

Abstract
Background
Emerging evidence suggests that distant placements and multiple moves may be detrimental to young people in care settings. Less is known about the characteristics of young people in secure care most affected by these processes.
Aims
This study examined distance from home and number of previous placements in English young people detained in secure care and their relationships with organisational and individual characteristics.
Methods
Data were derived from the (2016) cross‐sectional National Adolescent Study census of English young people in secure care, which included 1322 young people across secure mental health, welfare and Youth Justice establishments. Associations were described with odds ratios/95% confidence intervals (OR/CI).
Results
Overall, 285 young people (26.4%) were in secure placements over 100 miles from their family/local authority while 54 (5.6%) had 10 or more previous placements. These rates were higher in secure welfare than other settings (73.8%; OR (CI) = 9.62 (5.72, 16.18), 12.7%; OR (CI) = 2.76 (1.29, 5.91) respectively), and there was significant overlap between long‐distance placement and multiple placements (n = 22; OR (CI) = 2.26 (1.27, 4.04)). Younger age and presence of neurodevelopmental disorder were also associated with long‐distance placements while psychiatric diagnosis, previous secure placement, and previous service contact were linked to multiple placements.
Conclusions
Distant and/or multiple placements in young people in secure care appear common, particularly for those who are placed in secure welfare and who are younger and/or present with a psychiatric disorder. Multi‐agency evaluations that capture the longitudinal experience of these vulnerable young people are needed to understand how undesirable patterns of placement in secure care occur and prevent future instances.
Keywords: children and young people, mental health, secure care, welfare, youth justice
1. INTRODUCTION
The National Adolescent Study (NAS) census of secure care of English children and young people (CYP; Hales et al., 2018) found that 1 in 20 young people in secure care had been in 10 or more placements. Many young people were not located in their county of origin and were placed in secure units far away from home. Parents and professionals involved with the young people in secure care expressed concern that many were institutionalised far from home, disrupting ties with family and friends and complicating contact with supporting professionals. Interviewees complained about multiple moves and said young people were left with problems reintegrating into their home areas (Bartlett et al., 2018). Both distant placements and multiple moves seem likely to exacerbate the young person's (YP's) difficulties.
Distance from home issues also apply to non‐secure care of CYP, raising practical and psychological issues for child welfare. Children in care far from home (Children's Commissioner, 2019) point to the fracturing of familial and friendship bonds, difficulties contacting professionals from their own areas and an inability to continue either therapy or school easily. Similarly, children needing mental health care as inpatients are often sent long distances to access it. Such placements are considered to affect recovery adversely, decrease the chances of local services being able to help them and possibly increase the risk of suicide (Owen, 2018). In secure care, problems linked to distant placements may be particularly extreme by virtue of less access to life outside the institution and more restrictions within it. Over two‐thirds of young people in custody in England and Wales re‐offend within 12 months of release (Ministry of Justice, 2019), which is perhaps unsurprising considering resettlement of children from custody is badly planned with late provision of ongoing accommodation, health services and a plan for educational and training needs (HM Inspectorate of Probation and HM Inspectorate of Prisons, 2019). As the Inspectorates note, however, ineffective resettlement is understandable because so many children are imprisoned far from home.
In addition, multiple moves inflicted on young people who are already vulnerable highlight the mismatch between aspects of our current care system and what promotes healthy child development. By their very nature, multiple moves compromise consistent care, regardless of the care provider. The importance of consistent care in childhood has been recognised since Bowlby's (1944) original work on attachment difficulties in young offenders. Systematic review (Hoeve et al., 2012) evidence supports a relationship, based on 74 studies and over 55,000 participants, between poor attachment and juvenile delinquency, and there is a relationship between attachment insecurity and later mental health problems (Mikulincer & Shaver, 2012). A recent report (Hill et al., 2019) on a secure hospital adolescent population with multiple placements pre‐hospitalisation, neglect, abuse and inadequate parenting suggested all were risks for attachment disorder.
It is well known that young people in the different types of secure care have high rates of early trauma (Briggs et al., 2012; Hill et al., 2019; Stewart et al., 2020; Wright et al., 2016) and high rates of mental health difficulties (Fazel et al., 2008; Ford et al., 2007; Hill et al., 2014; Hill et al., 2016). Recent Scottish data shows that young people entering any kind of secure care are most likely to come from deprived households in poor areas and are much more likely than peers in the general population to have experienced several adverse childhood events (Gibson, 2020). The number of adverse events appears linked to the relative risk of subsequent violence to others and serious psychological problems but researching the timing, duration and degree of adverse events makes the interpretation of their significance difficult (Nelson et al., 2020).
This complex body of work explores relationships between adverse child events, social deprivation, attachment, mental health problems and delinquency in different ways, but does not establish the characteristics of young people in the secure care system most affected by the related processes of multiple moves and/or distant placement. This is important as the evidence above suggests both processes could be detrimental, especially to already troubled and disadvantaged young people.
The aim of this paper is to interrogate the NAS data (Hales et al., 2018) further to:
establish the relationship of distance from home and multiple placements to the legislative framework under which young people are detained;
examine whether or not YP who are far from home are also likely to have experienced multiple placements;
examine the individual characteristics of these two groups to establish potential related vulnerabilities; and
seek to establish whether there is a relationship between area of origin and placement pattern.
2. METHODS
Young people in England and Wales can be held in secure settings under three different types of legislation in units funded by Local Authorities (LAs; Welfare), NHS England (NHSE; secure mental health hospitals) and Youth Justice Services (YJS). English young people may also be detained in facilities in Scotland or Wales. The data analysed in this paper were obtained as part of the NAS study census undertaken in 2016 (Hales et al., 2018). Full details of methods employed, data collection and initial data analysis are provided in Appendix B of that report.
