

Abstract
Background:
Focal dermal hypoplasia is a genetic disease of multiple systems initially affecting the skin, skeleton, dental, eyes and face with developmental abnormalities and facial dysmorphism. Focal dermal hypoplasia is X-linked dominant disease affecting the ectoderm, mesoderm and endoderm. 95% feature de novo and 90% of these are females. Focal dermal hypoplasia is induced by a mutation in the PORCN gene.
Objective:
The aim of this article is to present a case of a one-year-old girl child with multi-hypopigmented reticulated atrophic macules and patches grouped in linear mode at the lines of blaschko, skeleton abnormalities, umbilical hernia, developmental delay, hypoplastic nails, syndactyly and lobster claw deformity.
Case report:
A one-year-old girl child presented to the dermatology clinic with asymptomatic lesions since childhood with no improvement, with multi- hypopigmented skin lesions on the trunk and extremities since birth as linear erosions that heal gradually during few days, leaving peripheral hypopigmentation with hyperpigmentation with anomalies of limbs and nails and delayed development. She was born by normal vaginal delivery and weighed 2.5 kg at birth. None of the family members had such features. She had dental enamel anomaly and partial anodontia in the lower jaw. Sparse hair and partial alopecia (scalp, eyebrows and eyelashes) were recorded.
Conclusion:
Focal dermal hypoplasia is a congenital skin disease with a unique clinical feature. Thorough examination of the extremities is indicated for early proper genetic counseling and therapy.
Keywords: Focal dermal hypoplasia, osteopathia striata
1. BACKGROUND
Focal dermal hypoplasia is a mesoectodermal disease with X-linked dominant gene, fatal in homozygous males. Focal dermal hypoplasia was presented initially as atrophoderma linearis maculosa and papillomatosis congenitalis (1) by Liebermann in 1935.It is induced by fresh mutations in the PORCN gene, encoding a protein that organizes Wnt signaling. It is featured by vermiculate dermal atrophy, swellings of fat, telangiectasias and hypopigmentation. Periorificial raspberry-like papillomas, dystrophic nails, sparse hair, pathological teeth, split hand/foot (“lobster claw”), ocular anomalies (e.g., microphthalmia), and the radiological osteopathia striata in long bones. This disease should be differentiated from Microphthalmia with linear skin defects, Incontinentia pigmenti, TP63-related disorders, Oculocerebrocutaneous syndrome and Rothmund-Thomson syndrome.
2. OBJECTIVE
The aim of this article is to present a case of a one-year-old girl child with multi-hypopigmented reticulated atrophic macules and patches grouped in linear mode at the lines of blaschko, skeleton abnormalities, umbilical hernia, developmental delay, hypoplastic nails, syndactyly and lobster claw deformity.
3. CASE REPORT
A one-year-old girl child presented to the Dermatology clinic with asymptomatic lesions since childhood with no improvement, with multi- hypopigmented skin lesions on the trunk and extremities since birth as linear erosions that heal gradually during few days, leaving peripheral hypopigmentation with hyperpigmentation with anomalies of limbs and nails and delayed development (Figure 1).
Figure 1. Skin lesions in focal dermal hypoplasia.

She was born by normal vaginal delivery and weighed 2.5 kg at birth. None of the family members had such features. She had dental enamel anomaly and partial anodontia in the lower jaw. Sparse hair and partial alopecia (scalp, eyebrows and eyelashes) were recorded. General examination featured microcephaly, hypertelorism, megalopinna, low-set ears, a broad nasal bridge and a pointed chin. Multi-hypopigmented atrophic linear streaks with variable macules were on the forehead, neck, trunk, thighs, gluteal region, genitalia and upper and lower limbs at the lines of blaschko. Syndactyly of left foot and lobster claw deformity (ectrodactyly) of right foot were present (Figure 2). Skin-colored growths were on the proximal nail fold of the right middle finger and right foot. Nails were dystrophic. There was alopecia (scalp, eyebrow and eyelashes). Her teeth were malformed with hypodontia and missing upper laterals. Skin demonstrated hypopigmented atrophic macules and patches in a linear mode over the lines of Blaschko on the face, trunk and the arm with facial asymmetry. There were multi- skin color papules over the nose. Multi- patchy areas of cicatricial alopecia were noted over the scalp.
