

Abstract
Transitioning out of the military can be a time of change and challenge. Research indicates that altered threat monitoring in military populations may contribute to the development of psychopathology in veterans, and interventions that adjust threat monitoring in personnel leaving the military may be beneficial. Australian Defence Force personnel (N = 59) transitioning from the military were randomized to receive four weekly sessions of either attention‐control training or a placebo attention training. The primary outcome was symptoms of posttraumatic stress disorder (PTSD), as measured using the PTSD Checklist for DSM‐5 (PCL‐5) at posttreatment. Following training, participants who received attention‐control training reported significantly lower levels of PTSD symptoms, Hedges’ g = 0.86, 95% CI [0.37, 1.36], p = .004, and significantly improved work and social functioning, Hedges’ g = 0.93, 95% CI [0.46, 1.39], p = .001, relative to those in the placebo condition. Moreover, no participants who received attention‐control training worsened with regard to PTSD symptoms, whereas 23.8% of those who received the placebo attention training experienced an increase in PTSD symptoms. The preliminary findings from this pilot study add to a small body of evidence supporting attention‐control training as a viable indicated early intervention approach for PTSD that is worthy of further research.
Threat monitoring, or the selective deployment of attention to potentially threatening stimuli, is adaptive and critical to human survival. However, it can become disrupted in the form of a maladaptive attention bias for threatening stimuli, which, in turn, leads to psychopathology (Naim et al., 2015). Research has shown that both exposure to traumatic events and military experiences are capable of producing a threat‐related attention bias. For example, threat‐related attention bias was found to be present in individuals who experienced a traumatic event but had not developed posttraumatic stress disorder (PTSD), whereas it was not observed in non–trauma‐exposed controls (Zhang et al., 2014). In the context of military populations, threat‐related attention bias is actively reinforced and adaptive, as hypervigilance toward potentially threatening cues can be life‐saving and necessary in deployment situations (Wald et al., 2016).
However, threat‐related attention bias is largely maladaptive in civilian settings, where a significant threat is no longer present and, indeed, may predispose veterans to a range of mental health issues (Naim et al., 2015). Attention bias is one key mechanism thought to underpin the development of PTSD, typically manifesting as attention bias both toward threatening stimuli (i.e., consistent with the PTSD symptom of hypervigilance) and away from threatening stimuli (i.e., initially attending to a threatening stimulus before actively and effortfully focusing attention elsewhere, consistent with the avoidance symptoms of PTSD; Badura‐Brack et al., 2015). There is considerable evidence from military samples that threat‐related attention bias predicts the long‐term development and maintenance of PTSD symptoms (Sipos et al., 2014; Wald et al., 2016, 2011) and that high levels of within‐individual variation in attention bias (i.e., fluctuating between hypervigilance and avoidance of threat, termed attention‐bias variability [ABV]) are correlated with PTSD symptom severity (Alon et al., 2019; Badura‐Brack et al., 2015; Iacoviello et al., 2014). In response, attention training has been developed to reduce attention bias and, in turn, PTSD symptoms. Attention‐control training is a simple computer‐based paradigm that involves neutral and threat‐related stimuli and is thought to work by rebalancing attention to a normal level of threat monitoring (Schoorl et al., 2014). A number of studies have now identified attention‐control training as an indicated treatment for individuals with PTSD (Badura‐Brack et al., 2015; Naim et al., 2015; Wald et al., 2011).
Given that threat monitoring is altered throughout the experience of traumatic events and military training, upon leaving the military, veterans may need a recalibration of threat monitoring to facilitate adaptation to civilian life and reduce the risk of developing mental health issues. Transitioning out of the military is increasingly recognized as a period of significant stress on the career continuum of military populations, and this process may predispose veterans to the development of mental health conditions (Van Hooff et al., 2018). For example, recent research has shown that the risk of PTSD doubles within 5 years of leaving the military and transitioning to civilian life (Van Hooff et al., 2018). Although attention training has been tested as a means of PTSD prevention and treatment, it may have potential as an early intervention to inhibit the escalation of PTSD symptoms.
