

Abstract
Background
Practices of Do-Not-Resuscitate (DNR) orders show discrepancies worldwide, but there are only few such studies from Saudi Arabia.
Objective:
To describe the practice of DNR orders in a Saudi Arabian tertiary care ICU.
Methods:
This retrospective study included all patients who died with a DNR order at the ICU of King Saud Medical City, Riyadh, Saudi Arabia, between January 1 to December 31, 2021. The percentage of early DNR (i.e., ≤48 hours of ICU admission) and late DNR (>48 hours) orders were determined and the variables between the two groups were compared. The determinants of late DNR were also investigated.
Results:
A total of 723 cases met the inclusion criteria, representing 14.9% of all ICU discharges and 63% of all ICU deaths during the study period. The late DNR group comprised the majority of the cases (78.3%), and included significantly more patients with acute respiratory distress syndrome (ARDS), community acquired pneumonia (CAP), acute kidney injury, and COVID-19, and significantly fewer cases of readmissions and malignancies. Septic shock lowered the odds of a late DNR (OR = 0.4, 95% CI: 0.2–0.9;P= 0.02), while ARDS (OR = 3.3, 95% CI: 2–5.4;P < 0.001), ischemic stroke (OR = 2.5, 95% CI: 1.1–5.4;P= 0.02), and CAP (OR = 2, 95% CI: 1.3–3.1;P= 0.003) increased the odds of a late DNR.
Conclusion:
There was a higher frequency of late DNR orders in our study compared to those reported in several studies worldwide. Cases with potential for a favorable outcome were more likely to have a late DNR order, while those with expected poorer outcomes were more likely to have an early DNR order. The discrepancies highlight the need for clearer guidelines to achieve consistency.
Keywords: Do-not-resuscitate, frequency, intensive care unit, resuscitation orders, Saudi Arabia, timing
INTRODUCTION
The intensive care unit (ICU) requires intensivists to care for critically ill patients needing multiple life-sustaining interventions and management decisions within a constrained timeframe.[1,2] Often, intensivists find themselves facing the critical decision to issue a Do-Not-Resuscitate (DNR) order, in view of the medical condition of a patient and the futility of resuscitation attempts.[3] Several guidelines and recommendations with regards to DNR are available;[4,5] however, they mostly focus on the ethical and communication (with patients and/or families) aspects of the decision. In Saudi Arabia, consent of the patient's family is not required to issue a DNR order and physicians have varying degrees of comfort in discussing this with families.[6,7] Guidelines are usually deficient or vague with regards to the practical components of making the decision such as the timing and the objective criteria in addition to them being outdated.
Consequently, heterogeneity in DNR practices is a recurrent finding in studies, with it existing between countries, healthcare institutes within a country, and even between physicians in the same ICU.[8,9,10] Numerous factors impact DNR practice, including work-related factors, such as the workload, physician-related factors, such as cultural norms and religious beliefs, and patient-related factors, such as age and severity of illness.[2,3,10,11]
In view of the discrepancies in DNR practices worldwide and the lack of such studies from Saudi Arabia, the current study was conducted with the aim of determining the timing of DNR orders (i.e., within or after 48 hours of ICU admission) and factors influencing late DNR orders at an ICU of a tertiary care hospital in Saudi Arabia. We hypothesized that in our ICU, DNR orders would more frequently be late (i.e., >48 hours after ICU admission).[12]
METHODS
Study design, setting, and participants
This retrospective study included all patients who died with a DNR order at the ICU of King Saud Medical City (KSMC), Riyadh, Saudi Arabia, between January 1 to December 31, 2021. The study's timeframe was chosen to include COVID-19 patients, as its diagnosis may be associated with the timing of the DNR order. The study was approved by the Institutional Review Board (IRB) of KSMC.
KSMC is a tertiary care hospital with a 1200 inpatient bed capacity and a 127-bed ICU capacity. The ICU is a closed unit run by intensivists round the clock, the nurse to patient ratio is 1:1, and the beds are equipped with facilities for invasive and noninvasive monitoring and ventilation.
