

Abstract
Background
Certain telemedicine programmes for heart failure (HF) have been shown to reduce all-cause mortality and heart failure-related hospitalisations, but their cost-effectiveness remains controversial. The SCAD programme is a home-based interactive telemonitoring service for HF, which is one of the largest and longest-running telemonitoring programmes for HF in France. The objective of this cost-utility analysis was to evaluate the cost-effectiveness of the SCAD programme with respect to standard hospital-based care in patients with HF.
Methods
A Markov model simulating hospitalisations and mortality in patients with HF was constructed to estimate outcomes and costs. The model included six distinct health states (three ‘not hospitalised’ states, two ‘hospitalisation for heart failure’ states, both depending on the number of previous hospitalisations, and one death state). The model lifetime in the base case was 10 years. Model inputs were based on published literature. Outputs (costs and QALYs) were compared between SCAD participants and standard care. Deterministic and probabilistic sensitivity analyses were performed to assess uncertainty in the input parameters of the model.
Results
The number of quality-adjusted life years (QALYs) was 3.75 in the standard care setting and 4.41 in the SCAD setting. This corresponds to a gain in QALYs provided by the SCAD programme of 0.65 over the 10 years lifetime of the model. The estimated total cost was €30,932 in the standard care setting and €35,177 in the SCAD setting, with an incremental cost of €4245. The incremental cost-effectiveness ratio (ICER) for the SCAD programme over standard care was estimated at €4579/QALY. In the deterministic sensitivity analysis, the variables that had the most impact on the ICER were HF management costs. The likelihood of the SCAD programme being considered cost-effective was 90% at a willingness-to-pay threshold of €11,800.
Conclusions
Enrolment of patients into the SCAD programme is highly cost-effective. Extension of the programme to other hospitals and more patients would have a limited budget impact but provide important clinical benefits. This finding should also be taken into account in new public health policies aimed at encouraging a shift from inpatient to ambulatory care.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12872-022-02878-1.
Keywords: Telemonitoring, France, Heart failure, Cost-effectiveness
Background
The management of patients with chronic heart failure (HF) is challenging due to the unpredictable occurrence of acute episodes of rapid onset, which can be life-threatening. In addition, patients with HF tend to be elderly and may have reduced mobility due to their disease, which can compromise timely and effective follow-up. For these reasons, HF is a promising candidate for the implementation of telemedicine programmes that allow patients to be managed at home. Such programmes have now been implemented in many different countries for over 20 years. Even though the nature of these programmes varies considerably, recent systematic reviews have generally concluded that intense programmes, notably those with dedicated nurse follow-up, can reduce all-cause mortality and heart failure-related hospitalisations [1–5].
Although providing important clinical benefits, effective telemedicine programmes carry a cost, and it is thus important to evaluate whether they are cost-effective for the management of HF. A number of economic studies have evaluated clinical outcomes and costs of these programmes [6–17], and provided somewhat inconsistent results. A recent systematic review has nonetheless concluded that telemonitoring programmes in HF are cost-effective, with their greatest impact and cost savings through reduced rehospitalisations [5].
Currently, health authorities in many countries are considering implementing and reimbursing telemedicine programmes for different chronic diseases with the goal of reducing the demand on hospital services and generating cost savings. In addition, the recent COVID-19 pandemic has illustrated the attractiveness of telemedicine interventions for managing patients with chronic diseases in their homes [18]. To this end, it is important for health authorities to dispose of national economic evaluations for individual telemonitoring programmes in the disease area of interest. The French health authorities are currently assessing the value of introducing a fully reimbursed telemonitoring programme at the national level for routine management of patients with HF. One of the candidate programmes for extension nationwide is the SCAD (Suivi Clinique A Domicile) programme, a home-based interactive telemonitoring service for HF established in the French region of Normandy in 2007 [19]. The programme is offered to all patients hospitalised for an acute exacerbation of HF, who are entered into the programme prior to discharge. Between 2007 and 2016, around 1000 patients in Normandy have been enrolled in the programme. The benefits of the SCAD programme in terms of reduced hospitalisations and mortality have been demonstrated both in a randomised clinical trial [20] and in a naturalistic setting [19]. In an analysis of the French national health insurance database (Système national des données de santé; SNDS), the rate of unplanned hospitalisations for a cardiovascular diagnosis was halved in SCAD participants compared to non-participants, the rate of unplanned hospitalisations for HF divided by three, and mortality reduced by around twenty percent [19]. The objective of this cost-utility analysis was to evaluate the cost-effectiveness of the SCAD home telemonitoring programme with respect to standard hospital-based care in patients with HF in France.
Methods
Study design
This was a cost-effectiveness analysis comparing the use of the SCAD programme in patients with HF compared with standard care without telemonitoring in the French setting. The cost data from this study have been presented at the European Society for Cardiology Congress in August 2020 [21].
Outcomes and costs were generated in a Markov model simulating hospitalisations and mortality in patients with HF. The Markov model was developed in Microsoft Excel (release 2010, Microsoft Inc, USA). The analysis was performed from a collective perspective, taking into account direct medical and non-medical costs borne by the national health insurance (NHI), by complementary private health insurance and by the patient. The analysis complied with the recommendations of the French Health Authorities for economic evaluations of innovative health technologies [22]. A discount rate of 2.5% was applied, as recommended in these guidelines [22].
SCAD programme
The SCAD programme is open to patients recently hospitalised for an acute exacerbation of heart failure in one of the participating hospital centres. Patients are enrolled into the programme mainly at the time of discharge from the hospital and remain in the programme for a period of three months, which can be renewed for a further three months if the patient and cardiologist so desire. Each patient is provided with a dedicated programme installed on a tactile pad for entering data and an internet link to the coordinating centre at the hospital. Over 6 days a week (Sunday excluded), the patient enters information on their clinical state (weight, blood pressure, heart rate and occurrence of cardiac symptoms), lifestyle factors (diet and physical activity), their psychological state (evaluation of fatigue and morale on a 10-point visual analogue score) and treatment compliance (assessed with an open question). The healthcare team can access the data entered by the patient through a secure internet portal during office hours. Personalised feedback is provided by a dedicated trained HF nurse from the hospital cardiology department through a telephone call or a text message. The data entered by the patient are also analysed in real-time by a risk algorithm in order to identify any risk of acute decompensation, and automatically generate an alert, if necessary. This enables the HF nurse to contact the patient, the general practitioner, the cardiologist or the emergency services whenever necessary in order to organise a consultation or a visit to the hospital. The computer interface also provides access for the patient to information and advice on treatment and on leading a healthy lifestyle. In addition, a secure chat tool is available for the patient throughout the duration of the programme which provides them with a direct contact with the care team and access to an information bank about heart failure. A full description of the organisation of the SCAD programme has recently been published [19].
