

Abstract
Background: We analyzed an original case series of the classic ear-molding method and evaluated the efficacy and complication rate of the method compared to commercial ear-molding products by meta-analysis to draw conclusions on the efficacy of the classic method. Methods: From January 2019 to March 2022, we selected patients who underwent classic ear molding for newborn ear deformities at our institution and reviewed the patient age, treatment time, efficiency and complications. Additionally, the PubMed, EMBASE, and Scopus databases were searched, and meta-analysis (following the PRISMA guidelines) was performed. Results: In the case study, the success rate (excellent and good outcomes) of the classic ear-molding method was 92.6%. The mean age at application and mean duration of application were 5.81 ± 6.09 days and 32.13 ± 7.90 days, respectively. In the systematic review, the classic method group showed a statistically smaller success rate (proportion of 0.79) and statistically smaller complication rate (proportion of 0.05) than the commercial product group (proportion of 0.83). Conclusions: Compared with commercial products, classic ear molding has remarkable and comparable therapeutic effects on neonatal auricular deformities. Additionally, the classic ear-molding method is more suitable for infants with auricular deformities from socioeconomically vulnerable areas. Thus, the classic ear-molding method could be a better option for congenital ear anomalies than commercial ear-molding products.
Keywords: ear molding, deformational ear anomaly, auricular anomaly, congenital ear anomaly, nonsurgical correction, newborn
1. Introduction
Neonatal ear anomalies are classified into malformations or deformations [1,2]. Ear malformations involve a partial loss of the skin or cartilage with underdevelopment of any part of the pinna. Ear deformations involve a fully developed but misshaped pinna with no deficiency of skin and cartilage [3]. Deformational anomalies of the ear are categorized into prominent, lidding/lop, conchal crus, Stahl’s, and helical rim deformities [4,5]. Fortunately, these deformational anomalies can be corrected with an ear-molding technique until the early neonatal period. Circulating levels of maternal estrogen and tissue hyaluronic acid, which favor newborn ear malleability, peak during the first 72 h after birth and decline to baseline by 6 weeks of age, when the auricle becomes more elastic and firm [6]. Thus, during this window, when the ear cartilage is malleable, ear anomalies can be corrected by ear molding. Ear molding in infants may eliminate the need for future surgical correction, and many authors have reported the effectiveness of this intervention [1]. The current literature on ear molding demonstrates the efficacy or timing of neonatal ear molding in the correction of deformational ear anomalies. However, no studies have focused on evaluating the efficacy of the classic ear-molding method. In this study, we evaluated the efficacy and complication rate of the classic ear-molding method compared to commercial ear-molding products. For evaluation, we describe an original case series from our institution. We also conducted a systematic literature review to draw conclusions on the efficacy of the classic ear-molding method.
2. Materials and Methods
2.1. Case Series
2.1.1. Patient Selection
From January 2019 to March 2022, we selected patients who underwent the classic ear-molding method for newborn ear deformities at our institution and analyzed the patient age at treatment, treatment time, efficiency and complications. Pretreatment and post-treatment photographs were assessed by three independent plastic surgeons, who rated the outcome as poor, moderate, good, and excellent. An agreement test was applied. Definitions of grading are explained in Table 1.
Table 1.
Photographic grading for ear anomalies.
| Grade | Shape | Deformation/Malformation |
|---|---|---|
| Excellent | Normal ear shape | No appearance of original deformation/malformation |
| Good | Nearly normal ear shape | Mild yet nondistracting retention of original deformation/malformation |
| Moderate | Improved but not a normal ear shape | Noticeable, distracting retention of original deformation/malformation |
| Poor | No improvement | Abnormal ear shape with retention of original deformation/malformation |
2.1.2. Treatment and Evaluation
The classic ear-molding materials are custom-made splints of metal wire, surgical tape, foam, and silicone tape (Figure 1).
Figure 1.

Treatment steps of classic ear molding. (A) Preparation before treatment. (B) Application of classic ear molding. (C) Protection of molding materials.
Step 1. The hair around the ear was shaved before ear molding (to avoid damage to the skin), and then the skin oil was wiped off with isopropyl alcohol so the cradle could adhere to the skin.
