

Abstract
Acute appendicitis is the most common cause of acute abdominal pain in the pediatric population. The physiopathology is secondary to luminal obstruction of the appendix by several causes, among these, one of the rarest is due to parasitosis by Enterobius vermicularis in 0.005–3 %. We hereby present a case of a 10-year-old Latin male with abdominal pain with irradiation to right iliac fossa, nausea, vomiting and fever, following the national Mexican guides for ultrasound and blood tests were ordered, patient was treated with laparoscopic appendectomy with intraoperative finding of live helminths, which pathology examination revealed to be Enterovirus vermicularis. The patient has an uneventful postoperative course and was discharged after completing antiparasitic therapy. The lessons from this case are the importance of a good and quick diagnosis for acute abdomen in children, the possibility of a parasitic entity in the finding of eosinophilia with appendicitis and the good results with the correct surgical treatment.
Keywords: Appendicitis, Enterobius vermicularis, Surgical intervention, Case report, Diagnosis
Highlights
-
•
Acute appendicitis (AA) is a cause of acute abdomen in the pediatric population, an unusual etiology is parasitosis.
-
•
Parasitosis by Enterobius vermicularis is caused infrequently by 0.05-3% of acute appendicitis.
-
•
Leukocytosis is a common parameter in these types of conditions, in the case of eosinophilia it is only reported in 14%.
-
•
The treatment consists of appendectomy (conventional/laparoscopic), complementing with an anthelmintic treatment.
1. Introduction and importance
AA is the most common cause of acute abdomen and one of the most frequent pathologies that will require surgical treatment. It happens commonly in young people, especially between the second and third decade of life [1]. Its pathophysiology is characterized by obstruction of the appendicular lumen caused by different etiologies including lymphoid hyperplasia, fecaliths, tumors, or foreign bodies, it can rarely be caused by parasitosis [2].
Parasitic infection by Enterobius vermicularis is responsible for 0.05 to 3 % of cases of acute appendicitis [2] [3]. It is proposed that the presence of parasites within the appendicular lumen generates an obstruction that favors the accumulation of mucus and bacterial overgrowth triggering the process of distension and causing an increase in the intraluminal pressure that progresses to the obstruction of venous flow, favoring the perforation and complication of the picture [3]. The workup of this case was made following the “Guías de Práctica Clínica (GPC)” from the Instituto Mexicano del Seguro Social [4]. We decide to share this case due to the scarce panorama of Mexico and the globe in the apparition of E. vermicularis as a possible etiology of appendicitis.
2. Case presentation
We present the case of a 10-year-old mexican male who was bringed by his parents, elementary school student and a 93 percentile according to weight and 90 percentile in height with a history of gastroenteritis a week before his admission and no other relevant interventions or diseases, patient showed up at the emergency room for a picture of acute abdominal pain of 12 h, located in mesogastrium with radiation to the right iliac fossa, accompanied with nausea, vomiting and anorexia, parents referred to give acetaminophen to child at the start of symptoms. Parents said the child has no allergies or other drug usage. Parents have history of diabetes type 2 in both, and the father also has history of essential hypertension.
On physical examination he presented a fever of 37.6 °C, abdomen with decreased peristalsis, pain on palpation in the right iliac fossa, with greater intensity at McBurney's point, with Blumberg's sign, positive obturator and talo-percusion.
Laboratories show a leukocyte figure of 7440 (4–10,000) with neutrophils of 68 % (50–70 %), eosinophils of 2.3 % [1], [2], [3], patient is classified with 6 points with the Alvarado scale. Ultrasound of the lower abdomen is performed, reporting hypoechogenic tubular image, corresponding to the cecal appendix, with a diameter of 7 mm, which presents an increase in Doppler flow, being compatible with an uncomplicated appendicular inflammatory process (Fig. 1). Before those steps, the differential diagnosis was mesenteric adenitis due the presence of pain on the right iliac fossa and the viral gastrointestinal infection predecessor.
Fig. 1.
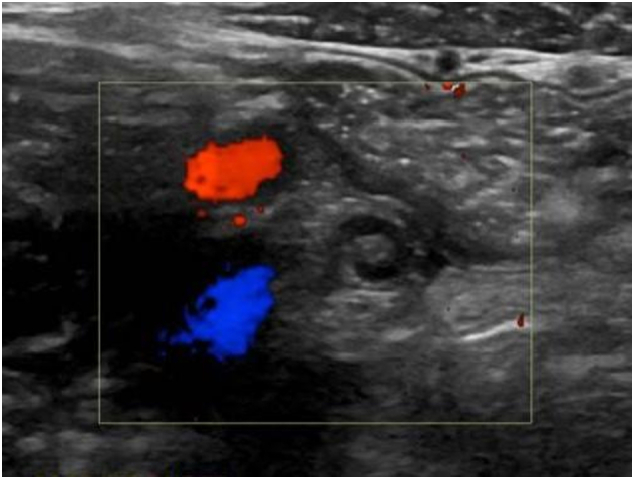
Appendicular ultrasound showing hypoechogenic tubular image, non-compressible, with a diameter of 7 mm, with increased Doppler flow, being compatible with appendicular inflammatory process. (Color must be used).