Figure 2. Lobster claw.

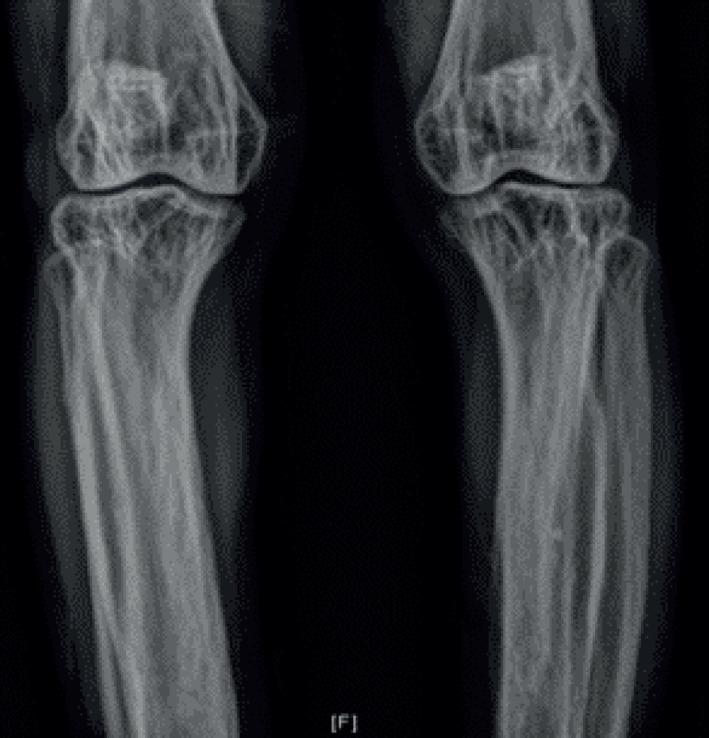
Complete blood count and chemistry were normal. Skin biopsy on the trunk demonstrated focal spongiosis, dyskeratotic keratinocytes, mild papillary edema and focal papillary dermal fibrosis with superficial perivascular lymphocytic infiltrate. Skin biopsy found remarkable dermal atrophy with thin collagen fibers of with Focal dermal hypoplasia. Ophthalmological examination and computed tomography scan of brain were normal. The clinical features and histopathological confirmation made the diagnosis. X-rays of long bones demonstrated the specific ‘osteopathia striata’ (longitudinal striations in metaphysis of long bones) (Figure 3). X-rays of hands and feet found hypoplastic metacarpals. Chest X-ray detected absence of the left first rib.
Figure 3. Osteopathia striata.
4. DISCUSSION
Focal dermal hypoplasia is an inherited severe disease with developmental defects of the skin and ocular, dental with skeletal anomalies. It affects tissues of ectomesodermal origin. Out of 90% are females with male fatality in utero because of X-chromosome mosaicism in males due to gametic half-chromatid mutation or postzygotic somatic mutation, with X-linked dominant inheritance (2). It is a mosaic state in males. The intensity variability in females is induced by the mosaicism of the Lyon hypothesis (3). Mosaicism for mutations in the PORCN gene on chromosome Xp11.23 was involved in Focal dermal hypoplasia.
The distribution mode states that Wnt proteins activate epidermal-dermal signals to modify the dermis (4). There were 6 reports of father-to-daughter transmission, the fathers having a milder phenotype. It is a developmental defect with mosaic involved tissues, due to a block of Wnt signal transmission from cells carrying a detrimental PORCN mutation on their active X-chromosome.
Focal dermal hypoplasia is characterized by thinning of the dermis, causing depressed linear lesions and soft, reddish-yellow swellings of the skin induced by herniation of subcutaneous fat. At birth, the lesions appear as blisters or erosions causing typical atrophic scars like incontinentia pigmenti. Red, hypopigmented or depigmented atrophic macules, grouped in a linear, blaschkoid or in a reticulate mode affect mostly the thighs, buttocks and trunk. Telangiectasias are intercalated between the atrophic plaques. Multi- soft pinkish yellow and brown nodules are seen at birth in the popliteal and cubital fossae. Raspberry-like papillomas around the lips, anus, genitalia and on the end of the digits could be found. Skin dryness with pruritus, photosensitivity, hyperkeratosis of palms and soles, sweating anomalies and dermatoglyphic modifications are seen (5).
