

Abstract
Background
Typically, the celiac trunk and superior mesenteric artery branch off separately from the anterior aspect of the abdominal aorta. The celiacomesenteric trunk (CMT) is a rare variant in which those arteries share a common origin. We sought to compare the prevalence of CMT in the Caribbean with the global prevalence as calculated by a systematic review.
Methods
In this study, we evaluated all consecutive patients who had multiphase contrast-enhanced CT scans at two major referral centres in the Caribbean from August 30, 2017, to September 1, 2019. In patients with a CMT, we recorded demographic and anatomic details. We then conducted a systematic literature search and retrieved raw data to calculate the global prevalence (number of individuals with a CMT divided by the sum total of study samples). We compared CMT prevalence in our sample with the global prevalence using Pearson's chi-square and Fisher's exact tests. Statistical significance was considered to be present when the P value was <0.05.
Results
From 832 CTs, 665 scans met the inclusion criteria. There were 16 (2.41%) CMTs: 3 (0.45%) classic CMTs, 12 (1.8%) hepato-mesenteric trunks, and 1 (0.15%) hepato-spleno-mesenteric trunk. Forty-two studies reported on CMTs in a total of 74,320 persons. The global CMT prevalence was comparable (3.88%; P = 0.054), but the incidence of hepato-mesenteric variants was significantly lower in our sample (1.8% vs. 3.24%; P = 0.0352).
Conclusion
There was no difference in the prevalence of a classic CMT in the Caribbean compared to the global prevalence. However, the hepato-mesenteric trunk (incomplete CMT variant) was significantly less prevalent in the Caribbean. Advances in Knowledge: Healthcare professionals performing hepatobiliary interventions must be aware of these differences in order to minimize morbidity during their interventions.
1. Introduction
The celiac trunk (CT) and superior mesenteric artery (SMA) branch off separately from the anterior aspect of the abdominal aorta. The celiacomesenteric trunk (CMT) is a rare variant in which those arteries share a common origin from the abdominal aorta [1]. This variant is clinically important because it may impact invasive procedures on the upper abdominal viscera.
Considering the fact that several variations of arterial supply to the upper abdominal viscera have been reported in persons of Caribbean descent [2–5], we sought to document the prevalence of the CMT in the Caribbean study sample. A secondary aim of this study was to determine whether this was different from the global prevalence as calculated by a systematic review of studies across the world.
2. Methods
This study was performed over a 24-month period at major referral centres in two countries in the Anglophone Caribbean [6]. Through an initiative from the Caribbean Chapter of the Americas Hepatopancreatobiliary Association, hepatobiliary referral centres were set up in these countries to serve the entire Caribbean population [7]. At these centres, multidisciplinary teams met weekly to review electronic images and plan the management of patients with liver and pancreatic diseases. The local institutional review board granted approval to review all images during these meetings.
All patients had multiphase computed tomography scans by using 64-slice multirow detector scanners. A nonionic contrast medium, Ultravist 300® (iopromide), in a volume of 100 ml, was routinely administered in all studies by using a pressure injector with bolus tracking. We included all scans with an arterial phase that adequately covered the CT, SMA, and IMA territories. Exclusion criteria included duplicated scans, those with incomplete demographic data, inadequate arterial phases, and patients with prior vascular surgery or abdominal interventional radiology procedures.
2.1. Definitions
Żytkowski et al. [8] pointed out that there are normal variations in anatomy in all body systems, but there are also classic anatomic descriptions to describe the most common anatomic patterns. We referred to these classic anatomic descriptions of arterial anatomy [1, 9], where three major arteries arise from the anterior aspect of the abdominal aorta to supply the intra-abdominal viscera. The CT scan is most cephalad and branches into the common hepatic, splenic, and left gastric arteries (Figure 1). The SMA gives off the inferior pancreaticoduodenal, middle colic, right colic, ileocolic, ileal, and jejunal arteries (Figure 2). The IMA arises at the third lumbar vertebral level and gives off the left colic, sigmoid, and superior rectal arteries.
Figure 1.

Three-dimensional volume rendering CT image shows normal branching patterns from the abdominal aorta. The celiac trunk (CT) is the most cephalad branch and gives off three branches: the splenic (S), left gastric (G), and common hepatic (CH) arteries. The superior mesenteric artery (SMA) arises at the L1 vertebral level from the aorta.
Figure 2.

Ramifications of the superior mesenteric artery (arrow) include the inferior pancreaticoduodenal (1), middle colic (2), jejunal (3), ileal (4), right colic (5), and ileocolic arteries (6).
Although there are many reported variants, there is no consensus on nomenclature. For the purposes of this study, we defined the CMT as a common arterial channel arising from the abdominal aorta, regardless of its vertebral level, and giving off branches that belong to CT and mesenteric artery territories. We defined two types: complete and incomplete [10–14].
A complete CMT was one in which a single common trunk arose from the aorta and gave origin to all branches of the mesenteric artery and celiac trunk territories. Two complete CMT subtypes were defined: the classic celiacomesenteric trunk (CT and SMA territorial branches) and a celiac-bi-mesenteric trunk (CT, SMA, and IMA territorial branches).
An incomplete CMT was one in which there was a shared origin for at least one arterial branch across the CT and mesenteric artery territories. Nomenclature was based on the branches from the common trunk, regardless of the origin of remaining arteries that did not originate at the shared trunk. Table 1 summarizes the definitions used in this study for the purposes of classification.
Table 1.
Anatomic variants of the ventral branches of the abdominal aorta in 665 persons.
| Anatomic variant | Description: arterial origin from the abdominal aorta | N (%) |
|---|---|---|
| Celiacomesenteric trunk | Arteries belonging to the celiac trunk and mesenteric artery territories have a common origin from the abdominal aorta | 16 (2.4%) |
|
| ||
| (i) Complete | A common origin for all arterial branches from CT and mesenteric artery territories | |
| (a) Celiacomesenteric | A common origin for all arterial branches from CT and SMA territories only | 3 (0.55%) |
| (b) Celiac-bi-mesenteric | A common origin for all arterial branches of the CT, SMA, and IMA territories | 0 |
|
| ||
| (ii) Incomplete | A common origin for some arterial branches from CT and mesenteric artery territories | |
| (a) Gastro-mesenteric | A common origin for the left gastric artery and SMA | 0 |
| (b) Spleno-mesenteric | A common origin for the splenic artery and SMA | 0 |
| (b) Hepato-mesenteric | A common origin for the hepatic artery and SMA | 12 (1.8%) |
| (c) Hepato-spleno-mesenteric | A common origin for the hepatic artery, splenic artery, and SMA | 1 (0.15%) |
| (d) Gastro-spleno-mesenteric | A common origin for the left gastric, splenic, and SMA | 0 |
| (e) Hepato-gastro-mesenteric | A common origin for the hepatic artery, left gastric, and SMA | 0 |
CT = celiac trunk; SMA = superior mesenteric artery; IMA = inferior mesenteric artery.
