

Abstract
Background:
Rabies is among the most deadly and fatal diseases of all human diseases, once clinical symptoms appear. In developing countries, including Ethiopia, rabies prevention and control practices is not adequate. The study aimed to assess knowledge, attitude, and practices toward rabies prevention and control and identified factors associated with prevention and control practices.
Methods:
A community-based cross-sectional study was conducted from July 30 to August 30, 2021. A total of 326 dog-owner households were selected from the total number of 6500 dog-owner households using a simple random sampling method. Pretested and structured questionnaire were used to collect the data. The sections of the questionnaire includes socio-demographic, knowledge, attitude, and practice toward rabies prevention practices, and health and personal-related characteristics of the participants. The data was analyzed using SPSS version 24. Bivariate and multivariable logistic regression were used to determine the association variables. Finally, a p-value of less than 0.05 was considered as a cut-off point for statistical significance.
Results:
Of 326 households involved in the study, 52.8% of the participants were found to have poor rabies prevention and control practices. More than half (52.1%) of the respondents had good knowledge of rabies prevention and control practices, and 49.1% had a positive attitude. Only 28.2% of the respondents reported a history of dog bites. Factors associated with good rabies prevention and control practices were; having good knowledge of human rabies virus [(Adjusted Odd Ratio (AOR) = 2.41 (95% CI: 2.25−4.83)], having good attitude on prevention and control [AOR = 2.06 (95% CI: 1.95–3.82)], having only one dog per household [AOR = 2.46 (95% CI: 1.25–4.83)], availability of vet clinic within 30 min distance from residents [AOR = 9.32 (95% CI: 4.19–20.70)], and getting health information from Mass media [AOR = 3.68(95% CI: 1.74–7.77)] or Health workers [AOR = 3.16 (95% CI: 1.60–6.23)].
Conclusions:
More than half (52.1%) of the participants had poor rabies prevention and control practices. Improving rabies prevention and control practices through improving the knowledge and attitude of the community is important to protect public health.
Keywords: Rabies, zoonotic disease, prevention and control practices, west Hararghe zone, Ethiopia
Background
Rabies, a viral zoonotic disease categorized as a neglected tropical disease, kills tens of thousands of people every year, mostly among underserved populations in Africa and the Asia region.1,2 More than 95% of human rabies deaths result from the bites of infected dogs.1,2 Rabies is almost always fatal,3–5 but it can be prevented by vaccination before and/or after suspected or proven exposure to the virus.4,6 Nearly 59,000 human deaths globally are attributable to rabies annually,7–9 of which more than a third occur in Africa.8,9
Dogs are the principal vector for human rabies and are responsible for more than 99% of human cases. Therefore, controlling rabies in dogs is the first priority for the prevention of human rabies.6,10 Many developing countries have recently faced public health challenges due to rabies, even though some areas have remained free from rabies.11 Similarly, rabies disease has an economic burden, particularly in developing countries.6 Therefore, rabies prevention and control, in general, must be adopted to restrict or eradicate virus transmission by immunizing selected reservoir populations.12
The prevention and control of human rabies have become difficult because of poor dog management, a lack of public knowledge, a lack of diagnostic capacity, and a lack of emphasis by the veterinary profession.13 Public awareness, health education, dog vaccination, and the availability and accessibility of post-exposure prophylaxis (PEP) are keys to rabies prevention and control.2,14,15 Additional measures such as dog population management and cooperation from all stakeholders, including dog owners, improve the cost-effectiveness of the vaccination intervention.14,16,17
In most developing countries, the number of patients who receive post-exposure prophylaxis has steadily increased over time, particularly in urban areas due to dog-related rabies.18 In sub-Saharan Africa, most of the rabies cases in animals and humans are caused by the canine rabies virus.18
In Ethiopia, rabies is a major public health concern, and highly endemic. For example, according to a systematic review and meta-analysis conducted in Ethiopia, the pooled prevalence of rabies was accounted for 32%, of which the pooled prevalence of rabies in humans accounted for 33%.19 Another study conducted in Ethiopia reported that the level of good prevention practices of rabies accounted for 43.3%.20 Similarly, another study conducted in Ethiopia revealed that about 51.9% of the respondents had a good knowledge, attitude, and practice.21
According to another study conducted in Ethiopia, the annual suspected rabid dog exposures were estimated at 135, 101, and 86 bites in urban, rural highland, and rural lowland districts, respectively, to about 1, 4, and 3 deaths per 100,000 population. According to the findings, an annual estimate of approximately 3200 human deaths results in approximately 194,000 DALYs per year and 97,000 exposed persons require on average 2 million USD in treatment costs per year across the country.22
Besides these problems, to our knowledge, there is no adequate information or evidence on the current status of rabies prevention and control practices and associated risk factors among dog owners households in Ethiopia, particularly in west Hararghe zone.