Step 2. The splint was selected and curved according to the desired shape of the helix and was then placed on the anterolateral surface of the auricle.
Step 3. Fixation on the anterolateral surface of the auricle in the groove between the helix and antihelix was achieved with surgical tape. Surgical tape was also used to position the auricle closer to the scalp.
Step 4. The ear was covered with foam to protect the molding materials.
For the first week of treatment, taping was used to counteract the significant resistive forces to expansion resulting from tissue deficiency. After that, the splint was curved according to the desired shape of the helix and then fixed on the anterolateral surface of the auricle. The infants wore the splint for 24 h per day.
When skin complications occurred, we continued the treatment because foam-covered molding materials absorb exudate and improve skin lesions. The splinting stopped only when pressure ulcers occurred.
When we first started treatment, patients visited the clinic to check for complications at three days after ear-molding. After we confirmed that five patients did not have any complications at three days after treatment, infants were scheduled for weekly follow-up routinely to monitor complications and auricle changes and to modulate the devices to obtain better correcting conditions. Splinting was performed continuously until 1 week after normalization of the auricular anatomy was achieved, and it was stopped after a maximum of 6 weeks of treatment even when no correction occurred.
2.1.3. Statistical Analysis
All analyses were performed using SPSS 21.0 software. Variables were analyzed using frequency analysis, descriptive analysis, one-way ANOVA, the Kruskal-Wallis test, and Fisher’s exact test where appropriate. A p value of <0.05 was used as the cutoff point for statistical significance.
2.2. Systematic Literature Review
2.2.1. Search Protocol
The PubMed, EMBASE, and Scopus databases were systematically searched. The following keywords were used to search the literature: ‘Neonatal ear molding’ OR ‘Ear molding’ OR ‘Earwell’ Or ‘InfantEar’. The preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines were followed to perform this systematic review and meta-analysis. An overview of the systematic review process is presented in Figure 2. Initially, we screened all publications by titles and/or abstracts. Next, we assessed eligibility based on full-text articles. Finally, for the included publications, we collected only cases with clear and relevant data, as described above. Consequently, a total of 13 studies were included in this systematic review (Table 2).
Figure 2.

Flow diagram used to identify and select studies.
Table 2.
Characteristics of the articles.
| Classic Method | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study No. |
Study | Device | Cases (n) | Type of Anomaly (%) | Initiation (Mean Weeks ± SD; Range) |
Duration (Mean Weeks ± SD; Range) |
Responder | Success * (n) | Complication † (n) |
| 1 | Chang 2017 [7] | Conformer, Velcro tape, and gel sealing | 33 | Helical (30.3); Lop (18.2); Prom. (21.2); Stahl’s (24.2); mixed (6.1) | 4.5; 0.86 to 15.1 |
3.9; 1.7 to 6.6 |
Physician | 30 | 2 |
| 2 | Leonardi 1 2012 [8] | Splinting and taping | 22 | Const. (36.4); Lop (9.1); Prom. (18.2); Stahl’s (18.2) | N/A; 0.29 to 6 | N/A; 5–8 | Parents | 17 | 0 |
| Leonardi 2 2012 [8] | Physician | 15 | |||||||
