

Abstract
Background
Nonpharmacologic mind-body therapies have demonstrated efficacy in low back pain. However, the mechanisms underlying these therapies remain to be fully elucidated.
Objective
In response to these knowledge gaps, the Stanford Center for Low Back Pain—a collaborative, National Institutes of Health P01–funded, multidisciplinary research center—was established to investigate the common and distinct biobehavioral mechanisms of three mind-body therapies for chronic low back pain: cognitive behavioral therapy (CBT) that is used to treat pain, mindfulness-based stress reduction (MBSR), and electroacupuncture. Here, we describe the design and implementation of the center structure and the associated randomized controlled trials for characterizing the mechanisms of chronic low back pain treatments.
Methods
The multidisciplinary center is running two randomized controlled trials that share common resources for recruitment, enrollment, study execution, and data acquisition. We expect to recruit over 300 chronic low back pain participants across two projects and across different treatment arms within each project. The first project will examine pain-CBT compared with MBSR and a wait-list control group. The second project will examine real versus sham electroacupuncture. We will use behavioral, psychophysical, physical measure, and neuroimaging techniques to characterize the central pain modulatory and emotion regulatory systems in chronic low back pain at baseline and longitudinally. We will characterize how these interventions impact these systems, characterize the longitudinal treatment effects, and identify predictors of treatment efficacy.
Results
Participant recruitment began on March 17, 2015, and will end in March 2023. Recruitment was halted in March 2020 due to COVID-19 and resumed in December 2021.
Conclusions
This center uses a comprehensive approach to study chronic low back pain. Findings are expected to significantly advance our understanding in (1) the baseline and longitudinal mechanisms of chronic low back pain, (2) the common and distinctive mechanisms of three mind-body therapies, and (3) predictors of treatment response, thereby informing future delivery of nonpharmacologic chronic low back pain treatments.
Trial Registration
ClinicalTrials.gov NCT02503475; https://clinicaltrials.gov/ct2/show/NCT02503475
International Registered Report Identifier (IRRID)
PRR1-10.2196/37823
Keywords: mind-body therapies, chronic low back pain, nonpharmacologic treatments, neuroimaging
Introduction
An astounding 50 million to 100 million Americans live with ongoing pain, with approximately 20 million enduring high-impact chronic pain that includes substantially restricted work, social, and self-care activities [1-3]. Chronic low back pain is cited as the most common type of chronic pain condition [3].
Globally, chronic low back pain has an estimated prevalence of 10% to 20% in adults [4,5], is the leading cause of disability [6,7], and is one of the most clinically and economically burdensome medical conditions [3,8-10]. Despite the availability and increased use of traditional surgical, pharmacological, and physical treatments [11,12], the prevalence of chronic low back pain continues to increase at an alarming rate [6,13], and the health of individuals with chronic low back pain is deteriorating [3,14].
Researchers have increasingly appreciated that chronic low back pain involves central nervous system abnormalities that cause, maintain, and amplify pain [15-20]. Acupuncture and other prominent “mind-body” treatments, such as cognitive behavioral therapy (CBT) and mindfulness-based stress reduction (MBSR), effectively engage participants in daily symptom self-management that impacts the central nervous system; these treatments offer low-risk, evidence-based, and economical therapies for this disabling condition [21-30]. However, there is a need to better characterize the underlying common and distinctive neurophysiological mechanisms of different mind-body treatments. Researchers can apply knowledge of these mechanisms to better optimize therapies targeted at an individual’s unique characteristics. Furthermore, this mechanistic information can serve as predictive biomarkers for whether a patient will be responsive to a particular mind-body therapy. A promising class of potential mechanisms relate to emotional reactivity and emotion regulation systems. Indeed, there is growing appreciation that these systems play a significant role in the perception, chronicity, and treatment efficacy of pain [17,31-35]. Research has established a clear link between emotion regulatory systems and pain perception in the brain (Figure 1) [36-46]. Importantly, CBT, MBSR, and acupuncture engage these same brain systems [28,29,47-52].
Figure 1.
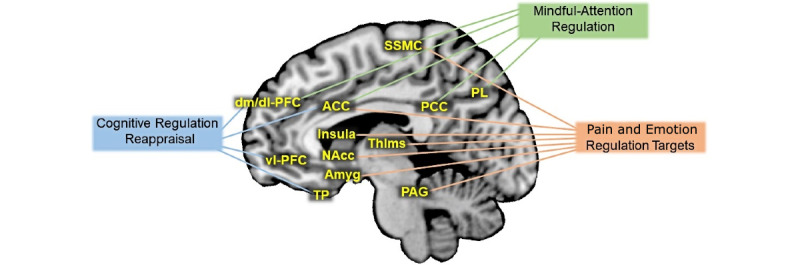
Schematic depiction of brain regions commonly involved in cognitive regulation reappraisal, mindful-attention regulation, and targets for pain and emotion regulation. ACC: anterior cingulate cortex; Amyg: amygdala; dm/dl-PFC: dorso medial and dorso lateral prefrontal cortex; NAcc: nucleus accumbens; PAG: periaqueductal gray; PCC: posterior cingulate cortex; PL: parietal lobe; SSMC: somatosensory motor cortex; Thlms: thalamus; TP: temporal pole; vl-PFC: ventro lateral prefrontal cortex.
Pain-CBT is tailored to meet the specific needs of a person living with chronic pain. It includes pain education, relaxation training, cognitive restructuring, and behavioral interventions to target and modify maladaptive pain beliefs, reduce emotional reactivity, and increase adaptive emotion regulation strategies to enhance descending modulation of pain. Randomized controlled trials (RCTs) demonstrate the acceptability and short- and long-term efficacy of pain-CBT [30,53-61], and pain-CBT is a recommended first-line treatment for chronic low back pain [62].
MBSR targets early attentional processes to enhance an experiential approach toward the ongoing stream of thoughts, emotions, and sensations, through formal and informal meditation practices [63-65]. MBSR RCTs have demonstrated short- and long-term clinical benefits by improving physical function and health-related quality of life, and by reducing pain intensity, pain unpleasantness, and disability [30,53,54,66-72].
Based on traditional Chinese medicine, acupuncture consists of inserting fine metallic needles through the skin and into specific locations along pathways considered to be special conduits for electrical signals, to stimulate and restore the body’s “vital energy” [73-75]. A meta-analysis [76] and systematic reviews [30,77] concluded that acupuncture is effective for pain reduction. Electroacupuncture uses small electric currents, passed between pairs of needles, to stimulate acupuncture points in a standardized fashion. Preclinical and animal studies suggest that electroacupuncture might be more effective at relieving chronic pain than manual acupuncture [78].
Although research and RCTs indicate a positive effect of these mind-body treatments, their common and distinct mechanisms, their relative treatment efficacy, and the suitability of specific treatment components to specific subgroups remain unclear [79]. In response to these knowledge gaps, the National Center for Complementary and Integrative Health (NCCIH) funded the Stanford Center for Low Back Pain (grant P01AT006651), which was established as one of two Centers of Excellence for Research on Complementary and Alternative Medicine (CERCs). The second CERC was awarded to the Massachusetts General Hospital (grant P01AT006663) [80-83]. Here, we provide an overview of the design and implementation of the Stanford Center for Low Back Pain and the two RCTs aimed at characterizing the mechanisms of chronic low back pain treatments.
Methods
Scientific Focus
The Stanford Center for Low Back Pain will conduct two linked RCTs to elucidate the underlying mechanisms of pain-CBT, MBSR, and electroacupuncture for chronic low back pain, with a specific focus on the intersection of pain modulatory and emotion regulatory systems.
Researchers have identified that emotions are subject to diverse regulatory processes [84-86], such as cognitive regulation and attention regulation (Figure 1). Cognitive regulation uses language-based reasoning strategies to reconstrue the meaning of an emotion-eliciting situation to up- or down-modulate features of emotion instantiated in the ventral emotion system. Attention regulation modifies alerting, orienting, and executive attention [87]. Attention regulation involves training to focus on a selected object while inhibiting irrelevant distracter stimuli. Cognitive regulation is thought to be an active mechanism in pain-CBT, whereas attention regulation is thought to be an active mechanism in MBSR. These regulatory processes form the basis for investigating the effects of mind-body therapies in these linked RCTs.
The first RCT extends and expands on previous RCTs by replicating the efficacy of pain-CBT and MBSR for chronic low back pain treatment [53,54,88] and assessing the behavioral and neural mechanisms underlying their impact on pain. We will elucidate how these therapies differentially enhance the behavioral and neural indices of cognitive regulation and attention regulation during evoked pain, prospectively, and in comparison with wait-list (WL) participants with chronic low back pain that undergo no treatment.
The second RCT will evaluate the mechanisms underlying electroacupuncture treatment of chronic low back pain. We will compare how verum (ie, real) and sham electroacupuncture for chronic low back pain impact temporal summation and conditioned pain modulation, as measures of ascending pain facilitation and descending pain inhibition, respectively (see Kong et al [89] for specific trial protocol). As with the first RCT, we will characterize the impact of electroacupuncture on emotion regulatory processes using cognitive regulation and attention regulation during evoked pain. We expect the scientific knowledge gained by this CERC to translate to improved pain intervention for chronic low back pain.
Stanford Center for Low Back Pain Organization
We organized the Stanford Center for Low Back Pain to promote cross-project collaborations, maintain recruitment consistency, enhance synergies across projects, provide common assessments and analyses, and optimize resource sharing. To facilitate administration, study execution, data collection, and analyses, the multidisciplinary projects will be supported by an Administrative Core, Clinical Research Core, Behavioral Core, and Neuroimaging and Psychophysics Core. The Administrative Core provides logistical and scientific coordination among the Scientific Cores and related individual projects. The Clinical Research Core supports scientific collaboration by focusing on regulatory submissions and oversight, participant recruitment and preliminary screening, participant safety, centralized data management and biostatistics, and education about human research. The Clinical Research Core will be the first contact for recruitment and preliminary screening of interested participants. This core will internally monitor recruitment progress, support data quality assurance, and perform between-project analyses to develop overall predictive models. The Behavioral Core will administer all behavioral measures (eg, validated questionnaires on pain, function, mood, expectancy, and quality of life) and oversee the pain-CBT and MBSR therapies. The Neuroimaging and Psychophysics Core will support all projects with a common battery to capture critical outcome measures administered by trained personnel using specialized psychophysics equipment. The battery consists of psychophysics (eg, evoked pain, temporal summation, and diffuse noxious inhibitory control) components. The neuroimaging aspect of the core will support acquisition, storage, and analysis of the structural and functional neuroimaging data.
Study Design
Overview
The study includes two thematically related, prospective, single-center RCTs. Trial 1 compares pain-CBT versus MBSR versus no treatment; trial 2 compares verum (ie, real) versus sham electroacupuncture. While the RCTs will assess and compare treatment efficacies, the primary goals are to elucidate the underlying mechanisms of the therapies.
Specific Aims
Overview
The aims and hypotheses from the original proposal are described below. We anticipate that this mechanistic study will generate many additional aims and hypotheses using the comprehensive baseline and treatment data.
Aim 1: Assess Immediate and Longer-Term Impact of Pain-CBT Versus MBSR
We will compare pain-CBT–related and MBSR-related improvements in pain symptom severity and well-being in participants with chronic low back pain to each other and to WL-MBSR or WL-CBT participants (1) immediately posttreatment and to each other and (2) at 6 months posttreatment.
