

Abstract
Introduction
Ultrasound assessment of fetuses subjected to hyperglycemia is recommended but, apart from increased size, little is known about its interpretation, and the identification of which large fetuses of diabetic pregnancy are at risk is unclear. Newer markers of adverse outcomes, abdominal circumference growth velocity and cerebro‐placental ratio, help to predict risk in non‐diabetic pregnancy. Our study aims to assess their role in pregnancies complicated by diabetes.
Material and methods
This is a retrospective analysis of a cohort of singleton, non‐anomalous fetuses of women with pre‐existing or gestational diabetes mellitus, and estimated fetal weight at the 10th centile or above. Gestational diabetes was diagnosed by selective screening of at risk groups. A universal ultrasound scan was offered at 20 and 36 weeks of gestation. Estimated fetal weight, abdominal circumference growth velocity, presence of polyhydramnios, and cerebro‐placental ratio were evaluated at the 36‐week scan. A composite adverse outcome was defined as the presence of one or more of perinatal death, arterial cord pH less than 7.1, admission to Neonatal Unit, 5‐minute Apgar less than 7, severe hypoglycemia, or cesarean section for fetal compromise. A chi‐squared test was used to test the association of estimated fetal weight at the 90th centile or above, polyhydramnios, abdominal circumference growth velocity at the 90th centile or above, and cerebro‐placental ratio at the 5th centile or below with the composite outcome. Logistic regression was used to assess which ultrasound markers were independent risk factors. Odds ratios of composite adverse outcome with combinations of independent ultrasound markers were calculated.
Results
A total of 1044 pregnancies were included, comprising 87 women with pre‐existing diabetes mellitus and 957 with gestational diabetes. Estimated fetal weight at the 90th centile or above, abdominal circumference growth velocity at the 90th centile or above, cerebro‐placental ratio at the 5th centile or below, but not polyhydramnios, were significantly associated with adverse outcomes: odds ratios (95% confidence intervals) 1.85 (1.21–2.84), 1.54 (1.02–2.31), 1.92 (1.21–3.30), and 1.53 (0.79–2.99), respectively. Only estimated fetal weight at the 90th centile or above and cerebro‐placental ratio at the 5th centile or below were independent risk factors. The greatest risk (odds ratio 6.85, 95% confidence interval 2.06–22.78) was found where both the estimated fetal weight is at the 90th centile or above and the cerebro‐placental ratio is at the 5th centile or below.
Conclusions
In diabetic pregnancies, a low cerebro‐placental ratio, particularly in a macrosomic fetus, confers additional risk.
Keywords: diabetes in pregnancy, fetal Doppler, cerebro‐placental ratio, fetal growth, estimated fetal weight
Abbreviations
- ACGV
abdominal circumference growth velocity
- CAO
composite adverse outcome
- CPR
cerebro‐placental ratio
- CS
cesarean section
- DM
diabetes mellitus
- EFW
estimated fetal weight
- GDM
gestational diabetes mellitus
- MCA
middle cerebral artery
- OR
odds ratio
- PI
pulsatility index
- Umb A
umbilical artery.
Key message.
In hyperglycemic pregnancies, large for dates and low cerebro‐placental ratio are independent and mutually enhancing risk factors for adverse perinatal outcome. It is the low cerebro‐placental ratio and not the abdominal circumference growth acceleration that predicts those large fetuses at most risk.
1. INTRODUCTION
Pre‐existing diabetes mellitus (DM) and gestational diabetes (GDM) are associated with adverse pregnancy outcomes. 1 These include, particularly with DM, perinatal mortality and morbidity related to poor placental function, 2 and to mechanical issues such as cesarean section (CS) or shoulder dystocia, in addition to long‐term sequelae. 1 Prevention primarily involves (1) glycemic control and (2) optimization of the time and method of birth, balancing the increased risks of preterm or early term birth against the risks of mortality and morbidity. 1
The most established manifestation of poor placental function is being small for gestational age. Methods are established to determine those at most risk. Yet fetuses subject to hyperglycemia, despite their increased risk, tend to be larger. 3 Hyperinsulinemia increases size and the effects of poor placental function are potentially masked. 2 Increased size appears to correlate with increased risk and is the only established ultrasound risk factor. 1 , 4 Regular ultrasound assessment of fetuses is recommended, but has moderate sensitivity and specificity for size, and poor predictive value for adverse outcomes. 1 , 4 The identification of which large fetuses of diabetic pregnancy are at most risk is even less clear. The American College of Obstetricians and Gynecologists (2018) states only that fetal umbilical artery (Umb A) Doppler may be useful in monitoring babies with fetal growth restriction. 1 This means that for the majority of diabetic pregnancies, fetal Doppler, so crucial to timing birth in other at‐risk pregnancies, has a little known role.