| 3 | Mohammadi 2016 [9] | Splinting and taping | 21 | Const. (38.1); Lop (23.8); Prom. (20.7) | 7.52 ± 5.6; 2 to 24 |
13.33 ± 2; 11 to 18 |
Physician | 12 | 0 |
| 4 | Tan 1997 [4] | Splinting and taping | 32 | Concha (3.1); Lop (65.6); Prom. (18.8); Stahl’s (6.3); mixed (6.3) | 2.4 ± 3.5; 0.14 to 10 |
10.9 ± 9; 5 to 38.5 |
Physician and parents | 17 | 1 |
| 5 | Tan 1 2003 [10] | Splinting and taping | 44 | Cup (18.2); Lop (38.6); Helical (11.4) Prom. (31.8) |
3.4; 0.14 to 15 | 7; 1 to 14 | Parents | 29 (total n: 35) |
4 |
| Tan 2 2003 [10] | Physician | 38 | |||||||
| 6 | Ullmann 1 2002 [11] | Splinting and taping | 92 | Costricted (21.7); Lop (30.4); Prom. (26.1); Stahl’s (21.7) |
N/A; 0.14 to 1.43 | 6.8; 6 to 12 | Parents | 80 | 0 |
| Ullmann 2 2002 [11] | Physician | 81 | |||||||
| Commercial Product | |||||||||
| 7 | Chan 2019 [1] | Earwell® | 71 | Concha (0.95); Constricted (32.4); Cryptotia (0.95); Helical (9.5); Lidding (28.6); Lop (4.8); Prom.(4.8); Stahl’s (18.1) | 2.24; 0 to 13.9 | 4.1; 1.5 to 6 | Physician | 61 | 20 |
| 8 | Daniali 2017 [12] | Earwell® | 303 | Concha (36.4); Helical (24.8); Lidding (19.1); Prom. (8.9); Stahl’s (20.8) | 1.79; N/A | 5.29; 1.7 to 15.6 |
Physician | 285 | 22 |
| 9 | Doft 2015 [13] | Earwell® | 158 | Constricted (18); Cryptotia (0.5); Helical (38); Prom. (18.5); Stahl’s (25) | N/A; N/A | 2; 1 to 6 | Parents | 152 | 5 |
| 10 | Nigam 2020 [14] | Earwell® /InfantEar® |
272 | Concha (2.2); Cup (7.7); Helical (14.3); Lidding/Lop (8.8); Prom. (23.2); Stahl’s (8.4) | 2.9; N/A | N/A | Parents | 85 (total n: 100) |
37 |
| 11 | Patel 2020 [15] | InfantEar® | 85 | Helical (100) | 4.9; 8.6 to 10.9 | 4.4; 1 to 10.3 | Survey | 54 (total n: 59) |
11 |
| 12 | Woo 2016 [16] | Earwell® | 28 | Constricted (62.4); Cryptotia (7.1); Prom. (7.1); Stahl’s (21.4) | 3.2; 0.7 to 7.4 | 4.7; 3.4 to 7.6 | Parents | 13 | N/A |
| 13 | Zhuang 2020 [17] | Earlimn® | 141 | Concha (7.8); Constricted (17.7); Cryptotia (9.2); Cup (9.2); Helical (18.4); Lop (16.3); Prom. (10.6); Stahl’s (10.6) | 5 ± 3.3; N/A | 2.5 ± 1.86; N/A | Physician | 121 | 2 |
Helical, helical deformity; Prom., prominent ear; Const., constricted ear; Concha, conchal deformity; * Normal to near normal ear shape; † skin irritation or superficial ulcer. The results of this divided to patients reported outcome and physician-reported outcome. 1 is for patients outcome and 2 is for physician outcome.
2.2.2. Inclusion and Exclusion Criteria
All studies meeting the following criteria were included: (1) English language and (2) full text available. Studies fulfilling the following criteria were excluded: (1) duplicate publications, (2) studies that did not include neonatal ear molding, (3) clinical trials or review articles, and (4) studies reporting unclear data or withdrawn studies.
2.2.3. Statistical Analysis
Data were retrieved by a single author, and the following information was retrieved from the included studies. Thirteen articles were included in the heterogeneity analysis. The successful correction rate and complication rate along with the 95% confidence interval (CI) were estimated. The Q statistic for heterogeneity and the I2 index were calculated. Values less than 50% indicated low heterogeneity; other values indicated high heterogeneity. If I2 < 50%, we used a fixed-effects model; if I2 > 50%, we employed a random-effects model in our meta-analysis.
