

Abstract
Background:
In a 2018 descriptive study, cancer incidence in children (age 0–19) in diagnosis years 2003–2014 was reported as being highest in New Hampshire and in the Northeast region.
Methods:
Using the Cancer in North America (CiNA) analytic file, we tested the hypotheses that incidence rates in the Northeast were higher than those in other regions of the United States either overall or by race/ethnicity group, and that rates in New Hampshire were higher than the Northeast region as a whole.
Results:
In 2003–2014, pediatric cancer incidence was significantly higher in the Northeast than other regions of the United States overall and among non-Hispanic Whites and Blacks, but not among Hispanics and other racial minorities. However, there was no significant variability in incidence in the states within the Northeast overall or by race/ethnicity subgroup. Overall, statistically significantly higher incidence was seen in the Northeast for lymphomas (RR 1.15; 99% CI 1.10–1.19), central nervous system neoplasms (RR 1.12; 99% CI 1.07–1.16), and neuroblastoma (RR 1.13; 99% CI 1.05–1.21).
Conclusion:
Pediatric cancer incidence is statistically significantly higher in the Northeast than in the rest of the United States, but within the Northeast, states have comparable incidence. Differences in cancer subtypes by ethnicity merit further investigation.
Impact:
Our analyses clarify and extend previous reports by statistically confirming the hypothesis that the Northeast has the highest pediatric cancer rates in the country, by providing similar comparisons stratified by race/ethnicity, and by assessing variability within the Northeast.
Keywords: childhood cancer, pediatric cancer, incidence, geographic, Northeast, race/ethnicity
Introduction
In 2018, Siegel et al. presented a report titled “Geographic Variation in Pediatric Cancer Incidence – United States, 2003–2014”, reporting that pediatric cancer incidence rates were highest in the Northeast and, by state, rates were “highest in New Hampshire (205.5 [per million per year]), DC (194.0), and New Jersey (192.3) and lowest in South Carolina (149.3) and Mississippi (145.2)”.1 The publication drew attention in New Hampshire where a pediatric cancer cluster and concerns about environmental pollution had received considerable media coverage.2,3 However, in that descriptive study, because no comparisons were formally tested, the importance of these findings was unclear. The purpose of this paper is to assess whether the Northeast region and New Hampshire are outliers in pediatric cancer incidence in the United States by testing the hypotheses that rates in the Northeast were higher than those in each of other three regions of the United States either overall or by race/ethnic group, or that rates in New Hampshire were higher than the Northeast region as a whole.
Materials and Methods
The Cancer in North America (CiNA) analytic file for researchers4 certified by the North American Association of Central Cancer Registries (NAACCR),5 was used to evaluate pediatric (ages 0–19 years) cancer incidence in the United States (US) during 2003–2014, the period reported by Siegel et al.1 Using age-standardized cancer incidence and rate ratios, we compared the individual states of the Northeast region (Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania Rhode Island, and Vermont) with the Northeastern region as a whole to identify outlier states, and we compared the Northeast with other United States Census regions, both overall and by race/ethnicity. Due to substantial variation in population distributions by race/ethnicity, with minorities comprising from 7% (Vermont) to 47% (New York) of state populations in the Northeast region (Supplementary Figure 1), we conducted separate analyses for each racial/ethnic population to calculate rate ratios comparing the Northeast with its constituent states, and to compare the Northeast with other US regions and the US as a whole.
All analyses were conducted using the Surveillance, Epidemiology, and End Results Program (SEER) statistical software package SEER*Stat version 8.3.9.6 SEER*Stat automatically suppressed cell sizes of <6 following NAACCR’s guidelines for data quality assurance.7 Race/ethnicity was defined using a combination of race and ethnicity variables provided in the CiNA data set, 1) race recode (White, Black, American Indian/Alaska Native (AIAN), Asian/Pacific Islander (API), Unknown) and 2) Origin Recode NAACCR Hispanic Identification Algorithm8 (Hispanic, non-Hispanic) to create the race/ethnicity variable for analysis with defined values of non-Hispanic White, non-Hispanic Black, non-Hispanic AIAN, non-Hispanic API and Hispanic (all races).9 Overall case counts included cases for which either race or ethnicity was unknown.
States can only contribute data to CiNA for years in which they meet criteria for high quality incidence data.10 Some data were excluded from the CiNA analytic file because of lack of permission from the state (Kansas) or failure to meet inclusion quality criteria during diagnosis years 2003 – 2014 (Nevada1); 2003 data were excluded for data quality reasons for Mississippi and Tennessee. Because data from California and Washington states were included, data from the smaller regional registries within these states were excluded to avoid double counting (Figure 1).5 Pediatric cases were selected from the “age recode with < 1 years olds” variable including 0–19 years age groups for the diagnosis years 2003 – 2014 using the International Classification of Childhood Cancer (ICCC) definition.11 Patients were included if tumor behavior was coded as “malignant”, “only malignant” in International Classification of Diseases for Oncology, 3rd edition (ICD-O-3)12, malignant 2010+ cases”6 and with one primary only or the first of two or more primaries were included. Cases from death certificate or autopsy reporting sources were excluded (Figure 1). We assessed 12 categories and 47 subtypes of invasive cancer defined by the ICCC as well as pediatric non-malignant brain tumors. Pediatric brain tumors were selected from the CiNA data set using the primary ICD-O-3 site codes C70.0 – C72.9 and C75.1 – C75.3 with benign or borderline malignant behavior (ICD-O-3 behavior code of /0 and /1); the analysis timeframe for these tumors was 2004 – 2014 based on the start date for data collection relative to benign or borderline malignant behavior nationally in 2004. For validation, case counts were compared with those reported by Siegel,1 taking into account an expectation of small differences in data selection criteria and the accrual of additional cases in the intervening years.
Figure 1.
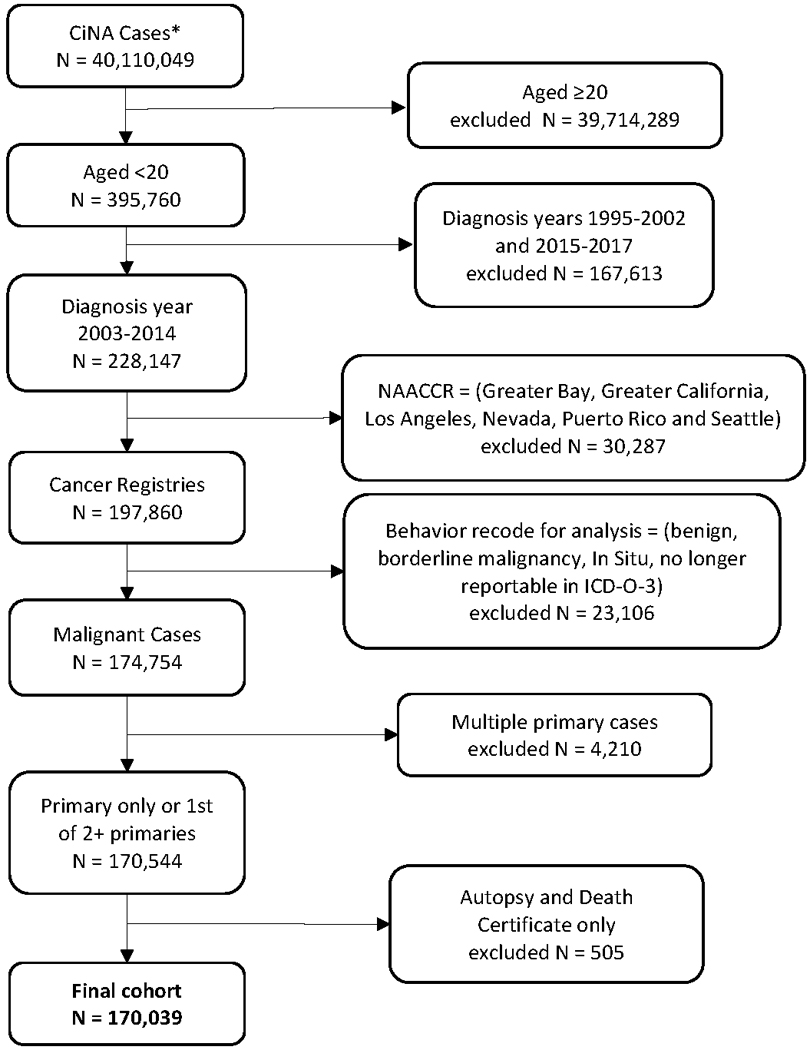
Derivation of Pediatric (0–19 years) Cancer Cases.
