

Abstract
Background
Sleep is beneficial for physical and mental health. Several mobile and wearable sleep-tracking devices have been developed, and personalized sleep feedback is the most common functionality among these devices. To date, no study has implemented an objective push-type feedback message and investigated the characteristics of habitual sleep behavior and diurnal symptoms when receiving sleep feedback.
Objective
We conducted a mobile health intervention trial to examine whether sending objective push-type sleep feedback changes the self-reported mood, physical symptoms, and sleep behavior of Japanese office workers.
Methods
In total, 31 office workers (mean age 42.3, SD 7.9 years; male-to-female ratio 21:10) participated in a 2-arm intervention trial from November 30 to December 19, 2020. The participants were instructed to indicate their momentary mood and physical symptoms (depressive mood, anxiety, stress, sleepiness, fatigue, and neck and shoulder stiffness) 5 times a day using a smartphone app. In addition, daily work performance was rated once a day after work. They were randomly assigned to either a feedback or control group, wherein they did or did not receive messages about their sleep status on the app every morning, respectively. All participants wore activity monitors on their nondominant wrists, through which objective sleep data were registered on the web on a server. On the basis of the estimated sleep data on the server, personalized sleep feedback messages were generated and sent to the participants in the feedback group using the app. These processes were fully automated.
Results
Using hierarchical statistical models, we examined the differences in the statistical properties of sleep variables (sleep duration and midpoint of sleep) and daily work performance over the trial period. Group differences in the diurnal slopes for mood and physical symptoms were examined using a linear mixed effect model. We found a significant group difference among within-individual residuals at the midpoint of sleep (expected a posteriori for the difference: −15, 95% credible interval −26 to −4 min), suggesting more stable sleep timing in the feedback group. However, there were no significant group differences in daily work performance. We also found significant group differences in the diurnal slopes for sleepiness (P<.001), fatigue (P=.002), and neck and shoulder stiffness (P<.001), which was largely due to better scores in the feedback group at wake-up time relative to those in the control group.
Conclusions
This is the first mobile health study to demonstrate that objective push-type sleep feedback improves sleep timing of and physical symptoms in healthy office workers. Future research should incorporate specific behavioral instructions intended to improve sleep habits and examine the effectiveness of these instructions.
Keywords: wearable activity monitor, smartphone app, sleep feedback, ecological momentary assessment, stabilized sleep timing, mood and physical symptoms
Introduction
Development of Mobile Health Technologies
Recent developments in internet and communication technologies, mobile sensing devices, and the Internet of Things (IoT) have enabled the acquisition of longitudinal multidimensional information, including real-time physiological, behavioral, and environmental data. For example, consumer-grade wearable fitness trackers (eg, Fitbit, Garmin, and Jawbone) can record health-related information such as physical activity, sleep, and heart rate objectively and repeatedly.
By using smartphones and their SMS text messaging, it is possible to provide effective support at the optimal time to promote awareness of one’s health condition and improve compliance with intervention trials. Mobile devices can be useful for changing health-related behaviors as a part of daily living. Following these technological advancements and their applicability, medical and public health practices supported by mobile devices, such as mobile health (mHealth) [1,2], have been attracting attention in recent years. Since 2017, more than 325,000 mHealth apps have become available in commercial app stores, and the number of available apps continues to grow [3]. mHealth apps have been used in several intervention trials targeting physical activity [4-6], smoking [7,8], and suicidal ideation [9], and their usefulness and effectiveness have been proven.
Health Effects of Habitual Sleep Behavior
Sleep is a significant aspect of recovery. In fact, adequate and good-quality sleep is associated with better physical and mental health [10-12] and improved daytime functioning, including decreased physical symptoms [13,14], better work performance [15], and improved quality of life [16].
Although research interest has focused on the importance of sleep duration and quality, recent studies indicate that sleep timing and stability of habitual sleep behavior also play important roles in health. In fact, delayed sleep timing is associated with obesity [17], congestive heart failure [18], poor glycemic control [19], and increased severity of depressive symptoms [20,21]. Additional studies have indicated that variability in day-to-day sleep behavior (ie, duration, timing, and quality), referred to as intraindividual variability [22], is linked to physiological dysfunction [23,24], adverse medical and mental health conditions [25], and poor psychological well-being [26]. Therefore, the multifaceted monitoring and regulation of habitual sleep behavior can contribute to the prevention and support for physical and mental health problems.
Applications of Mobile and Wearable Technologies to Improve Sleep
Sleep data, along with other health-related behavioral and physiological data, can be gathered in real time using mobile devices. The widespread use of mobile or wearable sensing devices (eg, bed sensors, smartphone apps, and activity monitors) makes it easier and more commonplace to monitor sleep behavior in real time [27]. Although most consumer devices do not have Food and Drug Administration clearance as medical devices, they are expected to provide opportunities to track habitual sleep behavior longitudinally in large-scale populations [28]. For instance, Crowley et al [29] attempted to incorporate consumer wearable devices into health-promoting trials. They investigated the efficacy of these devices in improving physical activity and sleep among 565 employees over a 12-month period and found that sleep duration increased steadily throughout the study period.
In addition, mHealth apps for treating sleep disturbance have been developed rapidly [30,31], and more than 2000 mHealth apps targeting sleep are presently available in commercial app stores [32]. Pulantara et al [33,34] developed the interactive Resilience Enhancing Sleep Tactics app and examined its clinical feasibility as a treatment for sleep behavior. They reported that using the app improved insomnia severity and overall sleep quality, and the app was not inferior to traditional in-person sleep treatment. Furthermore, Hoersch et al [35] and Kuhn et al [36] conducted randomized controlled trials and reported that participants who received mHealth interventions had improved insomnia severity and sleep quality compared with waitlisted control participants.
Remaining Issues
Despite the rapid growth of mHealth apps and mobile sensing technologies, recent reviews have indicated that scientific trials examining the usefulness of mHealth apps are limited [32], and further research is required to test whether objective data enhance sleep outcomes [37]. This research investigating the usefulness of mHealth apps in enhancing sleep has several limitations. First, most mHealth trials have not assessed sleep behavior objectively [31], and the feedback provided depended on self-report assessments by the participants. While some studies incorporated wearable devices into the trials [38,39], they used the measurements only to assess the efficacy of the trial but not to objectivize the feedback. Given the importance of self-management for habitual sleep behavior to prevent future health problems, it is beneficial to implement objective sleep feedback into the apps. Second, previous mHealth studies focused on improvement in limited aspects of habitual sleep behavior, such as sleep quality and sleep duration [31], and the dynamic aspects of sleep, including intraindividual variability in sleep measurements over the trial period, have tended to be ignored. To the best of our knowledge, only 1 mHealth study by Murawski et al [40] reported the dynamic aspects of sleep behavior and found that variability in sleep timing, as assessed by a self-report questionnaire, was improved after their intervention. Studying the dynamic features in sleep behavior may provide insight into the typical properties of sleep self-regulation processes when responding to feedback messages or other interventions. Finally, in view of the wide range of effects of sleep, including psychological well-being, the covariant relationships of sleep with daytime functions, such as mood, physical symptoms, and work performance, should be examined. The covariant relationships may contain important information about subordinate effects and facilitate a comprehensive understanding of sleep self-management.
Objective
The objective of this study was to conduct an mHealth trial sending objective push-type sleep feedback to healthy participants using a smartphone app and a wearable activity monitor. Specifically, we examined whether sending daily sleep feedback messages changed sleep behavior and self-reported symptoms of the participants, particularly depressive mood, anxiety, stress, sleepiness, fatigue, and neck and shoulder stiffness. We used exploratory analysis of the statistical properties of objectively measured sleep variables and the characteristics of momentary symptoms recorded during the day using ecological momentary assessment (EMA).
Methods
Study Design
In this study, we conducted a 2-arm intervention trial by performing random convenience sampling of office workers at an insurance company and stratifying them into control and feedback groups. By comparing the groups in terms of the characteristics of habitual sleep behaviors (sleep duration and midpoint of sleep), momentary symptoms (depressive mood, anxiety, stress, sleepiness, fatigue, and neck and shoulder stiffness), and daily work performance, we examined the effects of personalized sleep feedback. To minimize the memory distortion caused by retrospective recall, momentary symptoms were recorded on a smartphone app in real time. Habitual sleep behaviors were measured objectively using a wearable device. Possible extraneous variables, including pretrial psychological symptoms, habitual sleep behaviors, and work performance, were assessed before the trial.
EMA Method
We used the EMA method to acquire momentary mood and physical symptom data (ie, depressive mood, anxiety, stress, fatigue, sleepiness, and neck and shoulder stiffness) in real time. EMA is a method for recording participants’ behavior, psychological state, and physical symptoms in real time and at multiple time points, allowing the collection of self-report and objective data with reliability and ecological validity. Thus, EMA avoids potential distortions of retrospective recall in self-reported data [41,42].