Inclusion/exclusion criteria
Data was retrieved from the electronic database of the ICU. The study excluded all patients who were discharged from the ICU alive (with or without DNR order, or a reversed DNR order) as well as those who died without an official documentation of DNR. Therefore, only patients who died in the ICU with a documented DNR order were enrolled in the analysis. DNR orders in our institute fall into the following four categories: No cardiopulmonary resuscitation but with full support, withhold, withdraw, or limited escalation.
Variables
The dates of admission to the ICU, issuance of the DNR order, and death were recorded. In addition, we also recorded demographic variables (age and gender), and clinical characteristics including diagnosis, predicted mortality rate upon ICU admission (PMR) produced during calculation of Acute Physiology and Chronic Health Evaluation IV (APACHE IV) score, whether the patient was readmitted to ICU, and cardiopulmonary resuscitation (CPR) episode during the same ICU admission. Seven co-authors commenced data acquisition; inter-rater evaluation was not required given the objectivity of the recorded variables. No missing data were encountered because the recording of all the studied variables is mandatory for every ICU admission at our hospital.
Outcomes
The primary outcome of the study was to assess the percentage of late DNR orders (defined as DNR order >48 hours after ICU admission) as compared to early DNR orders (≤48 hours of ICU admission). The secondary outcomes of the study were determining the mean duration in days between ICU admission and the DNR order, mean duration between the DNR order and death, the different diagnostic categories, PMR, age, and gender. The secondary outcomes are presented for the cohort and as a comparison between patients with early and late DNRs. Lastly, the study also determined the predictors of late DNR.
Statistical analysis
Continuous variables were presented as mean and standard deviation (SD) as well as median and interquartile range (IQR), while discrete variables were presented as frequency and percentage. Group comparisons of continuous data was performed using Student's t-test or Wilcoxon Rank Sum test based on normality or otherwise distribution of the data, and of discrete variables using chi square test if ≤20% of expected cell counts is >5, otherwise using Fisher's exact test.
The predictors of late DNR (versus early) were explored in a multivariable logistic regression model and the results are presented as odds ratio (OR), using the backward elimination method, with variables being retained in the model if P < 0.1. The goodness-of-fit of the model was evaluated by the Hosmer–Lemeshow test, in addition to exploration of the assumptions of logistic regression. All statistical tests were two tailed, and P < 0.05 was considered statistically significant, without correction for multiple testing. STATA ® version 16 (StataCorp. 2019; College Station, TX: StataCorp LLC.) was used to perform all analyses and produce graphs.
RESULTS
There were 4845 discharges from the ICU during the study period, of which 4122 patients were excluded (3680 were discharged alive, 17 were discharged alive with DNR order, and 425 died without DNR order). Therefore, the study included the 723 patients who died with a DNR order [Figure 1]. There was a significant difference in the number of patients with early and late DNR orders (early DNR = 157 [21.7%]; late DNR: 566 [78.3%]; 95% CI: 52.1–60.8%, P < 0.001).
Figure 1.
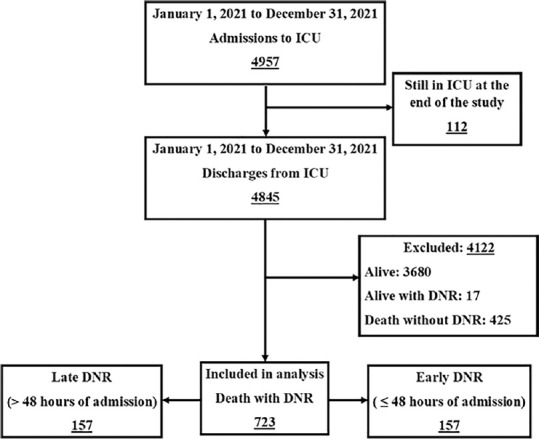
Patients' enrollment diagram
Description of the cohort
The included cohort represented 14.9% of all ICU discharges and 63% of all ICU deaths at our hospital. The majority of the patients were male (478; 66.1%), the mean age was 57.6 ± 18.5 years, the mean PMR was 26.1 ± 18.2, and 94 patients (13%) were readmitted to the ICU. The mean duration between ICU admission and DNR order was 12.7 ± 13.4 days, and the mean duration between DNR order and death was 4.1 ± 6.1 days. The most common diagnostic category in the cohort was ischemic stroke (488; 67.5%), followed by septic shock (426; 58.9%) and acute respiratory distress syndrome (ARDS) (284; 39.3%); one patient had multiple diagnoses [Table 1].
