

Abstract
Aim
To conduct an adjusted indirect treatment comparison (aITC) of the efficacy of tirzepatide 5/10/15 mg versus semaglutide 2 mg in patients with type 2 diabetes.
Materials and Methods
The primary analysis was a Bucher aITC of the change from baseline at week 40 in HbA1c (%) and body weight (kg). Aggregate data from the SURPASS‐2 study that met the HbA1c inclusion criterion of the SUSTAIN FORTE study and from SUSTAIN FORTE metformin‐only treated patients were used for primary analysis.
Results
The SURPASS‐2 refined population comprised 238/245/240 and 240 participants for tirzepatide 5/10/15 mg and semaglutide 1 mg, respectively. The SUSTAIN FORTE metformin‐only population comprised 222 and 227 participants for semaglutide 1 and 2 mg, respectively. In this aITC, tirzepatide 10 and 15 mg significantly reduced HbA1c versus semaglutide 2 mg with an estimated treatment difference (ETD) of −0.36% (95% confidence interval [CI] −0.63, −0.09) and −0.4% (95% CI −0.67, −0.13), respectively. Tirzepatide 10 and 15 mg significantly reduced body weight versus semaglutide 2 mg with an ETD of −3.15 kg (95% CI −4.84, −1.46) and −5.15 kg (95% CI −6.85, −3.45), respectively. There were no significant differences between tirzepatide 5 mg and semaglutide 2 mg on change from baseline in HbA1c and body weight.
Conclusions
In this aITC, HbA1c and weight reductions were significantly greater for tirzepatide 10 and 15 mg versus semaglutide 2 mg and were similar for tirzepatide 5 mg versus semaglutide 2 mg. These findings provide comparative effectiveness insights in the absence of a head‐to‐head clinical trial.
Keywords: adjusted indirect treatment comparison, GIP/GLP‐1 receptor agonist, incretin mimetic, incretins, matching‐adjusted indirect comparison, semaglutide, tirzepatide, type 2 diabetes
1. INTRODUCTION
Tirzepatide is a once‐weekly glucose‐dependent insulinotropic polypeptide and glucagon‐like peptide‐1 receptor agonist (GIP/GLP‐1 RA) recently approved by the US Food and Drug Administration (FDA) for the treatment of type 2 diabetes (T2D). The efficacy and safety of tirzepatide 5, 10 and 15 mg have been extensively investigated in the phase 3 SURPASS programme in various populations along the continuum of T2D management. 1 , 2 , 3 , 4 , 5 All doses of tirzepatide have shown superior reduction from baseline at the primary endpoint in HbA1c and body weight versus placebo (in the SURPASS‐1 study as monotherapy and in the SURPASS‐5 study as add‐on to titrated basal insulin), semaglutide 1 mg (SURPASS‐2), insulin degludec (SURPASS‐3) and insulin glargine 100 units/ml (SURPASS‐4). 1 , 2 , 3 , 4 , 5 In the SURPASS‐2 study, all doses of tirzepatide were superior to semaglutide 1 mg, a selective GLP‐1 RA, in both HbA1c and body weight change from baseline at week 40 in patients with T2D taking metformin with HbA1c above target. 2 The overall safety profile of tirzepatide was similar to that of semaglutide. Semaglutide was first approved as a once‐weekly injection at maintenance doses of 0.5 and 1 mg by the FDA in 2017 6 and by the European Medicines Agency (EMA) in 2018. 7 At the time of the SURPASS‐2 study design and conduct, 1 mg was the highest approved dose of semaglutide for the management of patients with T2D who had shown superiority in lowering glucose levels and reducing body weight compared with two selective GLP‐1 RAs, dulaglutide (0.75 and 1.5 mg) and exenatide (2 mg) once weekly, with a similar safety profile. 8 , 9
The progressive nature of T2D and thus, the requirement of treatment advancement to achieve and maintain glycaemic targets, has prompted the investigation of a higher dose of injectable semaglutide. The efficacy and safety of semaglutide 2 mg has been evaluated against the lower dose of 1 mg in the phase 3 SUSTAIN FORTE trial. 10 In SUSTAIN FORTE, treatment with semaglutide 2 mg versus 1 mg at week 40 showed superior reduction in HbA1c and additional body weight loss in patients with T2D and elevated glycaemic levels (HbA1c 8%‐10%) on background metformin with or without a sulphonylurea. The safety profile and gastrointestinal tolerability of semaglutide was similar for both doses. Semaglutide 2 mg was recently approved by the EMA and FDA.
At present, there is a lack of a head‐to‐head comparison of tirzepatide versus semaglutide 2 mg. Information on the relative efficacy of tirzepatide and semaglutide 2 mg may be relevant for clinicians when these agents are approved and available for use. The aim of this analysis was to compare the efficacy of tirzepatide 5, 10 and 15 mg with semaglutide 2 mg using an adjusted indirect treatment comparison (aITC) based on results from the SURPASS‐2 2 and SUSTAIN FORTE 10 trials.