Hypothesis 1 is as follows: immediately posttreatment, we expect that both pain-CBT and MBSR will yield greater improvements in pain symptom severity and well-being in chronic low back pain participants compared to WL-MBSR and WL-CBT participants. We expect equivalent improvement for MBSR and pain-CBT immediately and at 6 months posttreatment.
Aim 2: Examine Pain-CBT Versus MBSR Treatment-Related Changes in Cognitive Regulation and Attentional Regulation
We will investigate whether pain-CBT and MBSR differentially enhance behavioral and neural indices of the ability to implement cognitive regulation and attention regulation during evoked low back pain in participants with chronic low back pain.
Hypothesis 2 is as follows: we expect treatment-specific improvements for pain-CBT and MBSR from pre- to posttreatment, as follows: (1) pain-CBT will improve cognitive regulation but not attention regulation and (2) MBSR will improve attention regulation but not cognitive regulation.
Aim 3: Examine Whether Changes in Cognitive Regulation and Attention Regulation Mediate Effects of Pain-CBT and MBSR
We will test whether cognitive regulation and attention regulation changes during treatment and posttreatment mediate pain symptoms and well-being at 6 months posttreatment.
Hypothesis 3 is as follows: we expect that improvement in cognitive regulation will mediate pain-CBT but not MBSR outcomes, and that improvement in attention regulation will mediate MBSR but not pain-CBT outcomes.
Aim 4: Characterize Primary Pain Regulation as a Mediator of Reduction in Back Pain Bothersomeness in Response to Treatment (Primary Clinical Outcome)
Hypothesis 4 is as follows: (1) real versus sham electroacupuncture will lead to greater reduction in temporal summation from baseline to the end of week 4 (ie, after 8 biweekly treatment sessions) and (2) change in temporal summation from baseline to week 4 will mediate reduction in back pain bothersomeness over the treatment course (ie, baseline to posttreatment, around week 10).
Aim 5: Assess Expectation of Benefits (Primary Psychological Measure) as a Moderator of Reduction in Back Pain Bothersomeness in Response to Treatment (Primary Clinical Outcome)
Hypothesis 5 is as follows: participants’ expectations of benefits will predict reduction in back pain bothersomeness scores during the treatment period.
Additionally, in the Discussion section, we present several secondary aims and deliverables resulting from this rich data set.
Study Sample and Setting
Across both studies, we aim to enroll more than 300 adults with chronic axial low back pain without radicular symptoms. This sample size accounts for an expected 30% attrition and provides sufficient statistical power for each project. An additional 30 healthy adults will be enrolled for a single neuroimaging visit as the healthy control group. Study screening, enrollment, pre- and posttreatment assessments and procedures, and the pain-CBT and MBSR treatment sessions will take place at the Stanford Systems Neuroscience and Pain Lab of the Stanford Division of Pain Medicine in Palo Alto, California. Verum or sham electroacupuncture sessions will take place in one of 10 acupuncture offices located across the San Francisco Bay Area, based on proximity to each participant. Magnetic resonance imaging (MRI) will occur at the Stanford Lucas Center for Imaging.
Inclusion and Exclusion Criteria
Recruitment will include 21- to 65-year-old men and women with chronic low back pain as determined by the National Institutes of Health (NIH) Task Force on Research Standards for chronic low back pain [90]. Tables 1 and 2 list inclusion and exclusion criteria, respectively, and describe how the criteria will be ascertained. A healthy control group will be recruited consisting of adults with no chronic pain and no medical or mental health condition that would interfere with study procedures. The control group will be age matched (ie, ±2 years) and gender matched to the chronic low back pain group at baseline.
Table 1.
Inclusion criteria.
| Inclusion criteria | Rationale | Sources |
| Axial low back pain as primary pain complaint without radicular symptoms | Study restricted to low back pain | Aa, TSb, Sc |
| Pain duration ≥3 months and pain experienced on at least half the days in the past 6 months | As per recent NIHd Task Force on Research Standards for Chronic Low Back Pain [90] | A, TS, S |
| Average pain intensity ≥3/10 for the past 2 weeks after consent | No significant change in level of back pain | A, TS, S |
| Average pain intensity ≥4/10 for the past month at screening visit | Significant level of back pain to treat and to detect improvement | A, TS, S |
| English fluency | N/Ae | A, TS, S |
| Males and females, 21 to 65 years of age | N/Ae | A, TS, S |
aA: automated data gathered from REDCap (Research Electronic Data Capture) surveys.
bTS: telephone screening.
cS: screening visit.
dNIH: National Institutes of Health.
eN/A: not applicable; this criterion was also applied to the healthy control group.
Table 2.
Exclusion criteria.
| Exclusion criteria | Rationale | Sources |
| Previous CBTa or MBSRb treatment or similar coursework in the last 2 years, or previous acupuncture treatment for any reason in the past 5 years, respectively, for the two projectsc | Possible bias due to prior exposure to treatment | Ad, TSe, Sf |
| For the CBT and MBSR project, regular meditation practice (≥2 times/week, ≥15 minutes per meditation session, for ≥6 months) over the last 2 yearsc | Possible bias due to prior exposure to some essential aspects of MBSR | A, TS, S |
| Participating in any interventional research study or completed participation in the last 2 months; enrollment in an observational study is acceptablec | Treatment interference | A, TS, S |
| MRIg contraindications (eg, metal implants and claustrophobia)c | MRI safety | A, TS, S |
| Neurologic disorder, history of seizures, stroke, or brain abnormalities, at the discretion of the study teamc | Brain integrity interference | A, TS, S |
| Any radicular symptoms or other comorbid pain syndrome | Study restricted to low back pain | A, TS, S |
| Any medical condition (eg, active infection and heart disease) that would interfere with study procedures, at the discretion of the study teamc | Medical conditions may confound mechanistic inferences | A, TS, S |
| Mental health conditions or treatment for mental health problems that would interfere with study procedures, at the discretion of the study teamc | Mental health conditions may confound mechanistic inferences | A, TS, S |
| Medications: starting new medical treatment or medication for pain 2 months prior to initiation of study procedures; opioids ≥60 mg morphine equivalent units/day, anticonvulsants, benzodiazepines, beta-blockers, some antipsychotics, diabetic medications, or other medications that may interfere with study procedures at the discretion of the study team. TCAsh, gabapentinoids, SSRIsi, and SNRIsj are not exclusionary if on a stable dose of at least 2 monthsc | Medications may confound mechanistic inferences | A, TS, S |
| Ongoing legal or disability claim or worker’s compensation (permanent and stationary disability not exclusionary)c | Ongoing legal or disability claims may confound mechanistic inferences | A, TS, S |
| Currently pregnant or planning to become pregnantc | Pregnancy may confound mechanistic inferences | A, TS, S |
| Disorders indicated by the MINIk self-report questionnaire will be characterized and participants may be excluded at the discretion of the researcher | Condition that would make it difficult for a person to partake in treatments (eg, suicidality or psychotic disorders) | S |
aCBT: cognitive behavioral therapy.
bMBSR: mindfulness-based stress reduction.
cThis criterion was also applied to the healthy control group.
dA: automated data gathered from REDCap (Research Electronic Data Capture) surveys.
eTS: telephone screening.
fS: screening visit.
gMRI: magnetic resonance imaging.
hTCA: tricyclic antidepressant.
iSSRI: selective serotonin reuptake inhibitor.
jSNRI: serotonin and norepinephrine reuptake inhibitor.
kMINI: Mini–International Neuropsychiatric Interview.
Study Procedures
Following initial contact, consent, the in-person screening visit, and eligibility assessment, participants enter one of the two projects (ie, pain-CBT vs MBSR or verum vs sham acupuncture) based on eligibility and preference. Subsequently, after baseline and pretreatment behavioral and neuroimaging assessment (see Figure 2 for participant process), participants will be randomized within each project to a treatment arm (see details below in Randomization section). Immediately posttreatment, participants in both projects will undergo additional behavioral and neuroimaging assessments. Participants will subsequently receive questionnaire assessments 1, 3, 6, 9, and 12 months posttreatment.
Figure 2.
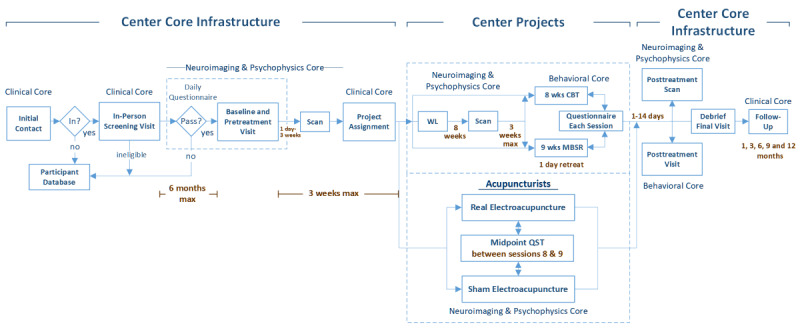
Flowchart overview of participant process in the Stanford Center for Low Back Pain project. btw: between; CBT: cognitive behavioral therapy; MBSR: mindfulness-based stress reduction; mo.: month; QST: quantitative sensory testing; wks: weeks; WL: wait-list.
Ethics Approval
The study protocols were approved for human subject research by the Stanford Institutional Review Board (reference Nos. 22436 and 11689).
Recruitment and Screening
Participants will be recruited from social media marketing, the Stanford Systems Neuroscience and Pain Lab database, and local advertisements in clinics and in the community. All advertisements will direct interested individuals to complete a secure, online REDCap (Research Electronic Data Capture [91]) self-screening form for initial eligibility screening. Responding individuals will be contacted by phone for additional screening and, if potentially eligible, will be invited to an on-site consent and screening visit for further eligibility assessment. During this visit, the Mini–International Neuropsychiatric Interview (version 7.0) [92] will be administered, and additional study-specific criteria will be assessed (Tables 1 and 2). We will subsequently use experiential sampling methods, requiring each potential participant to provide daily feedback on pain symptoms, emotional functioning, and general health and well-being for a 3-week period after consent. Participants who do not adequately provide daily feedback will be excluded prior to randomization.
Randomization
Eligible participants will be assigned to a project based on current recruitment needs and randomized within each project separately. For example, to maximize participant retention in the pain-CBT and MBSR groups we prioritize recruitment for that cohort several weeks before the start of the treatment course. If a participant is unwilling to participate in a particular project (ie, pain-CBT or MBSR or electroacupuncture), they will be assigned to the other.
For the pain-CBT an MBSR project, participants will be randomized at the group level (ie, pain-CBT, MBSR, WL–pain-CBT, or WL-MBSR) and sequentially assigned to a cohort, based on when they complete their baseline assessment, without participants or assessors knowing the assigned arm. Given that our target treatment group size is 10 to 15 participants, we will allocate up to 18 participants per class to account for participants who fail to show up for treatment and overall attrition.
For the acupuncture project, participants will be randomized to the verum or sham arm using a biased coin algorithm [93], an adaptive randomization process assuring participant similarity between arms in preselected characteristics. For example, each participant will be classified as having less or more extreme baseline pain severity, using 7 out of 10 as a cutoff. For example, the randomization algorithm will automatically adjust the randomization ratio from 50:50 probability of assignment to 40:60, such that a participant with extreme pain will be less likely randomized into the arm that has more participants with extreme pain.
Blinding
Treatment providers will not be blind to treatment allocation and will not be involved in outcome assessment. Assessors will be blind to the treatment arm at pre- and posttreatment, including follow-up assessments. In the acupuncture project, participants will be blinded [89]. In the pain-CBT and MBSR project, participants cannot be blinded to treatment; however, allocation will occur only after baseline measures are completed.