The following information is relevant to this paper: data were sought on a census day in September 2016 on all 1322 English young people either detained in secure placements in England (n = 1260, 95.3%) or detained in other UK jurisdictions (n = 62, 4.7%). Data (anonymised at extraction) were sourced from questionnaires completed either by unit clinicians, care workers for the young people on their caseload or a member of the study team reviewing clinical notes. The data set included information on gender, age, ethnicity, legislation under which detained, previous secure and open placements (number and type), contact with community services, mental and physical health needs, risk profile and area of origin. The varied nature of the units meant that data was not always obtained through individuals who regularly ascribe diagnoses. HH (Consultant in Adolescent Forensic Psychiatry) reviewed mental health information provided (needs, treatments, diagnoses and risks) and used ICD 10 criteria to suggest primary and other diagnoses.
2.1. Distance from home
Data considered secure care address and address of family or local authority with respect to driving distance between the two (collapsed into ≤50 miles/>50 miles and ≤100 miles/>100 miles) and whether secure care placement was in‐ or out‐of‐family or local authority UK region. For those responses where a specific city, town or (prefix) postcode (n = 983 or 74.4%), or in a smaller number of cases the (ceremonial) county (n = 97 or 7.3%), was provided for address of family or local authority, driving distance from home was calculated based on a postcode in the most central location of the relevant city, town, postcode, or county. There were no differences between young people with and without distance data with respect to legislative framework under which placed, gender, age (≤15 years vs. ≥16 years) or ethnic background (Black, Asian and minority ethnic (BAME) vs. white; for all comparisons, p > 0.137).
2.2. Placement history
Data considered whether a young person was previously placed away from home, had had a previous secure placement and number of previous placements. Missing placement frequency data was disproportionately higher in young people placed in Welfare (33.6%) and YJS (27.5%) settings than in those in hospital (21.2%; χ 2(2) = 7.82, p = 0.020) and in people of BAME (24.0%) compared with white ethnic background (16.6%; χ 2(1) = 8.72, p = 0.003); but gender and age were comparable (for both comparisons, p > 0.052).
2.3. Statistical analyses
Descriptive data is presented using frequencies and percentages. Associations between distance from home/local authority (number of) previous placements, legislative framework under which placed, and sociodemographic and clinical variables were initially examined with Chi‐square and Fisher's exact tests. For those individual‐level variables yielding significant associations, subsequent logistic regression analyses (using Generalised Linear Modelling with a logit link function) were administered for each with legislative framework under which placed as an additional independent factor. Exploratory analyses (Chi‐square and Fisher's exact tests) were also administered to compare differences between young people with ≥10 previous placements currently placed ≤100 miles versus >100 miles from home/local authority. Where multiple tests of association were administered (excluding post‐hoc pairwise comparisons and exploratory analyses), a false discovery rate (FDR) correction was applied to each set of analyses (controlled at level α = 5%; Benjamini & Hochberg, 1995). Otherwise, the criterion for statistical significance was set at p < 0.05. Statistical analyses were performed using SPSS (IBM, Version 26.0).
3. RESULTS
3.1. Distance from home
Overall, more than 1 in 4 (285, 26.4%) young people were in secure placements more than 100 miles from their family or local authority and 62.0% (670) of young persons' secure placements were outside the UK region of their family or local authority.
Both measures used to assess distance from home showed significant differences between the types of legislation used to detain (Table 1; for all comparisons χ 2(2)>26.56, p < 0.001). Out‐of‐area placements and placements >50 miles and >100 miles from home were significantly more frequent, using post‐hoc pair wise comparisons, for those placed under Welfare legislation compared with Mental Health placements and compared with YJS placements (for all comparisons, χ 2(1)>10.49, p < 0.002). The proportions of placements >50 miles and >100 miles from home were higher in Mental Health placements relative to YJS placements (for both comparisons, χ 2(1)>6.01, p < 0.015). The odds of young people in secure Welfare placements being placed outside the region of their family or local authority was more than threefold that of those under other (Mental Health or YJS) legislations (OR = 3.39, 95% CI = 1.85, 6.23), and this increased to more than nine times when considering placement >100 miles from home (OR = 9.62, 95% CI = 5.72, 16.18).
TABLE 1.
Number (percentage) of young persons in secure care placed outside their (UK) region and >50/>100 miles from their family or local authority and with previous placements, according to legislative framework under which placed
| All secure care (n = 1080) | Mental health (n = 254) | Welfare (n = 80) | YJS (n = 746) | |
|---|---|---|---|---|
| Placed outside home region | 670 (62.0) | 162 (63.8) | 67 (83.8) | 441 (59.1) |
| >50 miles from home | 647 (59.9) | 164 (64.6) | 67 (83.8) | 416 (55.8) |
| >100 miles from home | 285 (26.4) | 86 (33.9) | 59 (73.8) | 140 (18.8) |
| n = 1178 | n = 273 | n = 85 | n = 820 | |
|---|---|---|---|---|
| Previous placement (away from home) | 847 (71.9) | 250 (91.6) | 82 (96.5) | 515 (62.8) |
| Previous secure placement | 550 (47.9) | 151 (56.3) | 22 (26.8) | 377 (47.2) |
| Admitted from secure care | 194 (17.3) | 77 (29.6) | 7 (9.0) | 110 (14.0) |
| n = 972 | n = 246 | n = 71 | n = 655 | |
|---|---|---|---|---|
| Number of previous placements | ||||
| 1 | 191 (19.7) | 55 (22.4) | 10 (14.1) | 126 (19.2) |
| 2–3 | 210 (21.6) | 91 (37.0) | 17 (23.9) | 102 (15.6) |
| 4–9 | 186 (19.1) | 66 (26.8) | 32 (45.1) | 88 (13.4) |
| ≥10 | 54 (5.6) | 11 (4.5) | 9 (12.7) | 34 (5.2) |
Note: Overall n for ‘Previous secure placement’ and ‘Admitted from secure’ were 1149 (MH n = 268, Welfare n = 82, YJS n = 799) and 1123 (MH n = 260, Welfare n = 78, YJS n = 785), respectively; Percentages were calculated from available data.