Description of the model
A Markov model was developed to simulate six distinct health states, classified as ‘not hospitalised’ (three possible states), ‘hospitalisation for heart failure’ (two possible states), both depending on the number of previous hospitalisations, and death (one state). The structure of the model is illustrated in Fig. 1. Patients entered the model in one of three ‘not hospitalised’ health states, depending on the number of previous hospitalisations for HF, namely no previous hospitalisation for HF in the previous year, a single previous hospitalisation for HF, or multiple previous hospitalisations. The distribution of patients across these three health states was determined from the number of hospitalisations documented in the SNDS with HF as a primary diagnosis (identifying the reason for hospitalisation) in a population of patients with chronic HF enrolled into the SCAD telemonitoring programme in France between 2009 and 2016 [19]. Hospitalisations for HF were identified using the diagnostic algorithm developed by Tuppin et al. [23]. The characteristics of the patients in this population, overall and by age, LVEF category and NYHA class, are presented in Additional file 1.
Fig. 1.

Structure of the Markov model
In the next cycle, patients can either remain in the same ‘not hospitalised’ health state, transit to a hospitalisation state or die. Two hospitalisation states were considered, either a first hospitalisation for HF, or rehospitalisation for HF. From a hospitalisation health state, patients could either revert to the corresponding ‘not hospitalised’ state or die. Patients could not remain in a hospitalisation health state for more than one cycle and were obliged to transit at the end of the cycle. Death was considered the end state for the model. The cycle length was one month. This was based on the anticipated average duration of hospitalisation for heart failure [24], as patients cannot stay hospitalised for more than one cycle. The time horizon of the analysis was ten years in order to capture the effects and direct costs of the telemonitoring programme. No intercurrent events, such as the occurrence of adverse events, were modelled, in the absence of information on how these might influence transition probabilities or outcomes.
Model population
The analysis population modelled corresponded to a hypothetical cohort population of 10,000 adult patients with heart failure. This population size was chosen to match the incidence of first hospitalisation for heart failure derived from the SNDS [19].
Transition probabilities
Transition probabilities between each health state were based on published literature. For the initial hospitalisation and mortality, these were estimated from data collected in the ODIN study [25]. This was a large, prospective, multicentre French cohort of 3237 patients recruited by 61 French centres between 2007 and 2010 and followed up until 2013 [25]. For rehospitalisation, the transition probabilities were based on a more recent analysis of data from the SNDS [26]. All-cause mortality rates for the French general population were obtained from the French national statistics office [27]. All transitions used in the model were stratified by age (< 70 years and ≥ 70 years) and by HF severity (New York Heart Association grade) and the transition probabilities in each stratum were adjusted by the relative risk of hospitalisation and death observed in the ODIN study. Patients remained in the same age and severity class throughout the lifetime of the model. All transition probabilities are listed in Table 1.
Table 1.
Model inputs
| N° | Variable | Category | Value | Source |
|---|---|---|---|---|
| Model population | ||||
| 1 | Age group | < 70 years | 56.0% | SCAD cohort [19] |
| ≥ 70 years | 44.0% | SCAD cohort [19] | ||
| 2 | Severity | NYHA I/II | 61.0%a | SCAD cohort [19] |
| NYHA III/IV | 39.0% | SCAD cohort [19] | ||
| 3 | Extent of use of programme | Intermediate | 50.4% | SCAD cohort [19] |
| High | 49.6% | SCAD cohort [19] | ||
| 4 | Number of hospitalisations for HF | 0 in previous 12 months | 52.1% | SCAD cohort [19] |
| 1 in previous 12 months | 36.0% | SCAD cohort [19] | ||
| ≥ 2 in previous 12 months | 11.9% | SCAD cohort [19] | ||
| Transition probabilities | ||||
| 5 | Not hospitalised with no previous hospitalisation for HF to first hospitalisation for HF | 0.006 | ODIN study [25] | |
| 6 | Not hospitalised with one previous hospitalisation for HF to rehospitalisation for HF | 0.017 | AMELI study [28] | |
| 7 | Not hospitalised with ≥ 2 previous hospitalisations for HF to rehospitalisation for HF | 0.017 | AMELI study [28] | |
| 8 | Not hospitalised with no previous hospitalisation for HF to death | 0.0066 | ODIN study [25] | |
| 9 | Not hospitalised with one previous hospitalisation for HF to death | 0.0085 | ODIN study [25] | |
| 10 | Not hospitalised with ≥ 2 previous hospitalisations for HF to death | 0.0181 | ODIN study [25] | |
| 11 | First hospitalisation for HF to death (assumption) | 0.0085 | Equivalent to n° 9 | |
| 12 | Rehospitalisation for HF to death (assumption) | 0.0181 | Equivalent to n° 10 | |
| Adjustment factors (relative risk) | ||||
| 13 | Age < 70 years and NYHA I/II: risk of hospitalisation for HF | 0.79 | ODIN study [25] | |
| Age < 70 years and NYHA III/IV: risk of hospitalisation for HF | 1.43 | ODIN study [25] | ||
| Age ≥ 70 years and NYHA I/II: risk of hospitalisation for HF | 0.74 | ODIN study [25] | ||
| Age ≥ 70 years and NYHA III/IV: risk of hospitalisation for HF | 1.32 | ODIN study [25] | ||
| 14 | Age < 70 years and NYHA I/II: risk of death | 0.76 | ODIN study [25] | |
| Age < 70 years and NYHA III/IV: risk of death | 1.48 | ODIN study [25] | ||
| Age ≥ 70 years and NYHA I/II: risk of death | 0.71 | ODIN study [25] | ||
| Age ≥ 70 years and NYHA III/IV: risk of death | 1.36 | ODIN study [25] | ||
| Efficacy of intervention (relative risk) | ||||
| 15 | Risk of hospitalisation for HF | 0.500 | SCAD cohort [19] | |
| Risk of death | 0.535 | SCAD cohort [19] | ||
HF heart failure; NYHA New York Heart Association class
aData on NYHA class were unavailable for 9.1% of patients in the study
Interventions compared
The Markov model compared costs and outcomes between patients participating in the SCAD programme and non-participants (standard care setting). The relative risk of events (hospitalisation or death) for participants compared to non-participants was applied to the transition probabilities in the model. Relative risks were estimated from outcomes reported in a recent study in which 659 SCAD participants were linked to the SNDS database [19] (Table 1). In this study, three groups of patients who differed according to the extent of use of the SCAD programme (low, intermediate and high users) were defined by tercile and outcomes in each group analysed over the follow-up period [19]. However, there was no control group of patients with HF not participating in the programme.
The effectiveness of the telemonitoring programme varies with the extent of use, being greatest in the high users. Since there was no control group of patients with HF not participating in the programme, low users (including no users) were considered to represent non-participants and attributed a relative risk of effectiveness of 1. The efficacy of the SCAD programme was expressed as the relative risk of HF-related hospitalisation or of death for intermediate/high users versus low users of SCAD. The relative risks were estimated from Kaplan–Meier analysis of event rates. The survival curves are provided in Additional file 2. It was assumed that effectiveness was constant for the first 60 months of the model, as shown from a proportional hazard analysis of the Kaplan–Meier curves [19]. Over the next five years the SCAD programme was considered to be no longer effective, since no data is available beyond 60 months. These relative risks were then applied to the transition probabilities to generate use-level specific probabilities for intermediate/high users.
