

Abstract
Objectives:
To examine the effect of occupation on knee osteoarthritis (OA) and total knee replacement (TKR) in working-aged adults.
Methods:
We used longitudinal data from the Chingford, Osteoarthritis Initiative (OAI) and Multicentre Osteoarthritis (MOST) studies. Participants with musculoskeletal disorders and/or a history of knee-related surgery were excluded. Participants were followed for up to 19-years (Chingford), 96-months (OAI) and 60-months (MOST) for incident outcomes including radiographic knee OA (RKOA), symptomatic RKOA and TKR. In those with baseline RKOA, progression was defined as the time from RKOA incidence to primary TKR. Occupational job categories and work-place physical activities were assigned to levels of workload. Logistic regression was used to examine the relationship between workload and incident outcomes with survival analyses used to assess progression (reference group: sedentary occupations).
Results:
Heavy manual occupations were associated with a 2-fold increased risk (OR: 2.07, 95% CI 1.03 to 4.15) of incident RKOA in the OAI only. Men working in heavy manual occupations in MOST (2.7,95% CI 1.17 to 6.26) and light manual occupations in OAI (2.00,95% CI 1.09 to 3.68) had a 2-fold increased risk of incident RKOA. No association was observed among women. Increasing workload was associated with an increased risk of symptomatic RKOA in the OAI and MOST. Light work may be associated with a decreased risk of incident TKR and disease progression.
Conclusion:
Heavy manual work carries an increased risk of incident knee OA; particularly among men. Workload may influence the occurrence of TKR and disease progression.
Keywords: Occupation, Work-place activity, Knee osteoarthritis
Introduction
Knee osteoarthritis (OA) is a global health burden and a leading cause of pain, disability and loss of work in adults [1,2]. With ageing populations, the prevalence of knee OA is set to rise substantially in the next decade and in parallel, the number of knee joint replacements [3,4]. Due to an absence of disease-modifying treatments and an increased risk of premature mortality [5], attention has turned towards identifying modifiable risk factors.
OA is multifactorial with several established risk factors including increasing age, obesity [6], female sex, and knee joint injury [7]. Occupational mechanical loading of the knee joint has also been linked to knee OA [8–10]. Most data show an elevated risk of knee OA in physically demanding jobs that involve repetitive and/or excessive levels of knee loading [11] such as farming [12,13], floor-laying [14] and mining [15]. Further, occupational work-place physical activities including squatting, prolonged kneeling, climbing and lifting/carrying have been shown to carry an increased risk of knee OA [16–18].
Studies of occupational exposure and knee OA have been predominately cross-sectional/case-control [8,9] and have focused on male-dominated occupations. There is evidence to support differences in occupational exposure patterns between men and women, even within the same job category [19,20], and the association between female workers and knee OA remains unclear [16,17,21]. Subsequently, there is a need to clarify the risk of knee OA across levels of workload within sexes. A few longitudinal studies suggest that specific occupational work-place physical activities and/or job categories are associated with incidence of knee OA [16,22,23]; though differences in outcome and exposure definitions have limited comparisons across studies.
Most costs incurred by knee OA can be attributed too joint replacement surgery [24] which can be considered a proxy outcome for endstage OA. Observational studies have shown that heavy manual jobs such as farming, fishing and crafting carry an increased risk of knee replacement particularly among men [21,25,26]. There is, however, a need to examine risk across more broad occupational categories (e.g. cleaning/housework).
Our study aimed to identify occupational exposures, including occupational job categories and work-place physical activities, that carry an increased risk of knee OA and TKR and, to examine sex differences within occupational categories.
Methods
Study sample
Data were drawn from three cohort studies which had comprehensive data on occupational exposures (i.e. occupational job categories and/or work-place physical activities) and knee OA assessment: 1) Chingford study, 2) Osteoarthritis Initiative (OAI) and 3) Multicentre Osteoarthritis Study (MOST). Our aim was to determine the risk of; i) incident radiographic knee OA (RKOA), ii) incident symptomatic RKOA, iii) incident total knee replacement (TKR) in those with baseline RKOA and iv) progression in those with baseline RKOA. Participants with baseline evidence of inflammatory arthritis (rheumatoid arthritis, gout or psoriatic arthritis) and knee-related surgery were excluded.
Chingford study
We used data from the Chingford study [27]; a UK-population level, longitudinal study of middle-aged women (≥45 years) at risk of osteoporosis/OA [5]. Participant demographics including age, body mass index (BMI) and symptom data were captured at baseline and annually. Weight-bearing anteroposterior (AP) radiographs of the knee were acquired at baseline and at follow-ups (Years 5, 10, 15 & 20); with TKR status determined at each respective visit. Whilst data are available for 23-years of follow-up [5], we used data from the first 19-years of follow-up in line with knee radiograph acquisition.
Osteoarthritis initiative
OAI is an prospective multicentre, longitudinal observational study [28] tasked with identify risk factors associated with knee OA (https://nda.nih.gov/oai/). 4796 men and women aged 45–79 years with/at risk of knee OA were recruited across four sites in the United States. Participant demographics were captured at baseline and annually until the end of investigation (108-months follow-up). Symptom data and AP weight-bearing knee radiographs were available at baseline, 12,24,48,72 and 96-months follow-up.
Multicentre osteoarthritis study
MOST is a multicentre, longitudinal cohort of participants with/at high risk of knee OA (http://most.ucsf.edu/). Men and women (N = 3026) aged between 50–79 years who were overweight, had current knee symptoms, and/or a history of knee injury/surgery were recruited across communities in Birmingham and Iowa City [29]. Patient characteristics, symptom data and weight-bearing knee radiographs were available at baseline, 30 and 60-months follow-up. Data on TKR status, indexed by study visit, was only available up to 30-months follow-up (data available as of 1st August 2019).
Exposures
In an effort to standardise occupational exposures across the three cohorts, our two occupational exposures of occupational job categories and work-place physical activities were assigned to levels of workload (sedentary to heavy manual) and were modelled in the analysis as two separate exposures respectively.