3. Results
3.1. Case Series
We recruited 54 patients with a total of 94 ears. Twenty-five patients (41 ears) were male, and twenty-nine (53 ears) were female. The most common deformity was a lop ear (69.1 percent), followed by a constricted ear (12.8 percent). Forty-eight ears (51.1 percent) were graded excellent, thirty-nine (41.5 percent) were graded good, seven (14 percent) were graded moderate, and none were graded poor. The mean age at application was 5.81 ± 6.09 days. The mean duration of application for all patients was 32.13 ± 7.90 days (Table 3). Five of 94 ears (5.3 percent) experienced complications during the treatment period, which included dermatitis and skin excoriations. These skin complications healed spontaneously. Examples of successful correction are illustrated in Figure 3.
Table 3.
Summary of ear anomalies.
| n | % | ||
|---|---|---|---|
| Sex | M | 41 | 43.6 |
| F | 53 | 56.4 | |
| type | Lop ear | 65 | 69.1 |
| Constricted ear | 12 | 12.8 | |
| Helical rim deformity | 7 | 7.4 | |
| Stahl’s ear | 7 | 7.4 | |
| Prominent ear | 3 | 3.2 | |
| Grade | Excellent | 48 | 51.1 |
| Good | 39 | 41.5 | |
| Moderate | 7 | 7.4 | |
| Poor | 0 | 0 | |
| Age at application(days) | 5.81 ± 6.09 | 6.09 | |
| Duration of application(days) | 32.13 ± 7.90 | 7.9 | |
Figure 3.
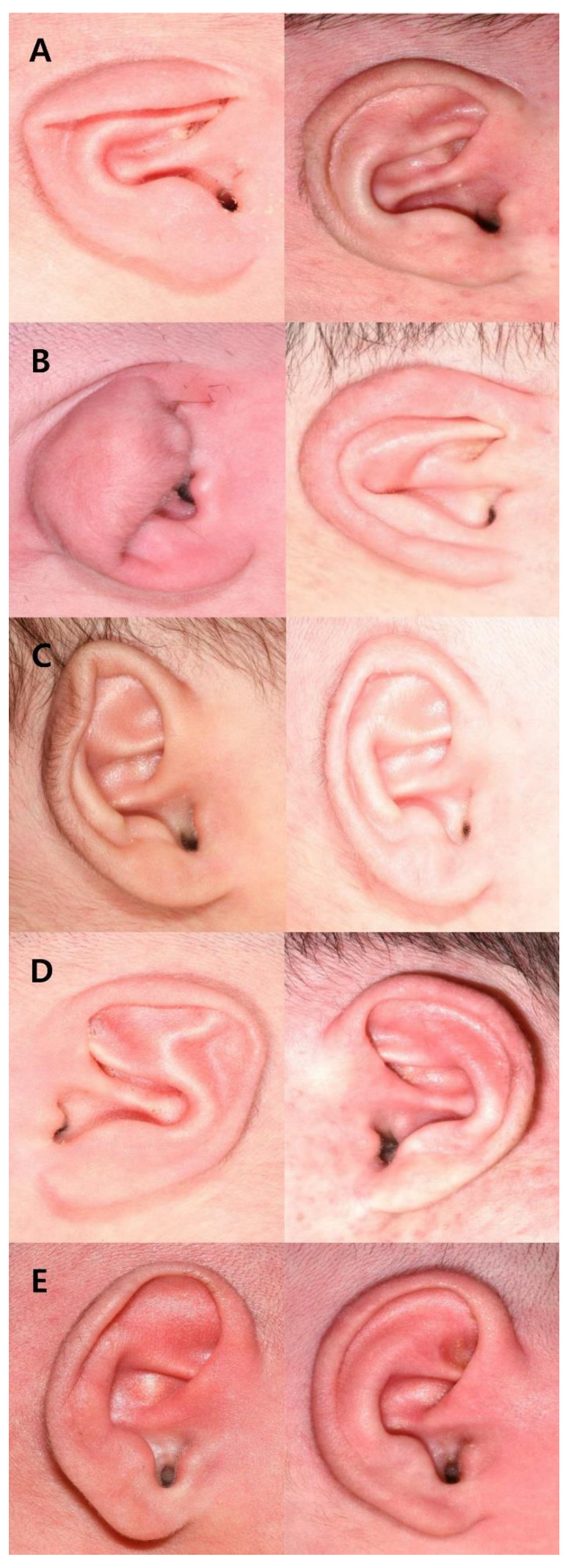
Typical results of classic ear molding for different types of ear deformities: (A) lop ear; (B) constricted ear; (C) helical rim deformity; (D) Stahl’s ear; (E) prominent ear.