Utilities
Utilities for the model were taken from a cost-utility analysis of data from the Systolic HF Treatment with the If Inhibitor Ivabradine Trial (SHIFT) [29, 30]. This analysis reported quality of life (QoL) data using the EuroQoL (EQ-5D) questionnaire, which was administered to 5313 patients. Using the data, a multilevel regression analysis was performed in order to estimate the variation in EQ-5D as a function of age, gender, NYHA class and hospitalisation status [31]. The regression coefficients were used to weight the baseline utility values of the four different patient subgroups (age < 70 years or ≥ 70 years, NYHA class I/II or III/IV) and to determine the disutility value for hospitalisation to be used in the Markov model. These derived utility values are presented in Table 2.
Table 2.
Utility data considered in the model
| Description | Baseline utility |
|---|---|
| < 70 years & NYHA I/II | 0.788 |
| < 70 years & NYHA III/IV | 0.669 |
| ≥ 70 years & NYHA I/II | 0.749 |
| ≥ 70 years & NYHA III/IV | 0.603 |
| Hospitalisation | − 0.212 |
NYHA New York Heart Association class
Costs
Cost inputs were derived from the SCAD cohort. Individual cost items were retrieved from the SNDS for the 528 patients included from 2010 onwards and who survived for at least twelve months [19] [21]. The reason for excluding patients enrolled prior to 2010 was to ensure collection of exhaustive data on healthcare resource utilisation, since complete information has only been available in the database since 2009. Patients with less than one year’s follow-up were excluded in order to enable annual costs to be determined accurately. The procedure for cost estimation complied with the guidelines of the French Health Authorities [22]. Hospitalisation costs were estimated using the National Reference System for Hospital Costs (2016 tariffs, applicable at the time the study was initiated), which provides consolidated unit costs for individual stays according to the reason for hospitalisation, defined by ICD-10 diagnostic groups. All costs were adjusted for inflation and are presented as 2021 Euros.
Unit costs for all healthcare resource expenditure items are provided in Additional file 3. Consolidated costs associated with all states in the Markov model are presented in Table 3. Management costs for the three ‘not hospitalised’ HF states (0, 1 or ≥ 2 previous hospitalisations) were estimated from the median community and outpatient costs accrued over the 12 months before enrolment into the SCAD programme for the patients in the ‘standard care’ setting and over the 12 months following enrolment for SCAD participants. Only those management costs that differed significantly between the two settings were integrated into the model. The cost of hospitalisation was determined individually according to the level of adherence to the SCAD programme (low, intermediate, high). The overall unit hospitalisation cost for patients in the SCAD setting was calculated from costs in the intermediate and high user groups, weighted by the distribution of patients across the two groups. Unit hospitalisation cost for patients in the standard care setting corresponded to that estimated for low users. The end-of-life cost was the cost of palliative care in the last three months before death. The cost of the SCAD programme was based on the tariffs billed by the hospital, which are specified by the national programme for the evaluation of telemedicine of the French Health Ministry (ETAPES programme). For HF, this corresponds to a 6 months renewable care package costed at €470 for 6 months. This tariff covers €300 for the supplier, €110 for the cardiologist and €60 for therapeutic education. In the model, a monthly cost of €78,33 was applied over a 6 months period.
Table 3.
Costs considered in the model
| Resource | Time period considered | Unit cost (€2021) |
|---|---|---|
| Cost of SCAD programme | Monthly for 6 months | €78.33 |
| Management cost for non-hospitalised patients: standard care | Monthly | €197.81 |
| Management cost for non-hospitalised patients: SCAD | Monthly | €268.52 |
| HF hospitalisation cost: standard care (low SCAD use) | Individual stay | €7138.29 |
| HF hospitalisation cost: SCAD users (weighted1) | Individual stay | €5742.21 |
| HF hospitalisation cost: intermediate SCAD user | Individual stay | €5877.70 |
| HF hospitalisation cost: high SCAD user | Individual stay | €5604.33 |
| Palliative care cost | Monthly for 3 months before death | €20,847.11 |
HF heart failure; SCAD Suivi Clinique A Domicile
1Weighted to take into account the patient mix between high and intermediate users
Model outputs
Outcomes were modelled as life-years (LYs), quality-associated life years (QALYs) and total cost for each management strategy (SCAD and standard care). Incremental differences in costs and QALYs between the SCAD programme and standard care were calculated and the incremental cost-effectiveness ratio (ICER) derived by dividing the incremental cost by the incremental effectiveness. ICERs were calculated for both QALYs and LYs.
Sensitivity analysis
Deterministic and probabilistic sensitivity analyses were performed to assess uncertainty in the input parameters of the model. In the deterministic sensitivity analysis (DSA), key model inputs were varied within their standard errors or 95% confidence intervals. If empirical data to inform these precision estimates were unavailable, an arbitrary range of ± 20% was applied. The variables used in the deterministic sensitivity analysis (DSA) and the range of values applied are listed in Table 4.
Table 4.
Deterministic sensitivity analysis: range of values tested
| Parameter | Base case | Lower bound | Upper bound |
|---|---|---|---|
| Duration of participation in the SCAD programme (months) | 6 | − 20% | + 20% |
| TP No previous hospitalisation for HF to death | 0.006 | − 20% | + 20% |
| TP One previous hospitalisation for HF to death | 0.008 | − 20% | + 20% |
| TP Two previous hospitalisations for HF to death | 0.018 | − 20% | + 20% |
| TP First hospitalisation for HF to death | 0.008 | − 20% | + 20% |
| TP Rehospitalisation for HF to death | 0.018 | − 20% | + 20% |
| TP No previous hospitalisation for HF to first hospitalisation for HF | 0.006 | − 20% | + 20% |
| TP One previous hospitalisation for HF to rehospitalisation for HF | 0.017 | − 20% | + 20% |
| TP Two previous hospitalisations for HF to rehospitalisation for HF | 0.017 | − 20% | + 20% |
| TP risk adjustment HF hospitalisation < 70 years NYHA I/II | 0.794 | − 20% | + 20% |
| TP risk adjustment HF hospitalisation < 70 years NYHA III/IV | 1.428 | − 20% | + 20% |
| TP risk adjustment HF hospitalisation ≥ 70 years NYHA I/II | 0.745 | − 20% | + 20% |
| TP risk adjustment HF hospitalisation ≥ 70 years NYHA III/IV | 1.324 | − 20% | + 20% |
| TP risk adjustment death < 70 years NYHA I/II | 0.756 | − 20% | + 20% |
| TP risk adjustment death < 70 years NYHA III/IV | 1.482 | − 20% | + 20% |
| TP risk adjustment death ≥ 70 years NYHA I/II | 0.706 | − 20% | + 20% |
| TP risk adjustment death ≥ 70 years NYHA III/IV | 1.360 | − 20% | + 20% |
| Relative risk of hospitalisation for HF due to SCAD | 0.5 | − 20% | + 20% |
| Persistence of effectiveness of SCAD programme (months) | 60 | 90 | 120 |
| Relative risk of death due to SCAD | 0.535 | − 20% | + 20% |
| Utility ≥ 70 years NYHA I/II | 0.749 | − 20% | + 20% |
| Utility under70 NYHA III/IV | 0.669 | − 20% | + 20% |
| Utility under70 NYHA I/II | 0.788 | − 20% | + 20% |
| Utility ≥ 70 years NYHA III/IV | 0.603 | − 20% | + 20% |
| HF hospitalisation cost with SCAD | 5742 | − 20% | + 20% |
| HH hospitalisation cost without SCAD | 7138 | − 20% | + 20% |
| Management cost without SCAD (monthly) | 197.8 | − 20% | + 20% |
| Management cost with SCAD (monthly) | 268.5 | − 20% | + 20% |
| Palliative care cost | 20,847 | − 20% | + 20% |
| Discount rate | 2.5% | 1.5% | 4% |
NYHA New York Heart Association class; SCAD Suivi Clinique A Domicile; TP transition probability
In the probabilistic sensitivity analysis (PSA), Monte Carlo simulations were performed allowing the values for the model inputs to vary according to their sampling distributions (5000 iterations). A log-normal distribution was applied for clinical data, a beta distribution for utilities and a gamma distribution for costs. The results of the analysis are expressed as the cost-effectiveness acceptability curve for the net benefit.