Early intervention for PTSD is typically defined as a treatment or intervention that is delivered within 3 months of a traumatic experience (Bisson et al., 2021). The key goal of early intervention is to prevent or attenuate the severity of psychological sequelae in high‐risk individuals by initiating treatment during the acute or subacute posttraumatic period (Giummarra et al., 2018). Given the unique nature of military service, where individuals can experience exposure to multiple traumatic events and attention bias is modified during training and deployment, mental health symptoms are often exacerbated after transitioning to civilian life; thus, the point of separation from the military presents an opportunity to intervene before the potential development or escalation of mental health symptoms. Help‐seeking military personnel transitioning to civilian life are a particularly vulnerable population, and veterans may present to providers with a range of mental health, well‐being, or transition‐related concerns, including issues related to PTSD. These individuals are, therefore, likely to gain significant benefit from an early intervention approach that targets and recalibrates threat monitoring.
The aim of the present study was to conduct a pilot randomized controlled trial (RCT) of attention‐control training for personnel transitioning out of the military in real‐world clinical service. We focused on help‐seeking individuals undergoing transition stress due to their potential vulnerability to the development of mental health disorders and the likelihood that they would benefit from a simple, early intervention treatment. We hypothesized that following the intervention, veterans who received attention‐control training would have significantly less severe PTSD symptoms and significantly improved functioning compared to veterans who received placebo attention training. Due to COVID‐19–related restrictions on face‐to‐face interactions, which were required for the attention training task, the RCT was terminated early in March 2020. The preliminary findings are reported here.
METHOD
Participants
Participants were treatment‐seeking military personnel and veterans recruited from Open Arms–Veteran and Families Counselling centers, Australia's leading government provider of mental health assessment and treatment for serving and formerly serving personnel and their families, between December 2018 and February 2020. The inclusion criteria were (a) being a serving member of the Australian Defence Force (ADF) who was leaving the military within the next 4 months or a formerly serving member who left within the past 4 months, (b) having served in the ADF for at least 12 months, and (c) being able to use a computer. There was no inclusion requirement concerning existing psychiatric disorders. The exclusion criteria were (a) having a medical condition that impaired reaction times and (b) currently receiving pharmacological treatment for bipolar or psychotic disorders that could impair cognition.
Procedure
A two arm‐parallel group RCT design was used. A research assistant at the testing site used online randomization software to randomize participants to either attention‐control training or placebo attention training. Participants were randomized at a ratio of 1:1. Both the onsite research assistant and participant were blinded to the intervention allocation and allocation sequence.
Both attention‐control training and placebo attention training were variations of the dot‐probe task, and both conditions involved four sessions, each lasting 10 min, delivered over 4 weeks. Each session consisted of 160 dot‐probe trials (Abend et al., 2014). In each trial, a fixation cross appeared for 500 ms, followed by a pair of words, presented one above the other, for 500 ms. Next, a probe display (either “<” or “>”) randomly appeared in the location of one of the previously presented words. The probe remained on the screen until the participant responded, which was followed by an intertrial interval of 500 ms. Participants were instructed to indicate the orientation of the arrowhead probe via a corresponding keyboard press and perform the task as quickly as possible without compromising accuracy. In the attention‐control training condition, participants were presented with both neutral (e.g., “chair”) and threat‐related (e.g., “death”) words and asked to respond to a target cue, per instructions issued at the beginning of the task. In this condition, the target appeared behind the threat word 50% of the time. In the placebo dot‐probe task, participants were presented with neutral words only and asked to respond to a target cue, per instructions issued at the beginning of the task. The trial was approved by the Departments of Defence and Veterans’ Affairs Human Research Ethics Committee (040‐18) and prospectively registered on the Australian and New Zealand Clinical Trials Registry (ACTRN12618001578291).
Measures
Participants were asked about sociodemographic characteristics; military service, including combat and deployment exposure; and current mental health treatment at pretreatment (Time 1 [T1]). Participants completed measures and PTSD symptoms and functional impairment at T1 and posttreatment (Time 2 [T2]), approximately four weeks later).