2.2. Caribbean Data
Using these definitions, three radiologists independently examined all computed tomography images encountered between August 30, 2017, and September 1, 2019. Image series in which a CMT was thought to be present were selected for detailed re-examination by all three radiologists. These were experienced radiologists who completed specialty training in radiology, each with more than 5 years of experience as consultant radiologists. Patients were only included in the study sample if there was an agreement between all radiologists that a CMT was present. In the event of a disagreement, this was resolved by group discussion and re-examination of images by the three radiologists.
In patients who possessed a CMT, we recorded demographic details and the relevant anatomic details. Data were recorded in a Microsoft Excel sheet. Descriptive analyses were performed by using the SPSS statistical software.
2.3. Systematic Literature Review
We then conducted a systematic literature review using medical archiving platforms, including Pubmed, Medline, Google Scholar, and the Cochrane Database of Systematic Reviews. We used the following search terms: “coeliaco-mesenteric trunk,” “coeliaco-bi-mesenteric trunk,” “coeliac axis variants,” “coeliac trunk variants,” “common trunk,”, “gastro-splenic,” “spleno-mesenteric,” “gastro-hepatic,” “spleno-hepatic,” “gastro-colic,” “splenocolic,” “hepato-colic,” and “hepato-mesenteric.” All relevant studies were retrieved, and the data and images were reviewed in detail. We used the raw data from these retrieved studies to calculate the global prevalence of CMTs. Global prevalence was calculated by dividing the number of individuals with a CMT by the sum total of study samples from studies across the globe. The prevalence of the CMT in our study sample was also calculated and compared with the global prevalence. We used Pearson's chi-square and Fisher's exact tests to compare 2 × 2 contingency tables, and statistical significance was considered to be present when the P value was <0.05.
3. Results
3.1. Caribbean Data
A total of 832 CT scans were examined, and 167 scans were excluded from the final study sample for duplications (64), prior intra-abdominal vascular procedures (51), inadequate arterial phase (48), and incomplete demographic data (4). The final study sample comprised 665 scans that met the inclusion criteria. A CMT variant was present in 16 (2.41%) persons in the study sample, as detailed in Table 1. Overall, there was a preponderance of CMT variants in males (10 : 6). All patients were asymptomatic, and there were no clinical sequelae directly attributable to CMT variants in any of these persons.
Three (0.45%) males had a complete “classic” CMT (Figures 3 and 4), and there were no persons with a celiac-bi-mesenteric trunk. The most common incomplete CMT variant was a hepato-mesenteric trunk in 12 (1.8%) persons, involving the origin of the common hepatic artery (CHA) in 5 persons (Figure 5), the replaced right hepatic artery (RHA) in 4 persons (Figure 6), and the replaced left hepatic artery (LHA) in 3 persons. The only other incomplete CMT variant was a male with the hepato-spleno-mesenteric trunk (Figure 7).
Figure 3.

Three-dimensional volume rendering CT image showing a complete celiacomesenteric trunk (CMT) inclusive of mesenteric (M) and celiac (C) ramifications.
Figure 4.

Three-dimensional volume rendering CT image showing a complete CMT (arrow). The celiac branches visible include the splenic (1), left gastric (2), common hepatic (3), and gastroduodenal arteries (4). The mesenteric branches visible include the inferior pancreaticoduodenal (4) and superior mesenteric ramifications (5).
Figure 5.

Fluoroscopic images during selective mesenteric angiography showing the common hepatic artery (CHA) arising from the superior mesenteric artery (SMA) and then bifurcating into the left (LHA) and right (RHA) hepatic arteries.
Figure 6.

Incomplete CMT: hepato-mesenteric variant showing a replaced right hepatic artery (C) arising from the superior mesenteric artery (B) instead of the celiac trunk (A).
Figure 7.
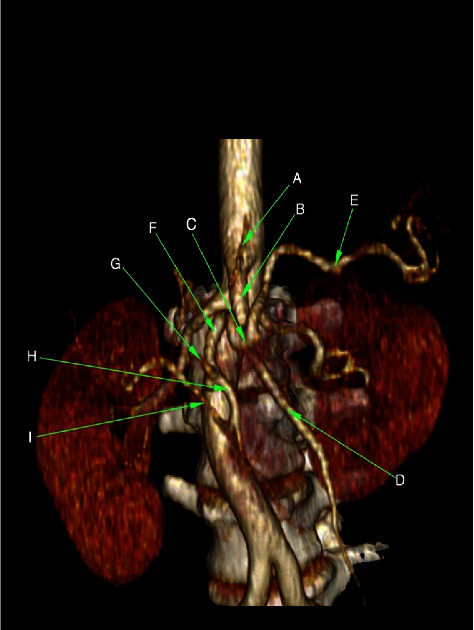
Three-dimensional volume rendering CT image demonstrating a hepato-spleno-mesenteric trunk. A = left gastric artery, B = celiacomesenteric trunk, C = celiac trunk, D = superior mesenteric artery, E = splenic artery, F = common hepatic artery, G = left hepatic artery, H = gastroduodenal artery, and I = right hepatic artery (reproduced with permission from Johnson PB, et al. Vascular Supply to the Liver: Report of a Rare Arterial Variant. Case Rep Radiology. 2013.969327:1-3. DOI: 10.1155/2013/969327 [2]).
3.2. Systematic Review
In our review of the medical literature, we encountered 42 population-based series that reported the prevalence of CMT variants in a total of 74,320 persons [1, 9–49]. In each study, the raw data were extracted and tabulated for the purpose of data analyses. The raw data and statistical comparisons are presented in Table 2. There was a statistically lower incidence of the hepato-mesenteric variant in this sample (1.8% vs. 3.24%; P=0.0352).
Table 2.
