

Abstract
Introduction:
Clinical research focused on aging, Alzheimer’s disease and related dementias (ADRD), and caregiving often does not recruit Asian Americans and Pacific Islanders (AAPIs).
Methods:
With funding from the National Institute on Aging, we designed and launched the Collaborative Approach for AAPIs Research and Education (CARE), a research recruitment registry to increase AAPIs’ participation in ADRD, aging, and caregiving research. We present the design of this novel recruitment program.
Results:
CARE uses community-based participatory research methods that are culturally and linguistically appropriate. Since CARE’s launch, it has enrolled >7000 AAPIs in a 1-year period. The majority enrolled in CARE via community organizations and reported never having participated in any kind of research before. CARE also engages researchers by establishing a recruitment referral request protocol.
Discussion:
CARE provides a promising venue to foster meaningful inclusion of AAPIs who are under-represented in aging and dementia-related research.
Keywords: aging, Alzheimer’s disease, Asian Americans, caregiving, Pacific Islanders, recruitment registry
1 |. BACKGROUND
Healthcare and long-term care for Alzheimer’s disease and related dementias (ADRD) are projected to cost the United States $355 billion in 2021, not including the estimated $257 billion in unpaid caregiving provided by family and friends.1 Despite investments in ADRD research to combat this public health crisis,2 low research participation, particularly from ethnically diverse individuals, may hinder progress and perpetuate health disparities.3–6 Preventing and effectively treating Alzheimer’s disease (AD) by 2025 and identifying strategies to diversify enrollment in AD research are goals of the National Plan to Address Alzheimer’s Disease.3,7 However, the gap for ADRD research participation among racial and ethnic communities, including Asian Americans and Pacific Islanders (AAPIs) remains unaddressed.
AAPIs encompass immigrants and their descendants from many countries with diverse histories, cultures, traditions, and languages. Since 2009, Asian American immigrants have outnumbered Hispanic immigrants.8 By 2055, Asian Americans will become the largest immigrant group in the United States, and by 2065, nearly two out of five immigrants will be Asian Americans.8 Additionally, the number of AAPIs aged 65 and older will increase by 352%, and comprise 21% of the total AAPI population by 2060.9
AAPIs are at risk for ADRD.10 The number of California’s AAPIs living with AD is projected to more than double from 2019 to 2040.11 Studies suggest disparities in ADRD12,13 knowledge and caregiving experiences among AAPIs compared to non-Hispanic Whites.14,15
AAPI are under-represented in clinical ADRD research. A query of the National Alzheimer’s Coordinating Center reveals that among 44,359 participants, only 2.6% were AAPI.16 AAPIs’ participation in ADRD trials is also very low.17,18 Clinical research focused on AAPIs receives <1% of federal funding19 resulting in widening health disparities. In a recent Alzheimer’s Association survey, higher proportions of Asian Americans than White Americans believed that medical research is biased against people of color and had less interest in participating in AD clinical and prevention research.1 Altogether, increasing representation of AAPIs in ADRD clinical and caregiving research is an imperative.3,7
While AAPIs may be interested in being engaged, barriers must be addressed to improve ADRD research participation.20–22 AAPIs may have lower willingness to participate in studies requiring specific procedures23 and may be disproportionately excluded from some studies.18 AAPIs are heterogeneous in English language proficiency, culture, nativity, and socioeconomic status,24 all of which contribute to health disparities and may create barriers to participation. Inadequate participation among AAPIs makes generalization of research findings difficult and can result in bias or scientific error.25,26
Successful recruitment of underserved populations requires significant engagement with community partners who are trusted sources of information.6,27 These efforts are time consuming and costly.6 In response to the goals of the National Plan to Address Alzheimer’s Disease and the dire need to meaningfully include AAPIs in ADRD research,7 we developed a novel research recruitment registry, Collaborative Approach for AAPIs Research and Education (CARE). Here, we describe the development, implementation, and early results of the CARE Registry. By applying principles of the community-based participatory research (CBPR) approach to the development and sustainment of CARE, including forming a collaborative team of “trusted sources of information,” we hope that the CARE Registry will fill a critical gap of limited AAPIs participation in ADRD research.25,26
2 |. METHODS
2.1 |. CARE Registry design
Like other recruitment registries,28 CARE was designed with the intention of being a low-burden opportunity for individuals to enroll and learn about research opportunities. A strong community partnership was deemed essential; numerous advisors representing community organizations, caregivers, and other older community members were involved in designing features. In addition, CARE’s community partners helped recruit 123 focus group participants from seven AAPI cultural groups to provide community perspectives regarding appropriate messaging, outreach, and recruitment methods to facilitate AAPI participation in CARE.29 A strategic decision was made to promote CARE as focused on health research more broadly, including ADRD research. To facilitate CARE’s enrollment goal of 10,000 older AAPIs, a primary modality of enrollment online was selected (Figure 1). In consultation with community partners, a $10 gift card was offered as an incentive.
FIGURE 1.