Abbreviation: YJS, Youth Justice System.
3.2. Number and type of previous (secure) placements of young people in secure care
In total, more than 70% of young people had previously been placed away from home, although just under half had previously been placed in secure accommodation (Table 1).
Numbers of previous placements (secure or otherwise) varied widely across young people and significantly differed across legislative frameworks (Table 1; χ 2(2) = 183.86, p < 0.001). Almost 1 in 4 had more than 3 previous placements and 54 young people had 10 or more; those in secure Welfare placements appeared particularly disadvantaged, with 57.8% having more than three previous placements, a higher rate than those placed in hospital (31.3%) or under the YJS (18.6%; for both pairwise comparisons, p < 0.001); the latter two also significantly differed (p < 0.001). Similarly, disproportionately higher numbers of young people in secure Welfare had 10 or more previous placements than those placed under other legislative frameworks (5.0%; χ 2(1) = 7.40, p = 0.007; OR = 2.76, 95% CI = 1.29, 5.91). More than three‐quarters (42, 77.8%) of those who had 10 or more previous placements had also had a previous secure placement, whereas two‐thirds (384, 66.9%; χ 2(1) = 2.68, p = 0.102) of those with one to nine placements had a previous secure placement. The patterns of previous placements (χ 2(2) = 111.28, p < 0.001) and of previous secure placements (χ 2(2) = 22.41, p < 0.001) were significantly different for the three legislative frameworks.
3.3. Relationship of young persons placed far from home and those with multiple placements
There was a significant overlap between those young people with 10 or more previous placements and being placed a long distance from home or local authority (Figure 1). More than 40% (44.0%) of those with ≥10 previous placements were currently placed >100 miles from home, compared to 25.8% of those with 0–9 previous placements (χ 2(1) = 8.00, p = 0.005). After controlling for legislative framework, the odds of being placed more than 100 miles from family home or local authority more than doubled in those young people who had 10 or more previous placements (OR = 2.26, 95% CI = 1.27, 4.04).
FIGURE 1.
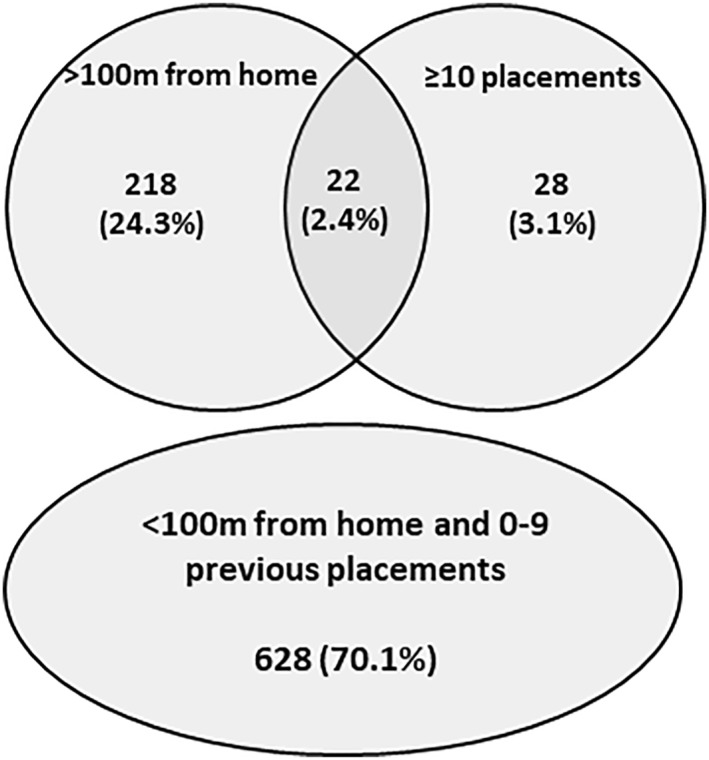
Overlap between young people in secure care >100 miles (>100 m) from home or local authority in current placement and with ≥10 previous placements (n = 896). Values represent frequencies (percentages)
3.4. Individual characteristics of young people associated with long distance from home/local authority and 10 or more previous placements
Given the significant overlap between those placed far from home and those with multiple placements and the fact that there are many young persons who have at least one of these characteristics (n = 268), it is logical to explore degrees of similarity and difference in these three populations. The sociodemographic characteristics, comorbid conditions, assessed risk level (in current placement) and previous contact with relevant services of young people in secure care placed a long way from home/local authority and with 10 or more previous placements are shown in Table 2.
TABLE 2.
