

Abstract
Introduction:
Experiencing adolescent relationship abuse (ARA) negatively impacts sexual health and influences risk behaviors of adolescent girls. ARA may be associated with more inequitable gender attitudes among girls, a potentially modifiable factor in violence prevention. This study examines the association among gender equitable attitudes, experiences of ARA, and sexual behaviors among girls participating in Sisterhood 2.0, a community-based violence prevention program implemented in low resource neighborhoods.
Methods:
Data were from baseline surveys collected for Sisterhood 2.0 implemented in Pittsburgh, PA. Participant demographics, gender equitable attitudes, self-efficacy to use condoms with partners, and self-efficacy to select appropriate contraception were assessed. A latent class analysis (LCA) estimated probability of responses to nine indicators, including sexual behavior self-efficacy and violence. Multigroup LCA by grade (9–12) was also estimated and analyses were performed with SAS V9.4.
Results:
Female-identified adolescents ages 13–19 (n = 246) were primarily Black (75%) and evenly distributed across grade in school. Sixty-five percent reported emotional relationship abuse and 31% reported physical abuse within the previous nine months. A three-class solution was best fitting for the LCA. Experiences of violence were related to less equitable gender attitudes, being sexually active, and lower condom and contraception self-efficacy. Younger participants who were sexual minorities with less educated heads of household had more experiences with ARA and less equitable gender attitudes.
Discussion:
Gender equitable attitudes were lower in adolescent girls with greater experiences of ARA and worse condom and contraception self-efficacy. Integrating discussions about healthy sexual relationships and gender equity may be salient factors in violence prevention.
Keywords: adolescent relationship abuse, sexual health, gender equitable attitudes, violence prevention, adolescent girls
Introduction
An estimated one third of all women in the United States reported physical or sexual intimate partner violence (IPV) in the 2015 National Intimate Partner and Sexual Violence Survey, underscoring the need for effective prevention measures (Breiding et al., 2014; Smith et al., 2018). Intimate partner violence may include any emotional, physical or sexual abuse from a romantic partner. IPV exposure may begin as early as adolescence, with an estimated 26% of all victims of IPV experiencing abuse in a romantic relationship before the age of 18 (Smith et al., 2018). In 2019, roughly 21% of girls that had been in a relationship in the past year reported physical or sexual IPV (Rome & Miller, 2020). Additionally, in one survey of school based health centers, 18% of adolescent girls reported recent experiences of physical or sexual IPV and an increasing likelihood of reproductive coercion resulting from those experiences (Hill et al., 2019). An emphasis on understanding influencers and determining appropriate prevention of adolescent relationship abuse (ARA), defined as any physical, sexual, or emotional abuse by a dating or romantic partner or ex-partner during adolescence, is necessary to reduce prevalence in adolescence.
There is robust evidence to suggest that men who endorse harmful gender attitudes are more likely to perpetrate violence in their relationships (Espelage, Basile, et al., 2018; Hequembourg et al., 2020; Hill et al., 2020; McCauley et al., 2013; Okeke et al., 2019). While less is known about this relationship in adolescent boys, literature increasingly demonstrates the relationship between harmful gender attitudes and violence perpetration (Das et al., 2014; Miller et al., 2020; Reyes et al., 2016). Numerous studies have also shown that inequitable gender norms among men are associated with increased risk for inconsistent condom use, HIV, sexually transmitted infections, and foregone medical care (American Psychological Association, 2018; Closson et al., 2020; Gage, 2008; Jewkes & Morrell, 2010; Marcell et al., 2007; Rolleri, 2013). There are decades of rigorous research demonstrating the adverse health consequences of experiencing violence, particularly in the realm of sexual and reproductive health (Boykins et al., 2010; Eisman et al., 2018; Hill et al., 2020; Preiser & Assari, 2017). Individuals who have been exposed to partner violence are less likely to use appropriate contraception and are more likely to have unintended pregnancy, as well as HIV and other sexually transmitted infections (Hill et al., 2019; World Health Organization, 2013).
In contrast, research among women regarding gender attitudes and their health impact is more nascent. For example, Vu et al. (2017) conducted a study in Uganda with male and female adolescents, discovering that inequitable norms were associated with both partner violence and early sexual debut. More research is needed to better understand how women’s endorsement of harmful societal norms around gender can impact experiences of IPV, ARA and sexual health. While women and minorities are not to blame for the experiences that happen to them, intervening to promote and enhance positive gender norms may be an untapped intervention tool to reduce the prevalence of ARA in minority young people. Evidence that ARA and gender-based harassment behaviors are prevalent in adolescence, and increase as youth age, strongly support the need to begin prevention programming aimed at promoting gender equitable attitudes, healthy relationships and healthy sexuality during early adolescence (Cui et al., 2013; Decker et al., 2014; Johnson et al., 2015; Straus & Mickey, 2012).
ARA is associated with health risk behaviors such as tobacco, alcohol, and drug use (Espelage et al., 2018), and poor health outcomes such as anxiety and depression (Catabay et al., 2019), sexually transmitted infections (STIs), and unintended pregnancy (Decker et al., 2005). Health behaviors, socioeconomic status, and environmental factors may interact differently to heighten risk of adverse outcomes among socially marginalized individuals based on their race/ethnicity, gender and sexual minority status, which are inextricably linked to social disadvantage and greater morbidity compared to White young women (Singer et al., 2017). Syndemics, a framework traditionally used to explain the interrelationship between violence, HIV risk, substance use and sexual behaviors, has increasingly been applied to elucidate factors associated with increased prevalence of STIs/HIV in women and the clustering and intersecting circumstances that exacerbate poor reproductive health outcomes (Singer et al., 2006). For example, some young sexually active women and girls find themselves at the intersections of multiple forms of marginalization (such as sexism, racism, homophobia, classism) and experiences with IPV or ARA that may impact their reproductive decision making (e.g., condom and contraception use) further amplifying and exacerbating adverse outcomes in the context of this marginalization (Cho et al., 2013). Additionally, repeat and continued marginalization may impact how the individual views themselves and may lead to internalized negative ideals that they in turn enact upon others that share similar identities (Jones, 2000; McKenney & Bigler, 2016; Puigvert et al., 2019). However, interventions to reduce these health inequities, including measures to reduce violence exposure among adolescent girls, are limited (Sabri & Gielen, 2019). More efforts are needed to reduce women’s experiences with ARA earlier in life.
Elucidating how gender attitudes may be associated with experiences of ARA, sexual health behaviors, and specific demographic characteristics may help to better tailor ARA prevention and sexual health promotion interventions for different subpopulations. Therefore, the objective of this study, grounded in a syndemic framework, was to examine the relationship between gender equitable attitudes, ARA victimization, condom and contraception self-efficacy indicators among a racially diverse sample of adolescent girls participating in a community-based violence prevention intervention. We hypothesized that ARA victimization would occur simultaneously with inequitable gender attitudes and low self-efficacy to use contraception.
