

Abstract
The COVID-19 pandemic has brought new urgency to a longstanding problem: the US health system is not well-equipped to accommodate the country’s large limited English proficient (LEP) population in times of national emergency. We examined the landscape of Spanish-language COVID-19 website information compared to information in English provided by health departments of the top 10 cities by population in the USA. For each city, coders evaluated three score measures (amount of information, presentation quality, and ease of navigation) for six content types (general information, symptoms, testing, prevention, vaccines, and live statistics) across six delivery modes (print resources, website text, videos, external links, data visualization, and media toolkits). We then calculated a grand average, combining all cities’ values per score measure for each content type-delivery mode combination, to understand the landscape of Spanish-language information across the country. Overall, we found that, for all cities combined, nearly all content types and delivery modes in Spanish were inferior or non-existent compared to English resources. Our findings also showed much variability and spread concerning content type and delivery mode of information. Finally, our findings uncovered three main clusters of content type and delivery mode combinations for Spanish-language information, ranging from similar to worse, compared to information in English. Our findings suggest that COVID-19 information was not equivalently provided in Spanish, despite federal guidance regarding language access during times of national emergency. These results can inform ongoing and future emergency communication plans for Spanish-preferring LEP and other LEP populations in the USA.
Supplementary Information
The online version contains supplementary material available at 10.1007/s40615-022-01428-x.
Keywords: Hispanic/Latino populations, Limited English Proficiency, COVID-19, Health communication
Introduction
The COVID-19 pandemic has brought new urgency to a longstanding problem: the US health system is not well-equipped to accommodate the country’s large limited English proficient (LEP) population in times of emergency and national crisis. The US Census Bureau defines LEP individuals as those who both speak a language other than English at home and also speak English less than “very well” [1]. An estimated 25 million people in the USA were LEP as of 2019 [2]; the LEP population is diverse, with Census calculations capturing individuals who predominantly speak dozens of non-English languages [3]. Spanish-preferring LEP individuals make up the majority of the US LEP population, as nearly two-thirds of LEP individuals (approximately 16 million people) report they speak Spanish at home [2]. Research has begun to uncover how LEP populations across the USA have been disproportionately affected by the pandemic and that the risks resulting from a lack of equitable language access in the health system have only increased [4–6]. Compared to English proficient groups, LEP populations were found to have higher COVID-19 infection rates and lower access to COVID-19 testing [5]. In particular, Spanish-preferring LEP patients had one of the highest COVID-19 positivity rates compared to other LEP groups [5].
Other research so far has similarly found Spanish-preferring LEP populations in the USA were at higher risk of contracting COVID-19 and also for having worse outcomes. One study found Spanish-preferring survey respondents were more likely than English-preferring respondents to have had contact with someone diagnosed with COVID-19 [7]. This disparity seems to extend nationwide, as US counties with larger shares of monolingual Spanish-speakers had higher rates of COVID-19 cases [8]. Hospital systems have likewise reported higher COVID-19 positivity rates among their Spanish-preferring and other LEP populations [9] and that most Hispanic/Latino hospital patients admitted for COVID-19 were Spanish-preferring LEP [10]. As almost all Spanish-preferring LEP individuals in the USA identify as Hispanic/Latino [3], racial and ethnic COVID-19 outcomes data [8] help frame the potential magnitude of disparities among Spanish-preferring LEP communities. Compared to non-Hispanic White (NHW) persons, Hispanics/Latinos are 1.5 times more likely to contract COVID-19, 2.4 times more likely to be hospitalized, and 1.9 times more likely to die from COVID-19 [11]. The Hispanic/Latino population is also less likely to be vaccinated and thus less protected from severe COVID-19 illness than NHW: only 62% of Hispanics/Latinos received at least one dose of any available COVID-19 vaccines between March 1, 2021, and January 31, 2022 [12]. Thus, these inequities are likely even further exacerbated for the 28% of the Hispanic/Latino population with LEP [13].