Individual characteristics of young people associated with >100 miles from home/local authority and more than 10 previous placements
| ≤100 miles from home (n = 788) | >100 miles from home (n = 283) | >100 miles versus ≤100 miles from home controlling for legislative framework under which placed | 0–9 previous placements (n = 910) | ≥10 previous placements (n = 54) | 0–9 versus ≥ 10 previous placements controlling for legislative framework under which placed | |||
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | OR (CI) | p | n (%) | n (%) | OR (CI) | p | |
| Sociodemographic factors | ||||||||
| Female gender | 146 (18.5) | 102 (36.0)*** | 1.19 (0.78, 1.82) | 0.429 | 219 (24.1) | 13 (24.1) | ||
| Age <16 years | 111 (15.2) | 80 (31.1)*** | 1.51 (1.03, 2.20) | 0.033 | 167 (20.0) | 12 (25.5) | ||
| BAME | 269 (38.3) | 81 (30.6) | 284 (34.4) | 17 (33.3) | ||||
| Comorbidity | ||||||||
| Physical disability | 171 (24.1) | 70 (28.6) | 184 (23.4) | 19 (38.8)* | 1.97 (1.08, 3.60) | 0.028 | ||
| Psychiatric diagnosis | 377 (51.2) | 159 (64.9)*** | 1.27 (0.87, 1.85) | 0.213 | 453 (54.8) | 38 (77.6)** | 3.92 (1.90, 8.10) | <0.001 |
| ≥3 psychiatric diagnoses | 71 (9.6) | 36 (14.7) | 91 (11.0) | 11 (22.4)* | 3.12 (1.43, 6.81) | 0.004 | ||
| NDD | 171 (23.2) | 93 (38.0)*** | 1.77 (1.27, 2.46) | <0.001 | 216 (26.1) | 24 (49.0)*** | 3.01 (1.64, 5.51) | <0.001 |
| Emotional dysregulation | 134 (18.2) | 54 (22.0) | 160 (19.3) | 16 (32.7)* | 2.67 (1.29, 5.53) | 0.008 | ||
| Risk level | ||||||||
| Risk to self | 239 (30.7) | 124 (45.4)*** | 0.92 (0.63, 1.37) | 0.691 | 305 (34.0) | 25 (46.3) | ||
| Risk to others | 238 (30.6) | 131 (48.0)*** | 1.65 (1.21, 2.26) | 0.001 | 319 (35.5) | 22 (40.7) | ||
| Previous secure placement | 361 (47.4) | 138 (51.5) | 384 (42.4) | 42 (77.8)*** | 5.74 (2.92, 11.29) | <0.001 | ||
| Admitted from secure | 113 (15.1) | 73 (27.3)*** | 2.18 (1.53, 3.10) | <0.001 | 157 (18.1) | 8 (15.4) | ||
| Previous service contact | ||||||||
| Social services | 338 (51.6) | 130 (63.1)** | 1.17 (0.83, 1.65) | 0.360 | 323 (45.9) | 49 (96.1)*** | 29.26 (7.00, 122.30) | <0.001 |
| Youth offending team | 508 (75.3) | 153 (64.8)** | 1.14 (0.71, 1.82) | 0.596 | 517 (67.0) | 45 (88.2)** | 6.75 (2.39, 19.10) | <0.001 |
| CAMHS | 381 (49.6) | 165 (63.7)*** | 1.24 (0.88, 1.75) | 0.229 | 458 (52.0) | 42 (82.4)*** | 5.19 (2.42, 11.15) | <0.001 |
Note: n values for groups (≤100 miles from home/>100 miles from home, 0–9 previous placements/≥10 previous placements) varied according to data available for the specific variable of interest – the n values stated are the maximum number in the group available for any variable. Gender data does not consider 6 young people identifying as transgender (n = 5) or intersex (n = 1), 2 of which were placed >100 miles from home (none of which had ≥10 placements). Asterisks indicate significant difference in pairwise comparisons of proportions (from Chi‐square tests): *p < 0.05, **p < 0.01, ***p < 0.001. OR, odds ratio, CI, 95% confidence intervals; OR and associated CI/p values were calculated using separate Generalised Linear Modelling for each variable controlling for legislative framework under which placed. Significant differences and associations are highlighted in bold. BAME, Black, Asian and minority ethnic; CAMHS, Child and Adolescent Mental Health Services; NDD, neurodevelopmental disorder.
Disproportionately more young people who were female, aged 15 years or less, white, with a psychiatric and/or neurodevelopmental (NDD) diagnosis, at risk to themselves and at risk to others, and had previous contact with social services (looked after care plan), Youth offending teams (YOT) and Child and Adolescent Mental Health Services (CAMHS) were placed more than 100 miles from their home or local authority (after FDR correction). However, once legislative framework under which placed was controlled for (see OR (95% CI) and p values on Table 2), only age, presence of a NDD and assessed as a risk to others significantly elevated the associated risk of long‐distance placement (by 50%–80%).
This understanding was refined by subsequent multivariate analysis. This included legislative framework and ≥10 previous placements, age, presence of a NDD and being assessed as a risk to others as independent variables and distance from home/local authority as the dependent variable. Being aged 15 years or less (OR = 1.62, 95% CI = 1.04, 2.53, p = 0.033) and the presence of a NDD (OR = 1.87, 95% CI = 1.25, 2.80, p = 0.033) were the only significant predictors of being placed more than 100 miles from home/local authority. Post‐hoc pairwise comparisons of specific NDDs showed that learning disability (LD; 12.2% vs. 6.3%), autistic spectrum condition (ASC; 15.5% vs. 9.8%) and attention deficit hyperactivity disorder (ADHD; 20.4% vs. 14.9%) were all disproportionately more frequent in young people placed more than 100 miles from home/local authority compared to those placed ≤100 miles from home/local authority (for all comparisons, p < 0.046).
Analysis of the characteristics of those with a high number of previous placements showed no association with sociodemographic characteristics or assessed risk. Rather, the presence of physical and/or psychiatric diagnoses, a previous secure placement, and previous contact with services were closely linked to frequency of previous placements (after FDR correction). These associations remained significant after controlling for the legislative framework under which young people were detained (Table 2). The magnitude of associations was strongest for contact with previous services and previous secure placement; there was a more than 5‐fold increase in odds of having contact with social services, YOT and CAMHS as well as having had a previous secure care placement. Having a physical disability doubled the associated risk of ≥10 previous placements while having a psychiatric disorder(s), emotional dysregulation and/or a NDD elevated the associated risk by approximately threefold. The small number of young people with 10 or more previous placements precluded a multivariate analysis of these related factors. On examination of specific NDDs, both LD (16.3% vs. 7.5%) and ADHD (38.8% vs. 15.0%) were more commonly observed in those young people with ≥10 previous placements compared to those with less (for both comparisons, p < 0.028) but the rates of ASC were comparable (8.2% vs. 11.7%; p = 0.644).