Health Care Internet of Things System
We developed a cloud-based health care Internet of Things (HIT) system that can continuously acquire health-related information, including momentary symptoms, biological signals, and surrounding environmental information, recorded as part of daily living. The HIT system consists of a cloud server and a smartphone app for data collection (HIT server and HIT app, respectively). The HIT app is equipped with an EMA and users can record their momentary symptoms in daily life (Multimedia Appendix 1). In addition, the HIT app can connect with various IoT devices, including a proprietary activity monitor (Sciencenet device, Sciencenet Inc) used in this study, using Bluetooth Low Energy (BLE). Data are transferred from the IoT devices to the HIT server. The app is compatible with both Android and iOS operating systems. The HIT server can store, integrate, and manage data uploaded from the app and send personalized messages (push-type feedback messages) to the HIT app users. HIT systems have been used to assess self-reported symptoms in real time [43].
Participants
A convenience sample of 31 office workers working at an insurance company participated in this study. The mean age of the participants was 42.3 (SD 7.9) years, and the male-to-female ratio was 21:10. All participants were working from home during the trial period at the request of their employer to prevent the spread of COVID-19.
Participants were randomly assigned to a control or feedback group using the “sample” function in the R statistical software (version 4.0.2; R Foundation for Statistical Computing) so that the ratio of the sample size was 1:1. No stratification by age or sex was observed. Coauthor KS conducted this randomization, independent of the primary researcher HT. Although author HT was also informed of who was assigned to which group after the random assignment, he was not allowed to contact the participants during the trial period.
During the trial period, the participants in the feedback group received personalized messages regarding their current sleep status every morning, whereas the participants in the control group did not receive any messages. The control group consisted of 16 participants, including 9 males and 7 females, with a mean age of 44.1 (SD 8.3) years. The feedback group consisted of 15 participants, including 12 males and 3 females, with a mean age of 40.5 (SD 7.2) years.
Instruments
Baseline Questionnaire
Before the trial, the participants completed a baseline questionnaire, including their demographic information (age, sex, and BMI), psychological symptoms (depressive and anxiety symptoms), habitual sleep behaviors (habitual sleep duration and self-reported sleep quality), and self-reported work performance. Items included in the baseline questionnaire are listed in subsequent sections.
Psychological Symptoms
Depressive symptoms were assessed using the Japanese version of the Beck Depression Inventory second edition (BDI-II) [44,45]. The BDI-II is a 21-item self-report inventory for measuring the presence and severity of depression (score range 0-63). A high level of internal consistency (Cronbach α=.87) and item homogeneity have been confirmed for the Japanese version of the BDI-II [45]. The BDI-II classifies individuals into 4 categories based on an overall score: minimal or no depression, 0 to 13; mild depression, 14 to 19; moderate depression, 20 to 28; and severe depression, 29 to 63. A score of ≥14 points was used as the clinical cutoff point for depression.
Anxiety symptoms were assessed using the Japanese version of the State-Trait Anxiety Inventory (STAI) Form Y [46]. The STAI is a standardized self-report inventory for measuring state and trait anxiety with 20 items (STAI Y-1 and STAI Y-2, respectively). The STAI Y-1 measures the intensity of the anxiety felt by an individual in the present, whereas the STAI Y-2 measures how often an individual feels anxious. Scores range from 20 to 80 for each subscale, with higher scores indicating higher levels of anxiety.
Habitual Sleep Behaviors
Habitual sleep duration on workdays and free days (SLw and SLf, respectively) was assessed using a single question for each (“How long do you sleep on weekdays?” and “How long do you sleep if tomorrow is a holiday?”). These measurements were used to compute an index representing participants’ sleep status during the trial period. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI). The PSQI is a self-report inventory used to assess sleep quality over the preceding month [47,48]. The PSQI consists of 19 items on self-reported sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Scores range from 0 to 21, with a higher total score indicating poorer sleep quality. The strong reliability and validity of this questionnaire have been confirmed in a recent meta-analysis [49].
Self-reported Work Performance
Self-reported work performance was measured using the World Health Organization Health and Work Performance Questionnaire (HPQ) [50,51]. The HPQ asks participants to rate their overall work performance over the preceding 4 weeks on a self-anchoring scale from 0 to 10: “On a scale of 0 to 10, how would you rate your usual work performance over the past four weeks?” The score was converted to a 100-point scale by multiplying the raw score by 10, with a higher score indicating better work performance.
EMA Questionnaire
The participants answered an EMA questionnaire 5 times per day using the HIT app. The EMA included the following measurements:
Depressive mood and anxiety were scored using the Depression and Anxiety Mood Scale [52]. This scale comprises the following 9 adjectives representing mood states: “vigorous,” “gloomy,” “concerned,” “happy,” “unpleasant,” “anxious,” “cheerful,” “depressed,” and “worried.” On the basis of the 9 items, anxious (the sum of “concerned,” “anxious,” and “worried” scores), positive (the sum of “vigorous,” “happy,” and “cheerful” scores), and negative (the sum of “gloomy,” “unpleasant,” and “depressed” scores) moods were calculated. Depressive mood scores were obtained by combining the last 2 mood scores as follows: (300-positive mood score) +negative mood score. The resulting depressive mood scores were rescaled to range from 0 to 100.
Physical symptoms, including stress, sleepiness, fatigue, and neck and shoulder stiffness were rated according to the participant’s response to being asked if they felt “stressed,” “sleepy,” or “fatigued” and “if their neck and shoulders were stiff.”
Daily work performance was rated after work in response to the question, “How would you rate your work performance of today?”
These measurements were rated using a visual analog scale from 0 to 100 displayed on the screen. All scores were transferred to the HIT server immediately after the completion of each EMA questionnaire.
Sleep Monitoring
The participants were instructed to wear a wristband-type activity monitor on their nondominant wrist during the trial period, except while bathing, showering, performing rigorous exercise, or any other activities likely to damage the device. The device is equipped with triaxial piezoelectric accelerometers capable of detecting small changes in bodily acceleration (≥0.01 G/rad/s). We confirmed that the device performs at a level equivalent to research-grade actigraphy (Ambulatory Monitors Inc), which is widely used in clinical settings. Results of the comparative analysis are presented in Multimedia Appendix 2.
The device was configured to transfer physical activity data to the HIT server using the HIT app whenever a participant launched the app. We used zero-crossing counts, which counts the number of times per epoch that the acceleration signal level crosses 0 [53], accumulated per minute, to compute objective sleep variables.
To estimate sleep variables, we adopted the Cole-Kripke algorithm with Webster’s rescoring rules [54,55] for zero-crossing count data to identify whether the recorded 1-minute epoch was sleep or wake. Next, we introduced the sleep probability function (SPF) θ(t) as follows:
 |
where t denotes the clock time converted to a numerical value (eg, 3 AM is transformed to 3.00, and 6:30 PM is converted to 18.50). Thus, the SPF is a value ranging from 0 to 1 and represents circadian oscillations.
Then, we estimated the effective SPF parameters (β0, β1, and β2) to fit the actual Cole-Kripke identification using a Bernoulli logistic regression model.
| CK(t)~bernoulli(θ(t))... (2) |
where CK(t) represents the result of Cole-Kripke identification when the clock time is t; CK(t) = 0 and CK(t) = 1 denote that the epoch at time t was labeled as wake and sleep, respectively.
Finally, we estimated the square waveform function θ’(t) from θ(t) by introducing onset and offset (ton and toff, respectively).
 |
Effective ton and toff were computed to maximize the R2 value between θ’(t) and CK(t) using the Nelder-Mead method. We assumed that ton and toff represent bedtime and wake-up time, respectively; thus, sleep duration and midpoint of sleep were determined using their interval and midpoint. We confirmed that the algorithm was performed at a level equivalent to Action-W version 2 software (AW2 software, Ambulatory Monitors Inc), which was used to analyze the research-grade actigraphy data (Multimedia Appendix 2).
The average sleep duration per day was calculated based on the habitual sleep duration on workdays and free days (Sw and Sf, respectively) in the baseline questionnaire using the following equation:
 |
which represents the expected sleep duration per day because the participants worked 5 days per week. Sleep debt and cumulative sleep debt were defined as follows:
| sleep debt = Average sleep duration − Estimated sleep duration...(5) |
| cumulative sleep debt = Σsleep debt...(6) |
Thus, sleep debt represents sleep insufficiency per day, and cumulative sleep debt represents its cumulative value over time. During the trial period, these values were automatically sent to the participants in the feedback group using the HIT app.
Data Collection Protocol
Trained researchers provided participants with a comprehensive explanation of the purpose and potential risks of the study. Subsequently, they signed an informed consent form and completed the baseline questionnaire. In addition, they received a sleep hygiene guide that listed daytime activities to improve their habitual sleep behaviors or health conditions (Multimedia Appendix 3). They were then asked to install the HIT app on their smartphones and wear an activity monitor on their nondominant wrist. All participants were instructed on the use of the app and the activity monitor. Using these instruments, we repeatedly measured their momentary symptoms and physical activity data in real time. The setup and operating procedures were presented on the web as much as possible using a communication service and videoconferencing system.