Analysis of population-based studies evaluating variants of the celiacomesenteric trunk.
| Country | Author | Method | Study sample | Conventional branches | CMT variants | Complete CMT | Incomplete CMT | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Celiac-bi-mesenteric | “Classic” CMT | G-M | S-M | H-M | H–S-M | G-S-M | H-G-M | ||||||
| France | Piquand et al., 1910 [15] | Cadaver | 50 | 41 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | Rio branco, 1912 [16] | Cadaver | 50 | 45 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| USA | Lipshutz et al., 1917 [1] | Cadaver | 83 | 62 | 2 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 |
| USA | Eaton et al., 1917 [17] | Cadaver | 206 | 186 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Japan | Adachi et al., 1928 [18] | Cadaver | 252 | 218 | 10E | 0 | 6 | 0 | 0 | 1 | 3 | 0 | 0 |
| USA | Michels et al., 1955 [9] | Cadaver | 200 | 110 | 32E | 0 | 0 | 0 | 1 | 31E,5 | 0 | 0 | 0 |
| USA | Nelson et al., 1988 [19] | Cadaver | 50 | 12 | 13E | 0 | 3 | 0 | 0 | 10 | 0 | 0 | 0 |
| Japan | Shoumura et al., 1991 [20] | Cadaver | 450 | 408 | 12E | 0 | 5 | 0 | 0 | 5 | 2 | 0 | 0 |
| U.S.A. | Hiatt J. et al., 1994 [21] | Transplant operations | 1,000 | 757 | 15E | 0 | 0 | 0 | 0 | 15 | 0 | 0 | 0 |
| Australia | Jones et al., 2001 [22] | Transplant dissection | 180 | 164 | 30E | 0 | 3 | 0 | 0 | 27 | 0 | 0 | 0 |
| Japan | Nakamura et al., 2003 [23] | Cadaver | 250 | NR | 3E | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 |
| Italy | Ferrari et al., 2007 [24] | Imaging (CT) | 60 | 34 | 6E | 0 | 1 | 0 | 0 | 5 | 0 | 0 | 0 |
| Italy | Ieezi et al., 2008 [25] | Imaging (CT) | 524 | 378 | 2E | 0 | 0 | 0 | NR | NR | 2 | 0 | 0 |
| Japan | Chen et al., 2009 [26] | Cadaver | 974 | 875 | 49E | 0 | 7 | 0 | 0 | 33 | 7 | 2 | 0 |
| South Korea | Song et al., 2010 [27] | Imaging (CT) | 5002 | 4,457 | 232E | 0 | 53 | 1 | 9 | 132 | 34 | 3 | 0 |
| Russia | Egorov et al., 2010 [28] | Imaging (CT) | 350 | 197 | 58E | 0 | 0 | 0 | 0 | 58E,4 | 0 | 0 | 0 |
| Poland | Kornafel et al., 2010 [29] | Imaging (CT) | 201 | 192 | 4E | 0 | 3 | 0 | 0 | 1 | 0 | 0 | 0 |
| Japan | Natsume et al., 2011 [30] | Imaging (CT) | 175 | 159 | 9E | 0 | 1 | 0 | 0 | 5 | 1 | 1 | 1 |
| Spain | Villa et al., 2012 [31] | Imaging (CT) | 100 | 85 | 15E | 0 | 1 | 0 | 0 | 14E,2 | 0 | 0 | 0 |
| Japan | Miyaki et al., 2012 [32] | Cadaver | 378 | NR | 8E | 0 | 2 | 0 | 0 | 6 | 0 | 0 | 0 |
| Romania | Matusz et al., 2012 [33] | Review | 10,750 | 9,751 | 73 | 0 | 73 | NR1 | NR1 | NR1 | NR1 | NR1 | NR1 |
| Greece | Panagouli et al., 2013 [10] | Systematic review | 12,196 | 10,906 | 446E | 1 | 93 | 0 | 0 | 297/9829E,7 | 49 | 6 | 0 |
| China | Mu et al., 2103 [34] | Imaging (CT) | 102 | 60 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Serbia | Ognjanovic et al., 2014 [35] | Imaging (CT) | 150 | 117 | 19E | 0 | 4 | 0 | 0 | 15 | 0 | 0 | 0 |
| China | Wang et al., 2014 [36] | Imaging (CT) | 1500 | 1,347 | 135E | 0 | 23 | 0 | 18 | 67 | 26 | 1 | 0 |
| Romania | Iacob et al., 2014 [37] | Imaging (CT) | 5442 | 4,942 | 30E | 0 | 23 | 0 | 0 | NR | 7 | 0 | |
| China | Huang et al., 2015 [38] | Imaging (CT) | 238 | 220 | 10E | 0 | 2 | 0 | 2 | 6 | 0 | 0 | 0 |
| India | Sharma et al., 2015 [39] | Imaging (CT) | 80 | 66 | 3 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| India | Babu et al., 2015 [11] | Imaging (CT) | 682 | 548 | 19E | 0 | 3 | 1 | 0 | 12E,3 | 3 | 0 | 0 |
| Poland | Torres et al., 2015 [40] | Imaging (CT) | 1569 | 1455 | 72E | 0 | 8 | 0 | 0 | 64 | 0 | 0 | 0 |
| Japan | Yuasa et al., 2016 [41] | Imaging (CT) | 279 | 253 | 8E | 0 | 3 | 0 | 1 | 3 | 1 | 0 | 0 |
| Egypt | Osman et al., 2016 [42] | Imaging (CT) | 1000 | 905 | 142E | 0 | 6 | 0 | 0 | 136 | 0 | 0 | 0 |
| Iran | Farghadani et al., 2016 [12] | Imaging (CT) | 607 | 308 | 72E | 0 | 4 | 0 | 2 | 66E,6 | 0 | 0 | 0 |
| Turkey | Alsaner et al., 2017 [43] | Imaging (CT) | 1000 | 890 | 4E | 0 | 1 | NR | NR | NR | 3 | 0 | 0 |
| Pakistan | Khan et al., 2017 [44] | Imaging (CT) | 160 | 139 | 2E | 0 | 1 | NR | NR | NR | 1 | 0 | 0 |
| Turkey | Caliskan et al., 2018 [45] | Imaging (CT) | 174 | 157 | 10E | 0 | 3 | 0 | 1 | 5 | 1 | 0 | 0 |
| Mexico | Pinal-Garcia et al., 2018 [13] | Cadaver | 140 | 61 | 4E | 0 | 0 | 0 | 1 | 3 | 0 | 0 | 0 |
| Romania | Bordei et al., 2019 [46] | Imaging (CT) | 2220 | NR | 12 | 0 | 12 | NR | NR | NR | NR | NR | NR |
| China | Tang et al., 2019 [47] | Imaging (CT) | 5580 | 5031 | 475E | 0 | 96 | 0 | 67 | 248 | 57 | 4 | 3 |
| China | Mao et al., 2019 [48] | Imaging (CT) | 2500 | 2243 | 225E | 0 | 85 | 0 | 27 | 112 | 1 | 0 | 0 |
| India | Ramadevi et al., 2020 [49] | Cadaver | 25 | 21 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czech Republic | Whitley et al., 2020 [14] | Meta-analysis | 17,391 | 15,639 | 620E | 0 | 125 | 4 | 30 | 378 | 78 | 5 | 0 |
| Global prevalence | Global | 74,320 | 63,439/71,472 (88.8%) | 2,886/74,320 (3.88%) | 2/74,320 (0.003%) | 659/74,320 (0.89%) | 6/60,190 (0.01%) | 159/59,666 (0.27%) | 1,758/54,224 (3.24%) | 276/61,350 (0.45%) | 22/61,350 (0.04%) | 4/61,350 (0.007%) | |
| Caribbean | Cawich et al. | Imaging (CT) | 665 | 649 (97.6%) | 16/665 (2.41%) | 0 | 3 (0.45%) | 0 | 0 | 12 (1.8%) | 1 (0.15%) | 0 | 0 |
| P value | Caribbean vs. global | 0.054 | — | 0.2985 | — | — | 0.0352 | 0.3798 | — | - | |||
E = extrapolated from raw data and/or published images. 1 = these authors reported an “incomplete CMT” in 63 (0.59%) cases but did not clearly define the meaning of this term. 2 = CHA from SMA (3) + accessory RHA from SMA (2) + replaced RHA from SMA (9). 3 = individual cases included CHA from SMA and LGA/SA from CT (9) + CHA from SMA and LGA/SA arising directly from the aorta (1) + replaced RHA from SMA (2). 4 = individual cases included CHA from SMA (9) + replaced RHA from SMA (49). 5 = individual cases included CHA from SMA (9) + replaced RHA from SMA (22). 6 = individual cases included CHA from SMA (8) + RHA from SMA (58). 7 = individual cases included splenogastric and hepato-mesenteric trunk (186) + splenogastric with CHA arising from SMA (111)
