

Abstract
Background
Retention of first‐time donors is pivotal for blood collection centers. The present study built on research showing the importance of donor identity among regular donors and sought to compare the effectiveness of various communication strategies on return rate.
Study Design and Methods
Postal letters were sent to a large sample of first‐time whole blood donors (N = 1219) a few weeks following their first donation. Four versions of this letter were differently constructed in a way to boost the acquisition of donor identity (i.e., by including information about their ABO and Rh(D) blood group, emphasizing the salience of donor identity, offering a keyring with personalized information, or specifying the percentage of those sharing the same ABO and Rh(D) blood group). One version with no identity‐related information served as a control condition. Participants' subsequent blood donations were tracked for 5–22 months after receiving the letter.
Results
Survival analysis showed that the return rate was significantly higher among those who had received information about the percentage of the country's population with the same ABO and Rh(D) blood group (in comparison with the four other versions). There was no significant effect on the blood type rarity.
Conclusion
Blood collection centers could orient the strategy employed to communicate with first‐time donors to improve donors' retention. Arousing a sense of social identification with others with the same blood type may reveal a promising avenue.
Keywords: blood donor retention, donor identity, first‐time donors, personalized communication
1. INTRODUCTION
Although more than 118 million blood donations are collected each year worldwide, demand for whole blood remains remarkably high. Blood collection centers spend significant effort recruiting new donors but face the challenge of encouraging first‐time donors to repeat donations and establish long‐term donation habits. Indeed, the retention of novice donors is crucial for securing a stable blood supply and saving financial costs that would otherwise be invested in recruiting new donors. 1 Unfortunately, the return of novice donors is relatively low. Approximately 50% of first‐time donors are estimated not to make a further donation in the United States. 2 The present research tested the effectiveness of various communication strategies that focus on developing donor identity on the proportion of first‐time donors who return over 5–22 months following their initial donation.
Impactful communication strategies and interventions are necessary to increase willingness to return and stabilize sufficient provision of blood components. Studies have tested, sometimes with mixed results, several modes of communication with donors, such as postdonation text messaging, 3 , 4 , 5 , 6 or letters, telephone calls, or electronic messaging. 7 , 8 The review by Irving et al. 9 showed that the intervention with the highest impact was a letter combined with a telephone call.
However, the authors 9 did not compare the content of the interventions (e.g., assessing the effect size of an altruistic script [be it by phone or by letter] compared to existing practice), leaving unresolved the question of the most effective communication content.
Some studies have specifically targeted first‐time donors, 5 , 10 , 11 , 12 and the meta‐analysis by Bagot showed that praising donors and sending a reminder had a small positive effect on return, while praise and commitment had a small negative effect. 2 The authors also conclude that the most successful predictive factors of return donation (such as the extended theory of planned behavior variables, attitudes, perceived behavioral control, intention, and self‐identity) have not been yet targeted by interventions, the most widespread type of intervention being incentives and reminders. This conclusion calls for intervention targeting determinants of behavior that have been shown to predict return donation.
A growing number of studies have shown that donor identity (i.e., the degree to which a person considers himself or herself a blood donor) is a significant determinant of the return of first‐time donors and maintenance of long‐term donation behaviors. 2 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 According to identity theory, role‐based identities develop as individuals repeatedly experience situations that require them to occupy specific roles. 16 , 17 , 21 In turn, the more individuals form an idea of themselves based on social roles, the more likely they are to act congruently with the central characteristics of such a self‐conception.
The formation of self‐identity as a blood donor has been shown to increase with repeated donations. 14 , 16 , 17 , 22 , 23 , 24 , 25 According to Callero and Piliavin, 26 it takes at least three donation sessions for people to identify themselves as regular donors and integrate blood donation as a significant part of themselves. It is fundamental that donors quickly establish a donor identity (ideally after the first donation) to perpetuate donation practices because of the considerable loss of donors occurring after the first donation. 2 As recommended by some, 13 , 27 , 28 blood collection centers could promote the construction of a donor identity by offering role‐identity cues or symbols such as badges, stickers, cards, or certificates.
Although the relationship between donor behavior and identity has been relatively well‐documented, there is a dearth of studies examining how to encourage the acquisition of a donor identity among first‐time donors and boost return rates (in the review of Bagot et al., 2 none of the interventions listed referred to identity). To the best of our knowledge, only the research conducted by Chamla et al. 1 approaches testing this question. Comparing an experimental group with a control group, the authors tested the effectiveness of an intervention to increase retention among samples of early‐career donors (i.e., who had previously donated one or two times in their lifetime). The experimental group received a letter with personalized information about the percentage of individuals with the same blood type who donate blood in New Zealand. The control group received a letter with only information about blood donation. Results showed that donors assigned to the experimental group returned significantly more than donors assigned to the control group. Although the initial aim of the authors was to increase self‐efficacy through the percentage information, they acknowledge in the discussion that the increased personalization of the recruitment letter might be responsible for the effect.