Table 1.
Cohort description and groups' comparison
| Variables | All cohort (n=723) | Early DNR (n=157) | Late DNR (n=566) | P (95% Cl of difference) |
|---|---|---|---|---|
| Males, n (%) | 478 (66.1) | 96 (61.1) | 382 (67.5) | 0.2 (−2.3–15.4) |
| Age (years) | ||||
| Mean±SD | 57.6±18.5 | 57±20.4 | 57.8±18 | 0.4* (−4.1–2.4) |
| Median (IQR) | 58 (47–71) | 56 (44–72) | 58 (47–70) | |
| PMR | ||||
| Mean±SD | 26.1±18.2 | 24.1±16.9 | 26.7±18.5 | 0.1* (−5.9–0.6) |
| Median (IQR) | 22.9 (11.5–37.6) | 20.5 (11–35.8) | 24.3 (11.8–52.4) | |
| Readmission, n (%) | 94 (13) | 29 (18.5) | 65 (11.5) | 0.03 (0.6–14.4) |
| ICU admission to DNR (days) | ||||
| Mean±SD | 12.7±13.4 | 0.6±2.1 | 16±13.3 | <0.001* (−17.5–−13.3) |
| Median (IQR) | 9 (3–18) | 1 (0–2) | 12 (7–21) | |
| DNR to death (days) | ||||
| Mean±SD | 4.1±6.1 | 4.8±6.7 | 3.9±5.9 | 0.06* (−0.2–2) |
| Median (IQR) | 2 (1–5) | 2 (1–7) | 2 (0–5) | |
| Diagnostic categories$, n (%) | ||||
| Ischemic stroke | 488 (67.5) | 95 (60.5) | 393 (69.4) | 0.04 (0.2–17.8) |
| Septic shock | 426 (58.9) | 86 (54.8) | 340 (60.1) | 0.3 (−3.7–14.4) |
| ARDS | 284 (39.3) | 27 (17.2) | 257 (45.4) | <0.001 (20.2–35.2) |
| CAP | 274 (37.9) | 32 (20.4) | 242 (42.8) | <0.001 (14.1–29.7) |
| AKI | 255 (35.3) | 42 (26.8) | 213 (37.6) | 0.02 (2.2–18.7) |
| COVID-19 | 250 (34.6) | 26 (16.6) | 224 (39.6) | <0.001 (15.1–29.9) |
| MOF | 148 (20.5) | 36 (22.9) | 112 (19.8) | 0.5 (−4.1–11.1) |
| Post-CPR | 113 (15.6) | 30 (19.1) | 83 (14.7) | 0.2 (−2.2–12) |
| Cranial bleeding | 82 (11.3) | 23 (14.6) | 59 (10.4) | 0.2 (−1.6–11.1) |
| Pulmonary embolism | 73 (10.1) | 16 (10.2) | 57 (10.1) | 0.9 (−5–6.4) |
| Brain death | 71 (9.8) | 16 (10.2) | 55 (9.7) | 0.9 (−4.6–6.8) |
| Malignancy | 50 (6.9) | 19 (12.1) | 31 (5.5) | 0.007 (1.5–13) |
| End-stage renal disease | 48 (6.6) | 12 (7.6) | 36 (6.4) | 0.7 (−3.1–6.8) |
*Wilcoxon rank sum test, $One patient had multiple diagnoses. All discrete data comparisons by Chi-square test. SD – Standard deviation; IQR – Interquartile range; CI – Confidence interval; DNR – Do not resuscitate; ARDS – Acute respiratory distress syndrome; AKI – Acute kidney injury; MOF – Multi-organ failure; CPR – Cardiopulmonary resuscitation; CAP – Community acquired pneumonia; ICU: Intensive care unit; PMR –Predicted Mortality Rate
Comparison of variables between early and late do-not-resuscitate groups
There were no differences between the early and late DNR groups in terms of age, gender distribution, and PMR. However, the cases of ICU readmissions and malignancies were higher in the early DNR group than in the late DNR group (ICU readmissions: 18.5% vs. 11.5%, respectively, P = 0.03; malignancies: 12.1% vs. 5.5%, respectively, P = 0.007). Obviously, the early DNR group had significantly shorter duration between admission and the DNR order compared to the late DNR group (0.6 ± 2.1 vs. 16 ± 13.3 days, 95% CI: −17.5 to − 13.3], P < 0.001); however, there was no significant difference between both groups in the duration between DNR order and death (early DNR: 4.1 ± 6.1 days; late DNR: 3.9 ± 5.9 days; 95% CI: −0.2 to 2], P = 0.06) [Table 1].
