

Abstract
Background:
There is no information about the clinical significance of the albumin-bilirubin (ALBI) score in patients with hypertrophic cardiomyopathy (HCM).
Objective:
We retrospectively performed clinical evaluations in 462 patients with HCM to estimate whether the ALBI score could be a new tool to predict mortality in HCM.
Methods and Results:
During a median follow-up of 4.7 years, HCM-related death occurred in 52 (11.3%) patients. Overall, there was a significant positive association between ALBI score and HCM-related death (adjusted hazard ratio [HR]: 1.79 per one standard deviation [SD] increment, 95% confidence interval [CI]: 1.36–2.35). When the score was assessed as tertiles, the adjusted HRs of HCM-related death were 1.30 (95% CI: 0.42–3.99) for the tertile 2 and 4.43 (95% CI: 1.65–11.89) for the tertile 3, compared with the tertile 1. Stratified analysis and E-value analysis suggested the robustness of the above-mentioned results. Meanwhile, time-dependent ROC analysis showed ALBI score could discriminate HCM-related death at various time points (AUC ranges: 0.725–0.850). Furthermore, exploratory analysis indicated the dynamic changes of ALBI score also could predict HCM-related death. Finally, multiple linear regression analysis suggested some pathogenetic pathways associated with HCM-related adverse outcomes significantly correlated with ALBI score, and the pathways included inflammation, myocardial injury, nutritional status and some clinical characteristics, but not abnormal cardiac structure and function itself.
Conclusions:
Higher ALBI score is a strong independent predictor of HCM-related death in patients with HCM.
Keywords: albumin, bilirubin, mortality, hypertrophic cardiomyopathy
1. Introduction
Hypertrophic cardiomyopathy (HCM) is a genetic heart disease that affects patients globally, with an estimated prevalence of at least 1:500 [1]. Innovative clinical science over the past two decades has greatly improved life expectancy and the quality of life for patients with HCM [2]. However, recent studies suggest that HCM is still associated with excess mortality [3,4,5]. Therefore, we need more researches about the risk associated with HCM-related death and for better risk stratification in patients with HCM.
Recently, a new scoring system assessing liver function, namely albumin-bilirubin (ALBI) score, was developed in patients with hepatocellular carcinoma [6], and many studies have shown that higher ALBI score is associated with adverse events in various gastrointestinal diseases [7,8,9,10]. Meanwhile, it is well established that liver function can predict the prognosis in patients with cardiovascular diseases (CVDs) [11,12,13]. However, only two studies assessed the relationship between ALBI score and CVDs: one showed the score was independently associated with in-hospital mortality in patients hospitalized for acute heart failure (HF) [14], and another suggested it could predict one-year mortality in patients with acute HF [15]. On the other hand, recent researches have demonstrated the two components of ALBI score, total bilirubin and albumin, are associated with inflammation and oxidative stress [13,16,17], which are related to ventricular remodeling, myocardial fibrosis, diastolic dysfunction, microvascular thrombosis, cardiac hypertrophy and left ventricular outflow tract obstruction in HCM [18,19,20,21,22]; meanwhile, total bilirubin and albumin also have some other properties [12,17], which could be associated with the prognosis in patients with HCM. Therefore, ALBI score may a potential prognostic indicator for HCM.
To our knowledge, there is no information about the clinical significance of ALBI score in patients with HCM. Therefore, we tested the hypothesis that higher ALBI score was associated with increased risk of death in patients with HCM.
2. Methods
2.1. Study patients
This was a retrospective, single-center cohort study, which was performed at West China Hospital of Sichuan University, and the hospital is a tertiary center located in Chengdu, China. We included the hospitalized patients with a discharge diagnosis of HCM (n = 546) between December 2008 to November 2018, and then, the diagnosis was rechecked by experienced cardiologist according to the criteria of the European Society of Cardiology (ESC) [23]. After rechecking, nine patients were excluded for cardiac amyloidosis (n = 5), restrictive cardiomyopathy (n = 2), dilated cardiomyopathy (n = 1) and myocarditis (n = 1). Among the remaining 537 patients, 72 patients with missing baseline data (n = 67) or age under 18 (n = 5) were excluded from the study, and 3 patients were also excluded from the study because of loss to follow-up after the first evaluation. Finally, a total of 462 adult patients were included for the present analysis.
The study was conducted according to the principles of the Declaration of Helsinki, and was approved by the Biomedical Research Ethics Committee, West China Hospital of Sichuan University (approval number: 2019–1147). The study has been registered on the website of Chinese Clinical Trial Registry (https://www.chictr.org.cn/enIndex.aspx; registration number: ChiCTR2000029352). Informed consent was waived due to the retrospective nature of the study. Some other detailed information has been reported in the recently published studies [24,25,26].
2.2. Clinical evaluation
Baseline characteristics were collected from medical records by experienced physicians, and these characteristics mainly included medical histories, therapies, Doppler echocardiography, peripheral blood parameters and 12-lead electrocardiogram. The twice-entry method was used for data entry. When the values of the two entries were consistent, the data would enter the database; otherwise, the raw data would be checked.
In our clinical medical laboratory center, which is accredited by the American CAP Medical Laboratory, normal ranges of total bilirubin (TBil) and serum albumin are 5.0–28.0 μmol/L and 35–55 g/L, respectively. Based on the literature [6], ALBI score was calculated using the following formula: ALBI score = 0.66*log10TBil (μmol/L) – 0.085*albumin (g/L). Patients were divided into three groups according to the tertiles of baseline ALBI score: tertile 1 (< –3.01), tertile 2 (–3.01 to < 2.71) and tertile 3 (>= –2.71).
2.3. Study outcome
On the basis of the previous studies [27,28,29], the common modes of HCM-related death include: HF-related death, stroke-related death and sudden cardiac death (SCD). Therefore, the study outcome was defined as a composite of the above-mentioned three modes of HCM-related death and other specific HCM-related death. Specially, HF-related death was defined as death preceded by signs and/or symptoms of HF of more than one hour duration, which was in the context of progressive cardiac decompensation more than one year before death [30]. Stroke-related death was defined as a result of probable or proven ischemic stroke [31], without distinguishing cardioembolic stroke from other ischemic subtypes in the present study. SCD was defined as witnessed sudden cardiac death within one hour of new symptoms or nocturnal death in patients who previously experienced a relatively stable or uneventful clinical course [32]. Other specific HCM-related death was defined as death due to HCM, but not in the aforementioned three conditions.
Patients were followed up via telephone interviews or medical records, and followed from the initial evaluation up to the outcomes or the most recent evaluation.
2.4. Statistical analysis
We conducted analyses with the following steps: (1) comparison of descriptive data at baseline; (2) determination of risk-adjusted estimates for HCM-related death, as well as the robustness of risk-adjusted estimates by stratified analysis in various subgroups and E-value analysis, and evaluating accuracy of ALBI score in discriminating HCM-related death at different time points; (3) comparisons of ALBI score versus other parameters of liver function and the HCM risk-SCD score in predicting HCM-related death; (4) exploring whether serial determinations of ALBI score could also predicting HCM-related death in 208 patients who had the second measurement of albumin and TBil. Changes in ALBI score from baseline to the second measurement were expressed by categorical changes and based on the changes in ALBI score across a threshold level (median ALBI score: –2.8), patients were divided into four groups: low-low (patients with ALBI score below the threshold at baseline and the second measurement); low-high (patients with ALBI score below the threshold at baseline and above at the second measurement); high-low (patients with ALBI score above the threshold at baseline and below at the second measurement); high-high (patients with ALBI score above the threshold at baseline and the second measurement); (5) exploring analysis the potential mechanisms why ALBI score could predict HCM-related death.
By the tertiles of ALBI score, continuous variables were presented as mean ± standard deviation or median with interquartile range (IQR) where appropriate, and number (percentage) for categorical variables. For continuous variables, p-value for trend across the three groups was computed from the Pearson test when row-variable was normal distribution and from the Spearman test when it was non-normal distribution. When the row-variable was categorical, p-value for trend was computed from Mantel-Haenszel test of trend.