An overview of the trial is shown in Figure 1. This trial was carried out for almost 3 weeks (from November 30 to December 19, 2020). During the trial period, the participants were asked to complete the EMA questionnaires (see the section EMA Questionnaire) at randomly selected times within +10 minutes to −10 minutes of predetermined times (10 AM and 2 PM). In addition, they were asked to complete the EMA when they woke up, finished their work, and went to bed (wake-up time, after work, and bedtime, respectively).
Figure 1.

Overview of the trial. HIT: health care Internet of Things.
At 9 AM every day, the physical activity data on the HIT server were collated and analyzed to estimate sleep duration, sleep debt, and cumulative sleep debt using a local data analysis server. On the basis of the estimated sleep data, personalized sleep feedback messages were generated and sent to participants in the feedback group. They were informed about their sleep status (estimated sleep debt and cumulative sleep debt) and requested to plan and adjust their daytime activities with reference to guidelines for reducing their sleep debt. The message read as follows: “You accumulated XX minutes of sleep debt yesterday. Your current overall debt is XX minutes. Sleep debt has adverse effects on physical and mental health. Adjust your daytime behavior to cancel your debt.”
If sufficient physical activity data (<720 records/day) had not been uploaded to the server by 9 AM, an alternative message was sent to the participant requesting them to confirm the BLE pairing of the activity monitor with their app: “It seems that your data have not been uploaded successfully. We will analyze the data again at 1 PM. Please check the BLE connection of your HIT app before then.” The same computation process was executed at 1 PM for the relevant participants. These processes were executed by the local servers and were fully automated.
After the trial period, the participants rated their overall work performance in the preceding 2 weeks on a self-anchoring scale from 1 to 10. The question was as follows: “On a scale from 0 to 10, how would you rate your work performance over the past two weeks?” While the HPQ was originally developed to evaluate work performance over the past month, the scale used in this study was modified to evaluate performance over the past 2 weeks, corresponding to the survey period.
Statistical Analysis
Sleep variables, including sleep duration and midpoint of sleep, and daily work performance were recorded once a day, while mood and physical symptoms were recorded several times a day using smartphone-based EMA. Owing to this difference in the frequency of data recording, we used different models to analyze the group differences in the obtained data.
For the sleep variables and daily work performance, we constructed a hierarchical Bayesian model to capture the daily trend, baseline level, and within-individual stability, as follows:
| yijk = βij 0 + βi 1 Dayijk + eijk |
| βij 0 = βi 0 + rij 0 |
| eijk ~ N(0, σiy) |
| rij0~ N(0,σ0) |
where yijk indicates the dependent variable (sleep duration, midpoint of sleep, or daily work performance) at the k-th recording for the j-th participant in the i-th group; Dayijk indicates the day on which the corresponding dependent variable was measured to record the trend (improving or worsening); βij0 is the intercept of the j-th participant in the i-th group; βi1 is the slope for the day of the i-th group; the random terms rij0 are the between-individual residuals; and eijk are the within-individual residuals. In particular, the variance component σiy can be interpreted as a measurement of how stable or fluctuating the sleep variables within an individual are at the group level. Therefore, σiy was assumed to be affected by whether the intervention was provided and estimated for each group. All random terms were assumed to follow a normal distribution.
For EMA-recorded mood and physical symptoms, we used linear mixed effect models to examine their diurnal slopes and group differences.
| yijk = βj 0 + β 1 Timeijk + β 2 Groupijk + β 3 Timeijk * Groupijk + eijk |
| βj 0 = β 0 + rj 0 |
| eijk ~ N(0, σy) |
| rj0~ N(0,σ0) |
where yijk indicates the moods or physical symptoms at the k-th recording for the j-th participant in the i-th group; Timeijk indicates the categorical variable representing the timing when the corresponding dependent variables were recorded; thus, Timeijk = 0 and Timeijk = 1 denote that the dependent variables were recorded at wake-up time and bedtime, respectively; Groupijk indicates the categorical variable representing the group in which the j-th participant was classed; thus, Groupijk = 0 and Groupijk = 1 denote that the dependent variable was obtained from the participant classed as the control and feedback groups, respectively; βj 0 is the intercept of the j-th participant; β1, β2, and β3 are the coefficients for Timeijk, Groupijk, and their interaction term, respectively; the random terms rj0 are the between-individual residuals and eijk are the within-individual residuals. All random terms were assumed to follow a normal distribution. When a significant interaction effect was observed, we performed multiple comparison tests with Tukey correction.
In addition, we performed two-tailed Welch t test and Fisher exact test for the baseline data to confirm that there were no significant group differences. As the HPQ scores were recorded in the baseline and follow-up questionnaires, we performed 2-way repeated measures ANOVA to examine the main effects of group (control vs feedback) and time (pre- vs postintervention) and their interaction effect. For the cumulative sleep debt, we performed the Welch 2-tailed t test and Levene test for equality of variances for the final observation data per participant to examine the group differences in terms of mean and variance.
All analyses were performed using R statistical software (version 4.0.2). In particular, the parameters of the statistical models were computed using the rstan [56] and lmerTest [57] packages. The emmeans package (also known as the lsmeans package) [58] was used for multiple comparison tests with Tukey correction. Statistical significance was defined as when the 95% credible interval (CI) did not include the null value or when a P value <.05.
Ethics Approval
The Ethics Committee of the University of Tokyo approved this study and the informed consent form (approval number 20-20).
Results
Demographic Characteristics
In total, 31 individuals agreed to participate in the study. However, the data of 4 participants were excluded from the statistical analyses because of their low response rates for wake-up time and bedtime on the EMA questionnaire (ie, <3 days; Figure 2). The demographic characteristics of the participants, including the control group (n=12) and the feedback group (n=15), are presented in Table 1. The mean age of the participants was 41.8 (SD 7.9) years, and 33% (9/27) were females. The Welch 2-tailed t test and Fisher exact test showed that there were no significant differences in demographic characteristics between the groups. The total number of EMA records was 1839, and the overall response rate was 64.88% (1839/2835).
Figure 2.
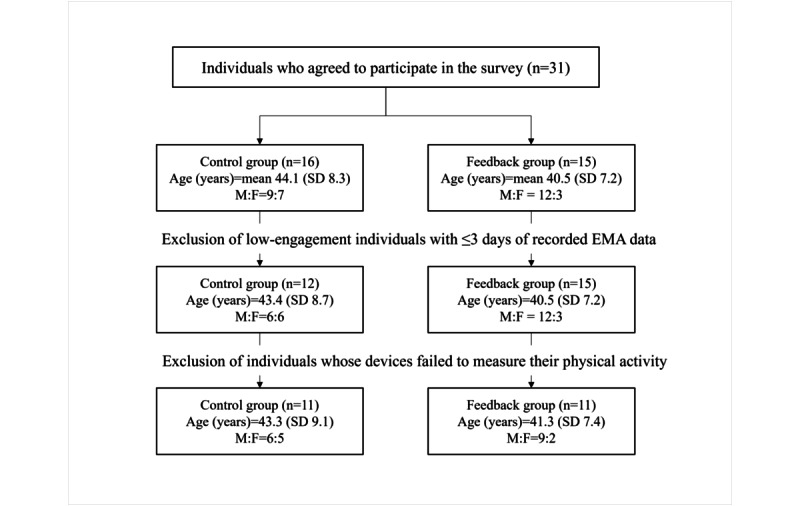
Flowchart of participant data selection for analyses. EMA: ecological momentary assessment; F: female; M: male.
Table 1.
Baseline demographic characteristics of participants by group.
|
|
Overall (N=27) | Control group (n=12) | Feedback group (n=15) | P value |
| Age (years), mean (SD) | 41.78 (7.90) | 43.42 (8.72) | 40.47 (7.21) | .35a |
| Female, n (%) | 9 (33) | 6 (50) | 3 (20) | .22b |
| BMI (kg/m2), mean (SD) | 21.65 (2.60) | 21.18 (2.54) | 22.03 (2.67) | .40a |
| BDI-IIc, mean (SD) | 6.51 (5.13) | 6.92 (4.94) | 6.20 (5.42) | .72a |
| BDI-II >13, n (%) | 4 (15) | 2 (17) | 2 (13) | .99b |
| STAI Y-1d, mean (SD) | 39.78 (11.05) | 38.75 (11.31) | 40.60 (11.17) | .67a |
| STAI Y-2e, mean (SD) | 40.74 (10.28) | 38.67 (8.50) | 41.20 (11.69) | .52a |
| PSQIf, mean (SD) | 4.73 (2.16) | 4.75 (2.05) | 4.71 (2.33) | .97a |
| Swg, mean (SD) | 6 h 18 min (1 h 4 min) | 6 h 20 min (1 h 18 min) | 6 h 16 min (53 min) | .88a |
| Sfh, mean (SD) | 6 h 49 min (1 h 23 min) | 6 h 35 min (1 h 23 min) | 7 h 00 min (1 h 25 min) | .45a |
aWelch t test.
bFisher exact test.
cBDI-II: Beck Depression Inventory second edition.
dSTAI Y-1: State Anxiety Scale.
eSTAI Y-2: Trait Anxiety Scale.
fPSQI: Pittsburgh Sleep Quality Index.
gSw: sleep duration on work days.
hSf: sleep duration on free days.