In the Chingford study, participants were asked at baseline to report their current occupational job category (e.g. farming, sales) (see Supplementary 1); categories were assigned to levels of workload (sedentary, light manual and heavy manual) [30]. Participants were also asked to report their occupational work-place physical activity ‘during a typical working week’ with responses including; i) sedentary, ii) sedentary with occasional exercise, iii) 50% sedentary and 50% active (or active housework; e.g. daily dust/hoover) and iv) predominantly manual (active all day). Such activities were assigned to increasing levels of workload (Supplementary 1) in accordance with published methods [31].
In the OAI, at each visit the Physical Activity Scale for the Elderly (PASE) survey [32] was administered; we used baseline data only. Occupational activity level in the past 7 days was captured with responses including; i) sitting, ii) sitting/standing/walking, iii) walking/handling <50 pounds (lbs) and iv) walking/handling >50 lbs. The categories were assigned to increasing levels of workload in accordance with previous methods [31]. Similarly, MOST captured occupational activity using the PASE survey though only at baseline - “What is or was your level of physical activity in the work you have done most of your adult life?”. Occupational job category was also captured at baseline (Supplementary 2). Such job categories were assigned to increasing levels of workload [30].
Outcome measures
Incident outcomes
RKOA
Knee radiographs were graded using Kellgren & Lawrence (KL) criteria [33]. In the Chingford and MOST studies, KL scoring was performed across the whole knee joint whilst in the OAI, scoring was performed for the tibio-femoral joint only. In those with no evidence of RKOA at baseline (KL<2 in both knees), incident RKOA was defined as KL≥2 in either/both knees during follow-up.
Symptomatic RKOA
In participants with no evidence of RKOA and symptoms at baseline (both knees), incident symptomatic RKOA was defined as the occurrence of knee symptoms with the presence of KL≥2, in the same knee, at least one of the visits across follow-up. Across the three cohorts, participants were classified as having ‘current knee pain’ if they reported pain for most days in the previous month; in accordance with previous guidelines [34].
In both OAI and MOST studies, symptoms were assessed using the National Health and Nutrition Examination Survey (NHANES). In the OAI, NHANES pain data were missing at baseline and so we used pain status at 12-months follow-up to define baseline symptomatic RKOA status. At early visits (12-months follow-up) participants were defined as having current knee pain if they were positive for “pain for most days of the previous month in the past 12 months”. Due to a change in questionnaire (at 24-months follow-up), current pain status was later defined as “Pain, aching or stiffness: more than half the days, past 30 days”.
In the Chingford study, participants were classified at baseline as having current knee pain if they reported the presence of pain as ‘Yes’ and duration of pain was ≥1 month in the past year. Due to a change in the questionnaire at follow-up (Year 5), the presence of painful symptoms was later defined as having painful symptoms for more than 15 days in the current month.
Incident TKR
In the Chingford study, TKR cases were identified by evidence of joint replacement seen on radiographs acquired during follow-up. Alternatively, in the OAI and in MOST, incident TKR cases were identified by date of replacement during follow-up.
Progression outcome
In those with baseline RKOA, progression of RKOA was defined as the time from date of RKOA incidence to the date of primary TKR. In the Chingford study, the exact date (dd-mm-yyyy) of replacement was not reported; rather, TKR status was recorded in discrete bands of time (5-year intervals). In OAI and MOST, the exact date of replacement was reported enabling calculation of the number of months/years from diagnosis to first surgery. It was not possible to determine the exact date of RKOA incidence across all studies and so we used the date of entry into the studies as a proxy of RKOA incidence; in those with baseline RKOA. In participants with RKOA in both knees at baseline, if TKRs occurred in both knees during follow-up we used the first occurrence as the event date.
Covariates
Baseline age, body mass index (BMI), sex, ethnicity and race were adjusted for when appropriate. It is likely that previous knee injury is on the causal pathway to knee OA and so adjustment was not performed.
Statistics
The analysis was performed using Stata (version 15.0). Participant characteristics were described using mean and standard deviation (SD) for continuous, normally distributed variables or median and interquartile range (IQR) for non-normally distributed variables.
To examine the relationship between occupational exposures (i.e. occupational job categories and work-place physical activities) and incident outcomes, we used logistic regression analyses. Results were presented as odds ratios (OR) with 95% confidence intervals (CIs) for crude and adjusted models. We simultaneously controlled for potential confounders using multiple logistic regression.
For the assessment of progression, only those with baseline RKOA were included. Using data from the Chingford study, we conducted a discrete-time hazard survival analysis. We constructed an indicator variable for whether the participant experienced the outcome (0 = no TKR, 1 =TKR) and estimated the ORs using logistic discrete-time hazard models. Analyses were adjusted for baseline age and BMI. The outcome was right censored at year 20 (19-years follow-up) and participants who were lost to follow-up, withdrew from the study before the event of interest or died were also censored. Alternatively, to model the time from baseline RKOA diagnosis to knee replacement surgery in the OAI and MOST, a time-to-event analysis was performed and hazard ratios (HRs) and 95% CIs were estimated. Models included index occupational level, with ‘sedentary’ individuals as the reference group. These models were adjusted for pre-specified potential confounders, including age, sex, BMI, race and ethnicity. The proportional hazard assumption was tested using Schoenfeld residuals test, and no violation was observed for any of the variables included. Again, the outcome was right censored at the lost to follow-up, withdrew from the study before the event of interest, died or final follow-up visit (96-months or 60-months) whichever came first. Data were unavailable for the exact number of months from entry to loss to follow-up so we used the visit prior to ‘missingness’ as the date of loss to follow-up.
For sensitivity analysis in OAI, we imputed missing baseline occupation status (N= 147) with 12-months follow-up data. Across the 3 studies, in cases of missing RKOA data across follow-up, though RKOA status was known either at the previous visit (i.e. RKOA positive) or at both the adjacent visits (i.e. RKOA negative), we used imputation to impute the missing values. We included participants who had the event prior to death and/or who were lost to follow-up and, those who did not have the event though had complete data on RKOA status up to their point of death. If participants had a missing outcome value though died within 12-months of that visit, it was assumed that the cause of the ‘missingness’ was due to the imminent death. Participants were considered to have ‘missing outcome data’ if we could not determine outcome state across follow-up; e.g. those with no evidence of RKOA at baseline though had missing RKOA data for the remainder of the study.