Therefore, the current study aimed to assess the knowledge and practice of rabies prevention and control measures among dog owners in Chiro Town, West Hararghe Zone, Oromia Regional State, and the factors that might impact them.
The finding of the current study can be used by concerned organizations/bodies, including federal, zonal, and town health sectors, livestock agencies, non-governmental organizations, and different stakeholders to take an appropriate measures.
Materials and methods
Study area, design, and period
The cross-sectional study was conducted in Chiro town, west Hararghe zone, Oromia regional state, Ethiopia, from July 30 to August 30, 2021. The town is located 326 km from Addis Ababa, the capital of Ethiopia. The town is divided into four kebeles (the smallest administrative unit in the country) with an estimated population of 84,000 people living in 1500 households. In the town, there are an estimated dog-owner households of 6500.
Source and study population
All dog-owner households represented the source population while the selected dog-owner households were the study population. The study included dog-owner households of the town who had a dog; dog with at least 3 months old prior; be a permanent resident of the town and have lived in town for at least 6 months. Dog-owner households that had lived less than 6 months in the town were excluded from this study. The dog-owner households were registered and the required sample size was drawn from it.
Sample size determination
The sample size for this study was calculated based on a previous study conducted in Ethiopia that reported 74.2% good rabies prevention practice.17 A single population formula was used to calculate the sample size with a 95% confidence interval and a 0.05 margin of error. Finally, a total of 326 dog owners were included in the data collection considering the 10% (30) non-response rate.
Therefore n = 296. By consideration a non-response rate of 10%, (10)/(100) × 295 = 39.5. n = 295 + 30 = 326.
Sampling procedure/sampling techniques
Before data collection, the town was classified into four kebeles: kebele 01 (had 1981 (30.5%) dog owner households); kebele 02 (had 1488 (22.9%) dog owners households); kebele 03 (had 1881 (28.9%) dog owners households), and kebele 04 (had 1150 (17.7%) dog owners households), yielding a total of 6500 dog owner households. A total of 326 dog-owner households were selected using a simple random sampling method after a proportional allocation of study participants for each kebele. Then, 99, 75, 94, and 58 study participants were selected from Kebele 1, 2, 3, and 4, respectively (Figure 1).
Figure 1.
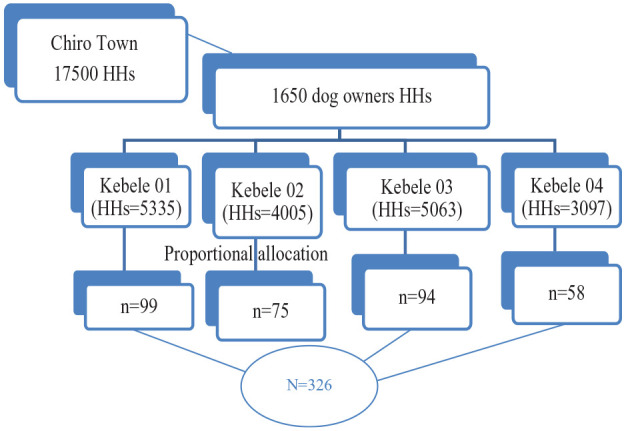
Sampling procedure or techniques used to select the study participants, 2022. Keys: HH: households; n: number of participants.