PTSD symptoms
PTSD symptoms, based on criteria in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM‐5; American Psychiatric Association, 2013), were assessed using the PTSD Checklist for DSM‐5 (Weathers et al., 2013). The PCL‐5 is a 20‐item, self‐report measure of past‐month PTSD symptoms, with responses scored on a 5‐point scale ranging from 0 (not at all) to 4 (extremely). Item scores were summed to give a total severity score ranging from 0 to 80, with higher scores indicating higher levels of symptom severity. Consistent with previous literature, scores of 33 or higher were used to indicate probable PTSD (Blevins et al., 2015). The PCL‐5 has demonstrated strong reliability and validity (Blevins et al., 2015). In the present study, Cronbach's alpha was .97 at time 1 and .96 at time 2.
Functional impairment
The five‐item Work and Social Adjustment Scale (Mundt et al., 2002) was used to assess functioning in the following domains: work, home management, social leisure activities, private leisure activities, and close relationships. Participants were asked to rate their level of impairment with respect to their ability to function in each of the five domains, scoring responses on a 9‐point scale ranging from 0 (not at all) to 8 (very severely). Scores are summed to create a total score ranging from 0 to 40, with higher scores indicating a higher level of impairment. Scores of 10 or higher indicate moderate impairment, and scores 20 or higher indicate severe impairment. The WSAS has demonstrated adequate‐to‐excellent internal scale consistency (Cronbach's αs = .70–.94) and a test–retest correlation of .73 (Mundt et al., 2002). In the present sample, Cronbach's alpha ranged from .70 to .94. Test–retest correlation was 0.73. In the present study, Cronbach's α was .93 at time 1 and .90 at time 2.
Data analysis
Initial power calculations were based on the prevention trial approach, with an expected PTSD prevalence rate of 20% in the control group and 15% in the treatment group, meaning a total sample size of 1,806 was required to detect a minimally important difference of 5% in PTSD prevalence rates, assuming 80% power and an alpha of .05. We used Mplus (Version 8.4; Muthén & Muthén, 1998–2017) to examine between‐ and within‐group differences on the PCL‐5 and WSAS. Two one‐way analyses of covariance (ANCOVAs) were estimated using the methods described by Green and Thompson (2012). Each ANCOVA compared the total scores on the dependent variable between the control and attention training groups at Time 2 (i.e., posttreatment), controlling for Time 1 total scores on the relevant dependent variable (i.e., PCL‐5 or WSAS total score). Missing data were managed using maximum likelihood ratio (MLR) estimation, which uses full information maximum likelihood to estimate model parameters, adjusting for the uncertainty due to missingness (Asparouhov et al., 2008, 2010) under Rubin's (1987) missing‐at‐random (MAR) assumption. To be consistent with the standard assumption of the homogeneity of slopes, the coefficients for the covariate were constrained to be equal across groups in each of the ANCOVAs; in addition, error variances were constrained to be equal across groups, consistent with the homogeneity of variance assumption. Within‐groups differences were then examined using paired‐samples t tests to examine whether Time 1 and Time 2 PCL‐5 and WSAS scores differed for each group separately. Hedges’ g is presented as a measure of effect size, with a value of 0.2 indicating a small effect, 0.5 a medium effect, and 0.8 a large effect (Cohen, 1988). Between‐group differences in demographic characteristics were tested using chi‐square tests.
In addition, exploratory analyses were conducted in SPSS (Version 26) to examine the ability of attention training to prevent increases in posttraumatic stress symptoms as assessed using the PCL‐5. Participants were split into two groups based on PCL‐5 scores: those whose scores decreased, remained the same or increased up to 4 points, and those who reported score increases of 5 points or more. This cutoff was chosen because a 5‐point difference is the minimum threshold of reliable change on the PCL‐5 and can be used to determine whether an individual has responded to treatment (Weathers et al., 2013). This variable was cross‐tabulated between groups, and a chi‐square test was conducted to examine whether the proportion of participants whose PCL‐5 score increased by 5 or more points varied by group. A two‐sided p value below .05 was considered significant throughout.
RESULTS
Figure 1 depicts the participant flow throughout the study. Demographic and service characteristics for the full sample (N = 59) are presented in Table 1. Groups were well‐matched on all variables (Table 1). Most participants attended all four sessions, and rates of intervention completion did not differ between the groups, with only three participants (12.0%) in the control group and two (5.9%) in the attention training group failing to complete all four training sessions, χ2(1, N = 59) = 0.695, p = .404, reflecting strong intervention adherence. Noncompleters were more likely to be commissioned officers (33.3%) and noncommissioned officers (7.4%), p = .025, compared to other ranks. No other significant differences were found between completers and noncompleters.
