Abstract
Objectives The present study aimed to assess whether preoperative spinopelvic parameters can influence the gain of segmental lordosis after one level of lateral lumbar interbody fusion.
Methods The following radiological parameters were measured in the X-rays: pelvic incidence, lumbar lordosis, pelvic tilt, L4S1 lordosis, index level segmental lordosis, intraoperative index segmental lordosis, pelvic mismatch (IP-LL), distal lordosis proportion, delta segmental lordosis, Pelvic Titlt (PT) > 20, actual sacral slope, and ideal sacral slope, and the correlation of these variables with the gain of segmental lordosis was investigated. Afterwards, an exploratory cluster analysis was performed to identify common characteristics between patients and segmental lordosis gain.
Results The sample of the present study comprised 104 patients, of which 76% presented segmental lordosis gain. The most correlated parameters with the segmental lordosis gain were preoperative segmental lordosis (−0.50) and delta intraoperative lordosis (0.51). Moreover, patients in the high PI groups had a trend to gain more segmental lordosis ( p < 0.05) and a reduced risk of losing segmental lordosis (Odds 6.08).
Conclusion Patients with low-medium PI profiles presented higher odds of loss of segmental lordosis. However, the preoperative spinopelvic parameters alone do not seem to play a significant role in the fate of segmental lordosis gain.
Keywords: lumbar vertebrae, spinal fusion, lordosis, pelvis
Introduction
Most degenerative lumbar diseases present good outcomes after nonsurgical treatments. 1 However, some groups of patients do not perceive such benefits from nonsurgical treatments, therefore requiring surgical intervention. 2
Several techniques can be applied to correct degenerative lumbar disorders, with decompressions, 3 arthrodesis, 4 and arthroplasties 5 being the most utilized approaches.
Among the arthrodesis group, we have lateral lumbar interbody fusion (LLIF), a minimally invasive technique developed by Dr. Luiz Pimenta in the late 2000s apud Ozgur et al., 6 that allows access to the lumbar discs through the psoas major muscle. Lateral lumbar interbody fusion relies on its capacity to promote indirect decompression and on its ability to maintain or correct sagittal parameters when needed, besides having a vast literature regarding its clinical and radiological benefits. 7 However, arthrodesis alone is not enough. If, when performing the fusion technique, the surgeon does not respect the spinopelvic parameters, even for degenerative conditions, he might create a biomechanical disarrangement in the lumbar region that leads to the overload of the discs and facet joints, culminating in the degeneration of adjacent levels and even to reoperations. 8
However, the LLIF technique is often regarded as one of the methods with the greater capability of restoring sagittal lordosis. 9 Recent revisions of the literature show an extensive heterogeneity regarding the capacity of LLIF to reestablish the lumbar lordosis, with authors pointing out significant segmental lordosis gains 10 and other authors presenting small to no gain in some cases 11 Different cage properties and positions might explain some parts of this heterogeneity. 12
However, the impact of preoperative spinopelvic parameters of patients in the gain of segmental lordosis is poorly studied in the literature. Therefore, our study aimed to assess whether preoperative spinopelvic parameters can increase segmental lordosis after one-level LLIF.
Methods
This was a single-center, noncomparative, nonrandomized study approved by the ethics commission (CAAE: 28761220.2.0000.8847). The study aimed to investigate the relationship of some spinopelvic parameters and other radiological measurements with the improvement of index level segmental lordosis in patients that underwent a LLIF procedure. All patients included in the present study have given their free-consent to have their data utilized in the study.
Inclusion Criteria
Patients who underwent LLIF surgery in our service had preoperative and postoperative X-rays and signed a free and informed consent form.
Exclusion Criteria
Patients who received anterior column realignment or have the anterior longitudinal ligament (ALL) unintentionally ruptured. Patients whose X-rays did not allow the correct visualization and measurements of the proposed spinopelvic parameters.
Study Variables
The following radiological parameters were measured in the X-rays: pelvic incidence, lumbar lordosis, pelvic tilt (PT), L4S1 lordosis, index level segmental lordosis, intraoperative index segmental lordosis.
