

Abstract
Given the disproportionate alcohol-related consequences experienced by North American Indigenous youth, there is a critical need to identify related risk and protective factors. Self-compassion, which has been found to mitigate the effects of trauma exposure, may serve as one such protective factor given the high-degree of historical trauma and contemporary discrimination identified as contributing to the alcohol-related disparities experienced by Indigenous communities. However, no research has examined how self-compassion (i.e., the ability to be kind and accepting and to extend compassion towards oneself) plays a unique role in Indigenous peoples’ experiences with alcohol. First Nation adolescents between the ages of 11 and 18 living on a reserve in Eastern Canada (N=106, Mage=14.6, 50.0% female) completed a pencil-and-paper survey regarding their alcohol use, alcohol-related problems, and self-compassion. Self-compassion was significantly inversely associated with alcohol-related problems (b=−.51, p=.01, 95%CI [−.90, −.12], and significantly interacted with frequency of alcohol use in predicting alcohol-related problems (b=−.42, p=.04, 95%CI [−.82, −.03]). Simple slopes analyses revealed that the association between frequency of alcohol use and frequency of experiencing alcohol-related problems was significant and positive at low (b=4.68, p<.001, 95%CI [2.62, 6.73]), but was not significant at high (b=−.29, p=.89, 95%CI [−4.35, 3.77]) levels of self-compassion. Binary logistic regression revealed that higher scores of self-compassion were associated with a lower odds of being in the high-risk group for AUD (OR=0.90, 95%CI [0.83, 0.98], p=.02). Our results suggest self-compassion may be protective against experiencing alcohol problems in Indigenous youth and thus may be a target for behavioral interventions.
Keywords: Indigenous, Adolescents, Alcohol use, Alcohol-Related Problems, Self-Compassion, Protective Factors
Alcohol use has been identified by North American Indigenous communities (e.g., American Indian [AI], Alaska Native, and Canadian First Nations people) as one of the most pressing health disparities they face (Dennis & Momper, 2012; Whitbeck et al., 2006). Further, Indigenous youth have identified alcohol use as a major concern within their community (Spillane et al., 2020). Indigenous youth in the United States have significantly higher lifetime rates of alcohol use across adolescence: 39.7%, 52.9%, and 72.5% of 8th, 10th, and 12th graders respectively (Swaim & Stanley, 2018), compared to 24.5%, 43.1% and 58.5% of 8th, 10th, and 12th graders in the general population (National Institute on Drug Abuse, 2020). Indigenous youth tend to initiate alcohol use at younger ages (Whitesell et al., 2012) and progress more rapidly to regular use (Bachman et al., 1991; Beauvais et al., 2007; Whitbeck et al., 2008). This is of great concern as early age of first intoxication is related to negative health outcomes including heavier rates of subsequent use, more alcohol-related problems, and greater likelihood of later being diagnosed with a substance use disorder (Henry et al., 2011; Novins & Baron, 2004). Indigenous youth also suffer disproportionately from negative consequences associated with alcohol use (Goldstein et al., in press; Indian Health Service, 2019; Szlemko et al., 2006). This disparity highlights the critical need to identify risk and protective factors that could be targeted to develop intervention and prevention programs.
The alcohol-related health disparity among Indigenous communities can be uniquely understood in the context of historical trauma. There is robust evidence for the role of historical trauma in Indigenous populations’ use of alcohol (Brave Heart, 2003; Morgan & Freeman, 2009; Skewes & Blume, 2019; Whitbeck et al., 2004; Wiechelt et al., 2012). Prior to colonial contact – with the exception of specific ceremonies – alcohol was not part of Indigenous culture (Brave Heart, 2003). Acts of oppression stemming from colonization such as the banning of traditional ways of healing, coupled with the emotional aftereffects of mass cumulative trauma (e.g., depression, posttraumatic stress), left North American Indigenous populations without mechanisms for coping with emotional distress and vulnerable to developing maladaptive ways of coping (Brave Heart, 1998). It is theorized that Indigenous populations began using alcohol as a way of escaping or avoiding traumatic memories and emotional pain associated with historical trauma (Brave Heart, 2003). Further, historical accounts note that alcohol was first introduced to Indigenous communities as a genocidal act, used to inhibit their capacity to refuse offers of trade and to “increase business and profits” for traders (Duran, 2018, p. 115), and to gain negotiating advantages for European political officials (Beauvais, 1998; Frank et al., 2000).
Theorists and Indigenous communities have clearly identified historical traumas as being likely to have resulted in alcohol problems in Indigenous communities, and in turn have placed emphasis on the use of strengths-based approaches, which take positive and holistic approaches to ameliorating problems through the identification of protective factors (Craven et al., 2016; LaFromboise & Dizon, 2003), perhaps partly in response to historical trauma and the stigmatization of alcohol use. Strengths-based approaches are consistent with Indigenous values, which tend to conceptualize health as being able, holistic, and encompassing the body and mind together (Craven et al., 2016). Moving towards applying a strengths-based approach to Indigenous alcohol use interventions would necessitate the identification of positive factors that may mitigate risk.
When considering the context of alcohol use and related historical trauma among Indigenous communities, one variable that may be particularly relevant is self-compassion. Self-compassion refers to the ability to be kind and accepting of and to extend compassion towards one’s self, including during instances of suffering or difficult circumstances (Neff, 2003a; Neff, 2003b). It is often conceptualized as comprising three facets: self-kindness (i.e., being kind to oneself rather than judging oneself harshly or being self-critical), common humanity (i.e., viewing one’s experiences as part of the larger human experience rather than viewing them as isolating), and mindfulness (i.e., a conscious direction of awareness involving taking a balanced approach to negative emotions and neither suppressing nor exaggerating emotions; Neff, 2003a; Neff, 2003b). It has been hypothesized that self-compassion mitigates the negative effects of trauma exposure (Barlow et al., 2017) and previous research has found that self-compassion is strongly related to recovery from trauma among non-Indigenous adolescents (Játiva & Cerezo, 2014). Given the history of trauma and suffering experienced by Indigenous people, self-compassion may be important to consider in relation to alcohol use and alcohol-related problems.