Survival curves were constructed using Kaplan-Meier estimates, and HCM-related death rates were compared using the log-rank test. For prognostic analysis, Cox proportional hazard regression model was applied. Baseline variables that showed a univariate relationship with HCM-related death (p < 0.05) were entered into the following multivariate Cox regression models 1–4 to evaluate the power of ALBI score predicting HCM-related death from different perspectives: (1) model 1, the basic model, included age and gender; (2) model 2 included the basic model and clinical parameters; (3) model 3 extended model 2 plus laboratory values; (4) model 4 included model 3 and echocardiographic data. For the final model 5, variables for inclusion were carefully chosen, given the number of events available, to ensure parsimony of the final model. The predictors of model 5 were sought using a backward stepwise modeling approach including all variables from models 1 to 4 (except ALBI score). Based on the literature [33], available variables associated HCM-related death in our study were also included in the final model, even if there was no statistical significance in this study. Furthermore, the robustness of the above-mentioned results was assessed by stratified analysis and E-value analysis. Specially, E-value analysis could assess the potential for unmeasured confounding between ALBI score and HCM-related death, and it quantifies the required magnitude of an unmeasured confounder that could negate the observed association between ALBI score and HCM-related death [34]. Meanwhile, a time-dependent receiver operating characteristic (ROC) curve was generated to evaluate the accuracy of ALBI score in discriminating HCM-related death at different time points. A generally accepted approach suggests that an area under the ROC curve (AUC) of less than 0.60 reflects poor discrimination; 0.60 to 0.75, possibly helpful discrimination; and more than 0.75, clearly useful discrimination [35].
Compared with ALBI score, we assessed some other parameters of liver function in predicting HCM-related death, and also evaluated the relationships between HCM risk-SCD score and the study outcome. In addition, we performed exploratory analysis to evaluate whether the changes of ALBI score during the follow-up could predict HCM-related death. Finally, the relationship between ALBI score and other indicators, which have been associated with HCM-related adverse outcomes, was analyzed to explore the potential mechanisms why the score could predict HCM-related death.
All analyses were performed with R version 4.1.0 (R Project for Statistical Computing) including the ‘compareGroups’, ‘rms’, ‘survminer’, ‘tidyverse’, ‘survival’, ‘timeROC’, ‘survivalROC’, ‘forestplot’ and ‘stats’ packages. All tests were two sided, and p values < 0.05 were considered statistically significant.
3. Results
3.1. Baseline characteristics
The present study comprised 462 patients (male: 54.76%) with a median age of 58.00 (IQR: 46.00–67.00) years. ALBI score ranged from –3.83 to –1.05 (median: –2.88, IQR: –3.11 to –2.61). Baseline characteristics of the three groups by the tertiles of ALBI score are summarized in Table 1. ALBI score was positively associated with age, NYHA III-IV, prior thrombo-embolic event, atrial fibrillation, TBil and neutrophil to lymphocyte ratio (NLR) at baseline; and were inversely associated with taking beta blockers, albumin, triglyceride (TG), low density lipoprotein cholesterin, hemoglobin and lymphocyte count at baseline, as well as left ventricular ejection fraction.
Table 1.
Population characteristics by tertiles of baseline ALBI score.
|
| |||||
|---|---|---|---|---|---|
| VARIABLE | ALL | ALBI SCORE | p VALUE FOR TREND | ||
|
| |||||
| TERTILE 1 (< –3.01) | TERTILE 2 (–3.01 to < 2.71) | TERTILE 3 (>= –2.71) | |||
|
| |||||
| No. of patients (n) | 462 | 151 | 152 | 159 | |
|
| |||||
| Gender, male | 253 (54.76%) | 89 (58.94%) | 76 (50.00%) | 88 (55.35%) | 0.540 |
|
| |||||
| Age (years) | 58.00 (46.00, 67.00) | 53.00 (42.00, 66.00) | 56.00 (46.75, 66.00) | 62.00 (49.00, 70.50) | <0.001 |
|
| |||||
| Family history of HCM | 40 (8.66%) | 16 (10.60%) | 12 (7.89%) | 12 (7.55%) | 0.344 |
|
| |||||
| Family history of SCD | 15 (3.25%) | 6 (3.97%) | 6 (3.95%) | 3 (1.89%) | 0.297 |
|
| |||||
| NYHA III-IV | 161 (34.85%) | 47 (31.13%) | 40 (26.32%) | 74 (46.54%) | 0.004 |
|
| |||||
| Symptom | |||||
|
| |||||
| Dyspnea | 257 (55.63%) | 72 (47.68%) | 92 (60.53%) | 93 (58.49%) | 0.059 |
|
| |||||
| Chest pain | 248 (53.68%) | 84 (55.63%) | 87 (57.24%) | 77 (48.43%) | 0.199 |
|
| |||||
| Syncope/pre-syncope | 144 (31.17%) | 44 (29.14%) | 56 (36.84%) | 44 (27.67%) | 0.760 |
|
| |||||
| Palpitation | 174 (37.66%) | 55 (36.42%) | 61 (40.13%) | 58 (36.48%) | 0.999 |
|
| |||||
| Medical history | |||||
|
| |||||
| Prior thrombo-embolic event | 22 (4.76%) | 4 (2.65%) | 3 (1.97%) | 15 (9.43%) | 0.005 |
|
| |||||
| Vascular diseases | 37 (8.01%) | 9 (5.96%) | 13 (8.55%) | 15 (9.43%) | 0.263 |
|
| |||||
| Hypertension | 147 (31.82%) | 54 (35.76%) | 52 (34.21%) | 41 (25.79%) | 0.058 |
|
| |||||
| diabetes | 39 (8.44%) | 10 (6.62%) | 12 (7.89%) | 17 (10.69%) | 0.197 |
|
| |||||
| Atrial fibrillation | 82 (17.75%) | 16 (10.60%) | 25 (16.45%) | 41 (25.79%) | <0.001 |
|
| |||||
| Hepatic disease | 41 (8.87%) | 10 (6.62%) | 14 (9.21%) | 17 (10.69%) | 0.209 |
|
| |||||
| Therapy | |||||
|
| |||||
| Aspirin | 85 (18.40%) | 34 (22.52%) | 24 (15.79%) | 27 (16.98%) | 0.215 |
|
| |||||