The following continuous variables were considered using the measured parameters: pelvic mismatch (PI-LL), distal lordosis proportion (defined as the percentage of L4S1 in the pelvic incidence), delta segmental lordosis (defined as the difference between the standing X-ray preoperative index level segmental lordosis and the intraoperative index level segmental lordosis). The following categorical variables were derived from the measured parameters: PT > 20°, actual sacral slope (high, medium, or low), and ideal sacral slope (ISS) (high, medium, or low). The ISS was defined by the following operation ISS = (PT – 20) + actual sacral slope (SS), when patients had PT > 20°. In cases of PT < 20°, the ISS is the actual SS. High, medium, and low SSs were defined according to the Roussouly Columns Classification, with values < 35° being considered low, > 45° being considered high, and values between these threshold values being considered medium. 13 14 The 20° threshold for PT is derived from the SRS-Schwab classification. 15
Study Outcomes
The primary goal of the present study was to evaluate the correlation between spinopelvic parameters and the gain of segmental lordosis after one-level LLIF surgery.
The secondary goal of the present study was to assess how these spinopelvic parameters could influence segmental lordosis after one-level LLIF surgery.
Statistical Analysis
The data were measured using Surgimap (Nemaris Inc., Toronto, Canada) software and compiled using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) software, and R software (R Foundation, Vienna, Austria) for the statistical analysis and graphs elaboration. The following non-native packages were also used: ggpubr, ggplot2, tydeverse, cluster, lsr.
For the analysis of the sample distribution, we applied the D'agostino normality test; then, following this analysis, we investigated the correlation of the continuous variables with the gain of segmental lordosis; we used the Pearson and the Spearman correlation methods for normal and nonparametric distributed samples, respectively, and the Cramer V test for correlation among categorical variables. Then, we applied the k-mean cluster method to assign study patients to groups by similarity. To assess the ideal number of clusters, the elbow method was chosen.
We used the T-test or the Wilcoxon Rank Sum Test to compare between groups, depending on the sample distribution for continuous variables, and the chi-squared or the Fisher exact test for discrete variables. When there were more than two groups, we performed the Kruskal-Wallis test for nonparametric distributions and the Dunn Test method for post-hoc comparison between groups. A p-value < 0.05 was rendered as a threshold for statistical significance.
Results
Characteristics of the Study Population
A total of 104 patients were included in the present study, of which 75 (76%) presented segmental lordosis gain. The mean segmental lordosis gain was 2.55° with L4L5 as the index level in 84 (80%) surgeries. The frequency of the other studied variables is shown in Table 1 .
Table 1. Frequency of the studied variables.
| Continuous Variables | Frequency | ||||||
|---|---|---|---|---|---|---|---|
| Min | 1 st quarter | Median | Mean | 3 rd quarter | Max | Standard deviation | |
| Pelvic incidence (°) | 29.40 | 45.45 | 53.20 | 54.22 | 61.15 | 83.90 | 11.96 |
| Lumbar lordosis (°) | 9.30 | 39.17 | 49.90 | 49.17 | 61.15 | 87.00 | 15.98 |
| Lordosis L4S1 (°) | 3.10 | 22.50 | 27.95 | 29.15 | 35.23 | 59.20 | 11.70 |
| Sacral slope (°) | 14.00 | 26.30 | 33.35 | 33.77 | 41.27 | 70.60 | 11.14 |
| Pelvic tilt (°) | 0.20 | 12.57 | 20.20 | 20.22 | 26.73 | 44.90 | 10.35 |
| Preoperative segmental lordosis (°) | −7.00 | 1.90 | 4.55 | 5.19 | 8.40 | 18.50 | 4.32 |
| Intraoperative segmental lordosis (NA = 77) (°) | 0.60 | 3.25 | 5.00 | 5.82 | 8.15 | 11.80 | 3.34 |
| Delta Segmental Lordosis (NA = 77) (°) | −8.40 | −3.75 | −1.40 | −0.02 | 3.40 | 8.80 | 4.71 |
| Segmental lordosis gain (°) | −16.3 | −0.12 | 2.10 | 2.42 | 6.20 | 12.5 | 5.35 |
| Pelvic mismatch (°) | −26.90 | −4.25 | 3.75 | 5.05 | 13.77 | 49.40 | 14.42 |
| Distal lumbar lordosis proportion (%) | 5.53 | 39.18 | 56.33 | 54.97 | 67.68 | 109.95 | 21.28 |
| Categorical variables | Frequency | ||||||
| Pelvic tilt > 20° | yes: 39 | no: 65 | |||||
| Segmental lordosis gain? | yes: 75 | no: 29 | |||||
| Actual sacral slope (high, medium, low) | Low: 57 | Medium: 33 | High: 14 | ||||
| Ideal sacral slope (high, medium, low) | Low: 39 | Medium: 38 | High: 27 | ||||
| Operated levels | T12L1: 1 | L1L2: 1 | L2L3: 5 | L3L4 : 13 | L4L5: 84 | ||
| Cage angulation (NA = 34) |
10: 69 | 12: 1 | |||||
Abbreviation: NA, not available.