*Cancer in North America (CiNA). Kansas and diagnosis year 2003 for Mississippi and Tennessee not included.5
The study protocol was approved by the Institutional Review Board of the North American Association of Central Cancer Registries.
Statistical measures
Incidence rates in the four US regions (Northeast, Midwest, South, West) and states within regions, were directly standardized for age to the 2000 US population (19 age groups, Census P25–1130) and presented as rates per 1,000,000 with 95% confidence intervals. Overall incidence rates for United States (“All States”) are also reported. Where the number of cases was smaller than 10 no calculations were made, in accordance with the recommendations of Morris et al. relative to data stability.13 Incidence rates were broken down further by race/ethnicity within region and states as non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic American Indian/Alaska Native, and non-Hispanic Asian/Pacific Islander. Incidence rate ratios were calculated as the ratio of age-standardized rates to directly compare each region with the Northeastern Region, and compare each state within the Northeast Region with the Northeast as a whole. Standard errors and hence confidence intervals were calculated using Tiwari’s method that adjusts for the non-independence introduced by the overlap between the whole group (e.g., Northeast region) and subgroup (e.g., New Hampshire).14 The rate ratios were also calculated after stratification by race/ethnicity. To control the type 1 error rate, a Bonferroni correction was used within each race/ethnic group with a modified p value of 0.05/number of tests used to test the composite hypothesis that there is no difference in incidence rates between the Northeast and any of its states or the other three Regions. Specific details of the corrections are shown as footnotes below each table. To make the interpretation of the confidence intervals consistent with the Bonferroni-adjusted p values, the confidence intervals were individually set at 99%. In this way 95% overall confidence level was preserved and therefore when rate ratios and their confidence intervals are presented by race/ethnicity using forest plots, statistical significance at the 5% level after adjustment for multiple testing is indicated by a confidence interval that does not cross the vertical null value line (1.0). Where there were fewer than 10 cases within a state/race/ethnicity group, the rate ratio was not calculated, and this is indicated by ‘NA’. Invasive cancer subtypes and pediatric non-malignant brain tumors were analyzed in the same way. We used major cancer subtype categories and then presented more granular data for subtypes that showed significant differences within the Northeast region and compared to the rest of the United States as a post-hoc analysis.
Data Availability Statement:
The data are available by application to the North American Association of Central Cancer Registries.4
Results
The analytic file included 170,039 cases of first primary invasive cancers diagnosed in the United States from 2003 through 2014 in patients aged <20 years (Figure 1) and 21,419 non-malignant brain tumors diagnosed from 2004 through 2014. Overall, pediatric invasive cancer incidence was highest among non-Hispanic White children (185.8/million/year), followed by Hispanics (169.2), American Indians/Alaska Natives (149.6), Asian/Pacific Islanders (147.7), and Blacks (134.3) and incidence in the Northeast was significantly higher than the US for Whites and for Blacks (Table 1 and Supplementary Table 1). Incidence was significantly lower in the other three regions than the Northeast for all races combined and among non-Hispanic Whites; (Midwest: RR 0.91; 99% CI 0.89–0.94, South: RR 0.90; 99% CI 0.88–0.92, and West: RR 0.92; 99% CI 0.90–0.94). Similar results were seen for non-Hispanic Whites (Midwest: RR 0.89; 99% CI 0.87–0.92, South: RR 0.90; 99% CI 0.87–0.92, and West: RR 0.92; 99% CI 0.89–0.95). There were no significant differences in the comparison of each northeastern state with the Northeast as a whole (Figure 2). Similar but less precise estimates were seen among non-Hispanic Blacks by region (Midwest: RR 0.89; 99% CI 0.83–0.97, South: RR 0.92; 99% CI 0.86–0.98, and West: RR 0.92; 0.84–1.02), and among the larger northeastern states that had sufficient numbers to report. There were no significant regional differences in incidence among Hispanics (Midwest: RR 0.94; 99% CI 0.87–1.01, South: RR 1.03; 99% CI 0.98–1.09 and West: RR 0.98; 99% CI 0.93–1.04), but a significantly lower incidence was seen in Rhode Island than the Northeast as a whole (RR 0.58; 99% CI 0.36–0.87). Non-Hispanic Asians/Pacific Islanders in the South experienced significantly higher incidence than their counterparts in the Northeast (RR 0.87; 99% CI 0.77–0.98). In contrast, the incidence for non-Hispanic American Indians/Alaska Natives was higher in other regions than the Northeast (Midwest: RR 1.40; 99% CI 0.87–2.36, South: RR 1.50; 99% CI 0.95–2.49, and West: RR 1.63; 99% CI 1.05–2.68).
Table 1.
Age-standardized Incidence* of Cancer among Persons Aged <20 Years, by United States (US) Total, US Census Regions, Northeast States, Overall** and by Race/Ethnicity, 2003–2014
| Overall | Non-Hispanic White | Non-Hispanic Black | Hispanic All Races | Non-Hispanic American Indian/Alaska Native | Non-Hispanic Asian/Pacific Islander | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | |
|
| ||||||||||||
| All States | 174.4# (173.6, 175.3) | 170,039 | 185.8# (184.7, 186.9) |
102,838 | 134.3# (132.4, 136.1) | 20,119 | 169.2 (167.5, 171.0) |
35,989 | 149.6 (142.1, 157.4) |
1,510 | 147.7 (144.3, 151.2) |
7,189 |
|
| ||||||||||||
| Northeast (Reference) | 188.8 (186.7, 190.9) |
32,016 | 201.8 (199.1, 204.5) |
21,696 | 144.8 (139.9, 149.7) |
3,428 | 169.8 (165, 174.7) |
4,744 | 98.9 (74.6, 128.5) |
56 | 154.7 (146.9, 162.7) |
1,509 |
|
| ||||||||||||
| Connecticut | 185.9 (177.9, 194.1) |
2,060 | 194.7 (184.6, 205.3) |
1,398 | 146.3 (126.7, 168) |
201 | 177.6 (159.7, 196.9) |
362 |
^ (^, ^) |
^ | 131.8 (100.9, 169.1) |
62 |
| Maine | 190.8 (177.1, 205.2) |
726 | 194.6 (180.3, 209.9) |
685 |
∼ (∼, ∼) |
9 |
^ (^, ^) |
^ |
∼ (∼ , ∼ |
9 | 213.9 (109.3, 377.8) |
12 |
| Massachusetts | 181.2 (175.3, 187.2) |
3,579 | 194.9 (187.6, 202.5) |
2,721 | 124.8 (108.6, 142.8) |
214 | 148.3 (134.3, 163.3) |
413 |
^ (^, ^) |
^ | 141.8 (121.2, 165) |
169 |
| New Hampshire | 204.0 (190.1, 218.6) |
812 | 205.9 (191.3, 221.4) |
742 | 119.9 (57.3, 221.5) |
10 | 177.9 (120.6, 252.7) |
31 |
^ (^, ^) |
^ | 155.2 (91.6, 246.7) |
18 |
| New Jersey | 193.1 (187.9, 198.3) |
5,322 | 212.8 (205.5, 220.3) |
3,183 | 149.1 (137.7, 161.2) |
635 | 177 (166.4, 188) |
1,050 |
^ (^>, ^) |
^ | 148.5 (133.3, 165.1) |
349 |
| New York | 191.2 (187.7, 194.8) |
11,441 | 210.4 (205.4, 215.5) |
6,714 | 148.5 (141.2, 156.1) |
1,543 | 178.4 (171.2, 185.8) |
2,319 | 87.5 (55.4, 131.6) |
23 | 168.6 (156.5, 181.5) |
714 |
| Pennsylvania | 187.8 (183.5, 192.2) |
7,215 | 194.6 (189.5, 199.8) |
5,521 | 143.9 (134, 154.3) |
786 | 154.1 (140.9, 168.2) |
505 |
∼ (∼, ∼ |
9 | 141.6 (121.1, 164.7) |
170 |
| Rhode Island | 171.2 (157.1, 186.2) |
551 | 197.6 (179.1, 217.4) |
432 | 102.2 (67.3, 148.7) |
27 | 98.3# (75, 126.6) |
60 |
^ (^, ^) |
^ | 112.8 (58.1, 196.6) |
12 |
| Vermont | 165.1 (147.1, 184.8) |
310 | 171.4 (152.3, 192.2) |
300 |
^ (^, ^) |
^ |
^ (^, ^) |
^ |
^ (^, ^) |
^ |
^ (^, ^) |
^ |
|
| ||||||||||||
| Midwest | 172.6# (170.9, 174.4) | 35,995 | 180.5# (178.4, 182.7) |
27,172 | 129.5# (125.4, 133.7) | 3,794 | 158.8 (153.4, 164.4) |
3,242 | 138.4 (121.8, 156.5) |
253 | 145.3 (136, 155) |
918 |
|
| ||||||||||||
| South | 169.4# (168.1, 170.7) | 62,085 | 181.3# (179.4, 183.2) |
34,970 | 133.1# (130.6, 135.5) | 11,188 | 175.2 (172.2, 178.2) |
13,221 | 148.3 (135, 162.4) |
463 | 134.6# (127.8, 141.6) |
1,470 |
|
| ||||||||||||
| West | 173.4# (171.7, 175.1) | 39,943 | 185.2# (182.6, 187.9) |
19,000 | 133.7 (127.4, 140.2) |
1,709 | 166.3 (163.6, 169) |
14,782 | 161.2# (149.7, 173.2) |
738 | 151.8 (146.7, 157.1) |
3,292 |
Rates are per 1,000,000 and age-adjusted to the 2000 US Std Population (19 age groups - Census P25–1130) standard; Confidence intervals (Tiwari, R.C. [2006] method) are 95% for rates.
