

Abstract
Rationale:
The 2016 U.S. presidential election and its aftermath involved political rhetoric and policies that especially targeted women, Latinos, and immigrants. It is possible that concerns about the political environment could affect mental health of individuals in targeted groups.
Objective:
In a cohort of 148 pregnant Latina women, this study investigated how demographics and political concerns related to each other and to maternal anxiety, depression, and perceived stress, which have been associated with adverse birth and child development outcomes.
Methods:
In this cross-sectional, self-report study, participants in Southern California completed a one-time questionnaire from January 2017 to May 2018.
Results:
The highest rates of endorsement were for concerns regarding President Trump’s racism, attitude towards women, and deportation risk for family or friends. From several demographic variables, the only significant predictor of state anxiety was expectant parents’ birthplaces. From several political concerns variables, the only significant predictor of state anxiety was President Trump’s attitude towards women or women’s rights. There were no significant effects on other mental health outcomes.
Conclusions:
Results suggest that birthplace and women’s issues may be particularly salient anxiety risk factors for Latina pregnant women in this context. Because of the cross-sectional study design, it is possible that, conversely, pregnant women with high anxiety levels are particularly sensitive to the issue of birthplace or women’s rights. Results imply that the political climate and events in the U.S. could have deleterious consequences that may cascade across generations of Latino Americans via effects on pregnant women.
Keywords: Minority health disparities, Intergenerational health, Prenatal anxiety, Maternal mental health, Political climate, 2016 election, Latina
1. Introduction
Health disparities exist in a political landscape whose changing contours alter health dynamics among the population. Accumulating evidence suggests that the 2016 U.S. presidential election (henceforth “election”) and its sociopolitical aftermath may represent a negative influence on Latino-American health and well-being (Gemmill et al., 2019; Morey, 2018). Henceforth, the term “Latino/a” is used because these were reported as the preferred terms among this cohort. The election may have been particularly consequential for individuals in demographic groups targeted by the rhetoric and policies of President Trump and his administration, such as women, Latinos, and immigrants. This study addresses these issues by investigating how demographic factors and political concerns relate to mental health among a cohort of Latina, pregnant women in Southern California. This area of study has important public health implications because a threatening political environment may exacerbate health disparities between Latinos and other ethnicities in the U.S (Morey, 2018). In this article, I argue for the particular value of focusing on pregnancy because of the importance of well-being during this life phase both for women’s mental health and health across generations.
Pregnancy represents a period of especially elevated mental health risk for women compared to other life phases, with a high rate of onset of mood disorders (Rayburn, 2018). Psychological distress and mood disorders during pregnancy can have long-term repercussions for maternal and child health (DiPietro et al., 2006; Rayburn, 2018; Schetter and Glynn, 2011). In the U.S., prenatal depression and anxiety afflict an estimated 12–27% and 9–22% of pregnant women, respectively (Ponting et al., 2020b). Latina women exhibit a higher prevalence of mood disorders than non-Latina pregnant women, e.g., depression prevalence as high as 50–61% (Lucero et al., 2012) and anxiety 20–36% (Lara-Cinisomo et al., 2019), underscoring the importance of investigating predictors of prenatal affect in this population.
Demographic factors have been implicated in mental health in perinatal Latinas. Previous studies with pregnant and postpartum Latinas found that mood disorders, such as depression or anxiety, were associated with demographic factors including low socioeconomic status (Rich-Edwards et al., 2006), food insecurity (Hromi-Fiedler et al., 2011), and U.S.-born or foreign-born status (Huang et al., 2007).
Most scholarship on the effects of the U.S. political climate on Latino health has focused on immigration and deportation policy, which have been associated with emotional distress (Lopez et al., 2017) and worry about deportation (Valdez et al., 2013), particularly among foreign-born Latinos (Hacker et al., 2012; Lopez et al., 2017). Anti-immigrant policies and political climate can affect all Latinos due to personal ties with undocumented, foreign-born, and deported individuals (Dominguez Villegas and Rietig, 2015; Vargas and Benitez, 2019), and also due to hostile attitudes conflating undocumented, immigrant, and all Latinos (Gemmill et al., 2019).
A small number of recent studies have investigated the relationships between political stressors and adverse birth outcomes among Latinas using large-scale databases. These studies demonstrate that recent U.S. political events may have enhanced rates of adverse birth outcomes for Latina mothers, although these studies cannot address mechanisms or individual experiences. Studies observed disproportionate adverse birth outcomes for Latina women after the election (Gemmill et al., 2019; Krieger et al., 2018), after an immigration raid (Novak et al., 2017), and the passage of a restrictive immigration law (Torche and Sirois, 2018). Also, various studies reported associations between non-political socio-cultural stress and prenatal mental health among pregnant Latinas (Campos et al., 2007; D’Anna-Hernandez et al., 2015; Davila et al., 2009), underscoring the broader phenomenon that socio-cultural stressors, of which political stressors are one type, can influence mental health among pregnant Latinas.
An individual’s appraisal of events and environments moderates how these influence mood (Folkman et al., 1986), which is relevant here because rather than assuming that the election would have a similar effect on mental health among all members of a targeted demographic group, individual appraisals of the election might explain effects. Crucially, pregnancy alters how women appraise events (Glynn et al., 2004). Therefore, in order to understand how the election could relate to mental health outcomes among pregnant women, it is necessary to examine this issue using self-report in a cohort of pregnant women.
Here, I assess how demographic factors and political concerns predict psychological distress in a Latina, pregnant cohort from January 2017 to May 2018. The analytic plan is designed to address the hypotheses that demographic factors and political concerns cause psychological distress in this population. However, this cross-sectional study design does not permit the testing of causality, so it is only possible to assess whether these data are consistent with the possibility of the hypotheses being supported. Demographic factors inherently reflect events prior to political concerns about the Trump administration. This study is motivated by the possibility that demographic factors may influence political concerns in a way that, then, influences mental health, but future longitudinal studies will be necessary to establish this chain of causality. I emphasize the correlational nature of these analyses.
2. Methods
2.1. Cohort and protocol
The cohort for this project derives from Wave 1 of the Mothers’ Cultural Experiences (MCE) study. MCE Wave 1 involved a one-time, anonymous survey administered in person by study staff. Potential participants were approached in clinic waiting rooms or at prenatal classes. To be eligible, women were aged at least 18-years old, English or Spanish speaking, pregnant or recently postpartum, and self-identified as Latina, Hispanic, Chicana, Mexicana, and/or Latin American. Written, informed consent was obtained after full study procedures were described. This study was approved by the Institutional Review Boards of all participating institutions with appropriate reliances. The study adheres to the tenets of the Declaration of Helsinki.
MCE’s Wave 1 included 361 women, and this study considers only the subset administered the political concerns questionnaire (n = 186 participants from January 25, 2017, to May 10, 2018).
2.2. Variables
Anxiety was assessed with the State form of the State-Trait Anxiety Inventory (STAI) (Spielberger, 1983), using the 6-item version developed as appropriate for pregnant women (Theresa M Marteau and Bekker, 1992b), validated (Tluczek et al., 2009), and used with other prenatal populations (Lo et al., 2019). Depression was assessed with the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987) validated among Latina pregnant women (Santos et al., 2007). See supplement for details of how the clinically significant thresholds for anxiety and depression were determined. The Perceived Stress Scale (PSS) (Cohen et al., 1983) 4-item version, validated among pregnant women (Karam et al., 2012), and the Pregnancy-Related Anxiety Scale (PRA) (Wadhwa et al., 1993) implemented in several studies among Latinas (Campos et al., 2007; Fleuriet and Sunil, 2014) were also administered. Cronbach’s alphas were STAI α = 0.81 (English α = 0.82; Spanish α = 0.79) EPDS α = 0.83 (English α = 0.85; Spanish α = 0.83), PSS α = 0.47 (English α = 0.54; Spanish α = 0.28), PRA α = 0.86 (English α = 0.73; Spanish α = 0.72).
Place of birth is an important demographic factor linked to mental health (Falah-Hassani et al., 2015). I incorporated both the proband (expectant mother) and the expectant father’s birthplace status into one summary variable to reflect whether 1 = neither, 2 = one, or 3 = both expectant parents were U.S.-born. See supplement for details. For models that included the expectant parents’ birthplaces variable, a supplementary set of models were fitted using three alternative codings or conceptions of this construct: expectant parents’ places of birth coded as four categories reflecting all combinations of mother/father U. S./foreign-born; maternal birthplace; maternal percent of life spent in the U.S. (Tables S1–3). The purpose of the supplementary models was to, post-hoc, confirm that thee findings were not a spurious result of the way the variable was coded or conceived.
Political concerns were measured with an original set of questions prefaced with the instructions “These questions are about your feelings and opinions. There are no right or wrong answers,” then the prompt “With Trump’s election as president of the US, I am concerned about,” then “Choose all that apply.” There were 8 statements, each with a checkbox, and 4 open slots marked “other.” The research team identified “other” responses that overlapped with the given response choices and re-coded participants’ answers as though they had checked that response. For example, it was decided that “Deportation of family members” and “my family being deported/affected” counted as an endorsement of “The risk that members of my family or friends will be deported.” Additionally, I calculated the total number of political concerns endorsed by each participant, including unique responses to the “other” options.