Recent analyses have examined ultrasound markers of placental function other than size. Fetal growth rate, as measured by the abdominal circumference growth velocity (ACGV), adds to the prediction of adverse outcomes in both small and large fetuses. 5 Equally, the ratio of Umb A to middle cerebral artery (MCA) pulsatility index (PI) (cerebro‐placental ratio [CPR]) is a predictor of adverse outcomes in appropriate‐for‐gestational‐age fetuses as well as in small‐for‐gestational‐age ones. 6
The aim of this paper is to assess the role of ACGV and CPR as markers of placental function, in predicting adverse perinatal outcome in pregnancies with GDM or pre‐existing DM.
2. MATERIAL AND METHODS
This is a retrospective analysis of all women with singleton pregnancies and diagnosed with GDM or pre‐existing DM, with an estimated delivery date between October 2016 and September 2019, who delivered from 35+0 completed weeks in a single large UK maternity unit. All except in vitro fertilization pregnancies were dated using crown‐rump length before 14 weeks or by head circumference between 14+0 and 18+0 weeks. The selection of the cohort is shown in Figure 1. All women underwent routine ultrasound with biometry between 18+0 and 21+6 weeks and a scan for fetal biometry, liquor volume assessment, and Umb A and MCA Doppler at 31+0–32+6 weeks and at 35+0–36+6 weeks. Pregnancies complicated by fetal abnormality or aneuploidy or those where a scan with full biometry had not also been performed were excluded. We also excluded fetuses with an estimated fetal weight (EFW) below the 10th centile because of their rarity and because, with GDM their management is largely irrespective of hyperglycemia. 7
FIGURE 1.
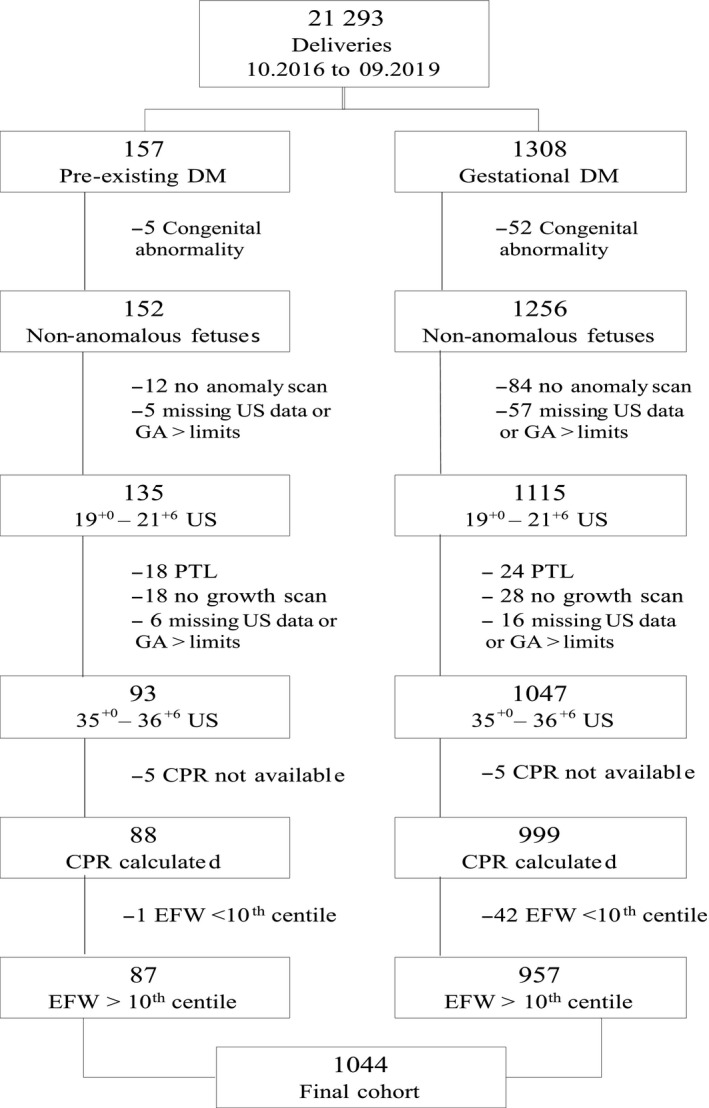
Flow diagram of the cohort selection. CPR, cerebro‐placental ratio; DM, diabetes mellitus; EFW, estimated fetal weight; GA, gestational age; PTL, preterm labor; US, ultrasound
The diagnosis of GDM was made using screening of at‐risk groups, according to National Institute for Health and Care Excellence criteria: body mass index greater than 30 kg/m2, previous macrosomic baby, previous gestational diabetes, family history of diabetes in a first‐degree relative, or ethnicity with a high prevalence of diabetes. 8 A 75‐g glucose tolerance test was administered between 24 and 30 weeks and, in addition, before 20 weeks in those with a history of GDM: hyperglycemia was diagnosed according to International Association of Diabetes in Pregnancy Study Group criteria. 9
Ultrasound examinations were carried out by accredited sonographers using Voluson E6 and E8 ultrasound machines (GE Healthcare) with a 2‐ to 8‐Hz convex probe. Measurements were recorded prospectively using archiving software (viewpoint, GE Healthcare) and transferred using DICOM. Doppler measurements were obtained according to International Society of Ultrasound in Obstetrics and Gynecology guidelines. 10 The EFW was calculated using Hadlock's 1985 equation. 11