(%): Values described as percentages. (°): Value described as cobb degrees.
Correlations among Segmental Lordosis Gain and Studied Parameters
To assess the relationship between the parameters and the gain of segmental lordosis, we performed a correlation analysis. The authors found that the parameters most correlated with segmental lordosis gain were preoperative segmental lordosis (−0.50) and delta intraoperative lordosis (0.51). The full correlation table is shown in Table 2 .
Table 2. Correlation among the studied parameters and the amount of segmental lordosis gain.
| Variables | p-value | Correlation |
|---|---|---|
| Delta segmental lordosis | 0.002 | 0.536 |
| Preoperative segmental lordosis | 0.000 | −0.500 |
| Intraoperative segmental lordosis | 0.046 | −0.382 |
| Pelvic tilt | 0.001 | 0.304 |
| Pelvic incidence | 0.001 | 0.282 |
| Pelvic mismatch | 0.018 | 0.216 |
| Distal lumbar lordosis proportion | 0.049 | −0.163 |
| Sacral slope | 0.486 | 0.052 |
| Distal lumbar lordosis | 0.648 | −0.029 |
| Lumbar lordosis | 0.946 | 0.010 |
The greener the cell, the more positively correlated are the variables; the bluish the cell, the more negatively correlated are the variables.
We also performed the Cramer V test to assess the association of categorical variables with the gain or the absence of segmental lordosis. The ISS presented a medium correlation with segmental lordosis gain ( Table 3 ).
Table 3. Correlation among the studied categorical parameters and the amount of segmental lordosis gain.
| Variable | Correlation |
|---|---|
| Ideal sacral slope | 0.22 |
| Pelvic tilt > 20 | 0.11 |
| Actual sacral slope | 0.06 |
The greener the cell, the more positively correlated are the variables; the bluish the cell, the more negatively correlated are the variables.
Differences between Patients with and without Segmental Lordosis Gain
We present the differences between the groups in Figure 1 . The patients who gained segmental lordosis presented lower preoperative segmental lordosis, higher PI, higher PT, and higher pelvic mismatch. These patients also showed an increase in the index level segmental lordosis when positioned for the surgery (delta segmental lordosis).
Fig. 1.

Boxplots representing differences in preoperative spinopelvic parameters between patients that gained segmental lordosis, and those who lost segmental lordosis. *p < 0.05, ** p < 0.01, ***p < 0.001.
Identifying Patient Clusters
Afterwards, a clustering analysis was performed to identify if patients with similar characteristics could be prone to experience a higher gain of lordosis than other patients. Four clouds were created based on the elbow method ( Figure 2 ). The clusters can be explained as two groups within two subgroups each.
Fig. 2.

Elbow plot to estimate the optimal number of clusters. Vertical Line: Optimal number of clusters.
The first group comprised patients with low-medium PI (47.24 °) and was subdivided into 1 cluster (3) with misaligned patients (PI-LL = −20.63°; PT = 27.24°) and 1 cluster with aligned patients (1) (PI-LL = −6.15°; PT = 11.54°) ( Table 4 ). The second group comprised patients with high PI (65.68°), also divided into 1 group (4) with misaligned parameters (PI-LL = 13.06°; PT = 28.90°) and 1 group (2) with more aligned parameters (PI-LL = 0.73°; PT = 19.62°) ( Table 4 ).