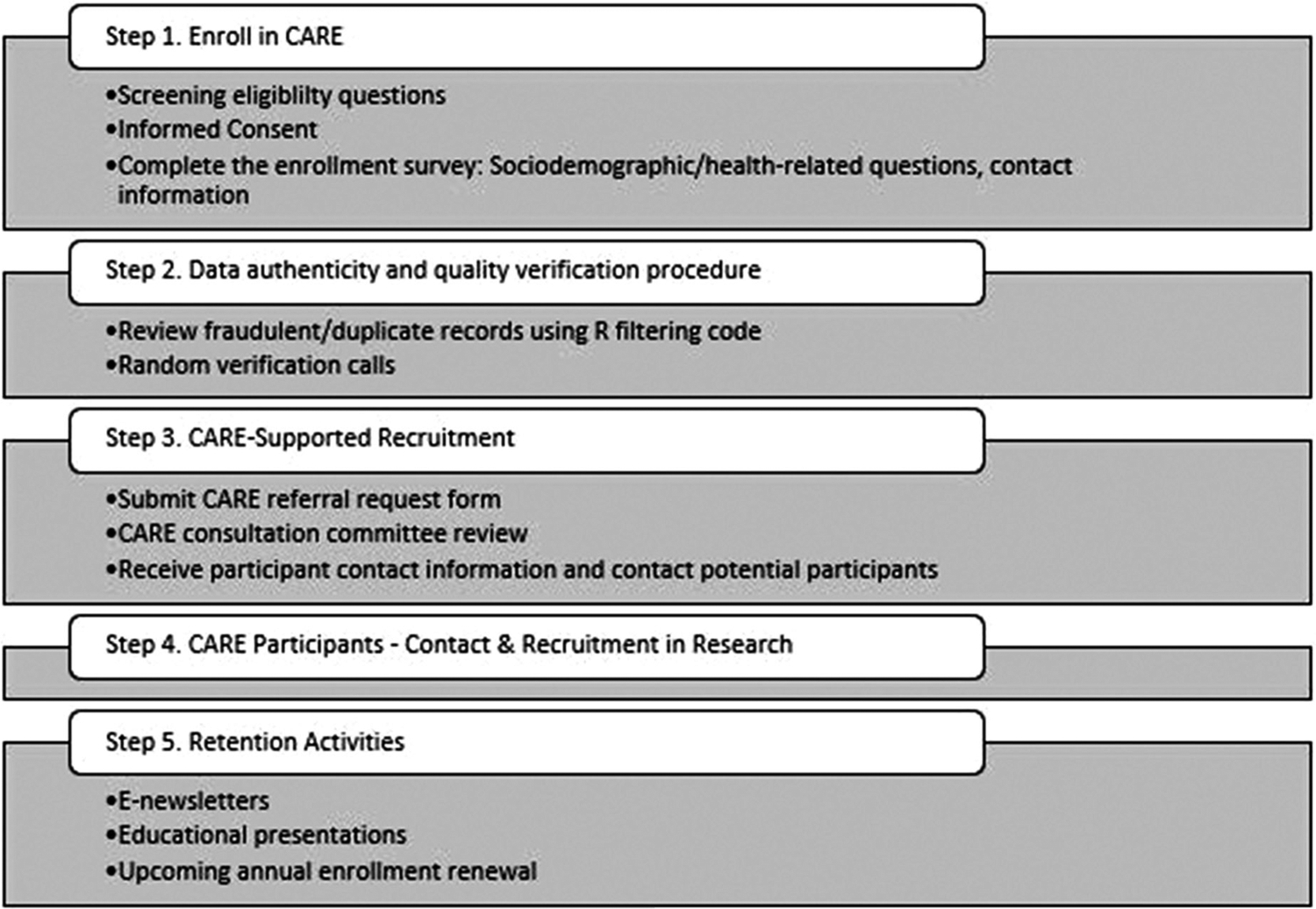
Collaborative Approach for Asian Americans and Pacific Islanders Research and Education (CARE) enrollment process. Illustration of the enrollment process for CARE participants
The online CARE Enrollment Survey uses Research Electronic Data Capture (REDCap) tools hosted at the University of California, San Francisco (UCSF).30 REDCap is a secure, web-based software platform that satisfies online data security concerns (e.g., Health Insurance Portability and Accountability Act compliance).31,32 This survey contains questions about demographics (e.g., race, ethnic/cultural group, sex, year of birth, nativity, English-language proficiency), health conditions, and status as a caregiver.
CARE developed a protocol to verify data quality and authenticity including a Completely Automated Public Turing test to tell Computers and Humans Apart (CAPTCHA); branching logic; an open-ended question for referral source; timestamps; IP address; honey-pot questions to aid identification of inconsistent or illogical responses that we later screened for via filter code (using R); individualized links for all our recruitment partners; and manual reviews for unusual, inconsistent, or automated response patterns to verifiable items.
2.2 |. CARE eligibility criteria
To enroll, individuals had to meet the following criteria: (1) self-identify as Asian, Asian American, and/or Pacific Islander alone or in combination with other races/ethnicities; (2) 18 years old or older; (3) able to read and/or speak English, Cantonese, Hindi, Mandarin, Korean, Samoan, or Vietnamese; (4) reside in the United States or US-associated Pacific Islands; and (5) willing to be contacted about participating in research. The age criterion was selected to ensure appropriate consent (i.e., legal adults) and allow for individuals to share and encourage older family members to join CARE. CARE was approved by the UCSF Institutional Review (19–18027).
2.3 |. CARE enrollment in multiple languages
The CARE website (https://careregistry.ucsf.edu) is available in five languages (English, Korean, simplified Chinese, traditional Chinese, Samoan, and Vietnamese; Hindi is in progress). All other CARE materials including the informed consent, enrollment survey, and several culturally tailored recruitment materials (e.g., flyers, PowerPoint slides, animated videos) were created with feedback from community partners and made available in six languages and adhered to World Health Organization’s translation guidelines and adaptation of instruments.33 Using this established translation method, we were able to attain “conceptually equivalent” Chinese, Korean, Samoan, and Vietnamese-language versions of the English materials that focused on cross-cultural and conceptual, over linguistic/literal, equivalence. Specific AAPI languages were selected because they are the commonly spoken languages among AAPIs with limited English proficiency,34 with plans to expand and include other languages as funding and staff capacity permit. Bilingual/bicultural Chinese, Korean, Samoan, and Vietnamese staff performed the translations (Figure 2).
FIGURE 2.