The relationship between self-compassion and alcohol use and alcohol-related problems has not been examined in samples of Indigenous people. In samples of non-Indigenous people self-compassion has been found to promote health and well-being (Gilbert, 2005; Neff, 2003b) and to improve the success rate of health behavioral interventions, such as those for smoking reduction (Kelly et al., 2010) and disordered eating (Kelly & Carter, 2015). Research with non-Indigenous people has found self-compassion is inversely associated with alcohol misuse in adolescents (Tanaka et al., 2011). Other studies in non-Indigenous adults have found that individuals entering a publicly funded drug and alcohol program to address problematic alcohol use reported significantly lower self-compassion than is typically seen in the general population (Brooks et al., 2012). Conversely, other work has identified self-compassion as a protective factor against alcohol-related problems among college females who experienced abuse in childhood (Miron et al., 2014). Finally, there is research to suggest that low self-compassion is associated with risk factors for the development of alcohol use disorder (AUD). For example, one study examining the associations among childhood maltreatment, self-compassion, and emotion dysregulation found that low levels of self-compassion predicted later emotion dysregulation over and above maltreatment history, severity of psychological distress, and current substance use (Vettese et al., 2011). This finding is concerning given the robust evidence that emotion dysregulation is a known risk factor underlying the development and maintenance of alcohol misuse and AUD (Weiss et al., 2015). Self-compassion has also been found to be negatively associated with other risk factors for developing AUD, including anxiety and depression (Green et al., 2012; Neff & Dahm, 2015; Phelps et al., 2018; Smith & Book, 2008). Thus, it is likely that self-compassion may buffer against these risk factors to reduce the likelihood of an individual developing AUD. However, while these associations have been observed in non-Indigenous samples, no such research has been conducted in Indigenous populations.
While previous literature has focused on the impact of historical trauma on Indigenous peoples and their relationship to alcohol use, and on the role of self-compassion in healing from trauma, no work has examined how self-compassion plays a unique role in Indigenous peoples’ experiences with alcohol. There is reason to believe that self-compassion might be related to alcohol use, alcohol-related problems, and AUD risk for Indigenous adolescents given the high-degree of historical trauma and contemporary discrimination experienced by Indigenous people (Brave Heart, 1998; Lee et al., 2019; Whitbeck et al., 2004). While Indigenous communities tend to subscribe to a collective view (Beckstein, 2014), it is possible that there are individual-level differences within communities with respect to levels of self-compassion that contribute to differing responses to historical trauma, such as risk for experiencing harm related to alcohol use. Further, previous research has found that historical trauma influences individual vulnerability to the negative effects of contemporary stressors, which in turn contributes to risk for a variety of adverse health outcomes (Bombay et al., 2014). Self-compassion has been previously found to mitigate the negative effects of trauma exposure (Barlow et al., 2017), perhaps because the common humanity component (i.e., viewing one’s experiences as connected to the larger collective experience versus viewing those experiences as isolating) decreases the personalization of trauma. Indeed, recognition of the effects of history on individual’s present circumstances has been identified by Indigenous communities as an essential component of the process of healing from historical trauma (Bombay et al., 2014; Brave Heart et al., 2011). Thus, self-compassion may be a worthwhile point of intervention to reduce risk for AUD and alcohol-related harm by aiding individuals in contextualizing their own responses to historical trauma (such as alcohol use).The goal of the present study was to examine how self-compassion relates to alcohol use, alcohol-related problems, and AUD risk in a sample of First Nation adolescents. Specifically, we hypothesized that self-compassion would be negatively associated with alcohol use, alcohol-related problems, and risk for AUD. Further, we expected that self-compassion would moderate the relation between frequency of alcohol use and alcohol-related problems, such that this association would be stronger for individuals reporting low (versus high) levels of self-compassion.
Materials and Methods
Participants and Procedures
A total of 106 First Nation adolescents from Indigenous communities located in Eastern Canada participated in this research. Data for this study were collected in the spring of 2017 as part of a larger community-based participatory research project examining risk and protective factors for substance use among First Nation adolescents (Spillane et al., in press). Participants ranged in age from 11 to 18 years (M = 14.6, SD = 2.2), were 50.0% female, and all self-reported that they were a member of a First Nation group and living on reserve. Demographic characteristics of the sample are presented in Table 1. Participants were recruited through a variety of methods including advertisements in the community, notices sent to people’s mailboxes, and snowball sampling. Advertisements and announcements indicated that the project was recruiting adolescents and their parents in the community for a study examining risk and protective factors associated with substance use among First Nation adolescents. All research procedures were approved by institutional IRB and the appropriate tribal chief and council members. Parent permission was acquired prior to recruiting each child into the study. Once parent permission was received, the investigators explained the study to the youth, all youth agreed to be a part of the study and provided written assent. Participants completed pencil-and-paper questionnaires, which took an average of 45 minutes to complete, and were compensated $25 for participating.
Table 1.