Overall case counts include 2,394 (1.4%) unknown race/ethnicity (non-Hispanic unknown: N=2,354; unknown all races: N=40).
Age standardized rate not calculated for counts < 10. Counts < 10 are italicized (Morris, J.K. [2018]).
Statistics not displayed due to fewer than 6 cases to preserve confidentiality.
The age-standardized rate is significantly different to the rate for Northeast after adjusting for multiple testing, (p<0.001, overall significance level).
Figure 2.
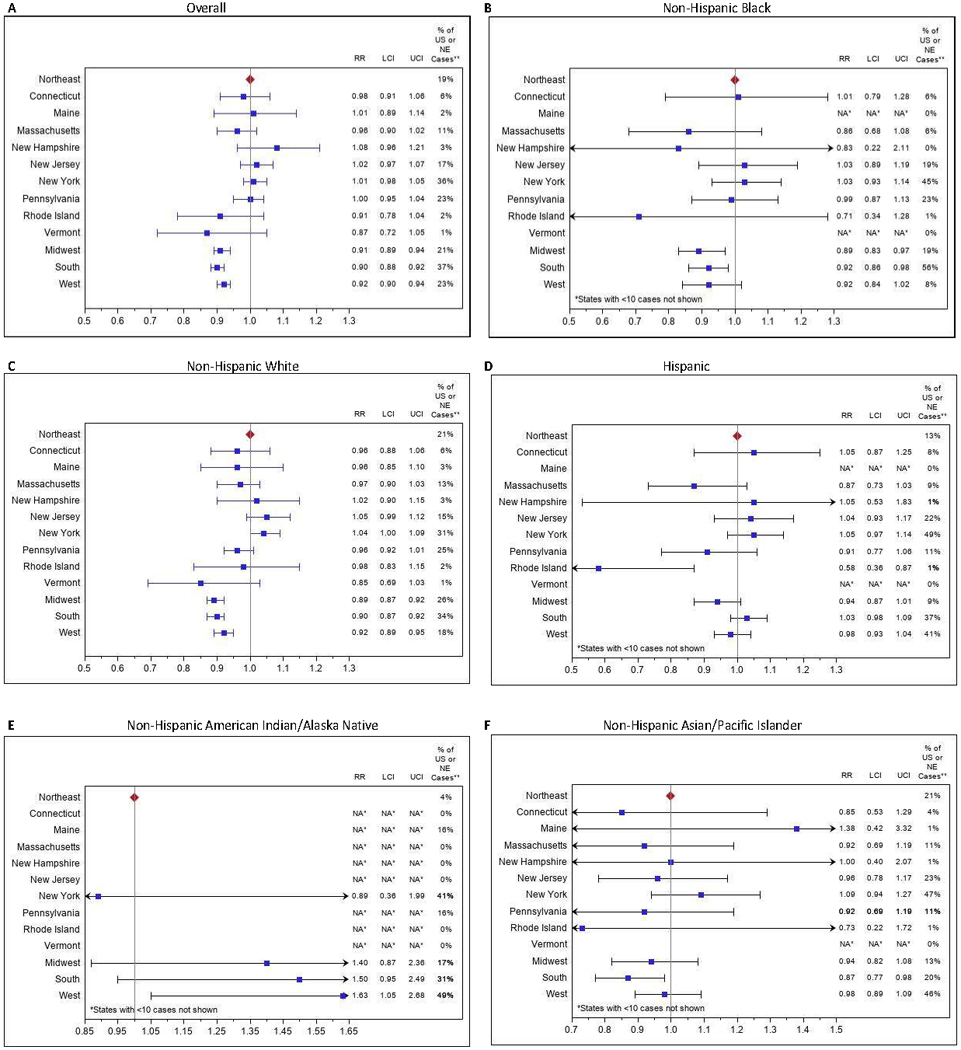
Rate Ratios (RR) and 99% confidence intervals (CI) Ɨ of age-standardized childhood cancer incidence rates for states and regions compared with Northeast (NE) among all races - overall§ (A); RR and 99% CIs for states and regions compared with NE among Non-Hispanic Black pediatric cancer cases (B); RR and 99% CIs for states and regions compared with NE among Non-Hispanic White pediatric cancer cases (C); RR and 99% CIs for states and regions compared with NE among Hispanic pediatric cases (D); RR and 99% CIs for states and regions compared with NEs among Non-Hispanic American Indian/Alaska Native (E); RR and 99% CIs for states and regions compared with NE among Non-Hispanic Asian/Pacific Islander pediatric cases (F).
Abbreviations: RR: rate ratio; LCI: lower confidence interval; UCI: upper confidence interval; US: United States; ME: Northeast.
†Bonferroni correction method used to allow for multiple comparisons. Confidence intervals are set at 99% to preserve the 95% confidence level overall
*Age standardized rate not calculated for counts < 10. Counts < 10 are italicized.
§Overall case counts include 2,394 (1.4%) unknown race/ethnicity (Non-Hispanic unknown: N = 2,354; unknown all races: N = 40).
** % of US cases defined as (number of US region cases/number of US total cases)% and ME cases as (number of ME state cases/number of ME total cases)%.
Note: The scale minimum-maximum for Figures e) Non-Hispanic American Indian/Alaska Native, f) Non-Hispanic Asian/Pacific Islander has been made different to the other graphs to accommodate the point estimates while retaining the same range. Hence the width of the confidence intervals is comparable to the other figures.
Incidence in the United States overall was highest for leukemias (45.9 per million), followed by central nervous system (CNS) (31.2) and lymphomas (26.4) (Table 2, Supplementary Tables 2a-f). Incidence rates in non-Hispanic White children in the Northeast were significantly higher than the US for leukemias (RR 1.07; 99% CI 1.03–1.12), lymphomas (RR 1.12; 99% CI 1.07–1.18), CNS neoplasms (RR 1.10; 99% CI 1.05–1.15), neuroblastoma (RR 1.11; 99% CI 1.01–1.20), and other malignancies (Figure 3). Within these categories, significantly elevated rates in the Northeast compared with the US were seen for lymphoid leukemias (RR 1.09; 99% CI 1.04–1.14), Hodgkin (RR 1.16; 99% CI 1.09–1.24) and non-Hodgkin (RR 1.14; 99% CI 1.05–1.25) lymphomas; astrocytomas (RR 1.12; 99% CI 1.05–1.19); other gliomas (1.19; 99% CI 1.07–1.32) (Supplementary Table 2b). In the United States and in the Northeast, there was a more than three-fold higher annual incidence of thyroid cancers among non-Hispanic Whites than non-Hispanic Blacks; among non-Hispanic Whites, thyroid cancer incidence in the Northeast was significantly higher than the US (RR 1.33; 99% CI 1.23–1.44) (Supplementary Table 2c).
Table 2.