The present research aimed to evaluate interventions to promote donor identity on retention to donate blood. Innovatively, we conducted a randomized field trial comparing five communication strategies embedded in postal letters sent to a large sample of first‐time donors within 2 weeks after their first donation. Four of those letters included various information and cues supposed to increase donor identity, and one version with standard postdonation information was used as a control condition. Over more than 1 year after the first donation, participants' subsequent donations were tracked and recorded. In comparison to the control condition, we expected each version to increase the likelihood of making a subsequent donation attempt. More specifically, because the content of the letters was built in an incremental structure, we expected the following pattern of results on return rate: control < Version 2 < Version 3 < Version 4 and Version 5.
2. MATERIALS AND METHODS
The blood donation center of the University Hospitals collects about 14,000 RBC units annually, of which first‐time donors donate 10%. The local procedure is to send a postal letter to each first‐time donor 2 weeks after the donation to confirm that no anomaly was detected in the screening testing and mention the delay for return donation for men and women. Of note, a whole blood donation is possible three to four times a year and platelet donation 12 times a year, according to our national prescriptions.
We tested different communication strategies by constructing five versions of this letter (including a control version). All versions contained common basic information: the letters started by thanking the person for their visit to the blood donation center and then contained standard information about the results of the mandatory tests for infectious diseases and the delay between donation for men and women. Next, donors were informed that they would receive an official card with their blood type after the second donation. Finally, the center's opening hours and the possibility to book online an appointment for the next donation were presented.
The control version contained only the basic information described above.
Version 2 contained additional information about the ABO and RhD blood type of the person through the sentence: “Based on the analysis carried out, we are pleased to inform you that you belong to the blood group [blood type]. After the second donation, you will receive an official blood group card.”
Version 3 contained the same text as Version 2, in addition to two statements highlighting the identity of the blood donor (after being thanked for coming to the blood donation center: “Through this act, you are now a blood donor”; and at the end of the letter: “As you are now a blood donor, it would be a pleasure to see you again soon”).
Version 4 comprised all the same content as Version 3, accompanied by a keyring representing a blood pouch inscribed with the person's blood type.
Version 5 comprised the same content as Version 3, with the difference that the blood type information was accompanied by the percentage of the country population having the same blood type as the person. “Based on the analysis carried out, we are pleased to inform you that you belong to the blood group [blood type]. This group is represented in [X]% of the population in Switzerland. After the second donation, you will receive an official blood group card.” No keyring was sent in Version 5.
The study procedure was approved by the University ethical board (n°PSE.20190104.11). The study flow diagram is presented in Figure 1, and the demographics and donor characteristics of the sample are presented in Table 1. Only donors who donated for the first time at the center from September 2019 to September 2020 were eligible. The duration of the study was determined by the fact that we estimated a minimum of 231 donors per study arm would be sufficient regarding statistical power, as calculated with G‐power 29 based on the results by Chamla et al. 1 showing a return rate of first‐time donors in the experimental group of 23%, and 13% in the control group.
FIGURE 1.
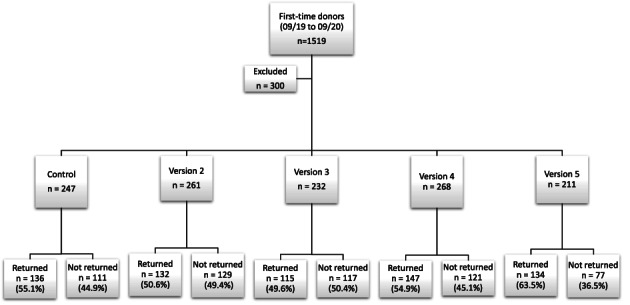
Flow diagam. Exclusions criteria are: Incorrect mailing address (letter returned to sender), N = 1; participants refusing the use of their data in the online survey, N = 2; donors not donating for the first time, N = 297
TABLE 1.
Sample description for each version of the letter
| Version 1—control (n = 247) | Version 2 (n = 261) | Version 3 (n = 232) | Version 4 (n = 268) | Version 5 (n = 211) | |
|---|---|---|---|---|---|
| Mean age (SD) | 32.43 (12.10) | 32.61 (12.04) | 30.58 (10.70) | 30.98 (11.10) | 31.27 (11.37) |
| Gender (% female) | 49.4% | 53.3% | 56.5% | 51.1% | 52.6% |
| Average number of days from the first donation to the end of the data collection (SD) min–max | 480 (94) 315–669 | 466 (102) 307–662 | 479 (107) 301–655 | 469 (104) 284–648 | 457 (114) 261–641 |
Note: Before data analysis, we excluded 297 donors from the sample because they had previously donated blood in other transfusion centers. Because these exclusion criteria were not anticipated at the time we performed the sample size calculation, one version suffers from many participants slightly below the minimum planned (211 instead of 231).