Study Treatments
Pain-CBT will be delivered in group format (10-18 participants) across eight 2-hour weekly sessions by doctoral-level psychologists. Study psychologists will be trained on the pain-CBT study protocol and supervised by BD, a senior psychologist and research team member. The pain-CBT treatment will follow the manualized and validated protocol specifically tailored for chronic low back pain [54,94,95]. It consists of psychoeducation about pain, goal setting, progressive muscle relaxation, activity scheduling, cognitive restructuring of pain cognitions and fear avoidance beliefs, exposure to feared physical activities, relapse prevention, and stress-coping skills. The protocol also provides participants with the following: (1) a participant workbook with relevant worksheets for home and in-class use, (2) two CDs with eight guided relaxation and imagery exercises for home use, and (3) Turk and Winter’s book, The Pain Survival Guide [96], for optional reading (see Table 3 for in-class curriculum details).
Table 3.
Pain-CBTa and MBSRb,c in-class curriculum.
| Session No. | Pain-CBT curriculum | MBSR curriculum |
| 1 | Welcome and introductions, including group rules, logistics, etc; CBT rationale; pain physiotherapy; relaxation rationale; importance of home practice; and diaphragmatic breathing | Introduction to program, foundations of mindfulness, more right with you than wrong, and introduction to body scan meditation |
| 2 | Goal setting, activation, and pacing (SMARTd, rest-activity cycle, etc); red flags; coping with flare-ups and creating a flare-up plan; and 7-muscle group PMRe | Patience, working with perceptions, the wandering mind, and the STOPf exercise |
| 3 | Role of thoughts and feelings in pain, introduction to CBT and terms, introduction to 3-column thought record, and 4-muscle group PMR | Nonstriving, introduction to awareness of breathing meditation, mindful lying yoga, and attention vs disattention |
| 4 | Evaluating and generating alternate thoughts, introduction to evidence gathering, introduction to 4-column thought record, and 4-muscle group PMR, no tension | Nonjudging, responding vs reacting, seeing our patterns, sitting meditation, standing yoga, and research on stress and stress hardiness |
| 5 | More on evidence gathering and alternate thoughts (more detail), working with thoughts review, and body scan | Acknowledgment, group reflections on halfway point, small and large groups, sitting meditation, and Qi Gong |
| 6 | Thought records review and walking body scan | Letting it be, skillful communication, avoiding difficulty vs entering and blending, lovingkindness meditation, and walking meditation |
| 7 | Review of skills, troubleshooting regarding thought records, pain and mood, pain core beliefs, and sleep tips | Sitting meditation, mindful movement, trust and self-reliance, learning how to practice on one’s own, and mindfulness in everyday life |
| 8 | Review of skills, “signs” of not using skills: creating a plan for maintaining gains and dealing with setbacks, termination and wrap-up, and guided imagery | Sitting meditation, mindful movement, the class never ends: practice for the rest of your life, and course review and group reflection |
aCBT: cognitive behavioral therapy.
bMSBR: mindfulness-based stress reduction.
cThe MBSR curriculum also includes an orientation pre-MBSR session and the daylong retreat.
dSMART: Specific, Measurable, Achievable, Realistic, and Time-bound.
ePMR: progressive muscle relaxation.
fSTOP: Stop, Take a breath, Observe, Proceed.
MBSR will be delivered in a similar group format (10-18 participants) by a certified instructor with extensive experience delivering MBSR in clinical trials. MBSR will consist of 10 sessions, including an introductory session, eight 2.5-hour weekly sessions, and an optional 1-day meditation retreat. MBSR consists of informal and formal mindful meditation exercises practiced in class and at home. Each class consists of guided meditations, gentle movement exercises, lectures, and group discussions. The course includes a daylong retreat weekend session (Table 4) within the last 3 weeks. Between classes, students engage in home practice through meditation CDs, homework assignments, and readings from the course textbook, Full Catastrophe Living by Kabat-Zinn and Hanh [97]. All participants will be provided with two meditation CDs, Full Catastrophe Living, and handouts for homework assignments (see Table 3 for in-class curriculum details).
Table 4.
Outline of mindfulness-based stress reduction group’s daylong retreat.
| Time | Activity |
| 9:30 AM | Introductions |
| 10 AM | Awareness of breathing |
| 10:15 AM | Lying yoga |
| 10:30 AM | Body scan meditation |
| 11:15 AM | Walking meditation |
| 11:45 AM | Sitting meditation |
| 12:15 PM | Lunch and rest |
| 1:30 PM | Yoga |
| 2 PM | Sitting meditation |
| 2:30 PM | Walking meditation |
| 2:45 PM | Sitting meditation |
| 3:10 PM | Walking meditation |
| 3:25 PM | Lovingkindness meditation |
| 3:45 PM | Group discussion (check out) |
| 4:10 PM | Farewell |
Participants in the WL arms will undergo no intervention for 8 weeks and then be assigned to pain-CBT or MBSR, according to availability. The initial 8 weeks of the WL condition will provide control for habituation to the assessments and for nonspecific factors, such as self-monitoring and contact with the research team.
A licensed acupuncturist will deliver both real and sham electroacupuncture over an 8-week period and 16 sessions. Treatment will consist of standardized electroacupuncture administration, both in terms of point selection and stimulation level. Each session will last approximately 45 minutes, except the first session, which will last 90 minutes and include an initial clinical assessment by the acupuncturist. The real electroacupuncture session will include the use of 20 needles per session. Flexibility in point selection is built into the standardized electroacupuncture protocol to allow for up to 10 more needles in cases where the patient reports hip or buttock pain or if the patient does not experience at least 30% pain reduction after the first four sessions. The sham electroacupuncture will include the use of nonpenetrating needles [98] at non–meridian points (ie, away from the center of the back) to minimize potential physiological effects, and since previous studies indicated potential pain relief attributed to nonpenetrating touch at the location of pain [99,100]. As previously implemented [101], sham electroacupuncture will be conducted by connecting broken wires to the electrical stimulators. The full protocol describing acupuncturist selection and training as well as treatment parameters, including point selection and location, has been published [89].
Treatment Fidelity
The manualized treatment protocols in pain-CBT and MBSR provide structured content for every treatment session, with little room for therapist drift. To further ensure treatment fidelity, a checklist was created for each session of both treatments. These fidelity checklists contain the essential components of the respective treatment session. Treatment fidelity ratings will be conducted in real time during each pain-CBT or MBSR session by a trained research specialist familiar with the treatment they are rating. Each treatment provider is given the criteria that will be used for treatment fidelity.
For acupuncture, treatment fidelity ratings will be based on reviews of structured case report forms completed by the acupuncturists after each session and audio session recordings. The review will include a random sample of 10% to 15% of sessions provided to participants seen by each acupuncturist. To minimize potential drift from treatment protocol and optimize fidelity, there will be quarterly meetings of the acupuncturists with JTK, who has extensive experience in delivering electroacupuncture for pain. During these meetings, corrective feedback of protocol deviations will be discussed, as needed.
Data Collection, Management, and Quality Control
Table 5 [92,102-127] summarizes the questionnaires, domains assessed, and timing of administration. All questionnaires will be completed via a Health Insurance Portability and Accountability Act–compliant REDCap platform. Participants will receive email reminders to complete their surveys via a secure link. Participants will also undergo physical assessment, quantitative sensory testing, and neuroimaging at pre- and posttreatment. The research team will assess data quality every 6 months by plotting data range and checking for missing values on REDCap, without unblinding the treatment assignment. Adherence and retention will be promoted by appointment reminders through email, text, and phone the day before scheduled assessments. In these reminders, we communicate the expectation and importance of attending all intervention and assessment visits. Participant compensation is contingent on the number of sessions they complete.
Table 5.
Schedule of measures administration.
| Measurement | Pretreatment | Treatment (8 weeks) |
Posttreatment | Follow-up month | Longitudinal surveysa |
|
|||||||
| Screening | Baseline |
|
|
1 | 3 | 6 | 9 | 12 |
|
||||
| Demographics | ✓b |
|
|
|
|
|
|
|
|
|
|
||
| Medical history | ✓ |
|
|
|
|
|
|
|
|
|
|
||
| Mini–International Neuropsychiatric Interview [92] | ✓ |
|
|
|
|
|
|
|
|
|
|
||
| Childhood Trauma Questionnaire [102] |
|
✓ |
|
|
|
|
|
|
|
|
|
||
| Marlowe-Crowne Social Desirability Scale [103] |
|
✓ |
|
|
|
|
|
|
|
|
|
||
| Stanford Expectations of Treatment Scale [104] |
|
|
✓ |
|
|
|
|
|
|
|
|
||
| Response Style Questionnaire [105] |
|
✓ |
|
✓ |
|
|
|
|
|
|
|
||
| Trait Meta Mood Scale and Toronto Alexithymia Scale hybrid [106] |
|
✓ |
|
✓ |
|
|
|
|
|
|
|
||
| Credibility Expectancy Questionnaire [107] |
|
|
|
✓ |
|
|
|
|
|
|
|
||
| Satisfaction with treatmentc |
|
|
|
✓ |
|
|
|
|
|
|
|
||
| Working Alliance Inventory [108] |
|
|
|
✓ |
|
|
|
|
|
|
|
||
| Daily questionnaired |
|
✓ | ✓ | ✓ |
|
|
|
|
|
|
|
||
| Anxiety Sensitivity Index [109] |
|
✓ |
|
✓ |
|
|
✓ |
|
✓ |
|
|
||
| Attentional Control Scale [110] |
|
✓ |
|
✓ |
|
|
✓ |
|
✓ |
|
|
||
| Cognitive Distortions Questionnaire [111] |
|
✓ |
|
✓ |
|
|
✓ |
|
✓ |
|
|
||
| Emotion Regulation Questionnaire [112] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Five-Facet Mindfulness Questionnaire [113] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Implicit Theories of Emotion Scale [114] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Positive and Negative Affect Schedule [115] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Short-form McGill Pain Questionnaire [116] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Patient Global Impression of Change [117] |
|
|
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Weekly questionnairee |
|
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
|
||
| Sleep bruxismc |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|
||
| Body pain map [118] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| NIHf PROMISg [119] (mobility, social isolation, and upper-extremity scales) |
|
|
|
✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| NIH PROMIS (anger, anxiety, depression, fatigue, pain behavior, pain intensity, pain interference, physical function, sleep disturbance, and sleep impairment scales) |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Back pain bothersomenessc |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Chronic Pain Acceptance Questionnaire [120] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Fear-Avoidance Belief Questionnaire [121] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Pain interference with sexual activities |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Pain Catastrophizing Scale [122] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Pain Self-Efficacy Questionnaire [123] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Perceived Stress Scale [124] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Roland-Morris Disability Questionnaire [125] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Self-esteemc |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| Satisfaction with Life Scale [126] |
|
✓ |
|
✓ |
|
✓ | ✓ | ✓ | ✓ | ✓ |
|
||
| NIH PROMIS (global health scale) |
|
✓ |
|
|
|
✓ |
|
|
|
✓ |
|
||
aLongitudinal surveys will be administered to participants who have been discontinued or withdrawn from the study. These questionnaires will be delivered electronically at 2 weeks and at 1, 2, 3, 6, and 12 months following the completion of their baseline behavioral appointment.
bA checkmark indicates that the measure was administered at the indicated time point.
cThis is a single-item measure.
dThe daily questionnaire consisted of several single items assessing pain severity, various physical health factors, and emotional coping. The questionnaire was administered in 2-week periods at baseline, at the beginning of weeks 1 and 3 of treatment, and posttreatment.
eThe weekly questionnaire consisted of a combination of the following validated measures: Five-Facet Mindfulness Questionnaire; Pain Catastrophizing Scale; Working Alliance Inventory; Pain Self-Efficacy Questionnaire; Fear-Avoidance Belief Questionnaire; PROMIS pain intensity, fatigue, sleep disturbance, sleep interference, depression, anxiety, and anger scales; Behavioral Activation for Depression Scale (short form) [127]; Chronic Pain Acceptance Questionnaire; and Positive and Negative Affect Schedule. Measures for assessing frequency and capability of using cognitive and attention regulation to modulate back pain were included, in addition to single-item questions on pain intensity and relaxation.
fNIH: National Institutes of Health.
gPROMIS: Patient-Reported Outcomes Measurement Information System.