Methods
Data were from the baseline assessment of a quasi-experimental pilot study examining the effectiveness of an ARA and SV prevention program for high school-aged adolescent girls (“A Feasibility Trial of Sisterhood 2.0”)(Clinical Trials Nct, 2020)(HIll et al., 2022). Participants were ages 13–19 years recruited between 2017–2019 through community organizations from neighborhoods in Pittsburgh, Pennsylvania (Eugene et al., 2017). Set in racially-segregated urban neighborhoods with concentrated disadvantage where ARA and violence prevention programs are scarce, community facilitators guided weekly discussions on racial and reproductive justice, social media and cyber abuse, sexual health and healthy relationships, gender attitudes, and norms surrounding bystander behaviors. The primary focus of the intervention was to reduce instances of ARA victimization and perpetration, improve self-efficacy for condom and contraceptive use, improve recognition of abuse and intentions to intervene when ARA is witnessed among peers, improve gender equitable attitudes and improve condom and contraceptive use at last sex. This study was reviewed and approved by the University of Pittsburgh Institutional Review Board.
The study population included middle and high school-aged girls (ages 13–19) living in socially disadvantaged, racially-segregated neighborhoods of Pittsburgh, Pennsylvania, where the prevalence of poverty, school suspension, and community violence are higher than in contiguous neighborhoods (Brinkman et al., 2019; Goodkind & Workgroup, 2019; Howell et al., 2019). The rationale for focusing on youth in neighborhoods with concentrated disadvantage was two-fold. First, racial/ethnic health inequities in Pittsburgh are stark (Howell, Goodkind, Jacobs, &, & Miller, 2019); tailored social and economic justice-informed prevention efforts are needed, especially programs that offer positive youth development opportunities. Second, through asset mapping and established partnerships (Eugene et al., 2017), the research team identified trusted and respected community members who used existing social networks to recruit adolescent girls in these neighborhoods (Abebe et al., 2018).
Measures
All measures included for this analysis were from baseline surveys of participants prior to randomization to intervention or control arms.
Demographics
Participants reported on their race/ethnicity, gender, sexual orientation, neighborhood of residence, grade, age and head of household highest education level. Because limited demographic and household information was collected, the head of household education status was used as a proxy for socioeconomic status.
Experiences with Adolescent Relationship Abuse or Partner Violence
A modified version of the revised conflict tactics scale by Cascardi and colleagues (Cascardi et al., 1999; Straus, 2007) which included only questions validated for adolescent girls was used to assess physical, emotional or sexual relationship abuse experiences in the last 9 months. Participants rated their experiences with each statement based on their current or most recent romantic relationship using “never”, “seldom”, “sometimes”, “often”, or “n/a”. Statements included: “My partner spoke to me in a hostile or mean tone of voice or insulted me with put-downs” to indicate emotional abuse, “My partner kicked, hit, punched, slapped me or pulled my hair” or “My partner threatened to hit, throw something at me, or hurt me” to indicate physical abuse, and “My partner forced me to have sex” to indicate sexual abuse. Responses were separated into three types of abuse, physical, emotional or sexual (Cronbach’s alpha: 0.98). Responses to the questions were dichotomized to “never” or any indication of physical, emotional or sexual violence exposure for inclusion in the LCA models. The specific type of abuse was reported separately in the demographic table and were included separately in the LCA. Responses of “n/a” were recoded as missing.
Gender Equitable Attitudes
A 13-item validated scale was used to measure participants’ views on gender norms and their ability to identify equitable or inequitable ideas around gender related activities (Cronbach’s alpha: 0.71) (Abebe et al., 2018; Carlyle et al., 2020; Chu et al., 2005; Pulerwitz & Barker, 2008; Weisz & Black, 2001). Statements included “A guy takes responsibility for his actions” and “A girl wearing revealing clothing deserves to have comments made about her.” Response options were on a 5-point scale from “strongly disagree” to “strongly agree”; items were appropriately reverse-coded, and a mean score across items was calculated (range 1 to 5), with a higher score indicating more equitable attitudes. To include this measure in the LCA, responses were dichotomized; those with a mean score of 4 or higher (i.e., top quartile: respondents who agreed or strongly agreed with the majority of gender equitable attitudes) were noted to have “gender equitable attitudes” and those with a mean score of below 4 (i.e., respondents who were neutral, disagreed, or strongly disagreed with the majority of gender equitable attitudes) were noted to have “gender inequitable attitudes”(Vu et al., 2017).
Sexual History and Behaviors
Participants were asked about the following sexual behaviors taken directly from the Youth Risk Behavior Survey (Frankel et al., 2018; Kann et al., 2018): (1) “Have you ever had vaginal sex (someone’s penis went into your vagina)?”; (2) “Have you ever had anal sex (someone’s penis went into your anus)?”; (3) “How old were you when you had sexual intercourse for the first time?”; and (4) “During your life, with how many people have you have sexual intercourse?” Response options were yes/no and free response to include the numeric age at first sex and the number of lifetime partners. For this analysis, questions 1 and 2 were collapsed into one variable indicating any lifetime sex and dichotomized to indicate yes or no.
Condom and Contraception Self-Efficacy
Self-efficacy was assessed using two different previously validated scales; the first employed a 15-item scale to assess participants’ confidence to negotiate condom use with a partner (Cronbach alpha: 0.81) (Brafford & Beck, 1991). Five response options ranged from “strongly disagree” to “strongly agree” and a mean score was calculated (range 1 to 5) with higher scores indicating greater condom negotiation self-efficacy. Based on previous studies (Abebe et al., 2018; K. A. Jones et al., 2016), responses were dichotomized to indicate “high condom negotiation self-efficacy” with a score of 4 or higher (i.e., respondents who agreed or strongly agreed with the majority of condom negotiation self-efficacy items) and scores less than 4 indicated “moderate and low condom negotiation self-efficacy” (i.e., respondents who were neutral, disagreed, or strongly disagreed with the majority of condom negotiation self-efficacy items) to be included in the LCA. The second scale included 10 positive- and negatively-worded statements assessing participants’ self-efficacy to select and appropriately use condoms and other contraceptives (e.g., “Using birth control is too much trouble or too much of a hassle to use”) (Cronbach alpha: 0.47) (Aalsma et al., 2012; Borrero et al., 2013; Carvajal et al., 2014). Responses were on a 5-point scale from “strongly disagree” to “strongly agree”; negative items were reverse-coded. A mean score was calculated (range 1 to 5); higher scores indicated greater self-efficacy to select and use condom and other contraceptives. Responses were dichotomized in a similar manner to the condom negotiation self-efficacy measure (Vasilenko et al., 2015).