Management was in a specialist clinic with multidisciplinary input from diabetologists, dieticians, obstetricians, and midwives. Glucose levels of those with GDM were monitored remotely using an app (GDm‐Health; Sensynehealth.com) and dietary modification and exercise advice; also, if appropriate, oral metformin and subcutaneous insulin were used. Women with pre‐existing diabetes were also monitored remotely. Target glucoses were less than 5.3 mmo/L (fasting) and less than 7.8 mmol/L (1 h postprandial).
Fetuses were defined as appropriate for gestational age when EFW was at the 10th centile or above and less than the 90th centile, and large for gestational age when EFW was at the 90th centile or above, according to Hadlock et al. 12 An ACGV above the 90th centile was calculated according to Vannuccini et al. 13 CPR was calculated as the ratio of the MCA PI to the Umb A PI and a CPR below the 5th centile was defined according to Ciobanu et al. 14 Polyhydramnios was defined as a deepest vertical pool of more than 8.0 cm. 15
Data were routinely collected prospectively and were merged according to a unique identifier from neonatal (Badgernet), maternity (Cerner), and ultrasound (Viewpoint, GE Healthcare) records.
The composite adverse outcome (CAO) was defined as the presence of at least one of perinatal death, arterial cord pH less than 7.1, admission to Neonatal Unit, 5‐minute Apgar score less than 7, severe hypoglycemia requiring treatment, or CS for suspected fetal compromise.
We considered the following ultrasound markers: EFW above or equal to the 90th centile, polyhydramnios, ACGV above or equal to the 90th centile and CPR below or equal to the 5th centile. A chi‐squared test, generating odds ratios (OR) with 95% confidence intervals (CI), was used to test their association with the CAO. Logistic regression was used to determine which ultrasound markers were independent risk factors. The OR for the CAO with different combination of ultrasound markers found to be independent predictors of CAO were calculated. The area under the curve (AUC) was calculated for these. Statistical analysis was performed with IBM SPSS Statistics, Version 26.0 (IBM).
2.1. Ethical approval
Ethical approval was granted on July 27, 2017 (IRAS project ID 222260; REC reference: 17/SC/0374).
3. RESULTS
A total of 1044 pregnancies were included, comprising 87 pregnancies involving pre‐existing diabetes, and 957 involving gestational diabetes. A flow diagram of the cohort is shown in Figure 1. Of those women with GDM, 148 (15.5%) were diagnosed before 24 weeks, the rest after.
The CAO was present in 174 (16.7%) pregnancies. Nulliparity, lower gestational age at birth, preeclampsia and possibly Caucasian ethnicity were associated with an increased incidence (Table 1).
TABLE 1.
