar]
- 12. Nalliah RP, Timothe P, Reddy MS. Diversity, equity, and inclusion interventions to support admissions have had little benefit to black students over past 20 years. J Dent Educ. 2021;85(4):448–55. [DOI] [PubMed] [Google Scholar]
- 13. U.S. Human Resources & Services Administration . Oral health workforce projections 2021. https://bhw.hrsa.gov/data-research/projecting-health-workforce-supply-demand/oral-health.
- 14.National Academy of Medicine. National Academies of Sciences, Engineering, and Medicine. The future of nursing 2020–2030: Charting a path to achieve health equity. Wakefield MK, Williams DR, Menestrel SL, Flaubert JL, editors. Washington, DC: The National Academies Press; 2021. [PubMed]
- 15. Tiwari T, Palatta A, Stewart J. The value of social determinants of health in dental education. NAM Perspectives. Commentary. Washington, DC: National Academy of Medicine; 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Tiwari T, Palatta AM. An adapted framework for incorporating the social determinants of Health into Predoctoral dental curricula. J Dent Educ. 2019;83(2):127–36. [DOI] [PubMed] [Google Scholar]
- 17. Racism is a Public Health Crisis . Health equity. Racism and health. Racism declarations. American Association of Public Health 2021. https://www.apha.org/topics-and-issues/health-equity/racism-and-health/racism-declarations.
- 18. Racism is a serious threat to the public's health. Health equity. Minority Health and Health Equity. Centers for Disease Control and Prevention 2021. https://www.cdc.gov/healthequity/racism-disparities/index.html.
- 19. Lin JS, Hoffman L, Bean SI, O'Connor EA, Martin AM, Iacocca MO, et al. Addressing racism in preventive services: methods report to support the US preventive services task force. JAMA. 2021;326:2412–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Shim RS. Dismantling structural racism in psychiatry: a path to mental Health equity. Am J Psychiatry. 2021;178(7):592–8. [DOI] [PubMed] [Google Scholar]
- 21. US Preventive Services Task Force . Actions to transform US preventive services task force methods to mitigate systemic racism in clinical preventive services. JAMA. 2021;326(23):2405–11. [DOI] [PubMed] [Google Scholar]