To assess SES, a compilation variable was created based on participants’ educational attainment, food (in)security, and subjective socioeconomic status. Each component was coded with higher values reflecting higher SES, normalized by unitization with zero minimum, and averaged. Household income data were deemed too unreliable to include in the SES composite variable.
2.3. Statistical methods
A series of Fisher’s Exact Tests explored if expectant parents’ birthplaces significantly predicted participant political concerns, in order to understand the relationships between all constructs of interest in these analyses.
Four multiple linear regressions explored how participants’ demographics related to each of the mental health outcomes. The predictors of interest in the models were variables reflecting demographic factors: expectant parents’ birthplaces, proband’s relationship status, SES, and age. The predictors serving as covariates (controls) in the model were parity, trimester, and the other mental health variables to distinguish the effects of each mental health outcome from each other. When necessary, variables were transformed to improve the symmetry of distributions.
How participants’ responses to each of the political concerns binary choices related to mental health was assessed in three ways. First, a series of independent sample two-sided t-tests measured the relationship between each of the political concerns and each of the mental health outcomes. Second, a series of multiple linear regressions measured the conditional relationship of each of the political concerns with mental health outcomes after controlling for expectant parents’ places of birth, relationship status, SES, age, parity, trimester, and the other mental health variables. Third, a series of multiple linear regressions examined how the number of political concerns related to each mental health outcome after controlling for the same list of covariates as above. All analyses were corrected for multiple testing using Bonferroni adjustment.
While a dimensional operationalization of mental health outcomes affords the most detailed understanding of the relationship between predictors and outcomes, it is also beneficial to examine whether predictors relate to clinically significant symptoms to appreciate medical and public health implications. Therefore, if depression or state-anxiety scores would be significantly associated with demographic factors or political concerns, a follow-up χ2 test measured the association between the item and clinically significant depression or state anxiety (the other mental health instruments do not have clinically significant cutoff thresholds). Clinically significant cutoff thresholds are described in the Supplemental Materials.
Multicollinearity was assessed using Breusch-Pagan tests of homoskedasticity, variance-inflation factors, and tolerance (Allison, 1999).
Data analysis was conducted using the R statistical programming language and environment. This study was pre-registered in Open Science Framework DOI 10.17605/OSF.IO/74CJV.
3. Results
3.1. Cohort descriptives
The political concerns questionnaire was administered to 186 participants. Before statistical analysis, seven of these were excluded based on the lack of eligibility determined by survey responses. Because only six women were postnatal, they were excluded and analyses focus exclusively on pregnant participants. Another 25 were omitted due to missingness for variables reflecting political concerns, mental health, or pregnancy information. For the 11 women who were excluded for missing political concerns data, I cannot rule out the possibility that missingness was non-random. Thus, statistical analyses were conducted with data from a total of 148 participants. For consistency in sample size, all information henceforth is presented for this dataset (Table 1).
Table 1.
Cohort demographics and mental health measures.
| n | 148 |
|---|---|
|
| |
| Recruitment site (%) | |
| MOMS Orange County | 53 (35.8) |
| Olive View-UCLA Medical Center | 67 (45.3) |
| Westside Family Health Center | 28 (18.9) |
| Age in years (mean (SD)) | 29.45 (6.21) |
| Country of birth (%) | |
| U.S. | 69 (46.6) |
| Mexico | 62 (41.9) |
| El Salvador | 7 (4.7) |
| Guatemala | 5 (3.4) |
| Another country | 5 (3.4) |
| Age moved to US, foreign-born subset (Years) (mean (SD)) | 16.61 (9.49) |
| Mexican heritage or origin (%) | |
| Yes | 118 (79.7) |
| No | 19 (12.8) |
| NA | 11 (7.4) |
| Anxiety score (1–4) (mean (SD)) | 1.65 (0.53) |
| Clinically significant anxiety symptoms = Yes (%) | 46 (31.1) |
| Depression score (0–30) (mean (SD)) | 5.38 (4.07) |
| Clinically significant depression symptoms = Yes (%) | 24 (16.2) |
| Pregnancy related anxiety score (1–4) (mean (SD)) | 1.83 (0.52) |
| Perceived stress score (0–16) (mean (SD)) | 5.08 (2.61) |
| Education (%) | |
| Elementary or incomplete secondary | 14 (9.5) |
| High school or GED | 66 (44.6) |
| Technical or vocational program | 24 (16.2) |
| Associate degree | 7 (4.7) |
| Bachelors or higher | 27 (18.2) |
| Other | 7 (4.7) |
| NA | 3 (2.0) |
| Food insecure (%) | |
| Yes | 56 (37.8) |
| No | 79 (53.4) |
| NA | 13 (8.8) |
| Household currently receiving Food Stamps/CalFresh/SNAP benefits (%) | |
| Yes | 30 (20.3) |
| No | 112 (75.7) |
| NA | 6 (4.1) |
| Household currently receiving WIC benefits (%) | |
| Yes | 77 (52.0) |
| No | 65 (43.9) |
| NA | 6 (4.1) |
| Subjective SES (1–10) (mean (SD)) | 5.70 (1.89) |
| Trimester (%) | |
| 1 | 11 (7.4) |
| 2 | 33 (22.3) |
| 3 | 104 (70.3) |
| Parity (%) | |
| 0 | 55 (37.2) |
| 1 | 39 (26.4) |
| 2 | 32 (21.6) |
| 3 | 11 (7.4) |
| 4 | 6 (4.1) |
| 5 | 1 (0.7) |
| 6 | 4 (2.7) |
| In a romantic relationship = Yes (%) | 134 (90.5) |
| Marital status (%) | |
| Married | 71 (48.0) |
| Never married | 60 (40.5) |
| Separated | 9 (6.1) |
| Divorced | 7 (4.7) |
| NA | 1 (0.7) |
| Language of questionnaire administration = Spanish (%) | 61 (41.2) |
| Baby’s father’s country of birth (%) | |
| U.S. | 54 (36.5) |
| Mexico | 65 (43.9) |
| Other Latin American countries 29 (19.6) | |
| Both parents’ countries of birth (%) | |
| Both foreign-born | 64 (43.2) |
| Father U.S.-born, mother foreign-born | 15 (10.1) |
| Mother U.S.-born, father foreign-born | 30 (20.3) |
| Both U.S.-born | 39 (26.4) |
| I speak Spanish ... (%) | |
| Extremely often or almost always | 82 (55.4) |
| Much or very often | 35 (23.6) |
| Moderately | 13 (8.8) |
| Very little or not very often | 8 (5.4) |
| Not at all | 3 (2.0) |
| NA | 7 (4.7) |
3.2. Political concerns
Participant responses to the political concerns items are displayed in Fig. 1. Twenty-four participants wrote “other” responses. New categories were created to reflect concerns described in the open-ended section that did not overlap with pre-written choices and were repeated by > 2 participants (Table 2).
Fig. 1.
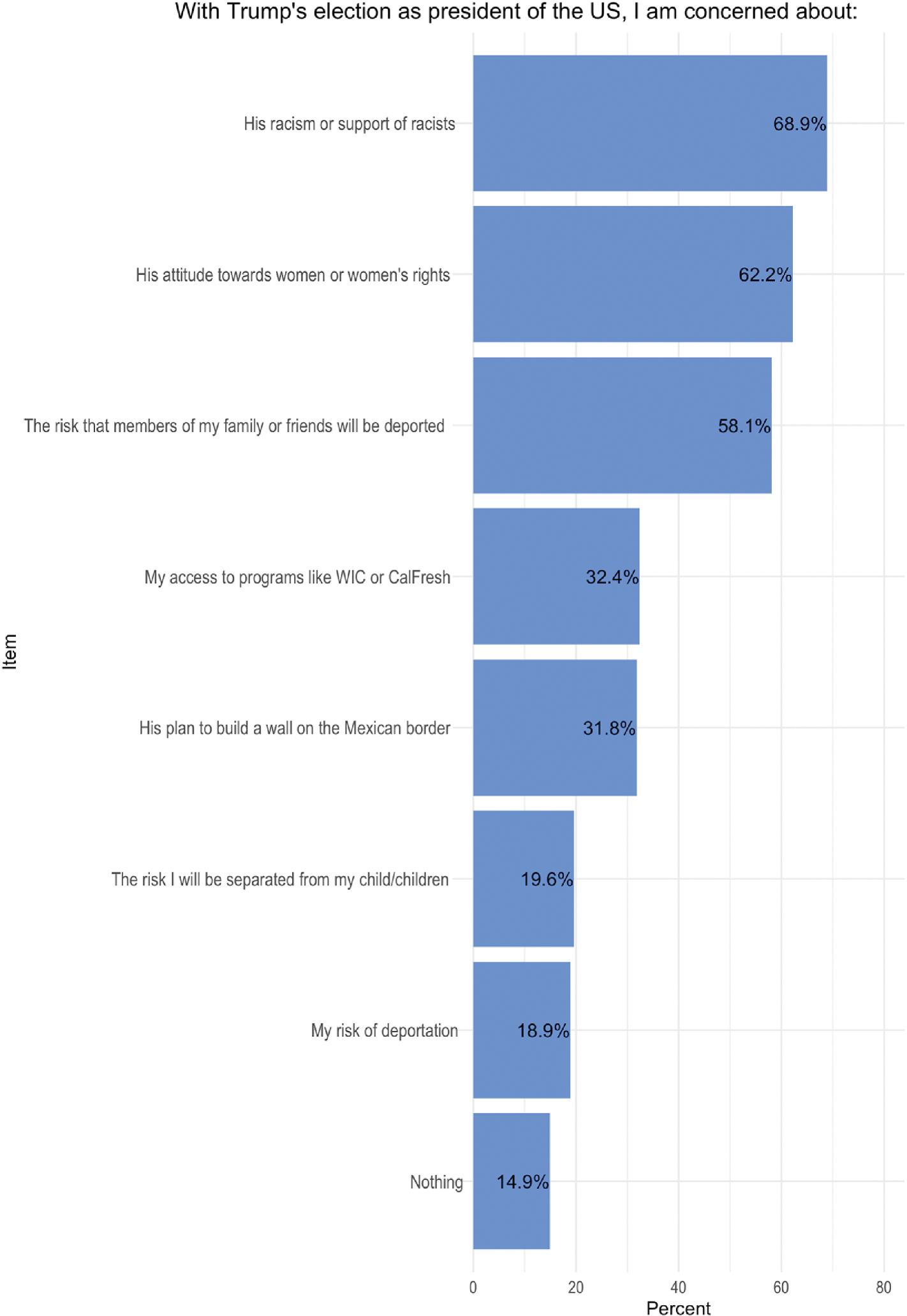
Percentages of participants who endorsed each answer choice. Note. Choices were presented as checkboxes. Instructions read “These questions are about your feelings and opinions. There are no right or wrong answers,” followed by the prompt, then, “Choose all that apply.”