Scenario analysis
Five scenario analyses were also performed. The first two evaluated cost-effectiveness in different patient subgroups and the remaining analyses evaluated changes in the parameters defining the structure of the model. In the first analysis, the model was reiterated in three subgroups of patients categorised by their left ventricular ejection fraction (LVEF). These were preserved ejection fraction (pEF: > 50%), mid-range ejection fraction (mrEF: 40–49%) and reduced ejection fraction (rEF: < 40%). Transition probabilities for initial hospitalisation and mortality according to LVEF class were based on data from the ODIN cohort [25]. Since rehospitalisation rates according to the type of ejection fraction are not available in the study of the SNDS [26], the same transition probabilities were used for all three LVEF categories as in the base-case analysis. Transition probabilities and relative risks of clinical outcomes used in this scenario analysis are provided in Additional file 4 and Additional file 5.
The second scenario analysis focused on subgroups of patients with mild-to-moderate (NYHA class I or II) and severe (NYHA class III or IV) heart failure. Transition probabilities and relative risks of clinical outcomes used in this scenario analysis are provided in Table 1.
In the third scenario analysis, the time horizon of the model was set at either five years or for the lifetime of the patient (compared to ten years in the base-case analysis). The five-year horizon was chosen as this is the length of time for which the SCAD programme has been shown to be effective at reducing hospitalisation and mortality [19]. ‘Lifetime’ was considered to be the time period between entry into the model and transition to the death state for each patient.
In the fourth scenario analysis, all patients entered the model in the ‘not hospitalised after one previous hospitalisation’ state. The justification for this is that the SCAD programme is only proposed to patients at the time of hospital discharge. In the base case, patients who enter the model in the ‘not hospitalised with no previous hospitalisation’ state and who are not hospitalised during the lifetime of the model will never be proposed the SCAD programme. The scenario analysis evaluates a scenario in which all patients are proposed the programme.
The final scenario analysis evaluated the situation in which participation in the SCAD programme was continued over the entire 10 years period over which costs and utilities were determined.
Results
Utility outcomes
Over the course of the model, the total number of hospitalisations was 0.749 in the standard care setting and 0.612 in the SCAD setting (Table 5). The number of life years was 5.11 and 6.03 respectively. The number of quality-adjusted life years (QALYs) was 3.75 in the standard care setting and 4.41 in the SCAD setting. This corresponds to a gain in QALYs provided by the SCAD programme of 0.65 over the 10 years lifetime of the model (Table 5).
Table 5.
Utility and cost outcomes
| SCAD | Standard care | Incremental | |
|---|---|---|---|
| Total number of hospitalisations for HF per patient | 0.612 | 0.749 | − 0.137 |
| First hospitalisations for HF | 0.156 | 0.186 | − 0.030 |
| Rehospitalisations for HF | 0.456 | 0.563 | − 0.108 |
| Life years | 6.03 | 5.11 | 0.93 |
| QALYs | 4.41 | 3.75 | 0.65 |
| Total Costs | €35,177 | €30,932 | €4,245 |
| SCAD costs | €461 | – | €461 |
| HF-specific management costs | €19,251 | €11,954 | €7297 |
| HF hospitalisation costs | €3120 | €4875 | €1755 |
| Palliative care costs | €12,345 | €14,103 | €1758 |
| ICER (€/LY) | €4579 | ||
| ICER (€/QALY) | €6491 |
HF heart failure; ICER incremental cost-effectiveness ratio; LY life year; QALY quality-adjusted life year; SCAD Suivi Clinique A Domicile
Cost outcomes
The estimated total cost was €30,932 in the standard care setting and €35,177 in the SCAD setting, with an incremental cost of €4245 (Table 5). The largest component of costs were the HF-specific management costs. The higher incremental cost in the SCAD setting was principally due to higher total management costs as the patients survived longer in this setting. The cost of the SCAD programme itself contributed < 2% of the total cost and around 10% of the incremental cost (Table 5).
Cost-utility
The ICER was €4579 in terms of incremental cost per life year gained and €6491 in terms of incremental cost per quality-adjusted life year gained (Table 5).
Sensitivity analysis
A deterministic sensitivity analysis was performed to identify variables that influenced the ICER of the SCAD programme compared to standard care. The results are presented in the form of a tornado plot in Fig. 2. The variables that had the most impact on the ICER were HF management costs, both in the standard care setting and the SCAD setting. Other variables whose precision influenced the ICER were hospitalisation costs, the utility value for patients aged ≥ 70 years in NYHA class III/IV and the persistence of the effectiveness of the SCAD programme. Varying the values of the other variables in either direction did not change the estimated ICER by more than €500/QALY.
Fig. 2.

Deterministic sensitivity analysis. Blue: lower limit of uncertainty; red: upper limit of uncertainty. All hospitalisation items in this analysis are restricted to hospitalisations for heart failure, as specified in Table 4
The effect of increasing the cost of the SCAD programme on the estimated ICER is illustrated in Fig. 3. A one-100-fold increase in cost would lead to an increase in the ICER to €76,280.
Fig. 3.
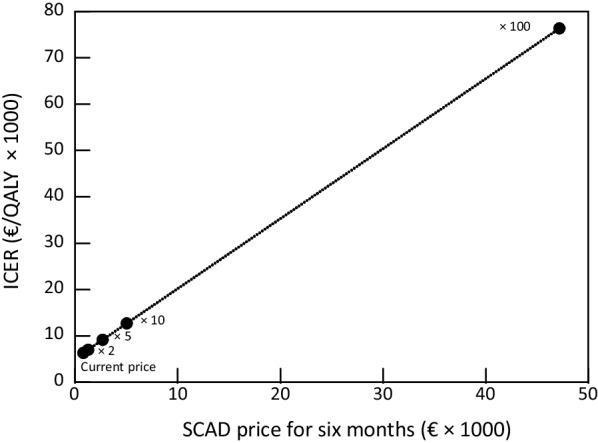
Effect on the ICER of varying SCAD cost
In the probabilistic sensitivity analysis, the mean incremental cost of the SCAD programme generated from the Monte Carlo simulations was €4314 and the mean incremental utility gained was 0.64 QALYs, corresponding to an ICER for the SCAD programme of €6689 €/QALY with a standard deviation of €3883. These values are very close to those observed in the base-case analysis. A scatter diagram of the outputs from the individual Monte Carlo simulations is presented in Fig. 4. The distribution of the outputs was symmetrical and centred on the mean values. It should be noted that in 3% of simulations, the SCAD strategy was dominant (less expensive and more effective than standard of care). A cost-effectiveness acceptability curve was plotted based on the PSA, which showed that the likelihood of the SCAD programme being considered cost-effective was 90% at a willingness-to-pay threshold of €11,800 (Fig. 5).