Physical Assessment
Various behavioral tasks will assess objective physical functioning [128,129]. The tasks include measures of forward-bending range of motion, sit-to-stand speed, single-leg balance, back muscle endurance, 10-meter walking speed, and 2-minute walking endurance. Trained staff administer the tests and document participant performance.
Quantitative Sensory Testing
A two-point discrimination task measures participant’s tactile acuity via an established protocol [130]. Using a dolorimeter (FDK-10; Wagner Instruments), pressure pain threshold and tolerance will be measured at the bilateral trapezius muscle bed, thumb nail beds, and lumbar regions (1-inch lateral to midline of L4-L5 interspinous space, because participants tend to be more sensitive in the low back). Pain threshold, tolerance, and curve response to thermal heat pain will be measured using a Medoc Pathway machine (Ramat Ishay). Testing tasks will proceed from the least to most stimulating. The test location is initially on the left hand over the thenar eminence and rotated to the opposite hand for each subsequent thermal testing. Although different in location, our methods for obtaining the blunt pressure and thermal sensitivity measures are similar to the German Research Network on Neuropathic Pain protocol [131]. Based on our lab’s published protocol [132], dynamic quantitative sensory testing, including thermal temporal summation and followed by conditioned pain modulation, will conclude the sensory testing module.
Neuroimaging
Most chronic low back pain participants will undergo two MRI scans of their brain: one pretreatment and one posttreatment. Participants allocated to the WL group will undergo three scans: before the waiting period, after the waiting period, and after the subsequent delivered treatment. The healthy control group will undergo one scan only as a baseline comparison to the pretreatment and pre-WL scans in the chronic low back pain group.
The brain scans will include structural and functional neuroimaging protocols. Structural scans include high-resolution gray and white matter scans. Functional scans will include a 10-minute resting-state scan and a heat-pain regulation task. This task is an experimental paradigm using heat as an evoked pain stimulus, applied to the low back. Prior to the scan, participants are trained in cognitive regulation and attention regulation, which will be implemented during evoked pain inside the scanner. While in the scanner, participants are presented with visual cues on a screen instructing them to respond to a 10-second heat stimulus in three different ways. The respond cue (ie, pain reaction) instructs participants to focus on the pain and allow their mind to react to the pain normally. The reframe cue (ie, cognitive regulation) instructs participants to reinterpret the way they think about the heat stimulus to reduce their negative reactivity to the pain. The observe cue (ie, attention regulation) instructs participants to observe and attend all aspects of their overall experience and to try not to focus on anything in particular. A fourth condition, rest (ie, no pain), serves as a baseline control and is not paired with a heat stimulus. After each heat stimulus, participants will rate their pain intensity and unpleasantness with a button box on a visual analogue scale ranging from 0 (“no pain”) to 10 (“worst imaginable pain”). The functional MRI heat-pain regulation task consists of a random sequence of the four conditions (10 trials per condition; no condition permitted to occur more than twice in a row) over 17.5 minutes. Though participants are instructed that each temperature may be the same or different than the one before, each heat stimulus is the same temperature: a pain intensity rating of approximately 6 out of 10 as determined by a fine thresholding procedure prior to scanning with each individual participant.
Standard analytic approaches will be used to preprocess and analyze the neuroimaging data, using common software packages, such as FSL, SPM, or both. The steps and algorithms of such software continue to improve, so the precise approach will be determined upon completion of data accrual. However, we anticipate that the general approaches will be similar to those of previously published methods [17,84,133-135]. For example, analysis of structural data may include probabilistic tissue segmentation, rigid co-registration for detecting within-individual differences, and high-dimensional normalization for establishing between-subject differences [134]. Preprocessing and analysis of functional data will most probably include head motion correction, spatial smoothing, high-pass temporal filtering, and usage of various general linear models to conduct various comparisons between conditions and groups [84].
Sample Size Determination
We determined sample sizes for both projects to ensure adequate power to detect significant mechanistic differences associated with the treatment comparisons.
Pain-CBT Versus MBSR
To estimate sample size, we conducted power analyses based on effect sizes derived from results from our pilot studies using G*Power (version 3; Heinrich-Heine-Universität Düsseldorf). Behavioral and functional MRI studies resulted in similar medium effect sizes. For Aim 1 (ie, pre- to posttreatment), testing a 2-way interaction in a 3-group (CBT, MBSR, and WL) × 3-time (pretreatment, posttreatment, and 6-month follow-up) repeated-measures analysis of variance (ANOVA) for clinical symptoms and well-being measures, a power of 0.80 can be obtained based on a medium effect (Cohen d=0.5), α=.05, and 32 participants per group. For Aim 2 (ie, treatment effect on cognitive regulation and attention regulation), testing a 2-way interaction in a 2-group (CBT and MBSR) × 2-time (pretreatment and posttreatment) repeated-measures ANOVA for negative emotion to evoked pain, a power of 0.80 can be obtained based on a medium effect (Cohen d=0.5), α=.05, and 32 participants per group. We anticipate 6 out of 40 (15%) dropped participants for each arm.
Acupuncture: Real Versus Sham
We computed sample size based on detecting differential changes in temporal summation, the primary mediator. Our pilot study suggested an average change of 10 to 25 points of the 100-point visual analogue scale with an SD of 12 following acupuncture. Prior studies suggest no treatment effect in controls receiving sham acupuncture [136]. However, given the imprecision of the pilot study’s estimates of effect sizes, we have powered the study to detect a medium effect (d=0.56) with 50 participants in each arm, using a 2-tailed test with α=.05 and β=.8. If the point estimates from the pilot prove accurate, this project will be very well powered (98% power) to detect large effects (d=0.833). To account for approximately 20% attrition, we will enroll around 120 study participants.
Statistical Considerations
Overview
Below, we outline analyses to address the hypotheses outlined in the original proposal. Given the project’s primary focus on mechanisms rather than efficacy, we will perform the primary analyses using longitudinal treatment data with the per-protocol sample. This sample will consist of participants who completed all 3 assessment sessions (ie, pretreatment, posttreatment, and midpoint) and 5 or more out of 8 pain-CBT or MBSR treatments (or ≥13 out of 16 acupuncture visits). During the study and after completion, we will propose additional secondary aims and hypotheses using baseline and longitudinal data on chronic low back pain and before conduct of the analyses. Some of these secondary aims are presented in the Discussion section. Future hypotheses focusing on baseline data will use all available data.
Aims 1 to 3: Pain-CBT Versus MBSR
To address the efficacy aim (Aim 1), we will compute change scores from baseline to immediately posttreatment and 6 months posttreatment for pain severity and well-being. We will conduct paired t tests to examine differential between-group changes immediately (CBT vs WL, MBSR vs WL, and CBT vs MBSR) and 6 months posttreatment (CBT vs MBSR). To test whether pain-CBT and MBSR differentially enhance behavioral and neural indices of the ability to implement cognitive regulation and attention regulation during evoked low back pain (Aim 2), we will conduct 2-treatment (CBT and MBSR) × 2-regulation (cognitive regulation and attention regulation) × 2-time (baseline and posttreatment) repeated-measures mixed-effects models and within and between-group t tests on (1) pain ratings and (2) neural responses in ventral emotion-generative and dorsal emotion-regulatory brain regions. To test whether changes in cognitive regulation mediate CBT but not MBSR outcomes, and whether changes in attention regulation mediate MBSR but not CBT outcomes (Aim 3), we will implement the MacArthur mediator model. Finally, we will test whether, immediately posttreatment, both CBT and MBSR yield greater improvements in pain symptom severity and well-being in chronic low back pain compared to WL participants. We expect equivalent improvement for MBSR and CBT immediately and 6 months posttreatment. Post-WL participants will enter CBT or MBSR treatment. If between-group t tests of immediate versus posttreatment WL-CBT and posttreatment WL-MBSR groups, separately, show no difference in pain symptoms and well-being, then we will use all participants treated with CBT or MBSR to conduct an exploratory moderator analysis to investigate whether any baseline demographic (eg, age and education), clinical (eg, comorbidity, prior treatment, age of onset, and symptom severity), or emotion (eg, depression, anxiety, and affect or trait emotion regulation) variables reliably identify who will benefit from CBT or MBSR.
Aims 4 to 5: Real Versus Sham Acupuncture
To test whether real electroacupuncture versus sham electroacupuncture leads to a greater reduction in temporal summation from baseline to the end of week 4 (Aim 4), we will conduct a 2-tailed, 2-sample t test. To test whether reduction in temporal summation from baseline to week 4 mediates reduction in weekly back pain bothersomeness scores (from baseline to posttreatment), we will use a McArthur mediation analysis. We will determine significant treatment effects on the clinical outcome using a mixed-effects model, with weekly back-pain bothersomeness scores as the dependent variable and treatment assignment as the independent variable. We will include a subject-specific intercept to account for within-patient correlations. We will test a second mixed-effects model, with longitudinally measured back-pain bothersomeness scores as the independent variable. Treatment arm, reduction in temporal summation from baseline to week 4, and their interaction will be independent variables. A significant main effect for change in temporal summation or interaction between change in temporal summation and treatment arm will be evidence of mediation. To test whether participant expectations of benefits predict reduction in back-pain bothersomeness scores (weeks 0-10; Aim 5), we will use a mixed-effects regression analysis with weekly measured back-pain bothersomeness scores as the dependent variable and expectation, treatment assignment, and their interaction as independent variables.
Results
Participant recruitment began on March 17, 2015, and will end in March 2023. Recruitment was halted in March 2020 due to COVID-19 and resumed in December 2021. The trials were registered in ClinicalTrials.gov (NCT02503475) on July 21, 2015. The initial protocols and subsequent revisions follow NCCIH guidelines.
Discussion
This NCCIH CERC P01–funded research strategy represents a novel direction for pain research for investigating common and distinct mechanisms of three mind-body therapies for chronic low back pain. The common and distinct mechanisms of these three mind-body therapies can be elucidated by comparing data across projects sharing phenotyping and data collection systems. While these therapies have been previously studied, the current effort extends them in several more ways. Specifically, we will be focusing on the role of different pain modulatory and emotion regulatory systems (ie, cognitive regulation and attention regulation) and their interactions. Moreover, we use neuroimaging to reveal underlying neural mechanisms that will support the development of biomarkers and neural targets for neuromodulatory techniques. These novel approaches will allow investigators to better delineate the biopsychosocial basis of chronic low back pain and support a personalized approach for treatment efficacy.