Table 2.
Write-in responses to political concerns prompt.
| Category | Number of participants | Two examples of write-in responses |
|---|---|---|
|
| ||
| Environmental | 3 | His lack of importance towards the environment. Impact (negative) on the environment! |
| Discrimination (besides racism) | 5 | His attitude towards people of low-income. Bigot. |
| Foreign policy | 5 | Foreign policy in general. North Korea. |
| Fitness | 7 | He is unfit mentally to run a country. He is a child. |
| Other | 8 | How it will affect our economy. Guns in schools. |
Results suggest that concerns about President Trump’s attitude towards women or women’s rights and access to public assistance programs were significantly lower when both expectant parents were foreign-born compared to when one or both parents were U.S. born (Fig. 2). Concerns about deportation were significantly higher when both expectant parents were foreign-born compared to both U.S.-born. Concerns about the risk of being separated from one’s children were significantly higher when both expectant parents were foreign-born compared to when one or both parents were U.S.-born (Fig. 2).
Fig. 2.
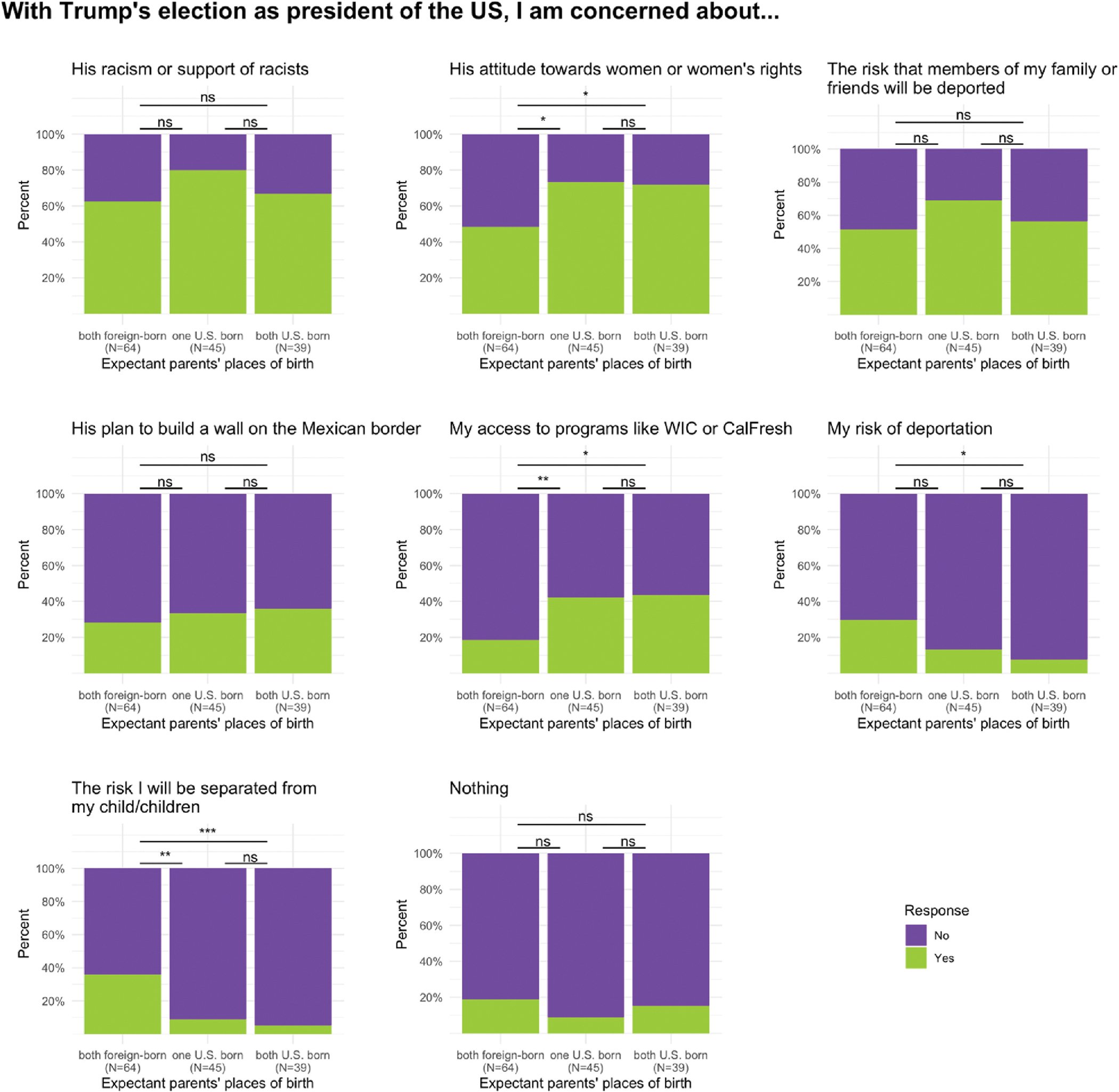
Variation in responses to the question of the political concern based on expectant parents’ places of birth. Note. *p < 0.05, **p < 0.01, ***p < 0.001, ns: not significant, Significance levels reflect Fisher’s Exact Test p-values.
3.3. Predictors of prenatal mental health
The only detected significant association between demographic predictors of interest and mental health outcomes was expectant parents’ birthplaces related to state anxiety, such that expectant parents being U.S.-born was associated with greater anxiety (β = 0.06, p = 0.044) (Table 3). Post-hoc, this model was repeated using alternative codings of birthplace yielding similar results (Tables S1–3). Expectant parents’ places of birth was not significantly associated with anxiety scores above the clinically meaningful threshold (Likelihood ratio χ2 = 0.678, p = 0.713; Pearson χ2 = 0.683, p = 0.711). Note that the short form of the state anxiety instrument is more accurate for classifying non-anxious individuals correctly than anxious individuals and may under-report clinically significant anxiety prevalence (Kruyen et al., 2013).
Table 3.
Multiple linear regression for demographic predictors of mental health.
| State anxiety | Depression | Perceived Stress | Pregnancy-related anxiety | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||||||
| β | Std. Error | p-value | β | Std. Error | p-value | β | Std. Error | p-value | β | Std. Error | p-value | |
|
| ||||||||||||
| (Intercept) | −0.328 | 0.345 | 0.344 | 1.123 | 0.382 | 0.004 ** | −0.601 | 2.831 | 0.832 | 0.41 | 0.306 | 0.182 |
| Expectant parents’ birth places | 0.062 | 0.03 | 0.044 * | 0.034 | 0.035 | 0.336 | −0.173 | 0.251 | 0.493 | −0.016 | 0.027 | 0.551 |
| Relationship status | −0.001 | 0.093 | 0.993 | −0.05 | 0.106 | 0.642 | −0.86 | 0.757 | 0.258 | 0.021 | 0.083 | 0.803 |
| Socio-economic status | 0.027 | 0.042 | 0.517 | −0.043 | 0.047 | 0.363 | −0.225 | 0.34 | 0.51 | −0.023 | 0.037 | 0.529 |
| Age (sqrt transformed) | 0.017 | 0.049 | 0.735 | 0.03 | 0.056 | 0.586 | 0.036 | 0.399 | 0.928 | −0.026 | 0.043 | 0.544 |
| Parity | 0.015 | 0.02 | 0.45 | −0.006 | 0.023 | 0.798 | −0.061 | 0.162 | 0.707 | 0.022 | 0.018 | 0.222 |
| Trimester | −0.059 | 0.039 | 0.136 | −0.005 | 0.045 | 0.914 | 0.44 | 0.32 | 0.172 | −0.056 | 0.035 | 0.112 |
| State anxiety (log transformed) | • | • | • | 0.348 | 0.101 | 0.001 ** | 1.363 | 0.749 | 0.071 | 0.133 | 0.082 | 0.107 |
| Depression (cube root transformed) | 0.265 | 0.077 | 0.001 ** | • | • | • | 2.431 | 0.624 | <0.0001 **** | 0.174 | 0.07 | 0.015 * |
| Perceived stress | 0.02 | 0.011 | 0.071 | 0.048 | 0.012 | <0.0001 **** | • | • | • | 0.02 | 0.01 | 0.048 * |
| Pregnancy-related anxiety (log transformed) | 0.167 | 0.103 | 0.107 | 0.289 | 0.116 | 0.015 * | 1.68 | 0.839 | 0.048 * | • | • | • |
Note.
p < 0.05
p < 0.01
p < 0.001.