Fig. 4.

Probabilistic sensitivity analysis. Each blue point represents the incremental cost (€) and utility (QALY) of the SCAD programme from an individual Monte Carlo simulation. The grey point represents the mean incremental cost and utility derived from all Monte Carlo simulations and the orange point the incremental cost and utility derived from the deterministic base case analysis.
Fig. 5.

Willingness to pay thresholds. Blue curve: SCAD programme; orange curve: standard care.
Scenario analyses
The outcomes of the scenario analyses based on patient subgroups are presented in Table 6. In the analysis of patients with different LVEF, the ICERs in the three scenario analyses ranged from €5843/QALY in patients with preserved ejection fraction to €6625/QALY in those with mid-range ejection fraction. Variation in both cost and utility outcome contributed to this difference.
Table 6.
Scenario analyses in patient subgroups
| Life years | QALYs | Total costs (€) | ICER (€/LY) |
ICER (€/QALY) | |
|---|---|---|---|---|---|
| Base case | |||||
| SCAD | 6.03 | 4.41 | 35,177 | ||
| SC | 5.11 | 3.75 | 30,932 | 4579 | 6491 |
| Difference | 0.93 | 0.65 | 4245 | ||
| Preserved ejection fraction | |||||
| SCAD | 5.88 | 4.24 | 34,707 | ||
| SC | 4.87 | 3.54 | 30,628 | 4045 | 5843 |
| Difference | 1.01 | 0.70 | 4079 | ||
| Mid-range ejection fraction | |||||
| SCAD | 6.19 | 4.54 | 34,107 | ||
| SC | 5.29 | 3.90 | 29,821 | 4741 | 6625 |
| Difference | 0.90 | 0.65 | 4287 | ||
| Reduced ejection fraction | |||||
| SCAD | 6.00 | 4.32 | 35,781 | ||
| SC | 5.03 | 3.65 | 31,448 | 4474 | 6431 |
| Difference | 0.97 | 0.67 | 4332 | ||
| NYHA Class I/II | |||||
| SCAD | 6.66 | 5.16 | 34,694 | ||
| SC | 5.87 | 4.55 | 30,144 | 5779 | 7500 |
| Difference | 0.79 | 0.61 | 4550 | ||
| NYHA Class III/IV | |||||
| SCAD | 5.06 | 3.23 | 35,933 | 3289 | 5176 |
| SC | 3.91 | 2.51 | 32,164 | ||
| Difference | 1.15 | 0.73 | 3769 | ||
ICER incremental cost-effectiveness ratio; LY life-years; NYHA New York Hospital Association; QALY quality-adjusted life year; SC standard care; SCAD Suivi Clinique A Domicile
In the scenario analysis evaluating different severity groups (Table 6), the QALYs gained were higher in the NYHA I/II subgroup than in the NYHA III/IV subgroup, although the incremental gain in QALYs in the SCAD group compared to the standard care group was greater in the NYHA III/IV group. Costs were somewhat higher in the NYHA III/IV group and the cost savings in the SCAD group compared to the standard care group lower in this group. The ICER was higher in the NYHA I/II group (€7500) than in the NYHA III/IV group (€5176).
The outputs of the scenario analyses in which the parameters defining the structure of the model were varied are presented in Table 7. When a 5 years time horizon was used, the SCAD setting was dominant over standard care, being both less expensive and more effective. When the horizon was extended over the entire patient’s lifetime, both costs and utilities were higher than in the base case analysis, and the ICER increased by around 20% from €6491/QALY to €8151/QALY.
Table 7.
Scenario analyses varying the model parameters
| Life years | QALYs | Total costs (€) | ICER (€/LY) | ICER (€/QALY) | |
|---|---|---|---|---|---|
| Base case | |||||
| SCAD | 6.03 | 4.41 | 35,177 | ||
| SC | 5.11 | 3.75 | 30,932 | 4579 | 6491 |
| Difference | 0.93 | 0.65 | 4245 | ||
| Five-year time-horizon | |||||
| SCAD | 4.03 | 2.92 | 21,290 | ||
| SC | 3.58 | 2.61 | 21,372 | SCAD | Dominant |
| Difference | 0.45 | 0.31 | -82 | ||
| Lifetime time-horizon | |||||
| SCAD | 7.49 | 5.51 | 45,451 | ||
| SC | 6.22 | 4.60 | 38,055 | 5841 | 8151 |
| Difference | 1.27 | 0.91 | 7396 | ||
| All patients previously hospitalised at model entry | |||||
| SCAD | 5.79 | 4.23 | 36,527 | ||
| SC | 4.73 | 3.47 | 32,679 | 3609 | 5082 |
| Difference | 1.07 | 0.76 | 3848 | ||
| SCAD participation for 10 years | |||||
| SCAD | 6.29 | 4.59 | 39,023 | ||
| SC | 5.11 | 3.75 | 30,932 | 6829 | 9680 |
| Difference | 1.18 | 0.84 | 8095 | ||
ICER incremental cost-effectiveness ratio; LY life-years; QALY quality-adjusted life year; SC standard care; SCAD Suivi Clinique A Domicile
In the analysis in which all patients entered the model in the ‘not hospitalised after one previous hospitalisation’ state (Table 7), the ICER was around 20% lower than for the base case (€5082/QALY). This difference was due both to a reduction in cost and to an increase in life-years gained. This scenario analysis is expected to reflect real-life practice more accurately than the base case analysis.
In the analysis in which patients participated in SCAD for the entire 10 years lifetime of the model (Table 7), the additional cost of the SCAD setting over standard care was twice as high as in the base case, but the number of QALYs gained was also somewhat higher. In consequence, the ICER in this scenario analysis was also higher than in the base case (€9680/QALY).
Discussion
In this cost-effectiveness evaluation of SCAD, a home-based interactive telemonitoring service for HF in France, we identified significant clinical benefits (one life-year gained in the ten years following initiation of the programme in the base case of the model) for a relatively modest cost (€4245 over the lifetime of the model). The estimated ICER was €6491/QALY. An intervention is considered to be cost-effective when the estimated ICER is below the willingness-to-pay threshold in the given country. While there is no formal willingness-to-pay threshold in France, a threshold of €150,000/QALY has been proposed [32]. The ICER for the SCAD programme is well below this threshold and, in the probabilistic sensitivity analysis, would be below a willingness-to-pay threshold of €11,800 in 90% of simulations.