Table 4. Table containing the median values regarding the patient clusters. Blue lines (High PI Cluster) Pink lines (Low-Medium PI Clusters).
| Cluster | PI | Lumbar lordosis | Distal lordosis (L4S1) | Sacral slope | Pelvic tilt | Preoperative segmental lordosis | Segmental lordosis gain | Pelvic mismatch | Distal lumbar lordosis proportion |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 47.59 | 53.75 | 31.99 | 35.48 | 11.54 | 6.99 | 0.26 | −6.15 | 68.93 |
| 2 | 69.20 | 68.47 | 48.04 | 49.58 | 19.62 | 5.94 | 4.00 | 0.73 | 70.14 |
| 3 | 46.91 | 26.28 | 15.23 | 19.67 | 27.24 | 4.49 | 1.77 | 20.63 | 33.73 |
| 4 | 62.17 | 49.10 | 24.89 | 33.26 | 28.90 | 2.43 | 5.52 | 13.06 | 40.83 |
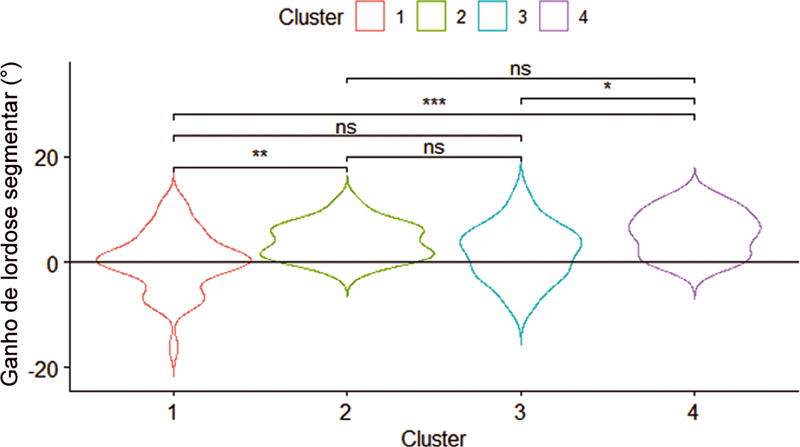
When comparing the segmental lordosis gain between the clusters, we could see that cluster 3 presented significantly more gain than the other clusters, except cluster 1 in the post-hoc analysis ( p < 0.05) ( Figure 3 ).
Fig. 3.

Violin-plot showing the segmental lordosis correction between the clusters. *p < 0.05, ** p < 0.01, ***p < 0.001.
A chi-squared test to assess the loss of segmental lordosis showed that patients in different clusters had different risks of losing segmental lordosis after the LLIF procedure ( p = 0.02). To investigate further, the clusters were aggregated into medium-low PI clusters (1 and 3) and high PI clusters (2 and 4), showing that patients in the low-medium PI clusters are more prone to present loss of segmental lordosis with an odds ratio (OR) of 6.08 (95% confidence interval [CI] = 4.93–7.23).
Discussion
The literature argues that LLIF is a reliable approach to correct lumbar spinal degenerative conditions. 16 However, some recently published works demonstrated a high heterogeneity of segmental lordosis capacity in this technique. 10
Parameters Associated with Segmental Lordosis Gain
Cage Conformity
Several studies have tried to identify possible parameters that could impact the correction of segmental lordosis. Sembrano et al. showed that cages with angulation (lordotic cages) provided better segmental lordosis correction than nonlordotic cages. 17 On the other hand, a biomechanical study conducted by Gambhir et al. 18 found that when treating L3-L4, the key factor influencing the gain of segmental lordosis was the cage height, mainly the posterior cage height, and that cages with 0° provided better angular correction than lordotic cages.
Cage Position
Moreover, some other studies showed that the cage position might play a critical role in the final segmental lordosis. Park et al. 12 showed that a cage within the anterior third of the vertebral body was the best position to restore segmental lordosis while not losing indirect decompression potential. Similarly, Kepler et al., 19 showed that placement of the cage in a more anterior position resulted in a mean 7.4° gain, while a more posterior position led to a 1.2° decrease (kyphotic effect) in segmental lordosis gain . Otsuki et al. 20 also analyzed the cage position and its impacts on segmental lordosis correction.