Comparison of Age-standardized Incidence*,¶ of Cancer, among Persons Aged <20 years, for Northeast Region§ with the United States by Race/Ethnicity, 2003–2014
| Overall | Non-Hispanic White | Non-Hispanic Black | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Cancer Type | All States (Population: 968,956,124; Reference) | Northeast (Population: 168,302,782) | All States (Population: 550,723,012; Reference) | Northeast (Population: 106,960,493) | All States (Population: 149,189,102; Reference) | Northeast (Population: 23,512,857) | ||||||
|
| ||||||||||||
| ICCC site recode ICD-O-3/WHO 2008 | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count |
|
| ||||||||||||
| I Leukemias, myeloproliferative & myelodysplastic diseases | 45.9 (45.5, 46.4) |
44,480 | 47.2 (46.1, 48.2) |
7,830 | 45.6 (45.1, 46.2) |
24,755 | 49.0# (47.6, 50.4) |
5,078 | 29.7 (28.8, 30.5) |
4,407 | 32.0 (29.7, 34.4) |
747 |
| II Lymphomas and reticuloendothelial neoplasms | 26.4 (26.0, 26.7) |
25,856 | 30.2# (29.4, 31.0) |
5,256 | 28.1 (27.7, 28.6) |
15,969 | 31.6# (30.5, 32.6) |
3,555 | 22.6 (21.8, 23.3) |
3,440 | 26.0# (24.0, 28.1) |
634 |
| III CNS and misc. intracranial and intraspinal neoplasms | 31.2 (30.9, 31.6) |
30,150 | 34.8# (33.9, 35.7) |
5,800 | 35.5 (35.0, 36.0) |
19,334 | 38.9# (37.8, 40.2) |
4,093 | 24.8 (24.0, 25.6) |
3,663 | 26.4 (24.4, 28.6) |
614 |
| IV Neuroblastoma and other peripheral nervous cell tumors | 8.5 (8.3, 8.7) |
8,217 | 9.6# (9.1, 10.1) |
1,552 | 10.1 (9.8, 10.4) |
5,330 | 11.1# (10.5, 11.8) |
1,094 | 7.3 (6.9, 7.8) |
1,078 | 7.8 (6.7, 9.0) |
176 |
| V Retinoblastoma | 3.2 (3.1, 3.3) |
3,104 | 3.3 (3.0, 3.6) |
533 | 2.9 (2.7, 3.0) |
1,500 | 3.0 (2.7, 3.4) |
293 | 3.5 (3.2, 3.8) |
514 | 3.8 (3.0, 4.6) |
85 |
| VI Renal tumors | 6.9 (6.7, 7.0) |
6,633 | 7.1 (6.7, 7.5) |
1,151 | 7.2 (7.0, 7.4) |
3,843 | 7.2 (6.6, 7.7) |
717 | 8.6 (8.1, 9.1) |
1,258 | 8.3 (7.2, 9.6) |
189 |
| VII Hepatic tumors | 2.3 (2.2, 2.4) |
2,279 | 2.5 (2.3, 2.8) |
419 | 2.3 (2.2, 2.4) |
1,226 | 2.4 (2.1, 2.7) |
240 | 1.7 (1.5, 2.0) |
257 | 2.0 (1.5, 2.7) |
47 |
| VIII Malignant bone tumors | 8.6 (8.4, 8.7) |
8,358 | 9.1 (8.7, 9.6) |
1,575 | 9.0 (8.8, 9.3) |
5,096 | 9.5 (9.0, 10.1) |
1,065 | 7.1 (6.6, 7.5) |
1,072 | 7.5 (6.5, 8.7) |
182 |
| IX Soft tissue and other extraosseous sarcomas | 11.7 (11.5, 11.9) |
11,422 | 12.5# (11.9, 13.0) |
2,118 | 11.8 (11.5, 12.1) |
6,565 | 12.7 (12.0, 13.4) |
1,371 | 12.6 (12.0, 13.2) |
1,896 | 13.7 (12.3, 15.3) |
327 |
| X Germ cell & trophoblastic tumors & neoplasms of gonads | 11.0 (10.8, 11.2) |
10,886 | 10.8 (10.4, 11.3) |
1,912 | 10.9 (10.7, 11.2) |
6,276 | 11. (10.9, 12.2) |
1,316 | 6.2 (5.8, 6.6) |
942 | 5.9 (5.0, 6.9) |
145 |
| XI Other malignant epithelial neoplasms and melanomas | 17.8 (17.6, 18.1) |
17,709 | 20.9# (20.3, 21.6) |
3,738 | 21.4 (21.0, 21.8) |
12,403 | 24.1# (23.2, 25.0) |
2,798 | 9.4 (8.9, 9.9) |
1,448 | 10.5 (9.3, 11.9) |
262 |
| XII Other and unspecified malignant neoplasms | 0.7 (0.7, 0.8) |
706 | 0.6 (0.5, 0.8) |
107 | 0.7 (0.6, 0.8) |
399 | 0.6 (0.4, 0.7) |
62 | 0.8 (0.6, 0.9) |
114 |
∼ (∼, ∼) |
∼ |
| Not classified by ICCC or in situ+ | 0.2 (0.2, 0.3) |
239 | 0.1 (0.1, 0.2) |
25 | 0.3 (0.2, 0.3) |
142 | 0.1# (0.1, 0.2) |
14 | 0.2 (0.1, 0.3) |
30 |
∼ (∼, ∼) |
^ |
|
| ||||||||||||
| Hispanic | Non-Hispanic American Indian/Alaska Native | Non-Hispanic Asian/Pacific Islander | ||||||||||
|
| ||||||||||||
| Cancer Type | All States (Population: 210,772,149; Reference) | Northeast (Population: 27,626,954) | All States (Population: 10,021,360; Reference) | Northeast (Population: 56,162) | All States (Population: 48,250,501; Reference) | Northeast (Population: 9,640,856) | ||||||
|
| ||||||||||||
| ICCC site recode ICD-O-3/WHO 2008 | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count |
|
| ||||||||||||
| I Leukemias, myeloproliferative & myelodysplastic diseases | 56.2 (55.2, 57.2) |
12,151 | 50.5# (47.9, 53.2) |
1,421 | 43.8 (39.8, 48.1) |
436 | 25.3 (13.8, 42.4) |
14 | 45.6 (43.7, 47.5) |
2,225 | 47.9 (43.7, 52.5) |
469 |
| II Lymphomas and reticuloendothelial neoplasms | 23.6 (22.9, 24.2) |
4,864 | 28.0# (26.1, 30.1) |
766 | 18.2 (15.6, 21.0) |
185 |
∼ (∼, ∼) |
8 | 22.0 (20.6, 23.3) |
1,060 | 22.7 (19.8, 25.9) |
218 |
| III CNS and misc. intracranial and intraspinal neoplasms | 24.9 (24.3, 25.6) |
5,364 | 26.5 (24.6, 28.5) |
738 | 26.4 (23.3, 29.8) |
263 | 17.7 (8.5, 32.7) |
10 | 22.2 (20.9, 23.5) |
1,073 | 23.0 (20.0, 26.2) |
223 |
| IV Neuroblastoma and other peripheral nervous cell tumors | 5.5 (5.2, 5.8) |
1,290 | 6.0 (5.2, 7.0) |
181 | 6.0 (4.6, 7.8) |
60 |
∼ (∼, ∼) |
^ | 6.8 (6.1, 7.6) |
341 | 6.9 (5.4, 8.7) |
72 |
| V Retinoblastoma | 3.5 (3.3, 3.8) |
839 | 3.3 (2.7, 4.0) |
102 | 2.8 (1.9, 4.1) |
28 |
∼ (∼, ∼) |
^ | 3.4 (2.9, 3.9) |
169 | 3.8 (2.7, 5.2) |
40 |
| VI Renal tumors | 5.3 (5.0, 5.6) |
1,199 | 6.1 (5.3, 7.1) |
180 | 6.5 (5.0, 8.3) |
64 |
∼ (∼, ∼) |
^ | 3.5 (3.0, 4.1) |
175 | 3.6 (2.5, 4.9) |
36 |
| VII Hepatic tumors | 2.6 (2.4, 2.8) |
594 | 2.8 (2.3, 3.5) |
84 | 3.1 (2.1, 4.4) |
31 |
∼ (∼, ∼) |
^ | 2.9 (2.4, 3.4) |
143 | 3.7 (2.6, 5.1) |
38 |
| VIII Malignant bone tumors | 8.4 (8.0, 8.8) |
1,691 | 8.8 (7.7, 10.0) |
236 | 7.1 (5.5, 8.9) |
72 |
∼ (∼, ∼) |
^ | 7.2 (6.5, 8.0) |
345 | 7.7 (6.0, 9.7) |
72 |
| IX Soft tissue and other extraosseous sarcomas | 10.8 (10.4, 11.3) |
2,273 | 11.0 (9.8, 12.3) |
305 | 11.0 (9.1, 13.3) |
112 |
∼ (∼, ∼) |
^ | 8.4 (7.6, 9.3) |
409 | 8.0 (6.3, 10.0) |
78 |
| X Germ cell & trophoblastic tumors & neoplasms of gonads | 14.2 (13.7, 14.7) |
2,875 | 11.1# (9.9, 12.4) |
306 | 9.5 (7.8, 11.6) |
100 |
∼ (∼, ∼) |
^ | 11.7 (10.7, 12.7) |
566 | 11.3 (9.3, 13.6) |
110 |
| XI Other malignant epithelial neoplasms and melanomas | 13.3 (12.8, 13.8) |
2,659 | 14.9 (13.5, 16.5) |
406 | 13.8 (11.7, 16.3) |
145 |
∼ (∼, ∼) |
^ | 13.4 (12.4, 14.5) |
649 | 15.0 (12.6, 17.7) |
143 |
| XII Other and unspecified malignant neoplasms | 0.7 (0.6, 0.8) |
141 | 0.5 (0.3, 0.8) |
14 |
∼ (∼, ∼) |
8 |
∼ (∼, ∼) |
^ | 0.5 (0.3, 0.8) |
25 |
∼ (∼, ∼) |
9 |
| Not classified by ICCC or in situ+ | 0.2 (0.2, 0.3) |
49 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
6 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
9 |
∼ (∼, ∼) |
^ |
Abbreviations: CI - Confidence Intervals.
