

Sir,
Prevotella species are anaerobic bacteria that form part of the oral microbiota and upper respiratory and genitourinary tracts. They are usually associated with oral infections, but it can be also observed in some other infections such as skin and soft tissue, and pleuropulmonary infections. Until now, there are only few reports on pleural infection published in the literature caused by Prevotella species and obtained in pure culture [1-7]. We here present two additional and uncommon cases of pleural infection caused by Prevotella species and a review of the cases previously published.
Case 1.- A 60-year-old man was admitted due to chest pain, general malaise and vomiting. Blood analysis showed increased levels of glucose (198 mg/dL), urea (200 mg/dL), creatinine (1.53 mg7dL), procalcitonin (65.26 ng/mL), AST (437 U/L), and ALT (308 U/L). A physical exam showed cervical edema, and a cervico-thoracic CT scan showed great quantity of gas affecting cervical region and mediastinum (Figure 1) along with a pleural effusion. A diagnosis of mediastinitis was established and a thoracotomy was performed along with drainage of pleural effusion as well. Treatment with piperacillin-tazobactam and linezolid was started.
Figure 1.
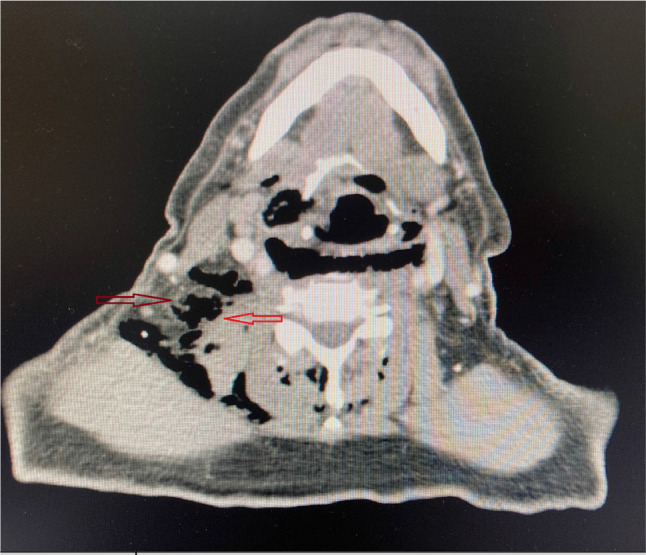
Cervical CT scan showing a big quantity of gas corresponding to a mediastinitis.
Case 2.- A 47-year-old woman was admitted due to drowsiness and inability to emit language and open the eyes. Blood analysis showed increased levels of glucose (150 mg/dL), sodium (105 mEq/L), C-reactive protein (42.7 mg/L) and decreased levels of potassium (3.10 mEq/L), chlorine (80 mEq/L) and white cell count (3.44 x 103/mm3). A brain CT scan was performed showing no abnormalities. The patient was admitted to the ICU and treatment with fluid and electrolyte replacement was initiated. A hormonal study was performed showing increased levels of TSH (31.59), antibodies anti-peroxidase (>1000 UI/mL) and decreased levels of thyroxine (<0.28 ng/dL). Moreover, the antinuclear antibodies were positives. The patient was diagnosed of systemic lupus erythematosus and myxedematous coma. Later, a chest ultrasound revealed a left pleural effusion; drainage was then performed.
Both pleural fluids were sent to the microbiology laboratory for culture. The two samples were inoculated onto both aerobic and anaerobic blood agar (Becton Dickinson), chocolate agar (Becton Dickinson), and thioglycolate broth (Becton Dickinson), incubating all media at 37º C for 5 days. Gram staining of both fluids exhibited abundant Gram-negative rods. On the second day of incubation, numerous colonies of microorganisms were observed in pure culture on anaerobic blood agar alone in both samples. MALDI-TOF MS (Bruker Biotyper, Billerica, MA) results identified the strains as P. oris and P. denticola (log scores of 2.20 in case 1 and 2.14 in case 2). Biotyper software version 9 was used (8468 msp) for analyses. The two strains were sent to the Centre of Genomic and Oncologic Research (GENYO, Granada, Spain) for 16S rRNA gene sequence analysis using a previously reported method [8]. Fragments of 1,363 bp (case 1) and 1,357 bp (case 2) were obtained. The strain from case 1 showed 99.42% similarity with the P. oris strain NCTC 13071 GenBank sequence (accession nº LR134384.1) and the strain from case 2, 99.2% similarity with the P. denticola strain SEQ210 17855 GenBank sequence (accession nº JN867285.1). 16S rRNA gene sequences of the isolates were submitted to GenBank (accession number OM909079 for case 1 and ON248549 for case 2).