Results
Table 1 shows characteristics of eligible study participants with baseline RKOA data. At baseline, 551 (54.9%) participants in Chingford, 1,936 (40.4%) participants in OAI and 908 (30.0%) participants in MOST were eligible (Fig. 1). Median age across the three studies was 59.3 years and most participants were female. Counts of incident RKOA, symptomatic RKOA and TKR by study cohort and occupational exposure are shown in Appendix 1.
Table 1.
Baseline demographics of eligible study participants from the Chingford Study, OA1 and MOST for primary analysis (incident RKOA).
| Variable | Chingford Study |
OAI |
MOST |
|||
|---|---|---|---|---|---|---|
| No RKOA (N = 551) | RKOA (N = 132) | No RKOA (N= 1936) | RKOA (N = 2570) | No RKOA (N= 908) | RKOA (N = 1007) | |
| Age (years) (median, IQR) | 53 (10) | 58 (9.5) | 58 (15) | 63 (15) | 60 (12) | 64 (13) |
| Sex, n (% female) | 551 (100) | 132 (100) | 1132 (58.5) | 1452 (57.8) | 553 (60.9) | 686 (68.1) |
| Occupation: Job Category, n (%) | ||||||
| Sedentary | 211 (38.3) | 36 (27.3) | - | - | 480 (52.9) | 6.8) |
| Light Manual | 184(33.4) | 34 (25.8) | - | - | 169 (71.5) | 8.9) |
| Heavy Manual | 72 (13.1) | 15 (11.3) | - | - | 96 (10.6) | 132 (13.1) |
| Missing | 84 (15.2) | 47 (35.6) | - | - | 163 (18.0) | 214 (21.2) |
| Occupation: Work-place physical activity, n (%) | ||||||
| Sedentary | 33 (6.0) | 6 (4.5) | 423 (21.8) | 470 (18.3) | 146 (16.1) | 4.0) |
| Light | 57 (10.3) | 4 (3.0) | 596 (30.8) | 707 (27.5) | 387 (42.6) | 3.2) |
| Light Manual | 370 (67.2) | 101 (76.5) | 354 (18.3) | 455 (17.7) | 284 (31.3) | 0.1) |
| Heavy Manual | 86 (15.6) | 20 (15.2) | 48 (2.5) | 70 (2.7) | 91 (10.0) | 2.7) |
| Missing | 5 (0.9) | 1 (0.8) | 516 (26.6) | 868 (33.8) | - | - |
| BMI (kg/m 2 ) (median, IQR) | 24.4 (4.7) | 27.02 (6.3) | 26.6 (6.1) | 29.2 (6.6) | 28.7 (6.2) | 31.0 (8.0) |
| Race | ||||||
| White or Caucasian | 551 (100) | 132 (100) | 1628 (84.1) | 1934 (75.3) | 800 (88.1) | 818 (81.2) |
| Black or African American | - | 261 (13.5) | 514 (20.0) | 93 (10.2) | 7.9) | |
| Other | - | 17 (0.9) | 21 (0.8) | 15 (1.7) | 9 (0.9) | |
| Unknown/Missing | 30 (1.5) | 101 (3.9) | - | - | ||
| Ethnicity (Hispanic or Latino) | - | |||||
| Yes | - | - | 25 (1.3)1911 | 28 (1.09)2541 | 4 (0.4) | 4 (0.4) |
| No | (98.7) 0 (0) | (98.9) 1 (0.01) | 902 (99.4) | 998 (99.1) | ||
| Don’t Know (or missing) | 2 (0.2) | 5 (0.5) | ||||
| Painful Symptoms in at least 1 knee | ||||||
| Yes | 155 (28.1) | 67 (48.5) | 585 (30.2) | 1265 (49.2) | 342 (37.7) | 626 (62.2) |
| No | 396 (71.9) | 67 (50.8) | 1351 (69.8) | 1305 (50.8) | 257 (28.3) | 230 (22.8) |
| Missing | . | 1 (0.7) | 0 (0) | 0 (0) | 309 (34.0) | 151 (15.0) |
Abbreviations: OAI, Osteoarthritis Initiative, MOST, Multicentre Osteoarthritis Study, IQR, interquartile range; BM1, body mass index; SD, standard deviation, RKOA, radiographic knee osteoarthritis.
Fig. 1.