Data collection method
Data was collected using a structured and pretested questionnaire by five trained health professionals.
The questionnaire was valid and reliable as it was adapted from world health organization2,12–14 and similar researches.15–18The socio-demographic characteristics, rabies prevention and control practices, attitude toward rabies prevention practices, knowledge about rabies and its prevention, and health and personal-related characteristics of the participants were assessed using 8, 7, 7, 5, and 4 questions, respectively. Data was collected through face-to-face interviews using questionnaire (paper record).
Data quality control
The questionnaire was first prepared in the English version and then translated into the local language (Afan Oromo) and back translated into English by a third person to verify consistency. The data was collected after training was provided to the data collectors. Furthermore, the data collection tool (questionnaire) was pretested on the 5% of the portico check its clarity, sequence, applicability, and validity. Then, the questionnaire was modified, and the second version was used to collect the data. Each day, the completeness and consistency of the questionnaires were checked to ensure the quality of the collected data. Finally, the data were cross-checked using a double data entry.
Data processing and analysis
The collected data were sorted, coded, and entered into Epi-data version 3.1. After the data was cleaned by checking for errors, it was exported to SPSS version 24. Each question developed to assess knowledge, attitude, and prevention (KAP) practice was changed into a dichotomous variable (yes or no). The knowledge, attitude, and practice questions were recoded into the various variables throughout the analysis and coded as (yes = 1) and (no = 0). Five, six, and seven questions were used to assess the knowledge, attitude, and rabies prevention practice, respectively.
Based on the mean score, knowledge and rabies prevention practice were categorized as good for those who had a score above or equal to the mean and poor for those who had a score below the mean. The study participants’ attitudes toward rabies and its prevention were classified as positive for those who scored above or equal to the mean and negative for those who scored below the mean.
Bivariate and multivariable logistic regression analyses were used to assess factors associated with rabies prevention and control practices. By using multivariate analysis, the adjusted odds ratio along with 95% CI was estimated to identify predictors of rabies prevention and control practices. Finally, a p-value of less than 0.05 was considered as a cut-off point for statistical significance.
Results
Socio-demographic characteristics of study participants
Overall, 326 dogs-owner households participated in the study with a response rate of 100%. More than half (53.7%) of the study participants run private businesses, followed by 112 (34.4%) of government workers. About three-fourths (76.1%) of households have one dog (Table 1).
Table 1.
Socioeconomic characteristics of dog owners in Chiro, West Hararghe zone, Oromia region, Ethiopia, 2021.
| Variables (n = 326) | Classification | Frequency (Percentage) |
|---|---|---|
| Sex | Male | 176 (54.0) |
| Female | 150 (46.0) | |
| Age group | 18–29 | 48 (14.7) |
| 30–45 | 204 (62.6) | |
| >45 | 74 (22.7) | |
| Marital status | Single | 27 (8.3) |
| Married | 256 (78.5) | |
| Divorced | 26 (8.0) | |
| Widowed | 17 (5.2) | |
| Occupations | Government | 112 (34.4) |
| Private | 175 (53.7) | |
| Housewife | 19 (5.8) | |
| Farmer | 8 (2.5) | |
| Others | 12 (3.7) | |
| Educations | No education | 58 (17.8) |
| Primary | 103 (31.6) | |
| Secondary | 55 (16.9) | |
| Higher education | 110 (33.7) | |
| Household size | 1–3 | 173 (53.1) |
| 4–6 | 112 (34.4) | |
| Above 6 | 41 (12.6) | |
| Total dog owned by households | 12 and above | 248 (76.1)78 (23.9) |
Health service and personal-related characteristics
Two hundreds twelve (64.7%) of the respondents resided near the veterinary clinic (within 30 min of walking), while 94 (28.2%) of the respondents had a history of dogs bites. However, 207 (63.5%) of respondents reported the availability of health services for dogs in veterinary clinics (Table 2).
Table 2.