Data Analysis
Latent class analysis (LCA) was used to examine similar characteristics of participants in this study. LCA allows for identification of unobserved subgroups in a population with a selected set of indicators of interest and provides a view of the association of these indicators that must be considered concurrently among a population of interest. In this study, LCA examined class membership probabilities related to indicators of any ARA, gender equitable attitudes, and sexual health self-efficacy. Descriptive statistics of the sample and variables of interest were reported first. Models were compared using common goodness-of-fit measures, including the G2 likelihood ratio chisquare test, the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and entropy (Nylund-Gibson & Choi, 2018). Lower values indicate optimal model fit and parsimony. The PROC LCA procedure in SAS was used to create these profiles. Missing data were handled with the maximum likelihood expectation maximization procedure and assumed to be missing completely at random in PROC LCA.
Before conducting the analysis, measurement invariance across grades (8th–12th) was examined to determine if responses from participants in different grades or age groups were significantly different (Lanza & Rhoades, 2013). Participants were from a wide range of ages (13–19) and may be at different developmental stages that impact their experiences with the variables of interest. Upon constraining the model to be similar, probabilities were found to be significantly different across grades (p < .0001) and a multigroup LCA was employed. The best fitting model was selected and conditional probabilities of girls within a latent class responding to each item were displayed in the results tables. Classes were interpreted based on variables having the highest reported conditional probabilities across classes. A total of 289 participants were recruited at baseline, with 246 (85%) providing complete data on the variables of interest and were retained for analysis.
Results
Young women in the sample were primarily Black (74%) or Multiracial (9%), were in the 9th (21%) or 10th grade (21%), and 27% had a parent or guardian who was college-educated (Table 1). Most girls reported heterosexual status (67%), with 33%) identifying as sexual minority. Only a third of participants (30%) endorsed ever having sex. Almost two thirds (63%) of participants reported any experiences with emotional abuse from a sexual or romantic partner in the past nine months. Approximately 31% of girls reported physical abuse, and 12% said they had been a victim of sexual relationship abuse in the past nine months.
Table 1.
Sample Characteristics for Sisterhood 2.0 girls ages 13–19, 2017–2019 (N = 246).
| Characteristics | Total (n = 246) No. (%) |
Missing |
|---|---|---|
|
| ||
| Grade level | ||
| 8th | 40 (16%) | |
| 9th | 53 (21%) | |
| 10th | 52 (21%) | |
| 11th | 36 (15%) | |
| 12th | 34 (14%) | 31 |
| Race/ethnicity | ||
| Black/African-American | 159 (74.3%) | |
| Multiracial | 20 (9.3%) | |
| White | 15 (7.0%) | |
| Otherb | 8 (3.7%) | |
| Hispanic/Latino | 12 (5.6%) | 32 |
| Sexual Minority Status | ||
| Heterosexual | 134 (67.0%) | |
| Sexual minority | 66 (33.0%) | 40 |
| Highest parental education | ||
| Less than high school | 76 (30.9%) | |
| High school graduate | 21 (8.5%) | |
| Some college | 46 (18.7%) | |
| College graduate/Graduate school | 67 (27.2%) | 36 |
| Experiences with Partner Violence | ||
| Any physical violence | 73 (30.8%) | |
| Any sexual violence | 29 (12.3%) | |
| Any emotional abuse | 149 (63%) | 27 |
| Sexual History | ||
| Ever had sex | 73 (30.4%) | 6 |
| Self-efficacy to effectively select and use contraception | ||
| High (average of 4 or higher) | 107 (45.7%) | |
| Moderate to low | 127 (54.3%) | 12 |
| Self-efficacy to effectively use condoms with a sex partner | ||
| High (average of 4 or higher) | 97 (41.4%) | |
| Moderate to low | 137 (58.6%) | 12 |
| Gender equitable attitudes | ||
| High (average of 4 or higher) | 99 (41.4%) | |
| Moderate to low | 140 (58.6%) | 7 |
Model fit criteria are displayed in Table 2; the three-class model provided optimal fit and parsimony and was selected as the appropriate model for these data. Table 3 displays the class memberships and probabilities of response from the LCA. Class 1 was comprised of n=95 girls who had roughly 55% chance of having a parent with a high school education or less. Approximately 71% had experienced physical abuse, and almost all endorsed experiences of emotional abuse (99%). Physical and emotional abuse was associated with less equitable gender attitudes (36%) and lower contraception (31%) and condom use self-efficacy (33%) in this group. Class 2 included n=53 girls who primarily had parents with a high school education or less (75%) and experienced emotional abuse (56%) from a partner, but endorsed higher gender equitable attitudes (64%), contraception (84%) and condom use self-efficacy (90%). Girls in Class 3 (n=98) made up the largest proportion of the sample. While the probability of having a parent with a high school education or less was higher (74%), the probability of experiencing any form of relationship abuse, being sexually active (11%), and having contraception (39%) and condom use (17%) self-efficacy were low. Figure 1 further delineates findings from the LCA. Multinomial logistic regression was used to estimate the influence of grade in school and race on class membership for Classes 1 and 2 with Class 3 as reference. Belonging to Class 2 was significantly associated with the participant’s grade in school (OR 2.74, 95% CI 1.71–4.39). No other significant relationships were found.
Table 2.
Fit indices and classification quality for Latent Class Analysis (LCA) model selection.
| No. of Classes | Log likelihood | Likelihood Ratio G2 | Degrees of freedom | AIC | BIC | Adjusted BIC | Entropy |
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1 | −1425.18 | 587.42 | 1013 | 607.42 | 642.47 | 610.78 | 1.00 |
| 2 | −1377.44 | 491.94 | 1002 | 533.94 | 607.55 | 540.98 | 0.66 |
| 3* | −1347.79 | 432.63 | 991 | 496.63 | 608.80 | 640.80 | 0.67 |
| 4 | −1340.04 | 417.13 | 980 | 503.13 | 653.85 | 517.55 | 0.67 |
| 5 | −1333.48 | 404.01 | 969 | 512.01 | 701.29 | 530.12 | 0.74 |
| 6 | −1323.76 | 384.58 | 958 | 514.58 | 742.42 | 536.37 | 0.75 |
Indicates selected model
Table 3.
Class membership, item response probabilities and covariate associations from Latent Class Analysis.
| Item/Variable | Class 1 (38.5%, n = 95) | Class 2 (21.8%, n = 53) | Class 3 (39.8%, n = 98) |
|---|---|---|---|
|
| |||
| Parent less than HS education | 0.55 | 0.75 | 0.74 |
| Identify as sexual minority | 0.45 | 0.25 | 0.26 |
| Experienced physical violence | 0.71 | 0.11 | 0.05 |
| Experienced sexual violence | 0.31 | 0.08 | 0.00 |
| Experienced emotional | 0.99 | 0.56 | 0.29 |
| violence | |||
| Ever had sex | 0.40 | 0.44 | 0.11 |
| High gender equitable attitudes | 0.36 | 0.64 | 0.31 |
| High contraception self | 0.31 | 0.84 | 0.39 |
| efficacy | |||
| High condom self efficacy | 0.33 | 0.90 | 0.17 |
| Grade | 1.11 (0.81–1.53) | 2.74 (1.71–4.39) | reference |
| Race | 1.04 (0.77–1.39) | 1.06 (0.69–1.63) | |
Bolded items indicate probabilities greater than 0.50.