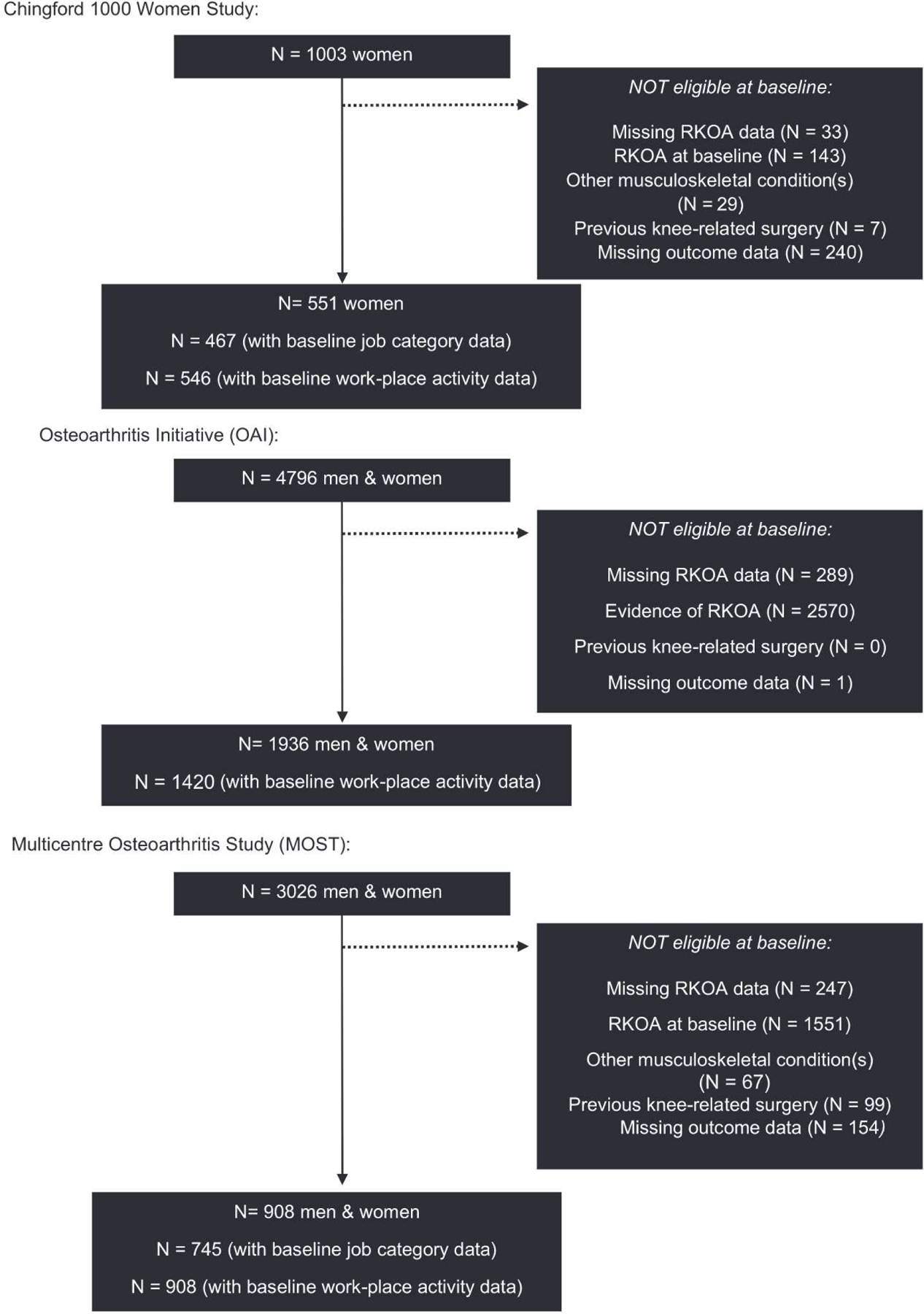
Flow chart of the studies; participants eligible for the main study investigation (incident RKOA analysis).
Risk of incident RKOA
Chingford
Using occupational job category as the occupational exposure, in multivariate analysis adjusted for baseline age and BMI there was no statistically significant association between increasing levels of workload and risk of incident RKOA (Fig. 2, Supplementary 3). Further, compared to sedentary individuals, there was no statistically significant increased risk of incident RKOA with increasing levels of work-placed physical activity in multivariate analysis; ‘light’ (OR: 1.43,95% CI 0.49 to 4.11), light manual (1.23, 95% CI 0.53 to 2.87) and heavy manual (1.49, 95% CI 0.55 to 4.03) work-place physical activities respectively (Fig. 2, Supplementary 3).
Fig. 2.
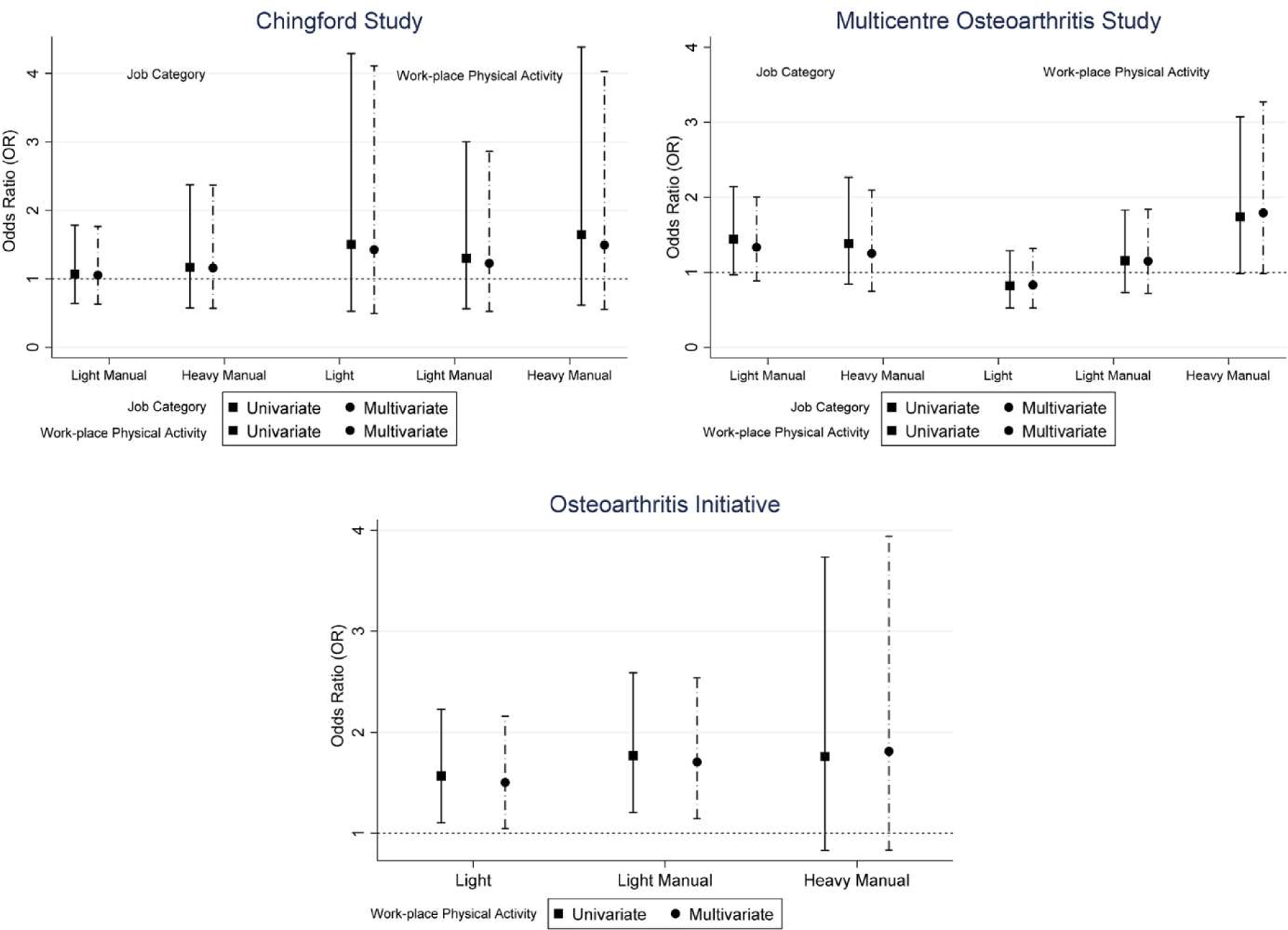
Risk of incident RKOA. (A) Results from the Chingford Study, (B) MOST and (C) OAI. The data markers indicate incidence odds ratios (OR) from primary analysis with the horizontal lines indicating 95% confidence intervals (CI).