The late DNR group included significantly more patients with the diagnoses of ischemic stroke, ARDS, community acquired pneumonia (CAP), acute kidney injury (AKI), and COVID-19 infections. Both groups were comparable with regards to the diagnoses of septic shock, multi-organ failure, post-cardiopulmonary resuscitation (post-CPR), cranial bleeding, pulmonary embolism (PE), brain death, and end stage renal disease (ESRD) [Table 1] [Figure 2].
Figure 2.

Percentage of diagnoses in late and early DNR groups: ARDS – Acute respiratory distress syndrome; CAP – Community acquired pneumonia; AKI – Acute kidney injury; MOF – Multi-organ failure; CPR – Cardiopulmonary resuscitation; PE – Pulmonary embolism; ESRD – End stage renal disease
In the multivariable logistic regression, the following four variables were significantly associated with late DNR: septic shock (OR = 0.4 [95% CI: 0.2–0.9], P = 0.02), ARDS (OR = 3.3 [95% CI: 2–5.4], P < 0.001), ischemic stroke (OR = 2.5 [95% CI: 1.1–5.4], P = 0.02), and CAP (OR = 2 [95% CI: 1.3–3.1], P = 0.003). Two additional variables (i.e., readmission and malignancy) were retained in the model with P < 0.1. [Table 2].
Table 2.
Multivariable logistic regression prediction model of late do-not-resuscitate orders
| Variable | OR (95% CI) | P |
|---|---|---|
| Septic shock | 0.4 (0.2–0.9) | 0.02 |
| ARDS | 3.3 (2–5.4) | <0.001 |
| Ischemic stroke | 2.5 (1.1–5.4) | 0.02 |
| CAP | 2 (1.3–3.1) | 0.003 |
| Readmission | 0.6 (0.4–1.03) | 0.07 |
| Malignancy | 0.6 (0.3–1.03) | 0.06 |
Pseudo R2=0.09; Hosmer–Lemeshow P=0.6 (model well fitted if P>0.05); Mean VIF=1.88 (no variables had VIF>4); Model correctly classified 78.3% of cases; AUC=70.2%. OR – Odds ratio; ARDS – Acute respiratory distress syndrome; CAP – Community acquired pneumonia; CI – Confidence interval; AUC – Area under the curve; VIF – Variable Inflation Factor
DISCUSSION
Patients who died with a DNR order in the ICU of our hospital accounted for about 15% of all ICU discharges and two-thirds of ICU deaths. In addition, about four-fifths of the DNR orders in this study were late. The late DNR group differed from the early DNR group primarily in terms of having fewer cases that were readmissions and with malignancies, but more cases of ischemic stroke, ARDS, CAP, AKI, and COVID-19. These results are supported by the logistic regression model that showed ORs of ARDS, ischemic stroke, and CAP increased the odds of a late DNR order by 230%, 150%, and 100%, respectively; odds of late DNR decreased by 60% with septic shock.
DNR orders are being practiced in ICUs worldwide for decades now, yet, substantial differences in practices either indicate a failure to serve the intended purposes (i.e., to protect patients' autonomy and avoid futile interventions)[13] or are reflective of regional differences in factors such as practice patterns, expectations, resources, culture, and law. Comparison of our results with those of others support the existence of such differences.
