

Abstract
Objective:
To explore the services community pharmacists in Lagos state provided to their communities during the COVID-19 pandemic.
Methods:
A cross-sectional survey of community pharmacists drawn from all the Association of Community Pharmacists’ zones in Lagos state was done from April to June 2021. Data were collected using a structured, self-reported online questionnaire via Google Forms and were analyzed using descriptive and inferential statistical analysis.
Findings:
Two hundred and forty community pharmacists participated in the study; the response rate was 80.5%. Patient counseling (99.6%), assessment and treatment of common acute ailments (99.6%), and patient education on hygiene (99.6%) were the most reported services provided by community pharmacists. The COVID-19 infection prevention and control measures most frequently practiced by the pharmacists include cleaning of floors with soap and water (98.4%), provision of hand sanitizers for staff use (97.1%), and taking precautions when handling prescriptions and dispensing drugs (96.7%). Significant barriers to the provision of the services were reduced workforce in the pharmacy, time constraints, and extended working hours. Zinc (98.3%), Vitamin C (97.5%), and ivermectin (95.0%) tablets were the most reported medications for the prevention and treatment of COVID-19 infection.
Conclusion:
Community pharmacists in Lagos state actively provide pharmacy services and practice various recommended infection prevention and control measures to mitigate the spread of COVID-19 infection in their communities.
Keywords: Community pharmacist, COVID-19, infection prevention and control, Lagos state
INTRODUCTION
The severe acute respiratory coronavirus 2 (SARS-CoV-2) termed COVID-19 was declared a pandemic on March 11, 2020.[1] Since then, multiple variants of the SARS-CoV-2 different from the strain first detected in Wuhan, China, have been identified, the most recent being the delta and omicron variants. The COVID-19 pandemic has convulsed the entire world, overwhelming the health systems of most developed nations. In low- and middle-income countries, the outbreak of COVID-19 is disquieting due to social inequalities, limited health budgets, and the significant burden of other infectious and chronic diseases.[2] In Nigeria, the Federal Ministry of Health reported the index case of COVID-19 infection on February 27, 2020.[3] Nigeria has since had over 250,000 confirmed cases of COVID-19, with about 3000 recorded deaths.[4]
Like other health-care professionals, pharmacists have vital roles in ensuring effective containment of the COVID-19 virus and reducing community transmission. Community pharmacists remain the most accessible health-care providers in many communities and the entry point of patient engagement with the health-care system.[5] Globally, pharmacists in different practice areas have contributed to essential patient care and the public's well-being in diverse ways during the COVID-19 pandemic.[6] The International Pharmaceutical Federation (FIP) issued guidelines that provided specific infection prevention measures, preparedness to ensure a timely and effective response, immediate actions that pharmacists should take, and postpandemic measures.[7] Accordingly, the community pharmacists’ roles have expanded to include other services such as providing reliable disease information, public education on preventive measures, referring suspected cases, maintaining a continuous supply of medicines and preventative products, and vaccination.[8]
Community pharmacy practice varies markedly across different geographical locations; so, amid a pandemic with a massive magnitude like the ongoing one, it becomes pertinent to examine the services that community pharmacists are providing to their communities and their contributions toward curbing the spread of the pandemic. Community pharmacists’ services in the ongoing pandemic have been reported in various parts of the world.[9,10] Lagos state is located in the South-Western part of Nigeria and is the nation's economic and commercial capital. It is considered the most populous city in Africa, with a 17.5 million estimated population.[11] The state has the highest number of confirmed COVID-19 cases and is the pandemic's epicenter in Nigeria,[4] presenting a need for concerted efforts to contain the virus and reduce community transmission. Little is known about the roles and services of community pharmacists in Lagos state to their communities during this pandemic. This study, therefore, aimed to explore the pharmaceutical services community pharmacists in Lagos state are providing during the pandemic and the infection prevention and control measures they practice to prevent community transmission. The findings from this study can inform future decisions about the restructuring of existing health services by the Government, public health bodies, and policymakers in response to public health crises such as the current pandemic.