2. METHODS
2.1. Primary analysis
The aITC of the efficacy of tirzepatide 5, 10 and 15 mg versus semaglutide 2 mg was conducted using the Bucher method. 11 Published aggregate data from two randomized controlled trials—SURPASS‐2 2 and SUSTAIN FORTE 10 —were used. The method accounts for cross‐trial differences by measuring relative treatment effects versus a common comparator arm. The aITC of SURPASS‐2 (tirzepatide vs. semaglutide 1 mg) and SUSTAIN FORTE (semaglutide 2 mg vs. semaglutide 1 mg), with the common comparator arm semaglutide 1 mg, is shown in Figure 1. The method is valid if there is similarity in the outcome of the common comparator (semaglutide 1 mg) in each trial (SURPASS‐2 and SUSTAIN FORTE). Thus, it was necessary to ensure that there were no relevant differences in study design and patient characteristics between the two trials or, if such differences existed, consideration on how they may have impacted the results was taken into account. For this analysis, individual patient data were also utilized from the SURPASS‐2 study because of existing differences between the two studies (as described below).
FIGURE 1.
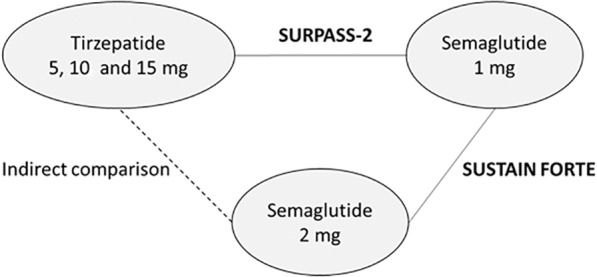
Adjusted indirect treatment comparison of tirzepatide 5, 10 and 15 mg versus semaglutide 2 mg using semaglutide 1 mg as common comparator
Table 1 shows an overview of the study characteristics and key inclusion criteria of the SURPASS‐2 and SUSTAIN FORTE trials. SURPASS‐2 was an open‐label, multinational, phase 3 trial and SUSTAIN FORTE was a double‐blind, multinational, phase 3b trial. There were two key differences across trials: (a) the inclusion criteria of HbA1c (7.0%‐10.5% in SURPASS‐2 vs. 8.0%‐10.0% in SUSTAIN FORTE) and (b) background antihyperglycaemic medication (metformin in SURPASS‐2 vs. metformin with or without a sulphonylurea in SUSTAIN FORTE). In SUSTAIN FORTE, all patients were using metformin and 53% of patients were using a sulphonylurea at baseline. These cross‐trial differences were accounted for in the aITC as follows. The more restrictive HbA1c inclusion criterion of SUSTAIN FORTE was applied to the population of SURPASS‐2. The subgroup of participants in SURPASS‐2 who fulfilled the inclusion criterion of HbA1c in SUSTAIN FORTE is hereby referred to as the SURPASS‐2 refined population. In SUSTAIN FORTE, subgroup analyses by baseline use of metformin with or without a sulphonylurea were only available for changes from baseline in HbA1c and body weight at week 40. Of note, the treatment by subgroup interaction was not statistically significant in the SUSTAIN FORTE population using metformin with or without a sulphonylurea. No data were available on the percentage of patients reaching HbA1c goals (e.g. <7% or ≤6.5%) for these subgroups from SUSTAIN FORTE. Therefore, the aITC used results from the SURPASS‐2 refined population and SUSTAIN FORTE metformin‐only population for change from baseline in HbA1c and body weight at week 40 as the primary analysis. Safety data for the metformin‐only population from SUSTAIN FORTE were also not available and, therefore, no formal adjusted indirect comparisons were conducted.
TABLE 1.
Overview of the study characteristics and key inclusion criteria of the SURPASS‐2 and SUSTAIN FORTE trials
| Trial name | SURPASS‐2 | SUSTAIN FORTE |
|---|---|---|
| Study design | Open‐label, parallel‐group, randomized, active‐controlled, phase 3, multinational | Double‐blind, parallel‐group, randomized, active‐controlled, phase 3b, multinational |
| Key inclusion criteria | ||
| HbA1c | 7.0%‐10.5% | 8.0%‐10.0% |
| Body mass index | ≥25 kg/m2 | 25‐40 kg/m2 |
| Background antihyperglycaemic medication | Metformin (≥1500 mg/d) for ≥3 mo | Metformin (≥1500 mg/d) with or without a sulphonylurea for ≥3 mo |
| Time of primary endpoint | 40 wk | 40 wk |
| Randomized treatment |
Tirzepatide 5, 10 and 15 mg Semaglutide 1 mg |
Semaglutide 1 and 2 mg |
| Number of randomized patients (ratio) | 1879 (1:1:1:1) | 961 (1:1) |
| Key regions of enrolment | Australia, Canada, Israel, Latin America, UK, United States | Canada, Europe, Japan, United States |
| Time of study conduct | 2019–2021 | 2019–2020 |
For the primary analysis, aITCs were based on results for the efficacy estimand (referred to as the trial product estimand in SUSTAIN FORTE), which was defined as the treatment effect among all patients who underwent randomization and received at least one dose of the study medication, excluding the data after the start of rescue therapy (for persistent hyperglycaemia) or study drug discontinuation. Bucher aITCs were performed using R version 3.4.4.