Each participant was assigned a specific version of the letter based on the week they donated blood. This method was chosen because individual randomization would have induced a too heavy workload for the regular staff of the blood donation center. Another reason was that if donors came with other people, sending the same version of the letter to each of them was preferable to prevent drawing attention to the experimental manipulation. The letters were sent over 1 year, and thus we expected any differences caused by any punctual event to be averaged out on the total sample. However, we considered the COVID‐19 crisis, which started during our project. A lockdown was installed in March 2020 in the country, and solidarity calls for donating blood appeared in the news during this period (see Spekman et al. 30 showing the increase in new donor registration in the Netherlands in the first peak of the COVID‐19 pandemic). Therefore, our analyses controlled for whether the first donation was performed before or after the beginning of the lockdown.
Due to the method of allocation in the experimental conditions, participants numbers vary slightly (N after exclusions): control condition = 247, Version 2 = 261, Version 3 = 232, Version 4 = 268, Version 5 = 211. Because of the recruitment method (i.e., donors entering the study at their first donation over 1 year), and the fact that the end of the study was the same for everyone, the follow‐up length varies between and within groups (see Table 1). One‐way analysis of variance showed that the difference in the average length of follow‐up among groups is not significant (F(4, 1214) = 1.86, p = .115). However, and because the length of follow‐up also varies between donors, survival analysis was used to take into account this variation. 31
Return data was obtained from computerized blood donation records. We considered returning donors any person who attempted to give blood (whole blood or platelets), independently of their eligibility status at the time of return. Because the main focus of the study was on the return of first‐time donors (in opposition to long‐term retention), we categorized the return data into a dichotomous variable: no‐repeat donation versus returned donor (attempting to donate blood at least one time after the first time).
In addition to the behavioral data collected from the center, we sent an online survey to a subsample of participants. To minimize the burden on donors and prevent losing future returns because of over‐solicitation, the choice was made to invite to participate only a subsample. The goal of the survey was to gain more insights into the processes underlying a potential effect on behavior. Because the sample answering to the online survey was small (between 25 and 46 answers by condition) and no differences emerged according to which version the respondent received, description of the items and the results are presented only in Appendix A.
3. RESULTS
Within the 5–22 months return was measured, 54.5% of the sample returned, while 45.5% did not come back. More specifically, 55.1% returned in the control condition, 50.6% in Version 2, 49.6% in Version 3, 54.9% in Version 4, and 63.5% in Version 5. Survival analyses were conducted, with the event of interest being an attempted return, and donors not returning before the end of the follow‐up were censored. Cox regression 32 was selected to control for gender and the first donation timing (before or after the beginning of the lockdown). Results are presented in Figure 2.
FIGURE 2.
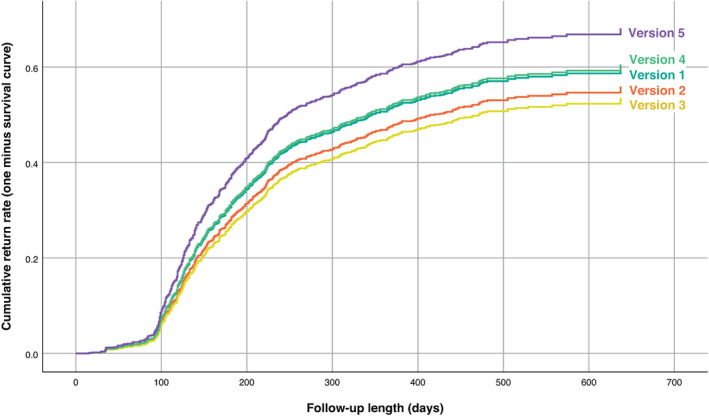
Cumulative return rate by letter's version with follow‐up length [Color figure can be viewed at wileyonlinelibrary.com]
Because the letters were built incrementally (i.e., each version of the letter contained an additional ingredient compared to the previous one), we used the difference contrast (also called reverse Helmert contrasts) to compare the return rate in each group (except the first) to the mean of previous groups. Comparisons are presented in Table 2.
TABLE 2.