Of critical and immediate importance during public health emergencies are actions to ensure the population has access to accurate information and, for LEP patients, to have access to this information in their preferred language. Federal guidance has been laid out for state and local health entities regarding language access during times of national emergency. The US Department of Justice (DOJ), which has the unique role and responsibility of coordinating language access across the federal government, has previously released guidance for language access specifically on pandemic preparedness [14]. This guidance includes how local entities who are required to provide meaningful access to receive federal funding should develop their own language access plans and disseminate information to their constituents in languages other than English. As noted in the National Security Council’s 2016 “pandemic playbook” [15], any such external communications are the responsibility of local health entities such as health departments. Despite a legal mandate for language access, a 2021 complaint [16] filed with several federal agencies suggested that such guidance related to COVID-19 information may not be adequately followed. The National Health Law Program’s analysis found that information about COVID-19 testing and vaccination was not being meaningfully provided under the law to LEP individuals, and local health departments relied instead on using internet webpages for communication, many of which had incomplete and inaccurate translations in other languages [16].
In addition to these administrative complaints, research has also begun to uncover the implications of inadequately following these language access policies. A previous study found that the provision of COVID-19 information in languages other than English on local health department websites was not equitable to information in the English language [17]. However, research is needed to better understand COVID-19 inequities related to language access specifically for the Spanish-preferring LEP population, to assist health departments in prioritizing critical information to a large proportion of their underserved constituents. Therefore, the purpose of this study was to examine the landscape of Spanish-language COVID-19 information provided by health department websites across the USA. Our results can inform ongoing and future emergency communication plans for LEP individuals in the USA.
Methods
To gather a representative picture of the communication of local health departments serving the largest number of constituents, we analyzed website content of local health departments of the top 10 cities by population in the USA (New York, New York; Los Angeles, California; Chicago, Illinois; Houston, Texas; Phoenix, Arizona; San Antonio, Texas; Philadelphia, Pennsylvania; San Diego, California; Dallas, Texas; San Jose, California). Sampling and analysis methods were published previously [17], and we encourage readers to review them for further detail and definitions.
Briefly, in those methods, each coder began on the same homepage for each city’s health department. Then coders were tasked to click around each site fully, following link to link in order to seek out all possible information available on each department’s entire website. To maintain records, one coder took screenshots of each webpage available and organized each screenshot according to each site’s layout. The same coder repeated this for all 10 cities.
Each coder rated information about six “content types” and six “delivery modes” [17]. The six content types included information on vaccines, testing, and prevention, among others [17]. The six “delivery modes” included videos, media toolkits, and links to other sites like the CDC) [17] among others. Finally, each coder rated these content types and delivery methods of the information in comparison to the information available in English with three score measures: “presentation quality,” “amount of information,” and “ease of navigability” [17]. There were three levels per score measure: better/more/easier, same/equal/same, and worse/less/harder. This resulted in one evaluation per coder for each possible three-part combination of content, delivery mode, and score measure. For example, a coder may be rating the presentation quality [one score measure] of vaccine information [one content type] available as a video [one delivery mode] in comparison to that same combination available in English. This nuanced analysis allowed coders to capture instances where a city may be simultaneously rated more highly in one score measure (e.g., amount of information) and less highly in another score measure (e.g., presentation quality). More details about these content types, delivery modes, and score measures can be found in the previously published methods [17]. Finally, as some of these scores can be subjective in nature as they reflect usability of the website, the previous study presents intercoder agreement processes and analyses using the Holsti method where four cities had high agreement (≥ 0.75) and six cities had lower levels of agreement (0.24–0.74) [17].
Whereas in the former study, several languages of the cities’ constituents were examined, in this study, we focused only on the Spanish language. This allowed us to conduct additional in-depth analyses into Spanish-language information to present an overall picture of COVID-19 information delivery in the second most spoken language in the USA. All analyses were performed in R, version 4.0.3 [18].