Statistical Properties of Sleep Variables
We examined group differences in the sleep variables such as cumulative sleep debt, sleep duration, and midpoint of sleep during the trial period. The data of 5 of the 27 (18%) participants were excluded from the analyses because of physical activity measurement failures (Figure 2). Thus, the data from 11 participants in the control group (mean age 43.3, SD 9.1 years; 6 males and 5 females) and 11 participants in the feedback group (mean age 41.3, SD 7.41 years; 9 males and 2 females) were analyzed.
Figure 3 presents the spaghetti plots of the computed sleep variables for all participants during the trial period. The Welch t test and Levene test for equality of variances indicated that there was no significant group difference in cumulative sleep debt per participant, t17.32=0.64, P=.53; F1,20=0.15, P=.70.
Figure 3.

Spaghetti plots of the estimated cumulative sleep debt (top panels), sleep duration (middle panels), and midpoint of sleep (bottom panels) per participant across the trial period. The left and right panels indicate the time series of the sleep variables for the control group and the feedback group, respectively.
We subsequently examined the group differences in the daily trend, baseline level, and within-individual residuals for sleep duration and midpoint of sleep using the hierarchical Bayesian model. The within-individual residuals for the midpoint of sleep in the feedback group were significantly smaller than those in the control group (expected a posteriori for the difference: −15, 95% CI −26 to −4 min; Table 2). This was also the case for the within-individual residuals for bedtime (−18, 95% CI−31 to −4 min; Multimedia Appendix 4). Both groups showed no significant slope of the day in terms of sleep duration (control group: 0 95% CI −3 to 3 min; feedback group: 1, 95% CI −3 to 1 min) or midpoint of sleep (control group: −1, 95% CI −4 to 1 min; feedback group: 1, 95% CI −1 to 3 min).
Table 2.
Results of the hierarchical Bayesian model for sleep duration and midpoint of sleep.
|
|
Control group | Feedback group | Difference | ||||||
|
|
EAPa (SD)b | 95% CIc | EAP (SD) | 95% CI | EAP (SD) | 95% CI | |||
| Sleep durationd | |||||||||
|
|
Intercept | 7 h 33 min (26 min) | 6 h 42 min to 8 h 23 min | 7 h 31 min (33 min) | 6 h 27 min to 8 h 36 min | −1 min (31 min) | −1 h 2 min to 58 min | ||
|
|
Day | 0 min (1 min) | −3 min to 3 min | 1 min (1 min) | −3 min to 1 min | −1 min (2 min) | −4 min to 3 min | ||
|
|
σ0e | 48 min (11 min) | 29 min to 1 h 14 min | 48 min (11 min) | 29 min to 1 h 14 min | N/Af | N/A | ||
|
|
σy | 1 h 13 min (5 min) | 1 h 4 min to 1 h 23 min | 1 h 13 min (6 min) | 1 h 3 min to 1 h 26 min | 0 min (8 min) | −14 min to 16 min | ||
| Midpoint of sleepd | |||||||||
|
|
Intercept | 3:30 (21 min) | 2:48 to 4:12 | 3:34 (26 min) | 2:44 to 4:26 | 4 min (24 min) | −42 min to 52 min | ||
|
|
Day | −1 min (1 min) | −4 min to 1 min | 1 min (1 min) | −1 min to 3 min | 2 min (1 min) | 0 min to 5 min | ||
|
|
σ0 | 41 min (9 min) | 27 min to 1 h 1 min | 41 min (9 min) | 27 min to 1 h 1 min | N/A | N/A | ||
|
|
σy | 1 h 1 min (4 min) | 53 min to 1 h 9 min | 46 min (4 min) | 39 min to 54 min | −15 min (5 min)g | −26 min to −4 min | ||
aEAP: expected a posteriori (expected value of the posterior distribution).
bSD of the posterior distribution.
cCI: credible interval.
dThe models were run after controlling for age and sex.
eThe difference in the interindividual variability for the intercept (σ0) was not computed because σ0 was assumed to be equal between groups.
fN/A: not applicable.
gItalicized values denote statistically significant group effects, at a 95% CI.
Self-reported Work Performance Assessment
We examined the group differences in daily work performance during the trial period using 307 EMA records obtained from 27 participants (Figure 4). We examined the statistical properties of daily work performance by using the statistical model used to analyze the sleep variables. However, there were no significant differences between the groups (Table 3). When comparing the HPQ score before and after the intervention using a 2-way repeated ANOVA, the main effects of group, F1,25=0.39, P=.54, and time, F1,25=0.01, P=.94, and their interaction, F1,25=0.05, P=.83, were not significant.
Figure 4.

Spaghetti plots of the daily work performance recorded using ecological momentary assessment per participant across the trial period. The left and right panels indicate the time series of the work performance for the control group and the feedback group, respectively.
Table 3.
Results of the hierarchical Bayesian model for daily work performance.
|
|
Control | Feedback | Difference | ||||||||||
|
|
EAPa (SD)b | 95% CIc | EAP (SD) | 95% CI | EAP (SD) | 95% CI | |||||||
| Daily work performanced | |||||||||||||
|
|
Intercept | 57.59 (6.67) | 44.60 to 70.54 | 61.45 (8.77) | 44.24 to 78.82 | 3.85 (8.01) | −11.92 to 19.84 | ||||||
|
|
Day | 0.32 (0.22) | −0.11 to 0.75 | 0.08 (0.17) | −0.26 to 0.41 | −0.24 (0.27) | −0.77 to 0.29 | ||||||
|
|
σ0e | 17.06 (2.89) | 12.38 to 23.54 | 17.06 (2.89) | 12.38 to 23.54 | N/Af | N/A | ||||||
|
|
σy | 13.28 (0.88) | 11.68 to 15.14 | 12.62 (0.72) | 11.31 to 14.12 | −0.66 (1.14) | −2.94 to 1.50 | ||||||
aEAP: expected a posteriori.
bSD of the posterior distribution.
cCI: credible interval.
dThe models were run after controlling for age and sex.
eThe difference in the interindividual variability for the intercept (σ0) was not computed because σ0 was assumed to be equal between groups.
fN/A: not applicable.
Diurnal Slopes for EMA Scores
The recorded EMA scores of 27 participants (760 records) were used to examine the diurnal slopes in momentary mood and physical symptoms (Figure 2). The linear mixed effect model results showed significant interaction effects between group and time in physical symptoms (fatigue, P=.002; sleepiness, P<.001; and neck and shoulder stiffness, P<.001; Table 4). In addition, a multiple comparison test with Tukey correction showed that the EMA scores of physical symptoms at wake-up time were significantly lower than those at bedtime in the feedback group (fatigue, sleepiness, and neck and shoulder stiffness, P<.001). In the control group, a significant difference between wake-up time and bedtime was observed only for fatigue (P<.001; Figure 5).
Table 4.
Results of the linear mixed effect model for mood and physical symptoms.
| Mood and physical symptomsa | Coefficient (SE) | Dfb | P value | ||||
| Depressive mood | |||||||
|
|
Interceptc | 41.27 (5.56) | 23.28 | <.001 | |||
|
|
Group | −9.87 (6.61) | 23.42 | .15 | |||
|
|
Time | −0.35 (1.10) | 731.32 | .75 | |||
|
|
Group×Time | 0.74 (1.51) | 731.6 | .63 | |||
| Anxiety | |||||||
|
|
Interceptc | 35.75 (7.42) | 23.31 | <.001 | |||
|
|
Group | −16.89 (8.82) | 23.46 | .07 | |||
|
|
Time | −1.29 (1.56) | 731.36 | .41 | |||
|
|
Group×Time | 3.03 (2.14) | 731.66 | .16 | |||
| Stress | |||||||
|
|
Intercept | 47.07 (8.02) | 23.42 | <.001 | |||
|
|
Group | −18.66 (9.54) | 23.6 | .06 | |||
|
|
Time | 2.49 (1.80) | 731.46 | .17 | |||
|
|
Group×Time | 0.46 (2.47) | 731.82 | .85 | |||
| Fatigue | |||||||
|
|
Intercept | 35.22 (7.24) | 23.72 | <.001 d | |||
|
|
Group | −16.47 (8.62) | 24.03 | .07 | |||
|
|
Time | 16.07 (2.14) | 731.78 | <.001 | |||
|
|
Group×Time | 9.31 (2.96) | 732.39 | .002 | |||
| Sleepiness | |||||||
|
|
Intercept | 55.75 (7.20) | 24.08 | <.001 | |||
|
|
Group | −9.81 (8.58) | 24.51 | .26 | |||
|
|
Time | 1.27 (2.49) | 732.14 | .61 | |||
|
|
Group×Time | 17.70 (3.42) | 732.96 | <.001 | |||
| Neck and shoulder stiffness | |||||||
|
|
Intercept | 43.33 (9.59) | 23.27 | <.001 | |||
|
|
Group | −12.99 (11.40) | 23.37 | .27 | |||
|
|
Time | −2.51 (1.64) | 731.3 | .13 | |||
|
|
Group×Time | 8.46 (2.26) | 731.51 | <.001 | |||
aThe df values correspond to the denominator df in ANOVA model.
bThe effects of group (control vs feedback group) and time (wake-up time vs bedtime) were assumed to be fixed effects, and those of individuals were assumed to be random effects.
cThe control group and wake-up time were used as the reference categories for each variable; thus, the intercept indicates the expected EMA score of moods or physical symptoms for the control group during the wake-up time.
dItalicized values denote statistically significant interaction effects. All models were run by controlling for age and sex.