2.2. Outcomes
The outcomes assessed in the aITC were the change from baseline in HbA1c and body weight at week 40. The change from baseline in HbA1c at week 40 corresponds to the primary endpoint in SURPASS‐2 and SUSTAIN FORTE. The change from baseline in body weight at week 40 corresponds to a confirmatory secondary endpoint in both SURPASS‐2 and SUSTAIN FORTE studies. Both outcomes were controlled for type 1 error rate in both trials. Mean estimated treatment difference (ETD) values with associated 95% confidence intervals (CIs) were reported.
2.3. Patient characteristics
The baseline characteristics of the participants enrolled in SURPASS‐2 and SUSTAIN FORTE are summarized in Table 2. Baseline data for the SURPASS‐2 refined population are also shown for comparison. Baseline data for the SUSTAIN FORTE metformin‐only population were not published previously. The aITC was anchored to the common comparator arm semaglutide 1 mg. Therefore, comparison of baseline characteristics was aimed to the semaglutide 1‐mg arm in the SURPASS‐2 refined population and the full population of SUSTAIN FORTE. Despite SUSTAIN FORTE having a larger sample size compared with the SURPASS‐2 refined population, approximately 50% of participants in SUSTAIN FORTE were on metformin with a sulphonylurea. 10 Therefore, the size of both the SUSTAIN FORTE metformin‐only population and the SURPASS‐2 refined population were comparable for the aITC. Further differences in baseline characteristics between the two trials were addressed in a sensitivity analysis (described in section 2.4).
TABLE 2.
Baseline characteristics in the SURPASS‐2 and SUSTAIN FORTE trials
| Trial name | SURPASS‐2 | SUSTAIN FORTE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Semaglutide 1 mg | Semaglutide 1 mg | Semaglutide 2 mg | ||||
| Population | Full | Refined a | Full | Refined a | Full | Refined a | Full | Refined a | ||
| n | 470 | 238 | 469 | 245 | 470 | 240 | 469 | 240 | 481 | 480 |
| Mean age (SD), y | 56.3 (10.0) | 55.7 (10.0) | 57.2 (10.5) | 56.3 (10.4) | 55.9 (10.4) | 56.1 (10.3) | 56.9 (10.8) | 56.2 (10.7) | 58.2 (9.9) | 57.9 (10.0) |
| Female, n (%) | 265 (56) | 140 (59) | 231 (49) | 124 (51) | 256 (55) | 132 (55) | 244 (52) | 128 (53) | 197 (41) | 201 (42) |
| Mean HbA1c (SD), % | 8.3 (1.1) | 8.8 (0.6) | 8.3 (1.0) | 8.8 (0.6) | 8.3 (1.0) | 8.8 (0.6) | 8.3 (1.0) | 8.8 (0.6) | 8.8 (0.6) | 8.9 (0.6) |
| Mean FPG b (SD), mg/dl | 173.8 (51.9) | 186.1 (49.0) | 174.2 (49.8) | 189.5 (49.2) | 172.4 (54.4) | 187.6 (54.4) | 171.4 (49.8) | 190.6 (48.4) | 196.2 (48.6) | 192.6 (50.4) |
| Mean duration of diabetes (SD), y | 9.1 (7.2) | 10.0 (7.4) | 8.4 (5.9) | 9.1 (5.9) | 8.7 (6.9) | 9.3 (7.4) | 8.3 (5.8) | 8.7 (5.8) | 9.8 (6.2) | 9.2 (6.2) |
| Mean body weight (SD), kg | 92.5 (21.8) | 90.9 (22.1) | 94.8 (22.7) | 94.7 (23.1) | 93.8 (21.8) | 92.6 (20.7) | 93.7 (21.1) | 93.0 (22.8) | 98.6 (24.4) | 100.1 (22.6) |
| Mean BMI (SD), kg/m2 | 33.8 (6.9) | 33.7 (7.5) | 34.3 (6.6) | 34.4 (6.7) | 34.5 (7.1) | 34.3 (7.2) | 34.2 (7.2) | 33.8 (6.8) | 34.4 (7.2) | 34.8 (6.8) |
| Mean waist circumference (SD), cm | 108.1 (14.8) | 106.4 (15.2) | 110.6 (16.1) | 110.4 (16.4) | 109.6 (15.6) | 109.6 (15.5) | 109.0 (14.9) | 109.5 (14.9) | 112.2 (16.4) | 113.4 (16.4) |
| Mean SBP (SD), mmHg | 131 (14) | 130 (14) | 131 (14) | 132 (13) | 130 (14) | 132 (14) | 130 (13) | 130 (13) | 134 (14) | 134 (14) |
| Mean DBP (SD), mmHg | 79 (9) | 78 (9) | 80 (10) | 81 (10) | 79 (9) | 80 (9) | 79 (9) | 80 (9) | 80 (10) | 81 (9) |
| Mean eGFR (SD), ml/min/1.73m2 | 96.6 (17.5) | 98.4 (17.4) | 95.5 (16.6) | 98.7 (15.4) | 96.3 (16.9) | 97.3 (16.8) | 95.6 (17.3) | 96.7 (18.0) | 93.0 (17.5) | 93.9 (16.4) |
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; SBP, systolic blood pressure; SD, standard deviation.