Spanish Language Scoring
In this study, the three score measures (i.e., amount of information, presentation quality, and ease of navigability) were evaluated across the six delivery modes (i.e., print resources, website text, videos, external links, data visualization, and media toolkits) for the six COVID-19 content types (i.e., general information, symptoms, testing, prevention, vaccines, and live statistics). The previously published methods describe the coding and scoring criteria, where each coder assigned a 0, 1, or 2 for each score measure of city-language-delivery mode-content type combination for languages other than English in comparison to English [17]. A score of 0 meant there was no Spanish (e.g., missing, or non-existent content) compared to English. A score of 1 meant less/lower/worse in Spanish than English but still present. A score of 2 meant similar/equal/better in Spanish to that in English. In the analysis, “better” was combined with “similar” due to substantially low counts of “better” in the data. Each of the 10 cities was coded by three coders.
Spanish Language Analysis
To assess the overall landscape of the Spanish-language resources on these websites, we averaged the scores of three coders to arrive at one numeric score (range 0–2) for each score measure-content type-delivery mode combination. An example of this would be one numeric value for the score measure “presentation quality” for Philadelphia for “general information” delivered by “media toolkits.” Holsti intercoder reliability of these scores were calculated and previously published [17]. Summarized ratings of all websites are also available and previously published [17]. These three score measures were then plotted in a three-dimensional scatterplot for each content type using the R package “scatterplot3d” [19]. We then calculated a grand average, combining all cities’ values per score measure for each content type-delivery mode combination. This resulted in one numeric value per content type-delivery mode combination, e.g., one grand average for the “amount of information” (score measure) about “general information” (content type) delivered by “toolkits” (delivery mode). These grand average score measures were plotted in a three-dimensional scatterplot combining content type and delivery mode. This grand average demonstrated which content type and delivery modes excelled across the nation in Spanish-language website information compared to English.
Results
Spanish Language Scoring
We found that, overall, content types and delivery modes of Spanish-language COVID-19 information were inferior or non-existent compared to those available in English for all 10 cities’ websites, combined. Summarized ratings for each separate city are previously published [17]. There were originally a total of 3240 scoring opportunities (10 cities × 3 coders/city × 3 score measures × 6 content types × 6 delivery modes). However, our study had 3132 final scoring opportunities as one coder was unable to code Dallas (3240 – [1 coder × 3 score measures × 6 content types × 6 delivery modes] = 3132).
There was variability in the information available in Spanish compared to English. There were several instances where Spanish-language information was non-existent compared to information available in English (1335/3132). This means information in Spanish was not available in 41.3% of instances compared to available information in English. Only 0.2% of total scoring opportunities for Spanish-language information (7/3132) were rated as better/more/easier for presentation quality, more information, or ease of navigation, compared to information in English. These seven instances comparing Spanish-language information to available English-language information are as follows: two coders of Phoenix rated the score measures “presentation quality” and “amount of information” to be “better” and “more,” respectively, for testing information delivered by video (4 instances total); one coder of Phoenix rated the score measure “ease of navigability” to be easier for testing information delivered by video (1 instance total); one coder of San Jose rated the “amount of information” to be “more” for prevention information delivered by text on the webpage and for prevention information delivered by external links (2 instances total).
Spanish Language Analysis
There was also variability and spread in the score measures by content type and delivery mode of that information, for Spanish compared to English. Appendix Tables 1–6 correspond to each of the six content types and present the average of the three coders’ scores (range 0–2) for each score measure by city and delivery mode. In these tables, variability is shown by the differences in scores found per score measure and per delivery mode. Spread can be seen by looking at the presence of both high and low scores per delivery mode (i.e., row) and per score measure (i.e., column). For example, in Appendix Table 1: General Information, in Los Angeles, whereas print resources scored highly across all three score measures (2, 2, 2 for amount of information, presentation quality, and ease of navigability, respectively), videos scored low across all three measures (0, 0, 0). Appendix Tables 7–12, corresponding to each of the six content types, present the grand average of all cities for each score measure by delivery mode. In these tables, each score represents the grand average of 30 data points (three coders per city × 10 cities). Figure 1 depicts the grand average data from all 10 cities as a three-dimensional scatterplot where the three axes correspond to each of the three score measures. The colors represent the six content types, and the shapes represent the six delivery modes. This results in 36 total points on the graph (i.e., six content types by six delivery modes) representing all cities’ scores averaged together.