In our study, the DNR rate was about 15% of all discharges, while it ranged from 6.4% to 9% in other reports.[2,3,5] Zingmond et al.[14] demonstrated a DNR rate accounting for up to 15% of all ICU discharges in hospitals with ≥300 beds. Therefore, the higher DNR rate in a tertiary care hospital such as KSMC is expected given the criticality and complexity of cases admitted to our ICU. Similarly, while the proportion of patients with a DNR order accounting for 63% of all ICU deaths at our hospital is higher compared to that reported in another study (40%),[3] a study with a large sample size reported 91.3% of all deaths in the ICU had a DNR order.[15] In terms of the frequency of cases with a late DNR, the study by Ouyang et al.[16] reported only about 54% of cases having a late DNR order; however, this findings should be taken in context of the study having a relatively smaller sample size compared to the current study. Overall, the discrepancies in the findings of the current study and those in the literature reflect differences in patients in terms of diagnoses and conditions, physicians, and cultural factors. Therefore, standardizing and making the DNR decision more objective would help avoid such discrepancies and clarify its process.
The results of the regression model point out that physicians may postpone DNR orders when the diagnosis could be treatable such as ARDS or CAP, particularly in an advanced center like our hospital, where we have the supportive facilities up to extra-corporeal membrane oxygenation, and a high number of physicians with long-term experience particularly in mechanical ventilation. DNR order may also be late when the diagnosis is not commonly associated with rapid mortality, such as ischemic strokes, where the usual outcome may be survival despite the presence of permanent disability.[17] On the other hand, DNR orders are issued early when a patient has low probability of survival, such as in cases of septic shock, which are associated with high mortality and failure of CPR.[18] Similarly, malignancies and ICU readmission appear to be indicators of futility of management in the current study given that these resulted in early DNR orders, which may be because both these factors are linked with poor outcomes.[19,20] However, it should be noted that in the multivariate analysis, both of these variables were not statistically significant.
Limitations
This study has a few limitations. First, it has the inherent limitations of a retrospective descriptive study. Second, the relatively modest sample size renders the inferences based on statistical tests inconclusive. Third, it was beyond the scope of the study to explore physician-related factors, such as cultural or religious beliefs, that may influence the decision to issue a DNR order, particularly in a mostly Muslim community. Fourth, a cost-effective analysis of the timing of DNR order may have demonstrated the burden late DNR imposes on healthcare systems, but the data were not available for such analysis. Finally, the inclusion of COVID-19 patients in the analysis may have biased the results.
CONCLUSION
The DNR practices in our ICU differ from those reported worldwide, resulting in a higher frequency of late DNR orders, especially in cases that have the potential for a favorable outcome; early DNR orders were more often with those expected to have poorer outcomes. The discrepancy in findings highlight the need for more recent and clearer guidelines to provide standardization of DNR practices and decision-making.
Ethical considerations
This study was approved by the IRB of King Saud Medical City, Riyadh, Saudi Arabia (Ref no. H1RI-08-Mar22-02; date: March 14, 2022), with requirement for consent being waived owing to the study design. This study followed the general principles of the Declaration of Helsinki, 2013.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Peer review
This article was peer-reviewed by two independent and anonymous reviewers.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank the Mrs. Rehab Al Fenaikh and Mrs. Ika Fibriantini Mualim, ICU Database Unit, King Saud Medical City.
REFERENCES
- 1.Flannery L, Ramjan LM, Peters K. End-of-life decisions in the Intensive Care Unit (ICU) – Exploring the experiences of ICU nurses and doctors – A critical literature review. Aust Crit Care. 2016;29:97–103. doi: 10.1016/j.aucc.2015.07.004. [DOI] [PubMed] [Google Scholar]