Furthermore, the comprehensive approach to systemically phenotyping people with chronic low back pain (expected N>300) will address a wealth of clinically important questions. Our comprehensive, longitudinal data set will represent one of the largest ever collected for chronic low back pain, with the exception of the anticipated deep phenotyping data of chronic low back pain by the NIH Back Pain Consortium several years out. The recruitment of healthy controls (ie, individuals without chronic pain, in general, and without chronic low back pain, specifically) allows investigators to elucidate novel mechanisms that may be unique to chronic low back pain, or that define clinically distinct chronic low back pain subtypes. Indeed, there is significant interest in defining subtypes of chronic pain, and its trajectories, that represent high-impact chronic pain. Additionally, the daily assessment data will provide valuable information on chronic low back pain symptom variability and flares.
Together, these extensive data collection efforts will help address the original overarching study hypotheses (see Methods section) and the following secondary clinically significant aims to advance clinical care for patients with chronic low back pain:
Identify biopsychosocial subsets of individuals with chronic low back pain with differing underlying pathogenesis defining their symptom severity, and define a diagnostic biomarker to classify chronic low back pain subtypes.
Identify predictive biomarkers using comprehensive baseline patterns of collected biopsychosocial data, combined with brief daily trajectories, to accurately predict treatment responsive to pain-CBT, MBSR, and real or sham acupuncture.
Identify differences in baseline and longitudinal emotion regulation characteristics that distinguish baseline characteristics of symptom severity in chronic low back pain and mediate treatment response to mind-body therapies.
Identify baseline pretreatment efficacy expectations associated with improved treatment outcomes and with distinctive neural imaging patterns.
Characterize symptom flares and mediating information on response to mind-body therapies through daily assessments of pain symptoms, emotional functioning, general health, and expectancy.
Determine whether individuals with longer chronic low back pain symptom duration have greater symptom severity, less psychosocial functioning, and different biological mechanisms than those with shorter symptom duration.
Determine whether individuals with localized chronic low back pain have different symptoms and underlying pathogenesis than those with chronic overlapping pain conditions and can be clustered based on baseline and longitudinal data.
Determine whether adverse childhood experiences are associated with greater symptom severity and decreased quality of life in individuals with chronic low back pain.
Determine whether various demographic factors, such as sex differences, ethnic background, and socioeconomic status, can distinguish baseline and longitudinal trajectories of symptom severity, neural mechanisms, and treatment responsiveness.
Results from these studies will advance our understanding of the pathophysiology and clinical characteristics of chronic low back pain, elucidate the mechanisms responsible for treatment response to mind-body therapies, and improve future clinical efforts for risk and treatment stratification to optimize care for individuals suffering from chronic low back pain.
Acknowledgments
We thank Dr Maisa S Ziadni for providing comments on an earlier version of this manuscript and Sara Miller for assistance in creating Figure 2. This work was supported, in part, through funding from the NIH’s National Center for Complementary and Integrative Health (NCCIH; grants P01 AT006651 [SM], P01 AT006651-S1 [BD], R01 AT008561 [BD and SM], and K23 AT008477 [J-TK]), the National Institute on Drug Abuse (NIDA; grants K24 DA029262 [SM] and K24 DA053564 [BD]), the National Institute of Neurological Disorders and Stroke (grant K24 NS126781 [SM]), the NIDA (grant T32 DA035165 [SM]), and the Redlich Pain Endowment (SM). All statements in this report are solely those of the authors and do not necessarily represent the views of the National Institutes of Health (NIH).
Abbreviations
- ANOVA
analysis of variance
- CBT
cognitive behavioral therapy
- CERC
Center of Excellence for Research on Complementary and Alternative Medicine
- MBSR
mindfulness-based stress reduction
- MRI
magnetic resonance imaging
- NCCIH
National Center for Complementary and Integrative Health
- NIDA
National Institute on Drug Abuse
- NIH
National Institutes of Health
- RCT
randomized controlled trial
- REDCap
Research Electronic Data Capture
- WL
wait-list
Footnotes
Conflicts of Interest: BD is Chief Science Advisor at AppliedVR, and her consulting role with this company (personal fees) is unrelated to the current work. BD receives royalties for four pain treatment books she has authored or coauthored. She is the principal investigator for pain research awards from the Patient-Centered Research Outcomes Research Institute and the National Institutes of Health (NIH) that investigate cognitive behavioral therapy (CBT) for chronic pain. BD serves on the Board of Directors for the American Academy of Pain Medicine and is on the Board of Directors for the Institute for Brain Potential. BD is a scientific member of the NIH Interagency Pain Research Coordinating Committee, a former member of the Centers for Disease Control and Prevention Opioid Workgroup (2020-2021), a former scientific advisory board member of the National Pain Advocacy Center (2021-2022), a current member of the Pain Advisory Group of the American Psychological Association, and serves on the Medical Advisory Board for the Facial Pain Association.
References
- 1.Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L, Kerns R, Von Korff M, Porter L, Helmick C. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018 Sep 14;67(36):1001–1006. doi: 10.15585/mmwr.mm6736a2. doi: 10.15585/mmwr.mm6736a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gatchel RJ, Reuben DB, Dagenais S, Turk DC, Chou R, Hershey AD, Hicks GE, Licciardone JC, Horn SD. Research agenda for the prevention of pain and its impact: Report of the Work Group on the Prevention of Acute and Chronic Pain of the Federal Pain Research Strategy. J Pain. 2018 Aug;19(8):837–851. doi: 10.1016/j.jpain.2018.02.015.S1526-5900(18)30107-X [DOI] [PubMed] [Google Scholar]
- 3.Institute of Medicine . Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press; 2011. [PubMed] [Google Scholar]
- 4.Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012 Jun;64(6):2028–2037. doi: 10.1002/art.34347. doi: 10.1002/art.34347. [DOI] [PubMed] [Google Scholar]
- 5.Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: Systematic review. Rev Saude Publica. 2015;49:1–10. doi: 10.1590/s0034-8910.2015049005874. http://www.scielo.br/pdf/rsp/v49/0034-8910-rsp-S0034-89102015049005874.pdf . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Lancet Low Back Pain Series Working Group What low back pain is and why we need to pay attention. Lancet. 2018 Jun 09;391(10137):2356–2367. doi: 10.1016/S0140-6736(18)30480-X.S0140-6736(18)30480-X [DOI] [PubMed] [Google Scholar]
- 7.GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017 Sep 16;390(10100):1211–1259. doi: 10.1016/S0140-6736(17)32154-2. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(17)32154-2 .S0140-6736(17)32154-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Demyttenaere K, Bruffaerts R, Lee S, Posada-Villa J, Kovess V, Angermeyer MC, Levinson D, de Girolamo G, Nakane H, Mneimneh Z, Lara C, de Graaf R, Scott KM, Gureje O, Stein DJ, Haro JM, Bromet EJ, Kessler RC, Alonso J, Von Korff M. Mental disorders among persons with chronic back or neck pain: Results from the World Mental Health Surveys. Pain. 2007 Jun;129(3):332–342. doi: 10.1016/j.pain.2007.01.022.00006396-200706000-00013 [DOI] [PubMed] [Google Scholar]
- 9.Dieleman JL, Baral R, Birger M, Bui AL, Bulchis A, Chapin A, Hamavid H, Horst C, Johnson EK, Joseph J, Lavado R, Lomsadze L, Reynolds A, Squires E, Campbell M, DeCenso B, Dicker D, Flaxman AD, Gabert R, Highfill T, Naghavi M, Nightingale N, Templin T, Tobias MI, Vos T, Murray CJL. US spending on personal health care and public health, 1996-2013. JAMA. 2016 Dec 27;316(24):2627–2646. doi: 10.1001/jama.2016.16885.2594716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shmagel A, Foley R, Ibrahim H. Epidemiology of chronic low back pain in US adults: Data from the 2009-2010 National Health and Nutrition Examination Survey. Arthritis Care Res (Hoboken) 2016 Nov;68(11):1688–1694. doi: 10.1002/acr.22890. doi: 10.1002/acr.22890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fishman SM, Ballantyne JC, Rathmell JP, editors. Bonica’s Management of Pain. 4th edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2009. [Google Scholar]
- 12.McMahon SB, Koltzenburg M, Tracey I, Turk D, editors. Wall & Melzack's Textbook of Pain. Philadelphia, PA: Elsevier Saunders; 2013. [Google Scholar]
- 13.Clark S, Horton R. Low back pain: A major global challenge. Lancet. 2018 Jun 09;391(10137):2302. doi: 10.1016/S0140-6736(18)30725-6.S0140-6736(18)30725-6 [DOI] [PubMed] [Google Scholar]
- 14.Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, Hollingworth W, Sullivan SD. Expenditures and health status among adults with back and neck problems. JAMA. 2008 Feb 13;299(6):656–664. doi: 10.1001/jama.299.6.656.299/6/656 [DOI] [PubMed] [Google Scholar]
- 15.Apkarian AV, Baliki MN, Farmer MA. Predicting transition to chronic pain. Curr Opin Neurol. 2013 Aug;26(4):360–367. doi: 10.1097/WCO.0b013e32836336ad.00019052-201308000-00006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Denk F, McMahon SB, Tracey I. Pain vulnerability: A neurobiological perspective. Nat Neurosci. 2014 Feb;17(2):192–200. doi: 10.1038/nn.3628.nn.3628 [DOI] [PubMed] [Google Scholar]
- 17.Jiang Y, Oathes D, Hush J, Darnall B, Charvat M, Mackey S, Etkin A. Perturbed connectivity of the amygdala and its subregions with the central executive and default mode networks in chronic pain. Pain. 2016 Sep;157(9):1970–1978. doi: 10.1097/j.pain.0000000000000606.00006396-201609000-00013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kucyi A, Davis KD. The dynamic pain connectome. Trends Neurosci. 2015 Feb;38(2):86–95. doi: 10.1016/j.tins.2014.11.006.S0166-2236(14)00217-3 [DOI] [PubMed] [Google Scholar]