Figure 1.
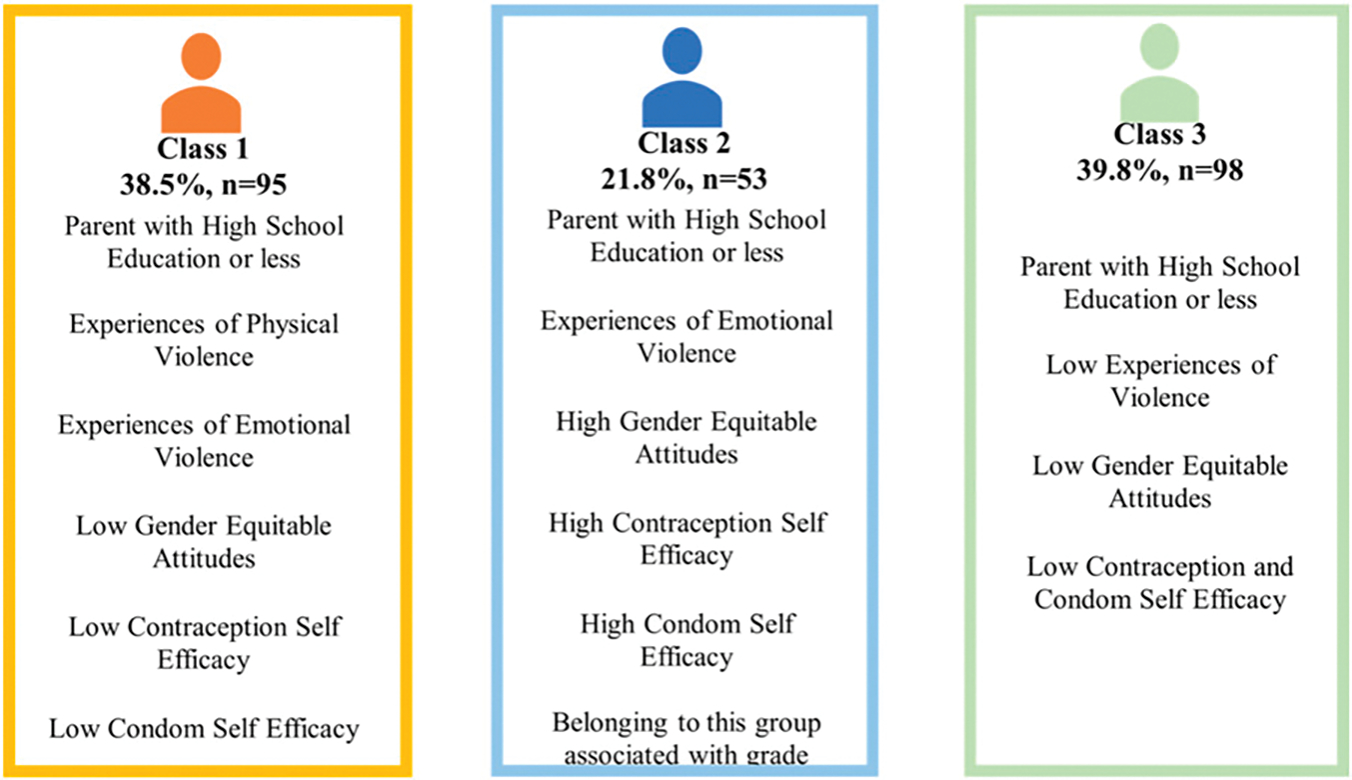
Description of Classes and Influence of Grade on Class Membership.
To determine specific predictors of class membership by grade, a multigroup LCA was performed (Table 4). Five levels of grade were used in the multigroup analysis and included 8th-12th grade. While all analyses are shown in Table 4, two grades revealed distinct patterns. Among 8th graders (n=40), class membership was approximately equal across each of the three classes. In the first class, participants primarily endorsed having a less educated parent (64%), experiencing physical (56%) and emotional abuse (100%), low gender equitable attitudes (24%), higher contraception (58%) and condom use self-efficacy (50%). In the second class of 8th graders, roughly half (52%) identified as sexual minorities, were more likely to experience physical (90%), sexual (50%) and emotional abuse (100%) and have moderate gender equitable attitudes (42%). The third class of 8th graders had primarily less educated parents (64%) and low gender equitable attitudes (21%) but no other co-occurring indicators.
Table 4.
Multigroup Latent Class Analysis by Participant Grade.
| Grade | 8th n = 40 (class #) | 9th n = 53 (class #) | 10th n = 52 (class #) | 11th n = 36 (class #) | 12th n = 34 (class #) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||||||
| Item/Variable | (1) 33% | (2) 30% | (3) 37% | (1) 30% | (2) 11% | (3) 59% | (1) 43% | (2) 17% | (3) 41% | (1) 40% | (2) 10% | (3) 50% | (1) 18% | (2) 19% | (3) 63% |
| Parent less than HS education | 0.64 | 0.48 | 0.60 | 0.09 | 1.00 | 0.46 | 0.43 | 0.63 | 0.39 | 0.72 | 0.28 | 0.56 | 0.61 | 1.00 | 0.54 |
| Identify as sexual minority | 0.36 | 0.52 | 0.40 | 0.45 | 0.00 | 0.12 | 0.44 | 0.00 | 0.37 | 0.36 | 0.00 | 0.25 | 0.20 | 0.49 | 0.31 |
| Experienced physical violence | 0.56 | 0.90 | 0.00 | 0.49 | 0.76 | 0.10 | 0.55 | 0.24 | 0.00 | 0.35 | 0.56 | 0.00 | 1.00 | 0.82 | 0.00 |
| Experienced sexual violence | 0.10 | 0.50 | 0.00 | 0.00 | 0.50 | 0.00 | 0.27 | 0.00 | 0.00 | 0.16 | 1.00 | 0.00 | 0.50 | 0.33 | 0.05 |
| Experienced emotional violence | 1.00 | 1.00 | 0.17 | 1.00 | 1.00 | 0.26 | 1.00 | 1.00 | 0.33 | 1.00 | 1.00 | 0.28 | 1.00 | 1.00 | 0.38 |
| Ever had sex | 0.00 | 0.51 | 0.07 | 0.51 | 0.00 | 0.00 | 0.48 | 0.70 | 0.17 | 0.68 | 0.53 | 0.29 | 0.35 | 1.00 | 0.25 |
| High gender equitable attitudes | 0.24 | 0.42 | 0.21 | 0.70 | 0.00 | 0.44 | 0.22 | 1.00 | 0.41 | 0.39 | 0.74 | 0.43 | 0.00 | 1.00 | 0.52 |
| High contraception self efficacy | 0.58 | 0.00 | 0.49 | 0.36 | 0.23 | 0.31 | 0.28 | 0.69 | 0.41 | 0.29 | 1.00 | 0.86 | 0.67 | 0.41 | 0.71 |
| High condom self efficacy | 0.50 | 0.00 | 0.15 | 0.60 | 0.45 | 0.21 | 0.43 | 1.00 | 0.24 | 0.44 | 0.21 | 0.76 | 0.40 | 0.37 | 0.75 |
Values are bolded if the probability is greater than 0.50.