The refined population in SURPASS‐2 is the subgroup of participants who adhered to the inclusion criteria of HbA1c in SUSTAIN FORTE (8%‐10%). Baseline data for the SUSTAIN FORTE metformin‐only population were not published previously.
SURPASS‐2 reports fasting serum glucose and SUSTAIN FORTE reports FPG (mmol/L).
2.4. Sensitivity analysis
Four different sensitivity analyses were conducted to assess the findings of the primary analysis (Table 3). The first three sensitivity analyses were conducted with the Bucher method. Sensitivity analysis 1 accounted for the SURPASS‐2 full population (without applying the HbA1c inclusion criterion of SUSTAIN FORTE). Sensitivity analysis 2 accounted for the full population in both trials. Sensitivity analysis 3 used the results from the treatment‐regimen estimand in both trials (referred to as the treatment policy estimand in SUSTAIN FORTE), which were only available for the full population in both trials. The treatment‐regimen estimand was defined as the treatment effect among all patients who underwent randomization (regardless of treatment discontinuation or rescue medication) and, therefore, accounts for the potential effects of use of rescue therapy or treatment discontinuation in the aITCs. In the final sensitivity analysis (sensitivity analysis 4), a matching‐adjusted indirect comparison (MAIC) method was used on the full population in both trials to adjust for potential treatment effect modifiers and imbalance in the baseline characteristics, such as baseline HbA1c and body weight, on the full population. Further details regarding MAIC are provided in the supporting information. The reweighted baseline characteristics following MAIC are shown in Table S1.
TABLE 3.
Sensitivity analyses
| Analysis | Method | Population | Estimand | Objective | |
|---|---|---|---|---|---|
| SURPASS‐2 | SUSTAIN FORTE | ||||
| Primary analysis | Bucher | Refined a | Metformin only | Efficacy (trial product) | Refine baseline HbA1c (8%‐10%) and background antihyperglycaemic medication (without SU) |
| Sensitivity analysis 1 | Bucher | Full | Metformin only | Efficacy (trial product) | Test the impact of inclusion of the full SURPASS‐2 population in the primary analysis |
| Sensitivity analysis 2 | Bucher | Full | Full | Efficacy (trial product) | Test the impact of inclusion of the full SURPASS‐2 and SUSTAIN FORTE population in the primary analysis |
| Sensitivity analysis 3 | Bucher | Full | Full | Treatment‐regimen (treatment policy) | Test the impact of inclusion of the full SURPASS‐2 and SUSTAIN FORTE population in the primary analysis while including the data after treatment discontinuation or use of rescue therapy |
| Sensitivity analysis 4 | MAIC | Full | Full | Efficacy (trial product) | Test the hypothesis using a different statistical method by matching the baseline HbA1c and body weight of patients using full population of both SURPASS‐2 and SUSTAIN FORTE |
Abbreviations: MAIC, matching‐adjusted indirect comparison; SU, sulphonylurea.
The refined population in SURPASS‐2 is the subgroup of participants who adhered to the inclusion criteria of HbA1c in SUSTAIN FORTE (8%‐10%).
3. RESULTS
A total of 1879 participants were randomized in SURPASS‐2 (tirzepatide 5 mg, N = 471; tirzepatide 10 mg, N = 469; tirzepatide 15 mg, N = 470; semaglutide 1 mg, N = 469) and 961 in SUSTAIN FORTE (semaglutide 1 mg, N = 481; semaglutide 2 mg, N = 480). The Bucher method assumes that the comparative efficacy results of SURPASS‐2 would have been the same had SURPASS‐2 been performed in the SUSTAIN FORTE population. Thus, this assumption is considered appropriate when there is reasonable similarity in baseline characteristics and inclusion/exclusion criteria between both trials. Age, baseline HbA1c and fasting plasma glucose were very similar in the semaglutide 1‐mg arm of the SURPASS‐2 refined population (refined on HbA1c inclusion criterion of 8.0%‐10.0%) and the SUSTAIN FORTE full population (Table 2). Baseline body weight‐related characteristics were slightly higher in the SUSTAIN FORTE full population versus the SURPASS‐2 refined population or full population.