Fig. 1.
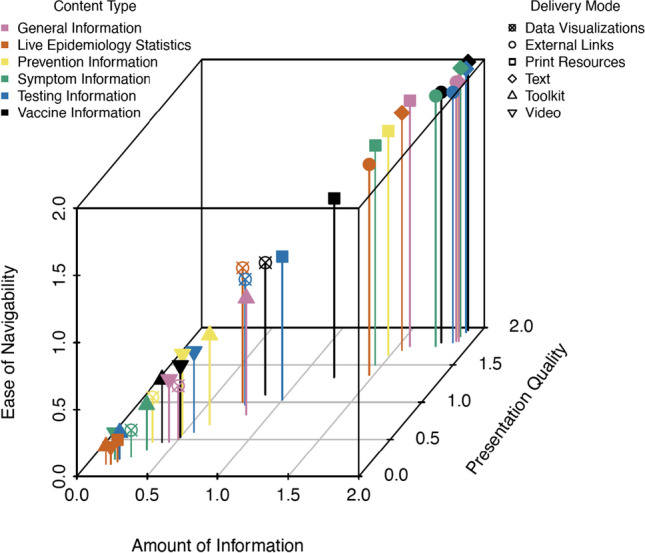
The grand average (all coders, all cities) of all three score measures (amount of information, ease of navigability, presentation quality) by content type and delivery mode for Spanish-language COVID-19 information of the websites of the local health departments of the top 10 cities by population in the USA, March 2021
As shown in Fig. 1, we found three main clusters of certain content types and delivery modes in Spanish present in the data based on scoring compared to English. The cluster at the top right of Fig. 1 indicates similarly scoring measures in Spanish compared to available information in English. For example, these measures included content types such as symptom, vaccine, and testing information and corresponded to the delivery modes of external links and text on the webpage. The cluster in the center of Fig. 1 corresponds to score measures that were worse in Spanish than in English. Some of these included data visualizations of vaccine and testing information, as well as live epidemiology statistics. Finally, the cluster at the bottom left of Fig. 1 indicates non-existent information in Spanish compared to English. These included toolkits and videos for nearly all content types, as well as data visualizations for general information, prevention information, and symptom information about COVID-19.
Discussion
This study is one of the first to evaluate the equivalence of COVID-19 information delivered in Spanish compared to English by local public health entities. Our aim was to examine the landscape of Spanish-language COVID-19 website information provided on health departments of the top 10 cities by population in the USA. To do so, we analyzed the amount of COVID-19 information provided, presentation quality, and ease of navigability of the websites across six types of content (general information, symptoms, testing, prevention, vaccines, live statistics) and in six delivery modes (printable resources, webpage text, media toolkits, videos, external links, data visualization). Overall, we found that most Spanish COVID-19 information with regard to content type and delivery mode were worse or non-existent compared to the same information provided in English. Specifically, we found variability and spread by content type and delivery mode of Spanish-language information compared to English. Finally, we found clusters of content type-delivery mode combinations for Spanish-language information compared to English. Our results provide further empirical evidence to support previous literature suggesting COVID-19 information has not been equitably delivered in languages other than English [17, 20, 21]. These findings also highlight how urgent action is needed to improve the quality of COVID-19 information provided to the already underserved Spanish-preferring LEP population across the USA.
First, we found that local health department websites overall did not provide equivalent COVID-19 information in Spanish compared to English in terms of content type or delivery mode. These results are concerning, given the large population of Spanish-preferring LEP individuals across the USA and the disproportionate vulnerability of this population to COVID-19. Hispanics/Latinos are overrepresented in occupations where they are more likely to be exposed to SARS-CoV-2 due to an inability to work remotely [22], such as in the service and agricultural industries [23], and overall, this population has also experienced significant financial hardship as a result of the pandemic [24]. Additionally, further barriers to seeking COVID-19 information have been noted for the Hispanic/Latino immigrant population, many of whom are LEP and live in areas impacted by social determinants that increase their COVID-19 vulnerability [25]. Such barriers may also include concerns about eligibility for testing, vaccination, and treatment due to immigration status, as well as the release of personal information to immigration officials and the ramifications of using health services as related to the public charge rule [26]. These factors, together with the observed communication inadequacies of Spanish-language COVID-19 information found in our study, highlight the necessity of addressing such inequities in language access related to COVID-19. Further research is needed to expand upon these findings, as this study only presents a preliminary investigation into the Spanish-language provision of COVID-19 information around the USA. For example, a broader scope of information content should be examined, such as additional cities, government entities at various levels, and other sources of information such as mass media channels, social media, or offline social networks. This will help to understand the breadth and depth of information available for the Spanish-preferring LEP population.