Rates are per 1,000,000 and age-adjusted to the 2000 US Std Population (19 age groups - Census P25–1130) standard; Confidence intervals (Tiwari, R.C. [2006] method) are 95% for rates.
Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont.
Incidence data are compiled from cancer registries that meet the data quality criteria for all years 2003–2014 (covering >99% of the U.S. population). Nevada is excluded; Kansas not included and diagnosis year 2003 not included for Mississippi and Tennessee. Registry-specific data quality information is available from NAACCR.5
Age standardized rate not calculated for counts < 10. Counts < 10 are italicized.
Statistics not displayed due to fewer than 6 cases to preserve confidentiality.
The age-standardized rate is significantly different to the rate for Northeast after adjusting for multiple testing, (p<0.01, overall significance level).
+ Note that in this study, we excluded in situs but have retained the ICCC site recode nomenclature
Figure 3.
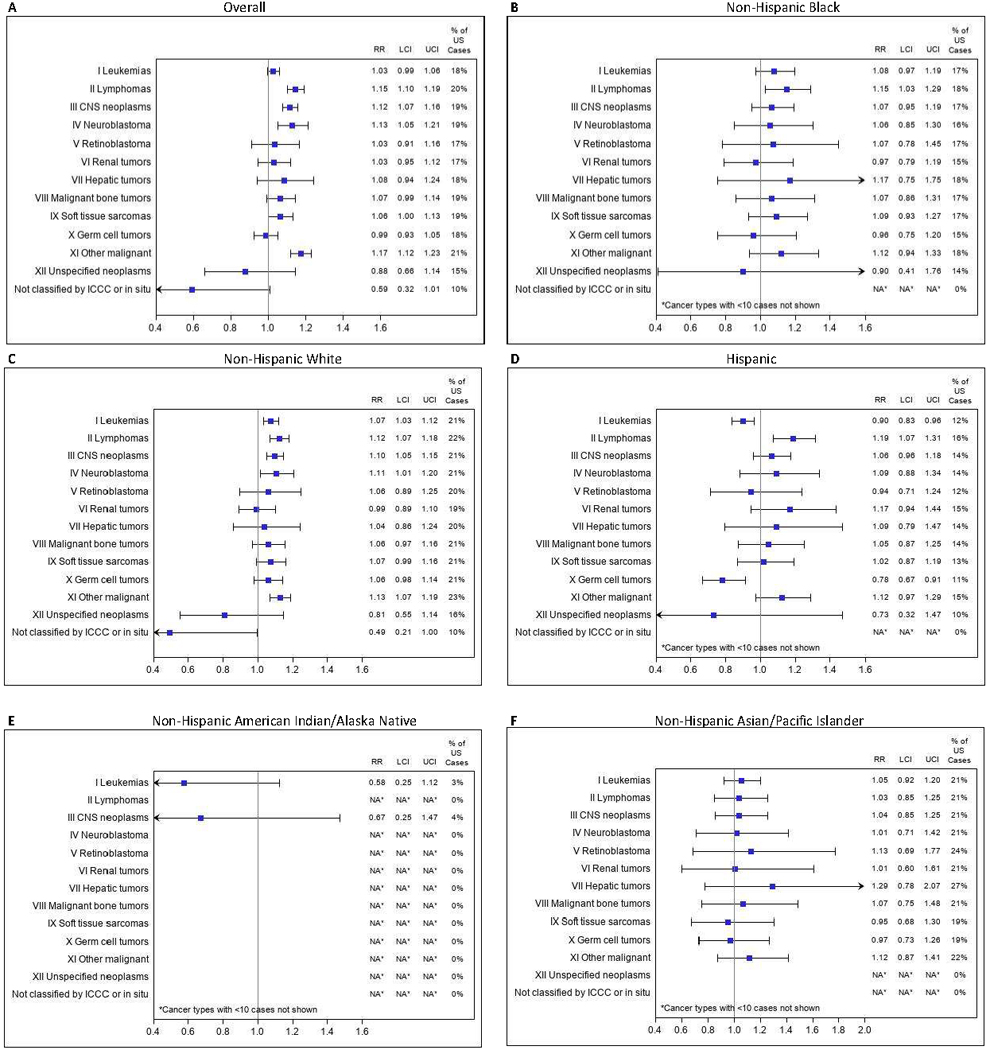
Pediatric cancer types Ɨ, * Rate Ratio (RR) and 99% confidence intervals (CI) β of age-standardized incidence rates for the Northeast (NE) compared with the United States (US) for all races - overall§ (A); RR and 99% CIs for NE pediatric cancer types compared with US among Non-Hispanic Black (B); RR and 99% CIs for NE pediatric cancer types compared with US among Non-Hispanic White (C); RR and 99% CIs for NE pediatric cancer types compared with US among Hispanic (D); RR and 99% CIs for NE pediatric cancer types compared with US among Non-Hispanic American Indian/Alaska Native (E); RR and 99% CIs for NE pediatric cancer types compared with US among Non-Hispanic Asian/Pacific Islander (F).
†Complete Cancer Types Titles: I Leukemias, myeloproliferative & myelodysplastic diseases; II Lymphomas and reticuloendothelial neoplasms; III CNS and misc intracranial and intraspinal neoplasms; IV Neuroblastoma and other peripheral nervous cell tumors; V Retinoblastoma; VI Renal tumors; VII Hepatic tumors; VIII Malignant bone tumors; IX Soft tissue and other extraosseous sarcomas; X Germ cell & trophoblastic tumors & neoplasms of gonads; XI Other malignant epithelial neoplasms and melanomas; XII Other and unspecified malignant neoplasms; Not classified by ICCC or in situ (Note that in this study, we excluded in situs but have retained the ICCC site recode nomenclature)
*Age standardized rate not calculated for counts < 10. Counts < 10 are italicized (Morris, J.K. [2018]).
βBonferroni correction method used to allow for multiple comparisons. Confidence intervals are set at 99% to preserve the 95% confidence level overall
§Overall case counts include 2,394 (1.4%) unknown race/ethnicity (Non-Hispanic unknown: N=2,354; unknown all races: N = 40).
Abbreviations: LCI: lower confidence interval; UCI: upper confidence interval; US: United States;
Note: The scale maximum for Figure f) Non-Hispanic Asian/Pacific Islander has been made different to the other graphs to accommodate the point estimates for XII Unspecified neoplasms.
The pattern for non-Hispanic Black children resembled that for Whites but with less precision in the estimates due to smaller numbers. However, Hispanic children in the Northeast had a different pattern than their counterparts in the US as a whole, with significantly lower incidence of leukemias (RR 0.90; 99% CI 0.83–0.96) (Figure 3), specifically lymphoid leukemias (RR 0.84; 99% CI 0.77–0.91) (Supplementary Table 2d) and germ cell tumors (RR 0.78; 99% CI 0.67–0.91) (Figure 3), specifically malignant gonadal germ cell tumors (RR 0.69; 99% CI 0.56–0.83) (Supplementary Table 2d). Hispanics had significantly higher incidence of lymphomas (RR 1.19; 99% CI 1.07–1.31) (Figure 3) as well as the renal tumor subcategory, renal carcinoma (RR 2.04; 99% CI 1.04–3.72) (Supplementary Table 2d). Asian/Pacific Islanders in the Northeast had incidence rates of the cancer subtypes that were comparable with the US as a whole (Figure 3 and Supplementary Table 2f).