Direct comparisons between treatments for change from baseline in HbA1c and in body weight at week 40, as reported in SURPASS‐2 and SUSTAIN FORTE, are shown in Table S2. Direct comparisons of tirzepatide 5, 10 and 15 mg versus semaglutide 1 mg on the refined population of SURPASS‐2 were also included. The results for the aITC of tirzepatide 5, 10 and 15 mg versus semaglutide 2 mg are shown in Figure 2.
FIGURE 2.
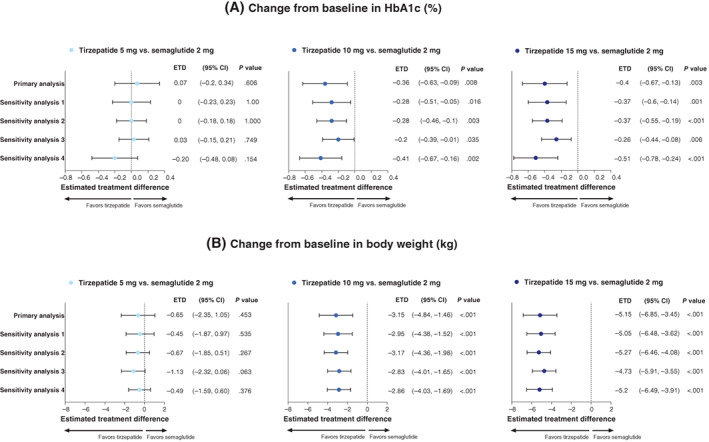
Adjusted indirect treatment comparison of tirzepatide 5, 10 and 15 mg versus semaglutide 2 mg in the change from baseline in A, HbA1c and B, Body weight at week 40. Primary and sensitivity analyses. CI, confidence interval; ETD, estimated treatment difference
3.1. Adjusted indirect comparison for change from baseline in HbA1c
In the primary analysis of this aITC, tirzepatide 10 and 15 mg reduced HbA1c from baseline significantly more than semaglutide 2 mg, with an ETD of −0.36% (95% CI −0.63, −0.09; P = .008) and −0.4% (95% CI −0.67, −0.13; P = .003) at week 40, respectively (Figure 2A). There were no significant differences between tirzepatide 5 mg and semaglutide 2 mg in change from baseline in HbA1c at week 40 with an ETD of 0.07% (95% CI −0.2, 0.34; P = .606).
The results from the sensitivity analyses accounting for either the full population of SURPASS‐2 (sensitivity analysis 1), the full population of both trials (sensitivity analysis 2), the treatment‐regimen estimand in the full population of both trials (sensitivity analysis 3) or the adjusted baseline HbA1c and body weight in the full population of both trials (sensitivity analysis 4) were consistent with those of the primary analysis (Figure 2A).
3.2. Adjusted indirect comparison for change from baseline in body weight
In the primary analysis of this aITC, tirzepatide 10 and 15 mg reduced the body weight from baseline significantly more than semaglutide 2 mg with an ETD of −3.15 kg (95% CI −4.84, −1.46; P < .001) and −5.15 kg (95% CI −6.85, −3.45; P < .001) at week 40, respectively (Figure 2B). There were no significant differences between tirzepatide 5 mg and semaglutide 2 mg on change from baseline in body weight at week 40 with an ETD of −0.65 kg (95% CI −2.35, 1.05; P = .453).
The results from the four sensitivity analyses were consistent with those of the primary analysis (Figure 2B).
3.3. Safety
A summary of key safety data from the full population of SURPASS‐2 and SUSTAIN FORTE was reviewed (Table 4). The overall safety profile was similar with tirzepatide and semaglutide treatment across all doses with gastrointestinal adverse events including nausea, diarrhoea and vomiting being commonly reported. Because the overall rates of treatment‐emergent adverse events and gastrointestinal adverse events were higher for the common comparator semaglutide 1‐mg arm in SURPASS‐2 (64% and 41%) than in SUSTAIN FORTE (52% and 31%), respectively, any quantitative comparisons for individual adverse events between tirzepatide and semaglutide 2 mg could be misleading without adjusted comparisons.
TABLE 4.