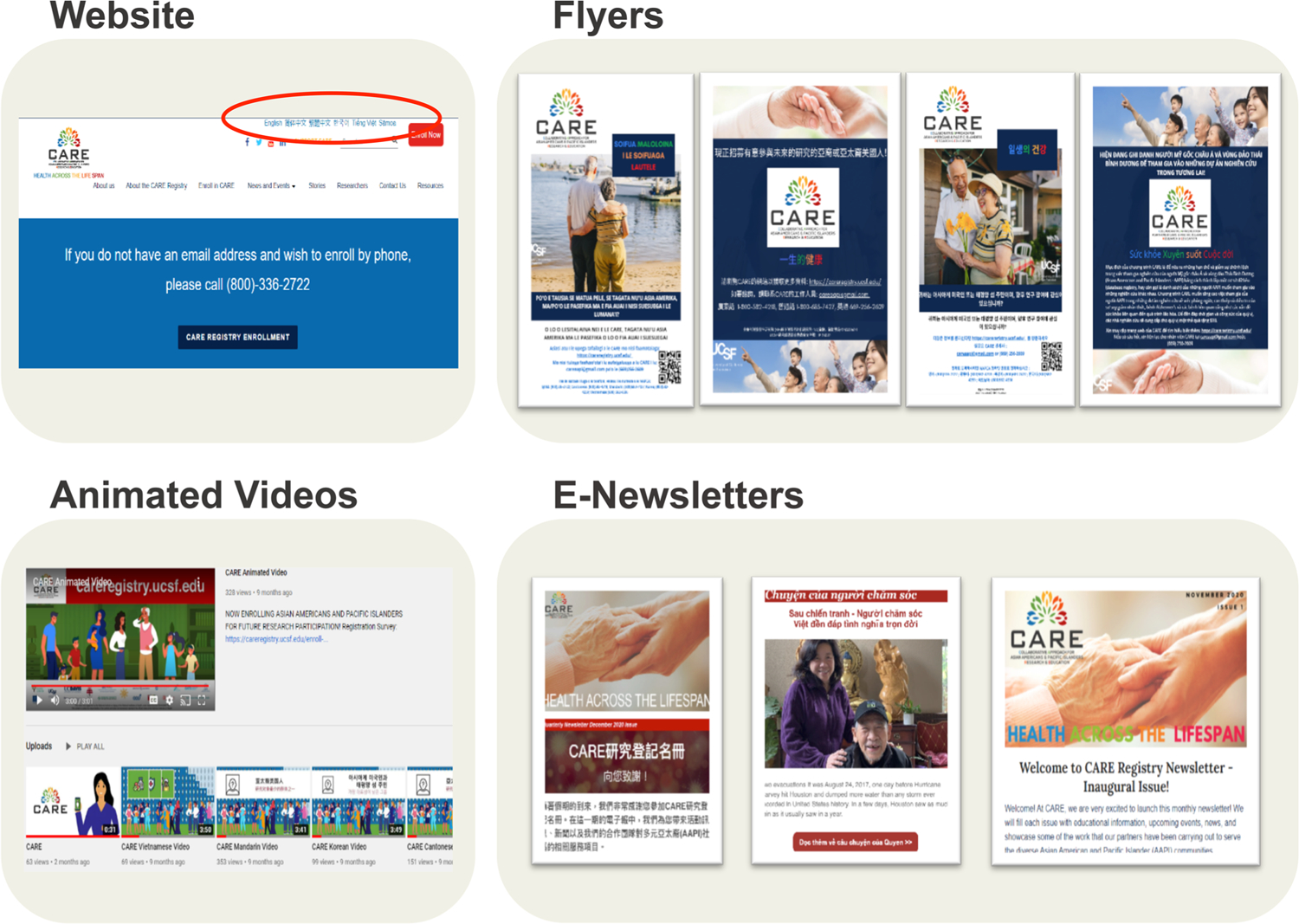
Collaborative Approach for Asian Americans and Pacific Islanders Research and Education (CARE) outreach materials in multiple languages. Clockwise, from the top left corner, examples of CARE outreach materials include CARE website; culturally tailored flyers; monthly e-newsletters in English to all CARE participants and quarterly in-language e-newsletters to Chinese, Korean, and Vietnamese CARE participants; and animated videos to introduce CARE and describe ways to enroll in CARE
CARE interviewed 10 ADRD caregivers from different AAPI cultural groups and their audio stories (including transcripts) are featured on the CARE website. These stories brought AAPI-specific perspectives on why AAPIs’ research participation is important.
For participants who lack access to the internet, the National Asian Pacific Center on Aging (NAPCA, a CARE community partner) set up toll-free numbers to help participants enroll by phone in five languages (English, Cantonese, Mandarin, Korean, and Vietnamese). In addition, CARE’s bilingual/bicultural staff are trained to provide survey administration assistance in several languages during outreach events or via a scheduled appointment by phone or Zoom.
2.4 |. CARE outreach and recruitment activities to AAPI communities
Working with CARE’s key partners (UCSF, University of California [UC] Davis, UC Irvine, NAPCA, Asian Resources Inc. [ARI], and International Children Assistance Network), CBPR principles are implemented throughout CARE activities. CBPR is a fundamental strategy to diversify the research participant pool by3,6 involving the community in all phases of research; it is a collaborative process between the community and researchers that recognizes each other’s strengths and assets; and its process requires committing to sustainability.35–37 CBPR has been used as an approach to develop a registry with older Blacks,38,39 as a recruitment tool for ADRD research,40,41 and for research with AAPI in other health conditions.42
2.4.1 |. Community advisory board
CARE’s 25 community advisory board (CAB) members represent community-based organizations serving diverse AAPI communities, key stakeholders and community leaders, caregivers, ethnic media, and health-care providers; they meet on a quarterly basis. Their roles and responsibilities include ensuring that CARE’s outreach and conduct adhere to the principles of cultural humility and appropriateness and provide perspectives and suggestions for community engagement.
2.4.2 |. Outreach and recruitment activities
CARE uses a multi-pronged approach to outreach and recruitment. The CARE team developed the CARE Outreach Metrics Survey, a REDCap online form that documents every outreach event across sites and community partners. In close collaboration with community partners, CARE members host, co-host, or serve as invited speakers at various community events, in English and Asian languages. To establish CARE’s community presence and to foster trust, regular community outreach events were organized (and in most cases presented) by members of the CARE team to provide education on health topics (e.g., ADRD and family caregiving) and to promote participation in CARE. CARE staff actively engage with followers on its social media accounts (i.e., Facebook, Twitter, and LinkedIn) by posting upcoming events from CARE and CARE’s community partners, as well as news and research concerning AAPI communities.
CARE has received substantial earned ethnic media coverage including newspapers (e.g., Sing Tao Daily, The Korea Times, Nichi Bei Weekly) and television (e.g., NBC Bay Area Asian Pacific America). CARE is listed on the Alzheimer’s Prevention Registry, a recruitment registry specifically designed to accelerate participant recruitment and enrollment to ADRD studies.43
The CARE Ambassador Program was created in the summer of 2021 to leverage AAPI youth activism and provide a venue for young adults to contribute to CARE’s mission. Through this program CARE hopes to contribute to the pipeline of future leaders in AAPI health.