METHODS
The study was a cross-sectional online survey carried out from April to June 2021 among registered community pharmacists practicing in different areas of Lagos State. The inclusion criteria were community pharmacists duly registered with the Pharmacists’ Council of Nigeria and practicing in Lagos state. Pharmacists in other pharmacy practice areas were excluded from the study. We obtained ethical approval for this study from the Health Research and Ethics Committee of the Lagos University Teaching Hospital, Lagos, with approval number: ADM/DCST/HREC/APP/4102. Participation in the study was voluntary and did not constitute any risk to the participants. A sample size of 298 was calculated using the Raosoft sample size calculator based on the number of registered community pharmacists in Lagos (1313), 95% confidence interval, and 5% error margin. The authors developed a structured, self-administered questionnaire following a thorough review of available literature on the study topic[12,13] and recommendations from professional organizations such as the FIP.[7] Some of the questionnaire's items were adapted from a similar study.[10] The first draft of the questionnaire was evaluated for face and content validity by five independent academics from the Faculty of Pharmacy, University of Lagos, and two community pharmacists. The research team reviewed their comments and feedback and applied them as appropriate to obtain the final version of the questionnaire. The questionnaire was organized into five sections and fit online administration using Google Forms. A pilot study using 30 community pharmacists was carried out to assess the internal consistency and reliability of the questionnaire. The pharmacists who took part in the pilot study were excluded from the final study. The reliability test gave a Cronbach's alpha value of 0.821 (Provision of patient services), 0.754 (COVID-19 infection preventative measures), and 0.882 (drivers and barriers to the provision of pharmaceutical services during COVID-19 pandemic). All the items on the questionnaire were considered appropriate for the study objectives. Data was collected online using the WhatsApp group platforms of the different Lagos state Association of Community Pharmacists of Nigeria (ACPN) zones. The Google form link of the study instrument was deployed on the various WhatsApp platforms for 8 weeks to enable consenting pharmacists to participate in the study. The authors sent occasional reminders to the community pharmacists through the different zonal leaders. SPSS Statistics for Windows, Version 27.0 (Armonk, NY: IBM Corp.). Descriptive statistics was used to summarize the participants’ demographic characteristics, services provided by community pharmacists, and barriers and drivers to the provision of pharmaceutical services. Association between the respondents’ demographic characteristics and services provided by the pharmacist and the drivers and barriers to providing services during the pandemic was tested using Pearson's Chi-square. The major services provided by community pharmacists during the pandemic and the barriers and drivers to providing these services were identified using principal component analysis based on the Varimax rotation method. Before performing the principal components analysis, the suitability of data for factor analysis was assessed using the Kaiser-Meyer-Olkin test for sampling adequacy and Bartlett's test of sphericity. Only factors having eigenvalue above one were considered significant and retained. Statistical significance was set at P < 0.05.
RESULTS
A total of 240 community pharmacists from 24 ACPN zones of Lagos state completed the questionnaire, giving a response rate of 80.5%. The respondents had a mean age of 40.1 ± 11.9 years, and 134 (55.8%) were females. More than half of the respondents had practiced community pharmacy for over 10 years, and 156 (65%) were superintendent pharmacists at their practice locations. Most of the respondents had received postgraduate training and professional qualifications, and 113 (47.1%) had participated in a COVID-19 training course [Table 1].
Table 1.
Sociodemographic characteristics and practice of the respondents
| Variable | n (%) | P |
|---|---|---|
| Age (years) | 0.791 | |
| 20-39 | 113 (47.1) | |
| 40-49 | 65 (27.1) | |
| 50-59 | 49 (20.4) | |
| 60-69 | 13 (5.4) | |
| 70+ | 0 | |
| Gender | 0.999 | |
| Male | 106 (55.8) | |
| Female | 134 (44.2) | |
| Number of years of pharmacy practice | 0.410 | |
| 0-4 | 32 (13.3) | |
| 5-9 | 59 (24.6) | |
| 10+ | 149 (62.1) | |
| Duration of community pharmacy practice at present location | 0.516 | |
| 0-4 | 105 (43.8) | |
| 5-9 | 59 (24.6) | |
| 10+ | 76 (31.7) | |
| Position at the community pharmacy | 0.049* | |
| Superintendent pharmacist | 156 (65.0) | |
| Full-time pharmacist | 57 (23.8) | |
| Part-time pharmacist | 14 (5.8) | |
| Other | 13 (5.4) | |
| Postgraduate training and qualifications | 0.212 | |
| MSc | 98 (40.8) | |
| Ph.D | 10 (4.2) | |
| WAPCP | 23 (9.6) | |
| Others | 109 (45.4) | |
| Completion of any COVID-19 training | 0.695 | |
| Yes | 113 (47.1) | |
| No | 127 (52.9) | |
| Willingness to participate in a WHO COVID-19 training course | ||
| Yes | 210 (87.5) | |
| No | 30 (12.5) | |
| Willingness to participate in FIP COVID-19 training course | ||
| Yes | 209 (87.1) | |
| No | 31 (12.9) |
*Significant association with services provided by the community pharmacists (Chi-squared statistics, statistical significance at P<0.05). FIP=International Pharmaceutical Federation
Principal components analysis with the Varimax rotation method identified seven components with eigenvalue exceeding 1. The eigenvalues for the seven components were 2.293, 1.792, 1.593, 1.415, 1.394, 1.374, and 1.108. The eigenvalues indicate that the first component provided the highest value. Hence, the items in the first component indicate the identified major services being provided by community pharmacists to their communities during the COVID-19 pandemic. These items include counseling patients, assessing and treating common acute diseases, educating patients on personal and environmental hygiene, prescription refilling and prescription screening for drug interaction, and detecting adverse drug reactions [Table 2].