Summary of key safety data reported in SURPASS‐2 and SUSTAIN FORTE
| Trial name | SURPASS‐2 (full population) | SUSTAIN FORTE (full population) | ||||
|---|---|---|---|---|---|---|
| Treatment | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Semaglutide 1 mg | Semaglutide 1 mg | Semaglutide 2 mg |
| N | 470 | 469 | 470 | 469 | 480 | 479 |
| Treatment‐emergent adverse events | 299 (64%) | 322 (69%) | 324 (69%) | 301 (64%) | 251 (52%) | 272 (57%) |
| Serious adverse events | 33 (7%) | 25 (5%) | 27 (6%) | 13 (3%) | 25 (5%) | 21 (4%) |
| Treatment discontinuation because of adverse events | 28 (6%) | 40 (9%) | 40 (9%) | 19 (4%) | 22 (5%) | 21 (4%) |
| Treatment discontinuation because of GI adverse events | 13 (3%) | 20 (4%) | 20 (4%) | 15 (3%) | 13 (3%) | 16 (3%) |
| GI adverse events overall | 188 (40%) | 216 (46%) | 211 (45%) | 193 (41%) | 148 (31%) | 163 (34%) |
| Treatment‐emergent adverse events in ≥5% in any treatment group, by preferred term | ||||||
| Nausea | 82 (17%) | 90 (19%) | 104 (22%) | 84 (18%) | 70 (15%) | 69 (14%) |
| Diarrhoea | 62 (13%) | 77 (16%) | 65 (14%) | 54 (12%) | 42 (9%) | 45 (9%) |
| Vomiting | 27 (6%) | 40 (9%) | 46 (10%) | 39 (8%) | 32 (7%) | 37 (8%) |
| Dyspepsia | 34 (7%) | 29 (6%) | 43 (9%) | 31 (7%) | 25 (5%) | 16 (3%) |
| Decreased appetite | 35 (7%) | 34 (7%) | 42 (9%) | 25 (5%) | 18 (4%) | 29 (6%) |
| Constipation | 32 (7%) | 21 (5%) | 21 (5%) | 27 (6%) | — | — |
| Abdominal pain | 14 (3%) | 21 (5%) | 24 (5%) | 24 (5%) | — | — |
Note. Data are n (%) in the safety population (modified intention‐to‐treat population with all the data from the start of treatment to the end of the safety follow‐up in SURPASS‐2 and data from the on‐treatment observation period including events occurring up to 49 d after the last day on trial drug in SUSTAIN FORTE).
Abbreviation: GI, gastrointestinal.
4. DISCUSSION
In the SURPASS‐2 study, all doses of tirzepatide were superior to semaglutide 1 mg in both HbA1c and body weight change from baseline at week 40 in patients with T2D and elevated glucose levels (HbA1c 8%‐10%) with metformin. 2 With the investigation and availability of semaglutide 2 mg, data on comparative efficacy between tirzepatide and this higher dose of semaglutide may be relevant to make clinical decisions. Indirect treatment comparisons of glucose‐lowering agents have previously been reported in the literature in the absence of head‐to‐head trials. 12 , 13 , 14 , 15
This is the first comparison of tirzepatide 5, 10 and 15 mg versus injectable semaglutide 2 mg on the change from baseline in HbA1c and body weight in patients with T2D and elevated glucose levels (HbA1c 8%‐10%) with metformin. An aITC method was used based on the results of two phase 3 multinational trials, SURPASS‐2 and SUSTAIN FORTE, with the common comparator arm semaglutide 1 mg. The primary analysis showed that the effects of tirzepatide 10 and 15 mg on the reduction of HbA1c and body weight were statistically significant and clinically meaningful compared with semaglutide 2 mg. The lowest dose of tirzepatide (5 mg) offered similar reductions from baseline in HbA1c and body weight versus the highest dose of semaglutide (2 mg). The American Diabetes Association recommends an HbA1c target of less than 7% and body weight loss of at least 5% for the majority of patients with T2D. In SUSTAIN FORTE, semaglutide 2 mg showed superiority over semaglutide 1 mg in HbA1c and weight change at 40 weeks; however, 32% and 41% of patients in the semaglutide 2‐mg arm did not achieve an HbA1c target of less than 7% and weight loss of at least 5%, respectively. The higher efficacy of tirzepatide, as shown here, comparing it with the highest approved dose of selective GLP‐1 RA semaglutide for the management of T2D, is probably a result of the additional GIP RA activity associated with tirzepatide. The incremental HbA1c reduction of 0.4% with tirzepatide 10 and 15 mg and greater body weight reduction of 3.2 kg with tirzepatide 10 mg and 5.2 kg with tirzepatide 15 mg compared with semaglutide 2 mg reported in this analysis may help more patients reach these clinically relevant goals.
The results of the primary analysis for both change from baseline in HbA1c and body weight were supported by the results of the sensitivity analyses, which accounted for different sets of populations, estimands and analytical approaches to minimize bias. The overall safety profile of tirzepatide and semaglutide appeared to be consistent, with gastrointestinal adverse events as the commonly reported events; however, adjusted quantitative comparisons were not feasible.