Functional Spinal Unit Mobility
Another important parameter to be considered in the gain of segmental lordosis is the mobility of the operating level. Two common ways to improve the mobility of a spinal level are posterior osteotomies (facetectomies or Smith Petersen) or releasing the anterior longitudinal ligament. 21 Although not related to a technical maneuver to increase mobility, our study also found indications that functional spinal unit (FSU) mobility may play a significant role in the gain of segmental lordosis, as patients with higher (positive) delta segmental lordosis presented increased amounts of segmental lordosis gain ( p < 0.05).
Segmental Lordosis and Spinopelvic Parameters
Other studies also pointed out that one key factor for estimating the amount of gain of segmental lordosis is the preoperative segmental lordosis. In a systematic review published by Uribe et al., 22 the authors showed that the preoperative segmental lordosis was inversely associated with the increase of segmental lordosis after the procedure. Similarly, our study showed that preoperative segmental lordosis had a −0.50 correlation with segmental lordosis gain. Also, patients presenting an increase in segmental lordosis had significantly lower preoperative segmental lordosis ( p < 0.001).
Our work also showed that patients who gained segmental lordosis had higher PI, PT, and PI-LL values ( p < 0.01; p < 0.05; and p < 0.05, respectively). Moreover, the present study showed that patients in the high PI values cluster (> 60°) not only gained more lordosis but were also less likely to experience loss of segmental lordosis ( Figure 3 and Table 4 ). Another interesting factor in our study was that the ISS had a medium to strong correlation with the gain of segmental lordosis, corroborating the results that the PI value might play a role in segmental lordosis correction.
However, the authors could not find any literature directly correlating these spinopelvic parameters with segmental lordosis gain. Therefore, based on other studies showing the effect of spinal parameters in the biomechanics of the spine, the authors hypothesize the possible impacts of spinopelvic parameters on segmental lordosis correction. As demonstrated by the literature, patients with high PI and SS (type 4) have hyperextended lumbar morphology. 23 24 Moreover, Roussouly et al = , 25 hypothesized that due to its more angulated conformity, type 4 Roussouly columns might possess smaller posterior vertebral elements when compared with type 2 Roussouly columns, which could make this type of patient more capable of posterior extension. A recently published study reported that asymptomatic patients with type 4 Roussouly columns had significantly larger intradiscal lordosis than patients with type 1 in L5-S1 and that Type 4 patients also had more significant intradiscal lordosis than Type 2 patients in L4-L5 and L2-L3. 26 For that, the authors think that it might be fair to speculate that due to the higher amount of "biomechanical resources" that patients with high PI might recruit, this group of patients can mitigate some of the impacts of both preoperative segmental lordosis and positional/conformational aspects of the cage to accommodate the FSU and avoid the loss of segmental lordosis.
The limitations of the present study include its retrospective design and the fact that only the spinopelvic parameters were analyzed, not including in the work other important factors such as cage position, cage angulation, and vertebral body angulation and shape. Another limitation of our study is that the L4L5 level counted for more than half of the included patients, impacting the generalizability our findings to other spine levels. Finally, the last limitation is a philosophical one: the amount of correction is achieved because of the spinopelvic parameters independent from the surgeon or is it an effect achieved by the previous knowledge of the sagittal parameters of the patient? This is a question that might be answered in the future by matching patients with different column types or PI values and similar cage conformities and positions.
Conclusion
Our work shows that surgeons might use the studied spinopelvic parameters to plan their surgical options goals when performing one-level LLIF, mainly in patients with low PI profile, because they presented higher odds of loss of segmental lordosis. The index level of the segmental lordosis might also play a role in increasing or not segmental lordosis after surgery.
However, the preoperative spinopelvic parameters do not seem to play a critical role in the fate of segmental lordosis gain but act more as coadjutants in a complex set of factors, as most of the parameters showed a moderate to weak correlation with segmental lordosis gain.
Conflito de Interesses Os autores não têm conflito de interesses para declarar.