Participants’ health and personal characteristics in Chiro City, west Hararghe zone, Oromia region, Ethiopia 2021.
| Variables (n = 326) | Category | Frequency (Percent) |
|---|---|---|
| Veterinary clinics within 30 min walks from residents | Yes | 212 (64.7) |
| No | 114 (35.3) | |
| Availability of health services for dog in veterinary clinics | Yes | 207 (63.5) |
| No | 119 (36.5) | |
| History of dog bites | Yes | 94 (28.8) |
| No | 232 (71.2) | |
| The main source of health information regarding rabies and its prevention. | Mass media | 109 (33.4) |
| Health professional | 111 (34.0) | |
| Friend/ neighbor | 106 (32.5) |
Knowledge and attitude toward rabies prevention and control practice
Of all respondents, 92% and 94.5% have heard about the dog-mediated human rabies virus, and reported that it is important to wash the hands after feeding and grooming the dogs, respectively. Overall, 52.1% of respondents had good knowledge (Table 3).
Table 3.
Knowledge toward rabies prevention and control practices of dog owners in Chiro town, West Hararghe, Oromia region, Ethiopia, 2021.
| Variables (n = 326) | Category | Frequency (Percent) |
|---|---|---|
| Heard of dog mediated human rabies diseases | Yes | 300 (92.0) |
| No | 26 (8.0) | |
| It is important to wash the hands after feeding and grooming the dogs | Yes | 308 (94.5) |
| No | 18 (5.5) | |
| Dog mediated human rabies have vaccine | Yes | 246 (75.5) |
| No | 80 (24.5) | |
| Rabies are transmitted from dog to human | Yes | 324 (99.4) |
| No | 2 (0.6) | |
| Rabies are transmitted from animal to animal | Yes | 246 (75.5) |
| No | 80 (24.5) | |
| Overall mean knowledge level to ward rabies prevention | Good | 170 (52.1) |
| Poor | 156 (47.9) |
Regarding the attitudes of dog owners toward rabies prevention and control, 98.2% and 99.1% believed that rabies is a fatal disease and can be transmitted from dogs to humans, respectively. In general, 49.1% of respondents had a positive attitude. While 235 (72.1%) believe that rabies outbreaks can be prevented by vaccination of dogs (Table 4).
Table 4.
Attitude toward rabies prevention and controls practices among dog owners in Chiro town, West Hararghe, Oromia region, Ethiopia, 2021.
| Variables (n = 326) | Category | Frequency (Percent) |
|---|---|---|
| I believe that rabies is a fatal disease | Yes | 320 (98.2) |
| No | 6 (1.8) | |
| I believe that rabies can be transmitted by dogs | Yes | 323 (99.1) |
| No | 3 (0.9) | |
| I believe that rabies can be transmitted by other animals | Yes | 215 (66.0) |
| No | 111 (34.0) | |
| I believe that rabies outbreaks can be prevented by vaccination of dogs | Yes | 235 (72.1) |
| No | 91 (27.9) | |
| I believe that suspected rabies can be confirmed by laboratory tests | Yes | 222 (68.1) |
| No | 104 (31.9) | |
| I believe that there are no locally available methods of treatment for dog mediated human rabies | Yes | 130 (39.9) |
| No | 196 (60.1) | |
| Overall mean attitudes level toward rabies prevention and controls | Positive | 160 (49.1) |
| Negative | 166 (50.9) |
Rabies prevention and control practices of dog owners
Of all the residents, 62.6% restricted the movement of their dogs outside, and 60.4% tied up their dogs full time in their homes. In addition, 85.3% of dog owners vaccinated their dogs in the last 12 months of the year. However, only 19% of the respondents said they wear PPE while handling dogs. Overall, the study found that 52.8% of the respondents had poor rabies prevention and control practices (Table 5).
Table 5.
