

Abstract
Studies on relationships between psychosocial factors and health among North African (NA) women are scarce. This research investigated the self‐perceived psychosocial well‐being of NA women by a structured questionnaire and anthropometric survey examining the possible explanatory variables of their mental health in comparison to a sample of NA migrants. The association of endogenous stress, psychological well‐being, discomfort, and quality of life with migrant/non‐migrant status, demographic characteristics, and adiposity indices was examined. Moreover, the internal consistency of the questionnaire was tested using Cronbach's alpha. A sample of 228 women living in Tunis and Casablanca participated in a survey in Tunisia and Morocco. According to multiple regression models, migrant/non‐migrant status was the best explanatory variable of well‐being and quality of life, marital status, educational level and the number of children were explanatory variables of discomfort and endogenous stress. Among anthropometric variables, central adiposity was a significant explanatory variable of well‐being. The comparison with women who migrated mainly from Morocco and Tunisia to Italy (NA migrants) exhibited higher weight status and central adiposity in NA migrants. The perceived stress and discomfort were the same in the two groups; the migrants, despite reporting lower psychological well‐being, presented a higher quality of life than residents. Our findings emphasise the potential to promote monitoring of the psychosocial health of NA women, planning effective interventions.
Keywords: anthropometry, migrants, native populations, North Africa, psychosocial factors, women
What is known about this topic?
Mental health is closely interrelated with quality of life, productivity, and social capital.
Mental disorders are more frequent in the Middle East and North Africa than in other regions, especially among women.
What this paper adds?
The psychosocial questionnaire, applied for the first time in Arabic, showed good reliability.
Among the anthropometric variables examined, central adiposity was found to be negatively correlated with well‐being.
In the comparison between resident and migrant women, being resident had a positive correlation with well‐being, but the quality of life increased with migration.
1. INTRODUCTION
Mental disorders and their complications are a major public health concern, inextricably linked to the quality of life, productivity, and social capital (World Health Organization [WHO], 2012–2016). In the Eastern Mediterranean Region (EMR), mental disorders are common (Mokdad et al., 2016; WHO, 2012–2016) and often more frequent than in other countries. There are several reasons for the different incidence of mental disorders due to physical boundaries, or to socio‐cultural and economic contexts (Ravindranath et al., 2015). In particular, the challenges faced in low‐ and middle‐income countries differ from those in high‐income countries in terms of type, characteristics, or scale (Ravindranath et al., 2015). Depression and anxiety are the most frequent mental disorders in the EMR, and women present a greater incidence than men, especially in the Middle East and North Africa (Eloul et al., 2009). Due to rapid socio‐economic changes in some parts of these territories, women face a cultural struggle between their traditional domestic role and their new role in modern society through their access to higher education and the labour market. This stressful situation can cause anxiety and depression (Eloul et al., 2009).
Another important issue is related to conflicts and revolutions occurring in the EMR, which contribute to the rise of mental disorders (Ferrari et al., 2013; Ravindranath et al., 2015). In these countries, where there is a lack of access to mental health services, people suffering from these diseases are less likely to be recognised and diagnosed (Toselli et al., 2014).
Empirical evidence on effective mental health interventions and psychosocial support for the most vulnerable populations, such as women and children, in humanitarian contexts, is scarce (Kamali et al., 2020). Given the need for practical evidence to determine the interventions required in these settings (Blanchet et al., 2017) and to characterise population groups that have greater susceptibility or resilience to psychosocial disorders (Ravindranath et al., 2015), the aims of the present study were (a) to assess the psychosocial well‐being of the North African (NA) women via a structured questionnaire; (b) to determine the possible explanatory variables of mental health outcomes in NA women, considering both socio‐demographic and adiposity indices; (c) to compare their mental health outcomes to those of NA women who emigrated from Africa to Europe. The last point is important to better understand NA women's socio‐cultural, economic, and mental health needs concerning the different living environments. Since it was the first time the questionnaire was applied in Arabic, another aim of the study was to assess its reliability; therefore it was tested for internal consistency through statistical analysis.
2. PARTICIPANTS AND METHODS
2.1. Participants
In January–February 2016, we randomly recruited 252 women among outpatients with an appointment for a check‐up at public health clinics in Tunis and Casablanca. Only women who volunteered to participate in the study after an explanation of the research purposes were included in this convenience sample, following receipt of their written consent. A total of 243 women (96.4%), 138 Moroccans living in Morocco and 105 Tunisians living in Tunisia, were recruited. One of the authors (NR) checked each subject for eligibility. Among them, 228 women (90.3%) met the selection criteria and thus were eligible for the study. Inclusion criteria were as follows: (a) not being pregnant; (b) being apparently healthy; (c) being within the age range of 18–60 years; (d) being born and currently resident in Morocco or Tunisia; and (e) no missing information about the previous points. The NA resident sample included in this study was composed of 228 women resident in North Africa: 124 women living in Morocco and the other 104 in Tunisia.
For comparative purposes, we included the previously collected data of 105 NA women who emigrated from Africa to Italy (Gualdi‐Russo et al., 2016; Toselli et al., 2018). The final immigrant subsample included 85.7% Moroccans, 7.6% Tunisians and 6.7% of women from other NA countries (Algeria, Egypt).
The data were collected via face‐to‐face interviews. Ethnic origin was based on the participant's country of birth and was self‐reported by the subject.
The interviews were based on a questionnaire (in Italian and English) previously used in Europe (Toselli et al., 2018). The questionnaire was then translated from English to Arabic by the NA co‐authors, both fluent in Arabic and the English language. The translation followed a forward–backward procedure, as suggested by literature (Koller et al., 2007).
The study was performed in line with the principles of the Declaration of Helsinki. Approval was obtained from the Ethics Committee of Azienda Unità Sanitaria Locale, Bologna, Italy. Informed consent was given by all participants prior to their recruitment in the study.
2.2. Measurements
2.2.1. Demographic questionnaire
The female participants completed a questionnaire detailing age, country of birth, educational level, marital status, employment status and number of children.
2.2.2. Psychosocial questionnaire
The questionnaire included several questions for the assessment of psychosocial well‐being, including items related to both positive and negative outcomes. In particular, perceived stress was valued in terms of daily stress, work stress and personal interactions. Well‐being was referred to autonomy, environmental command, interpersonal relationships and self‐acceptance. Psychological discomfort was related to sleep disturbance, anxiety, depression and irritability. Another question regarded the quality of life. A detailed description of the questionnaire was reported previously (Toselli & Gualdi‐Russo, 2008; Toselli et al., 2018).