- 19.Martucci K, Mackey S. Neuroimaging of pain: Human evidence and clinical relevance of central nervous system processes and modulation. Anesthesiology. 2018 Jun;128(6):1241–1254. doi: 10.1097/aln.0000000000002137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ung H, Brown J, Johnson K, Younger J, Hush J, Mackey S. Multivariate classification of structural MRI data detects chronic low back pain. Cereb Cortex. 2014 Apr;24(4):1037–1044. doi: 10.1093/cercor/bhs378.bhs378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Astin JA. Mind-body therapies for the management of pain. Clin J Pain. 2004;20(1):27–32. doi: 10.1097/00002508-200401000-00006. [DOI] [PubMed] [Google Scholar]
- 22.Braden BB, Pipe TB, Smith R, Glaspy TK, Deatherage BR, Baxter LC. Brain and behavior changes associated with an abbreviated 4-week mindfulness-based stress reduction course in back pain patients. Brain Behav. 2016 Mar;6(3):e00443. doi: 10.1002/brb3.443. doi: 10.1002/brb3.443.BRB3443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Egorova N, Gollub RL, Kong J. Repeated verum but not placebo acupuncture normalizes connectivity in brain regions dysregulated in chronic pain. Neuroimage Clin. 2015;9:430–435. doi: 10.1016/j.nicl.2015.09.012. https://linkinghub.elsevier.com/retrieve/pii/S2213-1582(15)00172-2 .S2213-1582(15)00172-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: Past, present, and future. Am Psychol. 2014;69(2):119–130. doi: 10.1037/a0035514.2014-04960-002 [DOI] [PubMed] [Google Scholar]
- 25.Hassed C. Mind-body therapies--Use in chronic pain management. Aust Fam Physician. 2013 Mar;42(3):112–117. http://www.racgp.org.au/afp/2013/march/mind-body-therapies/ [PubMed] [Google Scholar]
- 26.Lee C, Crawford C, Hickey A, Active Self-Care Therapies for Pain (PACT) Working Group Mind-body therapies for the self-management of chronic pain symptoms. Pain Med. 2014 Apr;15 Suppl 1:S21–S39. doi: 10.1111/pme.12383. [DOI] [PubMed] [Google Scholar]
- 27.Qaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of Physicians. Denberg TD, Barry MJ, Boyd C, Chow RD, Fitterman N, Harris RP, Humphrey LL, Vijan S. Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017 Apr 04;166(7):514–530. doi: 10.7326/M16-2367. https://www.acpjournals.org/doi/abs/10.7326/M16-2367?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .2603228 [DOI] [PubMed] [Google Scholar]
- 28.Seminowicz DA, Shpaner M, Keaser ML, Krauthamer GM, Mantegna J, Dumas JA, Newhouse PA, Filippi CG, Keefe FJ, Naylor MR. Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with chronic pain. J Pain. 2013 Dec;14(12):1573–1584. doi: 10.1016/j.jpain.2013.07.020.S1526-5900(13)01179-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shpaner M, Kelly C, Lieberman G, Perelman H, Davis M, Keefe FJ, Naylor MR. Unlearning chronic pain: A randomized controlled trial to investigate changes in intrinsic brain connectivity following cognitive behavioral therapy. Neuroimage Clin. 2014;5:365–376. doi: 10.1016/j.nicl.2014.07.008. https://linkinghub.elsevier.com/retrieve/pii/S2213-1582(14)00100-4 .S2213-1582(14)00100-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Skelly A, Chou R, Dettori J, Turner J, Friedly J, Rundell S, Fu R, Brodt E, Wasson N, Kantner S, Ferguson A. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update. Comparative Effectiveness Review No. 227. Rockville, MD: Agency for Healthcare Research and Quality; 2020. Apr, [2022-06-14]. https://effectivehealthcare.ahrq.gov/products/noninvasive-nonpharm-pain-update/research . [PubMed] [Google Scholar]
- 31.Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 2013 Jul;14(7):502–511. doi: 10.1038/nrn3516.nrn3516 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Konietzny K, Suchan B, Kreddig N, Hasenbring MI, Chehadi O. [Emotion regulation and pain: Behavioral and neuronal correlates: A transdiagnostic approach] [Article in German] Schmerz. 2016 Oct;30(5):412–420. doi: 10.1007/s00482-016-0162-1.10.1007/s00482-016-0162-1 [DOI] [PubMed] [Google Scholar]
- 33.Linton SJ. A transdiagnostic approach to pain and emotion. J Appl Biobehav Res. 2013 Jun;18(2):82–103. doi: 10.1111/jabr.12007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lumley MA, Cohen JL, Borszcz GS, Cano A, Radcliffe AM, Porter LS, Schubiner H, Keefe FJ. Pain and emotion: A biopsychosocial review of recent research. J Clin Psychol. 2011 Sep;67(9):942–968. doi: 10.1002/jclp.20816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Malfliet A, Coppieters I, Van Wilgen P, Kregel J, De Pauw R, Dolphens M, Ickmans K. Brain changes associated with cognitive and emotional factors in chronic pain: A systematic review. Eur J Pain. 2017 May;21(5):769–786. doi: 10.1002/ejp.1003. [DOI] [PubMed] [Google Scholar]
- 36.Baliki MN, Chialvo DR, Geha PY, Levy RM, Harden RN, Parrish TB, Apkarian AV. Chronic pain and the emotional brain: Specific brain activity associated with spontaneous fluctuations of intensity of chronic back pain. J Neurosci. 2006 Nov 22;26(47):12165–12173. doi: 10.1523/JNEUROSCI.3576-06.2006. http://www.jneurosci.org/cgi/pmidlookup?view=long&pmid=17122041 .26/47/12165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Baliki MN, Petre B, Torbey S, Herrmann KM, Huang L, Schnitzer TJ, Fields HL, Apkarian AV. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012 Jul 01;15(8):1117–1119. doi: 10.1038/nn.3153.nn.3153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Berna C, Leknes S, Holmes EA, Edwards RR, Goodwin GM, Tracey I. Induction of depressed mood disrupts emotion regulation neurocircuitry and enhances pain unpleasantness. Biol Psychiatry. 2010 Jun 01;67(11):1083–1090. doi: 10.1016/j.biopsych.2010.01.014.S0006-3223(10)00056-9 [DOI] [PubMed] [Google Scholar]
- 39.Buhle JT, Kober H, Ochsner KN, Mende-Siedlecki P, Weber J, Hughes BL, Kross E, Atlas LY, McRae K, Wager TD. Common representation of pain and negative emotion in the midbrain periaqueductal gray. Soc Cogn Affect Neurosci. 2013 Aug;8(6):609–616. doi: 10.1093/scan/nss038. https://academic.oup.com/scan/article-lookup/doi/10.1093/scan/nss038 .nss038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hashmi JA, Baliki MN, Huang L, Baria AT, Torbey S, Hermann KM, Schnitzer TJ, Apkarian AV. Shape shifting pain: Chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain. 2013 Sep;136(Pt 9):2751–2768. doi: 10.1093/brain/awt211.awt211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lapate RC, Lee H, Salomons TV, van Reekum CM, Greischar LL, Davidson RJ. Amygdalar function reflects common individual differences in emotion and pain regulation success. J Cogn Neurosci. 2012 Jan;24(1):148–158. doi: 10.1162/jocn_a_00125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ochsner K, Ludlow D, Knierim K, Hanelin J, Ramachandran T, Glover G, Mackey S. Neural correlates of individual differences in pain-related fear and anxiety. Pain. 2006 Jan;120(1-2):69–77. doi: 10.1016/j.pain.2005.10.014.00006396-200601000-00009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Schulz E, Stankewitz A, Witkovský V, Winkler AM, Tracey I. Strategy-dependent modulation of cortical pain circuits for the attenuation of pain. Cortex. 2019 Apr;113:255–266. doi: 10.1016/j.cortex.2018.12.014.S0010-9452(18)30436-2 [DOI] [PubMed] [Google Scholar]
- 44.Wager TD, Rilling JK, Smith EE, Sokolik A, Casey KL, Davidson RJ, Kosslyn SM, Rose RM, Cohen JD. Placebo-induced changes in fMRI in the anticipation and experience of pain. Science. 2004 Feb 20;303(5661):1162–1167. doi: 10.1126/science.1093065.303/5661/1162 [DOI] [PubMed] [Google Scholar]
- 45.Wiech K, Farias M, Kahane G, Shackel N, Tiede W, Tracey I. An fMRI study measuring analgesia enhanced by religion as a belief system. Pain. 2008 Oct 15;139(2):467–476. doi: 10.1016/j.pain.2008.07.030.00006396-200810150-00027 [DOI] [PubMed] [Google Scholar]
- 46.Woo C, Roy M, Buhle JT, Wager TD. Distinct brain systems mediate the effects of nociceptive input and self-regulation on pain. PLoS Biol. 2015 Jan;13(1):e1002036. doi: 10.1371/journal.pbio.1002036. https://dx.plos.org/10.1371/journal.pbio.1002036 .PBIOLOGY-D-14-02415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Gard T, Hölzel BK, Sack AT, Hempel H, Lazar SW, Vaitl D, Ott U. Pain attenuation through mindfulness is associated with decreased cognitive control and increased sensory processing in the brain. Cereb Cortex. 2012 Nov;22(11):2692–2702. doi: 10.1093/cercor/bhr352.bhr352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Goldin PR, Gross JJ. Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion. 2010 Feb;10(1):83–91. doi: 10.1037/a0018441.2010-01983-016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Jensen KB, Kosek E, Wicksell R, Kemani M, Olsson G, Merle JV, Kadetoff D, Ingvar M. Cognitive behavioral therapy increases pain-evoked activation of the prefrontal cortex in patients with fibromyalgia. Pain. 2012 Jul;153(7):1495–1503. doi: 10.1016/j.pain.2012.04.010.00006396-201207000-00024 [DOI] [PubMed] [Google Scholar]
- 50.Yoshino A, Okamoto Y, Okada G, Takamura M, Ichikawa N, Shibasaki C, Yokoyama S, Doi M, Jinnin R, Yamashita H, Horikoshi M, Yamawaki S. Changes in resting-state brain networks after cognitive-behavioral therapy for chronic pain. Psychol Med. 2018 May;48(7):1148–1156. doi: 10.1017/S0033291717002598.S0033291717002598 [DOI] [PubMed] [Google Scholar]
- 51.Zeidan F, Martucci KT, Kraft RA, Gordon NS, McHaffie JG, Coghill RC. Brain mechanisms supporting the modulation of pain by mindfulness meditation. J Neurosci. 2011 Apr 06;31(14):5540–5548. doi: 10.1523/JNEUROSCI.5791-10.2011. http://www.jneurosci.org/cgi/pmidlookup?view=long&pmid=21471390 .31/14/5540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Huang W, Pach D, Napadow V, Park K, Long X, Neumann J, Maeda Y, Nierhaus T, Liang F, Witt CM. Characterizing acupuncture stimuli using brain imaging with fMRI--A systematic review and meta-analysis of the literature. PLoS One. 2012;7(4):e32960. doi: 10.1371/journal.pone.0032960. https://dx.plos.org/10.1371/journal.pone.0032960 .PONE-D-11-10809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cherkin DC, Anderson ML, Sherman KJ, Balderson BH, Cook AJ, Hansen KE, Turner JA. Two-year follow-up of a randomized clinical trial of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care for chronic low back pain. JAMA. 2017 Feb 14;317(6):642–644. doi: 10.1001/jama.2016.17814.2601490 [DOI] [PubMed] [Google Scholar]
- 54.Cherkin DC, Sherman KJ, Balderson BH, Cook AJ, Anderson ML, Hawkes RJ, Hansen KE, Turner JA. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA. 2016;315(12):1240–1249. doi: 10.1001/jama.2016.2323.2504811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gatchel RJ, Rollings KH. Evidence-informed management of chronic low back pain with cognitive behavioral therapy. Spine J. 2008;8(1):40–44. doi: 10.1016/j.spinee.2007.10.007.S1529-9430(07)00900-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol. 2007 Jan;26(1):1–9. doi: 10.1037/0278-6133.26.1.1.2006-23340-001 [DOI] [PubMed] [Google Scholar]