FIGURE 1.
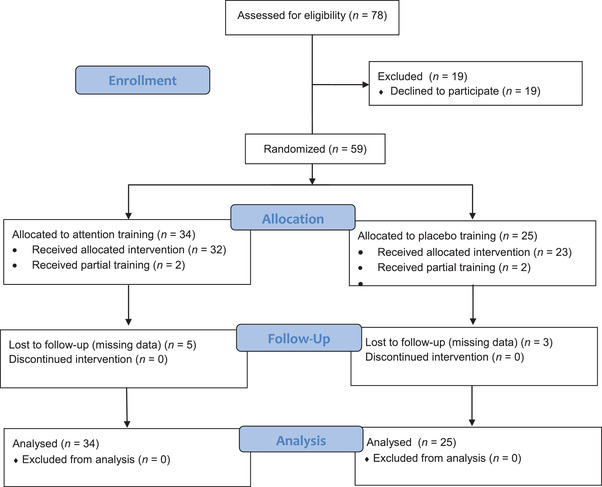
CONSORT 2010 flow diagram
TABLE 1.
Demographic and service characteristics, by attention task group
| Placebo training (n = 25) | Attention training (n = 34) | Total (n = 59) | |||||
|---|---|---|---|---|---|---|---|
| Variable | n | % | n | % | n | % | p |
| Sex | .365 | ||||||
| Male | 19 | 76.0 | 29 | 85.3 | 48 | 81.4 | |
| Female | 6 | 24.0 | 5 | 14.7 | 11 | 18.6 | |
| Age (years) a | .728 | ||||||
| 18–24 | 5 | 20.0 | 5 | 14.7 | 10 | 16.9 | |
| 25–34 | 9 | 36.0 | 10 | 29.4 | 19 | 32.2 | |
| 35–44 | 3 | 12.0 | 8 | 23.5 | 11 | 18.6 | |
| 45–54 | 6 | 24.0 | 6 | 17.6 | 12 | 20.3 | |
| ≥ 55 | 1 | 4.0 | 4 | 11.8 | 5 | 8.5 | |
| Rank a | .893 | ||||||
| Commissioned officer | 4 | 16.0 | 5 | 14.7 | 9 | 15.3 | |
| Noncommissioned officer | 10 | 40.0 | 17 | 50.0 | 27 | 45.8 | |
| Other ranks | 10 | 40.0 | 11 | 32.4 | 21 | 35.6 | |
| Ever deployed a | .947 | ||||||
| Yes | 16 | 64.0 | 23 | 67.6 | 39 | 66.1 | |
| No | 8 | 32.0 | 10 | 29.4 | 18 | 30.5 | |
| Ever experienced combat a | .197 | ||||||
| Yes | 2 | 8.0 | 9 | 26.5 | 11 | 18.6 | |
| No | 22 | 88.0 | 24 | 70.6 | 46 | 78.0 | |
| Involuntary discharge a | .616 | ||||||
| No | 10 | 40.0 | 18 | 52.9 | 28 | 47.5 | |
| Yes | 14 | 56.0 | 15 | 44.1 | 29 | 49.2 | |
| Currently treatment provider a | |||||||
| Psychologist | 13 | 52.0 | 20 | 58.8 | 33 | 55.9 | .867 |
| Psychiatrist | 10 | 40.0 | 10 | 29.4 | 20 | 33.9 | .658 |
| General practitioner | 11 | 44.0 | 8 | 23.5 | 19 | 32.2 | .228 |
| Counselor | 3 | 12.0 | 2 | 5.9 | 5 | 8.5 | .681 |
| Any professional | 17 | 68.0 | 21 | 61.8 | 38 | 64.4 | .830 |
Note: aMissing: Control group, n = 1 (4.0%); attention training group n = 1 (2.9%); total missing n = 2 (3.4%). bAmong participants who reported ever being exposed to a traumatic event. cAmong participants who reported ever being exposed to a traumatic event during deployment.