4. Discussion
The majority of persons in this Caribbean study sample had conventional branching from the abdominal aorta [50–53]. This classic pattern is reported to be present in 44% [13] to 91% [33] of persons in the international literature.
The CMT is recognized as a rare variant. Benjamin Lipshutz is credited with coining the term “truncus celiaco-mesenterica” when he described 2 cadavers with a variant where the SMA and CT took a common origin from the aorta [1]. In the subsequent decades, the CMT was documented in case reports [54–66] and larger population-based series [1, 9–49]. These data suggest that CMT occurs in 0.42% [37] to 2.7% [35] of unselected persons across the globe.
The CMT is believed to be an aberration in embryonic development. During embryogenesis, the visceral arteries arise from the primitive dorsal abdominal aorta through four roots (gastric, hepatic, splenic, and superior mesenteric roots) initially joined in a longitudinally-oriented primitive ventral anastomosis [1, 66]. The superior mesenteric root is the dominant arterial root [1] in the primitive ventral anastomosis. Usually, a cleft develops between the third and fourth arterial roots that separate the CT and SMA, respectively [66]. When the primitive cleft does not form, the primitive ventral anastomosis persists, and this gives rise to complete CMT. A partially formed primitive cleft does not separate all the primitive aortic roots and leads to the formation of an incomplete CMT. This was the basis of our classification.
Although many authors have written about CMT, there is no standardized definition in the medical literature. Most authors seem to agree that a CMT exists when there is a “common origin of the SMA and CT,” and it includes the three main CT branches [10, 12–14, 35]. However, some authors used other names to describe the same pattern, such as “gastro-hepato-spleno-mesenteric trunk” [55, 67], “CT arising from SMA” [64], or “persistent anastomotic channel” [27]. Still, others have required extra detail to meet their definition of a CMT. For example, Varma et al. [58] stipulated that the common origin for CT and SMA must “further divide into hepato-mesenteric and gastro-splenic trunks” to be defined as a CMT.
To add an additional layer of complexity, some authors include variants with only two main CT branches arising from the common origin in their definition of a CMT [14, 36, 47, 60]. For example, Tang et al. [47] defined the CMT as a “single common trunk arising from the aorta, and the branches include the SMA and at least two major branches of the CT.” Whitely et al. [14] also included variants with the SMA plus two major CT branches, defining this as an “incomplete CMT.” Yet, other authors reporting on the CMT ignore variants that include a combination of the SMA plus two CT branches [13, 27, 65]. For example, Bolintineanu et al. [65] reported on the presence of a hepato-spleno-mesenteric trunk that was not considered a CMT and, in fact, discussed CMTs separately in their paper.
Still, other authors include variants where the SMA plus one CT branch has a common origin from the aorta [11, 54, 60], while others do not consider these variants as CMTs [29, 36, 47]. For example, Kornafel et al. [29] excluded a variant in which the common hepatic artery (CT territory) arose from the SMA, instead terming this a “hepato-mesenteric trunk.” Meanwhile, other authors have introduced descriptive terms such as “complete vs. incomplete” CMTs [14, 33, 68] that inconsistently seem to be used interchangeably with “classic vs. variant” CMTs [11].
The wide variation in nomenclature and the multiplicity of classification systems [1, 9, 14, 18, 27, 36, 47, 54, 69] bear testimony to the fact that there is no standardized nomenclature or definition. We based our classification on the basis of embryologic development of the aortic branches, independent of the final ramifications of the CMT branches and/or origins of non-CMT arteries. We avoided numeric classifications that we found confusing and instead attempted to describe CMT ramifications using the combinations of the branch names as determined by their territorial supply. We thought this would allow for a better correlation with multifarious definitions and classification systems currently used in the medical literature.
In this study, we did not encounter any persons with a celiac-bi-mesenteric trunk. This was not surprising as it is extremely rare [10, 14], with a global prevalence of only 0.02%. The “classic” complete CMT was present in 0.45% of unselected persons in our study sample, and this was statistically similar to the global prevalence (0.82%).
The most common incomplete CMT variant in our sample was the hepato-mesenteric trunk (1.8%), but it was significantly less prevalent in our sample than was seen across the globe (3.24%; P=0.0352). Due to the multifarious existing classifications, comparisons were challenging because some authors reporting on the hepato-mesenteric trunk attempted to distinguish between variants with the CHA arising from the SMA versus a replaced or accessory HA arising from the common trunk [10–12, 19, 28, 31]. Others attempted to define the hepato-mesenteric trunk according to the terminal HA branches arising from the common trunk [9, 21]. One publication even attempted to make an unclear distinction between “a combination of splenogastric and hepato-mesenteric trunk” separate from “splenogastric trunk with CHA arising from the SMA,” both categories being reported individually [10]. In our study, we did not attempt to distinguish between persons with CHA and accessory or replaced hepatic arteries arising from the common trunk because there is clinical significance that once any one of these vessels arises from the common origin. The clinical significance of these variations is discussed below.