To ensure CARE enrollment reflects the diversity of AAPIs, investigators closely monitor enrollment by ethnicity and cultural groups and proactively partner with community-based organizations to conduct focused outreach and recruitment in the targeted communities. Because CARE was launched during the COVID-19 pandemic, most activities have been held online. However, as restrictions are lifted, in-person events such as tabling at health fairs and cultural events are expected to increase in frequency.
2.5 |. CARE participant engagement and retention
Personalized survey links are e-mailed to registry participants after enrollment to request updates of their information on an annual basis (via REDCap). Messages include the option to withdraw from CARE. Participants who do not have e-mail addresses are contacted by CARE staff or a community partner.
Implementation of retention activities are critical to registry sustainability. Multiple strategies are used to help participants maintain connections with CARE. Monthly E-newsletters have been published since October 2020 and catalogued on the CARE website. Each issue provides an update on CARE enrollment and information about upcoming events, news, research studies, or educational events, and showcase some of the work of community partners in diverse AAPI communities. In-language newsletters (simplified Chinese, traditional Chinese, Korean, and Vietnamese) are sent on a quarterly basis based on participants’ indicated language preference. E-cards are disseminated on holidays holding special meanings for AAPI communities (e.g., Lunar New Year, Diwali).
2.6 |. CARE-supported research
2.6.1 |. Recruitment referral request protocol
A CARE subcommittee developed a protocol for investigators to request participant data to recruit AAPI participants into their research studies. The draft protocol was shared with the CAB members and several meetings were convened in November 2020 to gather feedback; the protocol was finalized in December 2020.
There are five steps in the CARE recruitment referral protocol: (1) Investigators submit a CARE Referral Request Form asking for the study title, timeline, objectives, eligibility criteria, target sample size, funding source, and institutional review board (IRB) status. Investigators indicate their research team’s language proficiency and available study support if their study will recruit in one of the Asian CARE languages. (2) The CARE Consultation Committee (comprised of CARE investigators) reviews requests and a consultation meeting may be scheduled on a case-by-case basis. (3) Investigators may revise the form based on committee feedback and resubmit to CARE. (4) Investigators must have IRB approval to include language about including the CARE Registry as a recruitment source before CARE participant contact information is shared (name, language preference, and preferred contact method). (5) The requesting investigator is responsible for contacting CARE participants within 1 month of receiving their contact information and completing a CARE recruitment tracking form reporting the outcome of every participant contact. We also ask that CARE be cited in publications or presentations.
To facilitate this process, we created templates for e-mails, letters, and phone scripts. CARE also provides letter of support for grant applications and IRB review.
2.6.2 |. Promoting CARE to the research community
CARE held four Brain Trust Meetings between January 2021 and September 2021. Meetings were held online on different days of the week and times of the day to optimize participation. They were promoted broadly to the research community (e.g., professional organization listservs) and community partners with interest in partnering with researchers to conduct AAPI health research. At each meeting, we introduced CARE to community leaders and researchers (including the recruitment referral request protocol) and included perspectives from both community and academic partners with the goal of facilitating collaborative partnerships. Attendees are asked to complete an online evaluation survey that asks about their feedback on usefulness of the meeting, and intention to recommend CARE to eligible individuals, and to other researchers.
3 |. RESULTS
3.1 |. CARE participant characteristics
The CARE website and Enrollment Survey were soft launched in June 2020 and officially launched on October 15, 2020. As of October 31, 2021, 7040 participants had enrolled (Figure 3). Table 1 shows participant characteristics. Current mean age is 53.0 years (standard deviation [SD]: 17.3, range = 18 to 99). The major cultural groups include Vietnamese (35.6%), ethnic Chinese (including persons from China, Hong Kong, and Taiwan; 33.5%), and Korean (17.6%). Approximately half completed the enrollment survey in English (47.0%), followed by Vietnamese (23.4%), Chinese (15.8%), and Korean (12.5%).
FIGURE 3.

Collaborative Approach for Asian Americans and Pacific Islanders Research and Education (CARE) Registry enrollment as of October 31, 2021. Illustration of CARE enrollment status by month, showing target enrollment number of 10,000 AAPI participants (blue line), projected cumulative enrollment number (purple dotted line), actual cumulative enrollment number (dark green line), and actual monthly enrollment number (light green line)
TABLE 1.
Demographic characteristics of participants enrolled in CARE as of October 31, 2021 (N = 7040)
| Characteristics | N (%) |
|---|---|
| Age, mean (standard deviation) 53.0 (17.3) range 18 to 99 | |
| Cultural group | |
| Asian Indian | 394 (5.6) |
| Ethnic Chinesea | 2359 (33.5) |
| Filipino | 272 (3.9) |
| Japanese | 169 (2.4) |
| Korean | 1242 (17.6) |
| NHPIb | 156 (2.2) |
| Vietnamese | 2505 (35.6) |
| Mixed | 74 (1.1) |
| Other | 218 (3.3) |
| Language | |
| English | 3306 (47.0) |
| Chinese-simplified | 705 (10.0) |
| Chinese—traditional | 409 (5.8) |
| Korean | 878 (12.5) |
| Samoan | 92 (1.3) |
| Vietnamese | 1650 (23.4) |
| Sex | |
| Male | 2480 (35.2) |
| Female | 4434 (63.0) |
| Other/decline to state | 126 (1.8) |
| Nativity | |
| US-born | 1084 (15.4) |
| Foreign-born | 5956 (84.6) |
| Marital status | |
| Married/living with partner | 4480 (63.6) |
| Single | 1606 (22.8) |
| Separated/divorced/widowed | 838 (11.9) |
| Prefer not to answer | 116 (1.6) |
| Employment status | |
| Full time | 2186 (31.1) |
| Part time | 1196 (17.0) |
| Unemployed | 1010 (14.4) |
| Retired | 1602 (22.8) |
| Homemaker | 731 (10.4) |
| Other | 341 (4.8) |
| Prefer not to answer | 195 (2.8) |
| Education | |
| High school or less | 2670 (37.9) |
| Some college or technical school | 856 (12.2) |
| Bachelor’s degree | 1954 (27.8) |
| Master’s degree or higher | 1270 (18.0) |
| Prefer not to answer | 290 (4.1) |
| Annual household income ($) | |
| ≤ 25,000 | 2622 (37.2) |
| > 25,000 to 75,000 | 1904 (27.0) |
| >75,000 to 150,000 | 920 (13.1) |
| > 150,000 to 200,000 | 297 (4.2) |
| > 200,000 | 302 (4.3) |
| Decline to state | 995 (14.1) |
| Limited English proficiency c | |
| Yes | 4034 (57.3) |
| No | 3006 (42.7) |
| Caregiver of older adults or someone with special needs d | |
| Yes | 782 (11.0) |
| No | 6258 (89.0) |
| ADRD caregivers | |
| Yes | 261 (3.7) |
| Having ADRD | |
| Yes | 661 (9.4) |
| Region | |
| California | 6191 (88.1) |
| Non-California | 849 (11.9) |
| Who completed the survey? | |
| By myself | 4919 (70.4) |
| Family or friend helped me | 343 (4.9) |
| Research staff helped me | 1721 (24.7) |
| Prior research participation experience | |
| Yes | 910 (12.9) |
| No | 5635 (80.0) |
| Not sure | 495 (7.0) |
Abbreviations: ADRD, Alzheimer’s disease and related disorders; CARE,Collaborative Approach for Asian Americans and Pacific Islanders Research and Education; NHPI, Native Hawaiian and Pacific Islander.