Figure 5.

Average ecological momentary assessment scores for fatigue, sleepiness, and neck and shoulder stiffness at bedtime and wake-up time in the control group and the feedback group. The error bars indicate the SE per group.
Discussion
Principal Findings
We explored the effects of personalized feedback messages regarding the current sleep status on habitual sleep behavior and momentary mood and physical symptoms in Japanese office workers, using a unique cloud-based HIT system that included a web-based wearable activity monitor and a smartphone app. Specifically, we focused on group differences in the statistical properties of sleep variables and within-day momentary symptoms during the trial period. We found that the within-individual residuals for sleep timing were significantly smaller in the feedback group than in the control group. In addition, the diurnal slopes for physical symptoms (sleepiness, fatigue, and neck and shoulder stiffness) differed significantly between the feedback and control groups, largely because of better physical symptom scores in the feedback group at wake-up time. This is the first mHealth study to implement push-type sleep feedback based on objective measurements and to demonstrate improved sleep status and momentary symptoms associated with receiving the feedback message. The findings in this study suggest that objective push-type feedback messages may promote sleep self-management and solve habitual sleep behavior problems, despite the minor inconvenience.
Several mHealth apps have been developed for treating sleep disturbances such as insomnia [30,31], but the objective sleep feedback function has not been implemented in these apps. While users of consumer-grade wearable devices can take advantage of objective sleep measurements, these are regarded as pull-type interventions, as these devices require the user to actively access an app to receive feedback, which can sometimes be burdensome. Connecting mHealth apps with wearable sensing devices and sending objective push-type sleep feedback may be a feature to consider when developing or updating mHealth apps that target sleep disturbance.
Comparison With Previous Work
The within-individual residuals in sleep variables examined in this study can represent how sleep behavior varies across days, which is commonly referred to as intraindividual variability [22]. Recently, the stability of habitual sleep behavior has been considered a critical factor for physical and mental health, as previous studies have indicated that greater intraindividual variability in sleep behavior is associated with worse medical health conditions [25] and poorer psychological well-being [26]. In our study, participants may have attempted to improve their sleep habits by adopting strategies to stabilize their sleep timing (specifically their bedtime); for example, by not staying up late excessively. This inference is supported by evidence of a significant group difference in the within-individual residuals at bedtime but not in wake-up time. Similar results were reported by Murawski et al [40] who found improvement in the variability of sleep timing after the 3-month intervention. Given the fact that our survey period was relatively short, it is speculated that the improvement in sleep variability is an initial change caused by improved awareness of habitual sleep behaviors. Especially in modern industrial societies, the sleep-wake cycle adhering to social schedules, rather than endogenous circadian rhythms, leads to exposure to bright light at significantly different times from the natural environment. This causes disturbances in sleep and circadian rhythms, such as circadian misalignment [59] and social jet lag [60,61], which are linked to future health problems. Thus, the findings of this study suggest that sending personalized sleep feedback messages may potentially contribute to the primary prevention of physical and mental health problems as well as the improvement of the sleep-wake cycle.
Improvements in physical symptoms and stabilization of sleep timing were simultaneously observed in the feedback group, suggesting the covariant relationship between them. Indeed, previous studies have indicated that individuals with greater intraindividual variability in sleep timing and sleep duration show more dysregulated biomarkers related to endogenous circadian rhythm [23] and inflammatory functions [24], which can influence diurnal symptoms including sleepiness and fatigue. Therefore, improved physical symptoms at wake-up time in the feedback group may have been caused by stabilized sleep timing, mediated by regulated physiological systems. Thus, it is possible that improved physical symptoms were observed as a short-term effect or proximal outcome of the interventions that stabilized sleep timing and, by extension, functioned as an incentive to improve sleep habits and adjust daytime activities. However, inconsistent results have been reported in previous studies investigating the relationship between sleep and physical symptoms. In a cross-sectional study, there was no relationship between sleep variability and daytime fatigue and sleepiness [62], whereas daytime sleepiness was reduced among university students who were instructed to stabilize their sleep-wake schedule experimentally [63]. These mixed results may be due to the use of survey designs that evaluate symptoms at a single time point. In contrast, we measured physical symptoms several times per day using the EMA technique, with finer temporal resolution than in previous studies, and with ecological validity, resulting in the discovery of improved physical symptoms at wake-up time in the feedback group. When acquiring physical symptom data, the timing of the measurements can also be an important factor.
A previous study demonstrated that the use of wearable devices improved sleep duration in a healthy population [29]. However, the hierarchical Bayesian model demonstrated that the slope of day for sleep duration and midpoint of sleep were not statistically significant; thus, we did not find an improvement in sleep duration or midpoint of sleep by using only sleep feedback. This discrepancy may be due to the prompts of feedback messages. During the survey period, participants’ sleep debt did not accumulate much, and they seemed to receive messages indicating that their sleep status was better. Under such circumstances, they might have attempted to maintain their sleep status by stabilizing their sleep-wake cycle rather than to improve their sleep duration or sleep timing. In future studies, it will be necessary to provide further support for prolonging sleep duration and advancing sleep timing, in addition to an objective sleep feedback message. Improvements in sleep duration and timing can also be beneficial to daytime functions, such as momentary moods and work performance, which were not improved in this study.
Future Directions
The HIT app is primarily designed for collecting multidimensional data in daily life, unlike mHealth apps developed for treating sleep disturbance. Therefore, in the HIT app, the functions useful for improving sleep disturbances are limited to objective feedback messages, while other apps offer several support functions, such as psychoeducation, sleep hygiene, and data visualization [30]. It is possible to improve sleep duration and timing by incorporating additional intervention options into the HIT app. Behavioral instructions to build sufficient sleep pressure at night are an example of additional support. In the treatment of patients with insomnia, sleep restriction therapy, which induces mild sleep deprivation to build homeostatic sleep pressure, is used, and existing mHealth studies incorporating sleep restriction therapy demonstrate a significant improvement in insomnia severity and sleep efficacy [35,64,65]. Interventions that build sufficient homeostatic sleep pressure as part of daily living, for example, exercising in the evening and avoiding long naps, may improve sleep duration and daytime functions, including work performance. Other interventions include behavioral coordination that works on the endogenous circadian rhythm; for example, adjusting the timing of food intake and avoiding exposure to bright light before bedtime. Such expansions can facilitate the control of habitual sleep timing and enhance the applicability of an IoT system with mobile devices for the treatment of various sleep disorders. Measuring, integrating, and using multidimensional information, including environmental and behavioral data, requires additional research. Simultaneously, integrative health care information systems, such as an HIT system, may provide a solution and expand intervention options, facilitating the verification of their effectiveness.
Limitations
This study had several limitations. First, the small number of participants were recruited from a life insurance company in Japan, and the social schedules of participants appeared similar, limiting the generalizability of the results. Indeed, work-related factors, including occupation, job stress, work hours, shift work, and physically demanding work, are associated with habitual sleep duration and sleep quality [66-68], suggesting that sleep habits may differ by occupation. Thus, a representative study including various occupations and lifestyles is required to ensure generalizability of the findings of this study.
Second, in this study, the exclusive computational method estimating sleep debt was introduced by summing the differences between the estimated and expected sleep duration. Although similar methods have been used to estimate sleep debt in other studies (the difference between self-reported sleep need and sleep duration on weekdays) [69,70], sleep debt computed using these methods may not reflect the neurobehavioral impairment caused by chronic sleep loss commonly observed in the experimental condition [71,72]. Initially, we adopted this definition with the aim of having participants plan their daily activities to improve the status of sleep insufficiency, but it could be possible that actual sleep debt was not accurately estimated. Therefore, a reliable method to estimate current sleep status should be developed and used in future studies. Especially, combining EMA techniques and machine learning methods is expected to provide reliable sleep measurements in daily life. For instance, a recent study reported that machine learning techniques could estimate daily sleep quality by using complex life data obtained from EMA questionnaires [73]. Collecting and integrating multidimensional information would be meaningful not only in understanding the covariant associations of sleep behavior with daytime symptoms but also for developing novel sleep measurements.