2.2.3. Anthropometric measurements
A trained operator (NR) directly collected several anthropometric measurements according to standardised rules (Lohman et al., 1997; Weiner & Lourie, 1981). NR measured stature to the nearest 0.1 cm with a portable stadiometer (Raven minimetre; Raven) and weight to the nearest 0.1 kg with a calibrated electronic scale. Participants were measured in light clothing and with bare feet. Waist and hip girths were measured to the nearest 0.1 cm with a non‐stretchable tape. In particular, the former was taken at the midpoint between the lower margin of the ribs and the iliac crest and the latter at the level of maximal gluteal protrusion.
The following adiposity indices were calculated: body mass index (BMI), as the weight in kilograms divided by the square of the stature in meters (kg/m2), waist–hip ratio (WHR), as waist girth divided by hip girth in centimetres, and waist–stature ratio (WSR), as waist girth divided by stature in centimetres.
2.3. Statistical analysis
Descriptive statistics were performed by computing means and standard deviations for quantitative variables, and absolute frequencies and percentages for qualitative variables. We assessed possible differences in mental health characteristics between the woman living in North Africa (current sample) and NA migrant women (Toselli et al., 2018). Comparisons between groups for continuous variables were calculated using the t‐test for independent samples while for categorical variables the χ 2 test was used.
Cronbach's alpha coefficient was calculated for the psychosocial questionnaire applied to the NA residents to assess internal consistency.
Generalised linear regression models were used to analyse the relationship between the four psychosocial indicators (endogenous stress, psychological well‐being, discomfort and quality of life), tested as dependent variables, and the migrant/non‐migrant status demographic characteristics and adiposity indices, as independent variables. We performed two separate models for each psychosocial indicator. In the first model, we entered the individual demographic characteristics (age, migrant status, educational level, work status and number of children). In the second model, the biological characteristics (BMI, WHR and WSR) were added. The goodness‐of‐fit of the final model was assessed using the likelihood‐ratio test. No interaction between the independent variables was examined.
Significance was set at p < 0.05 for all tests. Statistical analyses were carried out with STATISTICA software, version 11.
3. RESULTS
3.1. Demographic information
The mean age of women resident in North Africa was 34.5 ± 13.5 (Moroccans: 39.5 ± 13.1; Tunisians: 28.7 ± 11.5) while that of NA migrants was 36.3 ± 7.8 years. There is no statistical difference between the mean ages of NA residents and migrants (Table 1). Instead, all the other socio‐demographic variables show a highly significant difference between migrants and residents. In particular, NA residents have a higher educational level than NA migrants. Instead, the incidence of illiterate NA women is similar between the two groups. Regarding marital status, NA residents show almost equal numbers of unmarried or married, whereas most of the NA migrants are married. The opposite trend is found for work status: while almost all resident women are employed or students, migrants are mostly unemployed. The difference in the number of children is highly significant since the migrants have more children than residents.
TABLE 1.
Socio‐demographic characteristics of the samples
| Variables | NA residents (n = 228) | NA migrants (n = 105) | p |
|---|---|---|---|
| M (SD) | M (SD) | ||
| Age | 34.5 (13.5) | 36.3 (7.8) | 0.188 |
| N (%) | N (%) | ||
| Educational level | <0.001 | ||
| None | 30 (13.3%) | 13 (12.4%) | |
| Primary school | 27 (11.9%) | 15 (14.3%) | |
| Junior high school | 26 (11.5%) | 30 (28.6%) | |
| High school | 35 (15.5%) | 29 (27.6%) | |
| University | 108 (47.8%) | 18 (17.1%) | |
| Marital status | <0.001 | ||
| Single | 119 (52.7%) | 7 (6.7%) | |
| Married | 98 (43.4%) | 90 (85.7%) | |
| Divorced | 6 (2.7%) | 8 (7.6%) | |
| Widow | 3 (1.3%) | 0 (0.0%) | |
| Work status | <0.001 | ||
| Unemployed | 23 (13.6%) | 82 (78.1%) | |
| Employed/student | 146 (86.4%) | 23 (21.9%) | |
| No. of children | <0.001 | ||
| None | 131 (57.5%) | 20 (19.0%) | |
| One or two | 53 (23.2%) | 50 (47.6%) | |
| Three or four | 30 (13.2%) | 32 (30.5%) | |
| More than four | 14 (6.1%) | 3 (2.9%) |
Abbreviation: NA, North African.
3.2. Anthropometric characteristics
BMI and WSR are highly significantly different between the two groups, with higher values in migrants (Table 2). Both subsamples have a mean BMI categorised as overweight, although the residents have higher percentages of normal weight and lower overweight and obesity.
TABLE 2.
Biological characteristics of the samples
| Variables | NA residents (n = 228) | NA migrants (n = 105) | p |
|---|---|---|---|
| M (SD) | M (SD) | ||
| BMI | 25.97 (4.79) | 28.43 (4.79) | <0.0001 |
| WHR | 0.83 (0.06) | 0.82 (0.06) | 0.4149 |
| WSR | 0.42 (0.08) | 0.46 (0.08) | 0.0003 |
| N (%) | N (%) | ||
| Weight status | |||
| Underweight | 13 (5.8%) | 0 (0.0%) | 0.0001 |
| Normal weight | 85 (37.8%) | 21 (20.2%) | |
| Overweight | 76 (33.8%) | 56 (53.8%) | |
| Obese | 51 (22.7%) | 27 (26.0%) | |
Abbreviations: BMI, body mass index; NA, North African; WHR, waist–hip ratio; WSR, waist–stature ratio.
We tested the internal consistency of the Arabic‐language psychosocial questionnaire for NA residents. Cronbach's alpha coefficient for the whole questionnaire is acceptable (0.72) (Table 3). Most of the questions with an item‐correlation that is negative or lower than 0.2 (indicating poor internal consistency of these items with the others) belong to the subgroups of well‐being and quality of life (Q13–Q18 and Q32). These items address the assessment of positive health outcomes, whereas the others (exogenous and endogenous stress, psychological discomfort) are for the assessment of negative outcomes.
TABLE 3.