Ethnic Chinese includes people from China, Hong Kong, Taiwanese and those who identify as Huaren.
Native Hawaiians/Pacific Islanders.
Self-reported as having “some,” “a little,” or “not at all” proficiency in speaking, reading, or writing English.
Caregiving status was ascertained by asking, “Are you responsible for the care of any individuals?” (Note: this question is accompanied by examples of care, such as assisting with bathing, cooking, providing transportation, providing supervision, etc., and the care provided can be in person or from a distance.) If the response is “yes,” participants are asked whether they are caring for older adults (yes/no) or caring for individuals with special needs (yes/no).
Most registry participants were female (63.0%), foreign-born (84.6%), had limited English proficiency (57.3%), and were married/living with a partner (63.6%). Only 11% reported being caregivers (with one-third being ADRD caregivers) and only 9.4% reported having ADRD or related symptoms. Most participants reside in California (88.1%), completed the survey by themselves (70.4%), and had no previous research participation experience (80%).
Recruitment sources are shown in Table 2. The majority (69.2%) of participants enrolled in CARE through community organizations, followed by 10% from word of mouth, and 8% from the Internet (e.g., Facebook advertisement, other social media posts, and websites). A smaller percentage of participants indicated they heard about CARE via e-mail/listserv (4%), university (3.4%), church (2.2%), newspaper/TV (1.3%), conference/workshop/webinar (1%), and health-care provider (0.2%).
TABLE 2.
Characteristics of Registry recruitment sources (N = 6951)
| Recruitment source | N (%) |
|---|---|
| Communitypartners | 4,812 (69.2) |
| Acquaintances | 676 (9.7) |
| Internet | 538 (7.7) |
| Social media & other websites | 347 (5.0) |
| Social media ads (via Facebook) | 191 (2.7) |
| E-mail/listserv | 277 (4.0) |
| University | 238 (3.4) |
| Faith-based organization | 152 (2.2) |
| Media (newspaper/TV) | 89 (1.3) |
| Conference/workshop/webinar | 70 (1.0) |
| Health-care provider | 11 (0.2) |
3.2 |. CARE outreach events summary
Between March 11, 2020 (when the first CARE outreach event was conducted) and November 5, 2021, CARE conducted a total of 128 outreach activities. Because CARE was launched during the COVID-19 pandemic, most (77.4%) outreach events were conducted online. With gradual reopening in some areas, some outreach events were done face-to-face at community organizations (9.7%), places of worship (5.6%), academic institutions (5.6%), and community clinics (1.6%). Most outreach events targeted AAPI community members (71.7%), although a smaller proportion were for both members in academia and the AAPI community (16.5%), and a few activities (11.8%) were completely geared toward researchers. Bilingual CARE team members or trusted members in health care (e.g., a physician, psychologist, or nurse) typically presented. As a result, although most (67.5%) events were held in English (n = 102), a sizeable number of events were conducted in AAPI languages including Cantonese (n = 13), Hindi (n = 2), Korean (n = 7), Mandarin (n = 15), and Vietnamese (n = 12).
3.3 |. Brain Trust meetings
Four Brain Trust meetings were held comprising 113 attendees, and 82 completed an evaluation survey. Most attendees were researchers (67.1%), resided in California (67.1%), and were from diverse racial and ethnic backgrounds (Table 3). Attendees heard about the Brain Trust meeting through word of mouth (43.9%), e-mail or listserv (26.8%), from a community organization (7.3%), and from other sources (22.0%) such as CARE CAB members. Respondents rated the meeting as either “very useful” (78.1%) or “somewhat useful” (21.9%). Nearly all respondents said that they would recommend CARE to eligible people (97.6%) or to researchers they knew (96.3%).
TABLE 3.
Characteristics of brain trust meeting attendees (N = 82)
| N (%) | |
|---|---|
| Age (years) | |
| 18 to 30 | 20 (24.4%) |
| 31 to 49 | 37 (45.1%) |
| 50+ | 25 (30.5%) |
| Attendees’ role (s) a | |
| Community member | 21 (25.6%) |
| Community organization representative | 14 (17.1%) |
| Researcher | 55 (67.1%) |
| Race and ethnic background b | |
| African American | 3 (3.7%) |
| Asian Indian | 10 (12.2%) |
| Chinese | 22 (26.8%) |
| Filipino | 13 (15.9%) |
| Hispanic | 1 (1.2%) |
| Hmong | 1 (1.2%) |
| Japanese | 5 (6.1%) |
| Korean | 6 (7.3%) |
| Okinawan | 1 (1.2%) |
| Samoan | 1 (1.2%) |
| Taiwanese | 7 (8.5% |
| Vietnamese | 17 (20.7%) |
| White | 5 (6.1%) |
| Other Pacific Islander | 1 (1.2%) |
| Area of residence | |
| Los Angeles and Orange Counties, California | 8 (9.7%) |
| San Francisco Bay area, California | 44 (53.7%) |
| Other area of Californiac | 3 (3.7%) |
| Outside of Californiad | 27 (32.9%) |
Evaluation survey respondents could select more than one role.