| Clopidogrel | 28 (6.06%) | 9 (5.96%) | 10 (6.58%) | 9 (5.66%) | 0.908 |
|
| |||||
| Beta blockers | 334 (72.29%) | 119 (78.81%) | 113 (74.34%) | 102 (64.15%) | 0.004 |
|
| |||||
| ACEI or ARB | 92 (19.91%) | 30 (19.87%) | 32 (21.05%) | 30 (18.87%) | 0.821 |
|
| |||||
| Intervention of obstruction | |||||
|
| |||||
| none | 410 (88.74%) | 132 (87.42%) | 133 (87.50%) | 145 (91.19%) | 0.649 |
|
| |||||
| alcohol septal ablation | 45 (9.74%) | 18 (11.92%) | 17 (11.18%) | 10 (6.29%) | |
|
| |||||
| septal myectomy | 7 (1.52%) | 1 (0.66%) | 2 (1.32%) | 4 (2.52%) | |
|
| |||||
| Device | |||||
|
| |||||
| none | 406 (87.88%) | 135 (89.40%) | 134 (88.16%) | 137 (86.16%) | 0.390 |
|
| |||||
| pacemaker | 21 (4.55%) | 7 (4.64%) | 5 (3.29%) | 9 (5.66%) | |
|
| |||||
| ICD | 35 (7.58%) | 9 (5.96%) | 13 (8.55%) | 13 (8.18%) | |
|
| |||||
| Hematological result | |||||
|
| |||||
| ALT (IU/L) | 22.00 (16.00, 34.00) | 23.00 (17.00, 37.50) | 21.00 (14.00, 29.25) | 23.00 (16.00, 36.50) | 0.482 |
|
| |||||
| AST (IU/L) | 26.00 (21.00, 33.00) | 26.00 (22.00, 32.00) | 24.00 (19.00, 29.25) | 27.00 (21.50, 38.00) | 0.135 |
|
| |||||
| TBil (μmol/L) | 12.35 (9.03, 17.70) | 10.90 (8.50, 13.35) | 12.15 (9.07, 16.92) | 15.00 (10.40, 21.10) | <0.001 |
|
| |||||
| Albumin (g/L) | 42.30 (39.50, 45.00) | 46.10 (44.60, 47.70) | 42.40 (41.60, 43.50) | 38.40 (35.50, 40.00) | <0.001 |
|
| |||||
| Creatinine (μmol/L) | 80.10 (67.00, 94.55) | 81.00 (68.50, 92.50) | 76.00 (65.00, 92.00) | 81.50 (68.10, 100.75) | 0.314 |
|
| |||||
| Urea nitrogen (mmol/L) | 6.04 (5.02, 7.78) | 6.01 (5.18, 7.13) | 5.80 (4.82, 7.38) | 6.41 (5.10, 8.72) | 0.072 |
|
| |||||
| TG (mmol/L) | 1.25 (0.94, 1.87) | 1.57 (1.08, 2.28) | 1.29 (0.99, 1.79) | 1.04 (0.80, 1.40) | <0.001 |
|
| |||||
| HDL-C (mmol/L) | 1.27 (1.03, 1.55) | 1.26 (1.02, 1.58) | 1.30 (1.08, 1.54) | 1.24 (0.96, 1.54) | 0.474 |
|
| |||||
| LDL-C (mmol/L) | 2.41 (1.83, 2.90) | 2.51 (1.91, 2.99) | 2.54 (1.92, 2.95) | 2.23 (1.77, 2.83) | 0.026 |
|
| |||||
| Hgb (g/L) | 136.04 (21.39) | 141.14 (19.70) | 134.88 (19.39) | 132.31 (23.81) | <0.001 |
|
| |||||
| WBCC (109/L) | 6.32 (5.20, 7.78) | 6.60 (5.36, 7.69) | 6.19 (5.28, 7.56) | 6.12 (4.99, 8.21) | 0.152 |
|
| |||||
| Neutrophils count (109/L) | 3.91 (3.04, 5.23) | 4.09 (3.21, 5.19) | 3.77 (3.04, 5.03) | 3.90 (2.95, 6.01) | 0.786 |
|
| |||||
| Lymphocyte count (109/L) | 1.61 (1.26, 1.98) | 1.80 (1.44, 2.27) | 1.61 (1.31, 1.95) | 1.42 (1.04, 1.84) | <0.001 |
|
| |||||
| NLR | 2.30 (1.70, 3.60) | 2.20 (1.60, 3.25) | 2.30 (1.70, 3.42) | 2.80 (1.90, 4.15) | <0.001 |
|
| |||||
| Echocardiographic | |||||
|
| |||||
| LVEDD (mm) | 43.00 (40.00, 46.75) | 44.00 (40.00, 47.00) | 42.50 (40.00, 46.00) | 42.00 (38.50, 47.00) | 0.054 |
|
| |||||
| LA diameter (mm) | 40.00 (35.00, 45.00) | 40.00 (35.00, 44.00) | 39.00 (35.00, 45.00) | 40.00 (36.00, 45.50) | 0.345 |
|
| |||||
| MWT (mm) | 19.00 (17.00, 22.00) | 19.00 (17.00, 22.00) | 19.00 (16.00, 22.00) | 19.00 (17.00, 21.00) | 0.501 |
|
| |||||
| LVEF (%) | 68.00 (63.00, 72.00) | 69.00 (64.00, 73.00) | 68.50 (64.75, 72.00) | 68.00 (62.00, 71.00) | 0.003 |
|
| |||||
| Resting LVOTG >= 30 mm Hg | 198 (42.86%) | 62 (41.06%) | 74 (48.68%) | 62 (38.99%) | 0.694 |
|
| |||||
Note: Values are mean ± SD, median (IQR) or n (%).
Abbreviations: ACEI = angiotensin-converting enzyme inhibitor, ALBI = albumin-bilirubin, ALT = alanine aminotransferase, ARB = angiotensin receptor blocker, AST = aspartate aminotransferase, HCM = hypertrophic cardiomyopathy, HDL-C = high density lipoprotein cholesterin, Hgb = hemoglobin, ICD = implantable cardioverter defibrillator, LA = left atrial, LDL-C = low density lipoprotein cholesterin, LVEDD = left ventricular end-diastolic dimension, LVEF = left ventricular ejection fraction, LVOTG = left ventricular outflow tract gradient, MWT = maximal left ventricular wall thickness, NLR = neutrophil to lymphocyte ratio, NYHA = New York Heart Association, SCD = sudden cardiac death, SD = standard deviation, TBil = total bilirubin, TG = triglyceride, WBCC = white blood cell count.
3.2. Association between ALBI score and HCM-related death
Patients were followed for a median period of 4.7 years (IQR: 2.1–6.8 years; total person-years [PYs]: 2157.9). During the follow-up, 52 patients (11.3%) reached the outcome of HCM-related death, including 26 HF-related deaths, 10 stroke-related deaths, 14 SCDs and 2 HCM-related postoperative deaths. The overall mortality rate was 2.4 (95% CI: 1.8–3.1) per 100 PYs.
Overall, there was a significant positive association between ALBI score and HCM-related death (adjusted HR: 1.79 per one SD increment, 95% CI: 1.36–2.35, p < 0.001) (Figure 1A). When ALBI score was assessed as tertiles, Kaplan-Meier curve showed the clinical course of HCM-related death was significantly worse in the higher tertile (log-rank p < 0.001, Figure 1B). To assess whether the abovementioned relationship might be caused by chance, we further evaluated the relationship between ALBI score and some specific modes of HCM-related death, and the similar results were also found (Figures S1 and S2). Univariate Cox regression analysis indicated that ALBI score and some other variables could predict HCM-related death (Table 2 and Table S1). With the tertile 1 as reference, adjusted HRs for HCM-related death were 1.30 for the tertile 2 (95% CI: 0.42–3.99, p = 0.648) and 4.43 for the tertile 3 (95% CI: 1.65–11.89, p = 0.003), respectively (Table 2).
Figure 1.
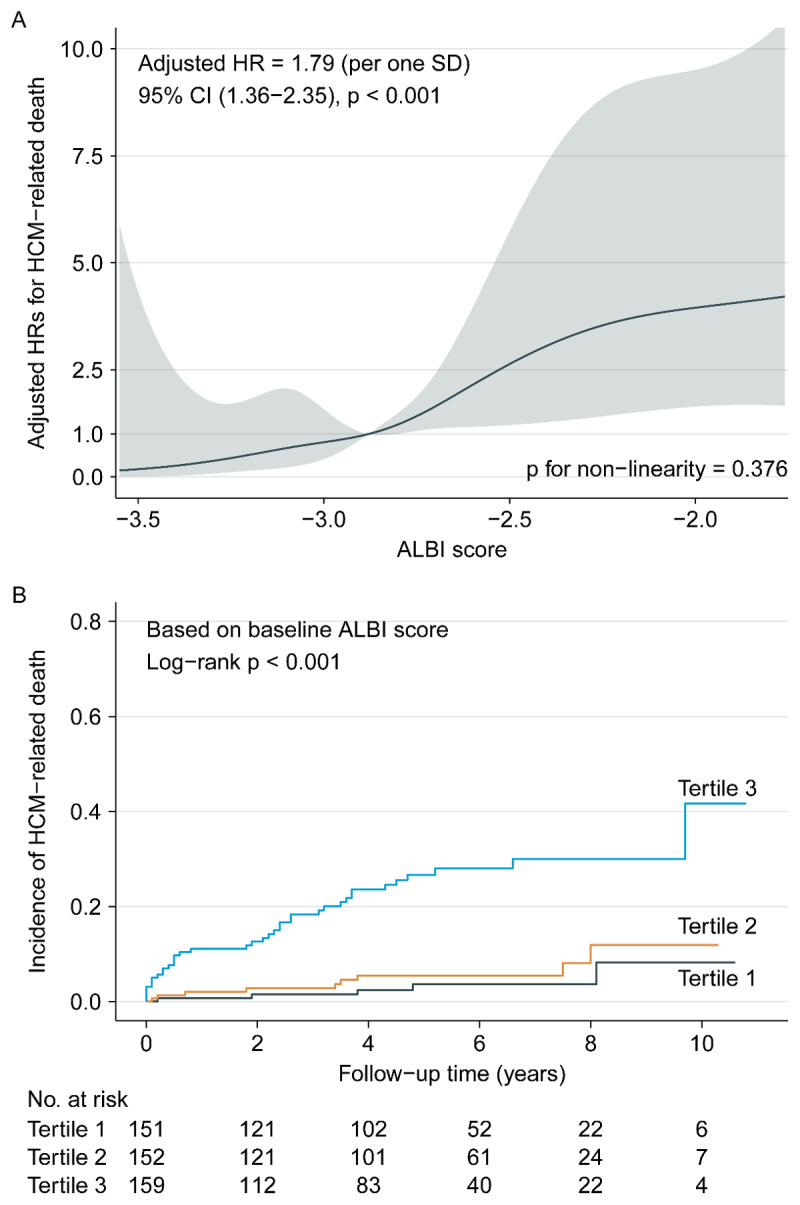
Association between ALBI score and HCM-related death.