The incidence of non-malignant brain tumors was significantly higher in the Northeast than the country overall, and for non-Hispanic Whites and for Hispanics; rates for non-Hispanic Blacks and non-Hispanic Asian/Pacific Islanders were higher in the Northeast but not significantly different than the US. Incidence by state within the Northeast varied widely from 17.4 to 33.0 per million per year (Table 3).
Table 3.
Age-standardized Incidence * of Non-Malignant Brain Tumors among Persons Aged <20 Years, by United States (US), US Census Regions, Northeast States, Overall and by Race/Ethnicity, 2004§−2014
| Overall | Non-Hispanic White | Non-Hispanic Black | Hispanic All Races | Non-Hispanic American Indian/Alaska Native | Non-Hispanic Asian/Pacific Islander | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | Rate (95% CI) | Count | |
|
| ||||||||||||
| All States | 23.8# (23.5, 24.1) |
21,419 | 25.3# (24.8, 25.7) |
12,970 | 19.4 (18.7, 20.2) |
2,711 | 22.3# (21.7, 23.0) |
4,284 | 25.4 (22.3, 28.8) |
239 | 16.3 (15.2, 17.5) |
732 |
|
| ||||||||||||
| Northeast (Reference) | 26.9 (26.1, 27.8) |
4,240 | 27.3 (26.3, 28.3) |
2,741 | 21.4 (19.5, 23.4) |
468 | 28.2 (26.2, 30.4) |
717 |
∼ (∼, ∼) |
8 | 20.1 (17.2, 23.2) |
178 |
|
| ||||||||||||
| Connecticut | 22.1# (19.3, 25.1) |
228 | 23.1 (19.6, 27.0) |
156 | 11.6 (6.5, 19.2) |
15 | 22.4 (16.1, 30.3) |
42 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
∼ |
| Maine | 17.1# (13.1, 22.1) |
61 | 17.4# (13.1, 22.6) |
57 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
| Massachusetts | 21.1# (19.0, 23.3) |
389 | 23.5 (21.0, 26.3) |
309 | 18.4 (12.3, 26.5) |
29 | 11.0# (7.3, 15.9) |
28 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
∼ |
| New Hampshire | 27.1 (22.1, 32.9) |
104 | 26.4 (21.3, 32.5) |
92 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
| New Jersey | 26.9 (24.9, 29.0) |
682 | 27.0 (24.4, 29.9) |
374 | 21.1 (16.8, 26.2) |
83 | 30.6 (26.1, 35.6) |
165 |
∼ (∼, ∼) |
^ | 19.3 (13.8, 26.3) |
40 |
| New York | 32.4# (30.9, 34.0) |
1,786 | 33.0# (31.0, 35.2) |
973 | 25.5 (22.4, 28.9) |
244 | 35.3# (32.0, 38.8) |
416 |
∼ (∼, ∼) |
^ | 24.9 (20.2, 30.4) |
97 |
| Pennsylvania | 24.4# (22.8, 26.0) | 882 | 25.7 (23.8, 27.7) |
690 | 17.8 (14.3, 21.8) |
91 | 17.2# (12.8, 22.7) |
51 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
∼ |
| Rhode Island | 19.2 (14.5, 25.0) |
57 | 20.3 (14.5, 27.7) |
41 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
9 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
| Vermont | 28.2 (21.0, 37.3) |
51 | 28.9 (21.3, 38.4) |
49 |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
∼ (∼, ∼) |
^ |
|
| ||||||||||||
| Midwest | 22.8# (22.1, 23.5) |
4,377 | 23.9# (23.1, 24.7) |
3,325 | 18.3 (16.8, 20.0) |
496 | 19.2# (17.2, 21.4) |
347 | 17.9 (12.0, 25.5) |
30 | 14.5 (11.6, 18.0) |
84 |
|
| ||||||||||||
| South | 23.1# (22.6, 23.7) |
7,844 | 24.7# (23.9, 25.4) |
4,427 | 19.0 (18.0, 20.0) |
1,492 | 23.1# (22.0, 24.3) |
1,565 | 19.0 (14.3, 24.6) |
56 | 15.5 (13.1, 18.1) |
156 |
|
| ||||||||||||
| West | 23.7# (23.1, 24.4) |
5,155 | 26.6 (25.6, 27.6) |
2,626 | 21.7 (19.1, 24.5) |
265 | 20.7# (19.7, 21.7) |
1,683 | 34.2 (28.9, 40.2) |
148 | 15.6# (13.9, 17.4) |
316 |
Abbreviations: CI - Confidence Intervals.
Rates are per 1,000,000 and age-adjusted to the 2000 US Std Population (19 age groups - Census P25–1130) standard; Confidence intervals (Tiwari, R.C. [2006] method) are 95% for rates.
Nationally, identification of benign brain tumors began in United States cancer registries on 1/1/2004 mandated by Public Law 107, 260, the Benign Brain Tumor Cancer Registries Amendment Act (https://training.seer.cancer.gov/brain/non-malignant/).
Age standardized rate not calculated for counts < 10. Counts < 10 are italicized.
Statistics not displayed due to fewer than 6 cases to preserve confidentiality.
The age-standardized rate is significantly different to the rate for Northeast after adjusting for multiple testing, (p<0.01, overall significance level).
Discussion
Pediatric cancer incidence is significantly higher in the Northeast than other regions of the United States with incidence of 188.8 per million per year compared to 174.4 overall. However, there was no significant variability in incidence in the states within the Northeast region – i.e., none of the Northeastern states was identified as an outlier within the region. For example, the incidence in New Hampshire, cited previously as the state with the highest rate, is not statistically distinguishable from other states within the Northeast both overall and when stratified by race. The populations of the Northeast show substantial variation in race/ethnicity distribution: minorities comprise fewer than 10% of the populations of the three most northern states (Maine, New Hampshire, and Vermont) but nearly half of the populations of New York and New Jersey. Because the age-standardized incidence rates vary by more than 38% across racial groups, with lowest rates in non-Hispanic Black children (144.8 per million per year) and highest in non-Hispanic Whites (201.8 per million per year), consideration of race in any regional comparisons is critical. The patterns we see indicate that there are differences in cancer types by race/ethnicity and region. In particular, the higher incidence of certain cancer types in the Northeast than the US were not mirrored in the Hispanic population, and Hispanic children in the Northeast have lower incidence of acute lymphoblastic leukemia (ALL) and germ cell tumors than elsewhere in the country. It has been reported previously that ALL is more common in Hispanics than non-Hispanics at most ages through the lifespan in the United States,15 although some studies in smaller populations within the US have found rates to be comparable,16,17 perhaps because the category “Hispanic” includes diverse ancestries and therefore diverse genetic and environmental risk factors. In our data, it is unclear why Hispanic children in Rhode Island have lower cancer incidence than their counterparts in the Northeast, and further study of the geographic differences in pediatric cancer incidence by ethnicity may provide clues to etiology and establish whether this is a real or chance observation.15,18 We could not study the incidence in children of mixed race because cancer registries do not capture these data, but a birth certificate-cancer registry linkage study in five states reported that patterns of risk tend to mirror those of the minority parent’s group.16
In addition to invasive cancers, non-malignant brain tumors also occur more commonly in the Northeast, but there is wide variation by state, as previously reported.19 Reporting of non-malignant brain tumors to cancer registries began in 2004, and these tumors make up 70% of all brain and CNS tumors.20 It has been shown that case ascertainment for non-malignant brain tumors varies substantially between states and there is wide variation by state in the proportions of these cases that are microscopically confirmed; these proportions are strongly correlated with reported incidence by state, suggesting that flawed case ascertainment may account for these differences.19
What might underlie the high incidence of pediatric cancer in the Northeast, even after stratifying by race? We know that the incidence of adult cancer is also higher in the Northeast21 and the reasons for that are also unclear but – as for childhood cancer – likely to be multifactorial. Few strong risk factors for pediatric cancer have been identified. Increasing maternal age at delivery is associated with a higher risk of pediatric cancer in the offspring;22–24 it has been linked to the rising pediatric cancer incidence over time,25 and average maternal age at delivery is higher in the Northeast.26 Higher socioeconomic status (SES) is another risk factor for pediatric cancer1,27,28 that is more prevalent in the Northeast;29,30 high SES may be a proxy for maternal age and for access to medical care, including testing such as imaging. Increased use of medical imaging may lead to geographic differences in thyroid cancer incidence via enhanced detection of low risk lesions, often as incidental findings;31–34 use of pediatric CT scans is higher with white race, increasing household income, and private health insurance.35–39 However, relative to other regions, there is evidence of less frequent use of CT scans in children in the Northeast,40,41 even though others cite more frequent use in the Northeast for some adult indications.42,43 Several studies report excess cancer risk as a result of ionizing radiation exposure during childhood CT scans.32–34,44 In a large retrospective cohort study, CT scans conducted before age 20 were associated with a 24% excess cancer risk during an average of 9.5 years of follow-up,33 and it has been estimated that the four million pediatric CT scans performed annually in the US will cause more than 4,000 future cancers during the lifespan.44 A host of other possible explanations with varying degrees of evidence have been summarized by Lupo and Spector, including use of chemicals including pesticides and herbicides, pollution, parental smoking and use of recreational drugs and alcohol, maternal obesity and diabetes, preterm birth and birth weight, and possible preventive factors include breast feeding and use of prenatal vitamins.45 High prevalence risk factors for adult cancers in northeastern states include arsenic in drinking water;46 radon;47 and woodsmoke due to use of wood-based fuels in the home,48 but the evidence supporting causal associations between these factors and pediatric cancer is weak.49–52 Although the Northeast tends to rank well on various EPA pollution metrics,53 the number of EPA National Priorities List (NPL) sites per capita is higher in some areas of the Northeast compared to other regions,54 and examples of pollution in specific areas have raised concerns about possible cancer risks, although epidemiologic studies often have difficulty identifying specific causal associations.55–59 However, individual level data in a large population-based sample would be needed to elucidate the causes of excess pediatric cancer risk in the Northeast, to identify modifiable risk factors and exposure reduction strategies that could be targeted by public health and environmental health interventions.