Similarly, ninth grade girls also belonged to three distinct classes. Majority of girls in the 9th grade (59%) were in Class 3 and did not overwhelmingly endorse any item. However, Class 1 (30%) primarily reported emotional abuse (100%), being sexually active (51%), having higher gender equitable attitudes (70%), and higher condom self efficacy (60%). Among Class 2 (11%), all participants had less educated parents (100%), majority primarily reported experiences of physical (76%), sexual (50%), and emotional abuse (100%). None of the girls in this class had high gender equitable attitudes.
Discussion
The findings of this study, conducted among a racially diverse sample of adolescent girls from low resource neighborhoods, suggest that girls who experienced less ARA reported higher gender equitable attitudes. However, greater experiences with ARA was most strongly associated with less equitable gender attitudes among the youngest participants. Girls who reported experiences of ARA also consistently reported less self-efficacy to negotiate condom use or select appropriate contraception. Younger girls, particularly those who are sexually active, may have less opportunity developmentally to learn about and identify unhealthy relationships, to challenge rigid gender norms or understand gender equity (McKenney & Bigler, 2016; Puigvert et al., 2019). It is plausible a correlation between reporting high levels of physical, sexual, and emotional abuse and identifying as a sexual minority exists in eighth grade respondents. Younger girls who identify as sexual minority may have already received harmful messages from peers and family members that reinforce gender inequity (Johnson, 2003). Studies should continue to explore the impact of multiple marginalized identities on adolescent girl’s gender attitudes and experiences with ARA.
Social context and factors play a major role in the development of gender equitable attitudes and healthy sexuality. Understanding the multiple influencing factors influencing self efficacy to effectively select and use contraception in adolescents may provide an opportunity to develop effective and culturally appropriate interventions to engage harder-to-reach adolescents, especially those living in low resource neighborhoods with concentrated disadvantage. Study participants were fairly racially homogenous, with roughly 75% identifying as Black in the present study. In the US, young Black women report disproportionately higher rates of IPV and SV compared to white women (Cheng & Lo, 2016). Roughly 7% of Black adolescent girls reported experiencing sexual ARA and 11% reported experiencing sexual violence in the past year (Alexander et al., 2019; Holliday et al., 2017). These disparities are also apparent in STIs, which disproportionately affect young Black women (CDC, 2018; L. Kann et al., 2018). It will continue to be important to understand the context of lived experiences of minority women at highest risk for experiences of partner and relationship violence and adverse sexual health. The findings from the current study highlight that there are significant differences in experiences with ARA, gender attitudes, and condom and contraception self efficacy among girls living in poverty (reflected in the lower levels of parental education). Notably, high levels of experiences with ARA tended to cluster with lower gender equitable attitudes and poor condom and contraception self efficacy, suggesting that trauma-focused interventions for youth with prior experiences with partner or relationship violence that intentionally address gender norms within dating and sexual relationships may be especially relevant (“A Feasibility Trial of Sisterhood 2.0”(Clinical Trials Nct, 2020; HIll et al., 2022; Reidy et al., 2017).
These findings highlight the prevalence of ARA in early adolescent girls, underscoring the need to focus on this developmental stage, especially among girls who may already be sexually active or identify as sexual minorities. Growing evidence supports the integration of gender and power in sexuality education and suggests this approach is more effective than sexual health programs that do not address gender equity (Haberland, 2015). Gender transformative interventions– approaches that challenge rigid gender norms and seek to promote gender equity– have gained attention within violence prevention efforts among boys and men especially (McCauley et al., 2013; Miller et al., 2020). However, evidence for violence prevention programs tailored for women and girls is still emerging. For example, examinations of gender attitudes among international populations have revealed that inequitable gender attitudes influence women’s acceptance of violence in their marriage (Thulaseedharan, 2019). Sexually active young women, aged 16–24, with higher sexual and relationship power equity were less likely to report recent partner violence (Closson et al., 2019). ARA and SV prevention programs that highlight that women are not to blame for the relationship violence they experience and encourage critical reflections on gender inequities are showing promise in the US with college-age young adults (Senn et al., 2015) and internationally with high school age youth (Sinclair et al., 2013). Adapting such programs for adolescent girls earlier in adolescence may be a promising approach to reduced ARA and improve sexual health self efficacy.
These are baseline findings from a gender transformative violence prevention program for girls currently being evaluated. Findings from this intervention are expected to contribute to the emerging research on effectiveness of gender transformative programming tailored for female-identified youth, with the goal of reducing relationship violence among women and girls. However, it is not clear from the present cross-sectional evaluation the extent to which relationship violence and ARA exposure may contribute to more internalized gender inequitable attitudes. Alternatively, perhaps having less equitable gender attitudes may, in turn, potentially influence risk for experiences with ARA/SV in adolescent girls. Partner violence prevention is inextricably linked to sexual health promotion, and including content in violence prevention programs that are explicitly focused on positive sexuality and sexual health are likely necessary for optimal effectiveness (Basile et al., 2016). Longitudinal studies are needed to evaluate prevention programs tailored for early adolescent girls that nurture more gender equitable attitudes and shift expectations for healthy relationships in general. However, this study suggests that tailoring messaging is likely needed for younger girls who may be from low income or low resource neighborhoods, who are sexually active and who identify as sexual minorities. Tailored interventions should interrogate the socialization processes through which young women and girls learn and internalize harmful gender stereotypes about themselves and their counterparts. These tailored interventions may offer approaches to increase awareness of their gender attitudes and promote positive sexual and reproductive health by integrating healthy sexuality, gender equity promotion and ARA prevention, among other relevant topics. Effective prevention strategies should tailor messages to include relevant information for populations at increased risk of reproductive health inequities, like Black and other minority girls and women (Anachebe & Sutton, 2003).