Descriptive Characteristics of the Sample
| M (SD) | n (%) | Range | |
|---|---|---|---|
| Age | 14.58 (2.15) | 11 – 18 | |
| Sex | |||
| Male | 53 (50.0%) | ||
| Female | 53 (50.0%) | ||
| Grade | 8.52 (2.62) | 6 – 12 | |
| Grade 6 | 19 (17.9%) | ||
| Grade 7 | 14 (13.2%) | ||
| Grade 8 | 12 (11.3%) | ||
| Grade 9 | 15 (14.2%) | ||
| Grade 10 | 13 (12.3%) | ||
| Grade 11 | 18 (17.0%) | ||
| Grade 12 | 11 (10.4%) | ||
| Not in school | 4 (3.8%) | ||
| Alcohol Use | |||
| Ever drank | 60 (56.6%) | ||
| RAPI1 | 7.56 (11.32) | 0 – 47 | |
| High Risk for AUD2 | 37 (34.9%) | ||
| Self-Compassion | 36.61 (5.87) | 15 – 53 |
Note.
RAPI = Rutgers Alcohol Problem Index (score reflects frequency of experiencing problems in the past year);
AUD = alcohol use disorder.
Measures
Demographics
Participants reported their age, sex, and grade in school.
Alcohol Use
The present study used one item from the Adolescent Drinking Questionnaire (ADQ; Donovan & Jessor, 1978) assessing frequency of alcohol use over the past three months. Possible response options ranged from 0 to 7, where 0 = never, I did not drink any alcohol in the past three months and 7 = everyday.
Self-Compassion
Participants completed the Self-Compassion Scale – Short Form (SCS-SF; Raes et al., 2011), a 12-item self-report questionnaire that measures the frequency of engaging in behaviors that are consistent with facets of self-compassion: self-kindness, common humanity, and mindfulness. Participants rated each item on a 5-point Likert-type scale where 1 = almost never and 5 = almost always. Item scores were summed to create a total self-compassion scale score. Coefficient alpha in the present study was .60, and McDonald’s omega was .51.
Alcohol-Related Problems
Participants completed the Rutgers Alcohol Problem Index (RAPI; Martens et al., 2007), a 23-item measure assessing frequency of experiencing negative consequences related to alcohol use. The RAPI has demonstrated good psychometric properties in a First Nation group in previous literature (Noel et al., 2010). Participants rated each item on a 4-point frequency scale (0 = never, 3 = more than 5 times) reflecting how many times they had experienced each event as a result of their alcohol use in the past year. Item scores were summed to create a total score, with higher scores reflecting greater frequency of experiencing alcohol-related problems. Coefficient alpha in the present study was .93.
AUD Risk
We created a high risk for AUD group using a cutoff of four problems on the RAPI for females and six for males. This process has been used in other studies that found these cutoffs have good specificity for identifying AUD based on Diagnostic and Statistical Manual of Mental Disorders-V criteria and differentially predict those with versus without AUD (Hagman, 2017).
Analytic Strategy
All study analyses were conducted using SPSS (Version 26.0). As recommended by Tabachnik, Fidell & Osterlind (2001), study variables were assessed for assumptions of normality, linearity, and heteroscedasticity. We then examined the bivariate correlations (i.e., Pearson product-moment to examine associations between continuous variables and point-biserial correlations to examine associations between one continuous and one dichotomous variable) to assess for multicollinearity among variables. Then, we used independent samples t tests with Cohen’s d effect size estimates to examine differences in self-compassion and alcohol-related problems between those in the high risk for AUD group or not. Next, using the PROCESS macro (Hayes, 2018), we examined the main and interactive effects of frequency of alcohol use and self-compassion on frequency of experiencing alcohol-related problems, controlling for the effects of age and sex. Predictor variables were mean centered prior to construction of the interaction term to aid in interpretation of parameter estimates and to reduce the correlation between the interaction term and its component variables (Cohen et al., 2013). The PROCESS procedures use ordinary least squares regression and bootstrapping methodology, which confer more statistical power than do standard approaches to statistical inference and do not rely on distributional assumptions (Hayes, 2018). Bootstrapping was done with 5,000 random samples generated from the observed covariance matrix to estimate bias-corrected 95% confidence intervals and significance values. Following the methods described by Aiken, West, and Reno (1991), we followed up significant interactions with simple slopes analyses and plotted regression slopes of differences in frequency of experiencing alcohol-related problems at high (one standard deviation above the mean) and low (one standard deviation below the mean) levels of self-compassion. Finally, we used a binary logistic regression model to examine the association between self-compassion and membership in the group at high risk for AUD, controlling for the effects of age and sex.
Results
Preliminary Analyses
All study analyses met assumptions of normality, linearity, heteroscedasticity, and there was no evidence of multicollinearity. Of those who reported ever having a full drink, the most commonly reported alcohol-related problems were going to school drunk (36.7%), getting into a fight or argument (36.7%), and having a bad time (36.7%). Bivariate correlations revealed that self-compassion was significantly negatively associated with both frequency of alcohol use (r[102] = −.23, p = .02), and with frequency of experiencing alcohol-related problems (r[100] = −.27, p = .007). See Table 2 for bivariate correlations among all variables of interest. There were significant differences between those in the group at high risk for AUD and those not at high risk for AUD on both self-compassion (t[103] = 2.22, p = .03, d = 0.48) and frequency of experiencing alcohol-related problems (t[100] = −11.29, p < .001, d = 1.99). Specifically, individuals in the high risk for AUD group had significantly lower self-compassion scores (M [SD] = 34.92 [4.08]) and significantly more frequent alcohol-related problems (M [SD] = 18.73 [12.27]) compared to the group not at high risk for AUD (self-compassion: 37.53 [6.50]; alcohol-related problems: 1.20 [2.03]).
Table 2.