In order to identify in which type of patient monitoring in the SCAD programme might be more effective, we performed two scenario analyses in different subgroups of patients. We observed modest differences in the estimated ICER of < 15% between the three LVEF subgroups. These differences can be explained by the fact that, in our cohort, these subgroups present different risk profiles. The mrEF group, which has the highest ICER, has the most favourable risk profile, being younger, more frequently less severe (NYHA class I/II), and less frequently previously hospitalised for HF, compared to the other two groups (see Additional file 1). For this reason, these patients are less likely to be hospitalised or die, and the absolute incremental benefit of SCAD participation compared to standard care will be numerically lower. This translates into a higher ICER in this group. In contrast, patients with preserved ejection fraction are on average older and have had more previous hospitalizations compared to patients with reduced ejection fraction. The ICER is correspondingly lower in this subgroup. Nonetheless, the observed differences in ICER between the three LVEF groups are small compared to the standard deviation of the ICER for the base case determined in the probabilistic sensitivity analysis (€3883). However, it should be noted that, in the absence of data on ejection fraction in the SNDS, from which transition probabilities were derived, the same transition probabilities were applied for all three ejection groups. If these probabilities in fact differ between groups, then this would have an impact on the estimated ICERs in these patient subgroups.
Differences in the cost-effectiveness of the SCAD programme between subgroups of different severity were more substantial, €7500 in patients with NYHA class I/II and €5176 in those with NYHA class III/IV HF. Again, this difference is principally driven by the risk of hospitalisation and death, and suggests that the SCAD programme is most cost-effective in patients with more severe heart disease. This is consistent with findings from the OSICAT study, a randomised clinical trial in France comparing telemonitoring with the Chronic Care Connect programme [33], which also reported that the largest clinical benefits of telemonitoring are observed in patients with more severe HF.
The ICER for the SCAD programme increases as the lifetime of the model is extended. This relationship can probably be explained by longer survival of patients included in the programme. These survivors continue to consume healthcare resources for longer, increasing total cost, whereas in standard care, more rapid attrition limits the cost of healthcare over the long term. However, even if the time horizon of the model is extended to the patient’s entire life expectancy, the ICER remains well below €10,000/QALY. When the time-horizon of the model was limited to five years, which is the longest period for which actual data on the impact of the SCAD programme on benefits and costs are available [19], the SCAD strategy is actually dominant over the standard care strategy, being both more effective in terms of QALYs gained and cost-saving. It is difficult to estimate accurately the long-term cost-effectiveness of the SCAD programme due to uncertainty over how long the clinical benefits in terms of reduced hospitalisation and mortality may be expected to last. In the model, a conservative approach was taken in which the benefits of the SCAD programme were limited to the five-year period for which data were available. It is possible that as more long-term data becomes available, estimations of the ICER for time horizons beyond five years may change.
The fourth scenario analysis in which all patients entered the model in the ‘not hospitalised after one previous hospitalisation’ state corresponds to how the SCAD programme currently operates, where only patients who are hospitalised are offered participation in the programme. The base case represented a conservative hypothesis, where certain patients are never hospitalised are also included in the model, and who will contribute equally to both the standard care and the SCAD strategy. In the base case, this will have the effect of diluting incremental utility and cost differences between the two strategies. The lower ICER determined in the fourth scenario analysis may for this reason reflect more accurately the cost-effectiveness of the SCAD programme as it is operated today.
Although telemonitoring programmes such as SCAD bear a cost, which is attributable both to the cost of the programme itself and to higher management costs related to higher outpatient costs and longer survival of the patients, this cost is relatively small compared to the total cost of management of HF. In France, there are around 540,000 patients managed for chronic HF, who generated a total cost to national health insurance in 2013 of €1186 million [34]. Since the SCAD programme is dominant in the short term (between 1 and 5 years), making it available to all patients in France at the current cost (€470 for 6 months) would generate short-term savings from the reduction in hospitalizations. It should however be noted that implementation of the SCAD programme bears a specific cost relating to funding for the full-time involvement of a trained nurse dedicated to patient monitoring, patient coaching and alert management.
Comparison of the present findings with those of cost-effectiveness analyses performed in other countries is not straightforward, due to differences in the nature of the telemonitoring programme considered, and in how they are financed. Nonetheless, recent studies of intense telemonitoring programmes for HF have consistently shown them to be cost-effective. For example, a Markov model similar to the present one has been used to evaluate cost-effectiveness of telehealth programs for congestive heart failure in the context of the United States health system [14]. Inputs were derived from a meta-analysis of multiple home telemonitoring programmes [35]. At the five-year time horizon, the authors found that enrolment in such a programme would result in cost savings of $4456 with a gain of 0.50 life years. A later analysis in the US health system reported found that telemonitoring was most cost-effective in patients with severe HF (NYHA class III/IV) [36]. In the European context, data from the Trans-European Network–Home-Care Management System (TEN–HMS) study [37] were used in a Markov model involving transitions between different NYHA severity classes [11]. At the twenty-year time horizon, the ICER was estimated to be €12,479/QALY. Most recently, Vesterggard et al. have reported on the TeleCare North HF study in Denmark [16]. This is a telemedicine programme implemented by nurses with a therapeutic education component and remote monitoring of clinical data provided by the patient. This cost-effectiveness analysis was not a modelling study but used real data on utilities and costs collected from patients participating in the programme. This analysis found the telemonitoring strategy to be dominant over standard care, with a net monetary benefit of £5164 (approximately €6100) at a time-horizon of one year. Taken together, the findings of these different studies provide a strong argument that intensive telemedicine programmes are a cost-effective way to manage patients with HF in different healthcare systems, consistent with the findings of the present study. Remote monitoring of patients with HF can thus make a beneficial contribution to a value-based approach to funding health services [38].
The study presents certain limitations. The model inputs come from multiple published sources, principally the ODIN study [25] and the SCAD-SNDS cohort [19], and the different source populations may not be fully comparable. In addition, in the SCAD-SNDS cohort, which was used as the source of the relative risks of hospitalisation and mortality, there was no control group without home telemonitoring, and the event rates in the low adherence group were used to represent standard care. However, in the SCAD study, even low-level users had lower rehospitalisation rates compared to the period before joining the SCAD programme, suggesting that the low adherence group may gain some benefit from the programme compared to non-participants. For this reason, the incremental gain in QALYs compared to standard care may have been underestimated.
Conclusions
Enrolment of patients into the SCAD programme is highly cost-effective. Extension of the programme to other hospitals and more patients would have a limited budget impact but provide important clinical benefits. This finding should also be taken into account in new public health policies aimed at encouraging a shift from inpatient to ambulatory care.
Supplementary Information
Additional file1. Description of patients from the SCAD cohort
Additional file2. Kaplan–Meier survival curves stratified by level of SCAD use
Additional file3. Costs for healthcare resource consumption determined in the SCAD–SNDS linkage study.
Additional file4. Input data for the scenario analyses: clinical events
Acknowledgements
Medical writing assistance was provided by Adam Doble (Foxymed, Paris, France).
Abbreviations
- CI
Confidence interval
- DSA
Deterministic sensitivity analysis
- EF
Ejection fraction
- HF
Heart failure
- HF-mrEF
Heart failure with mid-range ejection fraction
- HF-pEF
Heart failure with preserved ejection fraction
- HF-rEF
Heart failure with reduced ejection fraction
- HR
Hazard ratio
- ICER
Incremental cost-effectiveness ratio
- LL
Lower limit
- LVEF
Left ventricular ejection fraction
- LY
Life year
- mrEF
Mid range ejection fraction
- NHI
National Health Insurance
- NYHA
New York Heart Association class
- PSA
Probabilistic sensitivity analysis
- pEF
Preserved ejection fraction
- QALYs
Quality-adjusted life years
- QoL
Quality of life
- rEF
Reduced ejection fraction
- SC
Standard care
- SCAD
Suivi Clinique A Domicile
- SHIFT
Systolic HF treatment with the if inhibitor ivabradine trial
- TEN–HMS
Trans-European Network–Home-Care Management System
- TP
Transition probability
- UL
Upper limit
Author contributions
VD and LC were responsible of collecting source data. MC performed the modelling analysis. MC, RS, DL, LC, VD, FB, TdC, KH, AB and PM participated in the design or implementation of the study. MC, RS, DL, LC, VD, FB, TdC, KH, AB and PM were involved in the analysis and interpretation of the results and the development of this manuscript. MC, RS, DL, LC, VD, FB, TdC, KH, AB and PM had full access to the data and gave final approval before submission. All authors read and approved the final manuscript.