Next, in this study, we found variability and spread in both the Spanish-language COVID-19 content type (i.e., colors in Fig. 1) and the delivery mode of this information (i.e., shapes in Fig. 1) compared to English on local health department websites. Through pinpointing this gap in health department communication, our findings highlight the need to increase the availability of all types of COVID-19-related content, not just textual information or links to external resources, in a variety of formats on health department websites. This finding is especially concerning given that, in the current climate of widespread misinformation and mistrust, timely information from credible sources is essential to mitigate the negative health consequences of misinformation about COVID-19 [27]. Recent research found that a majority of Spanish-preferring LEP individuals expressed difficulty finding trusted COVID-19 information as well as Spanish language COVID-19 information, while a minority of Spanish-preferring LEP respondents viewed local public health entities and the CDC as trusted sources for COVID-19 communication [28]. Providing culturally and linguistically concordant COVID-19 information and outreach is an important step toward rebuilding trust in local health entities among Spanish-preferring LEP populations [28]. Spanish-preferring LEP individuals also reported receiving COVID-19 news mostly from television and radio, particularly from Spanish-language programming, as well as from social media [28], suggesting these sources may be effective messaging modes for health entities to reach these communities in addition to internet webpages. Our research provides further evidence that, though providing access to information in one’s preferred language is a legal obligation for health entities that receive federal funding [29], there is variability in how these laws continue to be interpreted and implemented [30–32], including at the local level. It is imperative that local health entities go further than simply meeting the minimum level of requirements for providing meaningful language access and instead aim to deliver high quality, diversified, and accessible Spanish-language COVID-19 information, tailored to the needs of their constituents. Future research using qualitative and community-based participatory methods are needed to explore the experiences of LEP populations with accessing COVID-19 information via different modes from health entities at multiple levels.
Finally, our findings uncovered three main clusters of content type and delivery mode combinations for Spanish-language information, ranging from similar to worse, compared to information in English. The only resources that we found to be equivalent in Spanish and English were webpage text and external links across various content types, likely because website text and links are the most easily (and cost-effectively) translated using automated translation software such as Google Translate. However, as found in previous analyses [16, 17], relying solely on these types of automatic page translators can result in incomplete and inaccurate translations. Together, these findings underscore the need to not only provide quality information, but also to focus on the manner in which information is delivered. Importantly, equitable access to COVID-19 information hinges not only on language access but also on content variety, format, and technological accessibility. Previous research has demonstrated that the format and design of healthcare providers’ informational and educational materials influence their accessibility and usability [33, 34]. For example, optimizing the design and formatting of the materials to match the audience’s needs and expectations can be a low-cost intervention that can increase the uptake of evidence in healthcare [34]. Specifically, making content more vivid, intuitive, and visual is a practical strategy to influence the usability of public health guidelines. This is especially effective to ease the cognitive load and facilitate information processing among English-speakers with lower literacy skills by using non-textual features such as graphic and visual elements [34, 35]. To identify best practices for effectively informing the LEP population regarding COVID-19 and increasing uptake of health guidelines, future research should explore LEP populations’ patterns of media use and preferred modes and channels of communication. While many people can understand and process information in all modes of communication, some may depend more heavily on a particular mode [35]. Further, more empirical studies are needed to understand the parameters of cultural, educational, literacy, and linguistical appropriateness of COVID-19-related messages.