Strengths of the study include the use of national, population-based cancer registry surveillance data that has undergone annual scrutiny for quality,5,60 the inclusion of all Northeastern states and their race/ethnicity data, and the use of rigorous statistical methods to compare the Northeast with its constituent states and with other regions or the country as a whole within race-specific strata. Restriction to first primary cancers avoids the potential problem that a first childhood cancer increases the risk of subsequent cancers, which in turn would tend to exaggerate any differences between states or regions with lower and higher incidence of first primaries. Limitations include the exclusion of data from Kansas, Nevada and from 2003 for Mississippi and Tennessee; uncertainty relating to data quality for non-malignant brain tumor reporting; and lack of information about mixed race/ethnicity.
In conclusion, the incidence of pediatric cancer in the Northeast is higher than the rest of the United States overall, and when race is taken into account. There is no evidence of any general trends towards higher rates in any states within the Northeast. Regional differences in incidence merit further exploration to identify potentially modifiable risk factors.
Supplementary Material
Acknowledgements
These analyses used NAACCR’s Cancer in North America data referenced below.4 Support for cancer registries is provided by the state, province, or territory in which the registry is located. In the US, registries also participate in the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program or the Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries (NPCR) or both. In Canada, all registries submit data to the Canadian Cancer Registry maintained by Statistics Canada. We thank the New Hampshire Drinking Water and Ground Water Trust Fund for funding this study. The New Hampshire State Cancer Registry is supported in part by the Centers for Disease Control and Preventions (CDC) National Program of Cancer Registries (NPCR) through cooperative agreement NU58DP006298 awarded to the New Hampshire Department of Health and Human Services, Division of Public Health Services, Bureau of Public Health Statistics & Informatics, Health Statistics and Data Management Section.
Financial Information:
This project was supported in part by the Centers for Disease Control and Preventions (CDC) National Program of Cancer Registries (NPCR) cooperative agreement NU58DP006298 awarded to the New Hampshire Department of Health and Human Services, Division of Public Health Services, Bureau of Disease Control and Health Statistics, Health Statistics and Data Management Section (A.B. Burke, PI). The New Hampshire State Registry is funded through a contract awarded to the Trustees of Dartmouth College (J.R. Rees, PI) and this project was funded by the New Hampshire Drinking Water and Ground Water Trust Fund through an amendment to the contract (J.R. Rees, PI).
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official positions of the New Hampshire Department of Environmental Services (DES), the New Hampshire Department of Health and Human Services (DHHS), or the Centers for Disease Control and Prevention (CDC).
Conflict of interest statement: The authors declare no potential conflicts of interest.
References
- 1.Siegel DA, Li J, Henley SJ, Wilson RJ, Lunsford NB, Tai E, et al. Geographic Variation in Pediatric Cancer Incidence - United States, 2003–2014. MMWR Morb Mortal Wkly Rep 2018;67:707–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pediatric Seacoast Cancer Cluster Investigation: A Summary of Investigation Findings as of April 30, 2017: State of New Hampshire, Department of Health and Human Services, Division of Public Health Services; 2017. [Google Scholar]
- 3.Investigation of Rhabdomyosarcoma (RMS) Cases in the Rye Area: New Hampshire Department of Health and Human Services, Division of Public Health Services; 2016. [Google Scholar]
- 4.SEER*Stat Database: NAACCR Incidence Data - CiNA Analytic File, 1995–2017, for NHIAv2 Origin, Standard File, Rees (20–07) - Revaluation of MMWR Geo Variation of Pediatric Cancer (which includes data from CDC’s National Program of Cancer Registries (NPCR), CCCR’s Provincial and Territorial Registries, and the NCI’s Surveillance, Epidemiology and End Results (SEER) Registries), certified by the North American Association of Central Cancer Registries (NAACCR) as meeting high-quality incidence data standards for the specified time periods, submitted December 2019. NAACCR; 2021. [Google Scholar]
- 5.Cancer in North America CiNA Data Products, 2018. at https://www.naaccr.org/cina-data-products-overview/.)
- 6.SEER*Stat Software, Version 8.3.9 - March 15, 2021. National Cancer Institute, 2021. at www.seer.cancer.gov/seerstat.) [Google Scholar]
- 7.CiNA Public Use Dataset. North American Association of Central Cancer Registries, 2021. at https://www.naaccr.org/cina-public-use-data-set/.)
- 8.NAACCR Guideline for Enhancing Hispanic-Latino Identification: Revised NAACCR Hispanic/Latino Identification Algorithm [NHIA v2.2.1]. Springfield, IL: North American Association of Central Cancer Registries; 2011. [Google Scholar]
- 9.Available Race Variables. National Cancer Institute, 2021. at https://seer.cancer.gov/seerstat/variables/seer/race_ethnicity/.)