Skin features are congenital patchy skin aplasia (95%) with atrophic and hypoplastic regions of the skin on the lines of Blaschko as depressed areas of pink or white color with a fibrous texture. Congenital skin hypo- or hyperpigmentation (90–100%) at Blaschko linear order. Congenital nodular fat herniation (60–70%) with soft, yellow-pink nodules on the skin (fat nodules in the dermis) and on the trunk and extremities. Telangiectasias (80%) on the face, trunk and extremities, verrucoid papillomas (65%) of the skin and mucous membranes, pebbled skin texture (58%) and photosensitivity (40%). Hair features are patchy alopecia of the scalp (80%) and hair shaft anomalies (80–90%). Nail anomalies are congenital ridged, dysplastic, or hypoplastic nails (80–90%).
Skeletal defects are found in 60-70% as the second frequent extracutaneous anomlay, including syndactyly, polydactyly, ectrodactyly, hypoplasia of the digits and vertebral anomalies as scoliosis, kyphosis, vertebral body fusions and spina bifida. Lobster claw deformity (split hand or split foot) is a crucial differential aspect of this disease (5). In 20%, osteopathia striata is present as longitudinal linear striations in the metaphyses of the long bones seen on x-ray. Eye anomalies are colobomas, microphthalmia, microcornea and ectopia lentis (5). Typical facial aspect with asymmetry, pointed chin, maxillary hypoplasia, broad nasal tip with a narrow bridge and notching of alae nasi is commonly present. Enamel defects, sparse and brittle hair, nail dystrophy, short stature, mental retardation, hearing loss, microcephaly, cleft lip and palate, duodenal atresia, intestinal malrotation, umbilical, inguinal, epigastric, or diaphragmatic hernia, horseshoe kidneys, bicornuate uterus and cardiac defects like patent ductus arteriosus, ventricular septal defect, and hypoplasia of lungs could be found. Absent nipples are recorded in literature (6). Skeletal anomalies are syndactyly (70–90%), ectrodactyly (75%), long bone reduction defect (50–80%), oligodactyly (20–40%) of central digits, and transverse limb defect (15%). Enamel hypoplasia exposing dental caries is the most frequent issue.
Others are: hypodontia, oligodontia, supernumerary teeth, and dental crowding with malocclusion of both primary and secondary dentition; vertical grooving of the teeth; microdontia, taurodontia, and abnormal root morphology.
Skin biopsy of an atrophic lesion demonstrated a normal or thinned epidermis over an intensely hypoplastic dermis with adipose tissue on the epidermis. Loosely grouped pathological scattered collagen bundles are seen (7). The main frequent differential confirmation for Focal dermal hypoplasia is incontinentia pigmenti, Rothmund-Thomson syndrome and MIDAS (MIDAS: Microphthalmia, dermal aplasia and sclerocornea syndrome). The linear mode, of pigmentary modifications, eosinophilic spongiosis and no fat herniation exclude incontinentia pigmenti.
Other differential confirmations are epidermal nevus, Bart syndrome, Adams-Oliver syndrome, ectodermal dysplasia and congenital erosive and vesicular dermatoses (8). There is no efficient therapy. Patients have a normal life span. Ocular features are: chorioretinal colobomas (60%), iris colobomas (50%), microphthalmia (45%), nystagmus (30%), strabismus (20%), cataracts (10%), and anophthalmos (5–10%) (9). Occasional hearing defects, microcephaly, horseshoe kidneys, umbilical, inguinal, epigastric, or diaphragmatic hernias, cardiac tumors can be found. 15% of diseased have mild intellectual disability. Skin with skeletal anomalies strengthen the clinical confirmation of Focal dermal hypoplasia. In our case, the child experienced typical aspect of Focal dermal hypoplasia. Musculoskeletal anomalies were reported in 70% and ocular with nail anomalies were reported in 30%. Asymmetric involvement of the hands and feet in 60% and. Scoliosis occurs in 20% (Table I).