Coding of contrasts used to compare the effectiveness of the letters versions
| Type of contrast | Comparison | Letters versions | ||||
|---|---|---|---|---|---|---|
| Version 1 (control) | Version 2 | Version 3 | Version 4 | Version 5 | ||
| Difference contrasts | V1 vs. V2 | −1 | 1 | 0 | 0 | 0 |
| V1 and V2 vs. V3 | −1 | −1 | 2 | 0 | 0 | |
| V1 and V2 and V3 vs. V4 | −1 | −1 | −1 | 3 | 0 | |
| V1 and V2 and V3 and V4 vs. V5 | −1 | −1 | −1 | −1 | 4 | |
| Simple contrasts (sensitivity analysis, see results in Appendix A) | V1 vs. V2 | −1 | 1 | 0 | 0 | 0 |
| V1 vs. V3 | −1 | 0 | 1 | 0 | 0 | |
| V1 vs. V4 | −1 | 0 | 0 | 1 | 0 | |
| V1 vs. V5 | −1 | 0 | 0 | 0 | 1 | |
| Repeated contrasts (sensitivity analysis, see results in Appendix A) | V1 vs. V2 | −1 | 1 | 0 | 0 | 0 |
| V2 vs. V3 | 0 | −1 | 1 | 0 | 0 | |
| V3 vs. V4 | 0 | 0 | −1 | 1 | 0 | |
| V4 vs. V5 | 0 | 0 | 0 | −1 | 1 | |
Results of these analyses showed that Version 2 was not significantly different from the control version (Wald = 0.83, p = .362, odds ratio [OR] = 0.89, 95% confidence interval [CI] [0.70–1.14]). Version 3 was not significantly different from the control and Version 2 (Wald = 1.17, p = .280, OR = 0.89, 95% CI [0.71–1.10]), neither Version 4 from the three preceding ones (Wald = 1.32, p = .251, OR = 1.12, 95% CI [0.92–1.35]). The only version that was significantly different from the others is Version 5 (Wald = 8.99, p = .003, OR = 1.34, 95% CI [1.11–1.62]). Donors who received Version 5 returned more than donors having received any of the other versions. Controlling for whether the first donation was performed before or after the beginning of the lockdown did not reveal a significant effect (Wald = 0.98, p = .322, OR = 1.08, 95% CI [0.93–1.27]), neither did the gender of the donor (Wald = 0.27, p = .600, OR = 1.04, 95% CI [0.89–1.21]).
To verify that the results do not depend on the choice of contrasts used in the primary analysis (difference contrasts), we conducted a sensitivity analysis using other types of contrasts (see the coding for simple contrasts and repeated contrasts in Table 2). The detailed results of the sensitivity analysis are presented in Appendix A. No changes in the interpretation of the results emerged following the sensitivity analysis, as Version 5 remained the version with the highest rate of return donors. However, the difference is marginally significant when comparing Version 5 to control (simple contrasts) and Version 5 to Version 4 (repeated contrast). For the sake of exhaustivity, we also compared Version 5 with Version 3, as they share similar content, with the only difference being the information about the percentage present in Version 5 and absent in Version 3. Results show that Version 5 significantly outperforms Version 3.
3.1. Rareness of the percentage
Because the percentage mentioned in Version 5 varied according to the donor blood type, we tested if the rareness of the group (based on the occurrence percentages in Switzerland 33 ) affected the effect of Version 5. Group type A RhD+ and O RhD+ were coded as nonrare (respectively, 40% and 35%), while A RhD−; B RhD+; B Rh D−; AB RhD +; AB RhD−; O RhD− were coded as rare (in order: 7%; 7%; 1%; 3%; 1%; 6%). A logistic regression showed that this factor did not have a significant impact on the return rate (Wald = 0.25, p = .614, OR = 0.86, 95% CI [0.47–1.56]). For more information on the percentage of return according to blood type in Version 5 and control version, see Table 3.
TABLE 3.
Return rate in each blood type according to the letter version
| A− | A+ | AB− | AB+ | B− | B+ | O− | O+ | |
|---|---|---|---|---|---|---|---|---|
| % return in Version 5 (total N) | 77.8 (18) | 70.1 (67) | 0 (0) | 50.0 (8) | 50.0 (6) | 41.2 (17) | 72.2 (18) | 58.7 (75) |
| % return in control version (total N) | 45.5 (22) | 58.7 (75) | 0 (1) | 33.3 (15) | 100 (1) | 41.7 (24) | 65.0 (20) | 58.6 (87) |
4. DISCUSSION
The current research aimed to test the effectiveness of various communication strategies on the return among a sample of first‐time donors.
Results showed that, compared to all the other versions, the version containing specific information about how many people possess the same blood type (Version 5) was significantly more effective in retaining first‐time donors.
Those findings replicate Chamla et al., 1 who also found that such personalized information was likely to double the return rates compared to a control condition. However, their material mentioned the percentage of people with the same blood type and also donating blood (and not the percentage of people sharing the same blood type in the population, as in our study). Comparing our results to theirs suggest that the information does not need to relate directly to blood donors for changes in behavior to emerge. Moreover, similar to what Chamla et al. 1 observed, the rarity of the blood type did not affect the effect of our material on the return rate.
Surprisingly, the strategies used to raise donor identity in Versions 2–4 did not increase returns. Since Version 5 effectively increased return, the percentage information might be seen as the active ingredient. Two main interpretations are possible: either as a dose–response effect (only the accumulation of the knowledge of blood type plus the statements highlighting donor identity combined with the percentage is strong enough to impact return behavior), or the percentage information is not triggering identity aspects, but other ones such as norms and perceived importance of donating, and identity aspects are not effective to impact return. Similar to the reasoning by Chamla et al. 1 on the percentage triggering self‐efficacy beliefs, knowing the percentage of people with the same blood type could have influenced the perceived importance of donating. By learning that they belong to a rare group, first‐time donors might perceive that donation is crucial because only a few people can provide blood among those sharing their blood type. Alternatively, if they are told that they are a member of a nonrare group, they might still think that their donation is essential as demand for that type of blood is more prevalent. Further studies are needed to clarify these mechanisms and disentangle them from identity‐based ones. Moreover, there are additional explanations, such as uncontrolled sources of variance, notably the COVID pandemic, which may complicate the interpretation of results. Those elements are discussed more in‐depth in the limitations section.