- 2.Lin KH, Huang SC, Wang CH, Chau-Chung, Chu TS, Chen YY. Physician workload associated with do-not-resuscitate decision-making in Intensive Care Units: An observational study using Cox proportional hazards analysis. BMC Med Ethics. 2019;20:15. doi: 10.1186/s12910-019-0355-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Monteiro NF, Simões I, Gaspar I, Carmo E. Do-not-resuscitate and treatment limitation decisions – Six years of experience from a Portuguese general Intensive Care Unit. Rev Assoc Med Bras (1992) 2019;65:1168–73. doi: 10.1590/1806-9282.65.9.1168. [DOI] [PubMed] [Google Scholar]
- 4.American Thoracic Society. Withholding and withdrawing life-sustaining therapy. Ann Intern Med. 1991;115:478–85. doi: 10.7326/0003-4819-115-6-478. [DOI] [PubMed] [Google Scholar]
- 5.Guidelines for the appropriate use of do-not-resuscitate orders. Council on Ethical and Judicial Affairs, American Medical Association. JAMA. 1991;265:1868–71. [PubMed] [Google Scholar]
- 6.Madadin M, Alsaffar GM, AlEssa SM, Khan A, Badghaish DA, Algarni SM, et al. Clinicians' attitudes towards do-not-resuscitate directives in a teaching hospital in Saudi Arabia. Cureus. 2019;11:e6510. doi: 10.7759/cureus.6510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gouda A, Al-Jabbary A, Fong L. Compliance with DNR policy in a tertiary care center in Saudi Arabia. Intensive Care Med. 2010;36:2149–53. doi: 10.1007/s00134-010-1985-3. [DOI] [PubMed] [Google Scholar]
- 8.Walkey AJ, Weinberg J, Wiener RS, Cooke CR, Lindenauer PK. Hospital variation in utilization of life-sustaining treatments among patients with do not resuscitate orders. Health Serv Res. 2018;53:1644–61. doi: 10.1111/1475-6773.12651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chang JC, Yang C, Lai LL, Chen YJ, Huang HH, Fan JS, et al. Differences in characteristics, hospital care and outcomes between acute critically Ill emergency department patients with early and late do-not-resuscitate orders. Int J Environ Res Public Health. 2021;18:1028. doi: 10.3390/ijerph18031028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Phua J, Joynt GM, Nishimura M, Deng Y, Myatra SN, Chan YH, et al. Withholding and withdrawal of life-sustaining treatments in Intensive Care Units in Asia. JAMA Intern Med. 2015;175:363–71. doi: 10.1001/jamainternmed.2014.7386. [DOI] [PubMed] [Google Scholar]
- 11.Connolly C, Miskolci O, Phelan D, Buggy DJ. End-of-life in the ICU: Moving from 'withdrawal of care' to a palliative care, patient-centred approach. Br J Anaesth. 2016;117:143–5. doi: 10.1093/bja/aew109. [DOI] [PubMed] [Google Scholar]
- 12.Baek MS, Koh Y, Hong SB, Lim CM, Huh JW. Effect of timing of do not resuscitate orders on the clinical outcome of critically ill patients. Korean J Crit Care Med. 2016;31:229–35. [Google Scholar]
- 13.Yuen JK, Reid MC, Fetters MD. Hospital do-not-resuscitate orders: Why they have failed and how to fix them. J Gen Intern Med. 2011;26:791–7. doi: 10.1007/s11606-011-1632-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zingmond DS, Wenger NS. Regional and institutional variation in the initiation of early do-not-resuscitate orders. Arch Intern Med. 2005;165:1705–12. doi: 10.1001/archinte.165.15.1705. [DOI] [PubMed] [Google Scholar]
- 15.Hua M, Halpern SD, Gabler NB, Wunsch H. Effect of ICU strain on timing of limitations in life-sustaining therapy and on death. Intensive Care Med. 2016;42:987–94. doi: 10.1007/s00134-016-4240-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ouyang DJ, Lief L, Russell D, Xu J, Berlin DA, Gentzler E, et al. Timing is everything: Early do-not-resuscitate orders in the Intensive Care Unit and patient outcomes. PLoS One. 2020;15:e0227971. doi: 10.1371/journal.pone.0227971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ng YS, Stein J, Ning M, Black-Schaffer RM. Comparison of clinical characteristics and functional outcomes of ischemic stroke in different vascular territories. Stroke. 2007;38:2309–14. doi: 10.1161/STROKEAHA.106.475483. [DOI] [PubMed] [Google Scholar]
- 18.Daviaud F, Grimaldi D, Dechartres A, Charpentier J, Geri G, Marin N, et al. Timing and causes of death in septic shock. Ann Intensive Care. 2015;5:16. doi: 10.1186/s13613-015-0058-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Balshi AN, Huwait BM, Noor AS, Alharthy AM, Madi AF, Ramadan OE, et al. Modified early warning score as a predictor of Intensive Care Unit readmission within 48 hours: A retrospective observational study. Rev Bras Ter Intensiva. 2020;32:301–7. doi: 10.5935/0103-507X.20200047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cornish M, Butler MB, Green RS. Predictors of poor outcomes in critically Ill adults with hematologic malignancy. Can Respir J. 2016;2016:9431385. doi: 10.1155/2016/9431385. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.