MOST
Using occupational job category as the occupational exposure, there was no association between workload and risk of incident RKOA in multivariate models adjusted for age, BMI, sex, race and ethnicity (Fig. 2, Supplementary 3). Heavy manual work-place physical activities just failed to reach conventional levels of statistical significance in multivariate analysis (1.79,95% CI 0.98 to 3.27). Stratification by sex suggested that men working in heavy manual occupations, defined using work-place physical activity, had a 2-fold (2.7, 95% CI 1.17 to 6.26) increased risk in multivariate analysis compared to the sedentary group (Supplementary 5). No association was observed in women.
OAI
Using occupational work-place physical activity as the occupational exposure, after adjusting for baseline age, BMI, sex and race both ‘light’ (1.50, 95% CI 1.05 to 2.16) and light manual (1.71, 95% CI 1.15 to 2.54) groups were associated with a 2-fold increased risk of incident RKOA respectively (Fig. 2, Supplementary 4). After imputing missing baseline occupation status, heavy manual work-place physical activities were also associated with an increased risk of incident RKOA (2.07,95% CI 1.03 to 4.15) (Supplementary 4). When stratifying by sex, we observed a consistent association between light manual work-place physical activity and an increased risk of incident RKOA in men in multivariate (2.15,95% CI 1.14 to 4.05) and imputed models (2.00, 95% CI 1.09 to 3.68) (Supplementary 6). No association was observed in women.
Risk of incident symptomatic RKOA
Chingford
Using occupational job category as the occupational exposure, there was no association between increasing levels of workload and risk of incident symptomatic RKOA in multivariate analysis; light manual (1.07, 95% CI 0.68 to 1.67) and heavy manual groups (0.75, 95% CI 0.41 to 1.41) (Fig. 3, Supplementary 7). When using work-place physical activity as the occupational exposure, both light manual (3.33,95% CI 1.15 to 9.70) and heavy manual (3.50,95% CI 1.13 to 10.9) work-place physical activities were associated with an increased risk of incident symptomatic RKOA respectively though statistical significance was lost after adjustment for baseline age and BMI.
Fig. 3.

Risk of symptomatic RKOA. (A) Data from the Chingford Study, (B) MOST study and (C) OA1. The data markers indicate incidence odds ratios from primary analysis with the horizontal lines indicating 95% confidence intervals (CI).
MOST
Using occupational job category as the occupational exposure, there was no association between increasing levels of workload and risk of incident symptomatic RKOA (Fig. 3, Supplementary 7). Using work-place physical activity as the occupational exposure, we did, however, observe an association between heavy manual work and incident symptomatic RKOA in multivariate analysis (1.98, 95% CI 1.03 to 3.82); this relationship was maintained in men only in multivariate (3.56, 95% CI 1.33 to 9.57) analysis (see Supplementary 9). No association was observed in women.
OAI
Using work-place physical activity as the occupational exposure, ‘light’ (1.30, 95% CI 1.03 to 1.65) work-place physical activities were associated with an increased risk of incident symptomatic RKOA after adjusting for baseline age, sex, BMI and race (Fig. 3, Supplementary 8). After imputation, light manual work-place physical activities also carried an increased risk of incident symptomatic RKOA (1.29, 95% CI 1.00 to 1.65) though no association was observed between heavy manual work-place physical activity and risk of incident symptomatic RKOA (1.38, 95% CI 0.83 to 2.27). Men working in ‘light’ and light manual occupations were consistently at greater risk of incident symptomatic RKOA in multivariate and imputed models (Supplementary 10). No association was observed in women.
Risk of incident TKR
Chingford
Using occupational job category as the occupational exposure, no association was observed between light manual (0.94, 95% CI 0.07 to 12.14) and heavy manual (1.56, 95% CI 0.1 to 23.22) occupations and risk of incident TKR in those with baseline RKOA (Supplementary 11). We were unable to determine the odds of TKR when using work-place physical activity as all TKRs occurred within the light manual category.
MOST & OAI
In MOST, there was no association between work-place physical activity and risk of incident TKR in those with baseline RKOA in univariate analysis (Supplementary 11). However, in multivariate analysis there was a negative, statistically significant association between ‘light’ work and risk of TKR (0.53, 95% CI 0.29 to 0.97). Using job category as the occupational exposure, there was no association between workload and risk of incident TKR. Using data from the OAI, there was no association between work-place activity and risk of incident TKR (Supplementary 11).
Progression of disease to TKR
There was no association between occupational exposures (i.e. job category and/or work-place physical activity) and progression of disease in those with baseline RKOA across Chingford and OAI studies (Supplementary 12 & 14). However, using work-place physical activity as the occupational exposure, in MOST ‘light’ workload was statistically significantly associated with a decreased risk of RKOA progression in multivariate analysis (HR: 0.53,95% CI 0.3 to 0.94) (Supplementary 13).