Finally, participants could identify the group they were assigned to because only the participants in the feedback group received feedback messages at 9 AM. Considering that physical symptoms were measured using self-report evaluations, EMA recordings were affected by cognitive biases such as the Hawthorne effect (the inclination of people who participate in an experimental study to change or improve their behavior only because it is being studied and not because of changes in the experimental stimulus). Optimizing the study design would help clarify this point. For example, by sending intervention messages that are not related to habitual sleep behavior to participants in the control group, we can determine whether the finding is based on a specific response to sleep feedback messages. In addition, implementing a microrandomized trial [74], which is equivalent to a within-individual randomized controlled trial, could also be helpful in investigating the effectiveness of the interventions. By randomizing whether feedback messages are sent, we could examine the causal relationships between sleep behaviors and daytime functions.
Conclusions
We conducted an mHealth trial with office workers and demonstrated that objective push-type sleep feedback stabilizes sleep timing and improves physical symptoms at wake-up time. However, we did not find evidence of prolonged sleep duration, advanced sleep timing, or improved work performance. Future research should incorporate specific behavioral instructions intended to improve sleep duration and sleep timing with the current protocol and investigate behavioral instruction effectiveness by integrating and using multidimensional information collected as part of daily life.
Acknowledgments
The authors would like to thank the director who afforded them the opportunity to conduct this study at the organization in which the participants work. This study was supported in part by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology, Japan, under grant 20H00569 and grant 17H00878, and Japan Science of Technology Agency Precursory Research for Embryonic Science and Technology grant JPMJPR19J3, Japan.
Abbreviations
- BDI-II
Beck Depression Inventory second edition
- BLE
Bluetooth Low Energy
- CI
credible interval
- EMA
ecological momentary assessment
- HIT
health care Internet of Things
- HPQ
Health and Work Performance Questionnaire
- IoT
Internet of Things
- mHealth
mobile health
- PSQI
Pittsburgh Sleep Quality Index
- SPF
Sleep Probability Function
- STAI
State-Trait Anxiety Inventory
Screenshots of the health care Internet of Things app.
Validity of the Sciencenet activity monitor.
Sleep hygiene guide.
Additional analyses of the statistical properties of sleep variables.
Data Availability
The participants of this study did not agree to their data being shared publicly; therefore, supporting data are not available.
Footnotes
Authors' Contributions: TN, KY, AK, and YY designed the study. HT, KS, and AK collected data. HT performed data analysis and wrote the first draft of the manuscript. All authors critically reviewed and approved the final version of the manuscript.
Conflicts of Interest: None declared.
References
- 1.Becker S, Miron-Shatz T, Schumacher N, Krocza J, Diamantidis C, Albrecht U. mHealth 2.0: experiences, possibilities, and perspectives. JMIR Mhealth Uhealth. 2014 May 16;2(2):e24. doi: 10.2196/mhealth.3328. https://mhealth.jmir.org/2014/2/e24/ v2i2e24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kumar S, Nilsen WJ, Abernethy A, Atienza A, Patrick K, Pavel M, Riley WT, Shar A, Spring B, Spruijt-Metz D, Hedeker D, Honavar V, Kravitz R, Lefebvre RC, Mohr DC, Murphy SA, Quinn C, Shusterman V, Swendeman D. Mobile health technology evaluation: the mHealth evidence workshop. Am J Prev Med. 2013 Aug;45(2):228–36. doi: 10.1016/j.amepre.2013.03.017. https://europepmc.org/abstract/MED/23867031 .S0749-3797(13)00277-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nikolova S. Top 3 therapy fields with the best market potential for digital health apps. Research2Guidance. 2017. [2021-08-01]. https://research2guidance.com/top-3-therapy-fields-with-the-best-market-potential-for-digital-health-apps .
- 4.Ganesan AN, Louise J, Horsfall M, Bilsborough SA, Hendriks J, McGavigan AD, Selvanayagam JB, Chew DP. International mobile-health intervention on physical activity, sitting, and weight: the Stepathlon cardiovascular health study. J Am Coll Cardiol. 2016 May 31;67(21):2453–63. doi: 10.1016/j.jacc.2016.03.472. https://linkinghub.elsevier.com/retrieve/pii/S0735-1097(16)01525-4 .S0735-1097(16)01525-4 [DOI] [PubMed] [Google Scholar]
- 5.Patel MS, Volpp KG, Rosin R, Bellamy SL, Small DS, Heuer J, Sproat S, Hyson C, Haff N, Lee SM, Wesby L, Hoffer K, Shuttleworth D, Taylor DH, Hilbert V, Zhu J, Yang L, Wang X, Asch DA. A randomized, controlled trial of lottery-based financial incentives to increase physical activity among overweight and obese adults. Am J Health Promot. 2018 Sep;32(7):1568–75. doi: 10.1177/0890117118758932. [DOI] [PubMed] [Google Scholar]
- 6.Klasnja P, Smith S, Seewald NJ, Lee A, Hall K, Luers B, Hekler EB, Murphy SA. Efficacy of contextually tailored suggestions for physical activity: a micro-randomized optimization trial of HeartSteps. Ann Behav Med. 2019 May 03;53(6):573–82. doi: 10.1093/abm/kay067. https://europepmc.org/abstract/MED/30192907 .5091257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carrasco-Hernandez L, Jódar-Sánchez F, Núñez-Benjumea F, Moreno Conde J, Mesa González M, Civit-Balcells A, Hors-Fraile S, Parra-Calderón CL, Bamidis PD, Ortega-Ruiz F. A mobile health solution complementing psychopharmacology-supported smoking cessation: randomized controlled trial. JMIR Mhealth Uhealth. 2020 Apr 27;8(4):e17530. doi: 10.2196/17530. https://mhealth.jmir.org/2020/4/e17530/ v8i4e17530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ubhi HK, Michie S, Kotz D, Wong WC, West R. A mobile app to aid smoking cessation: preliminary evaluation of SmokeFree28. J Med Internet Res. 2015 Jan 16;17(1):e17. doi: 10.2196/jmir.3479. https://www.jmir.org/2015/1/e17/ v17i1e17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tighe J, Shand F, Ridani R, Mackinnon A, De La Mata N, Christensen H. Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: a pilot randomised controlled trial. BMJ Open. 2017 Jan 27;7(1):e013518. doi: 10.1136/bmjopen-2016-013518. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=28132007 .bmjopen-2016-013518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shan Z, Ma H, Xie M, Yan P, Guo Y, Bao W, Rong Y, Jackson CL, Hu FB, Liu L. Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care. 2015 Mar;38(3):529–37. doi: 10.2337/dc14-2073.38/3/529 [DOI] [PubMed] [Google Scholar]
- 11.Cappuccio FP, Cooper D, D'Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J. 2011 Jun;32(12):1484–92. doi: 10.1093/eurheartj/ehr007.ehr007 [DOI] [PubMed] [Google Scholar]
- 12.Zhai L, Zhang H, Zhang D. Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress Anxiety. 2015 Sep;32(9):664–70. doi: 10.1002/da.22386. [DOI] [PubMed] [Google Scholar]
- 13.Chami HA, Ghandour B, Isma'eel H, Nasreddine L, Nasrallah M, Tamim H. Sleepless in Beirut: sleep duration and associated subjective sleep insufficiency, daytime fatigue, and sleep debt in an urban environment. Sleep Breath. 2020 Mar;24(1):357–67. doi: 10.1007/s11325-019-01833-3.10.1007/s11325-019-01833-3 [DOI] [PubMed] [Google Scholar]
- 14.Alves FR, de Souza EA, de França Ferreira LG, de Oliveira Vilar Neto J, de Bruin VM, de Bruin PF. Sleep duration and daytime sleepiness in a large sample of Brazilian high school adolescents. Sleep Med. 2020 Feb;66:207–15. doi: 10.1016/j.sleep.2019.08.019.S1389-9457(19)30305-3 [DOI] [PubMed] [Google Scholar]
- 15.Ishibashi Y, Shimura A. Association between work productivity and sleep health: a cross-sectional study in Japan. Sleep Health. 2020 Jun;6(3):270–6. doi: 10.1016/j.sleh.2020.02.016.S2352-7218(20)30082-6 [DOI] [PubMed] [Google Scholar]
- 16.Magee CA, Caputi P, Iverson DC. Relationships between self-rated health, quality of life and sleep duration in middle aged and elderly Australians. Sleep Med. 2011 Apr;12(4):346–50. doi: 10.1016/j.sleep.2010.09.013.S1389-9457(11)00024-4 [DOI] [PubMed] [Google Scholar]