The gradient diffusion strip method (Etest bioMérieux) was used for antimicrobial susceptibility testing based on 2022 EUCAST criteria [9]. MIC values for the strain isolated in case 1 were benzylpenicillin (0.125 mg/L), piperacillin-tazobactam (<0.016 mg/L), clindamycin (0.047 mg/L), meropenem (0.012 mg/L), and metronidazole (0.19 mg/L). Values for the strain isolated in case 2 were benzylpenicillin (8 mg/L), piperacillintazobactam (0.032 mg/L), clindamycin (>256 mg/L), meropenem (0.047 mg/L), and metronidazole (1 mg/L). In case 1, the patient rapidly developed to septic shock and dead after 6 days. In case 2, the patient was prescribed i.v. meropenem (500 mg/8 h) for 20 days and was discharged after 40 days.
Pleural infections caused by anaerobic bacteria are usually of polymicrobial nature, presented as mixed infections containing aerobes and anaerobes. We here reported two cases of pleural infection due to P. oris and P. denticola in pure culture. Table 1 shows the main characteristics of patients with pleural infections due to Prevotella spp.
Table 1.
Main characteristics of Prevotella pleural infections.
| Case (year of publication) [reference] |
Age (years)/sex | Prevotellaspecies | Identification method | Underlying conditions and/or risk factors | Possible source of infection | Clinical manifestations | CRP (mg/L) | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 (2013) [2] | 17/M | Prevotellaspp | PCR (16S rRNA) | NR | NR | Fever, cough, chest pain | NR | Antibiotics + drainage | Cure |
| 2 (2015) [5] | 76/M | Prevotellaspp | PCR (16S rRNA) | DM | NR | Fever, chest pain | 147.4 | Antibiotics + drainage | Cure |
| 3 (2018) [3] | 88/M | Prevotelladentalis | MALDI-TOF MS PCR (16S rRNA) |
CRD DM |
Lung | Chronic pleural effusion | 194.1 | Antibiotics + drainage | Died |
| 4 (2020) [5] | 42/M | Prevotellaoris | NR | DM | Lung | Chest pain, left upper limb weakness, cough | 399 | Antibiotics + drainage | Cure |
| 5 (2021) [6] | 12/M | Prevotellapleuritidis | Next-generation sequencing-based clinical metagenomics | DM | Lung | Fever, cough, chest pain, dyspnea | NR | Antibiotics + drainage | Cure |
| 6 (2021) [7] | 49/M | Prevotellaspp | PCR (16S rRNA) | NR | Lung | Asthenia, fever, weight loss, dyspnea | 87.5 | Antibiotics + thoracoscopic surgery | Cure |
| 7 (2022) [PR] | 60/M | Prevotellaoris | MALDI-TOF MS PCR (16S rRNA) |
Mediastinitis | Lung | Chest pain, general malaise, vomiting | Normal | Antibiotics + drainage | Died |
| 8 (2022) [PR] | 47/F | Prevotelladenticola | MALDI-TOF MS PCR (16S rRNA) |
Autoimmune disease | NR | Drowsiness, inhability to emit language | 42.7 | Antibiotics + drainage | Cure |
M: male; F: female; NR: not reported; CRP: C-reactive protein; PR: present report; DM: diabetes mellitus; CRD: chronic respiratory disease.
The introduction of MALDI-TOF MS for routine analyses in clinical laboratories has improved the identification of anaerobic bacteria and may help to detect new species. Last years, antimicrobial resistance is increasing among anaerobic bacteria worldwide. Prevotella species have been traditionally considered susceptible to penicillin, but an increasing rate of resistance to this drug has been documented over recent years, ranging from 33% to 60%, especially in P. bivia [10,11]. Thus, empirical treatment with penicillin cannot be recommended in infections caused by Prevotella species. Regarding to metronidazole, some studies reported resistance of some Prevotella strains to this drug [12,13]. The above findings indicate that Prevotella species cannot be considered as usually susceptible to antibiotics. Antimicrobial resistance of Prevotella spp. and other anaerobes is an emerging problem that warrants closer antimicrobial surveillance, increased resistance testing, and the stringent monitoring of treatment failures.