Rabies prevention and control practices among dog owners in Chiro town, West Hararghe zone, Oromia region, Ethiopia, 2021.
| Variables (n = 326) | Frequency (Percent) | |
|---|---|---|
| Not allowing family members to play with their dogs | Yes | 109 (33.4) |
| No | 217 (66.6) | |
| Wear personal protective equipments while handling dog(s) | Yes | 62 (19.0) |
| No | 264 (81.0) | |
| Restricting dog movement outside | Yes | 204 (62.6) |
| No | 122 (37.4) | |
| Tied up your dog’s 24 h a day to avoid or reduce the contact with you or your family | Yes | 197 (60.4) |
| No | 129 (39.6) | |
| Family members having contact with stray dogs | Yes | 80 (24.5) |
| No | 246 (75.5) | |
| Vaccinated your dogs in the last 12 months | Yes | 278 (85.3) |
| No | 48 (14.7) | |
| Feeding your dogs from a safe source or home food | Yes | 187 (57.4) |
| No | 139 (42.6) | |
| Overall mean practices of rabies prevention and control | PoorGood | 172 (52.8)154 (47.2) |
Factors associated with rabies prevention and control practices
The study revealed that those had a good knowledge, positive attitude, above one dogs, near to the veterinary clinic, had accessed information from media, and get information from health workers were about 2.4 [AOR = 2.41(95% CI: 2.25–4.8)], 2.03 [AOR = 2.06 (95% CI: 1.95–3.8)], 2.45 [(AOR = 2.46 (95% CI: 1.25–4.8)], 9.3 [(AOR = 9.32 (95% CI: 4.19–20.70)], 3.68[(AOR = 3.68 (1.74–7.77)] and 3.16 [(AOR = 3.16 (1.60–6.23)] times more likely to report good prevention and control practices, respectively compared to their counter parts (Table 6).
Table 6.
Factors associated with rabies prevention and control practices in the Chiro town of the West Hararghe zone, Oromia region, Ethiopia 2021.
| Variables (n = 326) | Good practices | Poor practices | COR (CI, 95%) | AOR (CI, 95%) | |
|---|---|---|---|---|---|
| Frequency (%) | Frequency (%) | ||||
| Sex | Male | 94 (53.4) | 82 (46.6) | 0.945 (0.611–1.462) | 0.581 (0.323–1.045) |
| Female | 78 (52) | 72 (48) | Ref. | Ref. | |
| Age group | 18–29 | 23 (47.9) | 25 (52.1) | 1.35 (0.652–2.798) | 3.308 (0.997–10.98) |
| 30–45 | 108 (52.9) | 96 (47.1) | 1.104 (0.647–1.885) | 1.185 (0.586–2.398) | |
| >45 | 41 (55.4) | 33 (44.6) | Ref. | Ref. | |
| Marital status | Single | 14 (51.9) | 13 (48.1) | 1.327 (0.389–4.52) | 0.773 (0.103–5.787) |
| Married | 135 (52.7) | 121 (47.3) | 1.280 (0.473–3.469) | 0.658 (0.171–2.536) | |
| Divorced | 13 (50) | 13 (50) | 1.429 (0.416–4.909) | 5.44 (0.941–31.497) | |
| Widowed | 10 (58.8) | 7 (41.2) | Ref. | Ref. | |
| Occupations | Government | 57 (50.9) | 55 (49.1) | 0.965 (0.293–3.174) | 0.318 (0.036–2.78) |
| Private | 95 (54.3) | 80 (45.7) | 0.842 (0.261–2.713) | 0.776 (0.134–4.504) | |
| Housewife | 7 (36.8) | 12 (63.2) | 1.714 (0.396–7.427) | 0.791 (0.101–6.184) | |
| Farmer | 7 (87.5) | 1 (12.5) | 0.143 (0.013–1.546) | 0.092 (0.05–1.566) | |
| Others | 6 (50) | 6 (50) | Ref. | Ref. | |
| Educations | No education | 35 (60.3) | 23 (39.7) | 0.645 (0.345–1.253) | 0.36 (0.07–1.855) |
| Primary | 54 (52.4) | 49 (47.6) | 0.907 (0.530–1.554) | 0.195 (0.041–0.924)* | |
| Secondary | 28 (50.9) | 27 (49.1) | 0.907 (0.505–1.842) | 0.349 (0.078–1.57) | |
| Higher education | 55 (50) | 55 (50) | Ref. | Ref. | |
| Household size | 1–3 | 80 (46.2) | 93 (53.8) | 3.17 (1.494–6.73) | 1.361 (0.533–3.473) |
| 4–6 | 62 (55.4) | 50 (44.6) | 2.199 (1.003–4.822) | 1.07 (0.371–2.547) | |
| >6 | 30 (73.2) | 11 (26.8) | Ref. | Ref. | |
| Number of dog owned by household | 1 | 118 (47.6) | 130 (52.4) | 2.479 (1.442–4.26) | 2.456 (1.249–4.827)* |
| 2 and above | 54 (69.2) | 24 (30.8) | Ref. | Ref. | |
| Veterinary clinic within 30 min walks from residents | Yes | 75 (35.4) | 137 (64.6) | 10.42 (5.794–18.75) | 9.319 (4.195–20.70)* |
| No | 97 (85.1) | 17 (14.9) | Ref. | Ref. | |
| Availability of health services for dog in vet clinic | Yes | 92 (44.4) | 115 (55.6) | 2.564 (1.601–4.106) | 0.978 (0.446–2.142) |
| No | 80 (67.2) | 39 (32.8) | Ref. | Ref. | |