Population characteristics as risk factors for composite adverse outcome in fetuses with an estimated fetal weight above the 10th centile
| All patients | CAO present | CAO absent | p value | |
|---|---|---|---|---|
| n = 1044 (100%) | n = 174 (16.7%) | 870 (83.3) | ||
| Maternal age (year), mean ± SD | 32.4 ± 5.5 | 31.5 ± 5.3 | 32.6 ± 5.5 | 0.018 |
| Body mass index (kg/m2), mean ± SD | 30.4 ± 6.8 | 31.0 ± 7.1 | 30.2 ± 6.7 | 0.169 |
| Body mass index ≥ 30 kg/m2, n/N (%) | 520/1038 (50.1) | 93/173 (53.8) | 427/865 (49.4) | 0.291 |
| Caucasian ethnicity, n/N (%) | 519/719 (72.2) | 71/110 (64.5) | 448/609 (73.6) | 0.052 |
| Nulliparity, n (%) | 413 (39.6) | 100 (57.5) | 313 (36.0) | <0.001 |
| In vitro conception, n (%) | 23 (2.2) | 3 (1.7) | 20 (2.3) | 0.637 |
| Hypertension, n/N (%) | 65/720 (9.0) | 11/109 (10.1) | 54/611 (8.8) | 0.674 |
| Smoker, n/N (%) | 100/1035 (9.7) | 18/173 (10.4) | 82/862 (9.5) | 0.717 |
| Pre‐eclampsia, n (%) | 68 (6.5) | 21 (12.1) | 47 (5.4) | 0.001 |
| Male fetuses, n (%) | 562 (53.8) | 99 (56.9) | 463 (53.2) | 0.374 |
| Gestational age at delivery (days), mean ± SD | 273.9 ± 8.6 | 271.0 ± 10.2 | 274.5 ± 8.1 | <0.001 |
| Birth at <37+0 weeks, n (%) | 38 (3.6) | 17 (9.8) | 21 (2.4) | <0.001 |
| Induction of labor, n (%) | 481 (46.1) | 85 (48.9) | 396 (45.5) | 0.421 |
Note: Continuous variables were compared using the Mann‐Whitney U test for non‐normally distributed independent samples.Categorical variables were compared using a chi‐squared test.CAO: Composite adverse outcome: 1+ of perinatal death, arterial cord pH < 7.1, admission to neonatal unit, 5‐minute Apgar <7, severe hypoglycemia requiring treatment, or CS for suspected fetal compromise.
Table 2 shows the association between the four ultrasound markers and the adverse outcome. In the entire cohort, EFW at the 90th centile or above, ACGV at the 90th centile or above, CPR at the 5th centile or below, but not polyhydramnios, were significantly associated with the CAO. Only EFW at the 90th centile or above and CPR at the 5th centile or below were independent risk factors. When sub‐divided into pre‐existing DM and GDM, no statistically significant associations were found.
TABLE 2.
Association between the ultrasound markers estimated fetal weight ≥90th centile, abdominal circumference growth velocity ≥90th centile, cerebro‐placental ratio ≤5th centile, and polyhydramnios and the incidence of composite adverse outcome
| Appropriate for gestational age fetuses | CAO present | ||||
|---|---|---|---|---|---|
| N (%) | N (%) | OR (95% CI) | AOR (95% CI) a | ||
| All hyperglycemic pregnancy | |||||
| Total | 1044 (100) | 174 (16.7) | |||
| Risk factor | US RF present | US RF absent | |||
| EFW ≥90th | 135 (12.9) | 34 (25.2) | 101 (74.8) | 1.85 (1.21–2.84) | 1.66 (1.002–2.75) |
| ACGV ≥90th | 167 (16.0) | 37 (22.2) | 130 (77.8) | 1.54 (1.02–2.31) | 1.21 (0.75–1.96) |
| CPR ≤5th | 75 (7.2) | 20 (26.7) | 55 (73.3) | 1.92 (1.21–3.30) | 1.91 (1.11–3.30) |
| Polyhydramnios | 52 (5.0) | 12 (23.1) | 40 (76.9) | 1.53 (0.79–2.99) | — |
| GDM only | |||||
| Total | 957 (100) | 137 (14.3) | |||
| Risk factor | |||||
| EFW ≥90th | 106 (11.1) | 19 (17.9) | 87 (82.1) | 1.357 (0.80–2.23) | — |
| ACGV ≥90th | 137 (14.3) | 20 (14.6) | 117 (85.4) | 1.027 (0.62–1.72) | — |
| CPR ≤5th | 58 (6.1) | 10 (17.2) | 48 (82.8) | 1.266 (0.63–2.57) | — |
| Polyhydramnios | 44 (4.6) | 9 (20.4) | 35 (79.5) | 1.625 (0.76–3.47) | — |
| Pre‐existing DM only | |||||
| Risk factor | 87 (100) | 37 (42.5) | |||
| EFW ≥ 90th | 29 (33.3) | 15 (51.7) | 14 (48.3) | 1.753 (0.71–4.32) | — |
| ACGV ≥ 90th | 30 (34.5) | 17 (56.7) | 13 (43.3) | 2.49 (0.98–5.96) | — |
| CPR ≤ 5th | 17 (19.5) | 10 (58.8) | 7 (41.2) | 2.28 (0.77–6.69) | — |
| Polyhydramnios | 8 (9.2) | 3 (37.5) | 5 (62.5) | 0.794 (0.18–3.56) | — |
Note: OR were calculated with Cochran‐Mantel‐Haenszel test. CAO: Composite adverse outcome. 1+ of perinatal death, arterial cord pH < 7.1, admission to neonatal unit, 5‐min Apgar score < 7, severe hypoglycemia requiring treatment, or CS for suspected fetal compromise.