Mean values, standard deviations, correlations and Cronbach's α coefficients of items
| Scale item | M | SD | Correlation with total items | α if item is deleted | Standardised Cronbach's α | |
|---|---|---|---|---|---|---|
| EsS | Q1. Loss of a relative | 1.57 | 0.50 | 0.18 | 0.72 | 0.72 |
| Q2. Separation | 1.01 | 0.10 | 0.07 | 0.72 | ||
| Q3. Change of job | 1.10 | 0.30 | 0.15 | 0.72 | ||
| Q4. Change of house | 1.22 | 0.41 | 0.20 | 0.72 | ||
| Q5. Change of city | 1.22 | 0.41 | 0.18 | 0.72 | ||
| Q6. Financial difficulties | 1.55 | 0.50 | 0.42 | 0.71 | ||
| Q7. Legal issues | 1.09 | 0.28 | 0.45 | 0.71 | ||
| Q8. New relationship | 1.30 | 0.46 | −0.13 | 0.73 | ||
| EnS | Q9. Stressed at work | 2.06 | 0.95 | −0.11 | 0.74 | |
| Q10. Seriously ill relatives | 1.90 | 1.17 | 0.26 | 0.71 | ||
| Q11. Tension at home | 1.92 | 0.98 | 0.39 | 0.70 | ||
| Q12. Feeling isolated | 2.12 | 1.07 | 0.29 | 0.71 | ||
| WB | Q13. Like the job | 2.72 | 1.03 | −0.27 | 0.75 | |
| Q14. Get along with co‐workers | 2.76 | 0.90 | −0.23 | 0.74 | ||
| Q15. Get along with partner | 2.60 | 1.08 | 0.11 | 0.72 | ||
| Q16. Relationship with housemates | 3.03 | 0.87 | −0.17 | 0.74 | ||
| Q17. Confidant | 2.80 | 1.07 | 0.04 | 0.73 | ||
| Q18. Relationship with people | 2.98 | 0.77 | 0.06 | 0.72 | ||
| PD | Q19. Difficulties falling asleep | 2.12 | 1.02 | 0.35 | 0.71 | |
| Q20. Disturbed sleep | 2.31 | 1.11 | 0.53 | 0.69 | ||
| Q21. Early morning awakenings | 2.55 | 1.11 | 0.17 | 0.72 | ||
| Q22. Waking up tired | 2.41 | 1.01 | 0.38 | 0.71 | ||
| Q23. Stomach ache | 1.89 | 0.96 | 0.32 | 0.71 | ||
| Q24. Fast heart rate | 2.01 | 1.14 | 0.55 | 0.69 | ||
| Q25. Emotional instability | 1.88 | 1.04 | 0.56 | 0.69 | ||
| Q26. Oppression | 2.26 | 1.14 | 0.65 | 0.68 | ||
| Q27. Breathlessness | 1.82 | 1.05 | 0.38 | 0.70 | ||
| Q28. Tiredness | 2.24 | 1.07 | 0.52 | 0.69 | ||
| Q29. Irritability | 2.66 | 1.11 | 0.54 | 0.69 | ||
| Q30. Sadness | 2.33 | 1.12 | 0.54 | 0.69 | ||
| Q31. Nervousness | 2.73 | 1.05 | 0.57 | 0.69 | ||
| QL | Q32. Quality of life | 2.90 | 1.02 | −0.42 | 0.76 | |
Abbreviations: EnS, endogenous stress; EsS, exogenous stress; PD, psychosocial discomfort; QL, quality of life; WB, well‐being.
3.3. Psychosocial health and quality of life
The psychosocial questionnaire revealed that NA residents experienced less stressful events than migrants in the previous year and the difference is highly statistically significant (Table 4). NA residents perceive significantly higher well‐being than NA migrants, but the latter group feels they have a better quality of life. The perceived stress and discomfort are similar between the two groups.
TABLE 4.
Psychosocial indicators of the samples
| Variables | NA residents (n = 228) | NA migrants (n = 105) | p |
|---|---|---|---|
| % | % | ||
| Exogenous stress (yes %) | 22.2 | 30.4 | <0.0001 |
| M (SD) | M (SD) | ||
| Endogenous stress | 1.9 (0.6) | 1.9 (0.5) | 0.8285 |
| Well‐being | 2.8 (0.6) | 2.7 (0.5) | 0.0372 |
| Discomfort | 2.1 (0.6) | 2.0 (0.5) | 0.4345 |
| Quality of life | 2.0 (0.9) | 3.2 (1.0) | 0.0052 |
We performed different linear regression models to evaluate the impact of socio‐demographic factors (model 1) and anthropometric characteristics (model 2) on the four psychosocial indicators. The selected independent variables are shown in the conceptual model (Figure 1). The results of these predictive models are presented in Tables 5, 6, 7, 8.
FIGURE 1.
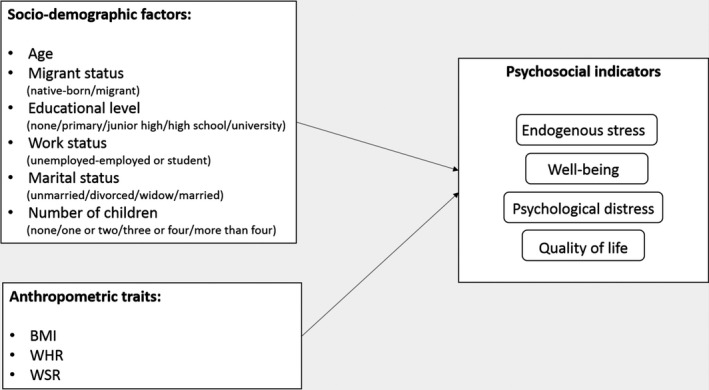
Conceptual framework illustrating the socio‐demographic and anthropometric factors selected as possible predictors of the four psychological indicators
TABLE 5.
Predictors of endogenous stress: results of multivariate regression analysis
| Predictor variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Age | 0.048 | 0.505 | 0.614 | 0.049 | 0.486 | 0.628 |
| Migrant status (native‐born) | 0.093 | 0.597 | 0.551 | 0.044 | 0.465 | 0.642 |
| Educational level | ||||||
| None | −0.093 | −0.634 | 0.527 | −0.061 | −0.409 | 0.683 |
| Primary | −0.121 | −1.031 | 0.304 | −0.115 | −0.960 | 0.338 |
| Junior high | 0.042 | 0.376 | 0.708 | −0.006 | −0.055 | 0.956 |
| High school | 0.135 | 1.266 | 0.207 | 0.127 | 1.157 | 0.249 |
| Work status (unemployed) | −0.042 | −0.464 | 0.643 | −0.037 | −0.405 | 0.686 |
| Marital status | ||||||
| Unmarried | −0.477 | −1.949 | 0.052 | −0.472 | −1.900 | 0.059 |
| Divorced | 0.093 | 0.555 | 0.580 | 0.052 | 0.305 | 0.761 |
| Widow | 0.392 | 1.489 | 0.138 | 0.477 | 1.789 | 0.075 |
| Number of children | ||||||
| No children | −0.019 | −0.158 | 0.875 | 0.013 | 0.101 | 0.920 |
| One or two children | 0.055 | 0.592 | 0.554 | 0.077 | 0.812 | 0.418 |
| Three or four children | −0.078 | −0.967 | 0.335 | −0.076 | −0.917 | 0.360 |
| BMI | 0.372 | 1.047 | 0.296 | |||
| WHR | −0.085 | −1.086 | 0.279 | |||
| WSR | −0.229 | −0.670 | 0.504 | |||
| R 2 | 0.067 | 0.081 | ||||
| Adjusted R 2 | 0.015 | 0.015 | ||||
| p | 0.222 | 0.245 | ||||
Model 1: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married) and number of children (none/one or two/three or four/more than four). Model 2: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married), number of children (none/one or two/three or four/more than four). BMI, WHR and WSR.