- 17.Sasaki N, Fujiwara S, Yamashita H, Ozono R, Monzen Y, Teramen K, Kihara Y. Association between obesity and self-reported sleep duration variability, sleep timing, and age in the Japanese population. Obes Res Clin Pract. 2018;12(2):187–94. doi: 10.1016/j.orcp.2017.10.008.S1871-403X(17)30120-5 [DOI] [PubMed] [Google Scholar]
- 18.Yan B, Li R, Li J, Jin X, Gao F, Gao Y, Ren J, Zhang J, Wang X, Wang G. Sleep timing may predict congestive heart failure: a community-based cohort study. J Am Heart Assoc. 2021 Mar 16;10(6):e018385. doi: 10.1161/JAHA.120.018385. https://www.ahajournals.org/doi/10.1161/JAHA.120.018385?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Reutrakul S, Siwasaranond N, Nimitphong H, Saetung S, Chirakalwasan N, Ongphiphadhanakul B, Thakkinstian A, Hood MM, Crowley SJ. Relationships among sleep timing, sleep duration and glycemic control in type 2 diabetes in Thailand. Chronobiol Int. 2015;32(10):1469–76. doi: 10.3109/07420528.2015.1105812. [DOI] [PubMed] [Google Scholar]
- 20.Levandovski R, Dantas G, Fernandes LC, Caumo W, Torres I, Roenneberg T, Hidalgo MP, Allebrandt KV. Depression scores associate with chronotype and social jetlag in a rural population. Chronobiol Int. 2011 Nov;28(9):771–8. doi: 10.3109/07420528.2011.602445. [DOI] [PubMed] [Google Scholar]
- 21.de Souza CM, Hidalgo MP. Midpoint of sleep on school days is associated with depression among adolescents. Chronobiol Int. 2014 Mar;31(2):199–205. doi: 10.3109/07420528.2013.838575. [DOI] [PubMed] [Google Scholar]
- 22.Bei B, Wiley JF, Trinder J, Manber R. Beyond the mean: a systematic review on the correlates of daily intraindividual variability of sleep/wake patterns. Sleep Med Rev. 2016 Aug;28:108–24. doi: 10.1016/j.smrv.2015.06.003. https://linkinghub.elsevier.com/retrieve/pii/S1087-0792(15)00090-8 .S1087-0792(15)00090-8 [DOI] [PubMed] [Google Scholar]
- 23.Bei B, Seeman TE, Carroll JE, Wiley JF. Sleep and physiological dysregulation: a closer look at sleep intraindividual variability. Sleep. 2017 Sep 01;40(9):zsx109. doi: 10.1093/sleep/zsx109. https://europepmc.org/abstract/MED/28651371 .3885856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Okun ML, Reynolds CF, Buysse DJ, Monk TH, Mazumdar S, Begley A, Hall M. Sleep variability, health-related practices, and inflammatory markers in a community dwelling sample of older adults. Psychosom Med. 2011;73(2):142–50. doi: 10.1097/PSY.0b013e3182020d08. https://europepmc.org/abstract/MED/21097658 .PSY.0b013e3182020d08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Slavish DC, Taylor DJ, Lichstein KL. Intraindividual variability in sleep and comorbid medical and mental health conditions. Sleep. 2019 Jun 11;42(6):zsz052. doi: 10.1093/sleep/zsz052. https://europepmc.org/abstract/MED/30843059 .5370458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lemola S, Ledermann T, Friedman EM. Variability of sleep duration is related to subjective sleep quality and subjective well-being: an actigraphy study. PLoS One. 2013 Aug 14;8(8):e71292. doi: 10.1371/journal.pone.0071292. https://dx.plos.org/10.1371/journal.pone.0071292 .PONE-D-12-32105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Perez-Pozuelo I, Zhai B, Palotti J, Mall R, Aupetit M, Garcia-Gomez JM, Taheri S, Guan Y, Fernandez-Luque L. The future of sleep health: a data-driven revolution in sleep science and medicine. NPJ Digit Med. 2020 Mar 23;3:42. doi: 10.1038/s41746-020-0244-4. doi: 10.1038/s41746-020-0244-4.244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tobin SY, Williams PG, Baron KG, Halliday TM, Depner CM. Challenges and opportunities for applying wearable technology to sleep. Sleep Med Clin. 2021 Dec;16(4):607–18. doi: 10.1016/j.jsmc.2021.07.002.S1556-407X(21)00054-0 [DOI] [PubMed] [Google Scholar]
- 29.Crowley O, Pugliese L, Kachnowski S. The impact of wearable device enabled health initiative on physical activity and sleep. Cureus. 2016 Oct 11;8(10):e825. doi: 10.7759/cureus.825. https://europepmc.org/abstract/MED/27882272 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Aji M, Gordon C, Stratton E, Calvo RA, Bartlett D, Grunstein R, Glozier N. Framework for the design engineering and clinical implementation and evaluation of mHealth apps for sleep disturbance: systematic review. J Med Internet Res. 2021 Feb 17;23(2):e24607. doi: 10.2196/24607. https://www.jmir.org/2021/2/e24607/ v23i2e24607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Arroyo AC, Zawadzki MJ. The implementation of behavior change techniques in mHealth apps for sleep: systematic review. JMIR Mhealth Uhealth. 2022 Apr 04;10(4):e33527. doi: 10.2196/33527. https://mhealth.jmir.org/2022/4/e33527/ v10i4e33527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Simon L, Reimann J, Steubl LS, Stach M, Spiegelhalder K, Sander LB, Baumeister H, Messner E, Terhorst Y. Help for insomnia from the app store? A standardized rating of mobile health applications claiming to target insomnia. J Sleep Res (forthcoming) 2022 May 27;:e13642. doi: 10.1111/jsr.13642. [DOI] [PubMed] [Google Scholar]
- 33.Pulantara IW, Parmanto B, Germain A. Development of a just-in-time adaptive mHealth intervention for insomnia: usability study. JMIR Hum Factors. 2018 May 17;5(2):e21. doi: 10.2196/humanfactors.8905. https://humanfactors.jmir.org/2018/2/e21/ v5i2e21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pulantara IW, Parmanto B, Germain A. Clinical feasibility of a just-in-time adaptive intervention app (iREST) as a behavioral sleep treatment in a military population: feasibility comparative effectiveness study. J Med Internet Res. 2018 Dec 07;20(12):e10124. doi: 10.2196/10124. https://www.jmir.org/2018/12/e10124/ v20i12e10124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Horsch CH, Lancee J, Griffioen-Both F, Spruit S, Fitrianie S, Neerincx MA, Beun RJ, Brinkman WP. Mobile phone-delivered cognitive behavioral therapy for insomnia: a randomized waitlist controlled trial. J Med Internet Res. 2017 Apr 11;19(4):e70. doi: 10.2196/jmir.6524. https://www.jmir.org/2017/4/e70/ v19i4e70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kuhn E, Miller KE, Puran D, Wielgosz J, YorkWilliams SL, Owen JE, Jaworski BK, Hallenbeck HW, McCaslin SE, Taylor KL. A pilot randomized controlled trial of the insomnia coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022 May;53(3):440–57. doi: 10.1016/j.beth.2021.11.003.S0005-7894(21)00133-7 [DOI] [PubMed] [Google Scholar]
- 37.Glazer Baron K, Culnan E, Duffecy J, Berendson M, Cheung Mason I, Lattie E, Manalo N. How are consumer sleep technology data being used to deliver behavioral sleep medicine interventions? A systematic review. Behav Sleep Med. 2022;20(2):173–87. doi: 10.1080/15402002.2021.1898397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kang SG, Kang JM, Cho SJ, Ko KP, Lee YJ, Lee HJ, Kim L, Winkelman JW. Cognitive behavioral therapy using a mobile application synchronizable with wearable devices for insomnia treatment: a pilot study. J Clin Sleep Med. 2017 Apr 15;13(4):633–40. doi: 10.5664/jcsm.6564. doi: 10.5664/jcsm.6564.jc-00376-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Reilly ED, Robinson SA, Petrakis BA, Kuhn E, Pigeon WR, Wiener RS, McInnes DK, Quigley KS. Mobile app use for insomnia self-management: pilot findings on sleep outcomes in veterans. Interact J Med Res. 2019 Jul 24;8(3):e12408. doi: 10.2196/12408. https://www.i-jmr.org/2019/3/e12408/ v8i3e12408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Murawski B, Plotnikoff RC, Rayward AT, Oldmeadow C, Vandelanotte C, Brown WJ, Duncan MJ. Efficacy of an m-health physical activity and sleep health intervention for adults: a randomized waitlist-controlled trial. Am J Prev Med. 2019 Oct;57(4):503–14. doi: 10.1016/j.amepre.2019.05.009.S0749-3797(19)30241-7 [DOI] [PubMed] [Google Scholar]
- 41.Stone AA, Shiffman S. Ecological momentary assessment (EMA) in behavioral medicine. Ann Behav Med. 1994;16(3):199–202. doi: 10.1093/abm/16.3.199. [DOI] [Google Scholar]
- 42.Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol. 2008;4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415. [DOI] [PubMed] [Google Scholar]