Time 1 (i.e., baseline) mean mental health and well‐being scores, by intervention group, are presented in Table 2. Participants in the control group reported a mean PCL‐5 score of 20.3 (SD = 20.3), whereas the mean score for participants in the attention training group was 19.7 (SD = 16.6). Among control group participants, 20.8% had probable PTSD (i.e., a score of 33 or higher on the PCL‐5), whereas 21.2% of those in the attention training group had probable PTSD. Participants in the control group reported a mean WSAS score of 12.4 (SD = 11.8), and those in the attention training group reported a mean of 11.3 (SD = 10.1), with both scores indicating moderate impairment. In total, 27.3% of participants in the control group and 30.0% in the attention training group reported a moderate level of impartment impairment based on WSAS scores, and 22.7% of the control group and 26.7% of the attention training group reported severe impairment. Independent‐samples t tests revealed no significant differences between the two intervention groups for any of the aforementioned comparisons (see Table 2 for exact values).
TABLE 2.
Posttraumatic Stress Disorder Checklist for DSM‐5 (PCL‐5) and Work and Social Adjustment Scale (WSAS) scores at Time 1, by attention training group
| Placebo training (n = 24) | Attention training (n = 33) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | M | SD | n | % | M | SD | n | % | p |
| PCL‐5 | 20.3 | 20.3 | 19.7 | 16.6 | .909 | ||||
| WSAS | 12.4 | 11.8 | 11.3 | 10.1 | .717 | ||||
| Work | 2.0 | 2.0 | 2.0 | 2.7 | .908 | ||||
| Home Management | 2.3 | 2.3 | 2.3 | 2.2 | .960 | ||||
| Social Leisure Activities | 3.0 | 2.6 | 2.7 | 2.5 | .624 | ||||
| Private Leisure Activities | 2.4 | 2.5 | 2.1 | 2.4 | .623 | ||||
| Family and Relationships | 2.4 | 2.7 | 2.2 | 2.2 | .787 | ||||
| PCL‐5 score ≥ 33 | 5 | 20.8 | 7 | 21.2 | .972 | ||||
| WSAS score ≥ 10 (moderate impairment) | 6 | 27.3 | 9 | 30.0 | ‐ | ||||
| WSAS ≥ 20 (severe impairment) | 5 | 22.7 | 8 | 26.7 | .890 | ||||
Note: Missing: WSAS control group, n = 2; attention training group, n = 3.
Two ANCOVAs were conducted to examine between‐group differences for Time 2 PCL‐5 and WSAS scores, controlling for Time 1 scores. The results of chi‐square difference tests showed that both models satisfied the homogeneity of slopes and homogeneity of variances assumptions (see Supplementary Table S1). Mean total PCL‐5 scores, Hedges’ g = 0.86, 95% CI [0.37, 1.36], p = .004, and total WSAS scores, Hedges’ g = 0.93, 95% CI [0.46, 1.39], p = .001, at Time 2 were significantly lower among participants in the attention training group compared to the control group. Within‐group means and differences are presented in Table 3.
TABLE 3.
Pre–post Posttraumatic Stress Disorder Checklist for DSM‐5 (PCL‐5) and Work and Social Adjustment Scale (WSAS) scores
| Variable | Time 1 (M) | Time 2 (M) | Hedges’ g | 95% CI | p |
|---|---|---|---|---|---|
| PCL‐5 | |||||
| Control | 19.81 | 19.69 | 0.01 | [−0.17, 0.18] | .952 |
| Attention training | 19.73 | 13.82 | 0.36 | [0.23, 0.50] | .000 |
| WSAS | |||||
| Control | 11.97 | 13.00 | −0.09 | [−0.28, 0.90] | .400 |
| Attention training | 11.33 | 9.13 | 0.22 | [0.06, 0.39] | .026 |
A chi‐square test was conducted to examine whether the proportion of participants whose PCL‐5 scores increased 5 points or more between Time 1 and Time 2 differed between groups (Table 4). The results showed that a significantly larger proportion of participants in the control group reported an increase of 5 or more points on the PCL‐5 compared to the attention training group, 0.0%, χ2(1, N = 50) = 7.672, p = .006.
TABLE 4.