3.1.1. Types of Anomalies and Outcomes
The posttreatment outcomes for the five types of ear deformities are shown in Table 4. The success rates (outcome graded as excellent and good) of the classic ear-molding method were 94%, 83%, 86%, 100%, and 100% for lop ear, constricted ear, helical rim abnormality, Stahl’s ear and prominent ear, respectively. The difference in outcome between the types was not statistically significant (p = 0.210).
Table 4.
Types of anomalies and outcomes.
| Grade | p | |||||
|---|---|---|---|---|---|---|
| Excellent | Good | Moderate | Poor | Total | ||
| Lop ear | 35(54) | 26(40) | 4(6) | 0(0) | 65(100) | 0.210 |
| Constricted ear | 3(25) | 7(58) | 2(17) | 0(0) | 12(100) | |
| Helical rim deformity | 2(29) | 4(57) | 1(14) | 0(0) | 7(100) | |
| Stahl’s ear | 6(86) | 1(14) | 0(0.0) | 0(0) | 7(100) | |
| Prominent ear | 2(67) | 1(33) | 0(0.0) | 0(0) | 3(100) | |
| Total | 48 | 39 | 7 | 0(0) | 94 | |
3.1.2. Patient Age and Duration of Application
The mean age at application was 5.81 ± 6.09 days. Within each outcome group, the average age at initiation was 4.58 days in the excellent group, 7.72 days in the good group, and 3.71 days in the moderate group. This was statistically significant (p = 0.035). The mean duration of application for all patients was 32.13 ± 7.90 days, with an average duration of application of 30.27 days in the group with excellent grading, 33.64 days in the group with good grading, and 36.43 days in the group with moderate grading. The difference in the duration of application between the groups was statistically significant (p = 0.044), as shown in Table 5.
Table 5.
Comparison of outcome grading with duration and age at application.
| Excellent | Good (n = 39) | Moderate (n = 7) | Total (n = 94) | p | |
|---|---|---|---|---|---|
| (n = 48) | |||||
| Age at application (days) | |||||
| Mean ± SD | 4.58 ± 4.74 | 7.72 ± 7.28 | 3.71 ± 4.64 | 5.82 ± 6.09 | 0.035 a |
| Median(range) | 4 (1–22) | 4 (1–22) | 2 (1–22) | 4 (1–22) | 0.007 b |
| Duration of application (days) | |||||
| Mean ± SD | 30.27 ± 8.58 | 33.64 ± 7.07 | 36.43 ± 2.94 | 32.13 ± 7.90 | 0.044 a |
| Median(range) | 35 (15–47) | 35 (15–47) | 35 (15–47) | 35 (15–47) | 0.159 b |
a: one way ANOVA. b: Kruskal Wallis test.
3.2. Systematic Review
3.2.1. Success Rate
A forest plot for the success rate is shown in Figure 4. A total of nine studies were included in the classic method group, and six studies were included in the commercial product group for this comparison. The results were extracted using a random-effects model because of high heterogeneity. The classic method group showed a statistically smaller success rate, with a proportion of 0.79 (95% CI = 0.69 to 0.86), than the commercial product group, with a proportion of 0.83 (95% CI = 0.76 to 0.94).
Figure 4.

A forest plot of the success rate [4,7,8,9,10,11,12,13,14,15,16,17]. The classic ear-molding method showed substantial efficacy in the treatment of newborn auricular deformities.
3.2.2. Complication Rate
A forest plot for the complication rate is shown in Figure 5. A total of six studies were included in the classic method group, and six studies were included in the commercial product group for this comparison. The results were extracted using a fixed-effects model in the classic method group because of low heterogeneity (I2 = 1%). A random-effects model was used because of high heterogeneity in the commercial product group (I2 = 85%). The classic method group showed a statistically smaller complication rate, with a proportion of 0.05 (95% CI = 0.03 to 0.10), than the commercial product group, with a proportion of 0.11 (95% CI = 0.06 to 0.19).