Abbreviations: ACGV, abdominal circumference growth velocity; AOR, adjusted odds ratio; CI, confidence interval; CPR, cerebro‐placental ratio; DM, diabetes mellitus; EFW, estimated fetal weight; GDM, gestational diabetes mellitus; OR, odds ratio; US RF, ultrasound risk factors.
Adjusted OR was calculated with logistic regression, including EFW ≥90th centile, ACGV ≥90th centile, CPR ≤5th centile.
Table 3 shows the OR at different combinations of these independent risk factors in the total cohort on multiple logistic regression. Some increase in risk was found with a low CPR or high EFW irrespective of the other, but the greatest risk of adverse outcome was where the EFW was at the 90th centile or above and the CPR was at the 5th centile or below (OR 6.85; 95% CI 2.06–22.78).
TABLE 3.
Simplified flow diagram of possible combinations of the independent ultrasound markers estimated fetal weight ≥90th centile and cerebro‐placental ratio ≤5th centile for prediction of composite adverse outcome
| EFW | CPR | Fetuses | CAO present | |
|---|---|---|---|---|
| N (%) | N (%) | OR (95% CI) | ||
| 1044 (100) | 174 (16.7) | |||
| 10th–90th | ≤5th | 64 (6.1) | 14 (8.0) | 1.44 (0.78–2.66) |
| >5th | 845 (80.9) | 126 (72.4) | 1 (reference) | |
| ≥90th | ≤5th | 11 (1.1) | 6 (3.4) | 6.85 (2.06–22.78) |
| >5th | 124 (11.8) | 28 (16.1) | 1.66 (1.05–2.64) |
Note: OR were calculated with Cochran‐Mantel‐Haenszel test. CAO: Composite adverse outcome: 1+ of perinatal death, arterial cord pH < 7.1, admission to neonatal unit, 5‐min Apgar < 7, severe hypoglycemia requiring treatment, or CS for suspected fetal compromise.
Abbreviations: CI, confidence interval; CPR, cerebro‐placental ratio; EFW, estimated fetal weight; OR, odds ratio.
The AUC for EFW alone was 0.542 (95% CI 0.494–0.591) and for CPR alone it was 0.525 (95% CI 0.477–0.574). The combination of these yielded an AUC of only 0.556 (95% CI 0.507–0.605).
4. DISCUSSION
This analysis suggests that large for dates and low CPR are independent and mutually enhancing risk factors for adverse outcome in a pregnancy complicated by high blood glucose levels. It is the low CPR and not the abdominal circumference growth acceleration that is most associated with increased risk.
Despite this, use of these additional ultrasound factors adds little to the prediction of our CAO, with poor AUC values. This is because of multiple risk factors, particularly for such a CAO which, although similar to other studies, 16 is partly dependent on other intrapartum events. Further, it is not sufficiently serious in itself to warrant screening. Nevertheless, our analysis informs the management of macrosomic babies in hyperglycemic pregnancy, suggesting that CPR may be worth assessing.
When DM and GDM were analyzed separately, no risk factor was shown to be significant. Given the reported risks associated with all three in non‐diabetic pregnancy 5 , 6 and the significance of the risk factors when all pregnancies with high blood glucose levels are analyzed together, this is likely to be a result of the small numbers involved. GDM and DM have in common abnormal glucose levels and a high incidence of macrosomia, and it is the clinical conundrum associated with this that we try to address.
