

Abstract
Lung adenocarcinoma is a common cancer; even though it has a strong association with previous smoking, there has been described nonsmokers‐related cases. Symptoms varies from asymptomatic to hemoptysis or pleural effusion. We describe a case of a patient who presented with painful scapula as primary manifestation of advanced pulmonary malignancy.
Keywords: bone metastases, lung adenocarcinoma, non‐small cell lung cancer, palliative radiotherapy, targeted therapy
This case report seeks to highlights the role of the interprofessional team in the management of advanced adenocarcinoma of the lung.
A healthy 58‐year‐old woman presented with right shoulder pain radiated to scapula for several weeks. She denied trauma, cough, respiratory symptoms, neither weight‐loss; referred pain persisted despite physiotherapy and painkillers. Vital signs unremarkable, physical examination with mild tenderness to palpation of the scapula, without swelling or myopenia, normal mobility testing, and rotator cuff examination. To evaluate osseous structures integrity and anatomic relationship in the shoulder girdle, an X‐ray was ordered, demonstrating in pulmonary parenchyma a well‐circumscribed oval soft‐tissue density mass in the right upper lobe of 58 × 51 mm (Figure 1).
FIGURE 1.
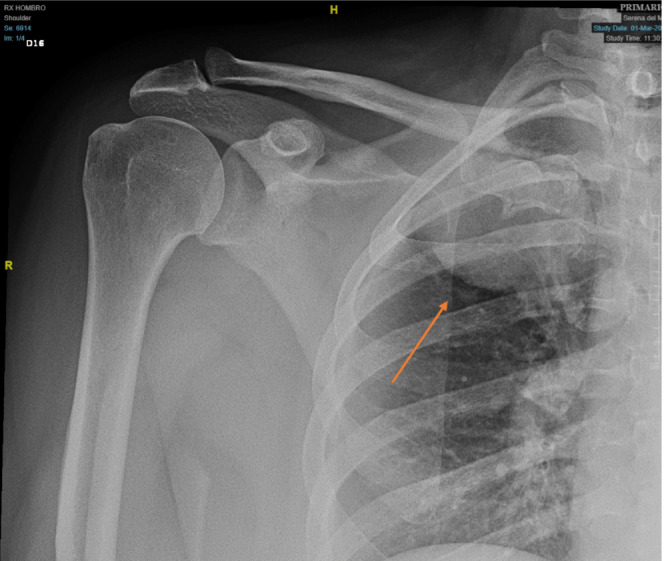
Shoulder X‐ray: in the right upper lobe, a well‐circumscribed mass is observed (orange arrow).
Suspecting malignancy and following NCCN Guidelines complementary staging studies were performed (Figures 2 and 3), brain and abdominal metastases were rule‐out. 1
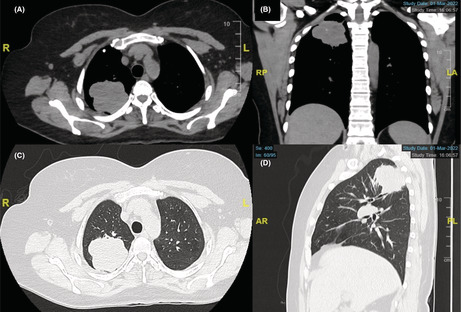
FIGURE 2.
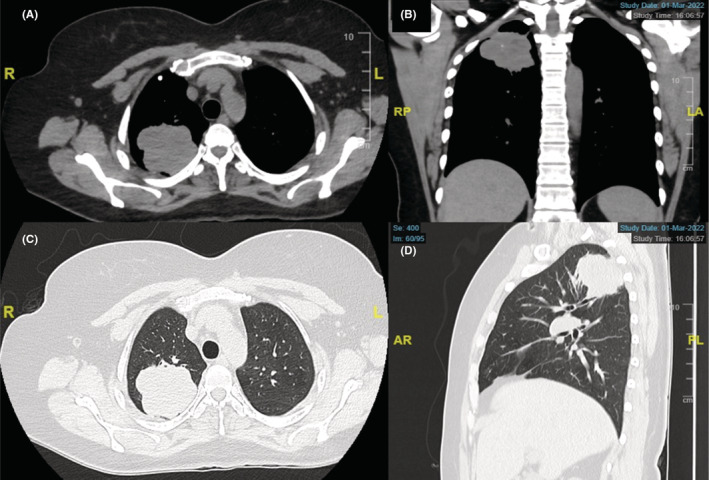
Chest CT: (A, C) axial view, (B) coronal view, (D) sagittal view; revealing an oval well‐circumscribed mass projected at the right lung apex.