Note: (A) smooth curve fitting. HR was adjusted for age, gender, family history of SCD, NYHA III-IV, dyspnea, syncope/pre-syncope, atrial fibrillation, AST, urea nitrogen, TG, NLR, LA diameter, MWT and Resting LVOTG >= 30 mm Hg. The solid line and ribbon depict the HR and 95% CI, respectively. (B) Kaplan-Meier curves.
Table 2.
Associations of ALBI score with HCM-related death.
|
| |||
|---|---|---|---|
| ALBI SCORE | |||
|
| |||
| TERTILE 1 (< –3.01) | TERTILE 2 (–3.01 to < 2.71) | TERTILE 3 (>= –2.71) | |
|
| |||
| No. of patients (n) | 151 | 152 | 159 |
|
| |||
| HCM-related death (n) | 5 | 9 | 38 |
|
| |||
| HF-related death | 2 | 2 | 22 |
|
| |||
| Stroke-related death | 1 | 2 | 7 |
|
| |||
| SCD | 1 | 5 | 8 |
|
| |||
| HCM-related postoperative death | 1 | 0 | 1 |
|
| |||
| Follow-up time (PYs) | 745 | 763.0 | 649.9 |
|
| |||
| Mortality rate for HCM-related death (95% CI)⁎ | 0.7 (0.1–1.3) | 1.2 (0.4–1.9) | 5.8 (4–7.7) |
|
| |||
| Unadjusted HR for HCM-related death (95% CI), p | 1 | 1.78 (0.60–5.32), 0.300 | 8.35 (3.28–21.22), <0.001 |
|
| |||
| Adjusted HR for HCM-related death (95% CI), p | |||
|
| |||
| Model 1 | 1 | 1.73 (0.58–5.17), 0.329 | 8.14 (3.16–20.94), <0.001 |
|
| |||
| Model 2 | 1 | 1.66 (0.55–5.01), 0.368 | 5.96 (2.28–15.55), <0.001 |
|
| |||
| Model 3 | 1 | 1.27 (0.41–3.90), 0.674 | 4.45 (1.66–11.99), 0.003 |
|
| |||
| Model 4 | 1 | 1.27 (0.42–3.89), 0.673 | 4.28 (1.59–11.50), 0.004 |
|
| |||
| Model 5 | 1 | 1.30 (0.42–3.99), 0.648 | 4.43 (1.65–11.89), 0.003 |
|
| |||
Note: Model 1 with adjustment for age and gender.
Model 2 with adjustment for model 1 plus clinical parameters, including NYHA III-IV, dyspnea, prior TE and atrial fibrillation.
Model 3 with adjustment for model 3 plus laboratory results, including AST, urea nitrogen, TG and NLR.
Model 4 with adjustment for model 4 plus echocardiographic parameters, including LA diameter and LVEF.
Model 5 with adjustment for age, gender, family history of SCD, NYHA III-IV, dyspnea, syncope/pre-syncope, atrial fibrillation, AST, urea nitrogen, TG, NLR, LA diameter, MWT and Resting LVOTG >= 30 mm Hg.
⁎Per 100 PYs.
Abbreviations: CI = confidence interval, HRs = hazard ratios, PYs = person-years, other abbreviations as in Table 1.
Due to a similar incidence in HCM-related death, we combined the patients in the tertiles 1 and 2 to construct a new group, namely tertiles 1–2. Then, we further performed stratified analysis in various subgroups (tertile 3 vs. tertiles 1–2) to assess the relationship between ALBI score and the risk of HCM-related death. The results showed that the mortality risk was consistently higher in the tertile 3 than in the tertiles 1–2 in all subgroups (Figure 2). In addition, the E-values for the effects of ALBI score on HCM-related death were 8.33 (lower limit of CI: 2.69) for the tertile 3 and 2.98 (lower limit of CI: 2.06) for the increment of one SD, respectively. This suggested that the main findings should be robust, unless an unmeasured confounder existed with a higher relative risk than the above-mentioned E-values.
Figure 2.
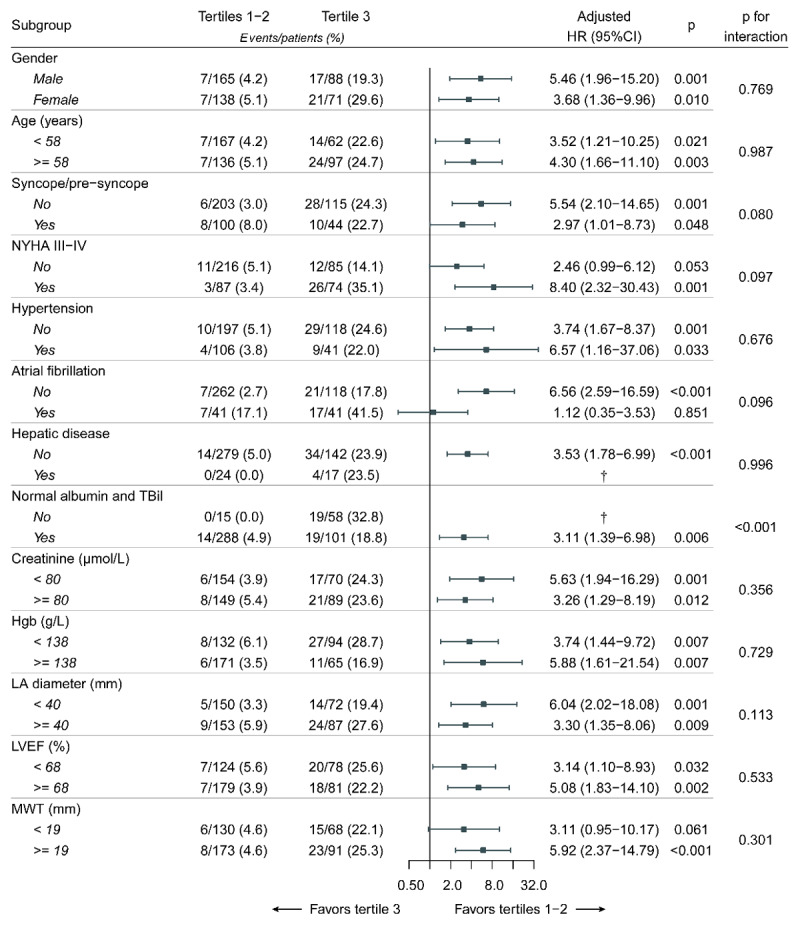
Stratified analyses of HCM-related death.
Note: each stratification was adjusted for age, gender, family history of SCD, NYHA III-IV, dyspnea, syncope/pre-syncope, atrial fibrillation, AST, urea nitrogen, TG, NLR, LA diameter, MWT and Resting LVOTG >= 30 mm Hg, except the stratification factor itself. Grouping criteria of continuous variables were based on the median values. The p value for interaction represents the likelihood of interaction between variable and ALBI score.
† The analyses failed because of no death in the tertiles 1–2.
In addition, hepatic diseases included viral hepatitis (n = 10), alcoholic hepatitis (1), fatty liver (n = 8), diseases of the biliary system (n = 16), liver cirrhosis (n = 2) and unknown reasons (n = 4).