Figure 5.

A forest plot of the complications [4,7,8,9,10,11,12,13,14,15,17]. The classic method showed a lower complication rate than commercial products.
4. Discussion
Congenital ear deformities occur in 5% to 15% of infants [14,16]. Patients with congenital ear deformities tend to suffer psychological distress manifesting as anxiety, low self-esteem, and behavioral problems [12]. Traditionally, auricular deformities have been corrected surgically at 6 years of age [18]. Recently, nonsurgical management by ear molding has emerged as a favorable approach for newborn auricular deformities. Ear molding has shown much better outcomes in the correction of auricular deformities than otoplasty [13]. Ear molding not only spares operative morbidity but also allows for much earlier correction compared to surgical options, which usually address deformities only after the auricle has reached its adult size.
Commercial products are mostly used for ear molding of auricular deformities. However, costs for commercial products are expensive, placing them beyond the affordability of most parents from rural areas [6]. Therefore, the advantage of this nonsurgical intervention to correct auricular deformities is not possible for many infants. In contrast, the classic ear-molding method is much cheaper than commercial ear-molding products, and the materials needed for classic ear molding are easy to obtain. Because of these advantages, the classic ear-molding method can be another treatment option for patients whose families cannot afford commercial products.
It should be noted that commercial products are well-promoted, and their effectiveness has been intensively described in articles in the last 10 years. During this period, there was a lack of research on classic ear molding. Through this study, we confirmed the efficacy of the classic method of ear molding. In the case series, we achieved a high success rate in the correction of ear deformities using classic ear molding. Through a systematic review, we determined that the classic ear-molding method showed substantial efficacy in the treatment of newborn auricular deformities (79% and 87%) and a lower complication rate than commercial products (5% and 11%).
To achieve satisfactory outcomes, the timing of ear molding is most important [19]. The ideal intervention of auricular deformities is started within the first 2 weeks after birth. Infants older than 2 weeks show poor outcomes of correction and require a longer period of molding for successful correction [20,21]. Considering these points, it was presumed that early application of classic ear molding (5.81 ± 6.09 days) (Table 3) had an effect on the high success rate. Patient age at application and duration of molding were correlated with the outcome (p = 0.035 and p = 0.044, respectively) (Table 5). There was a difference in the average age at initiation in each group. This does not mean that earlier molding gives poorer results, but it may suggest that the appropriate timing of classic ear molding could be 4–5 days. However, this study was not designed to determine the appropriate timing of classic ear molding. There should be a lot of logical leaps to conclude that the appropriate timing of classic ear-molding could be 4–5 days. Further research is needed. Neither age at application nor duration of application had clinical significance because most patients started treatment within 2 weeks of birth. The type of auricle deformity is also a crucial factor affecting the efficacy [1]. However, there was no difference in the outcome of classic ear molding depending on the type of deformity in our study (p = 0.21) (Table 4).
There were several limitations in our study. First, this was a retrospective study. However, every attempt was made to minimize review bias by blinding reviewers to each other and clinical details. Second, there was a small number of patients with various types of deformities. This may have led to inaccurate statistical results, which need further analysis of large sample data to draw more scientific conclusions. Third, a short period of follow-up may be insufficient to conclude that the treatment outcomes can be maintained over time. Long-term follow-up demonstrated that obvious recurrent deformities did occur in some ears that initially were treated [22]. It is necessary to study whether classic ear molding could be effective for a long time. Fourth, the absence of objective tools for evaluating outcomes is another limitation of this study. Our data relied on independent plastic surgeon observations of the outcomes, which is not objective.
5. Conclusions
Ear molding is an effective nonsurgical treatment for ear anomalies and should be readily available and offered to parents [23]. Interspecialty collaboration is crucial to facilitate early identification and initiate prompt treatment [24]. Classic ear molding had remarkable and comparable therapeutic effects on neonatal auricular deformities. In addition, compared to other options, the classic ear-molding method is more suitable for infants with auricular deformities from socioeconomically vulnerable areas. Considering these advantages, the classic ear-molding method could be a better option for patients with congenital ear anomalies than commercial ear-molding products.