One of the strengths of this analysis is the comparison method, which relies on the similarities of the study design and population from SURPASS‐2 and SUSTAIN FORTE, such as the background oral antihyperglycaemic medication and time of primary endpoint at week 40. The availability of efficacy data in the SUSTAIN FORTE metformin‐only population allowed for an indirect comparison in the primary analysis in patients receiving the same background antihyperglycaemic medication in both trials. Potential treatment effect modifiers were also accounted for in the primary analysis by restricting the SURPASS‐2 population to patients complying with the HbA1c inclusion criterion of SUSTAIN FORTE (referred to as the SURPASS‐2 refined population). The similarity in baseline characteristics (age, HbA1c and body mass index) between the SURPASS‐2 refined population and SUSTAIN FORTE full population in the semaglutide 1‐mg arms, as well as in HbA1c change from baseline in the SURPASS‐2 refined population versus the SUSTAIN FORTE metformin‐only population for the semaglutide 1‐mg arms (−2.2% vs. −2.1%), support the appropriateness of the Bucher approach. Overall, it was justified to assume that relative differences between treatments for HbA1c and body weight would be similar in the SUSTAIN FORTE metformin‐only population and the SURPASS‐2 refined population. Furthermore, the sample size of the SURPASS‐2 refined population and SUSTAIN FORTE metformin‐only population, which were compared in the primary analysis, were similar. The sensitivity analyses conducted on the full population supported the results of the primary analysis. In addition, the baseline HbA1c and body weight characteristics were adjusted for in the full population of both trials in sensitivity analysis 4, supporting the findings of the primary analysis. Another sensitivity analysis was conducted to assess the results accounting for the impact of potential effects of treatment discontinuation or the use of rescue therapy, which also provided consistent results with the primary analysis.
The first limitation of this analysis is that only two studies were available for the aITC. Second, no baseline characteristics were available in the SUSTAIN FORTE metformin‐only population. Therefore, baseline characteristics were compared between patients on metformin in SURPASS‐2 and patients on metformin with or without a sulphonylurea in SUSTAIN FORTE. This also had an impact on sensitivity analysis 4, which adjusted for baseline HbA1c and body weight in patients on metformin in SURPASS‐2 and patients on metformin with or without a sulphonylurea in SUSTAIN FORTE. Third, in an attempt to compare patients receiving the same background antihyperglycaemic medication in both trials, only endpoints with data available in the SUSTAIN FORTE metformin‐only population (change from baseline in HbA1c and body weight) were included in the aITC. Other glycaemic efficacy endpoints (e.g. the percentage of patients reaching an HbA1c target of <7%) were not included in the analysis as these were only reported for the full population of SUSTAIN FORTE (patients on metformin with or without a sulphonylurea) and not the SUSTAIN FORTE metformin‐only population. For the same reason as above, no quantitative comparison for safety outcomes was performed. In both treatments, the incidence of gastrointestinal adverse events was higher during the dose‐escalation period and decreased over time. 2 , 10 Fourth, it was not possible to compare the results of the treatment‐regimen estimand in the SURPASS‐2 refined population and SUSTAIN FORTE metformin‐only population because these results were not published in SUSTAIN FORTE. However, the sensitivity analysis conducted with the results of the treatment‐regimen estimand in the full population of both trials supported the results of the primary analysis. Finally, adjusted indirect comparisons may not account for residual confounding because of unobserved differences between trials and, therefore, these findings cannot replace a direct head‐to‐head trial, and conducting a trial to compare tirzepatide and semaglutide 2 mg would validate these findings.
Overall, this aITC showed significantly greater HbA1c and body weight reductions with tirzepatide 10 and 15 mg versus semaglutide 2 mg and similar reductions with tirzepatide 5 mg and semaglutide 2 mg. In the absence of a head‐to‐head comparison, these findings may help to guide clinician decisions and enable pharmacoeconomic assessment of the most suitable incretin‐based treatment for patients with T2D. In addition to efficacy and safety data, clinicians should also consider patient preference for the administration device, as it is an important driver of the choice of medication.
AUTHOR CONTRIBUTIONS
All the authors participated in the interpretation of the data and critical review of the manuscript and approved this manuscript to be submitted for publication. KV, HP, RM, JAL, MH and HS contributed to the conception of the manuscript. KV and HS contributed to the planning of the analyses and conducted the statistical analysis.
CONFLICT OF INTEREST
AYYC declares advisory board and/or speaking honoraria from Abbott, AstraZeneca, Bausch, Bayer, Boehringer Ingelheim, Dexcom, Eli Lilly and Company, HLS Therapeutics, Insulet, Janssen, Medtronic, Merck, Novo Nordisk, Pfizer, Sanofi and Takeda. KMP reports receiving research support from Bayer, Merck, Novo Nordisk and Twin Health; consulting honoraria from AstraZeneca, Bayer, Corcept Therapeutics, Diasome, Eli Lilly and Company, Merck, Novo Nordisk and Sanofi; and speaker honoraria from AstraZeneca, Corcept Therapeutics, Merck and Novo Nordisk. KV, HP, RM, JAL, MH and HS are employees and shareholders of Eli Lilly and Company.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1111/dom.14775.