This is a report of two additional cases of P. oris and P. denticola as cause of pleural effusion and indicates that Prevotella species can produce infections in pure culture at this location. These case reports and recent observations of antimicrobial resistance among Prevotella species highlight the need for caution when treating these infections with antibiotics and for the susceptibility testing of Gram-negative anaerobes in all cases.
FUNDING
None to declare
CONFLICT OF INTEREST
Authors declare no conflict of interest.
References
- 1.Cobo F, Calatrava E, Rodríguez-Granger J, Sampedro A, AliagaMartínez L, Navarro-Marí JM. A rare case of pleural effusion due to Prevotella dentalis. Anaerobe 2018; 54: 144-145. DOI: 10.1016/j.anaerobe.2018.09.004. [DOI] [PubMed] [Google Scholar]
- 2.Rayment JH, Weinstein M. An unusual cause of empyema in a teenage boy. CMAJ 2013; 185: 1151-1153. DOI: 10.1503/cmaj.122089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhou H, Shen Y, Shen Q, Zhou J. Thoracic empyema caused by Prevotella spp. diagnosed using 16S rDNA sequence analysis. Clin Respir J 2015; 9: 121-124. DOI: 10.1111/crj.12106. [DOI] [PubMed] [Google Scholar]
- 4.Sakamoto M, Ohkusu K, Masaki T, Kako H, Ezaki T, Benno Y. Prevotella pleuritidis sp. nov., isolated from pleural fluid. Int J Syst Evol Microbiol 2007; 57: 1725-1728. DOI: 10.1099/ijs.0.64885-0. [DOI] [PubMed] [Google Scholar]
- 5.Abufaied M, iqbal P, Yassin MA. A rare and challenging presentation of empyema necessitans/necessitasis leading to braquial plexopathy. Cureus 2020; 12: e8267. DOI: 10.7759/cureus.8267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Galliguez T, Tsou PY, Cabrera A, Fergie J. Next-generation sequencing-based clinical metagenomics identifies Prevotella pleuritidis in a diabetic adolescent with large parapneumonic effusion and negative growth of pleural fluid culture: a case report. Br j Biomed Sci 2021; 78: 101-105. DOI: 10.1080/09674845.2020.1827846. [DOI] [PubMed] [Google Scholar]
- 7.Diesler R, Kiakouama-Maleka L. A challenging case of thoracic empyema caused by Prevotella spp. Respir med Case Rep 2021; 35: 101567. DOI: 10.1016/j.rmcr.2021.101567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Klindworth A, Pruesse E, Schweer T, Peplies J, Quast C, Horn M, et al. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Research 2013; 41: e1-e1. DOI: 10.1093/nar/gks808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.European Committee on antimicrobial susceptibility testing . Breakpoint tables for interpretation of MICs and zone diameters. Version 12.0, 2022. http://eucast.org. Checked data: 04/21/2022.
- 10.Bancescu G, Didilescu A, Bancescu A, Bari M. Antibiotic susceptibility of 33 Prevotella strains isolated from Romanian patients with abscesses in head and neck spaces. Anaerobe 2015; 35: 41-44. DOI: 10.1016/j.anaerobe.2014.10.006. [DOI] [PubMed] [Google Scholar]
- 11.Jeverica S, Kolenc U, Mueller-Premru M, Papst L. Evaluation of the routine antimicrobial susceptibility testing results of clinically significant anaerobic bacteria in a Slovenian tertiary-care hospital in 2015. Anaerobe 2017; 47: 64-69. DOI: 10.1016/j.anaerobe.2017.04.007. [DOI] [PubMed] [Google Scholar]
- 12.Mory F, Carlier JP, Alauzet C, Thouvenin M, Schuhmacher H, Lozniewski A. Bacteremia caused by a metronidazole-resistant Prevotella sp strain. J Clin Microbiol 2005; 43: 5380-5383. DOI: 10.1128/JCM.43.10.5380-5383.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alauzet C, Mory F, Teyssiere C, et al. Metronidazole resistance in Prevotella spp. and description of a new nim gene in Prevotella baroniae. Antimicrob Agents Chemother 2010; 54: 60-64. DOI: 10.1128/AAC.01003-09. [DOI] [PMC free article] [PubMed] [Google Scholar]