Furthermore, we assessed the discriminative power of ALBI score for HCM-related death at different time points. During the follow-up, time-dependent AUCs ranged from 0.725 to 0.850, indicating a possibly helpful, even clearly useful, discrimination of ALBI score for HCM-related death, and the predictive power was relatively stable at different time points (Figure 3). At 5-year, time-dependent AUC, best threshold of ALBI score, sensitivity and specificity were 0.778, –2.67, 70.8% and 77.5%, respectively; at 10-year, these parameters were 0.780, –2.86, 84.8% and 69.2%, respectively.
Figure 3.
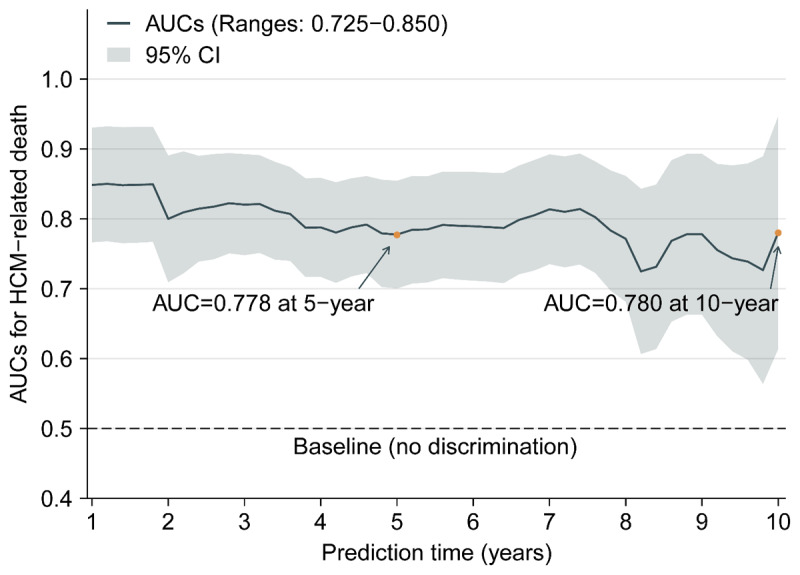
Time-dependent AUCs for ALBI score prdicting HCM-related death.
Note: the curve was calculated every 0.2 years (from 1 to 10 years). In the figure, the solid line depicts the AUCs, and the ribbon represents 95% CI.
3.3. Comparison with other biomarkers of liver function and HCM risk-SCD score
Moreover, we performed the comparisons of ALBI score versus other parameters of liver function, including alanine aminotransferase, aspartate aminotransferase (AST), model for end-stage liver disease-XI and the components of ALBI, in predicting HCM-related death. The results displayed that only albumin and AST were associated with HCM-related death, but weaker than ALBI score (Figure 1A, Figure 3 and Table S2).
HCM risk-SCD is originally used to assess the patients with an increased risk of SCD, and the score provides individualized 5-year risk estimates [23]. There was a complete subgroup (n = 126) with the components of HCM-risk SCD score in our study; therefore, we compared ALBI score with HCM-risk SCD score in predicting HCM-related death and SCD within five years. During the follow-up, 16 patients (12.7%) reached the outcome of HCM-related death, including seven HF-related deaths, one stroke-related deaths and eight SCDs. The results showed ALBI score had a better predictive and discriminative power than HCM risk-SCD score for HCM-related death and SCD (Table S3 and Figure S3).
3.4. Exploratory analysis: prognostic values of the changes of ALBI score for predicting HCM-related death
We also explored whether serial determinations of ALBI score could also provide useful information in predicting HCM-related death. Patients were followed for a median period of 3.6 years (IQR: 1.3–5.9 years), and 28 patients (13.5%) reached the outcome of HCM-related death after the second measurement. Based on the categorical changes, there were 80 patients in the low-low group (3 deaths, mortality rate: 3.8%), 29 in the low-high group (3 deaths, mortality rate: 10.3%), 25 in the high-low group (4 deaths, mortality rate: 16.0%) and 74 in the high-high group (18 deaths, mortality rate: 24.3%), respectively. Kaplan-Meier curve showed the clinical course was significantly worse in the high-high group, and the low-low group had the lowest mortality (log-rank p = 0.002, Figure 4). With the low-low group as reference, adjusted HRs were 2.96 for the low-high group (95% CI: 0.59–14.77, p = 0.186), 4.98 for the high-low group (95% CI: 1.11–22.37, p = 0.036) and 7.68 for the high-high group (95% CI: 2.21–26.69, p = 0.001). Due to the small number of deaths, the above analyses were only adjusted for age and gender.
Figure 4.
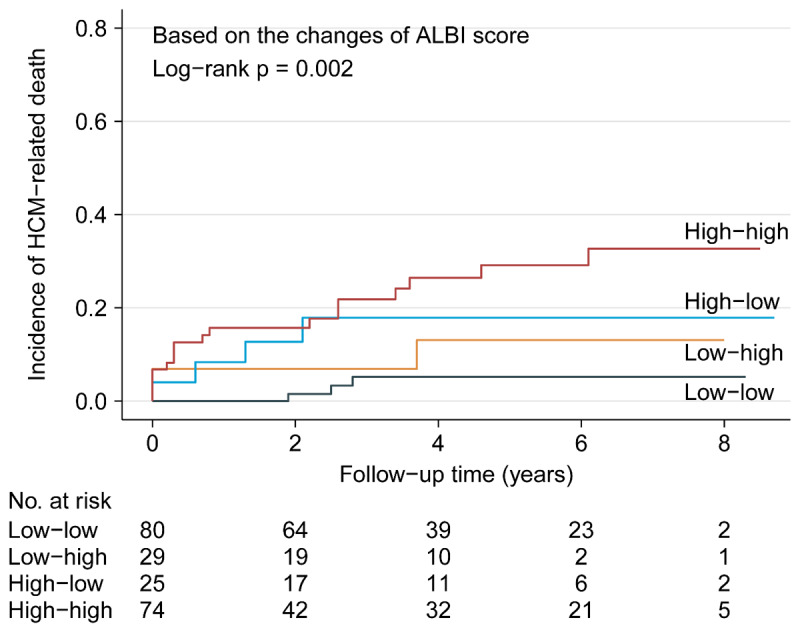
Kaplan-Meier analysis showing cumulative HCM-related death by categorical changes of ALBI score.
3.5. Correlates of ALBI score with other indicators
Some variables for important pathogenetic pathways, as shown in the model 5, in HCM-related adverse outcome were also measured in our cohort. Therefore, we further analyzed the relationship between ALBI score and these variables to explore the potential mechanisms why ALBI score could predict HCM-related death. To assess the complex relationship between these variables and ALBI score, multiple linear regression model was generated based on a stepwise forward selection process (Table 3), indicating that these variables explained approximately 20.3% of the variance of ALBI score, and statistically significant correlates of ALBI score in the model were: inflammation (NLR), myocardial injury (AST), nutritional status (TG) and clinical characteristics (age, NYHA III-IV).
Table 3.
Factors associated with ALBI score in multivariable linear models.
|
| |||
|---|---|---|---|
| β | SE OF β | p VALUE | |
|
| |||
| (Intercept) | –3.074 | 0.170 | <0.001 |
|
| |||
| NLR | 0.015 | 0.003 | <0.001 |
|
| |||
| TG | –0.069 | 0.018 | <0.001 |
|
| |||
| Age | 0.005 | 0.001 | <0.001 |
|
| |||
| AST | 0.001 | 0.000 | 0.001 |
|
| |||
| NYHA III-IV | 0.098 | 0.042 | 0.021 |
|
| |||
| Gender | 0.011 | 0.038 | 0.779 |
|
| |||
| Family history of SCD | –0.161 | 0.103 | 0.118 |
|
| |||
| Dyspnea | 0.039 | 0.040 | 0.327 |
|
| |||
| Syncope/pre-syncope | 0.031 | 0.040 | 0.441 |
|
| |||
| Atrial fibrillation | 0.078 | 0.051 | 0.129 |
|
| |||
| Urea nitrogen | 0.004 | 0.005 | 0.370 |
|
| |||
| LA diameter | –0.002 | 0.003 | 0.568 |
|
| |||
| MWT | –0.004 | 0.004 | 0.354 |
|
| |||
| Resting LVOTG >= 30 mm Hg | –0.002 | 0.039 | 0.951 |
|
| |||
Abbreviations: SE= standard error, other abbreviations as in Tables 1 and S1.