Funding
This work was funded by Amgen SAS, Boulogne-Billancourt, France, who were involved in planning, conducting, analysing and interpreting the study. Amgen SAS financed the costs associated with the development and publishing of the present manuscript.
Availability of data and materials
All data and software used to construct this model are identified either in the manuscript or in cited source references.
Declarations
Ethics approval and consent to participate
The study was a modelling study using previously published data and involved no interactions (interventions or data collection) with actual patients.
Consent for publication
Not applicable.
Competing interests
FB, MC and TdC are employees of Amgen SAS. VD and LC are employees of Cemka. RS, DL, KH, AB and PM have no conflict of interest to declare.
Footnotes
An abstract and poster relating to this work were presented at the European Society of Cardiology Congress 2020—The Digital Experience (August 2020) [21].
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Mégane Caillon and Remi Sabatier Contributed equally to this work as co-first authors
References
- 1.Inglis SC, Clark RA, Dierckx R, Prieto-Merino D, Cleland JG. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst Rev. 2015 doi: 10.1002/14651858.CD007228.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yun JE, Park JE, Park HY, Lee HY, Park DA. Comparative effectiveness of telemonitoring versus usual care for heart failure: a systematic review and meta-analysis. J Card Fail. 2018;24(1):19–28. doi: 10.1016/j.cardfail.2017.09.006. [DOI] [PubMed] [Google Scholar]
- 3.Clark RA. Telehealth in the elderly with chronic heart failure: What is the evidence? Stud Health Technol Inform. 2018;246:18–23. [PubMed] [Google Scholar]
- 4.Pandor A, Gomersall T, Stevens JW, Wang J, Al-Mohammad A, Bakhai A, et al. Remote monitoring after recent hospital discharge in patients with heart failure: a systematic review and network meta-analysis. Heart. 2013;99(23):1717–1726. doi: 10.1136/heartjnl-2013-303811. [DOI] [PubMed] [Google Scholar]
- 5.Driscoll A, Gao L, Watts JJ. Clinical effectiveness and cost-effectiveness of ambulatory heart failure nurse-led services: an integrated review. BMC Cardiovasc Disord. 2022;22(1):64. doi: 10.1186/s12872-022-02509-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Boyne JJ, Van Asselt AD, Gorgels AP, Steuten LM, De Weerd G, Kragten J, et al. Cost–effectiveness analysis of telemonitoring versus usual care in patients with heart failure: the TEHAF–study. J Telemed Telecare. 2013;19(5):242–248. doi: 10.1177/1357633X13495478. [DOI] [PubMed] [Google Scholar]
- 7.Chen YH, Ho YL, Huang HC, Wu HW, Lee CY, Hsu TP, et al. Assessment of the clinical outcomes and cost-effectiveness of the management of systolic heart failure in Chinese patients using a home-based intervention. J Int Med Res. 2010;38(1):242–252. doi: 10.1177/147323001003800129. [DOI] [PubMed] [Google Scholar]
- 8.Chen YH, Lin YH, Hung CS, Huang CC, Yeih DF, Chuang PY, et al. Clinical outcome and cost-effectiveness of a synchronous telehealth service for seniors and nonseniors with cardiovascular diseases: quasi-experimental study. J Med Internet Res. 2013;15(4):e87. doi: 10.2196/jmir.2091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.de Lusignan S, Wells S, Johnson P, Meredith K, Leatham E. Compliance and effectiveness of 1 year’s home telemonitoring. The report of a pilot study of patients with chronic heart failure. Eur J Heart Fail. 2001;3(6):723–730. doi: 10.1016/S1388-9842(01)00190-8. [DOI] [PubMed] [Google Scholar]
- 10.Frederix I, Vanderlinden L, Verboven AS, Welten M, Wouters D, De Keulenaer G, et al. Long-term impact of a six-month telemedical care programme on mortality, heart failure readmissions and healthcare costs in patients with chronic heart failure. J Telemed Telecare. 2019;25(5):286–293. doi: 10.1177/1357633X18774632. [DOI] [PubMed] [Google Scholar]
- 11.Grustam AS, Severens JL, De Massari D, Buyukkaramikli N, Koymans R, Vrijhoef HJM. Cost-effectiveness analysis in telehealth: a comparison between home telemonitoring, nurse telephone support, and usual care in chronic heart failure management. Value Health. 2018;21(7):772–782. doi: 10.1016/j.jval.2017.11.011. [DOI] [PubMed] [Google Scholar]
- 12.Henderson C, Knapp M, Fernández JL, Beecham J, Hirani SP, Cartwright M, et al. Cost effectiveness of telehealth for patients with long term conditions (Whole Systems Demonstrator telehealth questionnaire study): nested economic evaluation in a pragmatic, cluster randomised controlled trial. BMJ. 2013;346:f1035. doi: 10.1136/bmj.f1035. [DOI] [PubMed] [Google Scholar]
- 13.Jiménez-Marrero S, Yun S, Cainzos-Achirica M, Enjuanes C, Garay A, Farre N, et al. Impact of telemedicine on the clinical outcomes and healthcare costs of patients with chronic heart failure and mid-range or preserved ejection fraction managed in a multidisciplinary chronic heart failure programme: a sub-analysis of the iCOR randomized trial. J Telemed Telecare. 2020;26(1–2):64–72. doi: 10.1177/1357633X18796439. [DOI] [PubMed] [Google Scholar]
- 14.Liu SX, Xiang R, Lagor C, Liu N, Sullivan K. Economic modeling of heart failure telehealth programs: When do they become cost saving? Int J Telemed Appl. 2016;2016:3289628. doi: 10.1155/2016/3289628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Smith B, Hughes-Cromwick PF, Forkner E, Galbreath AD. Cost-effectiveness of telephonic disease management in heart failure. Am J Manag Care. 2008;14(2):106–115. [PubMed] [Google Scholar]
- 16.Vestergaard AS, Hansen L, Sørensen SS, Jensen MB, Ehlers LH. Is telehealthcare for heart failure patients cost-effective? An economic evaluation alongside the Danish TeleCare North heart failure trial. BMJ Open. 2020;10(1):e031670. doi: 10.1136/bmjopen-2019-031670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pandor A, Thokala P, Gomersall T, Baalbaki H, Stevens JW, Wang J, et al. Home telemonitoring or structured telephone support programmes after recent discharge in patients with heart failure: systematic review and economic evaluation. Health Technol Assess. 2013;17(32):1–207. doi: 10.3310/hta17320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cleland JGF, Clark RA, Pellicori P, Inglis SC. Caring for people with heart failure and many other medical problems through and beyond the COVID-19 pandemic: the advantages of universal access to home telemonitoring. Eur J Heart Fail. 2020;22(6):995–998. doi: 10.1002/ejhf.1864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sabatier R, Legallois D, Jodar M, Courouve L, Donio V, Boudevin F, et al. Impact of patient engagement in a French telemonitoring programme for heart failure on hospitalization and mortality. ESC Heart Fail. 2022 doi: 10.1002/ehf2.13978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sabatier R, Coutance G, Belin A, Biannic C, Loiselet P, Pradere G, et al. P666—Three months educational remote telemonitoring in elderly patients with heart failure reduces hospitalizations for acute heart failure at one year: a randomized trial. Eur J Heart Fail. 2013;12(S1):S313. [Google Scholar]
- 21.Sabatier R, Legallois D, Jodar M, Donio V, Courouve L, Hauchard K, et al. Cost-effectiveness analysis of a telemonitoring program on patients with heart failure in Normandy: an 8-year retrospective analysis (2009–2017) Eur Heart J. 2020;41(Supplement 2):ehaa946.3468. doi: 10.1093/ehjci/ehaa946.3468. [DOI] [Google Scholar]
- 22.Haute Autorité de Santé. Choix méthodologiques pour l'évaluation économique à la HAS. 2020.