Blood chemistry and clotting times were ordered with no abnormalities, allowing the next steps: Child began a preoperative scheme of cefalotine (500 mg IV each 12 h), and acetaminophen (500 mg IV each 8 h), for the surgery there was no special intestinal preparation.
A laparoscopic approach was executed with balanced general anesthesia, the patient was in supine position and surgical site is washed with chlorhexidine, the procedure was performed with laparoscopic equipment, evidencing an hyperemic, congestive cecal appendix with edema, presence of scarce free fluid, the mesoappendix was released with monopolar energy and ligation of the appendicular stump was performed using an endoloop of Vicryl 0 at the proximal end and another at the distal end. The appendicular artery was linked with hemoclips, the ports were closed with vicryl 1–0 aponeurosis and monocryl 3–0 for subcutaneous tissue and skin. It should be mentioned that at the time of sectioning the appendicular base, the exit of round and curved parasites, pearly white, was observed, which were cauterized. Appendix was removed with an endobag and the piece was sent to pathology who reports appendicular inflammatory process secondary to parasitosis by E. vermicularis. The histopathology report confirmed acute appendicitis associated with the intraluminal presence of structures compatible with Enterobius vermicularis (Fig. 2). Procedure was executed by a surgeon with 5 years of experience, in a high specialty hospital (third level). There wasn't any change in the planning of the surgery and the posterior realization.
Fig. 2.

Histopathology report confirmed acute appendicitis associated with the intraluminal presence of structures compatible with Enterobius vermicularis. (Color must be used).
In the postoperative period, drug regimen was similar, cefalotine (500 mg IV each 12 h), acetaminophen (500 mg IV each 8 h), adding omeprazole (20 mg IV each 24 h) for prophylaxis of infections and stress ulcers, the patient tolerated walking, medications and mild pain related to surgery wound, he did not present any complication during surgery and post-surgery, there wasn't an increased rate of mortality/morbidity on the thirty post-operative days, the postoperative instructions were mild rest, not carrying heavy things, wound healings with antiseptic every 8 h, acetaminophen (500 mg VO each 8 h for five days) and antibiotic amoxicillin-ac. Clavulanico 500 mg every 8 h for 7 days. The patient had an adequate postoperative evolution, so it was decided to discharge him on the fifth postoperative day, with indications to follow-up consultation 7 and 14 days after discharge for wound assessment and antiparasitic treatment (mebendazole). Abdomen and surgical wounds were examined, no laboratory or imaging studies were requested from the consultation.
He is currently asymptomatic after 1 year of follow-up and with a good prognosis according to Jerusalem guides for acute appendicitis. No scale was used to assess quality of life.
3. Clinical discussion
The relevant points of the case are that the realization of the diagnosis, treatment and follow-up were made on a 3rd level hospital in the north of Mexico, containing all the materials and expertise of specialists and health personnel such as the 1st world countries, another important point is the contribution to the literature of case reports to this low incidence disease, specially in the north of Mexico. The weakness of the case probably is the relative low-sharing impact of the knowing techniques, treatment and diagnosis, which all are well established in the medical field. On the next words, we discuss relevant comparative literature of this disease:
E. vermicularis infection is the most common helminth parasitosis worldwide, affecting 4 % to 40 % of children globally [5]. It is an oral fecal transmitted nematode, with a life cycle of 2–4 weeks [6]. The most common presentation of this infection is anal pruritus, the result of the migration of the female by leaving her eggs in the perianal region. However, they can also present as abscesses, urinary tract infections, salpingitis or as in this case, present as acute appendicitis, the latter caused by obstruction of light, favoring pathogenesis and classic symptoms [7] [8].
.The incidence of E. vermicularis as a cause of AA is varied, reports ranging from 0.2 to 4.18 % were found [6] [7] [8]. However, Dahlstrom, et al. in his 1867 study appendectomies he highlighted an incidence of 3.4 % [9]. In addition to E. vermicularis, other parasitosis have been reported to cause AA, such as Ascaris lumbricoides, Taenia saginata or Schistosomiasis [10].
Among the laboratory studies with AA, leukocytosis is usually reported and only 14 % report eosinophilia [8]. Once the diagnosis is suspected, like in our case by confirmation with blood and chemistry tests, and ultrasound, literature also recommend to use computed tomography for diagnosis as gold-standard for appendicitis. Treatment is performed by appendectomy, open or laparoscopic, it is important to supplement the treatment with an anthelmintic agent with albendazole or mebendazole, which should be indicated to the patient and family members, recommending a second dose to avoid reinfection [7] [10].
4. Patient perspective
Patient felt an important general malaise and mentioned the pain that I present as - “one of the strongest present that I have felt”, the parents mention that at the beginning of the condition they believed that it was a gastrointestinal infection like the one I had presented a week before, but with the passage of the hours the pain was increased in intensity and radiating to the lower abdomen, for this reason they decided to go to the emergency room for evaluation, the patient reported a significant improvement in pain after surgery which led to an improvement in his general condition, the parents mention the importance of going to a medical assessment when presenting any type of pain to avoid complications in the future, and that in turn they are satisfied with the management, evolution and improvement of the patient.