4. Discussion
In the present study, we found higher ALBI score was a strong independent predictor of HCM-related death. Our results fit into the recent series of observations on the predictive role of ALBI score in other CVDs [14,15], and extend these findings in patients with HCM. The potential mechanisms of ALBI score predicting HCM-related death may include multiple pathogenetic processes associated with HCM-related adverse outcome, including inflammation, myocardial injury, nutritional status and some clinical characteristics, but not abnormal cardiac structure and function itself. To our knowledge, this represents the first report of higher ALBI score as a potential prognostic marker for HCM-related death.
In our study, the results showed higher ALBI score could predict HCM-related death. Given the inherent biases of the retrospective study, occasionality cannot be ruled out completely. However, the high level of statistical significance was observed for HCM-related death and the relatively consistent findings across various subgroups minimize this possibility. Meanwhile, we used E-value analysis to quantify the potential implications of unmeasured confounders and found that an unmeasured confounder was unlikely to negate the risk of ALBI score for HCM-related death. Furthermore, exploratory analysis also indicated similar results. Therefore, these features support the validity of our findings.
The mechanisms underlying the association between ALBI score and HCM-related death are not clearly determined. Whereas, the present findings seemingly suggested the potential mechanisms might be out of abnormal cardiac structure and function itself, and the mechanisms may include multiple pathogenetic processes associated with HCM-related adverse outcome, including inflammation, myocardial injury, nutritional status and some clinical characteristics. Firstly, accumulating evidence suggests the existence of low-grade systemic [36,37,38] and local inflammation [18,21,22] in HCM, further resulting in adverse ventricular remodeling [22], and elevated high-sensitivity C-reactive protein has been significantly associated with increased risk of adverse outcomes in HCM [39]. Some other studies have also shown oxidative stress may be involved in the pathogenesis in HCM [19,20,40]. As a component of ALBI score, bilirubin has anti-inflammatory and antioxidant effects [12,41]; therefore, high level of bilirubin might be a reflection of increased chronic inflammation and oxidative stress. In addition, serum albumin is also a marker of inflammation and oxidative stress [42,43]. Therefore, the combination of the two indicators should be associated with inflammation and oxidative stress. In the present study, ALBI score was associated with NLR, which has been accepted as a novel marker indicating inflammation and oxidative stress [44,45], further supporting ALBI score should be a marker of inflammation and oxidative stress. Thus, based on these literature data and the novel observations of this study, inflammation and oxidative stress may be one of the potential mechanisms that ALBI score could predict HCM-related death. Secondly, recent studies have shown that cardiac troponin, an important marker of myocardial injury, is commonly elevated in HCM, and could predict the prognosis in HCM [46,47]. Myocardial injury may be caused by inappropriate cardiac hypertrophy [46] and microvascular dysfunction [48] in HCM. Currently, serum albumin and bilirubin have exerted anti-thrombotic activity [17,49] and protection of vascular endothelial cells [12,50]; therefore, abnormal serum albumin and bilirubin can deteriorate vascular function in HCM, further causing subsequent adverse outcomes. In our study, AST was designated as a marker of myocardial injury for lacking of cardiac troponin, and some studies have shown AST is associated with poor outcomes in HCM [51,52]. Our findings suggested ALBI score was associated with AST, indicating that the score may be related to myocardial injury. Therefore, myocardial injury could be another potential mechanism. Thirdly, TG is an indicator of nutritional status, and was in significant relationship with ALBI score in our study; meanwhile, albumin itself is also a marker of nutritional status. Undernutrition has been an independent prognostic factor for mortality in HCM [24]. Furthermore, ALBI score was also associated with some clinical characteristics, including age and NYHA III-IV, which can predict poor outcomes in HCM [23,30]. Taken together, it is plausible to hypothesize that ALBI score is a good integrative marker of complex clinical settings in HCM, including inflammation, myocardial injury, nutritional status and some clinical characteristics. These literature data and the novel observations of this study may help to understand why higher ALBI score is a powerful predictor for HCM-related death. Finally, the echocardiographic data was not associated with ALBI score in our study; even so, the relationship between the score and cardiac structure in HCM is still not ruled out completely. Echocardiography has inherent limitations than other imageological examinations, such as cardiac magnetic resonance (CMR), and Kuusisto J et al. [21] have described that circulatory inflammatory markers were associated with late gadolinium enhancement by CMR. Therefore, more researches are needed.
The study has several limitations. Firstly, this was a single center, retrospective study, and those patients were from China, lack of region diversification and race comparison. Secondly, since the study was performed at a tertiary referral hospital, which might have resulted in certain inherent selection biases. Thirdly, data about the drugs associated with albumin and TBil was missed. Fourthly, the study failed to perform CMR, and the measure may further help to explain the relation between ALBI score and adverse outcomes in HCM. Fifthly, the study failed to exclude patients with coronary heart disease and measure cardiac troponin, which may partly affect the exploratory analysis of potential mechanisms. Finally, we could not collect some known markers for HCM-related death, which might partly result in the biases of the results. While, E-value analysis could suggest the robustness of the findings in some degree. In spite of the above, our results are still able to clearly indicate that higher ALBI score is a risk factor of HCM-related death.
5. Conclusion
In summary, higher ALBI score is a strong independent predictor of HCM-related death, and the patients with higher ALBI score may warrant closer follow-up and more aggressive therapy with hopefully prevention of events in the future. Meanwhile, the present findings seemingly suggest the potential mechanisms of ALBI score predicting HCM-related death are out of abnormal cardiac structure and function itself, and the mechanisms may include multiple pathogenetic processes associated with HCM-related adverse outcome, including inflammation, myocardial injury, nutritional status and some clinical characteristics. In the future, more studies are needed to assess the association between ALBI score and outcome to better risk-stratify patients with HCM. Furthermore, it is unclear whether intervention of ALBI score, namely managing low serum albumin and high TBil, can improve the outcomes of HCM, but the exploratory analysis gives us some hints. The clinical significance of ALBI score deserves further investigations in patients with HCM.
Data Accessibility Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional Files
The additional files for this article can be found as follows:
Figures S1 to S3.
Tables S1 to S3.
Acknowledgements
We thank all staff members for data collection, data entry and monitoring as part of this study and all Funding Sources.
Funding Statement
The study was supported by Sichuan Science and Technology Program, China (Grant No. 2022YFS0186), and the National Natural Science Foundation of China (Grant No. 81600299).
Contributor Information
Yi Zheng, Email: drzhengyi1979@163.com.
Sen He, Email: hesensubmit@163.com.
Funding Information
The study was supported by Sichuan Science and Technology Program, China (Grant No. 2022YFS0186), and the National Natural Science Foundation of China (Grant No. 81600299).
Competing Interests
The authors have no competing interests to declare.
Authors Contributions
Ping Qiao and Liying Li: Data curation, Writing- Original draft preparation, Manuscript revise
Ziqiong Wang, Muxin Zhang, Haiyan Ruan and Xinran Li: Data curation, Software
Rufeng Shi, Xin Wei and Linjia Duan: Software, Validation, Investigation
Sen He and Yi Zheng: Writing- Reviewing, Funding acquisition
Sen He and Yi Zheng contributed equally to the article.