Discussion
This study is the first to examine the relationship between occupation and risk of knee OA using three, large, long-term studies of persons at risk of OA. Using work-place physical activity as the occupational exposure, we observed a relationship between increasing levels of workload and risk of incident RKOA in the OAI with heavy manual work associated with a 2-fold increased risk compared to sedentary workers (OR: 2.07, 95% CI 1.03 to 4.15); no relationship was observed in Chingford and MOST studies. Further, ‘light’ (1.26, 95% CI 1.01 to 1.57) and light manual (1.29,95% CI 1.00 to 1.65) occupations in the OAI and, heavy manual occupations (1.98, 95% CI 1.03 to 3.82) in MOST were associated with up to a 2-fold increased risk of incident symptomatic RKOA. Levels of workload may influence the occurrence of TKR and disease progression.
We hypothesised that exposure to high levels of manual loading may be less frequent in women [19,35] which may explain the absence of an association in the Chingford study. When stratifying by sex in the OAI and MOST, men working in either light manual or heavy manual work were at an increased risk of incident knee OA compared to sedentary workers; no association was observed in women. Our findings are consistent with previous studies. The Framingham Heart Study showed that men working in occupations entailing knee bending combined with medium to very heavy physical demands had a >2-foId increased risk of incident RKOA compared to occupations without knee bending (2.22, 95% CI 1.38 to 3.58); no such association was reported in women [16]. Such sex differences could be due to differences in the interpretation of low, medium and heavy ‘physical demands’. Further, the differences in occupational exposure patterns across men and women are well known. For instance, within the same occupation men are more likely to report exposure to whole body vibration compared to women [19] which is a known risk factor for knee OA [10]. Subsequently, differences between sexes in the amount of time spent performing specific occupational tasks and time spent in non-neutral task-specific postures [36], within the same occupation, may explain in part the observed differences between men and women.
We observed a relationship between ‘light’ work-place physical activity and a decreased risk of incident TKR in MOST. Workers with knee OA in physically demanding jobs may seek healthcare more frequently due to a greater chance of work-place injury. This may lead to better management of their disease thereby delaying/preventing the need for TKR. Alternatively, there is some evidence to suggest that certain levels of physical activity may be protective to TKR in those with OA [37] with a potential mechanism of muscle strengthening [38].
This study has several strengths. Firstly, we used data from three, large, high-quality cohort studies with extensive follow-up periods. This allowed us to explore the long-term temporal effects of occupational exposures on incident outcomes and to cross-validate across sexes. We described the effect of occupation on knee OA using two measures of workload; occupational job categories (e.g. farming) and work-place physical activities (e.g. carrying <50 lbs). Whilst occupational job categories may be less prone to recall bias, it is perhaps a less accurate measure of occupational exposure compared to the reporting of specific occupational work-place physical activities. We observed a relationship between both occupational exposures and an increased risk of knee OA which would support the robustness of our findings. The magnitude of the effect was however, greatest when using work-place physical activity as the exposure.
This study has several potential limitations. Firstly, as in all previous occupation-based cohort studies, occupational exposures are difficult to define and validate. In our study, all occupation data used were collected at baseline; with the exception of imputation in the OAI in which we used 12-month follow-up data. Questionnaires are subject to recall bias and data collected at baseline may not reflect long-term occupational status. Further, whilst the job categories used may have accurately reflected levels of workload in the 1980–2000’s (time of collection), due to changes in work regulations and, health and safety laws, jobs have evolved and may not necessarily reflect current levels of workload thereby limiting the generalisability of our findings. More so, the questions asked related to occupational status in the baseline questionnaires in Chingford, OAI and MOST studies varied slightly; we acknowledge this as a limitation. Future occupational studies of knee OA would benefit from more frequent capture of occupational exposure data. This is likely to be more feasible in the current age with the introduction of continuous monitoring using smart devices; this would ultimately help to minimize occupational exposure misclassification in epidemiology studies.
We attempted to harmonise outcome and exposure data across all three studies, though variation in study procedures prevented complete coherence. For instance, definitions of incident symptomatic RKOA varied across the three cohorts; we did however, harmonise in accordance with previously published guidelines [34]. Further, whilst we adhered to the conventional definition of knee OA (KL≥2), radiographic assessments varied across studies. In both the Chingford and MOST studies, KL≥2 was defined as definite osteophytes and joint space narrowing (JSN), whilst in the OAI KL≥2 was equal to the occurrence of definite osteophytes and questionable JSN. Osteophyte development with JSN is considered a stricter definition of RKOA [39] which could explain variance in our findings due to differences in incidence rates.
Despite using data from three large studies to investigate the effects of occupational exposures on the occurrence of TKRs, we were limited by power due to low incidence rates. Because of differences in study design, Chingford is a population-level cohort whilst MOST and OAI are enhanced with specific study populations, we felt it more appropriate to analyse the cohorts separately rather than combining all study participants. Our study focused on the impact of ‘current occupation’, which does not account for exposure to previous occupations/occupational tasks. Differences in the phrasing of the occupation-related questions may have also contributed to the differences seen across studies.
Conclusions
Compared to sedentary occupations, heavy manual work was associated with an increased risk of incident knee OA; particularly in men. No associations were observed between occupational exposures and incident and progression outcomes in women. Low levels of workload may protect against the occurrence of TKR and disease progression.
Supplementary Material
Acknowledgements
We would like to thank all the participants of the Chingford study, Professor Tim Spector, Dr Deborah Hart, Dr Alan Hakim, Maxine Daniels, Alison Turner and James Van Santen for their time and dedication and Versus Arthritis (formerly Arthritis Research UK) for their funding support to the study and the Oxford NIHR Musculoskeletal Biomedical Research Unit for funding contributions. We would also like to express our gratitude to the participants of MOST and OAI. Further, we would like to thank Professor Karen Walker-Bone for her expertise on the project. The Multicenter Osteoarthritis (MOST) Study was funded by the National Institute on Aging (NIA) under award numbers U01AG18820 (PI: Felson), U01AG18832 (PI: Torner), U01AG18947 (PI: Lewis), and U01AG19069 (PI: Nevitt). The OAI is a public-private partnership comprised of five contracts (NOl-AR-2-2258, NOl-AR-2-2259, NOl-AR-2-2260, NOl-AR-2-2261, NOl-AR-2-2262) funded by the National Institutes of Health, a branch of the U.S. Department of Health and Human Services, in four clinical sites and conducted by the OAI study investigators. Private funding partners include Merck Research Laboratories, Novartis Pharmaceuticals Corporation, GlaxoSmithKline, and Pfizer Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. The funders had no role in the design of this study; collection, analysis and interpretation of data; preparation of the manuscript; or the decision to submit the manuscript for publication.