These findings should be interpreted considering several limitations. Data from this study were collected at one time point, precluding any causal inferences, and included baseline responses from girls participating in a pilot intervention trial, thus may introduce both selection and participation bias. Responses from participants were collected prior to delivery of the intervention removing the need to account for intervention effects in this sample. Data were self-reported by girls at the beginning of the study and those with complete data were included for analysis regardless of their age. Additionally, measures of sexual activity with same sex partners were not captured and sexual behaviors may not be equally represented in this sample. The wide range of ages of the sample (13–19) include youth at different developmental and life stages. The analysis in this study attempted to account for that by examining latent classes by grade and determining some specific opportunities for intervention among younger participants. Roughly 5% (n=12) of participants had missing data on gender equitable attitude, condom and contraceptive self efficacy and were considered missing completely at random. Findings may only be applied to this sample of girls and may not be representative of girls in other geographic regions. The Cronbach alpha values of our measures fell below the commonly-cited threshold of 0.7; this may be because these scales are comprised of multiple factors (Nunnally, 1978). Despite these limitations, this study provides impetus to further explore the impacts of internalized harmful gender stereotypes on experiences of violence and sexual health self-efficacy for young girls.
Programs that challenge harmful gender norms currently exist, however few programs exclusively focus on younger minority girls. Internalized negative attitudes related to gender equity may impact young women’s experiences with partner violence and adolescent relationship abuse, such that experiences with such forms of violence is normalized and even expected. Including assessments of gender attitudes in ARA prevention demonstrates promise and may be particularly necessary for younger girls who may identify as sexual minorities. While integrating education on gender and power, respectful and equitable relationships, healthy sexuality and sexual behaviors is likely relevant for adolescents in general, ARA prevention efforts tailored for specific subpopulations of youth especially in early adolescence are needed.
Funding
This research was supported by a National Institute of Child Health and Human Development T32, HD087162 (PI: Miller) and a National Institute on Minority Health and Health Disparities L60 MD015553 supporting AV Hill. The funder did not participate in this work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Aalsma MC, Carpentier MY, Azzouz F, & Fortenberry JD (2012). Longitudinal effects of health-harming and health-protective behaviors within adolescent romantic dyads. Social Science & Medicine, 74(9), 1444–1451. 10.1016/j.socscimed.2012.01.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abebe KZ, Jones KA, Culyba AJ, Feliz NB, Anderson H, & Torres I (2018). Engendering healthy masculinities to prevent sexual violence: Rationale for and design of the Manhood 2.0 trial. Contemporary Clinical Trials, 71, 18–32. 10.1016/j.cct.2018.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alexander KA, Willie TC, McDonald-Mosley R, Campbell JC, Miller E, & Decker MR (2019). Associations between reproductive coercion, partner violence, and mental health symptoms among young black women in Baltimore, Maryland. Journal of Interpersonal Violence, 36(17–18), NP9839–NP9863. 10.1177/0886260519860900 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychological Association. (2018). APA guidelines for psychological practice with boys and men. https://www.apa.org/about/policy/boys-men-practice-guidelines.pdf
- Anachebe NF, & Sutton MY (2003). Racial disparities in reproductive health outcomes. American Journal of Obstetrics and Gynecology, 188(4), S37–S42. 10.1067/mob.2003.245 [DOI] [PubMed] [Google Scholar]
- Basile KC, DeGue S, Jones K, Dills J, Smith SG, & Raiford JL (2016). Stop SV: A technical package to prevent sexual violence. National Center for Injury Prevention and Contol, Centers for Disease Control and Prevention. [Google Scholar]
- Borrero S, Farkas A, Dehlendorf C, & Rocca CH (2013). Racial and ethnic differences in men’s knowledge and attitudes about contraception. Contraception, 88(4), 532–538. 10.1016/j.contraception.2013.04.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boykins AD, Alvanzo AA, Carson S, Forte J, Leisey M, & Plichta SB (2010). Minority women victims of recent sexual violence: Disparities in incident history. Journal of Women’s Health, 19(3), 453–461. 10.1089/jwh.2009.1484 [DOI] [PubMed] [Google Scholar]
- Brafford LJ, & Beck KH (1991). Development and validation of a condom self-efficacy scale for college students. J Am Coll Health, 39(5), 219–225. 10.1080/07448481.1991.9936238 [DOI] [PubMed] [Google Scholar]
- Breiding MJ, Smith SG, Basile KC, Walters ML, Chen J, & Merrick MT (2014). Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization–national intimate partner and sexual violence survey, United States, 2011. MMWR Surveill Summ, 63(8), 1–18. [PMC free article] [PubMed] [Google Scholar]
- Brinkman BG, Garth J, Horowitz KR, Marino S, & Lockwood KN (2019). Black Girls and sexuality education: Access, equity, justice gwendolyn J. Elliott Institute at Gwen’s Girls. [Google Scholar]
- Carlyle KE, Conley AH, & Guidry JP (2020). Development and evaluation of the red flag campaign for the primary prevention of sexual and dating violence on college campuses. Journal of American College Health, 9, 1–5. 10.1080/07448481.2020.1726924. [DOI] [PubMed] [Google Scholar]
- Carvajal DN, Ghazarian SR, Shea Crowne S, Bohrer Brown P, Carter Pokras O, Duggan AK, et al. (2014). Is depression associated with contraceptive motivations, intentions, and use among a sample of low-income Latinas? Women’s Health Issues: Official Publication of the Jacobs Institute of Women’s Health, 24(1), e105–113. 10.1016/j.whi.2013.10.003 [DOI] [PubMed] [Google Scholar]
- Cascardi M, Avery-Leaf S, O’Leary KD, & Slep AMS (1999). Factor structure and convergent validity of the Conflict Tactics Scale in high school students. Psychological Assessment, 11(4), 546–555. 10.1037/1040-3590.11.4.546 [DOI] [Google Scholar]
- Catabay CJ, Stockman JK, Campbell JC, & Tsuyuki K (2019). Perceived stress and mental health: The mediating roles of social support and resilience among black women exposed to sexual violence. Journal of Affective Disorders, 259, 143–149. 10.1016/j.jad.2019.08.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC. (2018). Sexually transmitted disease surveillance 2018. CDC [Google Scholar]
- Cheng TC, & Lo CC (2016). Racial disparities in intimate partner violence examined through the multiple disadvantage model. Journal of Interpersonal Violence, 31(11), 2026–2051. 10.1177/0886260515572475 [DOI] [PubMed] [Google Scholar]