The only other incomplete CMT variant we encountered was the hepato-spleno-mesenteric variant in 0.15% of unselected persons, and this was statistically similar to the 0.45% global incidence of this variant. There are existing reports on the hepato-spleno-mesenteric trunk in the medical literature [10, 11, 14, 18, 20, 25–27, 36, 37, 47, 48, 67, 70–72], although there is some variation in descriptions. For example, Loukas et al. [73] described a 74-year-old woman with an “anomalous splenic artery which arose as a branch of the mesenteric artery and gave rise to the common hepatic artery.” Although they did not use nomenclature, a detailed review of the anatomic description and published photographs reveal that this was actually a hepato-spleno-mesenteric trunk. Similarly, Hemant et al. [74] described a case in which the “SMA gave hepatosplenic trunk as its first branch,” and then, the “hepatosplenic trunk divided into the splenic artery and a branch to the common hepatic artery.” Published photographs suggest this is also a hepato-spleno-mesenteric trunk.
5. Clinical Significance
Some authors have noted that a CMT can be associated with other arterial variants [1, 9, 18, 27, 42, 46, 69], morphologic anomalies [11, 56, 63], and/or clinical sequelae [62, 63]. None of the patients in our study had clinical sequelae attributable to the presence of a CMT, and they were all incidentally discovered during imaging for other diagnoses. Nevertheless, awareness of this anatomic variation carries great clinical significance when it comes to invasive surgical or interventional procedures.
Interventional radiologists are often required to perform selective angiography of the aortic branches to identify a source of haemorrhage in patients with gastrointestinal bleeding, diagnostic angiography in trauma patients with solid visceral injuries, infusion of transarterial hepatic chemotherapy, angioembolization for pancreatic pseudoaneurysms, and solid organ injuries. In these cases, the presence of the CMT increases technical complexity and impacts procedural planning. These variations are also important in surgical practice as they herald technical difficulty at operation and require modification of operative procedures. The variation in CMT origin and course of the arterial branches increases the risk of iatrogenic arterial injury during pancreaticoduodenectomy, hepatectomy, and gastrectomy. For example, a CHA arising from a CMT often takes an aberrant course posterolateral to the pancreatic neck, which puts it at great risk of injury during a pancreaticoduodenectomy, leading to intraoperative haemorrhage, hepatic ischaemia, biliary strictures, anastomotic leaks, or death.
In addition, some oncologic operations require the division of arteries at their origin in order to achieve a proper nodal harvest. For example, the surgical oncologist is required to divide the left gastric artery at its origin during a gastrectomy or distal oesophagectomy [10, 26, 66]. These variations also increase the complexity of transplant surgery as it may increase the risk of graft failure [10, 66, 75] and also require modification of operative techniques. For example, Guglielmo et al. [66] reported a modification of their transplant techniques requiring harvesting an aortic patch of the common trunk in organ procurement for liver transplantation.
In some cases, the presence of the CMT may be beneficial. For example, during suprarenal aneurysmorrhaphy, the vascular surgeon would be able to harvest and re-implant a single aortic patch to the prosthetic graft to maintain visceral perfusion instead of performing multiple re-implantations of CT and mesenteric arteries. On the other hand, the lower origin of the CMT or CBMT may impact the landing zone for endovascular stent prostheses. Bordei et al. [46] reported that 42% of persons with a CMT had a low origin from the aorta at the lower body of the L1 or L1/2 intervertebral disk.
5.1. Study Limitations
We considered whether the low CMT incidence in our study sample was due to human error or misinterpretation. However, all scans were performed on high-resolution multislice scanners with conventional arterial phase protocols and were independently reviewed by three radiologists with specialist interests in vascular anatomy. Therefore, we believe that these data are representative of the variations in this study sample.
6. Conclusion
In Caribbean populations, 99.3% of unselected persons have conventional upper abdominal aortic branch anatomy. There was no difference in the prevalence of the classic CMT in the Caribbean compared to the global prevalence (0.45% vs. 0.82%, respectively). However, the hepato-mesenteric trunk (incomplete CMT variant) was significantly less prevalent in the Caribbean (1.8% vs. 3.24%, respectively). Healthcare professionals performing hepatobiliary interventions must be aware of these differences in order to minimize morbidity during their interventions.
Data Availability
Data will be made available from the corresponding author upon reasonable request.
Ethical Approval
This research was approved by the local institutional board.
Conflicts of Interest
The authors declare that they have no conflicts of interests.