- 57.Linton SJ, Nordin E. A 5-year follow-up evaluation of the health and economic consequences of an early cognitive behavioral intervention for back pain: A randomized, controlled trial. Spine (Phila Pa 1976) 2006 Apr 15;31(8):853–858. doi: 10.1097/01.brs.0000209258.42037.02.00007632-200604150-00003 [DOI] [PubMed] [Google Scholar]
- 58.Monticone M, Cedraschi C, Ambrosini E, Rocca B, Fiorentini R, Restelli M, Gianola S, Ferrante S, Zanoli G, Moja L. Cognitive-behavioural treatment for subacute and chronic neck pain. Cochrane Database Syst Rev. 2015 May 26;(5):CD010664. doi: 10.1002/14651858.CD010664.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999 Mar;80(1-2):1–13. doi: 10.1016/s0304-3959(98)00255-3. [DOI] [PubMed] [Google Scholar]
- 60.Turner J, Holtzman S, Mancl L. Mediators, moderators, and predictors of therapeutic change in cognitive-behavioral therapy for chronic pain. Pain. 2007 Feb;127(3):276–286. doi: 10.1016/j.pain.2006.09.005.00006396-200702000-00011 [DOI] [PubMed] [Google Scholar]
- 61.Williams ACDC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2012 Nov 14;11:CD007407. doi: 10.1002/14651858.CD007407.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM, Koes BW, Peul W, Turner JA, Maher CG, Lancet Low Back Pain Series Working Group Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet. 2018 Jun 09;391(10137):2368–2383. doi: 10.1016/S0140-6736(18)30489-6.S0140-6736(18)30489-6 [DOI] [PubMed] [Google Scholar]
- 63.Baer RA, editor. Mindfulness-Based Treatment Approaches: Clinician's Guide to Evidence Base and Applications. 2nd edition. London, UK: Academic Press; 2014. [Google Scholar]
- 64.Bishop SR. What do we really know about mindfulness-based stress reduction? Psychosom Med. 2002;64(1):71–83. doi: 10.1097/00006842-200201000-00010. [DOI] [PubMed] [Google Scholar]
- 65.Kabat-Zinn J. Mindfulness-based interventions in context: Past, present, and future. Clin Psychol. 2003 Jun;10(2):144–156. doi: 10.1093/clipsy.bpg016. [DOI] [Google Scholar]
- 66.Anheyer D, Haller H, Barth J, Lauche R, Dobos G, Cramer H. Mindfulness-based stress reduction for treating low back pain: A systematic review and meta-analysis. Ann Intern Med. 2017 Jun 06;166(11):799–807. doi: 10.7326/M16-1997.2622873 [DOI] [PubMed] [Google Scholar]
- 67.Cramer H, Haller H, Lauche R, Dobos G. Mindfulness-based stress reduction for low back pain. A systematic review. BMC Complement Altern Med. 2012 Sep 25;12:162. doi: 10.1186/1472-6882-12-162. https://bmccomplementalternmed.biomedcentral.com/articles/10.1186/1472-6882-12-162 .1472-6882-12-162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kabat-Zinn J, Lipworth L, Burncy R, Sellers W. Four-year follow-up of a meditation-based program for the self-regulation of chronic pain. Clin J Pain. 1986;2(3):159–774. doi: 10.1097/00002508-198602030-00004. [DOI] [Google Scholar]
- 69.Majeed MH, Ali AA, Sudak DM. Mindfulness-based interventions for chronic pain: Evidence and applications. Asian J Psychiatr. 2018 Feb;32:79–83. doi: 10.1016/j.ajp.2017.11.025.S1876-2018(17)30427-6 [DOI] [PubMed] [Google Scholar]
- 70.Morone NE, Greco CM, Weiner DK. Mindfulness meditation for the treatment of chronic low back pain in older adults: A randomized controlled pilot study. Pain. 2008 Feb;134(3):310–319. doi: 10.1016/j.pain.2007.04.038.00006396-200802000-00010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Rosenzweig S, Greeson JM, Reibel DK, Green JS, Jasser SA, Beasley D. Mindfulness-based stress reduction for chronic pain conditions: Variation in treatment outcomes and role of home meditation practice. J Psychosom Res. 2010 Jan;68(1):29–36. doi: 10.1016/j.jpsychores.2009.03.010.S0022-3999(09)00094-4 [DOI] [PubMed] [Google Scholar]
- 72.Schmidt S, Grossman P, Schwarzer B, Jena S, Naumann J, Walach H. Treating fibromyalgia with mindfulness-based stress reduction: Results from a 3-armed randomized controlled trial. Pain. 2011 Feb;152(2):361–369. doi: 10.1016/j.pain.2010.10.043.00006396-201102000-00022 [DOI] [PubMed] [Google Scholar]
- 73.Berman BM, Langevin HM, Witt CM, Dubner R. Acupuncture for chronic low back pain. N Engl J Med. 2010 Jul 29;363(5):454–461. doi: 10.1056/NEJMct0806114. [DOI] [PubMed] [Google Scholar]
- 74.Han J. Acupuncture analgesia: Areas of consensus and controversy. Pain. 2011 Mar;152(3 Suppl):S41–S48. doi: 10.1016/j.pain.2010.10.012.00006396-201103001-00007 [DOI] [PubMed] [Google Scholar]
- 75.Lewis K, Abdi S. Acupuncture for lower back pain: A review. Clin J Pain. 2010 Jan;26(1):60–69. doi: 10.1097/AJP.0b013e3181bad71e.00002508-201001000-00011 [DOI] [PubMed] [Google Scholar]
- 76.Vickers AJ, Cronin AM, Maschino AC, Lewith G, MacPherson H, Foster NE, Sherman KJ, Witt CM, Linde K, Acupuncture Trialists' Collaboration FT. Acupuncture for chronic pain: Individual patient data meta-analysis. Arch Intern Med. 2012 Oct 22;172(19):1444–1453. doi: 10.1001/archinternmed.2012.3654.1357513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, Fu R, Dana T, Kraegel P, Griffin J, Grusing S, Brodt ED. Nonpharmacologic therapies for low back pain: A systematic review for an American College of Physicians clinical practice guideline. Ann Intern Med. 2017 Apr 04;166(7):493–505. doi: 10.7326/M16-2459. https://www.acpjournals.org/doi/abs/10.7326/M16-2459?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .2603230 [DOI] [PubMed] [Google Scholar]
- 78.Langevin HM, Schnyer R, MacPherson H, Davis R, Harris RE, Napadow V, Wayne PM, Milley RJ, Lao L, Stener-Victorin E, Kong J, Hammerschlag R, Executive Board of the Society for Acupuncture Research Manual and electrical needle stimulation in acupuncture research: Pitfalls and challenges of heterogeneity. J Altern Complement Med. 2015 Mar;21(3):113–128. doi: 10.1089/acm.2014.0186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Burns JW. Mechanisms, mechanisms, mechanisms: It really does all boil down to mechanisms. Pain. 2016 Nov;157(11):2393–2394. doi: 10.1097/j.pain.0000000000000696.00006396-201611000-00001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lee J, Mawla I, Kim J, Loggia ML, Ortiz A, Jung C, Chan S, Gerber J, Schmithorst VJ, Edwards RR, Wasan AD, Berna C, Kong J, Kaptchuk TJ, Gollub RL, Rosen BR, Napadow V. Machine learning-based prediction of clinical pain using multimodal neuroimaging and autonomic metrics. Pain. 2019 Mar;160(3):550–560. doi: 10.1097/j.pain.0000000000001417.00006396-201903000-00003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Meints SM, Mawla I, Napadow V, Kong J, Gerber J, Chan S, Wasan AD, Kaptchuk TJ, McDonnell C, Carriere J, Rosen B, Gollub RL, Edwards RR. The relationship between catastrophizing and altered pain sensitivity in patients with chronic low-back pain. Pain. 2019 Apr;160(4):833–843. doi: 10.1097/j.pain.0000000000001461.00006396-201904000-00008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Tu Y, Jung M, Gollub RL, Napadow V, Gerber J, Ortiz A, Lang C, Mawla I, Shen W, Chan S, Wasan AD, Edwards RR, Kaptchuk TJ, Rosen B, Kong J. Abnormal medial prefrontal cortex functional connectivity and its association with clinical symptoms in chronic low back pain. Pain. 2019 Jun;160(6):1308–1318. doi: 10.1097/j.pain.0000000000001507.00006396-201906000-00008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Tu Y, Ortiz A, Gollub RL, Cao J, Gerber J, Lang C, Park J, Wilson G, Shen W, Chan S, Wasan AD, Edwards RR, Napadow V, Kaptchuk TJ, Rosen B, Kong J. Multivariate resting-state functional connectivity predicts responses to real and sham acupuncture treatment in chronic low back pain. Neuroimage Clin. 2019;23:101885. doi: 10.1016/j.nicl.2019.101885. https://linkinghub.elsevier.com/retrieve/pii/S2213-1582(19)30235-9 .S2213-1582(19)30235-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Dixon ML, Moodie CA, Goldin PR, Farb N, Heimberg RG, Gross JJ. Emotion regulation in social anxiety disorder: Reappraisal and acceptance of negative self-beliefs. Biol Psychiatry Cogn Neurosci Neuroimaging. 2020 Jan;5(1):119–129. doi: 10.1016/j.bpsc.2019.07.009.S2451-9022(19)30202-2 [DOI] [PubMed] [Google Scholar]
- 85.Gross JJ. Emotion regulation: Current status and future prospects. Psychol Inq. 2015 Mar 09;26(1):1–26. doi: 10.1080/1047840X.2014.940781. [DOI] [Google Scholar]
- 86.Opialla S, Lutz J, Scherpiet S, Hittmeyer A, Jäncke L, Rufer M, Grosse Holtforth M, Herwig U, Brühl AB. Neural circuits of emotion regulation: A comparison of mindfulness-based and cognitive reappraisal strategies. Eur Arch Psychiatry Clin Neurosci. 2015 Feb;265(1):45–55. doi: 10.1007/s00406-014-0510-z. [DOI] [PubMed] [Google Scholar]
- 87.Fan J, McCandliss BD, Fossella J, Flombaum JI, Posner MI. The activation of attentional networks. Neuroimage. 2005 Jun;26(2):471–479. doi: 10.1016/j.neuroimage.2005.02.004.S1053-8119(05)00098-4 [DOI] [PubMed] [Google Scholar]
- 88.Turner JA, Anderson ML, Balderson BH, Cook AJ, Sherman KJ, Cherkin DC. Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: Similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial. Pain. 2016 Nov;157(11):2434–2444. doi: 10.1097/j.pain.0000000000000635.00006396-201611000-00008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Kong J, MacIsaac B, Cogan R, Ng A, Law CSW, Helms J, Schnyer R, Karayannis NV, Kao M, Tian L, Darnall BD, Gross JJ, Mackey S, Manber R. Central mechanisms of real and sham electroacupuncture in the treatment of chronic low back pain: Study protocol for a randomized, placebo-controlled clinical trial. Trials. 2018 Dec 13;19(1):685. doi: 10.1186/s13063-018-3044-2. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-018-3044-2 .10.1186/s13063-018-3044-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, Carragee E, Carrino J, Chou R, Cook K, DeLitto A, Goertz C, Khalsa P, Loeser J, Mackey S, Panagis J, Rainville J, Tosteson T, Turk D, Von Korff M, Weiner DK. Report of the NIH Task Force on research standards for chronic low back pain. J Pain. 2014 Jun;15(6):569–585. doi: 10.1016/j.jpain.2014.03.005.S1526-5900(14)00680-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009 Apr;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. https://linkinghub.elsevier.com/retrieve/pii/S1532-0464(08)00122-6 .S1532-0464(08)00122-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33;quiz 34. [PubMed] [Google Scholar]
- 93.Smith MD. Encyclopedia of Statistical Sciences. Hoboken, NJ: John Wiley & Sons, Inc; 2014. Biased-coin randomization. [Google Scholar]