Mental health outcome variables were transformed to improve symmetry of distributions as depression (EPDS score) cube root of score plus constant transformed, state anxiety (STAI score) and pregnancy-related anxiety (PRA score) natural log transformed, and perceived stress (PSS) no transformation. Bonferroni adjustment was implemented to account for the four models. Overall model fitting statistics: State anxiety: R2 = 0.35, F(9,116) = 7, p < 0.0001 ****, Bonferroni p-value=<0.0001 ****, Depression: R2 = 0.43, F(9,116) = 9.75, p < 0.0001 ****, Bonferroni p-value=<0.0001 ****, Perceived stress: R2 = 0.34, F(9,116) = 6.68, p < 0.0001 ****, Bonferroni p-value=<0.0001 ****, Pregnancy-related anxiety: R2 = 0.29, F(9,116) = 5.15, p < 0.0001 ****, Bonferroni p-value=<0.0001 ****.
The only political concern that exhibited a significant relationship with a mental health outcome was President Trump’s “attitude towards women or women’s rights” related to state anxiety (t(109.04) = −3.32, p = 0.008; β = 0.15, p = 0.004) (Fig. 3; Table 4; Table S4). Endorsing concern over President Trump’s attitude towards women or women’s rights was associated with anxiety scores above the clinically meaningful threshold (p = 0.048, Fig. 4). There were no other observations of political concerns with significant relationships with mental health outcomes (Tables S5–7). The number of political concerns was not significantly related to any of the mental health outcomes (Table S8). For all regression models, there were no indications of multicollinearity, as Breusch-Pagan tests rejected null hypotheses of homoskedasticity (p > 0.05), variance-inflation factors (VIF) reflected no high degrees of multi-collinearity (VIF<2), and the minimum tolerance for any variable in each model was >0.4 (Table S9).
Fig. 3.
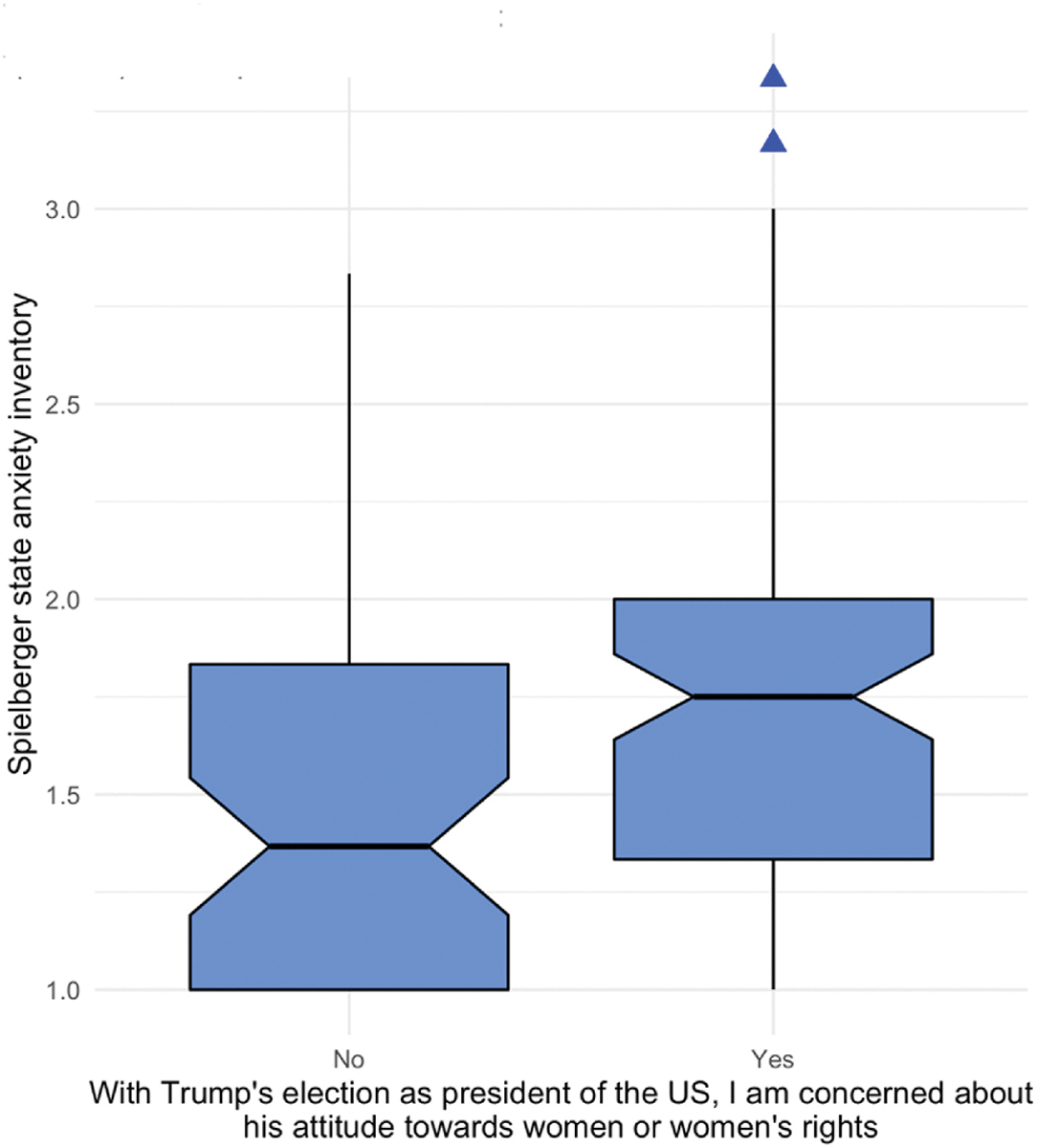
Relationship between concerns about women’s issues and state anxiety with Welch’s 2-sample 2-sided t-test results. Note. Welch’s two sample t-test 2- sided: t(109.04) = − 3.32, p = 0.001**. Upper hinge reflects the 75th percentile. Lower hinge reflects the 25th percentile. Upper whisker reflects the largest observation no further than the upper hinge +1.5 * interquartile range (IQR, i. e., distance between first and third quartiles). Lower whisker reflects the smallest observation no further than the lower hinge − 1.5 * IQR. Blue triangles reflect observations outside of this range. The notches are useful for group comparison. Because the notches of the two boxes do not overlap, “this suggests that the medians are significantly different.” (Source: https://github.com/tidyverse/ggplot2/blob/master/R/geom-boxplot.r) Upper edge of notch reflects median − 1.58 * IQR/sqrt(n). Lower edge of notch reflects median − 1.58 * IQR/sqrt(n). This approximates a 95% confidence interval for comparing medians (McGill et al., 1978).
Table 4.
Political concerns as predictors of prenatal anxiety.
| Variable | Two-sided t-tests |
Multiple linear regressions |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| t | df | p | Bonferroni p | β | P | Model R2 | Model p | Model p, Bonferroni | |
|
| |||||||||
| His racism or support of racists | −1.74 | 78.81 | 0.086 | 1 | 0.08 | 0.146 | 0.36 | <0.0001 **** | <0.0001 **** |
| His attitude towards women or women’s rights | −3.32 | 109.04 | 0.001 ** | 0.032 * | 0.15 | 0.004 ** | 0.40 | <0.0001 **** | <0.0001 **** |
| The risk that members of my family or friends will be deported | −1.63 | 126.70 | 0.105 | 1 | 0.03 | 0.557 | 0.35 | <0.0001 **** | <0.0001 **** |
| His plan to build a wall on the Mexican border | −1.26 | 88.75 | 0.211 | 1 | 0.06 | 0.285 | 0.36 | <0.0001 **** | <0.0001 **** |
| My access to programs like WIC or CalFresh | −0.78 | 95.74 | 0.438 | 1 | −0.05 | 0.318 | 0.36 | <0.0001 **** | <0.0001 **** |
| My risk of deportation | −1.21 | 39.40 | 0.235 | 1 | 0.09 | 0.128 | 0.37 | <0.0001 **** | <0.0001 **** |
| The risk I will be separated from my child/children | −0.73 | 45.93 | 0.47 | 1 | 0.10 | 0.118 | 0.37 | <0.0001 **** | <0.0001 **** |
| Nothing | −1.70 | 28.69 | 0.101 | 1 | 0.11 | 0.128 | 0.37 | <0.0001 **** | <0.0001 **** |
Note. Each row reflects two models, each with the same primary predictor of interest. First set of columns: Independent samples two-sided t-tests. Bonferroni adjusted p-values indicate that President Trump’s “... attitude towards women or women’s rights” is the only political concern that emerged as a significant predictor of prenatal anxiety. Second set of columns: Multiple linear regressions, each with one political concerns predictor (in “Variable” column), all models controlling for expectant parents’ places of birth, relationship status, SES, age, parity, trimester, and the other mental health variables. Details of each of these multiple linear regression models are presented in Table S4. Bonferroni adjustments were implemented to account for 32 comparisons (8 political concerns × 4 mental health outcomes).