Evaluation survey respondents could select more than one race and ethnic background.
Three of the attendees joined from the San Diego area.
Attendees joined from other US states including Arizona, Colorado, Connecticut, Florida, Georgia, Hawaii, Illinois, Maryland, Massachusetts, Minnesota, Missouri, Ohio, Pennsylvania, Texas, Washington, Washington DC, and Wisconsin. One participant joined from Canada.
3.4 |. Status of CARE-supported referral requests
CARE began to accept referral requests in late January 2021. As of January 11, 2022, CARE has received 32 referral requests from 29 investigators across the United States. Exactly half (n = 16) of the requesting studies are funded by the National Institutes of Health, of which the majority received support from the National Institute on Aging. Many of the studies were ADRD-related (n = 18), and others focus on a wide range of health conditions including cardiovascular disease, contraceptive decision-making, type 2 diabetes, lung cancer, depression, and substance use. Follow-up is conducted to determine how many of those contacted from the CARE Registry actually enroll in the research study. Results on these program outcomes will be reported in a future publication.
4 |. DISCUSSION
To our knowledge, CARE is the only research recruitment registry that purposively engages AAPI participants in multiple languages. CARE investigators used CBPR methods to design the registry in a manner that would be acceptable to AAPIs, both young and old. By using outreach evaluation metrics, we can better understand what approaches, venues, and messages would be most effective in recruiting AAPIs to the CARE Registry. So far, these approaches seem to be working, as we have outperformed expected accrual (Figure 3), despite severe limitations in our opportunity to engage in in-person community outreach due to the COVID-19 pandemic. This success has clearly been driven by our community-based partnerships, as about two-thirds of participants were recruited through partner organizations.
CARE participants are diverse in terms of age, languages, and AAPI subgroups. As with other registries, women made up many enrollees.43–46 Most participants were born in another country and less than half enrolled in English. Perhaps more importantly, 57% reported limited English proficiency, which may be a barrier to enrollment in studies conducted exclusively in English. Most of the participants had no prior experience in research participation. Not surprisingly, only 5.5% of participants who enrolled in a non-English language have previously participated in research compared to 21% among those enrolled in English. This underscores language barriers as a significant obstacle to AAPIs’ participation in research. CARE’s existence helps foster meaningful inclusion of AAPIs who are under-represented in research in large part due to the lack of culturally and linguistically appropriate outreach. CARE serves as a poignant reminder to researchers—including ADRD, aging, and caregiving—that AAPI are heterogeneous in cultures, spoken languages, as well as proficiency in English; thus, meaningful inclusion necessitates researchers to be purposeful in these considerations when developing study designs and methods.
The Brain Trust meetings have helped spread the word about CARE among researchers as well as community organizations and provided a platform to engage researchers nationally. The presentations not only highlighted the importance of increasing AAPIs’ representation in research but also provided an accessible venue to support researchers to reach a diverse pool of potential AAPI participants for their research. These events have been extremely well received, with nearly every attendee indicating that they would recommend enrollment among AAPI community members and use among researchers.
Though the CARE Registry features many strengths, there are also limitations. As yet, it is unclear whether the methods described will actually increase representation of AAPIs in ADRD, aging, and caregiving research. We are carefully tracking recruitment outcomes among studies using the registry and will describe these outcomes in a future paper. We also note the relatively low proportions of CARE participants who self-reported ADRD (9.4%) or are caregivers (11.0%, including caregivers for someone with ADRD). The COVID-19 pandemic likely exacerbated existing barriers to research recruitment.47,48 On the ground, the pandemic has resulted in fewer in-person outreach and recruitment activities where we can interact directly in real time with individuals interested in CARE. Moreover, it’s probable that persons with ADRD are not aware of their diagnosis or impairment and may lack insight or capacity to understand the purpose of CARE and to give informed consent. Highly ingrained cultural values (e.g., filial piety) may lessen the perception of “caregiving” as a distinct role49 for some CARE participants, resulting in under-reporting of this status. Nonetheless, we are continuing to work with our CAB and community partners to adjust our recruitment strategies to enroll more caregivers and persons with ADRD into CARE. Though we enroll participants in several AAPI languages, many AAPI languages remain unavailable. We also acknowledge that some large AAPI groups in the United States, namely Asian Indians and Filipinos, are relatively under-represented in the CARE Registry.
In conclusion, the CARE Registry has been developed and successfully implemented through a process that involves key stakeholders including community members, community organization leadership, and researchers. We have successfully recruited >7000 registry participants despite significant limitations in our ability to conduct face-to-face outreach and recruitment due to the COVID-19 pandemic. The registry provides an opportunity for AAPIs to feel they are meaningfully contributing to research50 and may provide a useful model to increase ADRD research participation among other under-represented populations.
RESEARCH IN CONTEXT.
Systematic review: The authors reviewed the literature using traditional sources (e.g., Pubmed) and meeting abstracts and presentations as well as consulted with experts in Alzheimer’s Disease and Related Dementias (ADRD) in the U.S. There are some ADRD, aging and caregiving related registries, but none that target Asian Americans and Pacific Islanders (AAPIs) in multiple languages.
Interpretation: Collaborative Approach for AAPIs Research and Education (CARE), a research recruitment registry, employs community based participatory research methods that are culturally/linguistically appropriate. CARE has enrolled more than 7,000 AAPIs in a 1-year period. The majority reported never having participated in any kind of research before. CARE also engages researchers by establishing a recruitment referral request protocol.
Future directions: Future research should examine the utility of the registry in increasing the meaningful inclusion of AAPIs into ADRD and health-related research. Additional outreach is needed to reach some AAPI groups who are underrepresented in CARE.
ACKNOWLEDGMENTS
This research was supported by the National Institute on Aging of the National Institutes of Health (R24AG063718). We are grateful to the CARE Registry participants, and our Community Advisory Board for their guidance and input. We also wish to acknowledge our community partners for their assistance with recruitment/outreach. Special appreciation goes to CARE’s staff and interns for their assistance with coordination and data entry/cleaning.