Abbreviations: β, regression coefficient; BMI, body mass index; WHR, waist–hip ratio; WSR, waist–stature ratio.
TABLE 6.
Predictors of well‐being: results of multivariate regression analysis
| Predictor variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Age | −0.011 | −0.117 | 0.907 | 0.036 | 0.360 | 0.719 |
| Migrant status (native‐born) | 0.253 | 2.761 | 0.006 | 0.281 | 3.020 | 0.003 |
| Educational level | ||||||
| None | 0.101 | 0.700 | 0.485 | 0.136 | 0.939 | 0.349 |
| Primary | −0.086 | −0.740 | 0.460 | −0.050 | −0.425 | 0.671 |
| Junior high | 0.096 | 0.872 | 0.384 | 0.109 | 0.984 | 0.326 |
| High school | −0.099 | −0.942 | 0.347 | −0.155 | −1.439 | 0.152 |
| Work status (unemployed) | 0.067 | 0.750 | 0.454 | 0.065 | 0.726 | 0.469 |
| Marital status | ||||||
| Unmarried | 0.203 | 0.839 | 0.403 | 0.293 | 1.206 | 0.229 |
| Divorced | 0.134 | 0.806 | 0.421 | 0.110 | 0.659 | 0.511 |
| Widow | −0.294 | −1.132 | 0.259 | −0.323 | −1.238 | 0.217 |
| Number of children | ||||||
| No children | 0.121 | 0.996 | 0.320 | 0.055 | 0.442 | 0.659 |
| One or two children | 0.068 | 0.745 | 0.457 | 0.057 | 0.613 | 0.540 |
| Three or four children | 0.162 | 2.028 | 0.044 | 0.143 | 1.775 | 0.077 |
| BMI | 0.467 | 1.338 | 0.182 | |||
| WHR | −0.170 | −2.242 | 0.026 | |||
| WSR | −0.493 | −1.467 | 0.144 | |||
| R 2 | 0.087 | 0.120 | ||||
| Adjusted R 2 | 0.036 | 0.057 | ||||
| p | 0.061 | 0.021 | ||||
Model 1: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married) and number of children (none/one or two/three or four/more than four). Model 2: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married), number of children (none/one or two/three or four/more than four). BMI, WHR and WSR.
Abbreviations: β, regression coefficient; BMI, body mass index; WHR, waist–hip ratio; WSR, waist–stature ratio.
TABLE 7.
Predictors of discomfort: results of multivariate regression analysis
| Predictor variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Age | 0.085 | 0.977 | 0.330 | 0.050 | 0.534 | 0.594 |
| Migrant status (native‐born) | 0.147 | 1.698 | 0.091 | 0.121 | 1.363 | 0.174 |
| Educational level | ||||||
| None | 0.288 | 2.159 | 0.032 | 0.317 | 2.333 | 0.021 |
| Primary | −0.079 | −0.740 | 0.460 | −0.089 | −0.809 | 0.419 |
| Junior high | 0.208 | 2.033 | 0.043 | 0.177 | 1.693 | 0.092 |
| High school | −0.143 | −1.451 | 0.148 | −0.144 | −1.422 | 0.156 |
| Work status (unemployed) | −0.047 | −0.573 | 0.568 | −0.069 | −0.820 | 0.413 |
| Marital status | ||||||
| Unmarried | −0.073 | −0.321 | 0.749 | −0.075 | −0.328 | 0.743 |
| Divorced | 0.120 | 0.772 | 0.441 | 0.100 | 0.638 | 0.524 |
| Widow | −0.004 | −0.019 | 0.985 | 0.053 | 0.219 | 0.827 |
| Number of children | ||||||
| No children | −0.247 | −2.312 | 0.022 | −0.223 | −2.038 | 0.043 |
| One or two children | −0.105 | −1.316 | 0.189 | −0.087 | −1.075 | 0.283 |
| Three or four children | −0.160 | −2.283 | 0.023 | −0.163 | −2.287 | 0.023 |
| BMI | 0.213 | 0.641 | 0.522 | |||
| WHR | 0.009 | 0.123 | 0.902 | |||
| WSR | −0.077 | −0.241 | 0.810 | |||
| R 2 | 0.190 | 0.202 | ||||
| Adjusted R 2 | 0.145 | 0.146 | ||||
| p | 0.000 | 0.000 | ||||
Model 1: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married) and number of children (none/one or two/three or four/more than four). Model 2: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married), number of children (none/one or two/three or four/more than four). BMI, WHR and WSR.
Abbreviations: β, regression coefficient; BMI, body mass index; WHR, waist–hip ratio; WSR, waist–stature ratio.
TABLE 8.
Predictors of quality of life: results of multivariate regression analysis
| Predictor variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Age | −0.067 | −0.720 | 0.472 | −0.033 | −0.328 | 0.743 |
| Migrant status (native‐born) | −0.182 | −1.974 | 0.050 | −0.176 | −1.870 | 0.063 |
| Educational level | ||||||
| None | −0.075 | −0.517 | 0.606 | −0.085 | −0.577 | 0.565 |
| Primary | −0.050 | −0.430 | 0.667 | −0.055 | −0.468 | 0.640 |
| Junior high | −0.116 | −1.059 | 0.291 | −0.062 | −0.556 | 0.578 |
| High school | 0.058 | 0.545 | 0.586 | 0.023 | 0.208 | 0.836 |
| Work status (unemployed) | 0.060 | 0.684 | 0.495 | 0.046 | 0.518 | 0.605 |
| Marital status | ||||||
| Unmarried | 0.168 | 0.701 | 0.484 | 0.185 | 0.764 | 0.446 |
| Divorced | −0.171 | −1.039 | 0.300 | −0.189 | −1.137 | 0.257 |
| Widow | −0.133 | −0.523 | 0.601 | −0.155 | −0.607 | 0.544 |
| Number of children | ||||||
| No children | 0.040 | 0.358 | 0.721 | −0.006 | −0.055 | 0.956 |
| One or two children | 0.003 | 0.032 | 0.974 | −0.011 | −0.131 | 0.896 |
| Three or four children | 0.026 | 0.355 | 0.723 | 0.011 | 0.152 | 0.879 |
| BMI | 0.274 | 0.774 | 0.440 | |||
| WHR | −0.091 | −1.206 | 0.229 | |||
| WSR | −0.359 | −1.055 | 0.293 | |||
| R 2 | 0.097 | 0.117 | ||||
| Adjusted R 2 | 0.046 | 0.054 | ||||
| p | 0.029 | 0.026 | ||||
Model 1: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married) and number of children (none/one or two/three or four/more than four). Model 2: Adjusted for socio‐demographic factors: age, migrant status (native‐born/migrant), educational level (none/primary/junior high/high school/university), work status (unemployed/employed‐student), marital status (unmarried/divorced/widowed/married), number of children (none/one or two/three or four/more than four). BMI, WHR and WSR.