Fig. 4.
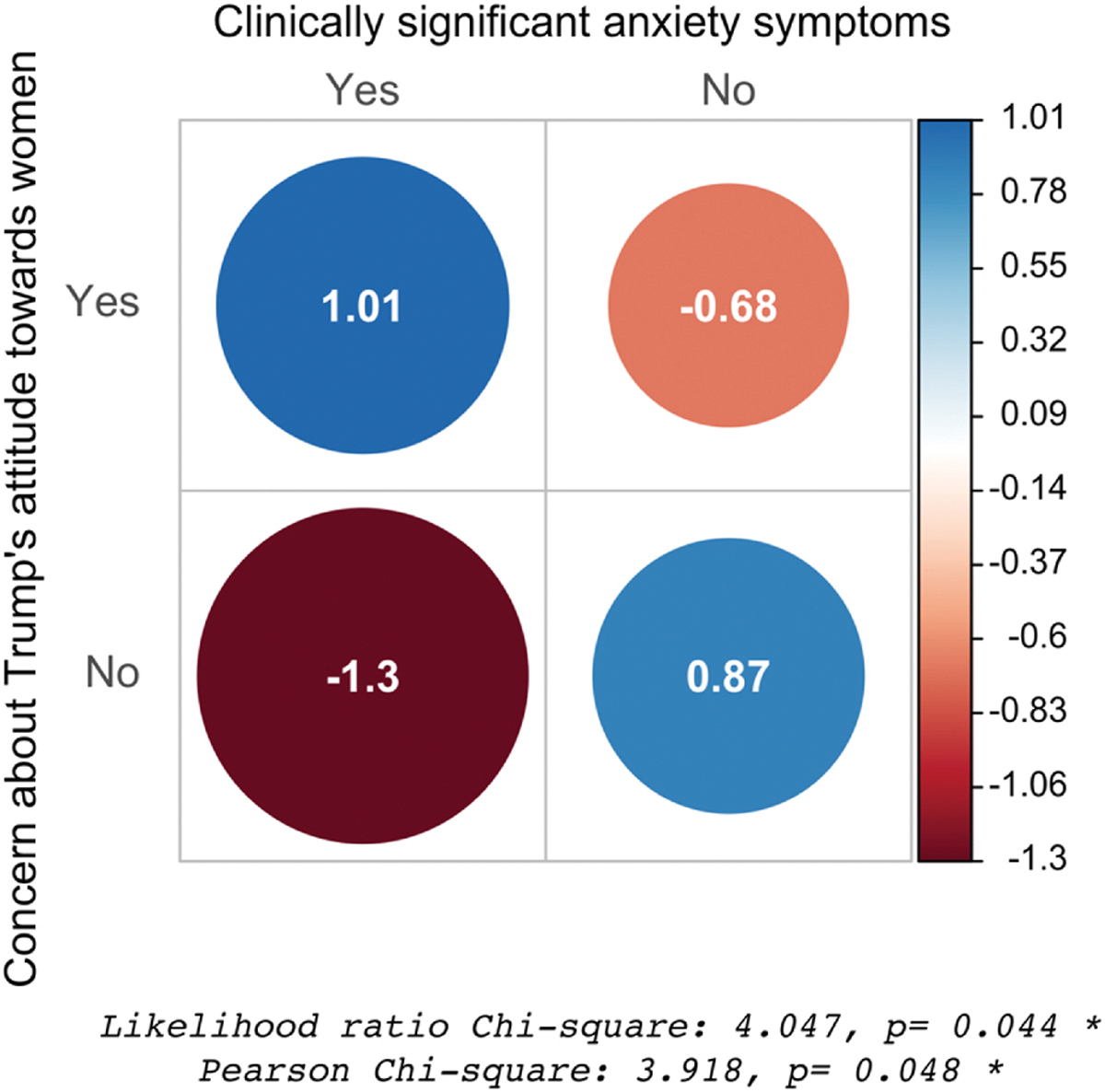
Relationship between concerns about women’s issues and clinically significant anxiety symptoms with χ2 test results. Note. This plot of the Pearson residuals indicates deviations from the null assumption that concerns about women’s issues have no biased associations with clinically significant anxiety symptoms; that is, visualization of the results of the χ2 test. Each cell in the contingency table is represented by a circle whose area is proportional to the absolute value of the correlation coefficient. Positive residuals are blue, indicating a positive association between the two variables. The strongest positive association is between endorsing concern about Trump’s attitude towards women and exhibiting clinically significant anxiety symptoms. Negative residuals are red, indicating a negative association between the two variables. The strongest negative association is between not endorsing concern about Trump’s attitude towards women and exhibiting clinically significant anxiety symptoms.
4. Discussion
From several potential demographic, pregnancy history, and political concerns predictors and mental health outcomes, only expectant parents’ birthplaces and concerns about President Trump’s attitude towards women or women’s rights emerged as significant predictors of state anxiety (Tables 3 and 4). I acknowledge an interpretation of the political concerns models with alternative causality to my hypothesis–having greater state anxiety levels makes women more attuned to women’s rights. This construal would be equally consistent with the study’s observations; a limitation of cross-sectional, observational research is that there is not the statistical ability to rule out this alternative. Regardless of the directionality of causality, an association of state anxiety with birthplaces and President Trump’s attitude towards women or women’s rights suggests these are salient issues among women who ultimately experience anxiety during pregnancy.
After back-transforming beta coefficients to account for natural log-transformed anxiety scores, results suggest that, after adjusting for the effects of covariates, both expectant parents being U.S.-born was associated with 0.10 points higher STAI score (which is on a 1–4 scale) than both foreign-born, equivalent to 2.0 prorated points higher on the full-length STAI (Farrell et al., 2020; Theresa M. Marteau and Bekker, 1992a). Endorsing concern about Trump’s attitude towards women was associated with 0.58 points higher STAI score, after adjusting for the effects of covariates, equivalent to 11.6 prorated points higher on the full-length STAI. To compare these effect sizes with other studies conducted with pregnant women, Gurung et al. found, prorated to the full-length STAI, that being married to the baby’s father was associated with 0.2 points lower and medical risk with 0.2 points higher scores, and for the Latina subset of the cohort, each unit increase of social support from the baby’s father (measured on a scale from 1 to 5) was associated with 0.3 points lower and each additional stressful life event with 0.6 points higher (Gurung et al., 2005); Roos et al. found each unit increase in social support (measured on a scale from 12 to 84) was associated with 0.4 (second trimester) and 0.3 (third trimester) points lower on the full-length STAI (Roos et al., 2013).
The results suggest that anxiety could have special relation to political stressors. Anxiety during pregnancy has particularly pernicious health consequences because it is strongly associated with adverse birth and child developmental outcomes, including preterm delivery, low birth weight (Schetter and Glynn, 2011), lower Apgar scores (Berle et al., 2005), mental developmental deficits at 8 months and 2 years (DiPietro et al., 2006), behavioral and emotional problems at 4 years (O’Connor et al., 2002), negative behavioral reactivity at 4 months (Davis et al., 2004), and problems with attention regulation and impulsivity at 3 and 8 months and 2.5, 4, 8, and 14 years (DiPietro et al., 2006). Gurung and colleagues observed that among Latina pregnant women, demographic factors and stressful life events (e.g., changes in where or with whom participants lived) predicted anxiety (Gurung et al., 2005). Life events predicted prenatal anxiety among the Latina and African American subsets only. Demographic factors were not predictive among the African American subset and only income was predictive among the White subset. Their results align with this study’s observation that demographic factors and sociopolitical events and conditions predict prenatal anxiety in a Latina cohort.
The expectant parents being foreign-born was associated with lower anxiety levels. This finding is consistent with the “Latino paradox” observation that foreign-born Latino Americans often exhibit superior mental health compared to U.S.-born peers (Cunningham et al., 2008; Ruiz et al., 2016). Similarly, foreign-born women typically exhibit better pregnancy outcomes than U.S.-born peers, such as lower rates of preterm birth (Cunningham et al., 2008; Flores et al., 2012). These patterns are sometimes, partly, attributable to a healthy migrant bias (Abraído-Lanza et al., 1999). Beyond that, the prevailing explanations for the foreign-born Latino health advantage are acculturative stress in the U. S.-born population, protective effects of Latino health behaviors such as nutritious diet, and traditional cultural values such as familismo (Abraído-Lanza et al., 2005; Fox et al., 2015; Lara et al., 2005; Teruya and Bazargan-Hejazi, 2013). However, this issue has only rarely been addressed in the context of prenatal mental health (Fox et al., 2015). Similar to this study’s results, Campos and colleagues found that foreign-born Latina women had lower anxiety levels than U.S.-born peers, although the differences were not statistically significant (Campos et al., 2008). This study expands this area of inquiry to consider the effects of birthplace not only of pregnant women but also of the fetus’s father.