Proportion of participants who reported an increase of 5 or more points on the Posttraumatic Stress Disorder Checklist for DSM‐5 (PCL‐5), by attention task group
| Placebo training | Attention training | Logistic regression | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | χ2(1, N = 50) | p | OR | 95% CI | p | |
| PCL‐5 | |||||||||
| Decrease or increase of ≤4 points | 16 | 76.2 | 29 | 100.0 | |||||
| ≥5‐point increase | 5 | 23.8 | 0 | 0.0 | 7.672 | .006 | |||
| PCL‐5 | |||||||||
| Decrease or remained the same | 10 | 47.6 | 24 | 82.8 | |||||
| Any increase | 11 | 52.4 | 5 | 17.2 | 6.912 | .009 | 5.28 | [1.46, 19.16] | .011 |
DISCUSSION
The aim of the present study was to examine whether attention‐control training, an emerging intervention for the prevention and treatment of PTSD, is a potentially viable early‐intervention strategy for veterans transitioning from the military. As predicted, participants who received four sessions of attention‐control training had significantly lower levels of PTSD symptoms and significantly improved functioning compared to those who received placebo attention training. These findings are consistent with previous studies in which attention‐control training has been shown to significantly reduce PTSD symptoms (Badura‐Brack et al., 2015; Schoorl et al., 2014). Moreover, no participants in the attention‐control training reported worsened in symptoms between pre‐ and posttreatment, whereas five participants (23.8%) who received placebo attention training scored at least 5 points higher on the PCL‐5 at posttreatment. This suggests that attention‐control training may play a preventative role in the development of PTSD.
Research indicates that military populations have altered threat monitoring. Both the experience of a traumatic event (Zhang et al., 2014) and military training (Naim et al., 2015) are capable of altering the human threat‐monitoring detection system. Researchers have found that an alternative version of attention training, known as attention bias modification training, used to increase attention bias to threat, is protective in combat situations, as it can increase an individual's hypervigilance regarding threats (Wald et al., 2016). As a result, attention bias modification training is now used in some military forces as part of a suite of military training. Yet although attention bias toward threatening stimuli is adaptive during deployment situations, this‐once adaptive cognitive processing style may become maladaptive for veterans reentering civilian life and, indeed, may increase the risk of developing PTSD. There is a need to rebalance a veteran's threat monitoring system as they leave the military to reduce their risk of developing psychopathology and increase the likelihood of a successful transition.
Although attention training has been used in a prevention and treatment approach, this novel proof‐of‐concept pilot tested the approach in the early intervention space. The findings show that a simple, brief, scalable early intervention delivered during the point of transition, when threat‐related attention bias is no longer adaptive, has significant potential. Improvements in functioning, including in the work, social, home, and relationship domains, were found. This effect is likely attributable to the negative consequences threat bias and PTSD symptoms have on multiple domains of an individual's functioning and well‐being.
The current study provides further evidence that transition from military to civilian life is a time during which there is the potential for mental health symptoms to worsen if there is no intervention. Almost one quarter of the control group (23.8%) experienced at least a 5‐point increase on the PCL‐5, indicating worsening PTSD symptoms, across the 4‐week study period, whereas no participants in the attention control group reported such symptom escalation. These preliminary findings speak to the potential for attention‐control training to be used in an early intervention capacity for treatment‐seeking military personnel who are at risk of experiencing the development or exacerbation of PTSD symptoms. The low dropout rate in both groups also suggests that the invention is acceptable to this population.
The limitations of this preliminary pilot trial include the small sample size and a lack of follow‐up data due to trial termination associated with COVID‐19 restrictions. The trial was significantly underpowered for a prevention trial, meaning the findings are extremely tentative. ABV was not systematically measured, and future research with a larger sample and follow‐up data collection to provide a better understanding of the exact cognitive mechanisms by which ABV is reduced through attention‐control training. Furthermore, specific subgroups of transitioning veterans, such as those who have been medically discharged or others at high risk of developing PTSD, may be more likely to benefit from this approach.
Military populations have altered threat‐monitoring systems that would benefit from recalibration upon transitioning from military service to reduce their risk of developing mental health disorders, including PTSD. Attention‐control training is a simple early intervention strategy that has the potential to rebalance threat monitoring to more adaptive levels suitable for civilian life. The results of the present study provide preliminary evidence that the provision of attention‐control training early in the military transition journey results in fewer PTSD symptoms and less functional impairment for veterans.