References
- 1.Lipshutz B. A composite study of the celiac axis artery. Annals of Surgery . 1917;65(2):159–169. doi: 10.1097/00000658-191702000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Johnson P. B., Cawich S. O., Shah S. D., et al. Vascular supply to the liver: a report of a rare arterial variant. Case Reports in Radiology . 2013;2013:3. doi: 10.1155/2013/969327.969327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cawich S. O., Sinanan A., Gosein M., et al. An investigative study of hepatic arterial anomalies in a west Indian population. Radiology Research and Practice . 2021;2021:6. doi: 10.1155/2021/9201162.9201162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cawich S. O., Naraynsingh V., Pearce N. W., et al. Surgical relevance of anatomic variations of the right hepatic vein. World Journal of Transplantation . 2021;11(6):231–243. doi: 10.5500/wjt.v11.i6.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Johnson P. B., Cawich S. O., Shah S. D., et al. Accessory renal arteries in a Caribbean population: a computed tomography based study. Springerplus . 2013;2:443–446. doi: 10.1186/2193-1801-2-443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Spence D., Dyer R., Andall-Brereton G., et al. Cancer control in the Caribbean island countries and territories: some progress but the journey continues. The Lancet Oncology . 2019;20(9):e503–e521. doi: 10.1016/S1470-2045(19)30512-1. [DOI] [PubMed] [Google Scholar]
- 7.Cawich S. O., Maharaj R., Naraynsingh V., et al. Clinical outcomes after major hepatectomy are acceptable in low-volume centers in the Caribbean. World Journal of Hepatology . 2019;11(2):199–207. doi: 10.4254/wjh.v11.i2.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Żytkowski A., Tubbs R. S., Iwanaga J., Clarke E., Polguj M., Wysiadecki G. Anatomical normality and variability: historical perspective and methodological considerations. Translational Research in Anatomy . 2021;23 doi: 10.1016/j.tria.2020.100105.100105 [DOI] [Google Scholar]
- 9.Michels N. A. Blood Supply and Anatomy of the Upper Abdominal Organs with a Descriptive Atlas . Philadelphia, PA, USA: Lippincott; 1955. [Google Scholar]
- 10.Panagouli E., Venieratos D., Lolis E., Skandalakis P. Variations in the anatomy of the celiac trunk: a systematic review and clinical implications. Annals of Anatomy . 2013;195(6):501–511. doi: 10.1016/j.aanat.2013.06.003. [DOI] [PubMed] [Google Scholar]
- 11.Ramesh Babu C., Joshi S., Gupta K., Gupta O. Celiacomesenteric trunk and its variants a multidetector row computed tomographic study. Journal of the Anatomical Society of India . 2015;64(1):32–41. doi: 10.1016/j.jasi.2015.04.007. [DOI] [Google Scholar]
- 12.Farghadani M., Momeni M., Hekmatnia A., Momeni F., Mahdavi M. B. Anatomical variation of celiac axis, superior mesenteric artery, and hepatic artery: evaluation with multidetector computed tomography angiography. Journal of Research in Medical Sciences . 2016;21(1):p. 129. doi: 10.4103/1735-1995.196611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pinal-Garcia D. F., Nuno-Guzman C. M., Gonzalez-Gonzalez M. E., Ibarra-Hurtado T. R. The celiac trunk and its anatomical variations: a cadaveric study. Journal of Clinical Medicine and Research . 2018;10(4):321–329. doi: 10.14740/jocmr3356w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Whitley A., Oliverius M., Kocian P., Havluj L., Gürlich R., Kachlik D. Variations of the celiac trunk investigated by multidetector computed tomography: systematic review and meta-analysis with clinical correlations. Clinical Anatomy . 2020;33(8):1249–1262. doi: 10.1002/ca.23576. [DOI] [PubMed] [Google Scholar]
- 15.Piquand G. Recherches Sur L’anatomie du Tronc Coeliaque et des ses Branches. Bibliotheca Anatomica . 1910;19:159–201. [Google Scholar]
- 16.Rio-Branco P. Essai sur l’anatomie et la medecine operatoire du tronc coeliaque et de ses branches, de l’artere hepatique en particulier . Hachette Livre, Paris, France: 1912. [Google Scholar]
- 17.Eaton P. B. The coeliac axis. The Anatomical Record . 1917;13(6):369–374. doi: 10.1002/ar.1090130605. [DOI] [Google Scholar]
- 18.Adachi B. Das Arteriensystem Der Japaner . Kyoto, Japan: University of kyoto; 1928. [Google Scholar]
- 19.Nelson T. M., Pollak R., Jonasson O., Abcarian H. Anatomic variants of the celiac, superior mesenteric, and inferior mesenteric arteries and their clinical relevance. Clinical Anatomy . 1988;1(2):75–91. doi: 10.1002/ca.980010202. [DOI] [Google Scholar]
- 20.Shoumura S., Emura S., Utsumi M., et al. Anatomical study on the branches of the celiac trunk (IV). Comparison of the findings with Adachi’s classification. Kaibogaku zasshi. Journal of anatomy . 1991;66(5):452–461. [PubMed] [Google Scholar]
- 21.Hiatt J. R., Gabbay J., Busuttil R. W. Surgical anatomy of the hepatic arteries in 1000 cases. Annals of Surgery . 1994;220(1):50–52. doi: 10.1097/00000658-199407000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jones R. M., Hardy K. J. The hepatic artery: a reminder of surgical anatomy. Journal of the Royal College of Surgeons of Edinburgh . 2001;46(3):168–170. [PubMed] [Google Scholar]
- 23.Nakamura Y., Miyaki T., Hayashi S., Iimura A., Itoh M. Three cases of the gastrosplenic and the hepatomesenteric trunks. Okajimas Folia Anatomica Japonica . 2003;80(4):71–76. doi: 10.2535/ofaj.80.71. [DOI] [PubMed] [Google Scholar]
- 24.Ferrari R., De Cecco C. N., Iafrate F., Paolantonio P., Rengo M., Laghi A. Anatomical variations of the coeliac trunk and the mesenteric arteries evaluated with 64-row CT angiography. Radiologia Medica, La . 2007;112(7):988–998. doi: 10.1007/s11547-007-0200-2. [DOI] [PubMed] [Google Scholar]
- 25.Iezzi R., Cotroneo A. R., Giancristofaro D., Santoro M., Storto M. L. Multidetector-row CT angiographic imaging of the celiac trunk: anatomy and normal variants. Surgical and Radiologic Anatomy . 2008;30(4):303–310. doi: 10.1007/s00276-008-0324-7. [DOI] [PubMed] [Google Scholar]
- 26.Chen H., Yano R., Emura S., Shoumura S. Anatomic variation of the celiac trunk with special reference to hepatic artery patterns. Annals of Anatomy - Anatomischer Anzeiger . 2009;191(4):399–407. doi: 10.1016/j.aanat.2009.05.002. [DOI] [PubMed] [Google Scholar]
- 27.Song S. Y., Chung J. W., Yin Y. H., et al. Celiac axis and common hepatic artery variations in 5002 patients: systematic analysis with spiral CT and DSA. Radiology . 2010;255(1):278–288. doi: 10.1148/radiol.09090389. [DOI] [PubMed] [Google Scholar]