Funding
This work was supported by Merck Serono Pty. Professor Hunter is supported by an Australian National Health and Medical Research Council (NHMRC) Practitioner Fellowship. The funders were not involved in the study design, data collection or interpretation.
Appendix
Appendix 1. Number of incident cases across study cohorts and occupational exposures.
| Study Cohort | Radiographic Knee OA (RKOA) | Symptomatic RKOA | Total Knee Replacement (TKR) |
|---|---|---|---|
| Chingford Study | |||
| Job category | 382 (82.0%) | 134 (29.1%) | 4 (8.5%) |
| Work-Place Physical Activity | 441 (80.8%) | 163 (30.0%) | 4 (8.5%) |
| Osteoarthritis Initiative | |||
| (work-place physical activity only) | 252 (17.8%) | 629 (25%) | 269 (15.8%) |
| MOST | |||
| Job category | 182 (24.4%) | 163 (22.2%) | 65 (8.2%) |
| Work-Place Physical Activity | 229 (25.2%) | 209 (23.0%) | 94 (9.3%) |
Footnotes
Availability of data and materials
All data generated and analysed in this study are available upon reasonable request. Access to data generated in this report should be sent to the corresponding author at thomas.perry@ndorms.ox.ac.uk whilst requests for the individual cohort data should be submitted to the cohort principle investigators.
Public and Patient Involvement (PPI) statement
PPI was not required nor involved with any aspect of the work presented.
Ethical approval
Ethical approval was not required for any aspect of the work presented in this manuscript.
Declaration of Competing Interest
TAP, XW, MS, CG, LG and CP declare no conflicts of interest. DJH provides consulting advice for Pfizer, Lilly, TLC bio and Merck Serono. NKA has received honorariums from Novartis, Alliance for Better Health, and Lilly; held advisory board positions (which involved receipt of fees) at Merck, Merck Sharp and Dohme, Roche, Novartis, Smith and Nephew, Q-MED, Nicox, Servier, GlaxoSmithKline, Schering-Plough, Pfizer, and Rottapharm; and received consortium research grants from Alliance for Better Bone Health, Amgen, Novartis, Merck Sharp and Dohme, Servier, Eli Lilly, and GlaxoSmithKline; he has no other relationships or activities that could appear to have influenced the submitted work. All fees did not exceed more than $10,000 for each item listed under consulting fees, speaking fees, or honoraria.
Supplementary materials
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.semarthrit.2020.08.003.
References
- [1].Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380(9859):2197–223. [DOI] [PubMed] [Google Scholar]
- [2].Sharif B, Garner R, Sanmartin C, Flanagan WM, Hennessy D, Marshall DA. Risk of work loss due to illness or disability in patients with osteoarthritis: a population-based cohort study. Rheumatology 2016;55(5):861–8. [DOI] [PubMed] [Google Scholar]
- [3].Patel A, Pavlou G, Mujica-Mota RE, Toms AD. The epidemiology of revision total knee and hip arthroplasty in England and Wales: a comparative analysis with projections for the United States. A study using the National Joint Registry dataset. Bone Joint J 2015;97-B(8):1076–81. [DOI] [PubMed] [Google Scholar]
- [4].Culliford DJ, Maskell J, Beard DJ, Murray DW, Price AJ, Arden NK. Temporal trends in hip and knee replacement in the United Kingdom: 1991 to 2006. J Bone Joint Surg Br 2010;92( 1): 130–5. [DOI] [PubMed] [Google Scholar]
- [5].Kluzek S, Sanchez-Santos MT, Leyland KM, Judge A, Spector TD, Hart D, et al. Painful knee but not hand osteoarthritis is an independent predictor of mortality over 23years follow-up of a population-based cohort of middle-aged women. Ann Rheum Dis 2016;75(10):1749–56. [DOI] [PubMed] [Google Scholar]
- [6].Lohmander LS, Gerhardsson de Verdier M, Rollof J, Nilsson PM, Engstrom G. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population-based prospective cohort study. Ann Rheum Dis 2009;68(4):490–6. [DOI] [PubMed] [Google Scholar]
- [7].Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4–6 fold after knee injury - a systematic review and meta-analysis. Br J Sports Med 2019. [DOI] [PubMed] [Google Scholar]
- [8].Palmer KT. Occupational activities and osteoarthritis of the knee. Br Med Bull 2012;102:147–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].McWilliams DF, Leeb BF, Muthuri SG, Doherty M, Zhang W. Occupational risk factors for osteoarthritis of the knee: a meta-analysis. Osteoarthritis Cartilage 2011;19(7):829–39. [DOI] [PubMed] [Google Scholar]
- [10].Gignac MAM, Irvin E, Cullen K, Van Eerd D, Beaton DE, Mahood Q, et al. Men and women’s occupational activities and the risk of developing osteoarthritis of the knee, hip, or hands: a systematic review and recommendations for future research. Arthritis Care Res (Hoboken) 2020;72(3):378–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Wang X, Perry TA, Arden N, Chen L, Parsons CM, Cooper C, et al. Occupational risk in knee osteoarthritis: a systematic review and meta-analysis of observational studies. Arthritis Care Res (Hoboken) 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Croft P, Coggon D, Cruddas M, Cooper C. Osteoarthritis of the hip: an occupational disease in farmers. Bmj 1992; 304(6837): 1269–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Holmberg S, Thelin A, Thelin N. Is there an increased risk of knee osteoarthritis among farmers? A population-based case-control study. Int Arch Occup Environ Health 2004;77(5):345–50. [DOI] [PubMed] [Google Scholar]
- [14].Jensen LK, Mikkelsen S, Loft IP, Eenberg W, Bergmann I, Logager V. Radiographic knee osteoarthritis in floorlayers and carpenters. Scand J Work Environ Health 2000;26(3):257–62. [DOI] [PubMed] [Google Scholar]
- [15].McMillan G, Nichols L Osteoarthritis and meniscus disorders of the knee as occupational diseases of miners. Occup Environ Med 2005;62(8):567–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Felson DT, Hannan MT, Naimark A, Berkeley J, Gordon G, Wilson PW, et al. Occupational physical demands, knee bending, and knee osteoarthritis: results from the Framingham Study. J Rheumatol 1991;18(10):1587–92. [PubMed] [Google Scholar]