Additional (exploratory) analyses considered the characteristics of the small number of individuals (n = 22) with 10 or more previous placements who were currently placed a long distance from their home or local authority. 10 of these young people were female, 8 of 18 (44.4%) for whom there were data on their age were 15 years or younger, and 10 (45.5%) were of BAME background. They were scattered across the secure system with 6 (27.3%) placed under Mental Health legislation (5 in low secure hospital, 1 in a Psychiatric Intensive Care Unit), 8 (36.4%) placed in secure Welfare (in a Secure Children's Home (SCH)) and 8 placed under the YJS (6 in a Young Offender Institution (YOI), one in a SCH and another in a Secure Training Centre (STC)). They were well known to all services with more than two‐thirds (15 or 68.2%) previously placed in secure care, while 19 of 20 (95.0%) with available data had previous contact with social services and CAMHS and 17 of 21 (81.0%) had previous contact with YOT. Ten of 20 (50.0%) with data available had an identified physical disability. Of the 19 young people with mental health data, 14 (73.7%) had at least one psychiatric diagnosis, 5 (26.3%) presented with emotional dysregulation, 5 (26.3%) had 3 or more psychiatric diagnoses and 9 (47.4%) had one or more NDDs. Almost two‐thirds (14 or 63.6%) were assessed as a risk to themselves while only half (11 or 50.0%) posed a risk to others. Compared to those with 10 or more placements but placed 100 miles or less from their home or local authority, this group were more likely to be placed under Mental Health (27.3% vs. 17.9%) and Welfare orders (36.4% vs. 3.6%) than under YJS legislation (36.4% vs. 78.6%; χ 2(2) = 11.51, p = 0.003). They were also more frequently female (45.4% vs. 10.7%), aged 15 years or less (44.4% vs. 16.0%), BAME (45.4% vs. 16.0%), assessed as a risk to themselves (63.6% vs. 35.7%), and had prior contact with CAMHS (95.0% vs. 70.4%; for all comparisons χ 2(1)>3.84, p < 0.050).
3.5. Areas of origin and unwanted outcomes
Large differences between UK regions in the rates of placement of English young people >100 miles from their home/local authority emerged (p < 0.001; Figure 2). The regions of East of England and South West England had the highest rates of long‐distance placements (>50%). However, the actual number of young people in each placement far from home in these areas was fewer than London and comparable to North West England. Those regions with YOIs (Yorkshire and the Humber, West Midlands, and London) tended towards lower rates of long‐distance placements.
FIGURE 2.
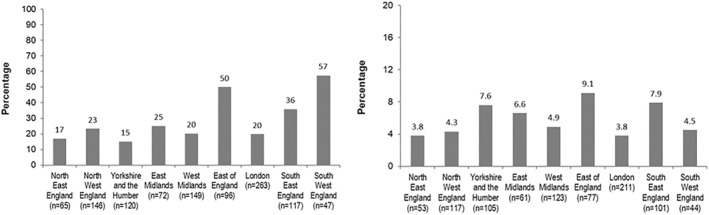
Percentage of young people placed in secure care more than 100 miles from their home or local authority (left) and with 10 or more previous placements (right) according to region of home or local authority. Data labels represent percentage values
In contrast, the proportion of young people with 10 or more previous placements did not significantly differ according to region of home/local authority (p = 0.652; Figure 2). Rates for all were less than 10%. Of the 22 young people with 10 or more previous placements who also were presently placed in secure care >100 miles from their area of origin, half (11) were from East of England (6) or South East England (5) while another 4 were from London.
4. DISCUSSION
The discussion centres on individual and organisational factors that might account for these undesirable patterns of placement and whether the organisation of secure care could develop a system whereby both distant and multiple placements might be avoided.
Significant differences, identified for the first time in this paper, emerged between the component parts of secure care. Strikingly, the smallest component of secure care, welfare, is far more likely to place young people far from home and to be detaining young people who have already experienced a high number of previous placements than either the YJS or mental health. However, the YJS accounts for a higher actual number of young people being placed far from home and of those with high numbers of previous placements. This finding is consistent with the established literature on the risk that children in the care system can subsequently enter the YJS (Bateman et al., 2019).
4.1. Individual factors
Some of the youngest individuals are placed furthest from home. The link between poor attachment and delinquency is stronger in younger individuals (Hoeve et al., 2012); additional separation from key attachment figures at younger ages may exacerbate this tendency. It is hard to see any justification for the placement of the youngest in the cohort far from home; that this pattern is discernible suggests little effective scrutiny of the overall system.
Having a NDD is a common risk factor for, separately, both longer distance placements and high numbers of placements. This may reflect the variation in the clarity of guidance about NDDs. While ADHD is a treatable disorder where medical care is paramount (National Institute for Health and Care Excellence (NICE), 2018), this is not true of either LD or ASC where neither of the relevant NICE guidelines (NICE, 2011, 2015) make clear which agency should lead care planning or, in what kind of setting institutional care, if needed, care should take place. The issue of neurodiversity in secure settings is sufficiently concerning to warrant a HM Inspectorate of Prisons (HMIP) thematic review (Criminal Justice Joint Inspection, 2021) but its recommendations are confined to the adult prison estate. Ambiguity about suitable treatment settings may allow some providers to refuse placement or to absolve themselves of ongoing responsibility for management in the event of challenging behaviour such that the young person is simply moved on to the next available placement.