Intercorrelations Among Primary Study Variables of Interest
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Age | - | |||||
| 2. Sex | −.02 | - | ||||
| 3. Frequency of Alcohol Use | .46*** | .07 | - | |||
| 4. Self-Compassion | −.01 | −.04 | −.23* | - | ||
| 5. Frequency of Alcohol-Related Problems | .22* | −.04 | .46*** | −.27** | - | |
| 6. AUD Risk | .35*** | −.06 | .47*** | −.21* | .75*** | - |
Note.
p < .05,
p < .01,
p < .001
Moderation Analysis Examining the Role of Self-Compassion in the Association Between Alcohol Use and Alcohol-Related Problems
The overall model examining the main and interactive effects of alcohol use and self-compassion on alcohol-related problems was significant (F[5, 94] = 7.16, p < .001, R2 = .28). There was no main effect for frequency of alcohol use (b = 2.19, SE = 1.12, t = 1.96, p = .05, 95% CI [−.03, 4.42]); however, there was a significant main effect for self-compassion (b = −.51, SE = .20, t = −2.59, p = .01, 95% CI [−.90, −.12]), controlling for the effects of age and sex. The interaction was also significant (b = −.42, SE = .20, t = −2.12, p = .04, 95% CI [−.82, −.03]). See Table 3 for a summary of moderation analyses. Probing this interaction revealed that the association between frequency of alcohol use and frequency of experiencing alcohol-related problems was significant at low (1 SD below the mean; b = 4.68, SE = 1.03, t = 4.53, p < .001, 95% CI [2.62, 6.73]), but not high (1 SD above the mean; b = −.29, SE = 2.05, t = −0.14, p = .89, 95% CI [−4.35, 3.77]) levels of self-compassion.
Table 3.
Main and Interactive Effects of Frequency of Alcohol Use and Self-Compassion on Frequency of Experiencing Alcohol-Related Problems
| Variable | B | SE | t | p | 95% CI |
|---|---|---|---|---|---|
| Constant | 4.49 | 7.88 | 0.57 | .57 | [−11.16, 20.13] |
| Age | .24 | .53 | 0.45 | .66 | [−.81, 1.29] |
| Female Sex | −2.34 | 2.03 | −1.16 | .25 | [−6.36, 1.68] |
| Alcohol Use Frequency | 2.19 | .20 | 1.96 | .054 | [−.03, 4.42] |
| Self-Compassion | −.51 | .20 | −2.59 | .01 | [−.90, −.12] |
| Alcohol Use Frequency X Self-Compassion | −.42 | .20 | −2.12 | .04 | [−.82, −.03] |
Note. Bolded typeface indicates significance at the level p < .05.
Logistic Regression Analysis Examining the Association Between Self-Compassion and AUD Risk
Binary logistic regression was used to examine the association between self-compassion and AUD risk (i.e., above cutoff of four for females and six for males on the RAPI; Hagman, 2017), controlling for age and sex. Higher scores on self-compassion were associated with lower likelihood of being in the high-risk group for AUD (OR = 0.90, 95% CI [0.83, 0.98], p =.02). The overall model was significant (χ2[3] = 19.30, p < .001, Nagelkerke R2 = .23). See Table 4 for a summary of logistic regression analyses.
Table 4.
Logistic Regression Analyses Examining the Association Between Self-Compassion and Membership in High Risk for AUD Group
| Variable | B | SE | p | OR | 95% CI |
|---|---|---|---|---|---|
| Constant | −2.91 | 2.06 | .16 | .05 | |
| Age | .39 | .11 | .001 | 1.47 | [1.18, 1.83] |
| Female Sex | .41 | .46 | .37 | 1.51 | [0.61, 3.69] |
| Self-Compassion | −.10 | .04 | .02 | 0.90 | [0.83, 0.98] |
Note. Bolded typeface indicates significance at the level p < .05.
Discussion
The current study aimed to explore the associations among self-compassion, alcohol use, alcohol-related problems, and risk for AUD in a sample of First Nation adolescents. Our results indicate that self-compassion was related to less alcohol use and fewer alcohol problems, and lower risk of AUD. This finding is consistent with research conducted in non-Indigenous individuals such that lower self-compassion was related to alcohol misuse (Tanaka et al., 2011) and others who have found that self-compassion may be related with substance use disorders (SUDs) and SUD risk factors (Brooks et al., 2012; Phelps et al., 2018; Vettese et al., 2011). Moreover, there was a significant interaction effect between self-compassion and frequency of alcohol use, indicating that self-compassion buffers the risk posed by alcohol use. That is, for those high in self-compassion, the effect of frequency of alcohol use on alcohol-related problems was not significant, while the association was significant for those low in self-compassion.