- 28.Egorov V. I., Yashina N. I., Fedorov A. V., Karmazanovsky G. G., Vishnevsky V. A., Shevchenko T. V. Celiaco-mesenterial arterial aberrations in patients undergoing extended pancreatic resections: correlation of CT angiography with findings at surgery. Journal of the Pancreas . 2010;11(4):348–357. [PubMed] [Google Scholar]
- 29.Kornafel O., Baran B., Pawlikowska I., Laszczyński P., Guziński M., Sąsiadek M. Analysis of anatomical variations of the main arteries branching from the abdominal aorta, with 64-detector computed tomography. Polish Journal of Radiology . 2010;75(2):38–45. [PMC free article] [PubMed] [Google Scholar]
- 30.Natsume T., Shuto K., Yanagawa N., et al. The classification of anatomic variations in the perigastric vessels by dual-phase CT to reduce intraoperative bleeding during laparoscopic gastrectomy. Surgical Endoscopy . 2011;25(5):1420–1424. doi: 10.1007/s00464-010-1407-1. [DOI] [PubMed] [Google Scholar]
- 31.Villa D., Dura S., Barberia E., Rosa S., Piera V. P. CT Angiogaphy and volume-rendered reconstructions for evaluation of celiac trunk and hepatic arterial variants: results of a series of 100 patients. European Society of Radiology Online System . 2012;2:1–40. [Google Scholar]
- 32.Miyaki A., Imamura K., Kobayashi R., Takami M., Matsumoto J., Takada Y. Preoperative assessment of perigastric vascular anatomy by multidetector computed tomography angiogram for laparoscopy-assisted gastrectomy. Langenbeck’s Archives of Surgery . 2012;397(6):945–950. doi: 10.1007/s00423-012-0956-2. [DOI] [PubMed] [Google Scholar]
- 33.Matusz P., Miclaus G. D., Ples H., Tubbs R. S., Loukas M. Absence of the celiac trunk: case report using MDCT angiography. Surgical and Radiologic Anatomy . 2012;34(10):959–963. doi: 10.1007/s00276-012-0989-9. [DOI] [PubMed] [Google Scholar]
- 34.Mu G. C., Huang Y., Liu Z. M., Lin J. L., Zhang L. L., Zeng Y. J. Clinical research in individual information of celiac artery CT imaging and gastric cancer surgery. Clinical and Translational Oncology . 2013;15(10):774–779. doi: 10.1007/s12094-013-1002-8. [DOI] [PubMed] [Google Scholar]
- 35.Ognjanović N., Jeremić D., Živanović-Mačužić I., et al. MDCT angiography of anatomical variations of the celiac trunk and superior mesenteric artery. Archives of Biological Sciences . 2014;66(1):233–240. doi: 10.2298/abs1401233o. [DOI] [Google Scholar]
- 36.Wang Y., Cheng C., Wang L., Li R., Chen J. H., Gong S. G. Anatomical variations in the origins of the celiac axis and the superior mesenteric artery: MDCT angiographic findings and their probable embryological mechanisms. European Radiology . 2014;24(8):1777–1784. doi: 10.1007/s00330-014-3215-9. [DOI] [PubMed] [Google Scholar]
- 37.Iacob N. Timişoara, Romania: “Victor Babeş” University of Medicine and Pharmacy; 2018. Study of the morphological variability of the celiac trunk and of the aberrant hepatic arteries by MDCT angiography. Doctoral Thesis. [Google Scholar]
- 38.Huang Y., Mu G. C., Qin X. G., Chen Z. B., Lin J. L., Zeng Y. J. Study of celiac artery variations and related surgical techniques in gastric cancer. World Journal of Gastroenterology . 2015;21(22):6944–6951. doi: 10.3748/wjg.v21.i22.6944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sharma B., Saxena D., Chauhan S., Agarwal S. K. CT angiography based study of variations in coeliac trunk and its surgical implications. IOSR Journal of Dental and Medical Science . 2015;14(12):63–67. [Google Scholar]
- 40.Torres K., Staskiewicz G., Denisow M., et al. Anatomical variations of the coeliac trunk in the homogeneous Polish population. Folia Morphologica . 2015;74(1):93–99. doi: 10.5603/fm.2014.0059. [DOI] [PubMed] [Google Scholar]
- 41.Yuasa Y., Okitsu H., Goto M., et al. Three-dimensional CT for preoperative detection of the left gastric artery and left gastric vein in laparoscopy-assisted distal gastrectomy. Asian Journal of Endoscopic Surgery . 2016;9(3):179–185. doi: 10.1111/ases.12280. [DOI] [PubMed] [Google Scholar]
- 42.Osman A. M., Abdrabou A. Celiac trunk and hepatic artery variants: a retrospective preliminary MSCT report among Egyptian patients. The Egyptian Journal of Radiology and Nuclear Medicine . 2016;47(4):1451–1458. doi: 10.1016/j.ejrnm.2016.09.011. [DOI] [Google Scholar]
- 43.Aslaner R., Pekcevik Y., Sahin H., Toka O. Variations in the origin of inferior phrenic arteries and their relationship to celiac axis variations on CT angiography. Korean Journal of Radiology . 2017;18(2):336–344. doi: 10.3348/kjr.2017.18.2.336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Khan R. N., Ali M., Sadiq M., Hasan N. Detecting anatomical variations of coeliac trunk branching pattern in the population of Karachi using 3D multidetector computed tomographic angiography. Annals Abbasi Shaheed Hospital & Karachi Medical & Dental College . 2017;22:262–269. [Google Scholar]
- 45.Caliskan E., Acar T., Ozturk M., et al. Coeliac trunk and common hepatic artery variations in children: an analysis with computed tomography angiography. Folia Morphologica . 2018;77(4):670–676. doi: 10.5603/FM.a2018.0037. [DOI] [PubMed] [Google Scholar]
- 46.Bordei P., Baz R., Rusali V., Jercan C., Ardeleanu V. Morphological characteristics of the celiac-mesenteric trunk. Romanian Journal of Military Medicine . 2019;122:31–35. doi: 10.55453/rjmm.2019.122.2.6. [DOI] [Google Scholar]
- 47.Tang W., Shi J., Kuang L. Q., Tang S. Y., Wang Y. Celiomesenteric trunk: new classification based on multidetector computed tomography angiographic findings and probable embryological mechanisms. World Journal of Clinical Cases . 2019;7(23):3980–3989. doi: 10.12998/wjcc.v7.i23.3980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Mao Y., Tang W., Jin B., Kuang L. Q., Zhang J., Wang Y. Absence of the celiac trunk: definition, classification, MDCT angiographic findings and their probable embryological mechanisms. Nuclear Medicine and Medical Imaging . 2019 doi: 10.21203/rs.2.10432/v1. [DOI] [Google Scholar]
- 49.Ramadevi G., Neelima P., Radha R. B., Srikanth M., Gandhi R. R., Rao S. S. P. Celíaco Bi mesenteric trunk with aberrant splenic artery from superior mesenteric artery – rare anatomical variation. Journal of Critical Reviews . 2020;7(14):2257–2262. [Google Scholar]