OPEN PRACTICES STATEMENT
The preregistration for this study can be accessed at: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=373973&isReview=true. Neither the data nor the materials have been made available on a permanent third‐party archive due to conditions of ethical approval; requests for the data or materials can be sent via email to the lead author at olivia.metcalf@unimelb.edu.au
ACKNOWLEDGMENTS
Open access publishing facilitated by The University of Melbourne, as part of the Wiley ‐ The University of Melbourne agreement via the Council of Australian University Librarians.
Metcalf, O. , O'Donnell, M. L. , Forbes, D. , Bar‐Haim, Y. , Hodson, S. , Bryant, R. A. , McFarlane, A. C. , Morton, D. , Poerio, L. , Naim, R. , & Varker, T. (2022). Attention‐control training as an early intervention for veterans leaving the military: A pilot randomized controlled trial. Journal of Traumatic Stress, 35, 1291–1299. 10.1002/jts.22828
This article was produced using funding provided by the Australian Government Department of Veterans’ Affairs. However, the views expressed do not necessarily represent the views of the Minister for Veterans’ Affairs or the Department of Veterans Affairs. The Commonwealth does not give any warranty nor accept any liability in relation to the contents of this work. This work is copyrighted by the Commonwealth of Australia (2022). Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced without prior written permission. Requests and inquiries concerning reproduction and rights should be directed in the first instance to the journal or to the Department of Veterans Affairs.
REFERENCES
- Abend, R. , Pine, D. S. , & Bar‐Haim, Y. (2014). The TAU‐NIMH Attention Bias Measurement Toolbox. In http://people.socsci.tau.ac.il/mu/anxietytrauma/research/
- Alon, Y. , Naim, R. , Pine, D. S. , Bliese, P. D. , & Bar‐Haim, Y. (2019). Validity of attention bias variability indices for posttraumatic stress disorder research: Evidence from patient data. Journal of Traumatic Stress, 32(5), 791–798. 10.1002/jts.22443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author. [Google Scholar]
- Asparouhov, T. , & Muthén, B. (2008). Auxiliary variables predicting missing data. Technical appendix. Muthén & Muthén. [Google Scholar]
- Asparouhov, T. , & Muthén, B. (2010). Chi‐square statistics with multiple imputation (Version 2). Technical appendix . Muthén & Muthén. [Google Scholar]
- Badura‐Brack, A. S. , Naim, R. , Ryan, T. J. , Levy, O. , Abend, R. , Khanna, M. M. , McDermott, T. J. , Pine, D. S. , & Bar‐Haim, Y. (2015). Effect of attention training on attention bias variability and PTSD symptoms: Randomized controlled trials in Israeli and US combat veterans. American Journal of Psychiatry, 172(12), 1233–1241. 10.1176/appi.ajp.2015.14121578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bisson, J. I. , Wright, L. A. , Jones, K. A. , Lewis, C. , Phelps, A. J. , Sijbrandij, M. , Varker, T. , & Roberts, N. P. (2021). Preventing the onset of posttraumatic stress disorder. Clinical Psychology Review, 86, 102004. 10.1016/j.cpr.2021.102004 [DOI] [PubMed] [Google Scholar]
- Blevins, C. A. , Weathers, F. W. , Davis, M. T. , Witte, T. K. , & Domino, J. L. (2015). The Posttraumatic Stress Disorder Checklist for DSM‐5 (PCL‐5): Development and initial psychometric evaluation. Journal of Traumatic Stress, 28(6), 489–498. 10.1002/jts.22059 [DOI] [PubMed] [Google Scholar]
- Giummarra, M. J. , Lennox, A. , Dali, G. , Costa, B. , & Gabbe, B. J. (2018). Early psychological interventions for posttraumatic stress, depression, and anxiety after traumatic injury: A systematic review and meta‐analysis. Clinical Psychology Review, 62, 11–36. 10.1016/j.cpr.2018.05.001 [DOI] [PubMed] [Google Scholar]