- 23.Tuppin P, Cuerq A, de Peretti C, Fagot-Campagna A, Danchin N, Juilliere Y, et al. Two-year outcome of patients after a first hospitalization for heart failure: a national observational study. Arch Cardiovasc Dis. 2014;107(3):158–168. doi: 10.1016/j.acvd.2014.01.012. [DOI] [PubMed] [Google Scholar]
- 24.McMurray JJ, Andersson FL, Stewart S, Svensson K, Solal AC, Dietz R, et al. Resource utilization and costs in the Candesartan in heart failure: assessment of reduction in mortality and morbidity (CHARM) programme. Eur Heart J. 2006;27(12):1447–1458. doi: 10.1093/eurheartj/ehl016. [DOI] [PubMed] [Google Scholar]
- 25.Juilliere Y, Jourdain P, Suty-Selton C, Beard T, Berder V, Maitre B, et al. Therapeutic patient education and all-cause mortality in patients with chronic heart failure: a propensity analysis. Int J Cardiol. 2013;168(1):388–395. doi: 10.1016/j.ijcard.2012.09.030. [DOI] [PubMed] [Google Scholar]
- 26.Feldman SF, Lesuffleur T, Olie V, Gastaldi-Menager C, Juilliere Y, Tuppin P. French annual national observational study of 2015 outpatient and inpatient healthcare utilization by approximately half a million patients with previous heart failure diagnosis. Arch Cardiovasc Dis. 2021;114(1):17–32. doi: 10.1016/j.acvd.2020.05.009. [DOI] [PubMed] [Google Scholar]
- 27.Institut National d'Etudes Demographiques. Mortality rates by sex and age in 2018 2020. Available from: https://www.ined.fr/en/everything_about_population/data/france/deaths-causes-mortality/mortality-rates-sex-age/.
- 28.Tuppin P, Cuerq A, de Peretti C, Fagot-Campagna A, Danchin N, Juilliere Y, et al. First hospitalization for heart failure in France in 2009: patient characteristics and 30-day follow-up. Arch Cardiovasc Dis. 2013;106(11):570–585. doi: 10.1016/j.acvd.2013.08.002. [DOI] [PubMed] [Google Scholar]
- 29.Swedberg K, Komajda M, Bohm M, Borer J, Robertson M, Tavazzi L, et al. Effects on outcomes of heart rate reduction by ivabradine in patients with congestive heart failure: is there an influence of beta-blocker dose?: findings from the SHIFT (Systolic Heart failure treatment with the I(f) inhibitor ivabradine Trial) study. J Am Coll Cardiol. 2012;59(22):1938–1945. doi: 10.1016/j.jacc.2012.01.020. [DOI] [PubMed] [Google Scholar]
- 30.Griffiths A, Paracha N, Davies A, Branscombe N, Cowie MR, Sculpher M. The cost effectiveness of ivabradine in the treatment of chronic heart failure from the UK National Health Service perspective. Heart. 2014;100(13):1031–1036. doi: 10.1136/heartjnl-2013-304598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Griffiths A, Paracha N, Davies A, Branscombe N, Cowie MR, Sculpher M. Analyzing health-related quality of life data to estimate parameters for cost-effectiveness models: an example using longitudinal EQ-5D data from the SHIFT randomized controlled trial. Adv Ther. 2017;34(3):753–764. doi: 10.1007/s12325-016-0471-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Téhard B, Detournay B, Borget I, Roze S, De Pouvourville G. Value of a QALY for France: a new approach to propose acceptable reference values. Value Health. 2020;23(8):985–993. doi: 10.1016/j.jval.2020.04.001. [DOI] [PubMed] [Google Scholar]
- 33.Galinier M, Roubille F, Berdague P, Brierre G, Cantie P, Dary P, et al. Telemonitoring versus standard care in heart failure: a randomised multicentre trial. Eur J Heart Fail. 2020;22(6):985–994. doi: 10.1002/ejhf.1906. [DOI] [PubMed] [Google Scholar]
- 34.Tuppin P, Rivière S, Rigault A, Tala S, Drouin J, Pestel L, et al. Prevalence and economic burden of cardiovascular diseases in France in 2013 according to the national health insurance scheme database. Arch Cardiovasc Dis. 2016;109(6–7):399–411. doi: 10.1016/j.acvd.2016.01.011. [DOI] [PubMed] [Google Scholar]
- 35.Xiang R, Li L, Liu SX. Meta-analysis and meta-regression of telehealth programmes for patients with chronic heart failure. J Telemed Telecare. 2013;19(5):249–259. doi: 10.1177/1357633X13495490. [DOI] [PubMed] [Google Scholar]
- 36.Jiang X, Yao J, You JH. Telemonitoring versus usual care for elderly patients with heart failure discharged from the hospital in the United States: cost-effectiveness analysis. JMIR mHealth uHealth. 2020;8(7):e17846. doi: 10.2196/17846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cleland JG, Louis AA, Rigby AS, Janssens U, Balk AH, Investigators T-H. Noninvasive home telemonitoring for patients with heart failure at high risk of recurrent admission and death: the Trans-European Network-Home-Care Management System (TEN–HMS) study. J Am Coll Cardiol. 2005;45(10):1654–1664. doi: 10.1016/j.jacc.2005.01.050. [DOI] [PubMed] [Google Scholar]
- 38.Piña IL, Allen LA, Desai NR. Managing the economic challenges in the treatment of heart failure. BMC Cardiovasc Disord. 2021;21(1):612. doi: 10.1186/s12872-021-02408-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file1. Description of patients from the SCAD cohort
Additional file2. Kaplan–Meier survival curves stratified by level of SCAD use
Additional file3. Costs for healthcare resource consumption determined in the SCAD–SNDS linkage study.
Additional file4. Input data for the scenario analyses: clinical events
Data Availability Statement
All data and software used to construct this model are identified either in the manuscript or in cited source references.