- 10.Copeland G, Lake A, Firth R, Wohler B, Wu XC, Schymura M, Hofferkamp J, Sherman R, Kohler B (eds). Cancer in North America: 2009–2013. Volume One: Combined Cancer Incidence for the United States, Canada and North America. Springfield, IL: North American Association of Central Cancer Registries, Inc. June 2016. [Google Scholar]
- 11.Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. International Classification of Childhood Cancer, third edition. Cancer 2005;103:1457–67. [DOI] [PubMed] [Google Scholar]
- 12.International classification of diseases for oncology (ICD-O) – 3rd edition, 1st revision: World Health Organization; 2013. [Google Scholar]
- 13.Morris JK, Tan J, Fryers P, Bestwick J. Evaluation of stability of directly standardized rates for sparse data using simulation methods. Popul Health Metr 2018;16:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tiwari RC, Clegg LX, Zou Z. Efficient interval estimation for age-adjusted cancer rates. Stat Methods Med Res 2006;15:547–69. [DOI] [PubMed] [Google Scholar]
- 15.Yamamoto JF, Goodman MT. Patterns of leukemia incidence in the United States by subtype and demographic characteristics, 1997–2002. Cancer Causes Control 2008;19:379–90. [DOI] [PubMed] [Google Scholar]
- 16.Chow EJ, Puumala SE, Mueller BA, Carozza SE, Fox EE, Horel S, et al. Childhood cancer in relation to parental race and ethnicity: a 5-state pooled analysis. Cancer 2010;116:3045–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Duncan MH, Wiggins CL, Samet JM, Key CR. Childhood cancer epidemiology in New Mexico’s American Indians, Hispanic whites, and non-Hispanic whites, 1970–82. J Natl Cancer Inst 1986;76:1013–8. [PubMed] [Google Scholar]
- 18.Miller KD, Fidler-Benaoudia M, Keegan TH, Hipp HS, Jemal A, Siegel RL. Cancer statistics for adolescents and young adults, 2020. CA Cancer J Clin 2020;70:443–59. [DOI] [PubMed] [Google Scholar]
- 19.Li XR, Kruchko C, Wu XC, Hsieh MC, Andrews PA, Huang B, et al. Are Benign and Borderline Brain Tumors Underreported? J Registry Manag 2016;43:187–94. [PubMed] [Google Scholar]
- 20.Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro Oncol 2020;22:iv1–iv96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2020 submission data (1999–2018): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; June 2021. [Google Scholar]
- 22.Panagopoulou P, Skalkidou A, Marcotte E, Erdmann F, Ma X, Heck JE, et al. Parental age and the risk of childhood acute myeloid leukemia: results from the Childhood Leukemia International Consortium. Cancer Epidemiol 2019;59:158–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Petridou ET, Georgakis MK, Erdmann F, Ma X, Heck JE, Auvinen A, et al. Advanced parental age as risk factor for childhood acute lymphoblastic leukemia: results from studies of the Childhood Leukemia International Consortium. Eur J Epidemiol 2018;33:965–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Johnson KJ, Carozza SE, Chow EJ, Fox EE, Horel S, McLaughlin CC, et al. Parental age and risk of childhood cancer: a pooled analysis. Epidemiology 2009;20:475–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kehm RD, Osypuk TL, Poynter JN, Vock DM, Spector LG. Do pregnancy characteristics contribute to rising childhood cancer incidence rates in the United States? Pediatr Blood Cancer 2018;65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bui Q, Miller CC. The Age That Women Have Babies: How a Gap Divides America. New York Times; 2018. [Google Scholar]
- 27.Francis SS, Wang R, Enders C, Prado I, Wiemels JL, Ma X, et al. Socioeconomic status and childhood central nervous system tumors in California. Cancer Causes Control 2021;32:27–39. [DOI] [PubMed] [Google Scholar]
- 28.Gradel KO, Kaerlev L. Antibiotic use from conception to diagnosis of child leukaemia as compared to the background population: A nested case-control study. Pediatr Blood Cancer 2015;62:1155–61. [DOI] [PubMed] [Google Scholar]
- 29.Poverty in the United States: Percentage of people in poverty by state: 2015. United States Census Bureau, 2016. at https://www.census.gov/library/visualizations/2016/comm/cb16-158_poverty_map.html.) [Google Scholar]
- 30.Singh GK, Miller BA, Hankey BF, Feuer EJ, Pickle LW. Changing area socioeconomic patterns in U.S. cancer mortality, 1950–1998: Part I--All cancers among men. J Natl Cancer Inst 2002;94:904–15. [DOI] [PubMed] [Google Scholar]
- 31.Lim H, Devesa SS, Sosa JA, Check D, Kitahara CM. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017;317:1338–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Abalo KD, Rage E, Leuraud K, Richardson DB, Le Pointe HD, Laurier D et al. Early life ionizing radiation exposure and cancer risks: systematic review and meta-analysis. Pediatr Radiol 2021;51:45–56. [DOI] [PubMed] [Google Scholar]
- 33.Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB, et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 2013;346:f2360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 2012;380:499–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fahimi J, Herring A, Harries A, Gonzales R, Alter H. Computed tomography use among children presenting to emergency departments with abdominal pain. Pediatrics 2012;130:e1069–75. [DOI] [PubMed] [Google Scholar]
- 36.Mannix R, Bourgeois FT, Schutzman SA, Bernstein A, Lee LK. Neuroimaging for pediatric head trauma: do patient and hospital characteristics influence who gets imaged? Acad Emerg Med 2010;17:694–700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Marin JR, Rodean J, Hall M, Alpern ER, Aronson PL, Chaudhari PP, et al. Racial and Ethnic Differences in Emergency Department Diagnostic Imaging at US Children’s Hospitals, 2016–2019. JAMA Netw Open 2021;4:e2033710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Marin JR, Wang L, Winger DG, Mannix RC. Variation in Computed Tomography Imaging for Pediatric Injury-Related Emergency Visits. J Pediatr 2015;167:897–904 e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Natale JE, Joseph JG, Rogers AJ, Mahajan P, Cooper A, Wisner DH, et al. Cranial computed tomography use among children with minor blunt head trauma: association with race/ethnicity. Arch Pediatr Adolesc Med 2012;166:732–7. [DOI] [PubMed] [Google Scholar]
- 40.Lodwick DL, Cooper JN, Lawrence AE, Kelleher KJ, Minneci PC, Deans KJ. Factors Affecting Emergency Department Computed Tomography Use in Children. J Surg Res 2019;241:294–301. [DOI] [PubMed] [Google Scholar]
- 41.Tasian GE, Pulido JE, Keren R, Dick AW, Setodji CM, Hanley JM et al. Use of and regional variation in initial CT imaging for kidney stones. Pediatrics 2014;134:909–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Balthazar P, Sadigh G, Hughes D, Rosenkrantz AB, Hanna T, Duszak R Jr., Increasing Use, Geographic Variation, and Disparities in Emergency Department CT for Suspected Urolithiasis. J Am Coll Radiol 2019;16:1547–53. [DOI] [PubMed] [Google Scholar]
- 43.Welch HG, Skinner JS, Schroeck FR, Zhou W, Black WC. Regional Variation of Computed Tomographic Imaging in the United States and the Risk of Nephrectomy. JAMA Intern Med 2018;178:221–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Miglioretti DL, Johnson E, Williams A, Greenlee RT, Weinmann S, Solberg LI, et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr 2013;167:700–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lupo PJ, Spector LG. Cancer Progress and Priorities: Childhood Cancer. Cancer Epidemiol Biomarkers Prev 2020;29:1081–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ayotte JD, Montgomery DL, Flanagan SM, Robinson KW. Arsenic in groundwater in eastern New England: occurrence, controls, and human health implications. Environ Sci Technol 2003;37:2075–83. [DOI] [PubMed] [Google Scholar]
- 47.EPA Map of Radon Zones. at https://www.epa.gov/sites/production/files/2015-07/documents/zonemapcolor.pdf.)
- 48.Rokoff LB, Koutrakis P, Garshick E, Karagas MR, Oken E, Gold DR, et al. Wood Stove Pollution in the Developed World: A Case to Raise Awareness Among Pediatricians. Curr Probl Pediatr Adolesc Health Care 2017;47:123–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Greenop KR, Hinwood AL, Fritschi L, Scott RJ, Attia J, Ashton LJ, et al. Vehicle refuelling, use of domestic wood heaters and the risk of childhood brain tumours: Results from an Australian case-control study. Pediatr Blood Cancer 2015;62:229–34. [DOI] [PubMed] [Google Scholar]
- 50.Engel A, Lamm SH. Arsenic exposure and childhood cancer--a systematic review of the literature. J Environ Health 2008;71:12–6. [PubMed] [Google Scholar]
- 51.Moore LE, Lu M, Smith AH. Childhood cancer incidence and arsenic exposure in drinking water in Nevada. Arch Environ Health 2002;57:201–6. [DOI] [PubMed] [Google Scholar]
- 52.Lu Y, Liu L, Chen Q, Wei J, Cao G, Zhang J. Domestic radon exposure and risk of childhood leukemia: A meta-analysis. J BUON 2020;25:1035–41. [PubMed] [Google Scholar]
- 53.Toxics Release Inventory Analysis 2019: Environmental Protection Agency; 2021. [Google Scholar]
- 54.Superfund National Priorities List (NPL). EPA, 2021. at https://www.epa.gov/superfund/superfund-national-priorities-list-npl.) [Google Scholar]
- 55.Panikkar B, Lemmond B, Allen L, DiPirro C, Kasper S. Making the invisible visible: results of a community-led health survey following PFAS contamination of drinking water in Merrimack, New Hampshire. Environ Health 2019;18:79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Daly ER, Chan BP, Talbot EA, Nassif J, Bean C, Cavallo SJ, et al. Per- and polyfluoroalkyl substance (PFAS) exposure assessment in a community exposed to contaminated drinking water, New Hampshire, 2015. Int J Hyg Environ Health 2018;221:569–77. [DOI] [PubMed] [Google Scholar]
- 57.Durant JL, Chen J, Hemond HF, Thilly WG. Elevated incidence of childhood leukemia in Woburn, Massachusetts: NIEHS Superfund Basic Research Program searches for causes. Environ Health Perspect 1995;103 Suppl 6:93–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Costas K, Knorr RS, Condon SK. A case-control study of childhood leukemia in Woburn, Massachusetts: the relationship between leukemia incidence and exposure to public drinking water. Sci Total Environ 2002;300:23–35. [DOI] [PubMed] [Google Scholar]
- 59.Cutler JJ, Parker GS, Rosen S, Prenney B, Healey R, Caldwell GG. Childhood leukemia in Woburn, Massachusetts. Public Health Rep 1986;101:201–5. [PMC free article] [PubMed] [Google Scholar]
- 60.Data Quality Assessments and Evaluations. North American Association of Central Cancer Registries, 2021. at https://www.naaccr.org/data-quality-assessments-and-evaluations/.)
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data are available by application to the North American Association of Central Cancer Registries.4