The risks of a low CPR are important because the literature is sparse regarding prediction of adverse outcome in pregnancies involving pre‐existing DM and GDM. Indeed, even the role and accuracy of EFW in diabetic pregnancies is not well established. The American College of Obstetricians and Gynecologists concludes that EFW is not superior to clinical assessment in the detection of large‐for‐gestational‐age fetuses. 1 Recently, the fetal weight centile and abdominal circumference centile were found to be relevant predictors of being large for gestational age, prematurity, and emergency CS. 17 However, the presence of pre‐existing DM and of a large fetus impacts negatively on the accuracy of EFW. 18
Polyhydramnios has been associated with worse maternal glycemic control, higher concentration of amniotic fluid glucose, and larger babies. 19 Polyhydramnios increases the risk of iatrogenic preterm birth, particularly via elective CS for suspected macrosomia. 20 In our study, polyhydramnios is not associated with adverse outcome: it is possible that this depends on the exclusion of pregnancies delivered at less than 35 weeks.
Limited data on the role of the newer markers ACGV and CPR in hyperglycemic pregnancies exist. In a study of ultrasound screening in 4512 nulliparous women, in which adjustment for maternal diabetes or gestational diabetes had minimal effect, 5 a high ACGV was found to be more important than high EFW, in that suspected macrosomic babies with a normal ACGV were not at significantly increased risk of adverse outcomes, and those with the highest risk had a high ACGV and were suspected of being macrosomic. This does not align with our results, but their analysis did not include Doppler findings.
Reduced resistance in the Umb A and MCA, and increased resistance in the renal artery were described in 147 fetuses of pregnancies complicated by GDM. 21 In 2017, Gibbons et al demonstrated that a low CPR (below the 10th centile) was associated with increased risk of CAO in diabetic pregnancies. They did not assess the role of fetal size or ACGV, and the incidence of the CAO was 36.4%. 22 Further their results may not apply to macrosomic babies because more than one‐third of their low CPR babies were SGA at birth, and very few were macrosomic. Finally, in a sample of just 130 pregnancies with GDM, Familiari et al reported that MCA PI may have a role in predicting minor adverse outcomes. 23
An inverse relation between neonatal weight and umbilical flow has been demonstrated in pregnancies complicated by type 1 diabetes and in GDM. 24 , 25 Umbilical pulsatility partly reflects placental resistance and this may not be the principal contributor to the vulnerability shown by diabetic pregnancies. The MCA, however, is thought to reflect brain sparing, which may be a fetal adaptation to pathology of multiple origins.
We have not evaluated the role of other ultrasound markers that have been proposed as predictors of adverse outcome in pregnancies affected by diabetes. These include the umbilical cord coiling index, 26 or assessment of umbilical vein area or flow, 27 as well as other biometric indexes for the evaluation of fetal soft tissues. 28 However, the use of these parameters is not yet widespread. We have decided to include standard fetal biometry, liquor volume, and basic Doppler velocimetry, as they are more commonly used in clinical practice.
The strength of this study is that almost every pregnancy had a standardized ultrasound assessment in the third trimester, with universal assessment of the CPR; however, in a few cases this was missing. Our findings remain relevant to pregnancies where CPR can be accurately measured. Some demographic data were also missing. The principal limitation of this study is its size and subsequent inability to determine the most important, serious outcomes such as death or disability. The use of a surrogate marker is therefore common in the literature and our choice is not dissimilar from other analyses: eg, neonatal unit admission, 22 intrapartum fetal distress. 22 , 29 In addition to the potential limitations of amalgamation of GDM and DM pregnancies, a treatment paradox may exist because of the retrospective nature of the study and results being available to clinicians: possible risk factors influence management. This, however, might be expected to reduce the associations with adverse outcomes. Further, this is a problem common to all but the rare prospective studies where clinicians are blinded to ultrasound findings. Since selective and not universal screening was used for the diagnosis of gestational diabetes, this cohort may not include all pregnancies in the time period but as no comparison with non‐diabetic pregnancy was made, this is unlikely to have influenced our outcomes. We have also not assessed the role of pregnancy glycemic control. It was our intention to explore how ultrasound assessment might be improved, rather than compare it with an established cornerstone of care of a diabetic pregnancy. High third‐trimester hemoglobin A1c levels have recently been shown to be predictive of perinatal death in women with pre‐existing diabetes. 30 Whether ultrasound can be used to better predict and possibly prevent such adverse outcomes is an important question.