The results suggest women’s issues may be particularly potent, compared to other political concerns, for predicting prenatal anxiety. I ponder whether there is something unique about the life phase of pregnancy that makes political threats towards women’s issues especially meaningful. Given the inherent physical, emotional, and financial vulnerabilities women experience during pregnancy, women may become more attuned to relevant threats during this phase. Anxiety may represent an adaptive state of heightened threat sensitivity (Stein and Nesse, 2011). One of the tenets of evolutionary theory is that traits are adaptive if they increase reproductive success, regardless of whether they promote health or well-being; hence, an unpleasant experience like anxiety could be adaptive if its manifestation ultimately improves an individual’s reproductive success. From an evolutionary perspective, it is plausible that biased attention towards pregnancy- or motherhood-specific threats could induce anxiety in a way that promotes precautionary behaviors that are ultimately adaptive (Hahn-Holbrook et al., 2011). Precautionary psychology and behaviors during pregnancy have been previously interpreted as adaptive mechanisms, such as mothers’ defensive aggression serving to protect against conspecific or predictor attacks (Gammie et al., 2008), and mothers’ anxiety about risks to children serving to prevent accidental harm (Leckman et al., 2004). Additionally, the results imply that political concerns may uniquely relate to state anxiety and not other mental health constructs. An evolutionary interpretation could suggest that stressors deriving from the political environment may require enhanced vigilance, therefore prompting an adaptive anxiety response (Petersen, 2015). Evolutionary political psychology is an emerging field of study, and further research is needed to apply evolutionary frameworks to the relationship between political environments and mental health in pregnancy.
Women’s issues may be particularly relevant to the Latina community compared to other groups due to cultural values such as marianismo, which encourages traditional gender roles for women, and familismo, which encourages the centrality of family in identity and behavior (Gamble et al., 2007). Relevant political events that I speculate could have contributed to participants’ concerns may have included the 23 accusations of the president’s sexual misconduct (Pearson et al., 2019), which contributed to the widespread outrage that led to the Women’s March, the largest single-day protest in U.S. history (Beckwith, 2018) 4 days before the survey started, which promoted Latina intersectional identity issues (Burns-Ardolino, 2019). Sexual violence and disrespectful rhetoric towards women conflict with marianismo and familismo values. However, these traditional values may be less relevant for more acculturated Latinas (Knight et al., 2010). Future studies should explore how these value systems interact with acculturation and political concerns among Latinas.
Participants’ endorsements of political concerns varied based on the expectant parents’ birthplaces (Fig. 2). As expected, foreign-born individuals had more concerns about deportation and family separation. It should be noted that the survey period ended merely 5 days after the Zero Tolerance/family separation policy was implemented, so the results do not reflect this policy. Unexpectedly, greater concern among expectant parents in which one or both were U.S.-born compared to both foreign-born regarding women’s issues and public benefits programs. One possibility could be that among participants for whom they or their fetus’ father are foreign-born, other concerns could overshadow. Further research would be needed to determine individuals’ ranked concerns and political priorities. Another possibility could be that foreign-born participants are less familiar with U.S. domestic policies regarding women’s rights and public benefits, or less aware of their own eligibility for public benefits. Women acclimatized to the President Obama era political environment may perceive present conditions to be more hostile (Gemmill et al., 2019). Interestingly, and in contrast to this study’s findings, not U.S.-born individuals but rather immigrants were threatened with losing access to public benefits or risk being denied green cards under a policy declared during Trump’s election campaign (before the survey period) and officially announced by the Trump administration in February 2018 (during the survey period) (Morey, 2018).
The experiences of foreign-born and U.S.-born individuals are highly variable depending on the circumstances and perceptions of their lives in each location. In some cases, some foreign-born individuals may perceive lower levels of racial discrimination despite being more often the target of discrimination compared to U.S.-born, for instance, if race is a less dominant social categorization or their ethnicity constituted the majority in their place of origin, due to less awareness of negative stereotypes Americans hold against their racial category (Brondolo et al., 2015), or due to discrimination for other social categories such as immigrant status overshadowing concerns about discrimination based on ethnicity. These possibilities are consistent with previous observations that U.S.-born Latinos reported higher levels of ethnic discrimination than foreign-born (Arellano-Morales et al., 2015). These ideas are opposite to this study’s observation of no significant differences, based on birthplaces, in concern over President Trump’s racism or support of racists. This concern had the highest endorsement of any concern for the overall cohort and for the cohort subsets with one and both foreign-born expectant parents. A possible, speculative explanation for why the findings differ from previous studies could be that even if some foreign-born individuals might not have been aware or concerned about racial discrimination in other moments of U.S. history (i.e., previous studies), they may be more aware of this element of President Trump’s rhetoric and agenda because it was especially prominent or more prominently discussed within the media or among foreign-born communities (i.e., this study). Other possible, speculative explanations for the discrepancy could be that racial discrimination levels in immigrants’ countries of origin have intensified since those previous studies were conducted, or, prejudices in different countries may influence each other, either way, diminishing differences certain immigrants encounter in discrimination in origin and host environments.
Relationships were not detected between demographic factors or political concerns and prenatal depression, perceived stress, or pregnancy-specific anxiety, nor were relationships detected between the total number of political concerns and mental health. The lack of observations adds to a growing, inconsistent landscape of findings in this area. Several previous studies have observed that foreign-born status was positively associated with postpartum depression among other national and ethnic groups (Falah-Hassani et al., 2015), although others found no association for Latinas in the U.S. (Lara-Cinisomo et al., 2016; Ponting et al., 2020a). Previous studies have not looked directly at political concerns, but other stressors have been associated with prenatal mental health, such as lack of social support associated with greater perceived stress and pregnancy-related anxiety in a pregnant cohort that was one-third Latina (Campos et al., 2008). Strahm et al. found, among pregnant Latinas, that social support was associated with lower pregnancy-related anxiety levels only among the foreign-born subset, with no effect observed for U.S.-born (Strahm et al., 2018).
4.1. Strengths and limitations
This study makes unique contributions. It directly measures individuals’ self-reported feelings and concerns related to the election and its sociopolitical aftermath, extending beyond previous studies’ methods of comparing data from large-scale databases. This study extends beyond previous studies’ focus on immigration to include multiple domains of potential political concerns. This study is the first to assess prenatal mental health in the context of political concerns related to the election and its aftermath. Also, the study is the first in this area to focus on a California cohort, which is important because California hosts 27% of the nation’s Latino population (Pew_Research_Center, 2016). California Latinos have been demonstrated to have greater concern for racial issues and higher levels of political knowledge than counterparts in another high Latino population state (Pantoja and Segura, 2003), and more recently, a study demonstrated that in Los Angeles, Latinos have the greatest level of political knowledge, attributed to having the largest Latino population of any U.S. city (DeSante and Perry, 2016). A greater concern for racial issues and higher levels of political knowledge could make this population more aware of political rhetoric and policies targeting their demographic group, and therefore more emotionally vulnerable to these factors. Additionally, data about fathers are included, which other studies in this area do not often include.
The results should be interpreted in light of certain limitations. Participant responses may have been influenced or limited by multiple-choice options designed based on the judgment of the research team only. A better method of survey design would have involved focus groups with members of the target community. The weaknesses of survey design methods were slightly offset by the inclusion of four blank “other” slots, of which n = 24 took advantage. This study is limited in using single items to assess each area of political concern. Future studies should use more comprehensive measures. Additionally, I am not able to address the extent to which participants were, in general, concerned about issues such as women’s rights, racism, deportation, or access to public benefits. Rather, this study’s data are limited by the specific question of whether participants were concerned about these issues only regarding the election of President Trump. Furthermore, political knowledge may play a moderating role, e.g., some participants may be unaware of President Trump’s rhetoric or policies related to some of these issues while others may follow politics more closely. This study did not ask about citizenship or (un)documented immigration status. This study’s cross-sectional data limits the ability to address questions related to participants’ changing political concerns over time, or birth and postnatal outcomes. Self-reports can be biased or inaccurate (Van de Mortel, 2008). The short forms of STAI and PSS lack the variance and depth of the full-length versions but have the advantage of maximizing compliance and minimizing error and fatigue (Theresa M Marteau and Bekker, 1992b; Spielberger, 1983; Tluczek et al., 2009). This study’s results related to perceived stress should be interpreted with caution because of the low Cronbach’s alphas for the PSS scale. This study only includes Latinas and mostly of Mexican heritage. It cannot be assumed that similar results would be observed for cohorts of Latinas with heritage from other Latin American countries or for other ethnic groups. Future research is needed in diverse Latina and multi-ethnic cohorts.