| History of dog bites | Yes | 48 (51.1) | 46 (48.9) | 1.1 (0.681–1.778) | 1.298 (0.599–2.812) |
| No | 124 (53.4) | 108 (46.6) | Ref | Ref. | |
| Source of health information of human rabies | Mass media | 55 (50) | 54 (50) | 2.172 (1.245–3.790) | 3.680 (1.744–7.765)* |
| Health worker | 44 (40) | 67 (60) | 3.368 (1.924–5.897) | 3.161 (1.604–6.228)* | |
| Friend/neighbor/Others | 73 (69) | 33 (31) | Ref. | Ref. | |
| Mean knowledge of human rabies virus | Good | 73 (42.9) | 97 (57.1) | 2.308 (1.48–3.603) | 2.416 (2.249–4.827)* |
| Poor | 99 (63.5) | 57 (36.5) | Ref. | Ref. | |
| Mean attitudes of human rabies prevention and controls | GoodPoor | 69 (43.1)103 (62) | 91(56.9)63 (38) | 2.156 (1.385–3.358)Ref. | 2.06 (1.951–3.827)*Ref. |
Ref: reference.
significancy: p-value < 0.05
Discussions
A community-based cross-sectional study was conducted to assess rabies prevention and control practices and associated factors among dog owners households in Chiro Town, West Hararghe, Oromia, Ethiopia. A total of 326 dog-owner households were selected from the total number of 6500 dog-owner households using a simple random sampling technique.
The findings indicated that the overall level of good rabies prevention and control practice was 47.2% in Chiro town, which is lower than the finding of another study conducted in Rwanda (66%)23 and in Ethiopia (61.3%).10 The variation may be related to the access to information, difference in the scope of the study and characteristics of the participants. The current study reported a higher good practice than the finding of another study in Nigeria that reported 24.7% of respondents had good rabies prevention practices.24 The variation may be attributed to the difference in management practices, access to health information, the scope of study location and education status of residents.
In the current study, 52.1% of the respondents had good knowledge about the prevention and control of rabies which was in line with the finding of another study conducted in Ethiopia, which reported 56.1% of the participants had good knowledge toward rabies prevention and control practices.10 However, higher than the finding of another study conducted in Nigeria that reported 43.7% of respondents had good knowledge of the cause and transmission of rabies.24 The variation might be related to the variation in educational status, access to sources of information, awareness and other services used to prevent and control rabies.
In the current study about 50.9% of the respondents had poor attitudes toward prevention and control of rabies which was in consistent with the finding of prior study conducted in Ethiopia that reported 43.8%,10 but lower compared with a finding from Rwanda (82.5%).23 The variation may be related to sources of information, difference in the scope of the study and characteristics of the participants
The current study revealed that about 28.2% of the respondents reported a previous history of dog bites which was consistent with the finding from Nigeria which reported 23.7%.24 The difference might be related to the differences in the health systems of the countries, sources of information, and application of rabies prevention and control strategies. Among the participants, 34% received health information about dog-mediated human rabies from health workers, followed by from media (33.4%). However, the study conducted in Nigeria reported 82.4% of respondents had their health information about dog-mediated human rabies from friends and neighbors.24
Respondents who obtained sources of health information from the media and health workers were 3.68 and 3.16 more odds of having good practice compared to their counterparts, respectively. This was supported by another study conducted in Tanzania.25 Furthermore, the current study found statistically significant association between knowledge, attitude about rabes prevention and control, and owners’ rabies prevention and control practices.