Recommendations
There are several practical steps local health departments can take to address the gaps highlighted in this study to provide more equitable language access in emergency settings. Of the highest importance, all health entities, including health departments, and healthcare organizations such as hospitals and hospital systems, should formulate more robust crisis language access strategies that are tailored to the specific needs of the communities they serve [36]. Critically, all entities’ pandemic response and preparedness plans at every level of government should outline detailed strategies for the translation and delivery of pandemic-related information in languages other than English via multiple delivery modes and channels (e.g., webpages, social media, radio, TV, print resources and printed materials, stand-up banners, wall signs, billboards, text messages, phone calls). For populations with lower literacy levels in their preferred language, videos and other visual resources such as pictorial infographics can be particularly effective messaging tools [37]. The mixture of delivery formats and channels helps ensure vertical and horizontal communication integration where messages are disseminated not only through a centralized government response but also through public and community entities [38].
Next, local health departments should earmark funding for quality translation of information using professional translation services as a part of pandemic preparedness and/or emergency fund allocation. Importantly, automated translation software such as Google Translate should only be used on webpages and other resources when such translations are also checked for accuracy by a certified medical translator [16]. These professional translators can be hired on staff or hired as needed for their services through translation companies. Related, public health entities should also utilize a portion of this funding to build a representative workforce. Specifically, governmental communication teams at all levels should be staffed with multi- or bilingual employees to center the linguistic and cultural needs of the communities they serve [39]. These teams should be tasked with evaluating and improving the efficacy of their public health messaging, in conjunction with community liaisons, communication experts, and professional translators.
Finally, given the continually changing nature of available information about COVID-19 testing, vaccination, and treatment, health departments should regularly evaluate information delivery in languages other than English to assess quality assurance of translations, messaging efficacy, and relevance to the populations being served. Communication strategies are most effective when planned from the perspective of the target population. These strategies should involve messages that are sensitive and relevant to the audience and delivered in a format that considers visual appeal as well as linguistic and educational appropriateness [40]. For example, children of immigrants are often the primary drivers of cultural adjustment, so communication strategies addressing this segment of the LEP population are especially important [40]. One study found that providing materials in “Spanglish” as well as in Spanish and English may appeal to people across different age groups [41]. Thus, the provision of meaningful language access requires local entities to evaluate and understand the diverse needs of their constituents and to tailor messaging in a culturally and linguistically appropriate manner. This further requires COVID-19 communication with LEP individuals to be more intentional in crafting messages, determining delivery modes, and choosing communication channels.
Limitations
Our study methodology has some limitations. Although not all coders were proficient in Spanish, the scope and purpose of this study was not to understand the Spanish resources, only to identify the presence of the resources compared to those available in English. Just as we did not assess the accuracy, quality, completeness, and cultural appropriateness of information in English, we also did not analyze those in Spanish. Future research must involve certified medical translators and fully bilingual community users of various demographics to assess those components. Additionally, though multiple coders were involved, the data gathered was subjective and based on coders’ determination of scoring measures, content types, and delivery modes. Finally, this study was meant to be a representative, not exhaustive, analysis of the local health departments in the USA serving the largest number of constituents. Although Spanish is a top language spoken in the largest 10 US cities by population, this is not necessarily indicative of the percentage of Spanish-preferring LEP individuals in each of those cities or in comparison to other cities around the country. Future research should aim to conduct more exhaustive analyses of other health departments, as well as evaluate how COVID-19 website communication may change over time as the pandemic continues. Despite these limitations, our study provides some of the first empirical evidence around the provision of Spanish-language, COVID-19-related information by local health departments.
Conclusion
Our findings suggest that COVID-19 information was not equivalently provided in Spanish on health department websites of the top 10 US cities by population. In fact, certain content types and delivery modes used in English were missing entirely in Spanish. It is necessary to provide not only equivalent information in Spanish, the most commonly spoken language among limited English proficient individuals in the USA, but also information in equivalent delivery modes. These results underscore a pressing issue: a system that does not account for the diversity in the population it serves will exacerbate disparities and increase risks to public safety during large-scale public health emergencies, such as the COVID-19 pandemic. Local government entities must ensure equitable information access across content types and delivery modes for all constituents, especially the most vulnerable, such as those with limited English proficiency.