References
- 1.Maron BJ. Clinical Course and Management of Hypertrophic Cardiomyopathy. N Engl J Med. 2018; 379(7): 655–68. DOI: 10.1056/NEJMra1710575 [DOI] [PubMed] [Google Scholar]
- 2.Maron BJ, Maron MS, Rowin EJ. Perspectives on the Overall Risks of Living With Hypertrophic Cardiomyopathy. Circulation. 2017; 135(24): 2317–9. DOI: 10.1161/CIRCULATIONAHA.117.027738 [DOI] [PubMed] [Google Scholar]
- 3.Ho CY, Day SM, Ashley EA, Michels M, Pereira AC, Jacoby D, et al. Genotype and Lifetime Burden of Disease in Hypertrophic Cardiomyopathy: Insights from the Sarcomeric Human Cardiomyopathy Registry (SHaRe). Circulation. 2018; 138(14): 1387–98. DOI: 10.1161/CIRCULATIONAHA.117.033200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pujades-Rodriguez M, Guttmann OP, Gonzalez-Izquierdo A, Duyx B, O’Mahony C, Elliott P, et al. Identifying unmet clinical need in hypertrophic cardiomyopathy using national electronic health records. PLoS One. 2018; 13(1): e0191214. DOI: 10.1371/journal.pone.0191214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lorenzini M, Anastasiou Z, O’Mahony C, Guttman OP, Gimeno JR, Monserrat L, et al. Mortality Among Referral Patients with Hypertrophic Cardiomyopathy vs the General European Population. JAMA Cardiol. 2020; 5(1): 73–80. DOI: 10.1001/jamacardio.2019.4534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johnson PJ, Berhane S, Kagebayashi C, Satomura S, Teng M, Reeves HL, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015; 33(6): 550–8. DOI: 10.1200/JCO.2014.57.9151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abdel-Rahman O. Prognostic Value of Baseline ALBI Score Among Patients with Colorectal Liver Metastases: A Pooled Analysis of Two Randomized Trials. Clin Colorectal Cancer. 2019; 18(1): e61–e8. DOI: 10.1016/j.clcc.2018.09.008 [DOI] [PubMed] [Google Scholar]
- 8.Bernardi N, Chedid MF, Grezzana-Filho TJM, Chedid AD, Pinto MA, Leipnitz I, et al. Pre-transplant ALBI Grade 3 Is Associated with Increased Mortality After Liver Transplantation. Dig Dis Sci. 2019; 64(6): 1695–704. DOI: 10.1007/s10620-019-5456-6 [DOI] [PubMed] [Google Scholar]
- 9.Oikonomou T, Goulis L, Doumtsis P, Tzoumari T, Akriviadis E, Cholongitas E. ALBI and PALBI Grades Are Associated with the Outcome of Patients with Stable Decompensated Cirrhosis. Ann Hepatol. 2019; 18(1): 126–36. DOI: 10.5604/01.3001.0012.7904 [DOI] [PubMed] [Google Scholar]
- 10.Imamura T, Okamura Y, Sugiura T, Ito T, Yamamoto Y, Ashida R, et al. Clinical Significance of Preoperative Albumin-Bilirubin Grade in Pancreatic Cancer. Ann Surg Oncol. 2021. DOI: 10.1245/s10434-021-09593-9 [DOI] [PubMed] [Google Scholar]
- 11.Kim MS, Kato TS, Farr M, Wu C, Givens RC, Collado E, et al. Hepatic dysfunction in ambulatory patients with heart failure: application of the MELD scoring system for outcome prediction. J Am Coll Cardiol. 2013; 61(22): 2253–61. DOI: 10.1016/j.jacc.2012.12.056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Boon AC, Bulmer AC, Coombes JS, Fassett RG. Circulating bilirubin and defense against kidney disease and cardiovascular mortality: mechanisms contributing to protection in clinical investigations. Am J Physiol Renal Physiol. 2014; 307(2): F123–36. DOI: 10.1152/ajprenal.00039.2014 [DOI] [PubMed] [Google Scholar]
- 13.Targher G, Byrne CD. Circulating Markers of Liver Function and Cardiovascular Disease Risk. Arterioscler Thromb Vasc Biol. 2015; 35(11): 2290–6. DOI: 10.1161/ATVBAHA.115.305235 [DOI] [PubMed] [Google Scholar]
- 14.Kawata T, Ikeda A, Masuda H, Komatsu S. Association Between Albumin-Bilirubin Score at Admission and In-Hospital Mortality in Patients with Acute Heart Failure. Int Heart J. 2021; 62(4): 829–36. DOI: 10.1536/ihj.21-080 [DOI] [PubMed] [Google Scholar]
- 15.Matsue Y, Kagiyama N, Yamaguchi T, Kuroda S, Okumura T, Kida K, et al. Clinical and Prognostic Values of ALBI Score in Patients with Acute Heart Failure. Heart Lung Circ. 2020; 29(9): 1328–37. DOI: 10.1016/j.hlc.2019.12.003 [DOI] [PubMed] [Google Scholar]
- 16.Kunutsor SK, Bakker SJ, Gansevoort RT, Chowdhury R, Dullaart RP. Circulating total bilirubin and risk of incident cardiovascular disease in the general population. Arterioscler Thromb Vasc Biol. 2015; 35(3): 716–24. DOI: 10.1161/ATVBAHA.114.304929 [DOI] [PubMed] [Google Scholar]
- 17.Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018; 52: 8–12. DOI: 10.1016/j.ejim.2018.04.014 [DOI] [PubMed] [Google Scholar]
- 18.Lamke GT, Allen RD, Edwards WD, Tazelaar HD, Danielson GK. Surgical pathology of subaortic septal myectomy associated with hypertrophic cardiomyopathy. Cardiovascular Pathology. 2003; 12(3): 149–58. DOI: 10.1016/S1054-8807(03)00036-X [DOI] [PubMed] [Google Scholar]
- 19.Nakamura K, Kusano KF, Matsubara H, Nakamura Y, Miura A, Nishii N, et al. Relationship Between Oxidative Stress and Systolic Dysfunction in Patients with Hypertrophic Cardiomyopathy. Journal of Cardiac Failure. 2005; 11(2): 117–23. DOI: 10.1016/j.cardfail.2004.05.005 [DOI] [PubMed] [Google Scholar]
- 20.Dimitrow PP, Undas A, Wołkow P, Tracz W, Dubiel JS. Enhanced oxidative stress in hypertrophic cardiomyopathy. Pharmacological Reports. 2009; 61(3): 491–5. DOI: 10.1016/S1734-1140(09)70091-X [DOI] [PubMed] [Google Scholar]
- 21.Kuusisto J, Karja V, Sipola P, Kholova I, Peuhkurinen K, Jaaskelainen P, et al. Low-grade inflammation and the phenotypic expression of myocardial fibrosis in hypertrophic cardiomyopathy. Heart. 2012; 98(13): 1007–13. DOI: 10.1136/heartjnl-2011-300960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Becker RC, Owens AP, 3rd, Sadayappan S. Tissue-level inflammation and ventricular remodeling in hypertrophic cardiomyopathy. J Thromb Thrombolysis. 2020; 49(2): 177–83. DOI: 10.1007/s11239-019-02026-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Authors/Task Force m, Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014; 35(39): 2733–79. DOI: 10.1093/eurheartj/ehu284 [DOI] [PubMed] [Google Scholar]
- 24.Wang Z, Zhao L, He S. Prognostic nutritional index and the risk of mortality in patients with hypertrophic cardiomyopathy. Int J Cardiol. 2021; 331: 152–7. DOI: 10.1016/j.ijcard.2021.01.023 [DOI] [PubMed] [Google Scholar]
- 25.Liao H, Wang Z, Zhao L, Chen X, He S. Myocardial contraction fraction predicts mortality for patients with hypertrophic cardiomyopathy. Sci Rep. 2020; 10(1): 17026. DOI: 10.1038/s41598-020-72712-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.He S, Wang Z, Cheem TH, Liao H, Chen X, He Y. External Validation of the Model of Thromboembolic Risk in Hypertrophic Cardiomyopathy Patients. Can J Cardiol. 2019; 35(12): 1800–6. DOI: 10.1016/j.cjca.2019.05.035 [DOI] [PubMed] [Google Scholar]
- 27.Ho HH, Lee KL, Lau CP, Tse HF. Clinical characteristics of and long-term outcome in Chinese patients with hypertrophic cardiomyopathy. Am J Med. 2004; 116(1): 19–23. DOI: 10.1016/j.amjmed.2003.09.020 [DOI] [PubMed] [Google Scholar]