Previous research suggests that raising self-compassion may be one way to address psychological distress (Allen & Leary, 2010; Phelps et al., 2018), such as the stress and suffering experienced by Indigenous individuals as a result of historical trauma. North American Indigenous populations have faced histories of genocide, colonization, forced assimilation, and exclusion that have undermined their health and well-being. The mass traumas that Indigenous populations have been subjected to have resulted in disruption and devastation of economic systems, sustenance practices, spiritual customs, kinship networks, and family ties, causing historical losses of people, land, family, and culture (Brave Heart, 1998; Brave Heart et al., 2011; Brave Heart & DeBruyn, 1998). Historical trauma describes the emotional and psychological wounding over the lifespan and across generations stemming from the massive cumulative trauma associated with these historical losses (Brave Heart, 1998). The distinguishing characteristics of historical trauma – its widespread quality among Indigenous populations, perpetration by outsiders with purposeful and often destructive intent, and resultant collective distress in contemporary communities – makes this form of trauma particularly devastating (Evans-Campbell, 2008). Existing research underscores the pervasive role that historical trauma has played in behavioral health disparities and risk factors for alcohol use among North American Indigenous people (Morgan & Freeman, 2009; Skewes & Blume, 2019). Given that self-compassion has been hypothesized to mitigate the negative effects of trauma exposure (Barlow et al., 2017) and to be strongly related to recovery from trauma (Játiva & Cerezo, 2014), we believe it may be an important target for alcohol-use intervention. Increasing self-compassion may subsequently reduce self-regulation vulnerabilities by helping individuals develop more adaptive strategies for emotion regulation and practice self-care (Allen & Leary, 2010). Moreover, extant research suggests that self-compassion can be improved upon and cultivated through skills-training and practice (Gilbert, 2009; Neff & Germer, 2013). It has been proposed that self-compassion could be beneficial for adolescents by providing a way for adolescents to perceive their failures or mistakes proportionately and in a balanced perspective and to experience supportive and warm feelings toward themselves without engaging in the problematic process of self-criticism, evaluation and social unfavorable comparisons (Neff & McGehee, 2010). Our results suggest that by providing adolescents with skills-training to increase their self-compassion, problems associated with alcohol use may be indirectly targeted. Self-compassion focused interventions could help individuals who have experienced alcohol problems seek help for their alcohol or substance misuse.
More broadly, self-compassion may function as a protective strategy and may be a malleable preventive and intervention target for adolescents in order to foster their resilience and well-being in various contexts of their lives (Cunha, Xavier, Castilho, 2016). For instance, greater self-compassion is found to be negatively associated with depressive symptoms, and with avoidance and symptom-focused rumination in individuals with depression (Krieger et al., 2013). Depression, in turn, has been found to be related to alcohol consumption and related problems (Brière et al., 2014). Moreover, a large-scale longitudinal study examined how the interaction of self-esteem and self-compassion predicted changes in adolescent mental health over the next year. Results demonstrated that among those high in self-compassion, low self-esteem had little effect on mental health; these findings suggest that self-compassion has a buffering effect against the negative effects of low self-esteem on mental health (Marshall et al., 2015). Therefore, it is important to increase and target self-compassion, as it may serve additional protections that are important in mental well-being beyond alcohol use and related problems, as suggested by our findings.
Limitations and Future Directions
Findings of this study should be considered within the context of its limitations. First, the cross-sectional, correlational nature of this study precludes the ability to examine the causal or temporal ordering among these associations. Our findings support the need for future research to examine these associations in prospective designs, and to examine the impact of self-compassion focused interventions on subsequent alcohol consumption and related problems. Second, data were collected from one band of reserve-dwelling First Nation adolescents in Eastern Canada. It is important to consider that there is significant variability across North American Indigenous communities; thus, our findings may not generalize to other Indigenous groups, Indigenous individuals in other geographic regions, or to adolescents living off-reserve or in urban areas. Third, though our sample of 106 adolescents makes up approximately one-third of adolescents within this age range from this cultural group (INAC, 2016), our relatively small sample size should be noted as a limitation. However, it is worth noting that sensitivity analyses revealed that we were adequately powered to detect effects as small as d = .27, which correspond to r = .15 and R2 = .02; our effects were above this threshold. Fourth, the self-compassion scale demonstrated low internal consistency in this sample, which underlines the longstanding argument that measures should not be applied indiscriminately to individuals who are not the normative group for whom that measure was developed (Suzuki & Ponterotto, 2007). Low reliability of the self-compassion scale is likely to have weakened associations found by introducing unwanted error variance. Future research should examine the meaning of the self-compassion construct to Indigenous adolescents, as there may be a larger collective compassion construct that is not presently being reflected and/or the need to develop instruments that are more developmentally and culturally appropriate.
Conclusions
In conclusion, our findings suggest that self-compassion is associated with less alcohol-related problems and buffers the association between alcohol use and related problems. Specifically, the association between alcohol use and alcohol-related problems was significant for those with low, but not high levels of self-compassion, and higher scores on self-compassion were associated with decreased odds of being in the high risk for AUD group. These findings underscore the importance of assessing self-compassion among Indigenous youth, and of encouraging adolescents to practice self-kindness to reduce harm associated with alcohol use.
Figure 1.