- Cho S, Crenshaw KW, & McCall L (2013). Toward a field of intersectionality studies: Theory, applications, and praxis. Signs: Journal of Women in Culture and Society, 38(4), 785–810. 10.1086/669608 [DOI] [Google Scholar]
- Chu JY, Porche MV, & Tolman DL (2005). The adolescent masculinity ideology in relationships scale: Development and validation of a new measure for boys. Men and Masculinities, 8(1), 93–115. 10.1177/1097184x03257453 [DOI] [Google Scholar]
- Closson K, Dietrich JJ, Beksinska M, Gibbs A, Hornschuh S, & Smith T (2019). Measuring sexual relationship power equity among young women and young men South Africa: Implications for gender-transformative programming. Plos One, 14(9), e0221554. 10.1371/journal.pone.0221554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Closson K, Hatcher A, Sikweyiya Y, Washington L, Mkhwanazi S, & Jewkes R (2020). Gender role conflict and sexual health and relationship practices amongst young men living in urban informal settlements in South Africa. Culture, Health & Sexuality, 22(1), 31–47. 10.1080/13691058.2019.1568578 [DOI] [PubMed] [Google Scholar]
- Clinical Trials Nct. (2020). A feasibility trial of sisterhood 2.0. Clinical Trials Nct. https://ClinicalTrials.gov/show/NCT04388696. [Google Scholar]
- Cui M, Ueno K, Gordon M, & Fincham FD (2013). The continuation of intimate partner violence from adolescence to young adulthood. Journal of Marriage and Family, 75(2), 300–313. 10.1111/jomf.12016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Das M, Ghosh S, Verma R, O’Connor B, Fewer S, & Virata MC (2014). Gender attitudes and violence among urban adolescent boys in India. International Journal of Adolescence and Youth, 19(1), 99–112. 10.1080/02673843.2012.716762 [DOI] [Google Scholar]
- Decker MR, Peitzmeier S, Olumide A, Acharya R, Ojengbede O, & Covarrubias L (2014). Prevalence and health impact of intimate partner violence and non-partner sexual violence among female adolescents aged 15–19 years in vulnerable urban environments: a multi-country study. Journal of Adolescent Health, 55(6), S58–S67. 10.1016/j.jadohealth.2014.08.022 [DOI] [PubMed] [Google Scholar]
- Decker MR, Silverman JG, & Raj A (2005). Dating violence and sexually transmitted disease/HIV testing and diagnosis among adolescent females. Pediatrics, 116(2), e272–e276. 10.1542/peds.2005-0194 [DOI] [PubMed] [Google Scholar]
- Eisman AB, Ngo QM, Kusunoki YY, Bonar EE, Zimmerman MA, & Cunningham RM (2018). Sexual violence victimization among youth presenting to an urban emergency department: The role of violence exposure in predicting risk. Health Education & Behavior, 45(4), 625–634. 10.1177/1090198117741941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Espelage DL, Basile KC, Leemis RW, Hipp TN, & Davis JP (2018). Longitudinal examination of the bullying-sexual violence pathway across early to late adolescence: Implicating homophobic name-calling. Journal of Youth and Adolescence, 47(9), 1880–1893. 10.1007/s10964-018-0827-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Espelage DL, Davis JP, Basile KC, Rostad WL, & Leemis RW (2018). Alcohol, prescription drug misuse, sexual violence, and dating violence among high school youth. Journal of Adolescent Health, 63(5), 601–607. 10.1016/j.jadohealth.2018.05.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eugene JM, Zelazny S, Torres I, Feliz N, Bamwine P, & Jones K (2017). Using community asset mapping and respondent-driven sampling to support recruitment and retention for a community-based sexual violence prevention program. Journal of Adolescent Health, 60(2), S79. 10.1016/j.jadohealth.2016.10.338 [DOI] [Google Scholar]
- Frankel AS, Bass SB, Patterson F, Dai T, & Brown D (2018). Sexting, risk behavior, and mental health in adolescents: An examination of 2015 Pennsylvania Youth Risk Behavior Survey data. Journal of School Health, 88(3), 190–199. 10.1111/josh.12596 [DOI] [PubMed] [Google Scholar]
- Gage EA (2008). Gender attitudes and sexual behaviors: Comparing center and marginal athletes and nonathletes in a collegiate setting. Violence Against Women, 14(9), 1014–1032. 10.1177/1077801208321987 [DOI] [PubMed] [Google Scholar]
- Goodkind S, & Workgroup, B. G. E. A. J. J. (2019). Institutionalized inequity: Pathways to juvenile Justice for Black Girls in Pittsburgh and allegheny county: Gwendolyn J. Elliot Institute at Gwen’s Girls [Google Scholar]
- Haberland NA (2015). The case for addressing gender and power in sexuality and HIV education: A comprehensive review of evaluation studies. Int Perspect Sex Reprod Health, 41(1), 31–42. 10.1363/4103115 [DOI] [PubMed] [Google Scholar]
- Hequembourg AL, Livingston JA, & Wang W (2020). Prospective associations among relationship abuse, sexual harassment and bullying in a community sample of sexual minority and exclusively heterosexual youth. Journal of Adolescence, 83, 52–61. 10.1016/j.adolescence.2020.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill AL, Jones KA, McCauley HL, Tancredi DJ, Silverman JG, & Miller E (2019). Reproductive coercion and relationship abuse among adolescents and young women seeking care at school health centers. Obstetrics and Gynecology, 134(2), 351. 10.1097/AOG.0000000000003374 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill AL, Miller E, Switzer GE, Yu L, Heilman B, & Levtov RG (2020). Harmful masculinities among younger men in three countries: Psychometric study of the Man Box Scale. Preventive Medicine, 139(3), 106185. 10.1016/j.ypmed.2020.106185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- HIll Ashley V., Mistry Sejal, Paglisotti TE, Dwarakanath Namita, Lavage Daniel, Iwuanyanwu Rosemary, Stokes Lynissa, Jones Kelley, & Miller Elizabeth (2022) (In press). Assessing feasibility of an adolescent relationship abuse prevention program for girl. Journal of Adolescence. DOI: 10.1002/jad.12026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holliday CN, McCauley HL, Silverman JG, Ricci E, Decker MR, & Tancredi DJ (2017). Racial/Ethnic differences in women’s experiences of reproductive coercion, intimate partner violence, and unintended pregnancy. Journal of Women’s Health, 26(8), 828–835. 10.1089/jwh.2016.5996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howell J, Goodkind S, Jacobs L, & Miller E (2019). Pittsburgh Inequality across Gender and race: City of pittsburgh gender equity commission. Pittsburgh’: Gender Equity Commission. [Google Scholar]
- Jewkes R, & Morrell R (2010). Gender and sexuality: Emerging perspectives from the heterosexual epidemic in South Africa and implications for HIV risk and prevention. Journal of the International AIDS Society Electronic Resource, 13, 6. 10.1186/1758-2652-13-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson EP (2003). Appropriating blackness: Performance and the politics of authenticity: Duke University Press. [Google Scholar]