In general, the current study revealed that there is a need to improve rabies prevention and control practices in the community in order to reduce the health consequences posed by rabies. The finding of this study elicits further awareness creation program through different mechanism for effective prevention of rabies in the community. Furthermore, implementation of rabies prevention strategies, including reduction of animal populations, mass vaccination, cooperation and coordination, adequate surveillance and monitoring, and other public health measures can play a major role in rabies prevention and control.2
Conclusions
More than half of the participants had poor rabies prevention and control practices. Similarly, the study found the association of practice and knowledge and attitude of dog owners. Therefore, there is a need to increase the prevention and control practices as well as the knowledge and attitude of dog owners to rabies disease and to protect public health. There is a need to implement a multi-disciplinary approach with stakeholders such as veterinarians, community members, public health workers, and other governmental and non-governmental organizations.
Acknowledgments
We would like to acknowledge Haramaya University, College of Health and Medical Sciences and west Hararghe Zone Health office for their support throughout this study.
Footnotes
Contributions of authors: MJA conceived the idea and collected, analyzed and interpreted the data and played a major role. The authors (DAM, MD, GD, and AG) contributed to data analysis, writing, and editing the document. All authors (MJA, DAM, GD, MD and AG) gave valuable ideas for the manuscript. Finally, the authors read and approved the final version to be published and agreed on all aspects of this work.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate: Ethical approval for this study was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the Faculty of Health and Medical Sciences, Haramaya University. Informed, voluntary and written consent was obtained from all individuals and concerned bodies included in this study. Confidentiality was also assured. All the procedures are done per the ethical guidelines of the institution.
Consent for publication: Not applicable
ORCID iDs: Gebisa Dirirsa  https://orcid.org/0000-0003-0246-6253
https://orcid.org/0000-0003-0246-6253
Dechasa Adare Mengistu
https://orcid.org/0000-0002-0076-5586
Abraham Geremew
https://orcid.org/0000-0001-5476-9673
Data Availability: All relevant data are within the manuscript and its Supporting Information files.
References
- 1. Hampson K, Coudeville L, Lembo T, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis 2015; 9(4): e0003709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. World Health Organization. WHO expert consultation on rabies: third report. World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/272364/9789241210218-eng.pdf (accessed 12 September 2021).
- 3. Garcia R, Abundabar F, Cruz-Cambe D, et al. Animal bite patterns and implementation of rabies prevention and control program in animal bite treatment center. Nur Primary Care 2019; 3(3): 1–5. [Google Scholar]
- 4. Rupprecht CE, Salahuddin N. Current status of human rabies prevention: remaining barriers to global biologics accessibility and disease elimination. Expert Rev Vaccines 2019; 18(6): 629–640. [DOI] [PubMed] [Google Scholar]
- 5. Li D, Liu Q, Chen F, et al. Knowledge, attitudes and practices regarding to rabies and its prevention and control among bite victims by suspected rabid animals in China. One Health 2021; 13: 100264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. González-Roldán JF, Undurraga EA, Meltzer MI, et al. Cost-effectiveness of the national dog rabies prevention and control program in Mexico, 1990-2015. PLoS Negl Trop Dis 2021; 15(3): e0009130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Fahrion AS, Taylor LH, Torres G, et al. The road to dog rabies control and elimination-what keeps us from moving faster? Public Health Front 2017; 5: 103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Haselbeck AH, Rietmann S, Tadesse BT, et al. Challenges to the fight against Rabies—The landscape of policy and prevention strategies in Africa. Int J Environ Res Public Health 2021; 18(4): 1736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. WHO. Rabies. https://www.who.int/health-topics/rabies#tab=tab_1 (accessed March 2, 2022).