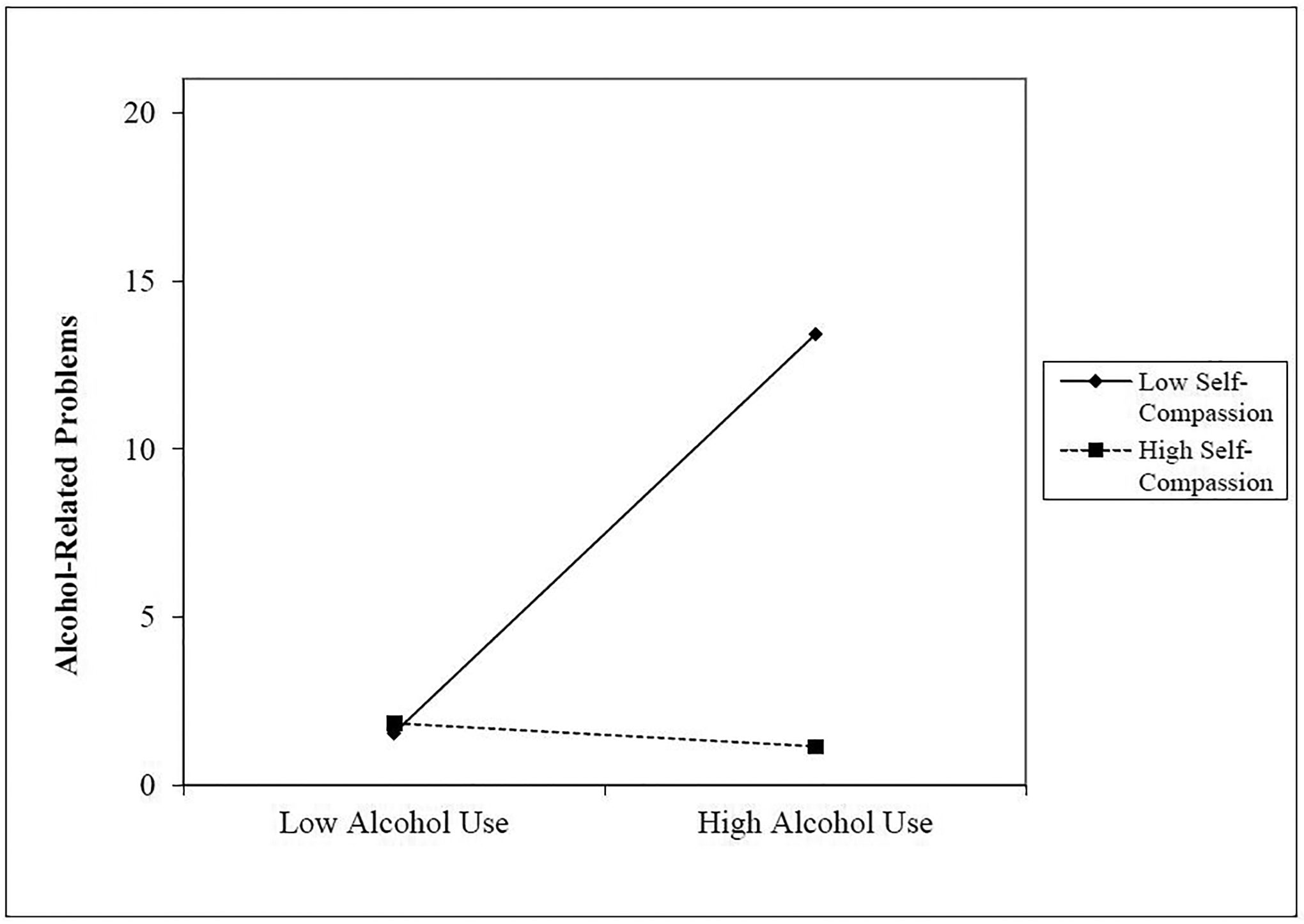
Alcohol Use by Self-Compassion Interaction for Alcohol-Related Problems
Conflicts of Interest and Source of Funding:
The authors declare no conflicts of interest. This work was supported by the National Institute on Drug Abuse (NIDA) grant (K08DA029094).
References
- Aiken LS, West SG, & Reno RR (1991). Multiple regession: Testing and interpreting interactions. Thousand Oaks, CA: SAGE. [Google Scholar]
- Allen AB, & Leary MR (2010). Self‐compassion, stress, and coping. Social and Personality Psychology Compass, 4(2), 107–118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bachman JG, Wallace JM Jr., O’Malley PM, Johnston LD, Kurth CL, & Neighbors HW (1991). Racial/ethnic differences in smoking, drinking, and illicit drug use among american high school seniors, 1976–89. American Journal of Public Health, 81(3), 372–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow MR, Turow REG, & Gerhart J (2017). Trauma appraisals, emotion regulation difficulties, and self-compassion predict posttraumatic stress symptoms following childhood abuse. Child Abuse & Neglect, 65, 37–47. [DOI] [PubMed] [Google Scholar]
- Beauvais F (1998). American indians and alcohol. Alcohol Research, 22(4), 253. [PMC free article] [PubMed] [Google Scholar]
- Beauvais F, Thurman PJ, Burnside M, & Plested B (2007). Prevalence of american indian adolescent tobacco use: 1993–2004. Substance Use and Misuse, 42(4), 591–601. 10.1080/10826080701202171 [DOI] [PubMed] [Google Scholar]
- Beckstein A (2014). Native american subjective happiness: An overview. Indigenous Policy Journal, 25(2). [Google Scholar]
- Bombay A, Matheson K, & Anisman H (2014). The intergenerational effects of indian residential schools: Implications for the concept of historical trauma. Transcultural Psychiatry, 51(3), 320–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brave Heart MYH (1998). The return to the sacred path: Healing the historical trauma and historical unresolved grief response among the Lakota through a psychoeducational group intervention. Smith College Studies in Social Work, 68(3), 287–305. [Google Scholar]
- Brave Heart MYH (2003). The historical trauma response among natives and its relationship with substance abuse: A Lakota illustration. Journal of Psychoactive Drugs, 35, 7–13. [DOI] [PubMed] [Google Scholar]
- Brave Heart MYH, Chase J, Elkins J, & Altschul DB (2011). Historical trauma among Indigenous peoples of the Americas: Concepts, research, and clinical considerations. Journal of Psychoactive Drugs, 43, 282–290. [DOI] [PubMed] [Google Scholar]
- Brave Heart MYH, & DeBruyn LM (1998). The American Indian holocaust: Healing historical unresolved grief. American Indian and Alaska Native Menta Health Research, 8, 56–78. [PubMed] [Google Scholar]
- Brière FN, Rohde P, Seeley JR, Klein D, & Lewinsohn PM (2014). Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Comprehensive Psychiatry, 55(3), 526–533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks M, Kay-Lambkin F, Bowman J, & Childs S (2012). Self-compassion amongst clients with problematic alcohol use. Mindfulness, 3(4), 308–317. [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2013). Applied multiple regression/correlation analysis for the behavioral sciences. Routledge. [Google Scholar]
- Craven RG, Ryan RM, Mooney J, Vallerand RJ, Dillon A, Blacklock F, & Magson N (2016). Toward a positive psychology of indigenous thriving and reciprocal research partnership model. Contemporary Educational Psychology, 47, 32–43. [Google Scholar]
- Dennis MK, & Momper SL (2012). “It’s bad around here now”: Tobacco, alcohol and other drug use among american indians living on a rural reservation. Journal of Ethnicity in Substance Abuse, 11(2), 130–148. 10.1080/15332640.2012.675244 [DOI] [PubMed] [Google Scholar]
- Donovan JE, & Jessor R (1978). Adolescent problem drinking. Psychosocial correlates in a national sample study. Journal of Studies on Alcohol, 39(9), 1506–1524. [DOI] [PubMed] [Google Scholar]
- Duran B (2018). Indigenous versus colonial discourse: Alcohol and american indian identity. In Dressing in feathers (pp. 111–128). Routledge. [Google Scholar]
- Evans-Campbell T (2008). Historical trauma in american indian/native alaska communities: A multilevel framework for exploring impacts on individuals, families, and communities. Journal of Interpersonal Violence, 23, 316–338. [DOI] [PubMed] [Google Scholar]
- Frank JW, Moore RS, & Ames GM (2000). Historical and cultural roots of drinking problems among american indians. American Journal of Public Health, 90(3), 344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert P (2005). Compassion: Conceptualisations, research and use in psychotherapy. Routledge. [Google Scholar]