Funding information
National Institute on Aging of the National Institutes of Health, Grant/Award Number: R24AG063718
Footnotes
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
- 1.Alzheimer’s Association. Alzheimer’s Disease Facts and Figures. Accessed October 8, 2021. https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf
- 2.Alzheimer’s Impact Movement. Alzheimer’s Research Funding at NIH Gets Important Boost in House Labor-HHS Appropriations Budget. Accessed October 8, 2021. https://alzimpact.org/press/press_release/id/121
- 3.Alzheimer’s Association International Conference. New National Strategy for Recruitment and Participation In Alzheimer’s Disease Clinical Trials Takes Shape. Accessed October 8, 2021. https://www.alz.org/aaic/downloads2018/Mon-pm-briefing-clinical-research-recruitment-strategy.pdf [Google Scholar]
- 4.Grill JD, Holbrook A, Pierce A, Hoang D, Gillen DL. Attitudes toward potential participant registries. J Alzheimers Dis. 2017;56(3):939–946. 10.3233/JAD-160873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Grill JD, Karlawish J. Addressing the challenges to successful recruitment and retention in Alzheimer’s disease clinical trials. Alzheimers Res Ther. 2010;2(6):34. 10.1186/alzrt58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Grill JD, Galvin JE. Facilitating Alzheimer disease research recruit ment. Alzheimer Dis Assoc Disord. 2014;28(1):1–8. 10.1097/WAD.0000000000000016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.National Institute on Aging. NIA and the National Plan to Address Alzheimer’s Disease. Accessed October 11, 2021. https://www.nia.nih.gov/about/nia-and-national-plan-address-alzheimers-disease
- 8.Pew Research Center. Key findings about U.S. immigrants. Pew Research Center. Accessed October 11, 2021. http://www.pewresearch.org/fact-tank/2017/05/03/key-findings-about-us-immigrants/ [Google Scholar]
- 9.National Asian Pacific Center on Aging. Asian Americans and Pacific Islanders in the United States Aged 65 Years and Older: Population, Nativity, and Language. Accessed November 2, 2021. https://napca.org/wp-content/uploads/2017/10/65-population-report-FINAL.pdf
- 10.Vincent GK, Velkoff VA. The Next Four Decades: the Older Population in the United States: 2010 to 2050: Population Estimates and Projections. U.S. Department of Commerce, Economics and Statistics Administration, U.S. Census Bureau. Accessed October 11, 2021. https://www.census.gov/prod/2010pubs/p25-1138.pdf [Google Scholar]
- 11.Ross L, Beld M, Yeh J. Alzheimer’s Disease and Related Dementias Facts and Figures in California: Current Status and Future Projections. University of California. Accessed October 11, 2021. https://www.cdph.ca.gov/Programs/CCDPHP/DCDIC/CDCB/CDPH%20Document%20Library/Alzheimers’%20Disease%20Program/151764_Alzheimers_Disease_Facts_and_Figures_Reportv3_ADA.pdf [Google Scholar]
- 12.Woo BK. Knowledge of dementia among Chinese American immigrants. Asian J Psychiatr. 2013;6(4):351–352. 10.1016/j.ajp.2013.03.010 [DOI] [PubMed] [Google Scholar]
- 13.Ta Park V, Nguyen K, Tran Y, et al. Perspectives and insights from Vietnamese American mental health professionals on how to cultureally tailor a Vietnamese dementia caregiving program. Clin Gerontol. 2018:41(3):184–199. 10.1080/07317115.2018.1432734 [DOI] [PubMed] [Google Scholar]
- 14.National Alliance for Caregiving, AARP Public Policy Institute. Caregiving in the U.S. 2015: Focused look at caregivers of adults age 50+. Accessed May 16, 2018. http://www.caregiving.org/wp-content/uploads/2015/05/2015_CaregivingintheUS_Care-Recipients-Over-50_WEB.pdf
- 15.Pinquart M, Sorensen S. Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: a meta-analysis. Gerontologist. 2005;45(1):90–106. [DOI] [PubMed] [Google Scholar]
- 16.National Alzheimer’s Coordinating Center (NACC). Web-Based Query System. Accessed October 11, 2021. https://naccdata.org/requesting-data/web-query
- 17.Franzen S, Smith JE, van den Berg E, et al. Diversity in Alzheimer’sdisease drug trials: the importance of eligibility criteria. Alzheimers Dement. 2021; 10.1002/alz.12433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Raman R, Quiroz YT, Langford O, et al. Disparities by race and ethnicity among adults recruited for a preclinical Alzheimer’s disease trial. JAMA Network Open. 2021;4(7) 10.1001/jamanetworkopen.2021.14364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Doan LN, Takata Y, Sakuma KK, Irvin VL. Trends in clinical research including Asian American, Native Hawaiian, and Pacific Islander participants funded by the US National Institutes of Health, 1992 to 2018. JAMA Netw Open. 2019;2(7):e197432. 10.1001/jamanetworkopen.2019.7432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tzuang M, Gallagher-Thompson D. Caring for Caregivers of a Person with Dementia. In: Pachana NA, Laidlaw K, eds. The Oxford Handbook of Clinical Geropsychology: International Perspectives. Oxford University Press; 2014:chap 39. [Google Scholar]
- 21.Watson JL, Ryan L, Silverberg N, Cahan V, Bernard MA. Obstacles and opportunities in Alzheimer’s clinical trial recruitment. Health Aff (Mill-wood). 2014;33(4):574–9. 10.1377/hlthaff.2013.1314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chao SZ, Lai NB, Tse MM, et al. Recruitment of Chinese American elders into dementia research: the UCSF ADRC experience. Gerontologist. 2011;51 Suppl 1:S125–S133. 10.1093/geront/gnr033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Salazar CR, Hoang D, Gillen DL, Grill JD. Racial and ethnic differences in older adults’ willingness to be contacted about Alzheimer’s disease research participation. Alzheimers Dement (N Y). 2020;6(1):e12023. 10.1002/trc2.12023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.U.S. Census Bureau. Facts for Features: Asian/Pacific American Heritage Month: May 2018. Accessed October 12, 2021. https://www.census.gov/newsroom/facts-for-features/2018/asian-american.html
- 25.Kasenda B, von Elm E, You J, et al. Prevalence, characteristics, and publication of discontinued randomized trials. JAMA. 2014;311(10):1045–1051. 10.1001/jama.2014.1361 [DOI] [PubMed] [Google Scholar]