Supplementary Information
Below is the link to the electronic supplementary material.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Source and methodology. 2020; Available from: https://www.lep.gov/source-and-methodology.
- 2.State immigration data profiles: language & education. Migration Policy Institute.
- 3.2019: ACS 5-year estimates detailed tables, in American Community Survey, U.S.C. Bureau, Editor. 2019.
- 4.Kucirek NK, et al. Stories from COVID-19 reveal hospitalized patients with limited English proficiency have always been uniquely prone to social isolation. J Gen Intern Med. 2021;36(3):786–789. doi: 10.1007/s11606-020-06383-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim HN, et al. Assessment of disparities in COVID-19 testing and infection across language groups in Seattle Washington. JAMA network Open. 2020;3(9):e2021213–e2021213. doi: 10.1001/jamanetworkopen.2020.21213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Himmelstein J, et al. COVID-19–related care for Hispanic elderly adults with limited English proficiency. Ann Intern Med. 2022;175(1):143–145. doi: 10.7326/M21-2900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mehring WM, et al. COVID-19 exposure risk by speakers of Spanish and English using a web-based self-assessment tool. J Gen Intern Med. 2021;36(6):1835–1836. doi: 10.1007/s11606-021-06756-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rodriguez-Diaz CE, et al. Risk for COVID-19 infection and death among Latinos in the United States: examining heterogeneity in transmission dynamics. Ann Epidemiol. 2020;52:46–53.e2. doi: 10.1016/j.annepidem.2020.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wilkins CH, et al. A systems approach to addressing COVID-19 health inequities. NEJM Catalyst Innovations in Care Delivery, 2021; 2(1).
- 10.Alvarez-Arango S, et al. Juntos: a model for language congruent care to better serve Spanish-speaking patients with COVID-19. Health Equity. 2021;5(1):826–833. doi: 10.1089/heq.2020.0124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Prevention, C.f.D.C.a. Risk for COVID-19 infection, hospitalization, and death By race/ethnicity. 2022 [cited 2022 February 1]; Available from: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html.
- 12.Ndugga, N.H., Latoya; Artiga, Samantha; Haldar, Sweta. Latest Data on COVID-19 Vaccinations by Race/Ethnicity. 2022 [cited 2022 February 7]; Available from: https://www.kff.org/coronavirus-covid-19/issue-brief/latest-data-on-covid-19-vaccinations-by-race-ethnicity/.
- 13.Jens Manuel Krogstad LN-B, Key facts about U.S. Latinos for National Hispanic Heritage Month. 2021, Pew Research Center.
- 14.Tips and tools for reaching limited English proficient communities in emergency preparedness, response, and recovery, C.R.D. Federal Coordination and Compliance Section, U.S. Department of Justice, Editor. 2016. Available from: https://www.justice.gov/crt/file/885391/download
- 15.Knight V, Evidence shows obama team left a pandemic ‘game plan’ for trump administration, in KHN & PolitiFact HealthCheck. 2020, Kaiser Health News.
- 16.Discriminatory provision of COVID-19 services to persons with limited English proficiency. 2021, National Health Law Program.
- 17.Kusters IS, Dean JM, Gutierrez AM, Sommer M, Klyueva A. Assessment of COVID-19 website communication in languages other than english by local health departments in the United States. Health Commun. 2021;31:1–11. [DOI] [PubMed]
- 18.R Core Team, R: A language and environment for statistical computing. 2020, R Foundation for Statistical Computing: Vienna, Austria.
- 19.Ligges U, Maechler M. scatterplot3d - an R package for visualizing multivariate data. J Stat Softw. 2003;8(11):1–20. doi: 10.18637/jss.v008.i11. [DOI] [Google Scholar]
- 20.David Velasquez NU, Numa Perez, Equitable access to health information for non-English speakers amidst the novel coronavirus pandemic. 2020, Health Affairs Blog.
- 21.Goldberg E, When coronavirus care gets lost in translation, in The New York Times. 2020: New York, NY.