- Gilbert P (2009). Introducing compassion-focused therapy. Advances in Psychiatric Treatment, 15(3), 199–208. [Google Scholar]
- Goldstein SC, Schick MR, Nalven T, & Spillane NS (2021). The role of valuing cultural activities in the association between alcohol expectancies and alcohol use among first nation adolescents. Journal of Studies on Alcohol and Drugs, 82(1), 112–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green KM, Zebrak KA, Fothergill KE, Robertson JA, & Ensminger ME (2012). Childhood and adolescent risk factors for comorbid depression and substance use disorders in adulthood. Addictive Behaviors, 37(11), 1240–1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagman BT (2017). Development and psychometric analysis of the brief dsm–5 alcohol use disorder diagnostic assessment: Towards effective diagnosis in college students. Psychology of Addictive Behaviors, 31(7), 797. [DOI] [PubMed] [Google Scholar]
- Hayes AF (2018). Introduction to mediation, moderation and conditional process analysis; A regression-based approach. New York, NY: The Guilford Press. [Google Scholar]
- Henry KL, McDonald JN, Oetting ER, Walker PS, Walker RD, & Beauvais F (2011). Age of onset of first alcohol intoxication and subsequent alcohol use among urban American Indian adolescents. Psychology of Addictive Behaviors, 25(1), 48–56. 10.1037/a0021710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Indian Health Service. (2019). Fact sheet: Disparities. Retrieved from https://www.ihs.gov/newsroom/factsheets/disparities/
- Indigenous and Northern Affairs Canada. (2016). First Nation profiles. Retrieved from https://fnp-ppn.aadnc-aandc.gc.ca/fnp/Main/index.aspx?lang=eng
- Játiva R, & Cerezo MA (2014). The mediating role of self-compassion in the relationship between victimization and psychological maladjustment in a sample of adolescents. Child Abuse & Neglect, 38(7), 1180–1190. [DOI] [PubMed] [Google Scholar]
- Kelly AC, Zuroff DC, Foa CL, & Gilbert P (2010). Who benefits from training in self-compassionate self-regulation? A study of smoking reduction. Journal of Social and Clinical Psychology, 29(7), 727–755. [Google Scholar]
- Krieger T, Altenstein D, Baettig I, Doerig N, & Holtforth MG (2013). Self-compassion in depression: Associations with depressive symptoms, rumination, and avoidance in depressed outpatients. Behavior Therapy, 44(3), 501–513. [DOI] [PubMed] [Google Scholar]
- LaFromboise T, & Dizon MR (2003). American Indian children and adolescents. In Gibbs JT & Huang LN (Eds.), Children of color: Psychological interventions with culturally diverse youth (p. 45–90). Jossey-Bass. [Google Scholar]
- Lee RT, Perez AD, Boykin CM, & Mendoza-Denton R (2019). On the prevalence of racial discrimination in the United States. PloS one, 14(1), e0210698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall SL, Parker PD, Ciarrochi J, Sahdra B, Jackson CJ, & Heaven PC (2015). Self-compassion protects against the negative effects of low self-esteem: A longitudinal study in a large adolescent sample. Personality and Individual Differences, 74, 116–121. [Google Scholar]
- Martens MP, Neighbors C, Dams-O’Connor K, Lee CM, & Larimer ME (2007). The factor structure of a dichotomously scored Rutgers Alcohol Problem Index. Journal of Studies on Alcohol and Drugs, 68(4), 597–606. [DOI] [PubMed] [Google Scholar]
- Miron LR, Orcutt HK, Hannan SM, & Thompson KL (2014). Childhood abuse and problematic alcohol use in college females: The role of self-compassion. Self and Identity, 13(3), 364–379. [Google Scholar]
- Morgan R, & Freeman L (2009). The healing of our people: Substance abuse and historical trauma. Substance Use & Misuse, 44, 84–98. [DOI] [PubMed] [Google Scholar]
- National Institute on Drug Abuse. (2020). Monitoring the future 2019 survey results: Overall findings. Retrieved from https://www.drugabuse.gov/related-topics/trends-statistics/infographics/monitoring-future-2019-survey-results-overall-findings
- Neff K (2003a). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. [Google Scholar]
- Neff KD (2003b). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250. [Google Scholar]
- Neff KD, & Dahm KA (2015). Self-compassion: What it is, what it does, and how it relates to mindfulness. In Handbook of Mindfulness and Self-Regulation (pp. 121–137). Springer. [Google Scholar]
- Neff KD, & Germer CK (2013). A pilot study and randomized controlled trial of the mindful self‐compassion program. Journal of Clinical Psychology, 69(1), 28–44. [DOI] [PubMed] [Google Scholar]
- Neff KD, & McGehee P (2010). Self-compassion and psychological resilience among adolescents and young adults. Self and Identity, 9(3), 225–240. [Google Scholar]
- Noel M, O’Connor R, Boudreau B, Mushquash C, Nancy Comeau M, Stevens D, & Stewart S (2010). The Rutgers Alcohol Problem Index (RAPI): A comparison of cut-points in first nations mi’kmaq and non-aboriginal adolescents in rural Nova Scotia (Vol. 8). 10.1007/s11469-009-9219-z [DOI] [Google Scholar]