5. CONCLUSION
This is the first analysis to evaluate ultrasound estimates of size, growth velocity, and Doppler together in pregnancies with high blood glucose values. It suggests that there could be benefit to assessing CPR in late pregnancy and that this may identify macrosomic babies at most risk. Although promising, much larger, and preferably prospective, analyses are required to determine its performance, and relation with markers of glycemic control in the prediction and prevention of serious adverse outcomes.
CONFLICT OF INTEREST
None.
AUTHOR CONTRIBUTIONS
MG and LI: Conception and design, data collection analysis and interpretation, drafting and revising. CA, AC, SM and CI: Conception and design, data collection analysis and interpretation.
Garbagnati M, Aye CY, Cavallaro A, Mathewlynn S, Ioannou C, Impey L. Ultrasound predictors of adverse outcome in pregnancy complicated by pre‐existing and gestational diabetes. Acta Obstet Gynecol Scand. 2022;101:787‐793. doi: 10.1111/aogs.14361
References
- 1. American College of Obstetricians and Gynecologists . ACOG practice bulletin no. 201: pregestational diabetes mellitus. Obstet Gynecol. 2018;132:e228‐e248. [DOI] [PubMed] [Google Scholar]
- 2. Gutaj P, Wender‐Ozegowska E. Diagnosis and management of IUGR in pregnancy complicated by type 1 diabetes mellitus. Curr Diab Rep. 2016;16:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Voormolen DN, DeVries JH, Sanson RM, et al. Continuous glucose monitoring during diabetic pregnancy (GlucoMOMS): a multicentre randomized controlled trial. Diabetes Obes Metab. 2018;20:1894‐1902. [DOI] [PubMed] [Google Scholar]
- 4. Esakoff TF, Cheng YW, Sparks TN, Caughey AB. The association between birthweight 4000 g or greater and perinatal outcomes in patients with and without gestational diabetes mellitus. Am J Obstet Gynecol. 2009;200:672‐e1. [DOI] [PubMed] [Google Scholar]
- 5. Sovio U, Moraitis AA, Wong HS, Smith GC. Universal vs selective ultrasonography to screen for large‐for‐gestational‐age infants and associated morbidity. Ultrasound Obstet Gynecol. 2018;51:783‐791. [DOI] [PubMed] [Google Scholar]
- 6. Morales‐Roselló J, Khalil A. Fetal cerebral redistribution: a marker of compromise regardless of fetal size. Ultrasound Obstet Gynecol. 2015;46:385‐388. [DOI] [PubMed] [Google Scholar]
- 7. Lees CC, Stampalija T, Baschat AA, et al. ISUOG Practice Guidelines: diagnosis and management of small‐for‐gestational‐age fetus and fetal growth restriction. Ultrasound Obstet Gynecol. 2020;56:298‐312. [DOI] [PubMed] [Google Scholar]
- 8. National Institute for Health and Care Excellence . Diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period. NG3. 2015;5(3):215‐223. [PubMed] [Google Scholar]
- 9. International Association of Diabetes and Pregnancy Study Groups Consensus Panel . International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33:676‐682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bhide A, Acharya G, Baschat A, et al. ISUOG Practice Guidelines (updated): use of Doppler velocimetry in obstetrics. Ultrasound Obstet Gynecol. 2021;58:331‐339. [DOI] [PubMed] [Google Scholar]
- 11. Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with the use of head, body, and femur measurements—a prospective study. Am J Obstet Gynecol. 1985;151:333‐337. [DOI] [PubMed] [Google Scholar]
- 12. Hadlock FP, Harrist RB, Martinez‐Poyer J. In utero analysis of fetal growth: a sonographic weight standard. Radiology. 1991;181:129‐133. [DOI] [PubMed] [Google Scholar]
- 13. Vannuccini S, Ioannou C, Cavallaro A, Volpe G, Ruiz‐Martinez S, Impey L. A reference range of fetal abdominal circumference growth velocity between 20 and 36 weeks' gestation. Prenat Diagns. 2017;37:1084‐1092. [DOI] [PubMed] [Google Scholar]
- 14. Ciobanu A, Wright A, Syngelaki A, Wright D, Akolekar R, Nicolaides KH. Fetal Medicine Foundation reference ranges for umbilical artery and middle cerebral artery pulsatility index and cerebroplacental ratio. Ultrasound Obstet Gynecol. 2019;53:465‐472. [DOI] [PubMed] [Google Scholar]