- [17].Coggon D, Croft P, Kellingray S, Barrett D, McLaren M, Cooper C. Occupational physical activities and osteoarthritis of the knee. Arthritis Rheum 2000:43 (7):1443–9. [DOI] [PubMed] [Google Scholar]
- [18].Cooper C, McAlindon T, Coggon D, Egger P, Dieppe P. Occupational activity and osteoarthritis of the knee. Ann Rheum Dis 1994;53(2):90–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Eng A, t Mannetje A, McLean D, Ellison-Loschmann L, Cheng S, Pearce N. Gender differences in occupational exposure patterns. Occup Environ Med 2011;68 (12):888–94. [DOI] [PubMed] [Google Scholar]
- [20].Locke SJ, Colt JS, Stewart PA, Armenti KR, Baris D, Blair A, et al. Identifying gender differences in reported occupational information from three US population-based case-control studies. Occup Environ Med 2014;71(12):855–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Franklin J, Ingvarsson T, Englund M, Lohmander S. Association between occupation and knee and hip replacement due to osteoarthritis: a case-control study. Arthritis Res Ther2010;12(3):R102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Toivanen AT, Heliovaara M, Impivaara O, Arokoski JPA, Knekt P, Lauren H, et al. Obesity, physically demanding work and traumatic knee injury are major risk factors for knee osteoarthritis-a population-based study with a follow-up of 22 years. Rheumatology (Oxford) 2010;49(2):308–14. [DOI] [PubMed] [Google Scholar]
- [23].Andersen S, Thygesen LC, Davidsen M, Helweg-Larsen K. Cumulative years in occupation and the risk of hip or knee osteoarthritis in men and women: a register-based follow-up study. Occup Environ Med 2012;69(5):325–30. [DOI] [PubMed] [Google Scholar]
- [24].Price AJ, Alvand A, Troelsen A, Katz JN, Hooper G, Gray A, et al. Knee replacement. Lancet (London, England) 2018;392(10158):1672–82. [DOI] [PubMed] [Google Scholar]
- [25].Leung YY, Bin Abd Razak HR, Talaei M, Ang L-W, Yuan J-M, Koh W-P. Duration of physical activity, sitting, sleep and the risk of total knee replacement among Chinese in Singapore, the Singapore Chinese Health Study. PLoS One 2018:13(9): e0202554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Apold H, Meyer HE, Nordsletten L, Furnes O, Baste V, Flugsrud GB. Risk factors for knee replacement due to primary osteoarthritis, a population based, prospective cohort study of 315,495 individuals. BMC Musculoskelet Disord 2014:15:217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Hart DJ, Doyle DV, Spector TD. Incidence and risk factors for radiographic knee osteoarthritis in middle-aged women: the Chingford Study. Arthritis Rheum 1999;42(1): 17–24. [DOI] [PubMed] [Google Scholar]
- [28].Eckstein F, Wirth W, Nevitt MC Recent advances in osteoarthritis imaging the osteoarthritis initiative. Nat Rev Rheumatol 2012;8(10):622–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Segal NA, Nevitt MC, Gross KD, Gross KD, Hietpas J, Glass NA, et al. The Multicenter Osteoarthritis Study: opportunities for rehabilitation research. Pm R 2013;5 (8):647–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Parsons CM, Gates LS, Perry T, Nevitt M, Felson D, Sanchez-Santos MT, et al. Pre-dominant lifetime occupation and associations with painful and structural knee osteoarthritis: an international participant-level cohort collaboration. Osteoarthritis Cartilage Open 2020:100085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Gates LS, Leyland KM, Sheard S, Jackson K, Kelly P, Callahan LF, et al. Physical activity and osteoarthritis: a consensus study to harmonise self-reporting methods of physical activity across international cohorts. Rheumatol Int 2017;37 (4):469–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Washburn RA, Montoye HJ. The assessment of physical activity by questionnaire. Am J Epidemiol 1986;123(4):563–76. [DOI] [PubMed] [Google Scholar]
- [33].Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis 1957; 16(4):494–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Leyland KM, Gates LS, Nevitt M, Felson D, Bierma-Zeinstra SM, Conaghan PG, et al. Harmonising measures of knee and hip osteoarthritis in population-based cohort studies: an international study. Osteoarthritis Cartilage 2018;26(7):872–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Aittomaki A, Lahelma E, Roos E, Leino-Arjas P, Martikainen P. Gender differences in the association of age with physical workload and functioning. Occup Environ Med 2005;62(2):95–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Heilskov-Hansen T, Svendsen SW, Frolund Thomsen J, Mikkelsen S, Hansson G-A. Sex differences in task distribution and task exposures among Danish house painters: an observational study combining questionnaire data with biomechanical measurements. PLoS One 2014;9(11):e110899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Ageberg E, Engstrom G, Gerhardsson de Verdier M, Rollof J, Roos EM, Lohmander LS. Effect of leisure time physical activity on severe knee or hip osteoarthritis leading to total joint replacement: a population-based prospective cohort study. BMC Musculoskelet Disord 2012:13:73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Culvenor AG, Wirth W, Ruhdorfer A, Eckstein F. Thigh muscle strength predicts knee replacement risk independent of radiographic disease and pain in women: data from the osteoarthritis initiative. Arthritis Rheumatol 2016;68(5):1145–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Schiphof D, Boers M, Bierma-Zeinstra SMA. Differences in descriptions of Kellgren and Lawrence grades of knee osteoarthritis. Ann Rheum Dis 2008;67(7): 1034–6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.