Suporte Financeiro
O presente estudo não recebeu nenhum apoio financeiro de fontes públicas, comerciais ou sem fins lucrativos.
Financial Support
The present study received no financial support from public, commercial, or not-for-profit sources.
Estudo desenvolvido no Instituto de Patologia da Coluna (IPC), São Paulo, SP, Brasil.
Study developed at the Instituto de Patologia da Coluna (IPC), São Paulo, SP, Brazil.
Referências
- 1.Lurie J D, Tosteson T D, Tosteson A. Long-term outcomes of lumbar spinal stenosis: eight-year results of the Spine Patient Outcomes Research Trial (SPORT) Spine (Phila Pa 1976) 2015;40(02):63–76. doi: 10.1097/BRS.0000000000000731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Moulton H, Tosteson T D, Zhao W. Considering Spine Surgery: A Web-Based Calculator for Communicating Estimates of Personalized Treatment Outcomes. Spine (Phila Pa 1976) 2018;43(24):1731–1738. doi: 10.1097/BRS.0000000000002723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Joaquim A F, Milano J B, Ghizoni E, Patel A A. Is There a Role for Decompression Alone for Treating Symptomatic Degenerative Lumbar Spondylolisthesis?: A Systematic Review. Clin Spine Surg. 2016;29(05):191–202. doi: 10.1097/BSD.0000000000000357. [DOI] [PubMed] [Google Scholar]
- 4.Yavin D, Casha S, Wiebe S. Lumbar Fusion for Degenerative Disease: A Systematic Review and Meta-Analysis. Neurosurgery. 2017;80(05):701–715. doi: 10.1093/neuros/nyw162. [DOI] [PubMed] [Google Scholar]
- 5.Abi-Hanna D, Kerferd J, Phan K, Rao P, Mobbs R. Lumbar Disk Arthroplasty for Degenerative Disk Disease: Literature Review. World Neurosurg. 2018;109:188–196. doi: 10.1016/j.wneu.2017.09.153. [DOI] [PubMed] [Google Scholar]
- 6.Ozgur B M, Aryan H E, Pimenta L, Taylor W R. Extreme Lateral Interbody Fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006;6(04):435–443. doi: 10.1016/j.spinee.2005.08.012. [DOI] [PubMed] [Google Scholar]
- 7.Oliveira L, Marchi L, Coutinho E, Pimenta L.A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements Spine (Phila Pa 1976) 201035(26, Suppl)S331–S337. [DOI] [PubMed] [Google Scholar]
- 8.Tempel Z J, Gandhoke G S, Bolinger B D. The Influence of Pelvic Incidence and Lumbar Lordosis Mismatch on Development of Symptomatic Adjacent Level Disease Following Single-Level Transforaminal Lumbar Interbody Fusion. Neurosurgery. 2017;80(06):880–886. doi: 10.1093/neuros/nyw073. [DOI] [PubMed] [Google Scholar]
- 9.Sembrano J N, Yson S C, Horazdovsky R D, Santos E R, Polly D W., Jr Radiographic Comparison of Lateral Lumbar Interbody Fusion Versus Traditional Fusion Approaches: Analysis of Sagittal Contour Change. Int J Spine Surg. 2015;9:16. doi: 10.14444/2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ahlquist S, Park H Y, Gatto J, Shamie A N, Park D Y. Does approach matter? A comparative radiographic analysis of spinopelvic parameters in single-level lumbar fusion. Spine J. 2018;18(11):1999–2008. doi: 10.1016/j.spinee.2018.03.014. [DOI] [PubMed] [Google Scholar]
- 11.Rothrock R J, McNeill I T, Yaeger K, Oermann E K, Cho S K, Caridi J M. Lumbar Lordosis Correction with Interbody Fusion: Systematic Literature Review and Analysis. World Neurosurg. 2018;118:21–31. doi: 10.1016/j.wneu.2018.06.216. [DOI] [PubMed] [Google Scholar]
- 12.Park S J, Lee C S, Chung S S, Kang S S, Park H J, Kim S H. The Ideal Cage Position for Achieving Both Indirect Neural Decompression and Segmental Angle Restoration in Lateral Lumbar Interbody Fusion (LLIF) Clin Spine Surg. 2017;30(06):E784–E790. doi: 10.1097/BSD.0000000000000406. [DOI] [PubMed] [Google Scholar]