Abbreviations: β, regression coefficient; BMI, body mass index; WHR, waist–hip ratio; WSR, waist–stature ratio.
Both models testing for endogenous stress (Table 5) are not significant, and the second model accounts for only 1.5% of the variance. Moreover, none of the independent variables proved to be a statistically significant explanatory variable of endogenous stress. As regards well‐being (Table 6), the first model does not lead to a significant R 2, but the migrant status and number of children are significantly associated with well‐being: being resident and having three or four children are positive explanatory variables of well‐being. After adding the biological characteristics, the second model is significant with a total explained variance of 6%. Beyond migrant status, WHR is negatively correlated with well‐being. Educational level and the number of children are the most predictive variables of discomfort in both models (Table 7). Being only a junior high school graduate (first model) and being illiterate (both models) are positively associated with discomfort, whereas the number of children is negatively associated with discomfort in both models: having more children decreases the perceived discomfort. Adding the biological variables does not make the second model more predictive. The first model explains 15% of the variance and the second 16%; both of them have highly significant R 2.
Being a resident is negatively associated with perceived quality of life (Table 8) in the first model, meaning that migrants perceive a better quality of life than residents. In the second model, there is a slight increase in R 2 but none of the variables is significantly associated with quality of life. More generally, the two models are significant with an explained variance of 5%.
4. DISCUSSION
This study aimed to analyse the psychosocial well‐being of NA resident women in comparison with a sample of NA women who emigrated to Italy. We successively used multiple regression models to identify the socio‐demographic and biological explanatory variables of the four dimensions of psychological well‐being. Moreover, we tested the psychometric properties of the five items of the psychosocial questionnaire administered to the NA residents.
Cronbach's alpha coefficient tested for the whole questionnaire was high, indicating the questionnaire's good reliability. The fact that some questions showed poor or negative correlations with the others was because most of them were meant to assess positive mental health outcomes (perceived well‐being and quality of life) while the others evaluated negative outcomes (stress and discomfort).
The comparison of the socio‐demographic characteristics between the NA migrants and residents showed that the latter had a significantly higher educational level, most being employed or students, and had fewer children. The difference in employment between the resident and migrant women could be also related to greater difficulties in gaining recognition for skills acquired abroad and discrimination faced by migrants in the labour market, which could lead them to accept lower‐wage jobs and harder working conditions or to experience unemployment or hardship episodes more frequently (Moullan & Jusot, 2014). Moreover, most of the migrant women were married. As we found in a previous study (Toselli et al., 2018), one of the main reasons for the migration of the examined sample of women is family reunification, followed by the search for a job. It is also clear from the literature (Levecque et al., 2009) that the relationships between relatives have a significant impact in activating the migration process. In particular, an Italian demographic study, based on a recent survey conducted by the Italian Institute of Statistics (ISTAT) on a wide sample of resident families with at least one member born abroad, showed a continuous increase in the family reunification process over 15 years (Barbiano di Belgiojoso & Terzera, 2018). The results for the socio‐economic characteristics of NA residents were following the changing role of women in the modernising Arab culture (Eloul et al., 2009). In the past, NA women had the role of maintaining and supporting cultural values and they were mostly responsible for domestic affairs; hence, unemployment suited this role. Being single or being financially independent may contrast with the NA cultural values linked to the family (Toselli et al., 2018). The progress has led to an improvement of the social and economic conditions of African women (Klaa, 2020). Nevertheless, many major social and economic challenges remain today that prevent African women from being enabled, since they still face obstacles and challenges to their participation and economic empowerment. According to Klaa (2020), there are still major social issues of unequal sharing of family levels between men and women, where women are expected to take on the bulk of childcare and family responsibilities, due to the stereotypical portrayal of the social role or social status of women in African societies.
Migrants showed higher adiposity indices than the residents of their home country except for WHR, which did not differ between groups but was above the cut‐off in both the subsamples (WHO, 2008), indicating an excess of central adiposity. Mean BMI values were lower in NA residents, who were mostly normal weight, although this sample had high frequencies of overweight/obese women. These results are in accordance with the review of Toselli et al. (2016) reporting a lower weight status in NAs than in African immigrants in the European Union (EU), albeit above the cut‐off for overweight in both groups. Moreover, the higher frequencies of weight disorders in the NA immigrant women than in the residents agree with the results of other studies conducted in Italy (Casali et al., 2015; Maqoud et al., 2016; Toselli et al., 2014). In particular, Casali et al. (2015) reported a weight gain in more than 60% of African women after immigration. This increase in weight was associated not only with age and lower education level (Casali et al., 2015) but also with the length of residence (Toselli et al., 2019). In general, NA migrants experience more stressful events than NA residents, given that migration has a great impact on psychological distress and anxiety, as suggested by literature (Dunlavy & Rostila, 2013; Lofors et al., 2006; Taloyan et al., 2008; Toselli et al., 2018; Uppaluri et al., 2001); however, in the present study, the perceived stress and discomfort were the same in the two groups. Nevertheless, even though they felt lower well‐being, the migrants reported a higher quality of life than residents, indicating that they considered migration an improvement of their living conditions.
The differences in socio‐demographic variables between migrants and non‐migrants, such as the presumed different expectations linked to the different educational qualifications and family responsibilities, may have influenced the results of the psychosocial variables. Regarding the well‐being of migrant women, some authors (Leopold et al., 2017; Paul & Moser, 2009; Wanberg, 2012) have reported that unemployment causes substantial and long‐term declines in subjective well‐being and other outcomes, such as mental and physical health. Most notably, migrants could carry high expectations of socio‐economic success in their host country (Bartram, 2011; Boneva & Frieze, 2001). The discrepancy between achievement and expectation could contribute to high rates of psychosis (Reininghaus et al., 2008). On the other side, the poorer quality of life perceived by NA residents could be connected to what was reported by Eloul et al. (2009). According to them, the higher rate of depression of these women has to do with the changing role of women in the modernising Arab culture and the stress of the conflict between their role as the centre of the family in the home and the modern necessity of participating in the workforce.