- Novins DK, & Baron AE (2004). American indian substance use: The hazards for substance use initiation and progression for adolescents aged 14 to 20 years. Journal of the American Academy of Child and Adolescent Psychiatry, 43(3), 316–324. 10.1097/00004583-200403000-00013 [DOI] [PubMed] [Google Scholar]
- Phelps CL, Paniagua SM, Willcockson IU, & Potter JS (2018). The relationship between self-compassion and the risk for substance use disorder. Drug & Alcohol Dependence, 183, 78–81. [DOI] [PubMed] [Google Scholar]
- Raes F, Pommier E, Neff KD, & Van Gucht D (2011). Construction and factorial validation of a short form of the self‐compassion scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. [DOI] [PubMed] [Google Scholar]
- Skewes MC, & Blume AW (2019). Understanding the link between racial trauma and substance use among american indians. American Psychologist, 74, 88–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith JP, & Book SW (2008). Anxiety and substance use disorders: A review. The Psychiatric Times, 25(10), 19. [PMC free article] [PubMed] [Google Scholar]
- Spillane NS, Kirk-Provencher KT, Schick MR, Nalven T, Goldstein SC, & Kahler CW (2020). Identifying competing life reinforcers for substance use in first nation adolescents. Substance Use & Misuse, 55(6), 886–895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spillane NS, Schick MR, Nalven T, Goldstein SC, Kirk-Provencher KT, Hill D, & Kahler CW (in press). Testing the competing life reinforcers model for substance use in reserve-dwelling first nation youth. American Journal of Orthopsychiatry. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suzuki LA, & Ponterotto JG (2007). Handbook of multicultural assessment: Clinical, psychological, and educational applications. John Wiley & Sons. [Google Scholar]
- Swaim RC, & Stanley LR (2018). Substance use among american indian youths on reservations compared with a national sample of us adolescents. JAMA network open, 1(1), e180382–e180382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szlemko WJ, Wood JW, & Thurman PJ (2006). Native americans and alcohol: Past, present, and future. Journal of General Psychology, 133(4), 435–451. 10.3200/genp.133.4.435-451 [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS, & Osterlind SJ (2001). Using multivariate statistics (4th ed.). Pearson. [Google Scholar]
- Tanaka M, Wekerle C, Schmuck ML, Paglia-Boak A, & Team MR (2011). The linkages among childhood maltreatment, adolescent mental health, and self-compassion in child welfare adolescents. Child Abuse & Neglect, 35(10), 887–898. [DOI] [PubMed] [Google Scholar]
- Vettese LC, Dyer CE, Li WL, & Wekerle C (2011). Does self-compassion mitigate the association between childhood maltreatment and later emotion regulation difficulties? A preliminary investigation. International Journal of Mental Health and Addiction, 9(5), 480. [Google Scholar]
- Weiss NH, Sullivan TP, & Tull MT (2015). Explicating the role of emotion dysregulation in risky behaviors: A review and synthesis of the literature with directions for future research and clinical practice. Current Opinion in Psychology, 3, 22–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitbeck LB, Chen X, Hoyt DR, & Adams GW (2004). Discrimination, historical loss and enculturation: Culturally specific risk and resiliency factors for alcohol abuse among American Indians. Journal of Studies on Alcohol, 65(4), 409–418. 10.15288/jsa.2004.65.409 [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Hoyt D, Johnson K, & Chen X (2006). Mental disorders among parents/caretakers of american indian early adolescents in the northern midwest. Social Psychiatry and Psychiatric Epidemiology, 41(8), 632–640. 10.1007/s00127-006-0070-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitbeck LB, Yu M, Johnson KD, Hoyt DR, & Walls ML (2008). Diagnostic prevalence rates from early to mid-adolescence among indigenous adolescents: First results from a longitudinal study. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 890–900. 10.1097/CHI.0b013e3181799609 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitesell NR, Kaufman CE, Keane EM, Crow CB, Shangreau C, & Mitchell CM (2012). Patterns of substance use initiation among young adolescents in a northern plains american indian tribe. American Journal of Drug and Alcohol Abuse, 38(5), 383–388. 10.3109/00952990.2012.694525 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiechelt SA, Gryczynski J, Johnson JL, & Caldwell D (2012). Historical trauma among urban American Indians: Impact on substance abuse and family cohesion. Journal of Loss and Trauma, 17, 319–336. [Google Scholar]