The data on the small number of young people both far from home and who have had 10 or more placements is important but needs to be treated with caution. The data suggests more are young, female and from a BAME group than might have been anticipated, trends which, for different reasons, warrant better understanding. A lack of availability of placements for young women combined with high rates of emotional dysregulation (Bartlett et al., 2021) contributing to crises within placements may be relevant.
Those with high numbers of previous placements, who are also more likely to have had previous secure placements, are most likely to have had contact with all agencies. This study lacks information on whether that contact is simultaneous or sequential. Both patterns would suggest that young people can pose significant challenges to the system as currently resourced, as it seems inconceivable that multiple moves would ever be seen as positive. This is supported by the finding that 10 or more placements and distant placements correlate significantly; the exhaustion of local placements may lead to the use of those further away. Detailed examination of decision‐making in relation to placement decisions might shed light on how individual factors are construed as these decisions are made.
4.2. Organisational factors
The organisational picture in England is complex; provider units sit in the public and private sector, commissioning of care is split across and within agencies and multiple inspectorates assess standards of care. This level of complexity must compromise organisational memory, coherent and consistent approaches to care, rapid responses to crisis and effective national planning with equitable distribution of resources.
The NAS study (Hales et al., 2018; Warner et al., 2018) examined the varied geography, number and use of different provider units. This information does not easily map onto the overall relationship established between distant placements and region of origin. The contrasting absence of significant differentials between regions in terms of the likelihood of their young people being subject to high numbers of moves might point to individual factors rather than organisational factors determining such moves as all regions are behaving in broadly similar ways.
It is hard to reconcile reviews of individual health and social care provider units with a sense of a system that does not work for a significant proportion of CYP, as this paper suggests, or as their parents indicate (Bartlett et al., 2018). The current focus on evaluation of individual units fails to capture the longitudinal experience of the young person. The Care Quality Commission (CQC) site does not allow comparison of adolescent secure mental hospital units and has done no thematic review of such units despite its recent focus on CAMHS services (CQC, 2017). Only 2% of 60 CAMHS inpatient units were rated “inadequate”; this number possibly includes some secure units. Mental health care to children and young people was fragmented and there were difficulties obtaining local urgent beds, but nothing was said about the child's journey within the wider system or the role mental health plays in multiple placements (CQC, 2017). The Inspecting Local Authority Services for Children (ILACS) inspection system covers secure children's homes. In 2020 none of the 13 SCHs were found inadequate (Ofsted, 2020). ILACS note the high turnover of providers in the sector generally, a potential additional contribution to placement instability. The most recent inspections of the seven STC/YOI sites included in the study are frank about serious failures (HMIP, 2019,2021a, 2021b) but again the focus is on what happens inside individual units. The four YOIs differ but there is evidence of high levels of violence and restricted access to health and education. In the STCs, within the recent past, there have been investigations into violence to young people leading to one unit's closure (Medway Safeguarding Children Board, 2019); in another there was an urgent notification to the Minster for Justice from the Chief Inspector of Prisons in view of conditions found there; children were being locked in their rooms for 19 hours a day (Her Majesty's Chief Inspector, 2021).
In sum, there is very little research or regulatory attention paid to the overall impact on a young person of secure care received in adolescence, despite the system allowing a quarter of all young people to be over 100 miles from home and a quarter to have more than 4 placements. This unsatisfactory bigger picture does not seem to be recognised, in part, because the accepted ways of measuring the adequacy of the system of care ignore this reality and make no attempt to include it in the quality measures that are applied.
4.3. Limitations
This study was cross‐sectional and it is not known if such patterns are consistent over time. Additionally, missing data for both distance from home and for multiple placements (as well as for a small number of other variables of interest, such as presence of a psychiatric disorder) must be noted. When checked, no systematic bias was detected but multiple placement data was limited with respect to BAME young people and those placed in secure welfare—the latter may be important given the high rates of ≥10 placements in these young people.
Distance from home was based in some instances on a central location of the city or county provided rather than a specific address, although this is less relevant to analyses based on UK region and large distance thresholds (placed >100 miles from home or local authority). The small number of young people with 10 or more previous placements precluded a multivariate analysis of these related factors, not allowing identification of the strongest correlates of multiple placements.
5. CONCLUSION
Changing the national approach to monitoring young people's secure care to include tailored never events (Improvement, NHS, 2018), as in the patient safety literature, could prevent both very distant placements and very frequent changes of placement. But this requires multi‐agency sign up mandated at a national level and an acceptance that the user's experience cannot properly be captured without information gleaned from them over time.
CONFLICT OF INTEREST
The authors declare they have no competing interests.
ETHICAL APPROVAL AND PARTICIPANT CONSENT
The HRA (Health Research Authority) confirmed that ethical approval was not required as this was a service evaluation, and CAG (Confidentiality Advisory Group) approval was given. Each healthcare provider ensured local clinical governance approval.
ACKNOWLEDGEMENT
The National Adolescent Study from which this manuscript's data is derived was financially supported by NHS England (NHSE) who provided a research assistant and part salary support for Heidi Hales, Annie Bartlett and Jared G Smith.