5. Conclusions and public health implications
In this cohort of Latina pregnant women in Southern California, the most frequently-endorsed political concerns regarding the Trump election were President Trump’s racism, attitudes towards women, and risk of family or friends’ deportation. The expectant parents’ places of birth were significantly associated with concerns about President Trump’s attitude towards women or women’s rights, access to public assistance programs, deportation, and the risk of being separated from one’s children, as well as state anxiety levels. Concerns about President Trump’s attitude towards women or women’s rights were positively associated with state anxiety. Public policies and political environments that disproportionately impact specific groups contribute to not only social disadvantage but also health disparities (Novak et al., 2017). The harmful effect of public policy on minority mental health has been demonstrated for various disadvantaged groups in the U.S. (Woolf and Braveman, 2011). Elucidating the relationship between socio-political conditions and prenatal mental health among Latinos may help forecast the public health burden of adverse birth outcomes in this group and other underserved communities. A better understanding of this relationship could also encourage targeting public resources toward mental health for pregnant women.
Supplementary Material
Acknowledgements
The author thanks the study participants and their families; she also thanks the students and volunteers of the Mothers’ Cultural Experiences Study, Kristine Chua, Delaney Knorr, Kotrina Kajokaite, the physicians, staff, and patients at the Westside Family Health Center, Olive View-UCLA Medical Center, and MOMS Orange County, as well as Michael Tzen and Kathy Maurer. This work was funded by the U.S. National Institute of Diabetes and Digestive and Kidney Diseases K01 DK105110–01 and 1R03DK125524–01 to M.F., and UCLA Center for the Study of Women Faculty Research Grant to M.F.
Footnotes
Declaration of competing interest
No potential conflict of interest was reported by the author.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.socscimed.2022.115171.
References
- Abraído-Lanza AF, Chao MT, Flórez KR, 2005. Do healthy behaviors decline with greater acculturation?: implications for the Latino mortality paradox. Soc. Sci. Med. 61, 1243–1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abraído-Lanza AF, Dohrenwend BP, Ng-Mak DS, Turner JB, 1999. The Latino mortality paradox: a test of the” salmon bias” and healthy migrant hypotheses. Am. J. Publ. Health 89, 1543–1548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allison PD, 1999. Multiple Regression: A Primer. Pine Forge Press. [Google Scholar]
- Arellano-Morales L, Roesch SC, Gallo LC, Emory KT, Molina KM, Gonzalez P, et al. , 2015. Prevalence and correlates of perceived ethnic discrimination in the hispanic community health study/study of Latinos sociocultural ancillary study. J. Latina/Psychol. 3, 160–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beckwith R, 2018. The Year in Trump: Memorable Moments from the President’s First Year in Office. Time Pp. New York, NY. https://time.com/5097411/donald-trump-first-year-office-timeline/. [Google Scholar]
- Berle J, Mykletun A, Daltveit AK, Rasmussen S, Holsten F, Dahl AA, 2005. Neonatal outcomes in offspring of women with anxiety and depression during pregnancy. Arch. Wom. Ment. Health 8, 181–189. [DOI] [PubMed] [Google Scholar]
- Brondolo E, Rahim R, Grimaldi S, Ashraf A, Bui N, Schwartz J, 2015. Place of birth effects on self-reported discrimination: variations by type of discrimination. Int. J. Intercult. Relat. : IJIR 49, 212–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns-Ardolino WA, 2019. Marching for change: intersectional coalition building, counter voices, and collective action at the US women’s March on Washington and beyond. J. Interdisciplin. Feminist Thought 11, 1–18. [Google Scholar]
- Campos B, Schetter CD, Abdou CM, Hobel CJ, Glynn LM, Sandman CA, 2008. Familialism, social support, and stress: positive implications for pregnant Latinas. Cult. Divers Ethnic Minor. Psychol. 14, 155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campos B, Schetter CD, Walsh JA, Schenker M, 2007. Sharpening the focus on acculturative change: ARSMA-II, stress, pregnancy anxiety, and infant birthweight in recently immigrated Latinas. Hisp. J. Behav. Sci. 29, 209–224. [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R, 1983. A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. [PubMed] [Google Scholar]
- Cox JL, Holden JM, Sagovsky R, 1987. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br. J. Psychiatr. 150, 782–786. [DOI] [PubMed] [Google Scholar]
- Cunningham SA, Ruben JD, Venkat Narayan KM, 2008. Health of foreign-born people in the United States: a review. Health Place 14, 623–635. [DOI] [PubMed] [Google Scholar]
- D’Anna-Hernandez KL, Aleman B, Flores A-M, 2015. Acculturative stress negatively impacts maternal depressive symptoms in Mexican-American women during pregnancy. J. Affect. Disord. 176, 35–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davila M, McFall SL, Cheng D, 2009. Acculturation and depressive symptoms among pregnant and postpartum Latinas. Matern. Child Health J. 13, 318–325. [DOI] [PubMed] [Google Scholar]
- Davis EP, Snidman N, Wadhwa PD, Glynn LM, Schetter CD, Sandman CA, 2004. Prenatal maternal anxiety and depression predict negative behavioral reactivity in infancy. Infancy 6, 319–331. [Google Scholar]
- DeSante CD, Perry BN, 2016. Bridging the gap: how geographic context affects political knowledge among citizen and non-citizen Latinos. Am. Polit. Res. 44, 548–577. [Google Scholar]
- DiPietro JA, Novak MFSX, Costigan KA, Atella LD, Reusing SP, 2006. Maternal psychological distress during pregnancy in relation to child development at age two. Child Dev. 77, 573–587. [DOI] [PubMed] [Google Scholar]
- Dominguez Villegas R, Rietig V, 2015. Migrants Deported from the United States and Mexico to the Northern Triangle: A Statistical and Socioeconomic Profile (Washington, DC). [Google Scholar]
- Falah-Hassani K, Shiri R, Vigod S, Dennis C-L, 2015. Prevalence of postpartum depression among immigrant women: a systematic review and meta-analysis. J. Psychiatr. Res. 70, 67–82. [DOI] [PubMed] [Google Scholar]
- Farrell MH, Kirschner ALP, Tluczek A, Farrell PM, 2020. Experience with parent follow-up for communication outcomes after newborn screening identifies carrier status. J. Pediatr. 224, 37–43 e32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleuriet KJ, Sunil TS, 2014. Perceived social stress, pregnancy-related anxiety, depression and subjective social status among pregnant Mexican and Mexican American women in south Texas. J. Health Care Poor Underserved 25, 546–561. [DOI] [PubMed] [Google Scholar]
- Flores ME, Simonsen SE, Manuck TA, Dyer JM, Turok DK, 2012. The “Latina epidemiologic paradox”: contrasting patterns of adverse birth outcomes in US-born and foreign-born Latinas. Wom. Health Issues 22, e501–e507. [DOI] [PubMed] [Google Scholar]
- Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongis A, Gruen RJ, 1986. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J. Pers. Soc. Psychol. 50, 992. [DOI] [PubMed] [Google Scholar]
- Fox M, Entringer S, Buss C, DeHaene J, Wadhwa PD, 2015. Intergenerational transmission of the effects of acculturation on health in Hispanic Americans: a fetal programming perspective. Am. J. Publ. Health 105, S409–S423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gamble WC, Ramakumar S, Diaz A, 2007. Maternal and paternal similarities and differences in parenting: an examination of Mexican-American parents of young children. Early Child. Res. Q. 22, 72–88. [Google Scholar]
- Gammie S, D’Anna K, Lee G, Stevenson S, 2008. Role of corticotropin releasing factor-related peptides in the neural regulation of maternal defense. Neurobiol. Parental Brain 103–114. [Google Scholar]
- Gemmill A, Catalano R, Casey JA, Karasek D, Alcalá HE, Elser H, et al. , 2019. Association of preterm births among US latina women with the 2016 presidential election. JAMA Netw. Open 2, e197084 e197084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glynn LM, Schetter CD, Wadhwa PD, Sandman CA, 2004. Pregnancy affects appraisal of negative life events. J. Psychosom. Res. 56, 47–52. [DOI] [PubMed] [Google Scholar]
- Gurung RA, Dunkel-Schetter C, Collins N, Rini C, Hobel CJ, 2005. Psychosocial predictors of prenatal anxiety. J. Soc. Clin. Psychol. 24, 497–519. [Google Scholar]
- Hacker K, Chu J, Arsenault L, Marlin RP, 2012. Provider’s perspectives on the impact of Immigration and Customs Enforcement (ICE) activity on immigrant health. J. Health Care Poor Underserved 23, 651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hahn-Holbrook J, Holbrook C, Haselton MG, 2011. Parental precaution: neurobiological means and adaptive ends. Neurosci. Biobehav. Rev. 35, 1052–1066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hromi-Fiedler A, Bermúdez-Millán A, Segura-Pérez S, Pérez-Escamilla R, 2011. Household food insecurity is associated with depressive symptoms among low-income pregnant Latinas. Matern. Child Nutr. 7, 421–430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang ZJ, Wong FY, Ronzio CR, Stella MY, 2007. Depressive symptomatology and mental health help-seeking patterns of US-and foreign-born mothers. Matern. Child Health J. 11, 257–267. [DOI] [PubMed] [Google Scholar]