On a practical level, our results provided empirical support for the effectiveness of communication strategies to increase the number of established donors. Simple, low‐cost interventions can be implemented to foster donor identity and increase the number of returns. Sending postal letters or emails is standard practice in many blood collection centers. However, attention to how adequately messaging is sometimes underworked. The present research offered evidence that simply including information such as how many people have one's blood type in common can make a difference in engaging first‐time donors to become established donors and integrate the practice of donation into their habits.
5. LIMITATIONS
First, the impact of the COVID pandemic is impossible to be entirely controlled for, even though we considered as a control variable the effect of whether the first donation was before or after the pandemic onset. Many aspects of the pandemic have links with blood donation: for example, travel restrictions influencing the ability to donate, solidarity calls in the media, and fear to leave home and catch the virus. However, the upheaval was equal for all the participants in each experimental condition. Thus, although the pandemic might have influenced the global level of donation rate (lowering it or increasing it compared to a world without the pandemic), there is no reason to believe that this may have differed across conditions.
Second, the number of days left for participants to return was not equivalent between the groups. This difference in return opportunity might be considered a source of bias. However, it should be noted that we found that the group with the shortest delay (Version 5) had the highest return rate. Therefore, if there were indeed a bias, it would have influenced our results by underestimating the observed effect. Third, Version 5 was the group with the smallest number of participants and the only one below the targeted sample size per group (n = 211 instead of 231). Thus, Version 5 is the least stable estimate. A wider confidence interval means that future studies' results might fall within a broader range of possibilities, including zero. Fourth, although we sent letters to participants' home addresses, we had no way of ensuring that they were read. The effectiveness of strategies may have been mitigated by donors who did not read our letter, did not read it carefully, or even missed the information manipulated. However, including all participants in the analysis (i.e., intention‐to‐treat 34 ) provides a more realistic effect size estimate. Indeed, when a center communicates to its donors, there will always be a share of recipients who will not receive or read the message carefully. Fifth, the survey that was sent to a subsample (results reported in Appendix A) may have influenced the return rate, either positive (e.g., by acting as a reminder), or negative (e.g., individuals might have reacted negatively to being solicited so soon after a donation by the center). Nevertheless, this hypothetical effect would have been the same in each experimental condition and, thus, not considered confounding. Sixth, participants' return was calculated based on personal donations collected at the blood donation center participating in the study. Some may have returned donating at other collection centers elsewhere in the country. If so, their subsequent donations could not have been included in our data. Seventh, in the control version, the donors were not informed about their blood type in the letter and had to donate blood once more to learn it. Some might have returned to learn their blood type and explain the slight (although not significant) decrease in return rate from Version 1 to Versions 2 and 3. A future study could test a similar design on increasing retention after the second donation to remove the aspect associated with being informed of one's blood type. Finally, it is important to mention that our communication strategies were designed with the idea of stimulating a sense of identity, which was theorized to energize a motivation to engage in repeated donation behavior. However, there is no clear evidence that identity is the aspect that was manipulated across the different versions of the letter; neither that it is, in fact, the ingredient responsible for the effects obtained in Version 5. As mentioned above, other interpretations of the results might be suggested. Further studies are needed to identify the psychological mechanisms underlying the effect of the strategies examined. Future work could also investigate the effect on long‐term return. Our results cannot tell if donors who return thanks to the letter became regular donors or if the effect occurred only on the subsequent return, and then vanished. If an identity of the donor was created as hypothesized, the effect is expected to be long‐term.
6. CONCLUSION
Encouraging early‐career donors to return donating blood is a major challenge for blood donation centers. The present study proposed to test the impact of a range of easy‐to‐implement communication techniques whose purpose was to promote the development of donor identity. Results showed that the most effective strategy is to emphasize the proportion of people sharing the same blood type. Therefore, we encourage collection centers to develop communication strategies that include and highlight information about how first‐time donors are socially connected and belong to a common group with those having their blood type.
CONFLICT OF INTEREST
The authors have disclosed no conflicts of interest.
ACKNOWLEDGMENTS
The authors thank Joëlle Herren‐Vichet, Noémie Faustino, and Valérie Montellier Delaigue from the Blood Transfusion Center for their contribution in sending the letters to donors, and their help with extracting return data. Open access funding provided by Universite de Geneve.
APPENDIX A.