These results are confirmed by the multiple regression models performed in the current study: the main explanatory variable of well‐being and quality of life was migrant status. Being a resident was positively correlated with well‐being, but the quality of life increased with migration. On the other hand, the main explanatory variables of negative outcomes were marital status, educational level and the number of children. Being unmarried decreased the perceived stress while having no children and being illiterate or poorly educated increased the discomfort.
Residents showed a higher prevalence of unmarried women, a condition related to a lower stress level. The women in this condition probably feel that they bear fewer family responsibilities and have higher freedom of choice. In the EU’s Mediterranean countries, social patterns have evolved and women now are strongly present in the labour market and have become financially independent. Nevertheless, inequalities persist, and women are more likely than men to take up part‐time jobs or interrupt their careers altogether to care for children or sick parents (Talani & Giusti, 2017). Thus, work conditions are easier for unmarried women.
The fact that having no children increases discomfort could be related to the role of the woman in the EMR. The desire of many young women to become a mother may be influenced by the high consideration attributed to children by the society within the family framework. Thus, infertile and childless women in Africa are confronted with social discrimination and stigmatisation which may lead to emotional problems such as anxiety and depression (Yakout et al., 2011). Only a few studies, with conflicting results, considered the relationships between the number of children and the migration distress of women. In some communities, due to a positive orientation of women towards motherhood, the presence of children in the household is associated with a lower level of distress. However, it is possible that emotional and financial strain counterbalances and diminishes any salutary effects that motherhood may have for migrants. The responsibility to have children before full adaptation to the new environment can increase levels of distress for migrants (Toselli et al., 2018). Urzúa et al. (2016) reported that about 50% of the migrants in their study had elevated levels of life discomfort, with mental health problems derived from their adjustment to social roles and relationships. In addition, they found a high correlation between acculturation stress levels and the severity of mental health symptoms.
Anthropometric traits, in particular central adiposity (WHR), were significant explanatory variables only of well‐being (negative correlation) in NA women. Weight status and body image are influenced by environmental, cultural and behavioural factors (Demarest & Allen, 2000; Gualdi‐Russo et al., 2016; Tovée et al., 2006). Although there is a certain variability in the ideal body image in Africa (Toselli et al., 2016), an ancestral ideal of female beauty (curvy figure) is still present, especially in people experiencing low socio‐economic status and isolation (Faber & Kruger, 2005; Gualdi‐Russo, 2018). Meanings associated with being overweight and obese in African populations are described in the literature (Meko & Nel, 2021; Puoane et al., 2012). In African society, overweight is often seen as culturally desirable, denoting beauty, affluence, and prosperity, and absence of the acquired immunodeficiency syndrome virus (Kruger et al., 2018; Meko & Nel, 2021; Puoane et al., 2012). However, a women's change in perceptions of ‘beauty’ has been found in some African populations. Benkeser et al. (2012) reported that women who spent the first 12 years of their childhood in an urban environment were at increased risk for overweight and obesity and at a decreased risk for desiring to be heavier. This finding seems to suggest there may be some credence to the westernisation and urbanisation hypotheses. In addition, according to Gitau et al. (2014), the younger generation of black girls now aims for slimmer body sizes, as influenced by the Western view of beauty.
The main strength of this study is to provide data on the psychosocial well‐being of NA female residents, for which knowledge is very limited (Brook et al., 2011; van Schalkwyk & Wissing, 2010), and on possible explanatory variables of discomfort, allowing us to assess both positive and negative psychosocial health outcomes.
This study has several limitations that may have influenced the interpretation and generalisation of the results. First, this is a cross‐sectional study. Second, caution should be taken in generalising the results to all NA women because of the potential sampling biases. Furthermore, while we are aware that the examined NA residents were living in large NA cities, we do not know whether the NA migrants came from urban or rural environments. Finally, we do not have any information about the psychosocial situation of the women used as a comparison prior to migration.
In conclusion, the results of the present study showed differences between the two samples of NA women analysed: if on the one hand, we have to pay attention to the perception of the quality of life of non‐immigrant women, trying to support their progress, on the other hand, we must pay attention to the increasing weight status and the perception of psychosocial well‐being of the migrants. The results of the literature relating to these aspects are few and often not very updated or recent, suggesting the need to collect further evidence (Benkeser et al., 2012; Gitau et al., 2014; Meko & Nel, 2021; Toselli et al., 2018). However, this study adds valuable information and maybe a good starting point for health policies as well as for future research both in the EMR and in NA migrants.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
AUTHOR CONTRIBUTION
EG‐R: Study conception & protocol. NR, MK and CL: Data acquisition. NR: Primary analysis. NR, EG‐R and ST: Final analysis and data interpretation. NR, EG‐R and ST: Original manuscript draft. Final manuscript draft: all authors.
ETHICAL STATEMENT
The study was performed in line with the principles of the Declaration of Helsinki. Approval was obtained from the Ethics Committee of Azienda Unità Sanitaria Locale (AUSL), Bologna, Italy. Informed consent was given by all participants prior to their recruitment in the study.
ACKNOWLEDGMENT
The authors would like to thank all participants of this study. Open Access Funding provided by Universita degli Studi di Ferrara within the CRUI‐CARE Agreement.
Rinaldo, N. , Gualdi‐Russo, E. , Khyatti, M. , Lakhoua, C. , & Toselli, S. (2022). Psychosocial health and quality of life among North African women. Health & Social Care in the Community, 30, 1827–1837. 10.1111/hsc.13562
Funding information
This study was supported by the EU 7th Framework Programme 2007–2013 (grant number 260715).
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the authors upon reasonable request.