- Johnson WL, Giordano PC, Manning WD, & Longmore MA (2015). The age–IPV curve: Changes in the perpetration of intimate partner violence during adolescence and young adulthood. Journal of Youth and Adolescence, 44(3), 708–726. 10.1007/s10964-014-0158-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones CP (2000). Levels of racism: A theoretic framework and a gardener’s tale. American Journal of Public Health, 90(8), 1212. 10.2105/ajph.90.8.1212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones KA, Cornelius MD, Silverman JG, Tancredi DJ, Decker MR, & Haggerty CL (2016). Abusive experiences and young women’s sexual health outcomes: Is condom negotiation self-efficacy a mediator? Perspectives on Sexual and Reproductive Health, 48(2), 57–64. 10.1363/48e8616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, & Queen B (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67(8), 1–114. 10.15585/mmwr.ss6708a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanza ST, & Rhoades BL (2013). Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prevention Science, 14(2), 157–168. 10.1007/s11121-011-0201-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marcell AV, Ford CA, Pleck JH, & Sonenstein FL (2007). Masculine beliefs, parental communication, and male adolescents’ health care use. Pediatrics, 119(4), e966–975. 10.1542/peds.2006-1683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCauley HL, Tancredi DJ, Silverman JG, Decker MR, Austin SB, & McCormick MC (2013). Gender-equitable attitudes, bystander behavior, and recent abuse perpetration against heterosexual dating partners of male high school athletes. American Journal of Public Health, 103(10), 1882–1887. 10.2105/AJPH.2013.301443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKenney SJ, & Bigler RS (2016). Internalized sexualization and its relation to sexualized appearance, body surveillance, and body shame among early adolescent girls. The Journal of Early Adolescence, 36(2), 171–197. 10.1177/0272431614556889 [DOI] [Google Scholar]
- Miller E, Culyba AJ, Paglisotti T, Massof M, Gao Q, & Ports KA (2020). Male adolescents’ gender attitudes and violence: Implications for youth violence prevention. American Journal of Preventive Medicine, 58(3), 396–406. 10.1016/j.amepre.2019.10.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nunnally JC (1978). Psychometric theory. 2d Ed: McGraw-Hill. [Google Scholar]
- Nylund-Gibson K, & Choi AY (2018). Ten frequently asked questions about latent class analysis. Translational Issues in Psychological Science, 4(4), 440. 10.1037/tps0000176 [DOI] [Google Scholar]
- Okeke NL, Mumford EA, & Rothman EF (2019). Adolescent relationship aggression perpetration and victimization in the context of neighborhood gender equality. Violence and gender, 6(2), 131–138. 10.1089/vio.2018.0028 [DOI] [Google Scholar]
- Preiser B, & Assari S (2017). Psychological predictors of sexual intimate partner violence against black and hispanic women. Behav Sci (Basel), 8(1), 3. 10.3390/bs8010003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puigvert L, Gelsthorpe L, Soler-Gallart M, & Flecha R (2019). Girls’ perceptions of boys with violent attitudes and behaviours, and of sexual attraction. Palgrave Communications, 5(1), 1–12. 10.1057/s41599-019-0262-5 [DOI] [Google Scholar]
- Pulerwitz J, & Barker G (2008). Measuring attitudes toward gender norms among young men in Brazil: development and psychometric evaluation of the GEM scale. Men and Masculinities, 10(3), 322–338. 10.1177/1097184x06298778 [DOI] [Google Scholar]
- Reidy DE, Holland KM, Cortina K, Ball B, & Rosenbluth B (2017). Evaluation of the expect respect support group program: A violence prevention strategy for youth exposed to violence. Preventive Medicine, 100, 235–242. 10.1016/j.ypmed.2017.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reyes HLM, Foshee VA, Niolon PH, Reidy DE, & Hall JE (2016). Gender role attitudes and male adolescent dating violence perpetration: Normative beliefs as moderators. Journal of Youth and Adolescence, 45(2), 350–360. 10.1007/s10964-015-0278-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rolleri LA (2013). Gender Norms and Sexual health Behaviors. Cornell University, University of Rochester, and New York State Center for School Safety. 2021 [Google Scholar]
- Rome ES, & Miller E (2020). Intimate partner violence in the adolescent. Pediatr Rev, 41(2), 73–80. 10.1542/pir.2018-0053 [DOI] [PubMed] [Google Scholar]
- Sabri B, & Gielen A (2019). Integrated multicomponent interventions for safety and health risks among Black female survivors of violence: A systematic review. Trauma, Violence, & Abuse, 20(5), 720–731. 10.1177/1524838017730647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senn CY, Eliasziw M, Barata PC, Thurston WE, Newby-Clark IR, & Radtke HL (2015). Efficacy of a sexual assault resistance program for university women. The New England Journal of Medicine, 372(24), 2326–2335. 10.1056/NEJMsa1411131 [DOI] [PubMed] [Google Scholar]
- Sinclair J, Sinclair L, Otieno E, Mulinge M, Kapphahn C, & Golden NH (2013). A self-defense program reduces the incidence of sexual assault in Kenyan adolescent girls. J Adolesc Health, 53(3), 374–380. 10.1016/j.jadohealth.2013.04.008 [DOI] [PubMed] [Google Scholar]
- Singer M, Bulled N, Ostrach B, & Mendenhall E (2017). Syndemics and the biosocial conception of health. Lancet, 389(10072), 941–950. 10.1016/S0140-6736(17)30003-X [DOI] [PubMed] [Google Scholar]
- Singer MC, Erickson PI, Badiane L, Diaz R, Ortiz D, & Abraham T (2006). Syndemics, sex and the city: understanding sexually transmitted diseases in social and cultural context. Social Science & Medicine, 63(8), 2010–2021. 10.1016/j.socscimed.2006.05.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith SG, Zhang X, Basile KC, Merrick MT, Wang J, & Kresnow M. j. (2018). The national intimate partner and sexual violence survey: 2015 data brief–updated release. CDC; [DOI] [PMC free article] [PubMed] [Google Scholar]
- Straus MA (2007). Conflict tactics scales. Encyclopedia of Domestic Violence, 190, 197. 10.1037/t02125-000. [DOI] [Google Scholar]
- Straus MA, & Mickey EL (2012). Reliability, validity, and prevalence of partner violence measured by the conflict tactics scales in male-dominant nations. Aggression and Violent Behavior, 17(5), 463–474. 10.1016/j.avb.2012.06.004 [DOI] [Google Scholar]
- Thulaseedharan JV (2019). Young women’s attitude toward gender-equitable norms on domestic chores and violence domains in Trivandrum. J Educ Health Promot, 8, 23. 10.4103/jehp.jehp_259_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vasilenko SA, Kugler KC, Butera NM, & Lanza ST (2015). Patterns of adolescent sexual behavior predicting young adult sexually transmitted infections: A latent class analysis approach. Archives of Sexual Behavior, 44(3), 705–715. 10.1007/s10508-014-0258-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vu L, Pulerwitz J, Burnett-Zieman B, Banura C, Okal J, & Yam E (2017). Inequitable gender norms from early adolescence to young adulthood in Uganda: Tool validation and differences across age groups. J Adolesc Health, 60(2s2), S15–s21. 10.1016/j.jadohealth.2016.09.027 [DOI] [PubMed] [Google Scholar]
- Weisz AN, & Black BM (2001). Evaluating a sexual assault and dating violence prevention program for urban youths. Social Work Research, 25(2), 89–100. 10.1093/swr/25.2.89 [DOI] [Google Scholar]
- World Health Organization. (2013). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence: World Health Organization. [Google Scholar]