A.1. SENSITIVITY ANALYSIS
To verify that the results do not depend on the choice of contrasts used in the main analysis, we conducted a sensitivity analysis using other types of contrasts. We tested the effect of each version compared to the control version, and then tested the effect of each version compared to the adjacent level (see coding in Table 2). In the simple contrasts (each version against control), Versions 2, 3, and 4 were not significantly different from the control (respectively, Wald = 0.83, p = .362, OR = 0.90, 95% CI [0.70–1.14]; Wald = 1.93, p = .164, OR = 0.84, 95% CI [0.65–1.08]; Wald = 0.02, p = .896, OR = 1.02, 95% CI [0.80–1.28]). Version 5 was marginally significant from the control version (Wald = 3.33, p = .068, OR = 1.25, 95% CI [0.98–1.59]). In the repeated contrasts, the control was not significantly different from Version 2 (Wald = 0.83, p = .362, OR = 1.12, 95% CI [0.88–1.42]). Version 2 was not significantly different from Version 3 (Wald = 0.26, p = .610, OR = 1.07, 95% CI [0.83–1.37]), nor Version 3 compared to Version 4 (Wald = 2.38, p = .123, OR = 0.83, 95% CI [0.65–1.05]). Version 4 was marginally different from Version 5 (Wald = 3.00, p = .083, OR = 0.81, 95% CI [0.64–1.03]). For the sake of exhaustivity, we also compared Version 5 with Version 3, as they share similar content with the only difference being the information about percentage present in Version 5 and absent in Version 3. This contrast showed that Version 5 is significantly different from Version 3, (Wald = 10.00, p = .002, OR = 1.50, 95% CI [1.17–1.92]).
A.2. ONLINE SURVEY
The online survey contained items measuring psychological variables possibly influenced by the content of the letters. All scales are 7‐points Likert scale ranging from “totally disagree” to “totally agree.”
A.2.1. Identification
Five items measured the identification of blood donor role: “Being a blood donor is important for me,” 35 “Being a blood donor is something that I am proud of,” “I feel similar to blood donors,” 36 “I identify myself to blood donors,” 36 “I really do not have any clear feelings about blood donation” (reversed item). 37 Cronbach α on the entire scale = .772, and increased to .746 when removing the last item. A score based on the first four items was used for the analysis.
A.2.2. Outcome expectancy
Three items measured the perceived importance of the donation, that is, outcome expectancy: “My blood donation is indispensable”; “If I were not to donate my blood, there wouldn't be enough”; “The fact that I come to donate blood is necessary.” The three items had satisfactory reliability (α = .776) and were averaged to create a score.
A.2.3. Intention
Three items measured the intention to donate blood in the future: “I intend to donate blood in the next four months”; “I am decided to donate blood in the next four months”; “I feel motivated to donate blood in the next four months.” The three items had very good reliability (α = .941) and were averaged to create a score.
The online survey was sent to donors included in the study who provided their email addresses to the blood donation center. All donors who matched the criteria on a specific week were included, and the procedure was repeated until we obtained at least 150 responses, that is, around 30 by condition. Due to unequal repartition among conditions, one condition has less than 30 respondents. Descriptive statistics for the three DVs in each experimental condition are presented in Table A1.
An ANOVA showed that the level of identification did not vary according to the content of the letters, F(4, 192) = 0.89, p = .470, ƞ 2 p = .018.
TABLE A1.
Means and SD for the DVs measured online according to the version of the letters
| Control (n = 44) | Version 2 (n = 42) | Version 3 (n = 42) | Version 4 (n = 46) | Version 5 (n = 25) | |
|---|---|---|---|---|---|
| Identification | 5.64 (0.14) | 5.71 (0.14) | 5.62 (0.14) | 5.90 (0.13) | 5.55 (0.18) |
| Outcome expectancy | 5.42 (0.16) | 5.80 (0.16) | 5.55 (0.17) | 6.02 (0.16) | 5.15 (0.21) |
| Intention | 6.42 (0.17) | 6.41 (0.17) | 6.17 (0.17) | 6.48 (0.16) | 6.27 (0.22) |
Another ANOVA was conducted on outcome expectancy, and showed that it varied according to the content of the letters, F(4, 188) = 3.57, p = .008, ƞ 2 p = .071. Difference contrasts analysis revealed that two comparisons were significant. Version 4 led to a higher level of OE compared to Versions 1, 2 and 3 grouped together, p = .015, 95% CI [0.09–0.80]. Version 5 led to a lower level of OE compared to Versions 1, 2, 3, and 4 grouped, p = .018, 95% CI [−0.97 to −0.09].
Finally, an ANOVA showed that the level of intention did not vary according to the content of the letters, F(4, 187) = 0.51, p = .732, ƞ 2 p = .011.