Author Contributions
J.K. (Jeonghoon Kim) drafted and analyzed the manuscript. T.J., J.C. and J.K. (Junhyung Kim) wrote sections of the manuscript. W.J. conceived the study idea, analyzed the data, wrote sections of the manuscript, and edited the figures. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Keimyung University Dongsan Medical Center (protocol code: 2022-09-072).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Funding Statement
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2021R1G1A1004556) and the Korea Medical Device Development Fund grant funded by the Korean government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: KMDFKD0003073G0003197).
Footnotes
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Chan S.L.S., Lim G.J.S., Por Y.C., Chiang M.F., Ho S., Saffari S.E., Chia H.L. Efficacy of ear molding in infants using the earwell infant correction system and factors affecting outcome. Plast. Reconstr. Surg. 2019;144:648e–658e. doi: 10.1097/PRS.0000000000006057. [DOI] [PubMed] [Google Scholar]
- 2.Rodríguez-Arias J.P., Gutiérrez Venturini A., Pampín Martínez M.M., Gómez García E., Muñoz Caro J.M., San Basilio M., Martín Pérez M., Cebrián Carretero J.L. Microtia ear reconstruction with patient-specific 3D models—A segmentation protocol. J. Clin. Med. 2022;11:3591. doi: 10.3390/jcm11133591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lennon C., Chinnadurai S. Nonsurgical management of congenital auricular anomalies. Facial Plast. Surg. Clin. N. Am. 2018;26:1–8. doi: 10.1016/j.fsc.2017.09.001. [DOI] [PubMed] [Google Scholar]
- 4.Tan S.T., Abramson D.L., MacDonald D.M., Mulliken J.B. Molding therapy for infants with deformational auricular anomalies. Ann. Plast. Surg. 1997;38:263–268. doi: 10.1097/00000637-199703000-00013. [DOI] [PubMed] [Google Scholar]
- 5.Lee D., Kim Y.S., Roh T.S., Yun I.S. Cryptotia recurrence lowering technique with additional acellular dermal matrix graft. Arch. Craniofacial Surg. 2019;20:170–175. doi: 10.7181/acfs.2019.00269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Xiong H., Wang X., Li G., Xu J., Zhai J., Chen S., Lu Y., Chen Y., Zheng Y., Yang H. Comparison of 2 ear molding systems for nonsurgical management of newborn auricular deformities. Ear Nose Throat J. 2021;100:652S–656S. doi: 10.1177/0145561320901398. [DOI] [PubMed] [Google Scholar]
- 7.Chang C.S., Bartlett S.P. A simplified nonsurgical method for the correction of neonatal deformational auricular anomalies. Clin. Pediatr. 2017;56:132–139. doi: 10.1177/0009922816641368. [DOI] [PubMed] [Google Scholar]
- 8.Leonardi A., Bianca C., Basile E., Ungari C., Arangio P., Filiaci F., Papoff P., Vellone V., Moretti C., Cascone P. Neonatal molding in deformational auricolar anomalies. Eur. Rev. Med. Pharmacol. Sci. 2012;16:1554–1558. [PubMed] [Google Scholar]
- 9.Mohammadi A.A., Imani M.T., Kardeh S., Karami M.M., Kherad M. Non-surgical management of congenital auricular deformities. World J. Plast. Surg. 2016;5:139–147. [PMC free article] [PubMed] [Google Scholar]
- 10.Tan S., Wright A., Hemphill A., Ashton K., Evans J. Correction of deformational auricular anomalies by moulding—Results of a fast-track service. N. Z. Med. J. 2003;116:U584. [PubMed] [Google Scholar]
- 11.Ullmann Y., Blazer S., Ramon Y., Blumenfeld I., Peled I.J. Early nonsurgical correction of congenital auricular deformities. Plast. Reconstr. Surg. 2002;109:907–913; discussion 914–915. doi: 10.1097/00006534-200203000-00013. [DOI] [PubMed] [Google Scholar]