FIGURE 3.
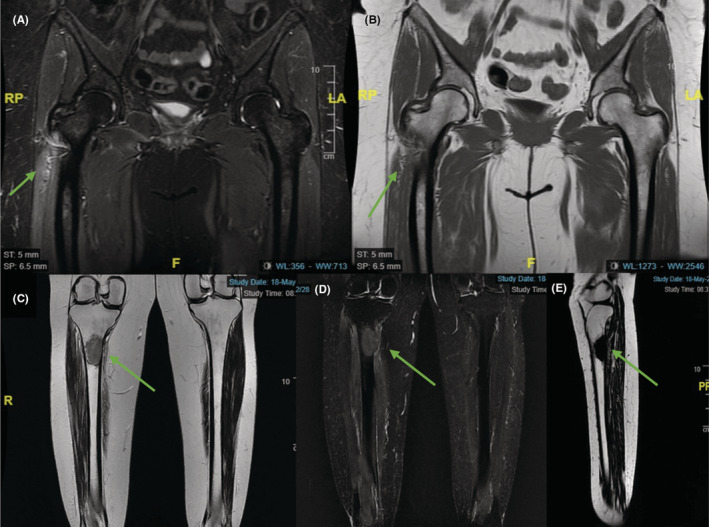
(A) Pelvis MRI coronal STIR sequence, (B) Pelvis MRI T1‐FSE sequence revealing a focal lesion in the lateral and inferior aspect of the right greater trochanter, which replaces the bone marrow, with apparent cortical disruption and associated bone marrow edema, which presents diffuse and homogeneous enhancement after the administration of intravenous contrast medium (green arrows). (C) MRI lower leg coronal T2 images, (D) MRI lower leg coronal STIR FSE sequence, (E) MRI lower leg sagittal DP FSE sequence identifying in the proximal diaphysis of the right tibia, of intramedullary location, a lesion that generates bone marrow replacement, with compromise of the posterior cortical of the tibia and exophytic component. The diameters of the lesion are longitudinal: 50.2 mm, transverse: 25 mm and anteroposterior 33 mm, its upper border is 44 mm from the tibial eminence and its lower margin is 26.6 cm from the tibiotalar joint as reference points (green arrows).
Histopathology confirmed a non‐small cell lung cancer stage IV (T3N2M1) positive for EGFR mutation, an unresectable stage. Targeted therapy (tyrosine kinase inhibitor: osimertinib) was given, orthopedic oncology stabilization surgery was performed prophylactically and palliative radiotherapy for pain relief and disruption of the mechanisms of tumor, reducing recurrence risk, was done.
Adenocarcinoma is the most common primary lung cancer in nonsmokers' women. 2 It's a silent killer; symptoms appear in advanced stages compromising prognosis and treatment. 1 Clinical stage is crucial to guide treatment. Multidisciplinary treatment approach (surgery, radiotherapy, chemotherapy, targeted therapy) is needed to reduce morbimortality. 1
AUTHOR CONTRIBUTIONS
All authors contributed equally to the elaboration of the manuscript. FCC, AAL, and VQC involved in surgical and medical practices, and literature searching. AHB and MCMA involved in concept and design. AHB, MCMA, FC, AAL, and VQC involved in writing. All authors approved the final report.
CONFLICT OF INTEREST
There is no conflict of interest.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGMENT
None.
Cabrera‐Cardozo F, Martínez‐Ávila MC, Hernández‐Blanquisett A, Quintero‐Carreño V, Álvarez‐Londoño A. Painful shoulder and scapula as initial presentation of advanced lung adenocarcinoma. Clin Case Rep. 2022;10:e06415. doi: 10.1002/ccr3.6415
DATA AVAILABILITY STATEMENT
Data available on request from the authors.
REFERENCES
- 1. Ettinger DS, Wood DE, Aisner DL, et al. Non‐small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20(5):497‐530. doi: 10.6004/jnccn.2022.0025 [DOI] [PubMed] [Google Scholar]
- 2. Bade BC, Dela Cruz CS. Lung cancer 2020: epidemiology, etiology, and prevention. Clin Chest Med. 2020;41(1):1‐24. doi: 10.1016/j.ccm.2019.10.001 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data available on request from the authors.