- Green, S. B. , & Thompson, M. S. (2012). A flexible structural equation modeling approach for analyzing means. In Hoyle R. H. (Ed.), Handbook of structural equation modeling (pp. 393–416). Guilford Press. [Google Scholar]
- Iacoviello, B. M. , Wu, G. , Abend, R. , Murrough, J. W. , Feder, A. , Fruchter, E. , Levinstein, Y. , Wald, I. , Bailey, C. R. , Pine, D. S. , Neumeister, A. , Bar‐Haim, Y. , & Charney, D. S. (2014). Attention bias variability and symptoms of posttraumatic stress disorder. Journal of Traumatic Stress, 27(2), 232–239. 10.1002/jts.21899 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mundt, J. C. , Marks, I. M. , Shear, M. K. , & Greist, J. H. (2002). The Work and Social Adjustment Scale: A simple measure of impairment in functioning. British Journal of Psychiatry, 180, 461–464. 10.1192/bjp.180.5.461 [DOI] [PubMed] [Google Scholar]
- Muthén, L. K. , & Muthén, B. O. (1998. –2017). Mplus user's guide (8th ed.). Muthén & Muthén. [Google Scholar]
- Naim, R. , Abend, R. , Wald, I. , Eldar, S. , Levi, O. , Fruchter, E. , Ginat, K. , Halpern, P. , Sipos, M. L. , & Adler, A. B. (2015). Threat‐related attention bias variability and posttraumatic stress. American Journal of Psychiatry, 172(12), 1242–1250. 10.1176/appi.ajp.2015.14121579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin, D. B. (1987). Multiple imputation for nonresponse in surveys. Wiley. [Google Scholar]
- Schoorl, M. , Putman, P. , Van Der Werff, S. , & Van Der Does, A. W. (2014). Attentional bias and attentional control in posttraumatic stress disorder. Journal of Anxiety Disorders, 28(2), 203–210. 10.1016/j.janxdis.2013.10.001 [DOI] [PubMed] [Google Scholar]
- Sipos, M. L. , Bar‐Haim, Y. , Abend, R. , Adler, A. B. , & Bliese, P. D. (2014). Postdeployment threat‐related attention bias interacts with combat exposure to account for PTSD and anxiety symptoms in soldiers. Depression and Anxiety, 31(2), 124–129. 10.1002/da.22157 [DOI] [PubMed] [Google Scholar]
- Van Hooff, M. , Lawrence‐Wood, E. , Hodson, S. , Sadler, N. , Benassi, H. , Hansen, C. , & McFarlane, A. (2018). Mental health prevalence, mental health and wellbeing transition study. Canberra The Department of Defence and the Department of Veterans Affairs. https://www.dva.gov.au/sites/default/files/twrp_mhpr.pdf [Google Scholar]
- Wald, I. , Fruchter, E. , Ginat, K. , Stolin, E. , Dagan, D. , Bliese, P. , Quartana, P. , Sipos, M. , Pine, D. , & Bar‐Haim, Y. (2016). Selective prevention of combat‐related post‐traumatic stress disorder using attention bias modification training: A randomized controlled trial. Psychological medicine, 46(12), 2627–2636. 10.1017/S0033291716000945 [DOI] [PubMed] [Google Scholar]
- Wald, I. , Shechner, T. , Bitton, S. , Holoshitz, Y. , Charney, D. , Muller, D. , Fox, N. , Pine, D. , & Bar‐Haim, Y. (2011). Attention bias away from threat during life‐threatening danger predicts PTSD symptoms at 1‐year follow‐up. Depression and Anxiety, 28(5), 406–411. 10.1002/da.20808 [DOI] [PubMed] [Google Scholar]
- Weathers, F. W. , Litz, B. T. , Keane, T. M. , Palmieri, P. A. , Marx, B. P. , & Schnurr, P. P. (2013). The PTSD Checklist for DSM‐5 (PCL‐5) . Scale available from the National Center for PTSD at https://www.ptsd.va.gov/professional/assessment/adult‐sr/ptsd‐checklist.asp
- Zhang, Y. , Kong, F. , Han, L. , ul Hasan, A. N. , & Chen, H. (2014). Attention bias in earthquake‐exposed survivors: An event‐related potential study. International Journal of Psychophysiology, 94(3), 358–364. 10.1016/j.ijpsycho.2014.09.004 [DOI] [PubMed] [Google Scholar]