Moussaoui LS, Blondé J, Chaduc‐Lemoine C, Baldelli S, Desrichard O, Waldvogel S. How to increase first‐time donors' returns? The postdonation letter's content can make a difference. Transfusion. 2022;62(7):1377–1387. 10.1111/trf.16933
REFERENCES
- 1. Chamla JH, Leland LS, Walsh K. Eliciting repeat blood donations: tell early career donors why their blood type is special and more will give again. Vox Sang. 2006;90(4):302–7. 10.1111/j.1423-0410.2006.00756.x [DOI] [PubMed] [Google Scholar]
- 2. Bagot KL, Murray AL, Masser BM. How can we improve retention of the first‐time donor? A systematic review of the current evidence. Transfus Med Rev. 2016;30(2):81–91. 10.1016/j.tmrv.2016.02.002 [DOI] [PubMed] [Google Scholar]
- 3. Moussaoui LS, Herren‐Vichet J, Baldelli S, Waldvogel S, Desrichard O. Examining if sending text messages to thank blood donors for saving lives is a “great idea”? Evidence from a randomized field experiment. J Nonprofit Publ Sect Market. 2019;31(5):486–506. [Google Scholar]
- 4. Gemelli CN, Carver A, Garn A, Wright ST, Davison TE. Evaluation of the impact of a personalized postdonation short messaging service on the retention of whole blood donors: impact of sms on donor retention. Transfusion. 2018;58(3):701–9. 10.1111/trf.14463 [DOI] [PubMed] [Google Scholar]
- 5. Pongsananurak C, Norasetthada L, Tantiworawit A, Rattarittamrong E, Rattanathammethee T, Hantrakool S, et al. The effects of text messaging for promoting the retention of the first‐time blood donors, a randomized controlled study (TEXT study). Transfusion. 2020;60(10):2319–26. 10.1111/trf.15984 [DOI] [PubMed] [Google Scholar]
- 6. Rodrigues Lucena TF, Queiroz Negri L, Marcon D, Yamaguchi MU. Is WhatsApp effective at increasing the return rate of blood donors? Telemed J E Health. 2020;26(3):304–9. 10.1089/tmj.2019.0024 [DOI] [PubMed] [Google Scholar]
- 7. Bachegowda LS, Timm B, Dasgupta P, Hillyer CD, Kessler D, Rebosa M, et al. Impact of predictive scoring model and e‐mail messages on African American blood donors. Transfusion. 2017;57(6):1515–21. 10.1111/trf.14113 [DOI] [PubMed] [Google Scholar]
- 8. Moussaoui LS, Naef D, Tissot JD, Desrichard O. “Save lives” arguments might not be as effective as you think: a randomized field experiment on blood donation. Transfus Clin Biol. 2016;23(2):59–63. 10.1016/j.tracli.2016.03.003 [DOI] [PubMed] [Google Scholar]
- 9. Irving AH, Harris A, Petrie D, Mortimer D, Ghijben P, Higgins A, et al. A systematic review and network meta‐analysis of incentive‐ and non‐incentive‐based interventions for increasing blood donations. Vox Sang. 2020;115(4):275–87. 10.1111/vox.12881 [DOI] [PubMed] [Google Scholar]
- 10. Hashemi S, Maghsudlu M, Nasizadeh S, Esmaielifar G, Pourfathollah AA. Effective ways to retain first‐time blood donors: a field‐trial study. Transfusion. 2019;59(9):2893–8. 10.1111/trf.15404 [DOI] [PubMed] [Google Scholar]
- 11. Porto‐Ferreira FA, de Almeida‐Neto C, Murphy EL, Montebello SC, Nogueira FAH, Koga da Silva EM, et al. A randomized trial to evaluate the use of text messaging, letter, and telephone call reminders to improve return of blood donors with reactive serologic tests. Transfusion. 2017;57(1):102–7. 10.1111/trf.13882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Reich P, Roberts P, Laabs N, Chinn A, McEvoy P, Hirschler N, et al. A randomized trial of blood donor recruitment strategies. Transfusion. 2006;46(7):1090–6. 10.1111/j.1537-2995.2006.00856.x [DOI] [PubMed] [Google Scholar]
- 13. Masser BM, White KM, Hyde MK, Terry DJ. The psychology of blood donation: current research and future directions. Transfus Med Rev. 2008;22(3):215–33. 10.1016/j.tmrv.2008.02.005 [DOI] [PubMed] [Google Scholar]
- 14. Masser BM, Bednall TC, White KM, Terry D. Predicting the retention of first‐time donors using an extended theory of planned behavior. Transfusion. 2012;52(6):1303–10. 10.1111/j.1537-2995.2011.03479.x [DOI] [PubMed] [Google Scholar]
- 15. Wevers A, Wigboldus DHJ, van Baaren R, Veldhuizen IJT. Return behavior of occasional and multigallon blood donors: the role of theory of planned behavior, self‐identity, and organizational variables: determinants of donor return behavior. Transfusion. 2014;54(3pt2):805–13. 10.1111/trf.12309 [DOI] [PubMed] [Google Scholar]