REFERENCES
- Barbiano di Belgiojoso, E. , & Terzera, L. (2018). Family reunification – Who, when, and how? Family trajectories among migrants in Italy. Demographic Research, 38, 737–772. 10.4054/DemRes.2018.38.28 [DOI] [Google Scholar]
- Bartram, D. (2011). Economic migration and happiness: Comparing immigrants’ and natives’ happiness gains from income. Social Indicators Research, 103(1), 57–76. 10.1007/s11205-010-9696-2 [DOI] [Google Scholar]
- Benkeser, R. M. , Biritwum, R. , & Hill, A. G. (2012). Prevalence of overweight and obesity and perception of healthy and desirable body size in urban Ghanaian women. Ghana Medical Journal, 46(2), 66–75. [PMC free article] [PubMed] [Google Scholar]
- Blanchet, K. , Ramesh, A. , Frison, S. , Warren, E. , Hossain, M. , Smith, J. , Knight, A. , Post, N. , Lewis, C. , Woodward, A. , Dahab, M. , Ruby, A. , Sistenich, V. , Pantuliano, S. , & Roberts, B. (2017). Evidence on public health interventions in humanitarian crises. The Lancet, 390(10109), 2287–2296. 10.1016/S0140-6736(16)30768-1 [DOI] [PubMed] [Google Scholar]
- Boneva, B. S. , & Frieze, H. I. (2001). Toward a concept of a migrant personality. Journal of Social Issues, 57(3), 477–491. 10.1111/0022-4537.00224 [DOI] [Google Scholar]
- Brook, D. W. , Rubenstone, E. , Zhang, C. , Morojele, N. K. , & Brook, J. S. (2011). Environmental stressors, low well‐being, smoking, and alcohol use among South African adolescents. Social Science & Medicine, 72(9), 1447–1453. 10.1016/j.socscimed.2011.02.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casali, M. E. , Borsari, L. , Marches, I. , Borella, P. , & Bargellini, A. (2015). Lifestyle and food habits changes after migration: A focus on immigrant women in Modena (Italy). Annali di Igiene: Medicina Preventiva e di Comunità, 27, 748–759. [DOI] [PubMed] [Google Scholar]
- Demarest, J. , & Allen, R. (2000). Body image: Gender, ethnic, and age differences. The Journal of Social Psychology, 140, 465–472. 10.1080/00224540009600485 [DOI] [PubMed] [Google Scholar]
- Dunlavy, A. C. , & Rostila, M. (2013). Health inequalities among workers with a foreign background in Sweden: Do working conditions matter? International Journal of Environmental Research and Public Health, 10(7), 2871–2887. 10.3390/ijerph10072871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eloul, L. , Ambusaidi, A. , & Al‐Adawi, S. (2009). Silent Epidemic of Depression in Women in the Middle East and North Africa Region Emerging tribulation or fallacy? Sultan Qaboos University Medical Journal, 9(1), 5–15. [PMC free article] [PubMed] [Google Scholar]
- Faber, M. , & Kruger, H. S. (2005). Dietary intake, perceptions regarding body weight, and attitudes toward weight control of normal weight, overweight, and obese black females in a rural village in South Africa. Ethnicity and Disease, 15, 238–245. [PubMed] [Google Scholar]
- Ferrari, A. J. , Charlson, F. J. , Norman, R. E. , Patten, S. B. , Freedman, G. , Murray, C. J. , Vos, T. , & Whiteford, H. A. (2013). Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Medicine, 10(11), e1001547. 10.1371/journal.pmed.1001547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gitau, T. M. , Micklesfield, L. K. , Pettifor, J. M. , & Norris, S. A. (2014). Eating attitudes, body image satisfaction and self‐esteem of South African black and white male adolescents and their perception of female body silhouettes. Journal of Child & Adolescent Mental Health, 6(3), 193–205. 10.2989/17280583.2014.901224 [DOI] [PubMed] [Google Scholar]
- Gualdi‐Russo, E. (2018). Body image perception in ethnic minorities: Implications for prevention. In Modesti P. A., Cappuccio F. P., & Parati G. (Eds.), Ethnic diversities, hypertension and global cardiovascular risk (pp. 201–206). Springer International Publishing AG. [Google Scholar]
- Gualdi‐Russo, E. , Rinaldo, N. , Khyatti, M. , Lakhoua, C. , & Toselli, S. (2016). Weight status, fatness and body image perception of North African immigrant women in Italy. Public Health Nutrition, 19(15), 2743–2751. 10.1017/S1368980016000872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamali, M. , Munyuzangabo, M. , Siddiqui, F. J. , Gaffey, M. F. , Meteke, S. , Als, D. , Jain, R. P. , Radhakrishnan, A. , Shah, S. , Ataullahjan, A. , & Bhutta, Z. A. (2020). Delivering mental health and psychosocial support interventions to women and children in conflict settings: A systematic review. BMJ Global Health, 5(3), e002014. 10.1136/bmjgh-2019-002014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klaa, C. (2020). Role of African women in development and economic life: Reality and challenges. International Journal of Inspiration & Resilience Economy, 4(1), 1–9. [Google Scholar]
- Koller, M. , Aaronson, N. K. , Blazeby, J. , Bottomley, A. , Dewolf, L. , Fayers, P. , Johnson, C. , Ramage, J. , Scott, N. , West, K. ; EORTC Quality of Life Group . (2007). Translation procedures for standardised quality of life questionnaires: The European Organisation for Research and Treatment of Cancer (EORTC) approach. European Journal of Cancer, 43(12), 1810–1820. 10.1016/j.ejca.2007.05.029 [DOI] [PubMed] [Google Scholar]
- Kruger, H. S. , Seru, T. , Mchiza, Z. J. , & Speakman, J. R. (2018). The relationship between female adiposity and physical attractiveness amongst adults in rural Ranaka village, Botswana. South African Journal of Clinical Nutrition, 33(1), 17–22. 10.1080/16070658.2018.1502909 [DOI] [Google Scholar]
- Leopold, L. , Leopold, T. , & Lechner, C. M. (2017). Do immigrants suffer more from job loss? Unemployment and subjective well‐being in Germany. Demography, 54(1), 231–257. 10.1007/s13524-016-0539-x [DOI] [PubMed] [Google Scholar]
- Levecque, K. , Lodewyckx, I. , & Bracke, P. (2009). Psychological distress, depression and generalised anxiety in Turkish and Moroccan immigrants in Belgium. A general population study. Social Psychiatry and Psychiatric Epidemiology, 44(3), 188–197. 10.1007/s00127-008-0431-0 [DOI] [PubMed] [Google Scholar]
- Lofors, J. , Ramírez‐León, V. , & Sundquist, K. (2006). Neighbourhood income and anxiety: A study based on random samples of the Swedish population. European Journal of Public Health, 16(6), 633–639. 10.1093/eurpub/ckl026 [DOI] [PubMed] [Google Scholar]