- 22.Asfaw A, Racial disparity in potential occupational exposure to COVID-19. Journal of racial and ethnic health disparities, 2021: 1–14. [DOI] [PMC free article] [PubMed]
- 23.Chicas R, et al. COVID-19 and agricultural workers: a descriptive study. J Immigr Minor Health. 2022;24(1):58–64. doi: 10.1007/s10903-021-01290-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Luis Noe-Bustamante JMK, Mark Hugo Lopez, For U.S. Latinos, COVID-19 has taken a personal and financial toll. 2021, Pew Research Center.
- 25.Vilar-Compte M, et al. Pre-COVID-19 social determinants of health among Mexican migrants in Los Angeles and New York city and their increased vulnerability to unfavorable health outcomes during the COVID-19 pandemic. J Immigr Minor Health. 2022;24(1):65–77. doi: 10.1007/s10903-021-01283-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lechuga J, et al., Latinx immigrants’ legal concerns about SARS-CoV-2 testing and COVID-19 diagnosis and treatment. Journal of Immigrant and Minority Health, 2022: 1–9. [DOI] [PMC free article] [PubMed]
- 27.Mohammed M, et al. Assessment of COVID-19 information overload among the general public. J Racial Ethn Health Disparities. 2022;9(1):184–192. doi: 10.1007/s40615-020-00942-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.SteelFisher GK, et al. Getting critical information during the COVID-19 pandemic: experiences of Spanish and Chinese speakers with limited english proficiency. Health security, 2022. [DOI] [PubMed]
- 29.Frequently asked questions on legal requirements to provide language access services. [cited 2022 August 17].
- 30.Chen AH, Youdelman MK, Brooks J. The legal framework for language access in healthcare settings: title VI and beyond. J Gen Intern Med. 2007;22(2):362–367. doi: 10.1007/s11606-007-0366-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.National Standards for Culturally and Linguistically Appropriate Services in Health Care, O.o.M.H. U.S. Department of Health & Human Services, Editor. 2001. [PubMed]
- 32.The Department of Health and Human Services: Language Access Plan, U.S.D.o.H.H. Services, Editor. 2013.
- 33.Lurie NH, Mason CH. Visual representation: Implications for decision making. J Mark. 2007;71(1):160–177. doi: 10.1509/jmkg.71.1.160. [DOI] [Google Scholar]
- 34.Versloot J, et al. Format guidelines to make them vivid, intuitive, and visual: use simple formatting rules to optimize usability and accessibility of clinical practice guidelines. Int J Evid Based Healthc. 2015;13(2):52–57. doi: 10.1097/XEB.0000000000000036. [DOI] [PubMed] [Google Scholar]
- 35.King SR, McCaffrey DJ, Bouldin AS. Health literacy in the pharmacy setting: defining pharmacotherapy literacy. Pharmacy Practice. 2011;9(4):213. doi: 10.4321/S1886-36552011000400006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ensuring Civil Rights During the COVID-19 Response, U.S.D.o.H. Security, Editor. 2020.
- 37.Mbanda N, et al. A scoping review of the use of visual aids in health education materials for persons with low-literacy levels. Patient Educ Couns. 2021;104(5):998–1017. doi: 10.1016/j.pec.2020.11.034. [DOI] [PubMed] [Google Scholar]
- 38.Choi S, Powers TL. COVID-19: Lessons from South Korean pandemic communications strategy. Int J Healthcare Manag. 2021;14(1):271–279. doi: 10.1080/20479700.2020.1862997. [DOI] [Google Scholar]
- 39.Goode T, et al. 2010 Cultural and linguistic competence family organization assessment instrument. National Center for Cultural Competence, Georgetown University Center for Child and Human Development: Washington, DC
- 40.Vaughan E, Tinker T. Effective health risk communication about pandemic influenza for vulnerable populations. Am J Public Health. 2009;99(S2):S324–S332. doi: 10.2105/AJPH.2009.162537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kerrigan D, et al. Context and considerations for the development of community-informed health communication messaging to support equitable uptake of COVID-19 vaccines among communities of color in Washington, DC. Journal of Racial and Ethnic Health Disparities, 2022: 1–15. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.