Smith, J. G. , Bartlett, A. , & Hales, H. (2022). Exploration of adverse patterns of placement of young people in secure care: The unwanted child? Criminal Behaviour & Mental Health, 32(3), 212–226. 10.1002/cbm.2233
DATA AVAILABILITY STATEMENT
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- Bartlett, A. , Smith, J. G. , Warner, L. , & Hales, H . (2021). Young men and young women in secure care: Gender differences in the placement of those with mental health needs. BMC Psychiatry, 21, 433. 10.1186/s12888-021-03440-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartlett, A. , Warner, L. , & Hales, H . (2018). Young People’s Secure Care: Professionals’ and Parents’ Views of its Purpose, Placements and Practice. NHS Central and NW London. Retrieved November 9, 2021, from https://www.england.nhs.uk/wp‐content/uploads/2018/10/secure‐settings‐for‐young‐people‐a‐national‐scoping‐exercise‐paper‐3‐interview‐report.pdf [Google Scholar]
- Bateman, T. , Day, A. ‐M. , & Pitts, J . (2019). Looked After Children and Custody: A Brief review of the relationship between care status and child incarceration and the implications for service provision. University of Bedfordshire. Retrieved February 18, 2021, from https://mk0nuffieldfounpg9ee.kinstacdn.com/wp‐content/uploads/2020/04/nuffield‐literature‐review‐final.pdf [Google Scholar]
- Benjamini, Y. , & Hochberg, Y . (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B, 57(1), 289–300. [Google Scholar]
- Bowlby, J . (1944). Forty‐four juvenile thieves: Their characters and home life. International Journal of Psycho‐Analysis, 25, 107–127. [Google Scholar]
- Briggs, E. C. , Greeson, J. K. , Layne, C. M. , Fairbank, J. A. , Knoverek, A. M. , & Pynoos, R. S . (2012). Trauma exposure, psychosocial functioning, and treatment needs of youth in residential care: Preliminary findings from the NCTSN Core Data Set. Journal of Child & Adolescent Trauma, 5(1), 1–15. 10.1080/19361521.2012.646413 [DOI] [Google Scholar]
- Care Quality Commission . (2017). Review of children and young people’s mental health services. London: Care Quality Commission. Retrieved November 16, 2021, from https://www.cqc.org.uk/sites/default/files/20171103cypmhphase1report.pdf [Google Scholar]
- Children’s Commissioner . (2019). Pass the parcel: Children posted around the care system. Children’s Commissioner for England. Retrieved August 18, 2021, from https://www.childrenscommissioner.gov.uk/wp‐content/uploads/2019/12/cco‐pass‐the‐parcel‐children‐posted‐around‐the‐care‐system.pdf [Google Scholar]
- Criminal Justice Joint Inspection . (2021). Neurodiversity in the Criminal Justice System A Review of Evidence. HM Crown Prosecution Service Inspectorate, 2021. Retrieved November 10, 2021, from https://www.justiceinspectorates.gov.uk/cjji/wp‐content/uploads/sites/2/2021/07/Neurodiversity‐evidence‐review‐web‐2021.pdf [Google Scholar]
- Fazel, S. , Doll, H. , & Långström, N . (2008). Mental disorders among adolescents in juvenile detention and correctional facilities: A systematic review and metaregression analysis of 25 surveys. Journal of the American Academy of Child & Adolescent Psychiatry, 47(9), 1010–1019. 10.1097/CHI.0b013e31817eecf3 [DOI] [PubMed] [Google Scholar]
- Ford, T. , Vostanis, P. , Meltzer, H. , & Goodman, R . (2007). Psychiatric disorder among British children looked after by local authorities: Comparison with children living in private households. The British Journal of Psychiatry, 190(4), 319–325. 10.1192/bjp.bp.106.025023 [DOI] [PubMed] [Google Scholar]
- Gibson, R . (2020). Secure Care Census. Centre for Youth and Criminal Justice. Retrieved November 9, 2021, from https://www.cycj.org.uk/wp‐content/uploads/2020/07/ACEs‐Places‐and‐Status.pdf [Google Scholar]
- Hales, H. , Warner, L. , Smith, J. , & Bartlett, A . (2018). Census of young people in secure settings on 14 September 2016: characteristics, needs and pathways of care. NHS Central and NW London. Retrieved February 10, 2021, from https://www.england.nhs.uk/wp‐content/uploads/2018/10/secure‐settings‐for‐young‐people‐a‐national‐scoping‐exercise‐paper‐2‐census‐report.pdf [Google Scholar]
- Her Majesty’s Chief Inspector . (2021). Urgent notification: Oakhill Secure Training Centre. Ofsted. Retrieved November 16, 2021, from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1025078/Urgent_notification_letter_to_the_Secretary_of_State_Oakhill_STC_October_2021.pdf [Google Scholar]
- Her Majesty’s Inspectorate of Prisons and Her Majesty’s Inspectorate of Probation . (2019). Youth resettlement work: Interim report into work in custody October 2018–April 2019. Retrieved November 9, 2021, from https://www.justiceinspectorates.gov.uk/cjji/wp‐content/uploads/sites/2/2019/08/Youth‐resettlement‐work‐Web‐2019.pdf
- Hill, S. A. , Argent, S. A. , Lolley, J ., & Wallington, F . (2016). Characteristics of male patients admitted to an adolescent secure forensic psychiatric hospital. Journal of Forensic Psychiatry and Psychology, 27(1), 21–37. 10.1080/14789949.2015.1094117 [DOI] [Google Scholar]
- Hill, S. A. , Brodrick, P. , Doherty, A. , Lolley, J. , Wallington, F. , & White, O . (2014). Characteristics of female patients admitted to an adolescent secure forensic psychiatric hospital. Journal of Forensic Psychiatry and Psychology, 25, 503–519. [Google Scholar]
- Hill, S. A. , Ferreira, J. , Chamorro, V. , & Hosking, A . (2019). Characteristics and personality profiles of first 100 patients admitted to a secure forensic adolescent hospital. Journal of Forensic Psychiatry and Psychology, 30(2), 352–366. 10.1080/14789949.2018.1547416 [DOI] [Google Scholar]