5. Methods
This case report has been reported in line with the SCARE Criteria [11].
6. Conclusion
E. vermicularis parasitosis is one of the least common etiologies that cause AA, but it must be taken into perspective among our differential diagnoses. It should be in the mind of any doctor in the face of clinical symptoms, especially in the presence of eosinophilia. The treatment consists of appendectomy, complementing the patient and his family with an anthelmintic treatment, in general, well-treated patients have a good prognosis with excellent postoperative escenarios and low complications.
Ethical approval
This study gets an ethical approval by the hospital's ethics committee already established.
Registration of research studies
It does not apply.
Guarantor
Alejandro Flores Uribe.
Sources of funding
This study did not receive any specific support from funding agencies, in the public, commercial or non-profit sector.
Ethical considerations
Protection of people and animals: The authors state that no experiments have been carried out on humans or animals for this research.
Confidentiality of data: The authors state that they have followed their workplace protocols on the publication of patient data.
Right to privacy and informed consent
The authors declare that no patient data appears in this article.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Credit authorship contribution statement
Alejandro Flores Uribe: Patient care, clinical case, writing
Jorge Pablo Pérez Macías: Patient care, clinical case
Jorge Alberto González Arévalo: Writing and translation
Oscar Armando Flores Uribe: Data analysis and writing
Declaration of competing interest
The authors declare that they have no conflict of interest in the writing of this manuscript.
References
- 1.Khan G.M., Grillo I.A., Abu-Eshy S.A., Khan A.R., Mubarak J., Jastaniah S. Pathology of the appendix. J. Natl. Med. Assoc. 2000 Nov;92(11):533–535. https://www.ncbi.nlm.nih.gov/pubmed/11152086 Available from: [PMC free article] [PubMed] [Google Scholar]
- 2.Echazarreta-Gallego E., Córdoba-Díaz de Laspra E., Mejia-Urbaez E., Hernáez-Arzoz A., Sánchez-Blasco L., Elía-Guedea M. Apendicitis y parásitos: a propósito de 2 casos. Rev. Chil. Cir. 2016 Sep 1;68(5):373–375. https://www.sciencedirect.com/science/article/pii/S0379389316000065 Available from: [Google Scholar]
- 3.Bhangu A., Søreide K., Di Saverio S., Assarsson J.H., Drake F.T. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015 Sep 26;386(10000):1278–1287. doi: 10.1016/S0140-6736(15)00275-5. Available from: [DOI] [PubMed] [Google Scholar]
- 4.Rodríguez Fernández Z. Complicaciones de la apendicectomía por apendicitis aguda. Revista Cubana de Cirugía [Internet] 2010. http://scielo.sld.cu/scielo.php?pid=S0034-74932010000200006&script=sci_arttext&tlng=pt Available from:
- 5.Dunphy L., Clark Z., Raja M.H. Enterobius vermicularis (pinworm) infestation in a child presenting with symptoms of acute appendicitis: a wriggly tale! BMJ Case Rep. 2017 Oct 6;2017 doi: 10.1136/bcr-2017-220473. Available from: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sosin M., Kent J.R., Chahine A.A. Enterobius vermicularis appendiceal colic. J. Laparoendosc. Adv. Surg. Tech. A. 2019 May;29(5):717–719. doi: 10.1089/lap.2018.0693. https://www.liebertpub.com/doi/10.1089/lap.2018.0693 Available from: [DOI] [PubMed] [Google Scholar]
- 7.Thanikachalam M.P., Kasemsuk Y., Mak J.W., Sharifah Emilia T.S., Kandasamy P. A study of parasitic infections in the luminal contents and tissue sections of appendix specimens. Trop. Biomed. 2008 Aug;25(2):166–172. https://www.ncbi.nlm.nih.gov/pubmed/18948889 Available from: [PubMed] [Google Scholar]
- 8.Sodergren M.H., Jethwa P., Wilkinson S., Kerwat R. Presenting features of Enterobius vermicularis in the vermiform appendix. Scand. J. Gastroenterol. 2009;44(4):457–461. doi: 10.1080/00365520802624227. Available from: [DOI] [PubMed] [Google Scholar]
- 9.Dahlstrom J.E., Macarthur E.B. Enterobius vermicularis: a possible cause of symptoms resembling appendicitis. Aust. N. Z. J. Surg. 1994 Oct;64(10):692–694. doi: 10.1111/j.1445-2197.1994.tb02059.x. Available from: [DOI] [PubMed] [Google Scholar]
- 10.Zakaria O.M., Zakaria H.M., Daoud M.Y., Al Wadaani H., Al Buali W., Al-Mohammed H., et al. Parasitic infestation in pediatric and adolescent appendicitis: a local experience. Oman. Med. J. 2013 Mar;28(2):92–96. doi: 10.5001/omj.2013.25. Available from: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Agha RA Franchi T., Sohrabi C Dec; 84:226–30. Available from. 2020 doi: 10.1016/j.ijsu.2020.10.034. [DOI] [Google Scholar]