- 28.Lee CH, Liu PY, Lin LJ, Chen JH, Tsai LM. Clinical characteristics and outcomes of hypertrophic cardiomyopathy in Taiwan--a tertiary center experience. Clin Cardiol. 2007; 30(4): 177–82. DOI: 10.1002/clc.20057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Songsirisuk N, Kittipibul V, Methachittiphan N, Charoenattasil V, Zungsontiporn N, Spanuchart I, et al. Modes of death and clinical outcomes in adult patients with hypertrophic cardiomyopathy in Thailand. BMC Cardiovascular Disorders. 2019; 19(1). DOI: 10.1186/s12872-018-0984-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Coats CJ, Gallagher MJ, Foley M, O’Mahony C, Critoph C, Gimeno J, et al. Relation between serum N-terminal pro-brain natriuretic peptide and prognosis in patients with hypertrophic cardiomyopathy. Eur Heart J. 2013; 34(32): 2529–37. DOI: 10.1093/eurheartj/eht070 [DOI] [PubMed] [Google Scholar]
- 31.Haruki S, Minami Y, Hagiwara N. Stroke and Embolic Events in Hypertrophic Cardiomyopathy: Risk Stratification in Patients Without Atrial Fibrillation. Stroke. 2016; 47(4): 936–42. DOI: 10.1161/STROKEAHA.115.012130 [DOI] [PubMed] [Google Scholar]
- 32.Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A, et al. Sudden death in hypertrophic cardiomyopathy: identification of high-risk patients. J Am Coll Cardiol. 2000; 36(7): 2212–8. DOI: 10.1016/S0735-1097(00)01003-2 [DOI] [PubMed] [Google Scholar]
- 33.Liu Q, Li D, Berger AE, Johns RA, Gao L. Survival and prognostic factors in hypertrophic cardiomyopathy: a meta-analysis. Sci Rep. 2017; 7(1): 11957. DOI: 10.1038/s41598-017-12289-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Haneuse S, VanderWeele TJ, Arterburn D. Using the E-Value to Assess the Potential Effect of Unmeasured Confounding in Observational Studies. JAMA. 2019; 321(6): 602–3. DOI: 10.1001/jama.2018.21554 [DOI] [PubMed] [Google Scholar]
- 35.Alba AC, Agoritsas T, Walsh M, Hanna S, Iorio A, Devereaux PJ, et al. Discrimination and Calibration of Clinical Prediction Models: Users’ Guides to the Medical Literature. JAMA. 2017; 318(14): 1377–84. DOI: 10.1001/jama.2017.12126 [DOI] [PubMed] [Google Scholar]
- 36.Hogye M, Mandi Y, Csanady M, Sepp R, Buzas K. Comparison of circulating levels of interleukin-6 and tumor necrosis factor-alpha in hypertrophic cardiomyopathy and in idiopathic dilated cardiomyopathy. Am J Cardiol. 2004; 94(2): 249–51. DOI: 10.1016/j.amjcard.2004.03.078 [DOI] [PubMed] [Google Scholar]
- 37.Zen K, Irie H, Doue T, Takamiya M, Yamano T, Sawada T, et al. Analysis of circulating apoptosis mediators and proinflammatory cytokines in patients with idiopathic hypertrophic cardiomyopathy: comparison between nonobstructive and dilated-phase hypertrophic cardiomyopathy. Int Heart J. 2005; 46(2): 231–44. DOI: 10.1536/ihj.46.231 [DOI] [PubMed] [Google Scholar]
- 38.Iwasaki J, Nakamura K, Matsubara H, Nakamura Y, Nishii N, Banba K, et al. Relationship between circulating levels of monocyte chemoattractant protein-1 and systolic dysfunction in patients with hypertrophic cardiomyopathy. Cardiovasc Pathol. 2009; 18(6): 317–22. DOI: 10.1016/j.carpath.2008.12.004 [DOI] [PubMed] [Google Scholar]
- 39.Zhu L, Zou Y, Wang Y, Luo X, Sun K, Wang H, et al. Prognostic Significance of Plasma High-Sensitivity C-Reactive Protein in Patients with Hypertrophic Cardiomyopathy. J Am Heart Assoc. 2017; 6(2). DOI: 10.1161/JAHA.116.004529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Christiansen LB, Dela F, Koch J, Hansen CN, Leifsson PS, Yokota T. Impaired cardiac mitochondrial oxidative phosphorylation and enhanced mitochondrial oxidative stress in feline hypertrophic cardiomyopathy. Am J Physiol Heart Circ Physiol. 2015; 308(10): H1237–47. DOI: 10.1152/ajpheart.00727.2014 [DOI] [PubMed] [Google Scholar]
- 41.Brites D. Bilirubin injury to neurons and glial cells: new players, novel targets, and newer insights. Semin Perinatol. 2011; 35(3): 114–20. DOI: 10.1053/j.semperi.2011.02.004 [DOI] [PubMed] [Google Scholar]
- 42.Wiedermann CJ. Anti-inflammatory activity of albumin. Crit Care Med. 2007; 35(3): 981–2; author reply 2–3. DOI: 10.1097/01.CCM.0000257234.87784.91 [DOI] [PubMed] [Google Scholar]
- 43.Roche M, Rondeau P, Singh NR, Tarnus E, Bourdon E. The antioxidant properties of serum albumin. FEBS Lett. 2008; 582(13): 1783–7. DOI: 10.1016/j.febslet.2008.04.057 [DOI] [PubMed] [Google Scholar]
- 44.Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther. 2016; 14(5): 573–7. DOI: 10.1586/14779072.2016.1154788 [DOI] [PubMed] [Google Scholar]
- 45.Katipoglu Z, Mirza E, Oltulu R, Katipoglu B. May Monocyte/HDL Cholesterol Ratio (MHR) and Neutrophil/Lymphocyte Ratio (NLR) Be an Indicator of Inflammation and Oxidative Stress in Patients with Keratoconus? Ocul Immunol Inflamm. 2020; 28(4): 632–6. DOI: 10.1080/09273948.2019.1611876 [DOI] [PubMed] [Google Scholar]
- 46.Kubo T, Kitaoka H, Yamanaka S, Hirota T, Baba Y, Hayashi K, et al. Significance of high-sensitivity cardiac troponin T in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2013; 62(14): 1252–9. DOI: 10.1016/j.jacc.2013.03.055 [DOI] [PubMed] [Google Scholar]
- 47.Kehl DW, Buttan A, Siegel RJ, Rader F. Clinical utility of natriuretic peptides and troponins in hypertrophic cardiomyopathy. Int J Cardiol. 2016; 218: 252–8. DOI: 10.1016/j.ijcard.2016.05.031 [DOI] [PubMed] [Google Scholar]
- 48.Tardiff JC, Carrier L, Bers DM, Poggesi C, Ferrantini C, Coppini R, et al. Targets for therapy in sarcomeric cardiomyopathies. Cardiovascular Research. 2015; 105(4): 457–70. DOI: 10.1093/cvr/cvv023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kundur AR, Singh I, Bulmer AC. Bilirubin, platelet activation and heart disease: a missing link to cardiovascular protection in Gilbert’s syndrome? Atherosclerosis. 2015; 239(1): 73–84. DOI: 10.1016/j.atherosclerosis.2014.12.042 [DOI] [PubMed] [Google Scholar]
- 50.Iba T, Hamakubo T, Nagaoka I, Sato K, Thachil J. Physiological Levels of Pentraxin 3 and Albumin Attenuate Vascular Endothelial Cell Damage Induced by Histone H3 In Vitro. Microcirculation. 2016; 23(3): 240–7. DOI: 10.1111/micc.12269 [DOI] [PubMed] [Google Scholar]
- 51.McCullough SA, Fifer MA, Mohajer P, Lowry PA, Reen CO, Baggish AL, et al. Clinical Correlates and Prognostic Value of Elevated Right Atrial Pressure in Patients with Hypertrophic Cardiomyopathy. Circ J. 2018; 82(5): 1405–11. DOI: 10.1253/circj.CJ-17-0959 [DOI] [PubMed] [Google Scholar]
- 52.Lee HJ, Kim HK, Kim M, Moon I, Lee H, Kim BS, et al. Clinical impact of atrial fibrillation in a nationwide cohort of hypertrophic cardiomyopathy patients. Ann Transl Med. 2020; 8(21): 1386. DOI: 10.21037/atm-20-1817 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figures S1 to S3.
Tables S1 to S3.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.