- 15. Moise KJ Jr. Toward consistent terminology: assessment and reporting of amniotic fluid volume. Semin Perinatol. 2013;37:370‐374. [DOI] [PubMed] [Google Scholar]
- 16. Martinez‐Portilla RJ, Caradeux J, Meler E, Lip‐Sosa DL, Sotiriadis A, Figueras F. Third‐trimester uterine artery Doppler for prediction of adverse outcome in late small‐for‐gestational‐age fetuses: systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2020;55:575‐585. [DOI] [PubMed] [Google Scholar]
- 17. Antoniou MC, Gilbert L, Gross J, et al. Main fetal predictors of adverse neonatal outcomes in pregnancies with gestational diabetes mellitus. J Clin Med. 2020;9:2409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Hendin N, Levin G, Tsur A, Ilan H, Rottenstreich A, Meyer R. Factors associated with more than 500 grams inaccuracy in sonographic fetal weight estimation. Isr Med Assoc J. 2021;23:43‐47. [PubMed] [Google Scholar]
- 19. Vink JY, Poggi SH, Ghidini A, Spong CY. Amniotic fluid index and birth weight: is there a relationship in diabetics with poor glycemic control? Am J Obstet Gynecol. 2006;195:848‐850. [DOI] [PubMed] [Google Scholar]
- 20. Idris N, Wong SF, Thomae M, Gardener G, McIntyre DH. Influence of polyhydramnios on perinatal outcome in pregestational diabetic pregnancies. Ultrasound Obstet Gynecol. 2010;36:338‐343. [DOI] [PubMed] [Google Scholar]
- 21. Liu F, Liu Y, Lai YP, Gu XN, Liu DM, Yang M. Fetal hemodynamics and fetal growth indices by ultrasound in late pregnancy and birth weight in gestational diabetes mellitus. Chinese Med J. 2016;129:2109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Gibbons A, Flatley C, Kumar S. Cerebroplacental ratio in pregnancies complicated by gestational diabetes mellitus. Ultrasound Obstetr Gynecol. 2017;50:200‐206. [DOI] [PubMed] [Google Scholar]
- 23. Familiari A, Neri C, Vassallo C, et al. Fetal Doppler Parameters at Term in Pregnancies Affected by Gestational Diabetes: Role in the Prediction of Perinatal Outcomes. Ultraschall Med. 2020;41:675‐680. [DOI] [PubMed] [Google Scholar]
- 24. Maruotti GM, Rizzo G, Sirico A, et al. Are there any relationships between umbilical artery Pulsatility Index and macrosomia in fetuses of type I diabetic mothers? J Mat Fetal Neonat Med. 2014;27:1776‐1781. [DOI] [PubMed] [Google Scholar]
- 25. Quintero‐Prado R, Bugatto F, Sánchez‐Martín P, Fajardo‐Expósito MA, Torrejón R, Bartha JL. The influence of placental perfusion on birthweight in women with gestational diabetes. J Mat Fetal Neonat Med. 2016;29:32‐35. [DOI] [PubMed] [Google Scholar]
- 26. Najafi L, Khamseh ME, Kashanian M, et al. Antenatal umbilical coiling index in gestational diabetes mellitus and non‐gestational diabetes pregnancy. Taiwan J Obstet Gynecol. 2018;57:487‐492. [DOI] [PubMed] [Google Scholar]
- 27. Rizzo G, Mappa I, Bitsadze V, Khizroeva J, Makatsarya A, D'Antonio F. The added value of umbilical vein flow in predicting fetal macrosomia at 36 weeks of gestation: a prospective cohort study. Acta Obstet Gynecol Scand. 2021;100:900‐907. [DOI] [PubMed] [Google Scholar]
- 28. Garabedian C, Vambergue A, Salleron J, Deruelle P. Prediction of macrosomia by serial sonographic measurements of fetal soft‐tissues and the liver in women with pregestational diabetes. Diab Metab. 2013;39:511‐518. [DOI] [PubMed] [Google Scholar]
- 29. Bracero LA, Figueroa R, Byrne DW, Han HJ. Comparison of umbilical Doppler velocimetry, nonstress testing, and biophysical profile in pregnancies complicated by diabetes. J Ultrasound Med. 1996;15:301‐308. [DOI] [PubMed] [Google Scholar]
- 30. Murphy HR, Howgate C, O'Keefe J, et al. Characteristics and outcomes of pregnant women with type 1 or type 2 diabetes: a 5‐year national population‐based cohort study. Lancet Diab Endocrinol. 2021;9:153‐164. [DOI] [PubMed] [Google Scholar]