- HM Inspectorate of Prisons . (2019). Report on an unannounced inspection of HMYOI Feltham A Children’s Unit by HM Chief Inspector of Prisons, 4–19 July 2019. HM Inspectorate of Prisons. Retrieved November 16, 2021, from https://www.justiceinspectorates.gov.uk/hmiprisons/wp‐content/uploads/sites/4/2019/10/Feltham‐A‐Web‐2019.pdf [Google Scholar]
- HM Inspectorate of Prisons . (2021a). Children in Custody 2019–20: An analysis of 12–18‐year‐olds’ perceptions of their experiences in secure training centres and young offender institutions. HM Inspectorate of Prisons. Retrieved November 16, 2021, from https://www.justiceinspectorates.gov.uk/hmiprisons/wp‐content/uploads/sites/4/2021/02/CYP‐report‐2019‐20‐web.pdf [Google Scholar]
- HM Inspectorate of Prisons . (2021b). Report on an unannounced inspection of HMYOI Cookham Wood by HM Chief inspector of Prisons, 9–13 August 2021. HM Inspectorate of Prisons. Retrieved November 16, 2021, from https://www.justiceinspectorates.gov.uk/hmiprisons/wp‐content/uploads/sites/4/2021/11/Cookham‐Wood‐web‐2021.pdf [Google Scholar]
- Hoeve, M. , Stams, G. J. J. , Van der Put, C. E. , Dubas, J. S. , Van der Laan, P. H. , & Gerris, J. R . (2012). A meta‐analysis of attachment to parents and delinquency. Journal of Abnormal Child Psychology, 40(5), 771–785. 10.1007/s10802-011-9608-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Improvement, NHS . (2018). Revised never events policy and framework and never events list 2018. NHS Improvement. Retrieved November 16, 2021, from https://www.england.nhs.uk/wp‐content/uploads/2020/11/Revised‐Never‐Events‐policy‐and‐framework‐FINAL.pdf [Google Scholar]
- Medway Safeguarding Children Board . (2019). Serious case review ‘Learning for organisations arising from incidents at Medway Secure Training Centre’. MSBC. Retrieved November 11, 2020, from https://www.medway.gov.uk/mscb/downloads/file/167/2019–‐mscb–‐medway‐stc‐overview‐report [Google Scholar]
- Mikulincer, M. , & Shaver, P. R . (2012). An attachment perspective on psychopathology. World Psychiatry, 11(1), 11–15. 10.1016/j.wpsyc.2012.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Justice . (2019). Proven offending statistics: January to March 2017. Retrieved Janury 4, 2022, from http://publishing.service.gov.uk [Google Scholar]
- National Institute for Health and Care Excellence . (2011). Autism spectrum disorder in under 19s: Recognition, referral and diagnosis. The National Institute for Health and Care Excellence. Retrieved November 10, 2021, from https://www.nice.org.uk/guidance/cg128/resources/autism‐spectrum‐disorder‐in‐under‐19s‐recognition‐referral‐and‐diagnosis‐pdf‐35109456621253 [Google Scholar]
- National Institute for Health and Care Excellence . (2015). Challenging behaviour and learning disabilities: Prevention and interventions for people with learning disabilities whose behaviour challenges LD and challenging behaviour. The National Institute for Health and Care Excellence. Retrieved November 10, 2021, from https://www.nice.org.uk/guidance/ng11/resources/challenging‐behaviour‐and‐learning‐disabilities‐prevention‐and‐interventions‐for‐people‐with‐learning‐disabilities‐whose‐behaviour‐challenges‐pdf‐1837266392005 [PubMed] [Google Scholar]
- National Institute for Health and Care Excellence . (2018). Attention Deficit Hyperactivity Disorder: Diagnosis and Management. Department of Health, 2018. Retrieved November 10, 2021, from https://www.nice.org.uk/guidance/ng87/resources/attention‐deficit‐hyperactivity‐disorder‐diagnosis‐and‐management‐pdf‐1837699732933 [Google Scholar]
- Nelson, C. A. , Scott, R. D. , Bhutta, Z. A. , Harris, N. B. , Danese, A. , & Samara, M . (2020). Adversity in childhood is linked to mental and physical health throughout life. BMJ, 371, m3048. 10.1136/bmj.m3048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ofsted . (2020). National Statistics Main findings: children’s social care in England 2020. Updated 22 September 2020. UK Government, 2020. Retrieved November 16, 2021, from https://www.gov.uk/government/statistics/childrens‐social‐care‐data‐in‐england‐2020/main‐findings‐childrens‐social‐care‐in‐england‐2020 [Google Scholar]
- Owen, J . (2018). Children are still being forced to travel far for mental healthcare. BMJ, 362. 10.1136/bmj.k3769 [DOI] [PubMed] [Google Scholar]
- Stewart, S. L. , Thornley, E. , Lapshina, N. , Erickson, P. , Vingilis, E. , Hamilton, H. , & Kolla, N . (2020). Sex differences in youth with mental health problems in inpatient, outpatient and youth justice settings. BMC Psychiatry, 20(1), 1–16. 10.1186/s12888-019-2413-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner, L. , Hales, H. , Smith, J. G. , & Bartlett, A . (2018). Secure settings for young people: A national scoping exercise. NHS Central and NW London. Retrieved February 10, 2021, from https://www.england.nhs.uk/publication/secure‐settings‐for‐young‐people‐a‐national‐scoping‐exercise/ [Google Scholar]
- Wright, S. , Liddle, M. , & Goodfellow, P . (2016). Young Offenders and Trauma: Experience and Impact A Practitioner’s Guide. Beyond Youth Custody. Retrieved November 9, 2021, from http://www.beyondyouthcustody.net/wp‐content/uploads/Young‐offenders‐and‐trauma‐experience‐and‐impact‐a‐practitioner%E2%80%99s‐guide.pdf [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.