- 12.Daniali L.N., Rezzadeh K., Shell C., Trovato M., Ha R., Byrd H.S. Classification of newborn ear malformations and their treatment with the earwell infant ear correction system. Plast. Reconstr. Surg. 2017;139:681–691. doi: 10.1097/PRS.0000000000003150. [DOI] [PubMed] [Google Scholar]
- 13.Doft M.A., Goodkind A.B., Diamond S., DiPace J.I., Kacker A., LaBruna A.N. The newborn butterfly project: A shortened treatment protocol for ear molding. Plast. Reconstr. Surg. 2015;135:577e–583e. doi: 10.1097/PRS.0000000000000999. [DOI] [PubMed] [Google Scholar]
- 14.Nigam M., Kotha V.S., Barra C., Baker S.B. Nonoperative molding of congenital ear deformities: The impact of birth-initiation delay on correction outcome. J. Craniofacial Surg. 2020;31:1588–1592. doi: 10.1097/SCS.0000000000006473. [DOI] [PubMed] [Google Scholar]
- 15.Patel V., Mazzaferro D.M., Swanson J.W., Taylor J.A., Bartlett S.P. Public perception of helical rim deformities and their correction with ear molding. J. Craniofacial Surg. 2020;31:741–745. doi: 10.1097/SCS.0000000000006400. [DOI] [PubMed] [Google Scholar]
- 16.Woo T., Kim Y.S., Roh T.S., Lew D.H., Yun I.S. Correction of congenital auricular deformities using the ear-molding technique. Arch. Plast. Surg. 2016;43:512–517. doi: 10.5999/aps.2016.43.6.512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhuang Q., Wei N., Zhou Q., Wang H., Wu Y., Chen Z., Yu D., Wang P., Shi H. Efficacy and timing of neonatal ear correction molding. Aesthetic Plast. Surg. 2020;44:872–878. doi: 10.1007/s00266-019-01596-y. [DOI] [PubMed] [Google Scholar]
- 18.Lee J.S., Kim J.S., Lee J.W., Choi K.Y., Yang J.D., Chung H.Y., Cho B.C. Correction of microtia with constriction features using a superficial temporal fascial flap combined with a rib cartilage graft. Arch. Plast. Surg. 2020;47:317–323. doi: 10.5999/aps.2018.01165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Byrd H.S., Langevin C.J., Ghidoni L.A. Ear molding in newborn infants with auricular deformities. Plast. Reconstr. Surg. 2010;126:1191–1200. doi: 10.1097/PRS.0b013e3181e617bb. [DOI] [PubMed] [Google Scholar]
- 20.Zhang J.L., Li C.L., Fu Y.Y., Zhang T.Y. Newborn ear defomities and their treatment efficiency with earwell infant ear correction system in china. Int. J. Pediatr. Otorhinolaryngol. 2019;124:129–133. doi: 10.1016/j.ijporl.2019.06.001. [DOI] [PubMed] [Google Scholar]
- 21.Joukhadar N., McKee D., Caouette-Laberge L., Bezuhly M. Management of congenital auricular anomalies. Plast. Reconstr. Surg. 2020;146:205e–216e. doi: 10.1097/PRS.0000000000006997. [DOI] [PubMed] [Google Scholar]
- 22.Zhong Z., Zhang J., Xiao S., Liu Y., Zhang Y. Long-term effectiveness of ear molding in infants using the earwell infant correction system in china. Plast. Reconstr. Surg. 2021;148:616–623. doi: 10.1097/PRS.0000000000008293. [DOI] [PubMed] [Google Scholar]
- 23.Javed M.U., Lazarou M., Kyle A., Jones N.W. Neonatal ear splinting for congenital ear deformities. J. Plast. Reconstr. Aesthet. Surg. 2020;73:2239–2260. doi: 10.1016/j.bjps.2020.05.064. [DOI] [PubMed] [Google Scholar]
- 24.Schultz K., Guillen D., Maricevich R.S. Newborn ear deformities: Early recognition and novel nonoperative techniques. Semin. Plast. Surg. 2017;31:141–145. doi: 10.1055/s-0037-1603958. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.