- 10. Hagos WG, Muchie KF, Gebru GG, et al. Assessment of knowledge, attitude and practice towards rabies and associated factors among household heads in Mekelle city, Ethiopia. BMC Public Health 2020; 20: 57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kiratitana-olan K, Chaisowwong W, Thongkorn K, et al. Keys to good knowledge, attitude and practice on rabies prevention in disease-free communities. Vet Integr Sci 2021; 19(3): 407–422. [Google Scholar]
- 12. Lankau EW, Cohen NJ, Jentes ES, et al. Prevention and control of rabies in an age of global travel: a review of travel- and trade-associated rabies events - United States, 1986-2012. Zoonoses Public Health 2014; 61(5): 305–316. [DOI] [PubMed] [Google Scholar]
- 13. WHO, Food and Agriculture Organization of the United Nations and World Organisation for Animal Health. Global elimination of dog-mediated human rabies, report of the rabies global conference 10-11 December 2015, Geneva, Switzerland. World Health Organization. [Google Scholar]
- 14. FAO. Developing a stepwise approach for rabies prevention and control. In: Proceedings of the FAO/GARC workshop, Rome, Italy, 2012. FAO Animal Production and Health Proceedings 18. [Google Scholar]
- 15. Mshelbwala PP, Weese JS, Sanni-Adeniyi OA, et al. Rabies epidemiology, prevention and control in Nigeria: scoping progress towards elimination. PLoS Negl Trop Dis 2021; 15(8): e0009617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Aklilu M, Tadele W, Alemu A, et al. Situation of rabies in Ethiopia: a five-year retrospective study of human rabies in Addis Ababa and the surrounding regions. J Trop Med 2021; 2021: 6662073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Letebrhan G, Gebretsadik B, Aregawi G, et al. Rabies prevention and control practice and associated factors among dog owners in Aksum town and LaelayMachew district, north Ethiopia. CC-BY 4.0 International license. 2018. DOI: 10.1101/436493. [DOI] [Google Scholar]
- 18. Aga AM, Hurisa B, Urga K. Current situation of rabies prevention and control in developing countries: Ethiopia perspective. J Infect Dis Preve Med 2016; 4: 128. [Google Scholar]
- 19. Belete S, Meseret M, Dejene H, et al. Prevalence of dog-mediated rabies in Ethiopia: a systematic review and meta-analysis from 2010 to 2020. One Health Outlook 2021; 3: 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Wolelaw GA, Yalew WA, Azene AG, et al. Rabies prevention practices and associated factors among household heads in Bure Zuria district, North West Ethiopia. Sci Rep 2022; 12: 7361. 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Nejash A, Boru M, Jemal J, et al. Knowledge, attitudes and practices towards rabies in Dedo district of Jimma zone, southwestern Ethiopia: a community based cross-sectional study. Int J Med Med Sci 2017; 9(5): 61–71. [Google Scholar]
- 22. Yohannes YB, Ikenaka Y, Ito G, et al. Assessment of DDT contamination in house rat as a possible bioindicator in DDT-sprayed areas from Ethiopia and South Africa. Environ Sci Pollut Res Int 2017; 24(30): 23763–23770. [DOI] [PubMed] [Google Scholar]
- 23. Ntampaka P, Nyaga PN, Niragire F, et al. Knowledge, attitudes and practices regarding rabies and its control among dog owners in Kigali city, Rwanda. PLoS One 2019; 14(8): e0210044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Abdulsalam AL, Oche MO, Awosan KJ, et al. Knowledge and practices regarding rabies prevention among dog owners in Sokoto Nigeria. Int J Sci Stud 2018; 6(4): 57–65. [Google Scholar]
- 25. Sambo M, Lembo T, Cleaveland S, et al. Knowledge, attitudes and practices (KAP) about rabies prevention and control: a community survey in Tanzania. PLoS Negl Trop Dis 2014; 8(12): e3310. [DOI] [PMC free article] [PubMed] [Google Scholar]