- 16. Callero PL. Role‐identity salience. Soc Psychol Q. 1985;48(3):203–15. 10.2307/3033681 [DOI] [Google Scholar]
- 17. Charng HW, Piliavin JA, Callero PL. Role identity and reasoned action in the prediction of repeated behavior. Soc Psychol Q. 1988;51(4):303–17. 10.2307/2786758 [DOI] [Google Scholar]
- 18. Thorpe R, Masser BM, Jensen K, Van Dyke N, Davison TE. The role of identity in how whole‐blood donors reflect on and construct their future as a plasma donor. J Community Appl Soc Psychol. 2020;30(1):73–84. 10.1002/casp.2429 [DOI] [Google Scholar]
- 19. White KM, Poulsen BE, Hyde MK. Identity and personality influences on donating money, time, and blood. Nonprofit Volunt Sect Q. 2017;46(2):372–94. 10.1177/0899764016654280 [DOI] [Google Scholar]
- 20. Mauny N, Mange J, Mortier A, Somat A, Sénémeaud C. When a refusal turns into donation: the moderating effect of the initial position toward blood donation in the door‐in‐the‐face effectiveness. J Soc Psychol. 2022;XX:1–18. [DOI] [PubMed] [Google Scholar]
- 21. Stets JE, Burke PJ, Serpe RT, Stryker J. Getting identity theory (IT) right. In: Thye SR, Lawler EJ, editors. Advances in Group Processes. Bingley, UK: Emerald Publishing Limited; 2020. p. 191–212. [Google Scholar]
- 22. Piliavin JA, Callero PL. Giving Blood: The Development of an Altruistic Identity. Baltimore, MD: Johns Hopkins University Press; 1991. [Google Scholar]
- 23. Piliavin JA, Evans DE, Callero P. Learning to “give to unnamed strangers”. In: Staub E, Bar‐Tal D, Karylowski J, Reykowski J, editors. Development and Maintenance of Prosocial Behavior. Boston, MA: Springer; 1984. p. 471–92. 10.1007/978-1-4613-2645-8_29 [DOI] [Google Scholar]
- 24. Piliavin J. Why do they give the gift of life? A review of research on blood donors since 1977. Transfusion. 1990;30(5):444–59. 10.1046/j.1537-2995.1990.30590296381.x [DOI] [PubMed] [Google Scholar]
- 25. Sugden N, King N. A descriptive phenomenological analysis of the experience of blood donation as a regular donor. J Health Psychol. 2021;26(11):1821–32. 10.1177/1359105319890014 [DOI] [PubMed] [Google Scholar]
- 26. Callero PL, Piliavin JA. Developing a commitment to blood donation: the impact of one's first experience. J Appl Social Pyschol. 1983;13(1):1–16. 10.1111/j.1559-1816.1983.tb00883.x [DOI] [Google Scholar]
- 27. Ringwald J, Zimmermann R, Eckstein R. Keys to open the door for blood donors to return. Transfus Med Rev. 2010;24(4):295–304. 10.1016/j.tmrv.2010.05.004 [DOI] [PubMed] [Google Scholar]
- 28. Ferguson E, Murray C, O'Carroll RE. Blood and organ donation: health impact, prevalence, correlates, and interventions. Psychol Health. 2019;34(9):1073–104. 10.1080/08870446.2019.1603385 [DOI] [PubMed] [Google Scholar]
- 29. Faul F, Erdfelder E, Lang AG, Buchner A. G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91. 10.3758/BF03193146 [DOI] [PubMed] [Google Scholar]
- 30. Spekman MLC, Ramondt S, Quee FA, Prinsze FJ, Huis in't Veld EMJ, Hurk K, et al. New blood donors in times of crisis: increased donation willingness, particularly among people at high risk for attracting SARS‐CoV‐2. Transfusion. 2021;61(6):1822–9. 10.1111/trf.16334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Swinscow D. Survival analysis. Statistics at Square One. London, UK: BMJ Publishing Group; 1997. [Google Scholar]
- 32. Cox DR. Regression models and life‐tables. J R Stat Soc B Methodol. 1972;34(2):187–202. 10.1111/j.2517-6161.1972.tb00899.x [DOI] [Google Scholar]
- 33. Groupes Sanguins . Transfusion CRS Suisse. Available from: https://www.blutspende.ch/fr/donnees-sur-le-sang/groupes-sanguins
- 34. Kleist P. Le principe de l'intention‐to‐treat. Forum Medical Suisse. 2009;9:450–3. [Google Scholar]
- 35. Armitage CJ, Conner M. Social cognitive determinants of blood donation. J Appl Soc Psychol. 2001;31(7):1431–57. [Google Scholar]
- 36. Doosje B, Ellemers N, Spears R. Perceived intragroup variability as a function of group status and identification. J Exp Soc Psychol. 1995;31(5):410–36. 10.1006/jesp.1995.1018 [DOI] [Google Scholar]
- 37. Callero PL, Howard JA, Piliavin JA. Helping behavior as role behavior: disclosing social structure and history in the analysis of prosocial action. Soc Psychol Q. 1987;50(3):247. 10.2307/2786825 [DOI] [Google Scholar]