Table I. Incidence of anomalies in literature.
| Anomalie | % |
|---|---|
| Skin features | |
| Congenital patchy skin aplasia | 95 |
| Congenital skin hypo- or hyperpigmentation | 90-100 |
| Congenital nodular fat herniation | 60-70 |
| Telangiectasias | 80 |
| verrucoid papillomas | 65 |
| pebbled skin texture | 58 |
| photosensitivity | 40 |
| Hair features | |
| patchy alopecia of the scalp | 80 |
| Hair shaft anomalies | 80-90 |
| Nails | |
| hypoplastic nails | 80-90 |
| Musculoskeletal anomalies | 70 |
| Skeletal defects | 60-70 |
| osteopathia striata | 20 |
| syndactyly , | 70-90 |
| ectrodactyly | 75 |
| Long bone reduction defect | 50-80 |
| long oligodactyly of central digits | 20-40 |
| transverse limb defect | 15 |
| Asymmetric involvement of the hands and feet | 60 |
| Scoliosis occurs | 20 |
| Ocular | |
| Ocular chorioretinal colobomas | 60 |
| iris colobomas | 50 |
| microphthalmia | 45 |
| nystagmus | 30 |
| strabismus | 20 |
| cataracts | 10 |
| anophthalmos | 5-10 |
| ocular with nail anomalies | 30 |
5. CONCLUSION
Focal dermal hypoplasia is a congenital skin disease with a unique clinical features. The specific features include atrophic linear hypo or hyperpigmented patches, fat herniation via dermal defects, and multiple papillomas of the mucous membranes or skin. Recently, the gene is located at the Xp terminal region (10). Thorough examination of the extremities is indicated for early proper genetic counseling and therapy.
Authors contribution:
All authors were involved in a designed research concept, prepared, and drafted a manuscript. Final proofreading was made by the first author.
Conflict of interest:
There is no conflict of interest.
Financial support and sponsorship:
None.
REFERENCES
- 1.Sahana MS, Ravi H. Focal Dermal Hypoplasia: A Rare Case Report. Indian J Dermatol. 2015;60(1):106. doi: 10.4103/0019-5154.147876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Giam YC, Khoo BP. What syndrome is this? Focal dermal hypoplasia (Goltz syndrome) Pediatr Dermatol. 1998;15:399–402. doi: 10.1046/j.1525-1470.1998.1998015399.x. [DOI] [PubMed] [Google Scholar]
- 3.Mahé A, Couturier J, Mathé C, et al. Minimal focal dermal hypoplasia in a man: a case of father to daughter transmission. J Am Acad Dermatol. 1991;25:879–881. doi: 10.1016/0190-9622(91)70274-6. [DOI] [PubMed] [Google Scholar]
- 4.Paller AS. Wnt signalling of focal dermal hypoplasia. Nat Genet. 2007;39:820–821. doi: 10.1038/ng0707-820. [DOI] [PubMed] [Google Scholar]
- 5.Temple IK, MacDowall P, Baraitser M, et al. Focal dermal hypoplasia (Goltz syndrome) J Med Genet. 1990;27:180–187. doi: 10.1136/jmg.27.3.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Riyaz N, Riyaz A, Chandran R, et al. Focal dermal hypoplasia (Goltz syndrome) Indian J Dermatol Venereol Leprol. 2005;71:279–281. doi: 10.4103/0378-6323.16624. [DOI] [PubMed] [Google Scholar]
- 7.Del Carmen Boente M, Asial RA, Winik BC. Focal dermal hypoplasia: Ultrastructural abnormalities of the connective tissue. J Cutan Pathol. 2007;34:181–187. doi: 10.1111/j.1600-0560.2006.00589.x. [DOI] [PubMed] [Google Scholar]
- 8.Jain A, Chander R, Garg T, et al. A rare multisystem disorder: Goltz syndrome-case report and brief overview. Dermatol Online J. 2010;16:2. [PubMed] [Google Scholar]
- 9.Alsharif SA, Hindi SB, Khoja F. Unilateral Focal Dermal Hypoplasia (Goltz Syndrome): Case Report and Literature Review. Case Rep Dermatol. 2018;10:101–109. doi: 10.1159/000488521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Najeeba R, Riyaz A, Rajesh C, et al. Focal dermal hypoplasia (Goltz syndrome) Focal dermal hypoplasia (Goltz syndrome) Indian J Dermatol Venereol Leprol. 2005;71(4):279–281. doi: 10.4103/0378-6323.16624. [DOI] [PubMed] [Google Scholar]