- 50.Nigah S., Patra A., Chumbar S., Chaudhary P. Topographic location and branching pattern of the superior mesenteric artery with its clinical relevance: a cadaveric study. Folia Morphologica . 2022;81(2):372–378. doi: 10.5603/fm.a2021.0031. [DOI] [PubMed] [Google Scholar]
- 51.Muro S., Sirirat W., Ban D., Nagakawa Y., Akita K. What comprises the plate-like structure between the pancreatic head and the celiac trunk and superior mesenteric artery? A proposal for the term “P-A ligament” based on anatomical findings. Anatomical Science International . 2021;96(3):370–377. doi: 10.1007/s12565-020-00597-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ito K., Takemura N., Inagaki F., et al. Diagnosis of celiac artery stenosis using multidetector computed tomography and evaluation of the collateral arteries within the mesopancreas of patients undergoing pancreaticoduodenectomy. Clinical Anatomy . 2021;34(7):1035–1042. doi: 10.1002/ca.23716. [DOI] [PubMed] [Google Scholar]
- 53.Bonardelli S., Spampinato B., Ravanelli M., et al. The role of emergency presentation and revascularization in aneurysms of the peripancreatic arteries secondary to celiac trunk or superior mesenteric artery occlusion. Journal of Vascular Surgery . 2020;72(1):46S–55S. doi: 10.1016/j.jvs.2019.11.051. [DOI] [PubMed] [Google Scholar]
- 54.Morita M. Reports and conception of three anomalous cases in the area of the celiac and superior mesenteric arteries. Igaku Kenkyu . 1935;9 [Google Scholar]
- 55.Detroux M., Anidjar S., Nottin R. Aneurysm of a common celiomesenteric trunk. Annals of Vascular Surgery . 1998;12(1):78–82. doi: 10.1007/s100169900120. [DOI] [PubMed] [Google Scholar]
- 56.Saeed M., Murshid K. R., Rufai A. A., Elsayed S. E., Sadiq M. S. Coexistence of multiple anomalies in the celiac-mesenteric arterial system. Clinical Anatomy . 2003;16(1):30–36. doi: 10.1002/ca.10093. [DOI] [PubMed] [Google Scholar]
- 57.Yi S. Q., Terayama H., Naito M., et al. A common celiacomesenteric trunk, and a brief review of the literature. Annals of Anatomy - Anatomischer Anzeiger . 2007;189(5):482–488. doi: 10.1016/j.aanat.2006.11.013. [DOI] [PubMed] [Google Scholar]
- 58.Varma K. S., Pamidi N., Vollala V. R. Common celiacomesenteric trunk. Jornal Vascular Brasileiro . 2009;8(3):271–273. [Google Scholar]
- 59.Subhash R. Celiaco mesenteric trunk—a case report. Med . 2013;6 [Google Scholar]
- 60.Okamura A., Alvarez D., Genovez P., Caldeira E. J., Da Cunha M. R., Carvalho C. A. F. A different origin of the right gastro-omental artery. International Journal of Morphology . 2015;33(4):1343–1347. doi: 10.4067/s0717-95022015000400025. [DOI] [Google Scholar]
- 61.Yadav S. P., Khan Z. T., Kankhare S. Hepatomesenteric and gastrosplenic trunks- a case report. Int J Healt Biomed Res . 2015;3(2):84–87. [Google Scholar]
- 62.Bindi E., Molinaro F., Angotti R., Aglianò M., Messina M., Messina M. Pediatric presentation of a celiaco-mesenteric trunk in association with a pelvic bilateral renal ectopia: an undescribed association. Journal of Case Reports . 2017;7(2):155–157. doi: 10.17659/01.2017.0044. [DOI] [Google Scholar]
- 63.Al-Zoubi N. A., Ghalayini I., Al-Okour R. Nutcracker syndrome associated with celiacomesentric trunk anomaly: case report. International Journal of Nephrology and Renovascular Disease . 2017;10:285–288. doi: 10.2147/ijnrd.s146814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Enkhbold C., Chinburen J., Amina O., Chinzorig M., Tserendorj D. Case report: pancreaticoduodenectomy for pancreatic ductal adenocarcinoma with a rare anomaly of celiac trunk originating from superior mesenteric artery. American Journal of Medical Case Reports . 2019;7(2):29–32. [Google Scholar]
- 65.Bolintineanu La, Costea A. N., Iacob N., Pusztai A. M., Pleş H., Matusz P. Hepato-spleno-mesenteric trunk, in association with an accessory left hepatic artery, and common trunk of right and left inferior phrenic arteries, independently arising from left gastric artery: case report using mdct angiography. Romanian Journal of Morphology and Embryology . 2019;60(4):1323–1331. [PubMed] [Google Scholar]
- 66.Guglielmo N., Meniconi R. L., Vennarecci G., Ettorre G. M. Celiaco-mesenteric trunk: a rare variation that must be known before liver transplant. Digestive and Liver Disease . 2020;52(3):p. 354. doi: 10.1016/j.dld.2019.11.003. [DOI] [PubMed] [Google Scholar]
- 67.Hiremath R., Aishwarya K. C., Pailoor A., Bhatt R. CT angiographic diagnosis of hepatosplenomesenteric trunk - a rare variation. IJAV . 2014;737e39 [Google Scholar]
- 68.Selvaraj L., Sundaramurthi I. Study of normal branching pattern of the coeliac trunk and its variations using CT angiography. Journal of Clinical and Diagnostic Research . 2015;9(9):AC01–AC04. doi: 10.7860/JCDR/2015/12593.6523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Uflacker R. Atlas of vascular anatomy: an angiographic approach. Baltimore: Williams & Wilkins citied in the British Journal of Anatomy . 2010;83:661–667. [Google Scholar]
- 70.Hirai Y., Yamaki K. I., Saga T., et al. An anomalous case of the hepatospleno-mesenteric and the gastro-phrenic trunks independently arising from the abdominal aorta. The Kurume Medical Journal . 2000;47(2):189–192. doi: 10.2739/kurumemedj.47.189. [DOI] [PubMed] [Google Scholar]
- 71.Varma K. S., Pamidi N., Vollala V. R., Bolla S. E. Hepato-spleno-mesenteric trunk: a case report. Romanian Journal of Morphology and Embryology . 2919;51(2):401–402. [PubMed] [Google Scholar]
- 72.Samarawickrama M. B. Hepatospleno-mesenteric trunk: a rare variation of the celiac trunk. Galle Medical Journal . 2010;15(1):39–41. doi: 10.4038/gmj.v15i1.2399. [DOI] [Google Scholar]
- 73.Loukas M., Shah R., Tubbs S., Merbs W. Multiple variations of the hepato-biliary vasculature including a splenomesenteric trunk. Singapore Medical Journal . 2010;51:6–8. [PubMed] [Google Scholar]
- 74.Hemant K., Garg S., Yadav T. D., Sahni D. Hepato-gastro-phrenic and hepato-spleno-mesenteric trunk: a rare anatomical variation. Tropical Gastroenterology . 2011;32:56–59. [PubMed] [Google Scholar]
- 75.Deshpande R. R., Heaton N. D., Rela M. Surgical anatomy of segmental liver transplantation. British Journal of Surgery . 2002;89(9):1078–1088. doi: 10.1046/j.1365-2168.2002.02153.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be made available from the corresponding author upon reasonable request.