- Karam F, Bérard A, Sheehy O, Huneau M-C, Briggs G, Chambers C, et al. , 2012. Reliability and validity of the 4-item perceived stress scale among pregnant women: results from the OTIS antidepressants study. Res. Nurs. Health 35, 363–375. [DOI] [PubMed] [Google Scholar]
- Knight GP, Gonzales NA, Saenz DS, Bonds DD, Germán M, Deardorff J, et al. , 2010. The Mexican American cultural values scales for adolescents and adults. J. Early Adolesc. 30, 444–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krieger N, Huynh M, Li W, Waterman PD, Van Wye G, 2018. Severe sociopolitical stressors and preterm births in New York City: 1 September 2015 to 31 August 2017. J. Epidemiol. Community Health 72, 1147–1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kruyen PM, Emons WHM, Sijtsma K, 2013. Shortening the S-STAI: consequences for research and clinical practice. J. Psychosom. Res. 75, 167–172. [DOI] [PubMed] [Google Scholar]
- Lara M, Gamboa C, Kahramanian MI, Morales LS, Hayes Bautista DE, 2005. Acculturation and Latino health in the United States: a review of the literature and its sociopolitical context. Annu. Rev. Publ. Health 26, 367–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lara-Cinisomo S, Fujimoto EM, Oksas C, Jian Y, Gharheeb A, 2019. Pilot study exploring migration experiences and perinatal depressive and anxiety symptoms in immigrant Latinas. Matern. Child Health J. 23, 1627–1647. [DOI] [PubMed] [Google Scholar]
- Lara-Cinisomo S, Girdler SS, Grewen K, Meltzer-Brody S, 2016. A biopsychosocial conceptual framework of postpartum depression risk in immigrant and U.S.-born latina mothers in the United States. Wom. Health Issues 26, 336–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leckman JF, Feldman R, Swain JE, Eicher V, Thompson N, Mayes L, 2004. Primary parental preoccupation: circuits, genes, and the crucial role of the environment. J. Neural. Transm. 111, 753–771. [DOI] [PubMed] [Google Scholar]
- Lo T-K, Chan KY-K, Kan AS-Y, So P-L, Kong C-W, Mak S-L, et al. , 2019. Decision outcomes in women offered noninvasive prenatal test (NIPT) for positive Down screening results. J. Matern. Fetal Neonatal Med. 32, 348–350. [DOI] [PubMed] [Google Scholar]
- Lopez WD, Kruger DJ, Delva J, Llanes M, Ledón C, Waller A, et al. , 2017. Health implications of an immigration raid: findings from a Latino community in the Midwestern United States. J. Immigr. Minority Health 19, 702–708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucero NB, Beckstrand RL, Callister LC, Sanchez Birkhead AC, 2012. Prevalence of postpartum depression among Hispanic immigrant women. J. Am. Acad. Nurse Pract. 24, 726–734. [DOI] [PubMed] [Google Scholar]
- Marteau TM, Bekker H, 1992a. The development of a six-item short-form of the state scale of the Spielberger State—trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 31, 301–306. [DOI] [PubMed] [Google Scholar]
- Marteau TM, Bekker H, 1992b. The development of a six-item short-form of the state scale of the Spielberger State—trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 31, 301–306. [DOI] [PubMed] [Google Scholar]
- McGill R, Tukey JW, Larsen WA, 1978. Variations of box plots. Am. Statistician 32, 12–16. [Google Scholar]
- Morey BN, 2018. Mechanisms by which anti-immigrant stigma exacerbates racial/ethnic health disparities. Am. J. Publ. Health 108, 460–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Novak NL, Geronimus AT, Martinez-Cardoso AM, 2017. Change in birth outcomes among infants born to Latina mothers after a major immigration raid. Int. J. Epidemiol. 46, 839–849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor TG, Heron J, Glover V, Team AS, 2002. Antenatal anxiety predicts child behavioral/emotional problems independently of postnatal depression. J. Am. Acad. Child Adolesc. Psychiatry 41, 1470–1477. [DOI] [PubMed] [Google Scholar]
- Pantoja AD, Segura GM, 2003. Fear and loathing in California: contextual threat and political sophistication among Latino voters. Polit. Behav. 25, 265–286. [Google Scholar]
- Pearson C, Gray E, Vagianos A, 2019. A Running List of the Women Who’ve Accused Donald Trump of Sexual Misconduct. HuffPost, New York, NY. [Google Scholar]
- Petersen MB, 2015. Evolutionary Political Psychology. Handbook of Evolutionary Psychology. [Google Scholar]
- Pew_Research_Center, 2016. Ranking the Latino Population in the States. Pew Research Hispanic Trends Project Pp. Pew Research Center, Washington, DC. https://www.pewresearch.org/hispanic/2016/2009/2008/2014-ranking-the-latino-population-in-the-states/. [Google Scholar]
- Ponting C, Chavira DA, Ramos I, Christensen W, Guardino C, Dunkel Schetter C, 2020a. Postpartum depressive symptoms in low-income Latinas: cultural and contextual contributors. Cult. Divers Ethnic Minor. Psychol. 26, 544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ponting C, Mahrer NE, Zelcer H, Dunkel Schetter C, Chavira DA, 2020b. Psychological interventions for depression and anxiety in pregnant Latina and Black women in the United States: a systematic review. Clin. Psychol. Psychother. 27, 249–265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rayburn WF, 2018. Pregnancy: an opportune time to evaluate and treat mental health disorders. Obstetr. Gynecol. Clinic. 45, xiii–xiv. [DOI] [PubMed] [Google Scholar]
- Rich-Edwards JW, Kleinman K, Abrams A, Harlow BL, McLaughlin TJ, Joffe H, et al. , 2006. Sociodemographic predictors of antenatal and postpartum depressive symptoms among women in a medical group practice. J. Epidemiol. Community Health 60, 221–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roos A, Faure S, Lochner C, Vythilingum B, Stein D, 2013. Predictors of distress and anxiety during pregnancy. Afr. J. Psychiatr. 16, 118–122. [DOI] [PubMed] [Google Scholar]
- Ruiz JM, Hamann HA, Mehl MR, O’Connor M-F, 2016. The Hispanic health paradox: from epidemiological phenomenon to contribution opportunities for psychological science. Group Process. Intergr. Relat. 19, 462–476. [Google Scholar]
- Santos IS, Matijasevich A, Tavares BF, Barros AJ, Botelho IP, Lapolli C, et al. , 2007. Validation of the Edinburgh postnatal depression scale (EPDS) in a sample of mothers from the 2004 pelotas birth cohort study. Cad. Saúde Pública 23, 2577–2588. [DOI] [PubMed] [Google Scholar]
- Schetter CD, Glynn L, 2011. The handbook of stress science: biology, psychology, and health. In: C R, B A (Eds.), Handbook of Stress Science: Biology, Psychology, and Health. Springer Publishing Company, New York, NY, pp. 321–343. [Google Scholar]
- Spielberger CD, 1983. Manual for the State-Trait Anxiety Inventory: STAI (Form Y). Consulting Psychologists Press, Palo Alta, CA. [Google Scholar]
- Stein DJ, Nesse RM, 2011. Threat detection, precautionary responses, and anxiety disorders. Neurosci. Biobehav. Rev. 35, 1075–1079. [DOI] [PubMed] [Google Scholar]
- Strahm AM, Hilmert CJ, Campos B, Dvorak RD, Sandman CA, Hobel CJ, et al. , 2018. Latina acculturation and pregnancy from a biopsychosocial perspective: anxiety, social support, and blood pressure. Psychosom. Med. 80, A148. A148. [Google Scholar]
- Teruya SA, Bazargan-Hejazi S, 2013. The immigrant and Hispanic paradoxes: a systematic review of their predictions and effects. Hisp. J. Behav. Sci. 35, 486–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tluczek A, Henriques JB, Brown RL, 2009. Support for the reliability and validity of a six-item state anxiety scale derived from the State-Trait Anxiety Inventory. J. Nurs. Meas. 17, 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torche F, Sirois C, 2018. Restrictive Immigration law and birth outcomes of immigrant women. Am. J. Epidemiol. 188, 24–33. [DOI] [PubMed] [Google Scholar]
- Valdez CR, Padilla B, Valentine JL, 2013. Consequences of Arizona’s immigration policy on social capital among Mexican mothers with unauthorized immigration status. Hisp. J. Behav. Sci. 35, 303–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van de Mortel TF, 2008. Faking it: social desirability response bias in self-report research. Aust. J. Adv. Nurs. 25, 40. [Google Scholar]
- Vargas ED, Benitez VL, 2019. Latino parents’ links to deportees are associated with developmental disorders in their children. J. Community Psychol. 47, 1151–1168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wadhwa PD, Sandman CA, Porto M, Dunkel-Schetter C, Garite TJ, 1993. The association between prenatal stress and infant birth weight and gestational age at birth: a prospective investigation. Am. J. Obstet. Gynecol. 169, 858–865. [DOI] [PubMed] [Google Scholar]
- Woolf SH, Braveman P, 2011. Where health disparities begin: the role of social and economic determinants—and why current policies may make matters worse. Health Aff. 30, 1852–1859. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.