- Lohman, T. G. , Roche, A. F. , & Martorell, R. (1997). Manuale di riferimento per la standardizzazione antropometrica. EDRA Medical Publishing & New Media. [Google Scholar]
- Maqoud, F. , Vacca, E. , & Tommaseo‐Ponzetta, M. (2016). From Morocco to Italy: How women's bodies reflect their change of residence. Collegium Antropologicum, 40(1), 9–15. [PubMed] [Google Scholar]
- Meko, N. L. , & Nel, M. (2021). Body satisfaction of female staff members working in primary schools in Mangaung, Bloemfontein. Health SA, 26, 1555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mokdad, A. H. , Forouzanfar, M. H. , Daoud, F. , Mokdad, A. A. , El Bcheraoui, C. , Moradi‐Lakeh, M. , Kyu, H. H. , Barber, R. M. , Wagner, J. , Cercy, K. , Kravitz, H. , Coggeshall, M. , Chew, A. , O'Rourke, K. F. , Steiner, C. , Tuffaha, M. , Charara, R. , Al‐Ghamdi, E. A. , Adi, Y. , … Murray, C. J. L. (2016). Global burden of diseases, injuries, and risk factors for young people's health during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet, 387(10036), 2383–2401. 10.1016/S0140-6736(16)00648-6 [DOI] [PubMed] [Google Scholar]
- Moullan, Y. , & Jusot, F. (2014). Why is the 'healthy immigrant effect' different between European countries? The European Journal of Public Health, 24(Suppl. 1), 80–86. 10.1093/eurpub/cku112 [DOI] [PubMed] [Google Scholar]
- Paul, K. I. , & Moser, K. (2009). Unemployment impairs mental health: Meta‐analysis. Journal of Vocational Behaviour, 74, 264–282. 10.1016/j.jvb.2009.01.001 [DOI] [Google Scholar]
- Puoane, T. R. , Tsolekile, L. , Igumbor, E. U. , & Fourie, J. M. (2012). Experiences in developing and implementing health clubs to reduce hypertension risk among adults in a South African population in transition. International Journal of Hypertension, 2012, 913960. 10.1155/2012/913960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ravindranath, V. , Dang, H. M. , Goya, R. G. , Mansour, H. , Nimgaonkar, V. L. , Russell, V. A. , & Xin, Y. (2015). Regional research priorities in brain and nervous system disorders. Nature, 527(7578), S198–S206. 10.1038/nature16036 [DOI] [PubMed] [Google Scholar]
- Reininghaus, U. A. , Morgan, C. , Simpson, J. , Dazzan, P. , Morgan, K. , Doody, G. A. , Bhugra, D. , Leff, J. , Jones, P. , Murray, R. , Fearon, P. , & Craig, T. K. (2008). Unemployment, social isolation, achievement‐expectation mismatch and psychosis: Findings from the AESOP study. Social Psychiatry and Psychiatric Epidemiology, 43, 743–751. [DOI] [PubMed] [Google Scholar]
- Talani, L. S. , & Giusti, S. (2017). Women in the mediterranean: Still discriminated against? Journal of Balkan and Near Eastern Studies, 19(5), 461–463. 10.1080/19448953.2017.1296253 [DOI] [Google Scholar]
- Taloyan, M. , Johansson, S. E. , Sundquist, J. , Koctürk, T. O. , & Johansson, L. M. (2008). Psychological distress among Kurdish immigrants in Sweden. Scandinavian Journal of Public Health, 36(2), 190–196. 10.1177/1403494807085077 [DOI] [PubMed] [Google Scholar]
- Toselli, S. , & Gualdi‐Russo, E. (2008). Psychosocial indicators and distress in immigrants living in Italian reception centres. Stress and Health, 24(4), 327–334. 10.1002/smi.1195 [DOI] [Google Scholar]
- Toselli, S. , Gualdi‐Russo, E. , Marzouk, D. , Sundquist, J. , & Sundquist, K. (2014). Psychosocial health among immigrants in central and southern Europe. European Journal of Public Health, 24(Suppl. 1), 26–30. 10.1093/eurpub/cku100 [DOI] [PubMed] [Google Scholar]
- Toselli, S. , Rinaldo, N. , Caccialupi, M. G. , & Gualdi‐Russo, E. (2018). Psychosocial indicators in North African immigrant women in Italy. Journal of Immigrant and Minority Health, 20(2), 431–440. 10.1007/s10903-017-0562-z [DOI] [PubMed] [Google Scholar]
- Toselli, S. , Rinaldo, N. , & Gualdi‐Russo, E. (2016). Body image perception of African immigrants in Europe. Globalization and Health, 12, 48. 10.1186/s12992-016-0184-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toselli, S. , Rinaldo, N. , & Gualdi‐Russo, E. (2019). Length of residence and obesity risk among North African immigrant women in Italy. Economics & Human Biology, 19, 74–79. 10.1016/j.ehb.2019.03.008 [DOI] [PubMed] [Google Scholar]
- Tovée, M. J. , Swami, V. , Furnham, A. , & Mangalparsad, R. (2006). Changing perceptions of attractiveness as observers are exposed to a different culture. Evolution and Human Behavior, 27, 443–456. 10.1016/j.evolhumbehav.2006.05.004 [DOI] [Google Scholar]
- Uppaluri, C. R. , Schumm, L. P. , & Lauderdale, D. S. (2001). Self‐reports of stress in Asian immigrants: Effects of ethnicity and acculturation. Ethnicity and Disease, 11(1), 107–114. [PubMed] [Google Scholar]
- Urzúa, M. A. , Heredia, B. O. , & Caqueo‐Urízar, A. (2016). Mental health and stress by acculturation in immigrants from South America in northern Chile. Revista Medica de Chile, 144(5), 563–570. [DOI] [PubMed] [Google Scholar]
- van Schalkwyk, I. , & Wissing, M. P. (2010). Psychosocial well‐being in a group of South African adolescents. Journal of Psychology in Africa, 20(1), 53–60. 10.1080/14330237.2010.10820342 [DOI] [Google Scholar]
- Wanberg, C. R. (2012). The individual experience of unemployment. Annual Review of Psychology, 63, 369–396. 10.1146/annurev-psych-120710-100500 [DOI] [PubMed] [Google Scholar]
- Weiner, J. S. , & Lourie, J. A. (1981). Practical human biology. Academic Press. [Google Scholar]
- World Health Organization (WHO) . (2008). Waist circumference and waist‐hip ratio: Report of a WHO expert consultation, Geneva, 8–11 December 2008. Retrieved January 24, 2020, from https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf;jsessionid=F2ACF2189A495F5301930AF3E0DF7D10?sequence=1 [Google Scholar]
- World Health Organization (WHO) . (2012–2016). Strategy for mental health and substance abuse in the Eastern Mediterranean Region 2012–2016. Technical paper August 2011. Retrieved February 3, 2020, from http://applications.emro.who.int/docs/RC_technical_papers_2011_5_14223.pdf [Google Scholar]
- Yakout, S. M. , Kamal, S. M. , & Moawed, S. (2011). Menopausal symptoms and quality of life among Saudi women in Riyadh and Taif. Journal of American Science, 7(5), 778–782. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the authors upon reasonable request.