- 13.Roussouly P, Pinheiro-Franco J L.Biomechanical analysis of the spino-pelvic organization and adaptation in pathology Eur Spine J 201120(5, Suppl 5)609–618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Roussouly P, Berthonnaud E, Dimnet J. [Geometrical and mechanical analysis of lumbar lordosis in an asymptomatic population: proposed classification] Rev Chir Orthop Repar Appar Mot. 2003;89(07):632–639. [PubMed] [Google Scholar]
- 15.International Spine Study Group . Terran J, Schwab F, Shaffrey C I. The SRS-Schwab adult spinal deformity classification: assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery. 2013;73(04):559–568. doi: 10.1227/NEU.0000000000000012. [DOI] [PubMed] [Google Scholar]
- 16.Malham G M, Parker R M, Goss B, Blecher C M. Clinical results and limitations of indirect decompression in spinal stenosis with laterally implanted interbody cages: results from a prospective cohort study. Eur Spine J. 2015;24 03:339–345. doi: 10.1007/s00586-015-3807-3. [DOI] [PubMed] [Google Scholar]
- 17.Sembrano J N, Horazdovsky R D, Sharma A K, Yson S C, Santos E RG, Polly D W., Jr Do Lordotic Cages Provide Better Segmental Lordosis Versus Nonlordotic Cages in Lateral Lumbar Interbody Fusion (LLIF)? Clin Spine Surg. 2017;30(04):E338–E343. doi: 10.1097/BSD.0000000000000114. [DOI] [PubMed] [Google Scholar]
- 18.Gambhir S, Wang T, Pelletier M H, Walsh W R, Ball J R. How Does Cage Lordosis Influence Postoperative Segmental Lordosis in Lumbar Interbody Fusion. World Neurosurg. 2019;126:e606–e611. doi: 10.1016/j.wneu.2019.02.100. [DOI] [PubMed] [Google Scholar]
- 19.Kepler C K, Huang R C, Sharma A K. Factors influencing segmental lumbar lordosis after lateral transpsoas interbody fusion. Orthop Surg. 2012;4(02):71–75. doi: 10.1111/j.1757-7861.2012.00175.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Otsuki B, Fujibayashi S, Takemoto M. Analysis of the Factors Affecting Lumbar Segmental Lordosis After Lateral Lumbar Interbody Fusion. Spine. 2020;45(14):E839–E846. doi: 10.1097/BRS.0000000000003432. [DOI] [PubMed] [Google Scholar]
- 21.Nakashima H, Kanemura T, Satake K. Factors Affecting Postoperative Sagittal Alignment after Lateral Lumbar Interbody Fusion in Adult Spinal Deformity: Posterior Osteotomy, Anterior Longitudinal Ligament Rupture, and Endplate Injury. Asian Spine J. 2019;13(05):738–745. doi: 10.31616/asj.2018.0275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Uribe J S, Myhre S L, Youssef J A. Preservation or Restoration of Segmental and Regional Spinal Lordosis Using Minimally Invasive Interbody Fusion Techniques in Degenerative Lumbar Conditions: A Literature Review. Spine (Phila Pa 1976) 2016;41 08:S50–S58. doi: 10.1097/BRS.0000000000001470. [DOI] [PubMed] [Google Scholar]
- 23.Barrey C, Jund J, Noseda O, Roussouly P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur Spine J. 2007;16(09):1459–1467. doi: 10.1007/s00586-006-0294-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005;18(01):40–47. doi: 10.1097/01.bsd.0000117542.88865.77. [DOI] [PubMed] [Google Scholar]
- 25.Roussouly P, Pinheiro-Franco J L.Sagittal parameters of the spine: biomechanical approach Eur Spine J 201120(5, Suppl 5)578–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chung N S, Lee H D, Jeon C H. Differences in lumbar segment angle among Roussouly types of global sagittal alignment in asymptomatic adult subjects. Spine Deform. 2020;8(02):227–232. doi: 10.1007/s43390-019-00010-6. [DOI] [PubMed] [Google Scholar]