- 26.Vellas B, Pesce A, Robert PH, et al. AMPA workshop on challenges faced by investigators conducting Alzheimer’s disease clinical trials. Alzheimers Dement. 2011;7(4):e109–e117. 10.1016/j.jalz.2010.05.2020 [DOI] [PubMed] [Google Scholar]
- 27.Rabinowitz YG, Gallagher-Thompson D. Recruitment and retention of ethnic minority elders into clinical research. Alzheimer Dis Assoc Disord. 2010;24 Suppl:S35–S41. [PubMed] [Google Scholar]
- 28.Aisen P, Touchon J, Andrieu S, et al. Registries and cohorts to accelerate early phase Alzheimer’s trials. A report from the E.U./U.S. Clinical Trials in Alzheimer’s Disease Task Force. J Prev Alzheimers Dis. 2016;3(2):68–74. 10.14283/jpad.2016.97 [DOI] [PubMed] [Google Scholar]
- 29.Ta Park V, Grill JD, Zhu J, et al. Asian Americans and Pacific Islanders’perspectives on participating in the CARE recruitment research registry for Alzheimer’s disease and related dementias, aging, and caregiving research. Alzheimers Dement. 2021;7(1):e12195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Harris PA, aylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Patridge EF, Bardyn TP. Research electronic data capture (REDCap). JMed Libr Assoc. 2018;106(1):142–144. [Google Scholar]
- 32.Obeid JS, McGraw CA, Minor BL, et al. Procurement of shared data instruments for Research Electronic Data Capture (REDCap). J Biomed Inform. 2013;46(2):259–65. 10.1016/j.jbi.2012.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.World Health Organization. Process of Translation and Adaptation of Instruments. Accessed October 12, 2021. http://www.who.int/substance_abuse/research_tools/translation/en/
- 34.AAPI DATA. Infographic - Percentage of Asian Americans With LimitedEnglish Proficiency. Accessed October 12, 2021. https://aapidata.com/infographic-limited-english-2-2/
- 35.Israel BA EE, Schulz AJ, Parker EA. Introduction to methods in community-based participatory research for health. In: Israel EE,Schulz AJ, Parker E, ed. Methods in Community-Based Participatory Research for Health. Jossey-Bass; 2005:3–26. [Google Scholar]
- 36.Faridi Z, Grunbaum JA, Gray BS, Franks A, Simoes E. Community-based participatory research: necessary next steps. Prev Chronic Dis. 2007;4(3):A70. [PMC free article] [PubMed] [Google Scholar]
- 37.Minkler M, Blackwell AG, Thompson M, Tamir H. Community-based participatory research: implications for public health funding. Am J Public Health. 2003;93(8):1210–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lichtenberg PA. The generalizability of a participant registry for minority health research. Gerontologist. 2011;51 Suppl 1:S116–S124. 10.1093/geront/gnr021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chadiha LA, Washington OG, Lichtenberg PA, Green CR, Daniels KL,Jackson JS. Building a registry of research volunteers among older urban African Americans: recruitment processes and outcomes from a community-based partnership. Gerontologist. 2011;51 Suppl 1:S106–S115. 10.1093/geront/gnr034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Green-Harris G, Koscik RL, Houston S, et al. Using asset-based community involvement to address health disparities and increase African American Participation in ad research: experiences from the Wisconsin Alzheimer’s Institute. Alzheimers Dement. 2017;13(7):P897–P898. 10.1016/j.jalz.2017.07.308 [DOI] [Google Scholar]
- 41.Austrom MG, Bachman J, Altmeyer L, Gao S, Farlow M. A collaborative Alzheimer disease research exchange using a community-based Helpline as a recruitment tool. Alzheimer Dis Assoc Disord. 2010;24 Suppl:S49–S53. [PubMed] [Google Scholar]
- 42.Katigbak C, Foley M, Robert L, Hutchinson MK. Experiences and lessons learned in using community-based participatory research to recruit Asian American immigrant research participants. J Nurs Scholarsh. 2016;48(2):210–218. 10.1111/jnu.12194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Langbaum JB, High N, Kettenhoven C, Reiman EM, Tariot PN. The Alzheimer’s prevention registry: a large, internet-based participant recruitment registry to accelerate referrals to Alzheimer’s-focused studies. J Prev Alzheimers Dis. 2020;7(4):242–250. 10.14283/jpad.2020.31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ashford MT, Eichenbaum J, Williams T, et al. Effects of sex, race, ethnicity, and education on online aging research participation. Alzheimers Dement (N Y). 2020;6(1):e12028. 10.1002/trc2.12028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Grill JD, Hoang D, Gillen DL, et al. Constructing a local potential participant registry to improve Alzheimer’s Disease Clinical Research recruitment. J Alzheimers Dis. 2018;63(3):1055–1063. 10.3233/JAD-180069 [DOI] [PubMed] [Google Scholar]
- 46.Walter S, Clanton TB, Langford OG, et al. Recruitment into the Alzheimer Prevention Trials (APT) Webstudy for a trial-ready cohort for preclinical and prodromal Alzheimer’s Disease (TRC-PAD). JPrev Alzheimers Dis. 2020;7(4):219–225. 10.14283/jpad.2020.46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mirza M, Siebert S, Pratt A, et al. Impact of the COVID-19 Pandemicon Recruitment to Clinical Research Studies in Rheumatology. Musculoskeletal Care. 2021; 10.1002/msc.1561 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Mitchell EJ, Ahmed K, Breeman S, et al. It is unprecedented:trial management during the COVID-19 pandemic and beyond. Trials. 2020;21(1):784. 10.1186/s13063-020-04711-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Pan Y, Chen R, Yang D. The relationship between filial piety and caregiver burden among adult children: a systematic review and meta-analysis. Geriatr Nurs. 2021;43:113–123. 10.1016/j.gerinurse.2021.10.024 [DOI] [PubMed] [Google Scholar]
- 50.Krysinska K, Sachdev PS, Breitner J, Kivipelto M, Kukull W, Brodaty H. Dementia registries around the globe and their applications: a systematic review. Alzheimers Dement. 2017;13(9):1031–1047. 10.1016/j.jalz.2017.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]