- 43.Qian K, Koike T, Nakamura T, Schuller B, Yamamoto Y. Learning multimodal representations for drowsiness detection. IEEE Trans Intell Transport Syst. 2022 Aug;23(8):11539–48. doi: 10.1109/tits.2021.3105326. [DOI] [Google Scholar]
- 44.Beck AT, Steer RA, Brown GK. BDI-II: Beck Depression Inventory. 2nd edition. San Antonio, TX, USA: Psychological Corporation; 1996. [Google Scholar]
- 45.Kojima M, Furukawa TA, Takahashi H, Kawai M, Nagaya T, Tokudome S. Cross-cultural validation of the Beck Depression Inventory-II in Japan. Psychiatry Res. 2002 Jul 31;110(3):291–9. doi: 10.1016/s0165-1781(02)00106-3.S0165178102001063 [DOI] [PubMed] [Google Scholar]
- 46.Hidano T, Fukuhara M, Iwawaki S, Soga S, Spielberger CD. New STAI for the State-Trait Anxiety Inventory-Form JYZ. Tokyo, Japan: Jitsumu Kyouiku Press; 2000. [Google Scholar]
- 47.Buysse DJ, Reynolds 3rd CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989 May;28(2):193–213. doi: 10.1016/0165-1781(89)90047-4.0165-1781(89)90047-4 [DOI] [PubMed] [Google Scholar]
- 48.Doi Y, Minowa M, Uchiyama M, Okawa M, Kim K, Shibui K, Kamei Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000 Dec 27;97(2-3):165–72. doi: 10.1016/s0165-1781(00)00232-8.S0165178100002328 [DOI] [PubMed] [Google Scholar]
- 49.Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016 Feb;25:52–73. doi: 10.1016/j.smrv.2015.01.009.S1087-0792(15)00021-0 [DOI] [PubMed] [Google Scholar]
- 50.Kessler RC, Barber C, Beck A, Berglund P, Cleary PD, McKenas D, Pronk N, Simon G, Stang P, Ustun TB, Wang P. The World Health Organization health and work performance questionnaire (HPQ) J Occup Environ Med. 2003 Feb;45(2):156–74. doi: 10.1097/01.jom.0000052967.43131.51. [DOI] [PubMed] [Google Scholar]
- 51.Kawakami N, Inoue A, Tsuchiya M, Watanabe K, Imamura K, Iida M, Nishi D. Construct validity and test-retest reliability of the World Mental Health Japan version of the World Health Organization Health and Work Performance Questionnaire Short Version: a preliminary study. Ind Health. 2020 Aug 07;58(4):375–87. doi: 10.2486/indhealth.2019-0090. doi: 10.2486/indhealth.2019-0090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Fukui I. The Depression and Anxiety Mood Scale (DAMS): scale development and validation. Jpn J Behav Ther. 1997 Sep;23(2):83–93. [Google Scholar]
- 53.Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003 May 01;26(3):342–92. doi: 10.1093/sleep/26.3.342. [DOI] [PubMed] [Google Scholar]
- 54.Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC. Automatic sleep/wake identification from wrist activity. Sleep. 1992 Oct;15(5):461–9. doi: 10.1093/sleep/15.5.461. [DOI] [PubMed] [Google Scholar]
- 55.Webster JB, Kripke DF, Messin S, Mullaney DJ, Wyborney G. An activity-based sleep monitor system for ambulatory use. Sleep. 1982;5(4):389–99. doi: 10.1093/sleep/5.4.389. [DOI] [PubMed] [Google Scholar]
- 56.Carpenter B, Gelman A, Hoffman MD, Lee D, Goodrich B, Betancourt M, Brubaker M, Guo J, Li P, Riddell A. Stan: a probabilistic programming language. J Stat Soft. 2017 Jan 11;76(1):1–32. doi: 10.18637/jss.v076.i01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Kuznetsova A, Brockhoff PB, Christensen RH. lmerTest package: tests in linear mixed effects models. J Stat Soft. 2017 Dec 6;82(13):1–26. doi: 10.18637/jss.v082.i13. [DOI] [Google Scholar]
- 58.Lenth RV. Least-squares means: the R package lsmeans. J Stat Soft. 2016 Jan 29;69(1):1–33. doi: 10.18637/jss.v069.i01. [DOI] [Google Scholar]
- 59.Baron KG, Reid KJ. Circadian misalignment and health. Int Rev Psychiatry. 2014 Apr;26(2):139–54. doi: 10.3109/09540261.2014.911149. https://europepmc.org/abstract/MED/24892891 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1-2):497–509. doi: 10.1080/07420520500545979.TP463290637N5735 [DOI] [PubMed] [Google Scholar]
- 61.Roenneberg T, Pilz LK, Zerbini G, Winnebeck EC. Chronotype and social jetlag: a (self-) critical review. Biology (Basel) 2019 Jul 12;8(3):54. doi: 10.3390/biology8030054. https://www.mdpi.com/resolver?pii=biology8030054 .biology8030054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kang JH, Chen SC. Effects of an irregular bedtime schedule on sleep quality, daytime sleepiness, and fatigue among university students in Taiwan. BMC Public Health. 2009 Jul 19;9:248. doi: 10.1186/1471-2458-9-248. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-9-248 .1471-2458-9-248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Manber R, Bootzin RR, Acebo C, Carskadon MA. The effects of regularizing sleep-wake schedules on daytime sleepiness. Sleep. 1996 Jun;19(5):432–41. doi: 10.1093/sleep/19.5.432. [DOI] [PubMed] [Google Scholar]
- 64.Miller CB, Espie CA, Epstein DR, Friedman L, Morin CM, Pigeon WR, Spielman AJ, Kyle SD. The evidence base of sleep restriction therapy for treating insomnia disorder. Sleep Med Rev. 2014 Oct;18(5):415–24. doi: 10.1016/j.smrv.2014.01.006.S1087-0792(14)00016-1 [DOI] [PubMed] [Google Scholar]
- 65.Aji M, Glozier N, Bartlett D, Peters D, Calvo RA, Zheng Y, Grunstein R, Gordon C. A feasibility study of a mobile app to treat insomnia. Transl Behav Med. 2021 Mar 16;11(2):604–12. doi: 10.1093/tbm/ibaa019.5813538 [DOI] [PubMed] [Google Scholar]
- 66.Akerstedt T, Knutsson A, Westerholm P, Theorell T, Alfredsson L, Kecklund G. Sleep disturbances, work stress and work hours: a cross-sectional study. J Psychosom Res. 2002 Sep;53(3):741–8. doi: 10.1016/s0022-3999(02)00333-1.S0022399902003331 [DOI] [PubMed] [Google Scholar]
- 67.Luckhaupt SE, Tak S, Calvert GM. The prevalence of short sleep duration by industry and occupation in the National Health Interview Survey. Sleep. 2010 Feb;33(2):149–59. doi: 10.1093/sleep/33.2.149. https://europepmc.org/abstract/MED/20175398 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Shockey TM, Wheaton AG. Short sleep duration by occupation group - 29 states, 2013-2014. MMWR Morb Mortal Wkly Rep. 2017 Mar 03;66(8):207–13. doi: 10.15585/mmwr.mm6608a2. doi: 10.15585/mmwr.mm6608a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Léger D, Roscoat ED, Bayon V, Guignard R, Pâquereau J, Beck F. Short sleep in young adults: insomnia or sleep debt? Prevalence and clinical description of short sleep in a representative sample of 1004 young adults from France. Sleep Med. 2011 May;12(5):454–62. doi: 10.1016/j.sleep.2010.12.012.S1389-9457(11)00088-8 [DOI] [PubMed] [Google Scholar]
- 70.Regestein Q, Natarajan V, Pavlova M, Kawasaki S, Gleason R, Koff E. Sleep debt and depression in female college students. Psychiatry Res. 2010 Mar 30;176(1):34–9. doi: 10.1016/j.psychres.2008.11.006.S0165-1781(08)00411-3 [DOI] [PubMed] [Google Scholar]
- 71.Belenky G, Wesensten NJ, Thorne DR, Thomas ML, Sing HC, Redmond DP, Russo MB, Balkin TJ. Patterns of performance degradation and restoration during sleep restriction and subsequent recovery: a sleep dose-response study. J Sleep Res. 2003 Mar;12(1):1–12. doi: 10.1046/j.1365-2869.2003.00337.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0962-1105&date=2003&volume=12&issue=1&spage=1 .337 [DOI] [PubMed] [Google Scholar]
- 72.Van Dongen HP, Maislin G, Mullington JM, Dinges DF. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003 Mar 15;26(2):117–26. doi: 10.1093/sleep/26.2.117. [DOI] [PubMed] [Google Scholar]
- 73.Lim J, Jeong CY, Lim JM, Chung S, Kim G, Noh KJ, Jeong H. Assessing sleep quality using mobile EMAs: opportunities, practical consideration, and challenges. IEEE Access. 2022 Apr 1;10:2063–76. doi: 10.1109/ACCESS.2021.3140074. [DOI] [Google Scholar]
- 74.Klasnja P, Hekler EB, Shiffman S, Boruvka A, Almirall D, Tewari A, Murphy SA. Microrandomized trials: an experimental design for developing just-in-time adaptive interventions. Health Psychol. 2015 Dec;34S:1220–8. doi: 10.1037/hea0000305. https://europepmc.org/abstract/MED/26651463 .2015-56045-003 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Screenshots of the health care Internet of Things app.
Validity of the Sciencenet activity monitor.
Sleep hygiene guide.
Additional analyses of the statistical properties of sleep variables.
Data Availability Statement
The participants of this study did not agree to their data being shared publicly; therefore, supporting data are not available.