Supporting information
Appendix S1 Supporting Information
ACKNOWLEDGEMENTS
The authors would like to thank Amelia Torcello Gomez, PhD, from Eli Lilly and Company, for writing and editorial contributions; Mark Belger, BSc, from Eli Lilly and Company, for providing statistical guidance; and Brian D. Benneyworth, MD, from Eli Lilly and Company, for providing scientific review.
Vadher K, Patel H, Mody R, et al. Efficacy of tirzepatide 5, 10 and 15 mg versus semaglutide 2 mg in patients with type 2 diabetes: An adjusted indirect treatment comparison. Diabetes Obes Metab. 2022;24(9):1861‐1868. doi: 10.1111/dom.14775
Funding information Eli Lilly and Company; Eli Lilly and Company, Grant/Award Number: N/A
DATA AVAILABILITY STATEMENT
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request six months after the indication studied has been approved in the US and EU and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after a receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.
REFERENCES
- 1. Rosenstock J, Wysham C, Frias JP, et al. Efficacy and safety of a novel dual GIP and GLP‐1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS‐1): a double‐blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143‐155. [DOI] [PubMed] [Google Scholar]
- 2. Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503‐515. [DOI] [PubMed] [Google Scholar]
- 3. Ludvik B, Giorgino F, Jodar E, et al. Once‐weekly tirzepatide versus once‐daily insulin degludec as add‐on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS‐3): a randomised, open‐label, parallel‐group, phase 3 trial. Lancet. 2021;398(10300):583‐598. [DOI] [PubMed] [Google Scholar]
- 4. Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS‐4): a randomised, open‐label, parallel‐group, multicentre, phase 3 trial. Lancet. 2021;398(10313):1811‐1824. [DOI] [PubMed] [Google Scholar]
- 5. Dahl D, Onishi Y, Norwood P, et al. Effect of subcutaneous tirzepatide vs placebo added to titrated insulin glargine on glycemic control in patients with type 2 diabetes: the SURPASS‐5 randomized clinical trial. JAMA. 2022;327(6):534‐545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. FDA . Ozempic (semaglutide). Highlights of prescribing information. 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/209637lbl.pdf. Accessed February 2022.
- 7. EMA . Ozempic (semaglutide). Summary of product characteristics. 2020. https://www.ema.europa.eu/en/documents/product‐information/ozempic‐epar‐product‐information_en.pdf. Accessed February 2022.
- 8. Ahmann AJ, Capehorn M, Charpentier G, et al. Efficacy and safety of once‐weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): a 56‐week, open‐label, randomized clinical trial. Diabetes Care. 2018;41(2):258‐266. [DOI] [PubMed] [Google Scholar]
- 9. Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open‐label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275‐286. [DOI] [PubMed] [Google Scholar]
- 10. Frias JP, Auerbach P, Bajaj HS, et al. Efficacy and safety of once‐weekly semaglutide 2.0 mg versus 1.0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double‐blind, randomised, phase 3B trial. Lancet Diabetes Endocrinol. 2021;9(9):563‐574. [DOI] [PubMed] [Google Scholar]
- 11. Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta‐analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683‐691. [DOI] [PubMed] [Google Scholar]
- 12. Pratley RE, Catarig AM, Lingvay I, et al. An indirect treatment comparison of the efficacy of semaglutide 1.0 mg versus dulaglutide 3.0 and 4.5 mg. Diabetes Obes Metab. 2021;23(11):2513‐2520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Evans M, Billings LK, Hakan‐Bloch J, et al. An indirect treatment comparison of the efficacy of insulin degludec/liraglutide (IDegLira) and insulin glargine/lixisenatide (iGlarLixi) in patients with type 2 diabetes uncontrolled on basal insulin. J Med Econ. 2018;21(4):340‐347. [DOI] [PubMed] [Google Scholar]
- 14. Lingvay I, Bauer R, Baker‐Knight J, Lawson J, Pratley R. An indirect treatment comparison of semaglutide 2.0 mg versus dulaglutide 3.0 mg and 4.5 mg using multilevel network meta‐regression. J Clin Endocrinol Metab. 2022;107(5):1461‐1469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Martin AA, Parks D. An indirect comparison of HbA1c treatment effect with albiglutide and exenatide 2.0 mg QW using the Bucher method. Diabetes Metab Syndr Obes. 2016;9:163‐168. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1 Supporting Information
Data Availability Statement
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request six months after the indication studied has been approved in the US and EU and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after a receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.