- 94.Cherkin DC, Sherman KJ, Balderson BH, Turner JA, Cook AJ, Stoelb B, Herman PM, Deyo RA, Hawkes RJ. Comparison of complementary and alternative medicine with conventional mind-body therapies for chronic back pain: Protocol for the Mind-body Approaches to Pain (MAP) randomized controlled trial. Trials. 2014 Jun 07;15:211. doi: 10.1186/1745-6215-15-211. https://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-15-211 .1745-6215-15-211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Darnall BD, Ziadni MS, Roy A, Kao M, Sturgeon JA, Cook KF, Lorig K, Burns JW, Mackey SC. Comparative efficacy and mechanisms of a single-session pain psychology class in chronic low back pain: Study protocol for a randomized controlled trial. Trials. 2018 Mar 06;19(1):165. doi: 10.1186/s13063-018-2537-3. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-018-2537-3 .10.1186/s13063-018-2537-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Turk DC, Winter F. The Pain Survival Guide: How to Reclaim Your Life. Washington, DC: American Psychological Association; 2020. [Google Scholar]
- 97.Kabat-Zinn J, Hanh TN. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness. New York, NY: Bantam Books; 2013. [Google Scholar]
- 98.Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998 Aug 01;352(9125):364–365. doi: 10.1016/S0140-6736(97)10471-8.S0140-6736(97)10471-8 [DOI] [PubMed] [Google Scholar]
- 99.Campbell A. Role of C tactile fibres in touch and emotion--Clinical and research relevance to acupuncture. Acupunct Med. 2006 Dec;24(4):169–171. doi: 10.1136/aim.24.4.169. [DOI] [PubMed] [Google Scholar]
- 100.Han J. Acupuncture and endorphins. Neurosci Lett. 2004 May 06;361(1-3):258–261. doi: 10.1016/j.neulet.2003.12.019.S0304394003014009 [DOI] [PubMed] [Google Scholar]
- 101.Wayne PM, Krebs DE, Macklin EA, Schnyer R, Kaptchuk TJ, Parker SW, Scarborough DM, McGibbon CA, Schaechter JD, Stein J, Stason WB. Acupuncture for upper-extremity rehabilitation in chronic stroke: A randomized sham-controlled study. Arch Phys Med Rehabil. 2005 Dec;86(12):2248–2255. doi: 10.1016/j.apmr.2005.07.287.S0003-9993(05)00914-7 [DOI] [PubMed] [Google Scholar]
- 102.Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. Validity of the Childhood Trauma Questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry. 1997 Mar;36(3):340–348. doi: 10.1097/00004583-199703000-00012.S0890-8567(09)66437-6 [DOI] [PubMed] [Google Scholar]
- 103.Crowne DP, Marlowe D. A new scale of social desirability independent of psychopathology. J Consult Psychol. 1960;24(4):349–354. doi: 10.1037/h0047358. [DOI] [PubMed] [Google Scholar]
- 104.Younger J, Gandhi V, Hubbard E, Mackey S. Development of the Stanford Expectations of Treatment Scale (SETS): A tool for measuring patient outcome expectancy in clinical trials. Clin Trials. 2012 Dec;9(6):767–776. doi: 10.1177/1740774512465064.1740774512465064 [DOI] [PubMed] [Google Scholar]
- 105.Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta Earthquake. J Pers Soc Psychol. 1991 Jul;61(1):115–121. doi: 10.1037//0022-3514.61.1.115. [DOI] [PubMed] [Google Scholar]
- 106.Parker JD, Taylor GJ, Bagby R. The 20-item Toronto Alexithymia Scale. J Psychosom Res. 2003 Sep;55(3):269–275. doi: 10.1016/s0022-3999(02)00578-0. [DOI] [PubMed] [Google Scholar]
- 107.Devilly GJ, Borkovec TD. Psychometric properties of the credibility/expectancy questionnaire. J Behav Ther Exp Psychiatry. 2000 Jun;31(2):73–86. doi: 10.1016/s0005-7916(00)00012-4. [DOI] [PubMed] [Google Scholar]
- 108.Tracey TJ, Kokotovic AM. Factor structure of the Working Alliance Inventory. Psychol Assess. 1989 Sep;1(3):207–210. doi: 10.1037/1040-3590.1.3.207. [DOI] [Google Scholar]
- 109.Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav Res Ther. 1986;24(1):1–8. doi: 10.1016/0005-7967(86)90143-9. [DOI] [PubMed] [Google Scholar]
- 110.Derryberry D, Reed MA. Anxiety-related attentional biases and their regulation by attentional control. J Abnorm Psychol. 2002 May;111(2):225–236. doi: 10.1037/0021-843x.111.2.225. [DOI] [PubMed] [Google Scholar]
- 111.de Oliveira IR. Trial-Based Cognitive Therapy: A Manual for Clinicians. New York, NY: Routledge; 2014. Introducing the Cognitive Distortions Questionnaire; pp. 25–40. [Google Scholar]
- 112.Gross JJ, John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003 Aug;85(2):348–362. doi: 10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- 113.Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006 Mar;13(1):27–45. doi: 10.1177/1073191105283504.13/1/27 [DOI] [PubMed] [Google Scholar]
- 114.Tamir M, John OP, Srivastava S, Gross JJ. Implicit theories of emotion: Affective and social outcomes across a major life transition. J Pers Soc Psychol. 2007 Apr;92(4):731–744. doi: 10.1037/0022-3514.92.4.731.2007-05059-011 [DOI] [PubMed] [Google Scholar]
- 115.Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi: 10.1037/0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- 116.Dworkin R, Turk D, Revicki D, Harding G, Coyne K, Peirce-Sandner S, Bhagwat D, Everton D, Burke L, Cowan P, Farrar J, Hertz S, Max M, Rappaport B, Melzack R. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2) Pain. 2009 Jul;144(1-2):35–42. doi: 10.1016/j.pain.2009.02.007.S0304-3959(09)00125-0 [DOI] [PubMed] [Google Scholar]
- 117.Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, Kerns RD, Stucki G, Allen RR, Bellamy N, Carr DB, Chandler J, Cowan P, Dionne R, Galer BS, Hertz S, Jadad AR, Kramer LD, Manning DC, Martin S, McCormick CG, McDermott MP, McGrath P, Quessy S, Rappaport BA, Robbins W, Robinson JP, Rothman M, Royal MA, Simon L, Stauffer JW, Stein W, Tollett J, Wernicke J, Witter J, IMMPACT Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005 Jan;113(1-2):9–19. doi: 10.1016/j.pain.2004.09.012.S0304-3959(04)00440-3 [DOI] [PubMed] [Google Scholar]
- 118.Cramer E, Ziadni M, Scherrer K, Mackey S. The somatic distribution of chronic pain and emotional distress utilizing the Collaborative Health Outcomes Information Registry (CHOIR) bodymap. J Pain. 2018 Mar;19(3):S53–S54. doi: 10.1016/j.jpain.2017.12.128. [DOI] [Google Scholar]
- 119.Cella D, Yount S, Rothrock N, Gershon R, Cook K, Reeve B, Ader D, Fries JF, Bruce B, Rose M, PROMIS Cooperative Group The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med Care. 2007 May;45(5 Suppl 1):S3–S11. doi: 10.1097/01.mlr.0000258615.42478.55.00005650-200705001-00002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Fish R, McGuire B, Hogan M, Morrison T, Stewart I. Validation of the chronic pain acceptance questionnaire (CPAQ) in an internet sample and development and preliminary validation of the CPAQ-8. Pain. 2010 Jun;149(3):435–443. doi: 10.1016/j.pain.2009.12.016.00006396-201006000-00009 [DOI] [PubMed] [Google Scholar]
- 121.Williamson E. Fear Avoidance Beliefs Questionnaire (FABQ) Aust J Physiother. 2006;52(2):149. doi: 10.1016/s0004-9514(06)70052-6. [DOI] [PubMed] [Google Scholar]
- 122.Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychol Assess. 1995;7(4):524–532. doi: 10.1037/1040-3590.7.4.524. [DOI] [Google Scholar]
- 123.Tonkin L. The pain self-efficacy questionnaire. Aust J Physiother. 2008;54(1):77. doi: 10.1016/s0004-9514(08)70073-4. [DOI] [PubMed] [Google Scholar]
- 124.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983 Dec;24(4):385. doi: 10.2307/2136404. [DOI] [PubMed] [Google Scholar]
- 125.Roland M, Fairbank J. The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine (Phila Pa 1976) 2000 Dec 15;25(24):3115–3124. doi: 10.1097/00007632-200012150-00006. [DOI] [PubMed] [Google Scholar]
- 126.Diener E, Emmons RA, Larsen RJ, Griffin S. The Satisfaction With Life Scale. J Pers Assess. 1985 Feb;49(1):71–75. doi: 10.1207/s15327752jpa4901_13. [DOI] [PubMed] [Google Scholar]
- 127.Manos RC, Kanter JW, Luo W. The behavioral activation for depression scale-short form: Development and validation. Behav Ther. 2011 Dec;42(4):726–739. doi: 10.1016/j.beth.2011.04.004.S0005-7894(11)00090-6 [DOI] [PubMed] [Google Scholar]
- 128.Harding VR, de C Williams AC, Richardson P, Nicholas M, Jackson J, Richardson I, Pither C. The development of a battery of measures for assessing physical functioning of chronic pain patients. Pain. 1994 Sep;58(3):367–375. doi: 10.1016/0304-3959(94)90131-7.00006396-199409000-00009 [DOI] [PubMed] [Google Scholar]
- 129.Lee C, Simmonds MJ, Novy DM, Jones S. Self-reports and clinician-measured physical function among patients with low back pain: A comparison. Arch Phys Med Rehabil. 2001 Feb;82(2):227–231. doi: 10.1053/apmr.2001.18214.S0003-9993(01)99985-X [DOI] [PubMed] [Google Scholar]
- 130.Luomajoki H, Moseley GL. Tactile acuity and lumbopelvic motor control in patients with back pain and healthy controls. Br J Sports Med. 2011 Apr;45(5):437–440. doi: 10.1136/bjsm.2009.060731.bjsm.2009.060731 [DOI] [PubMed] [Google Scholar]
- 131.Rolke R, Magerl W, Campbell K, Schalber C, Caspari S, Birklein F, Treede RD. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur J Pain. 2006 Jan;10(1):77–88. doi: 10.1016/j.ejpain.2005.02.003.S1090-3801(05)00027-3 [DOI] [PubMed] [Google Scholar]
- 132.Mackey IG, Dixon EA, Johnson K, Kong J. Dynamic quantitative sensory testing to characterize central pain processing. J Vis Exp. 2017 Feb 16;(120):54452. doi: 10.3791/54452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Zaki J, Ochsner KN, Hanelin J, Wager TD, Mackey SC. Different circuits for different pain: Patterns of functional connectivity reveal distinct networks for processing pain in self and others. Soc Neurosci. 2007;2(3-4):276–291. doi: 10.1080/17470910701401973.780679894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Younger J, Shen Y, Goddard G, Mackey S. Chronic myofascial temporomandibular pain is associated with neural abnormalities in the trigeminal and limbic systems. Pain. 2010 May;149(2):222–228. doi: 10.1016/j.pain.2010.01.006.00006396-201005000-00012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Weber II KA, Wager TD, Mackey S, Elliott JM, Liu W, Sparks CL. Evidence for decreased Neurologic Pain Signature activation following thoracic spinal manipulation in healthy volunteers and participants with neck pain. Neuroimage Clin. 2019;24:102042. doi: 10.1016/j.nicl.2019.102042. https://linkinghub.elsevier.com/retrieve/pii/S2213-1582(19)30389-4 .S2213-1582(19)30389-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Zheng Z, Feng S, Costa CD, Li C, Lu D, Xue C. Acupuncture analgesia for temporal summation of experimental pain: A randomised controlled study. Eur J Pain. 2010 Aug;14(7):725–731. doi: 10.1016/j.ejpain.2009.11.006.S1090-3801(09)00241-9 [DOI] [PubMed] [Google Scholar]