Table 2.
Services provided by community pharmacists during COVID-19 pandemica
| Services provided by community pharmacists | Component | ||||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Counseling services to patients | 0.951 | ||||||
| Assessing and treating common acute diseases (e.g., malaria, cold, catarrh, sore throat) | 0.951 | ||||||
| Educating patients/clients on personal and environmental hygiene (e.g., hand hygiene) | 0.909 | ||||||
| Prescription refilling | 0.819 | ||||||
| Prescription screening for drug interaction and detection of ADR | 0.706 | ||||||
| Blood pressure monitoring | 0.879 | ||||||
| Point-of-care testing (e.g., blood glucose, cholesterol) | 0.819 | ||||||
| Tele-pharmacy and tele-medicine consulting | 0.715 | ||||||
| Home delivery services to vulnerable groups (e.g., elderly, patients with chronic diseases) | 0.601 | ||||||
| Reporting and referral of COVID-19 cases (e.g., risk assessment, triage) | 0.817 | ||||||
| Information centre for COVID-19 | 0.635 | ||||||
| Uninterrupted supply of medicines and PPEs (e.g., face masks, hand gloves, hand sanitizers) | 0.838 | ||||||
| Health education and promotion | 0.532 | ||||||
| Syndromic management of STIs | 0.795 | ||||||
| Assessing and treating minor soft tissue injuries | 0.660 | ||||||
| Immunization services | 0.562 | ||||||
Sixteen variables were considered and were analyzed individually using PCA. The PCA was carried out based on the varimax rotation method. Only factors having eigenvalue above one were considered significant and retained. The eigenvalues indicate that the first component provided the highest value. Items in bold indicate the identified major services provided by community pharmacists to their communities during the COVID-19 pandemic. PCA=Principal component analysis, ADR=Adverse drug reactions, PPEs=Personal protective equipment, STIs=Sexually transmitted infections
More than 85% of the pharmacists reported practicing appropriate and recommended infection and control practices (IPC) measures such as the washing of hands with soap and water, use of alcohol-based hand sanitizers, regular cleaning of the floor and work surfaces with soap and water, use of face masks/shields, and precautionary handling and dispensing of patient prescriptions. The least practiced IPC measures reported by the pharmacists include the installation of counter-top barrier screens (23.3%), patient triage/COVID-19 risk assessment (46.3%), and floor signs for patients within the pharmacy for social distancing (48%) [Table 3]. There was a significant association between the pharmacists’ demographic factors and infection prevention and control measures practiced during the pandemic (χ2 = 17.012; P < 0.05).
Table 3.
COVID-19 infection prevention and control measures practices by the community pharmacists
| Questions | Responses (%) | ||||
|---|---|---|---|---|---|
|
| |||||
| Never | Rarely | Sometimes | Very often | Always | |
| Cleaning of workspace with soap and water, and sanitizing same (e.g., counter-tops) | 0 | 1.3 | 10.8 | 28.3 | 59.6 |
| Cleaning of floors with soap and water | 0 | 0 | 1.7 | 19.6 | 78.8 |
| Provision of waiting area for customers outside the pharmacy | 7.1 | 10.4 | 15.0 | 16.7 | 50.8 |
| Floor signs for patients within the pharmacy for social distancing | 15.4 | 14.2 | 22.5 | 12.1 | 35.8 |
| Sanitizing of commonly used handheld tools (e.g., phones, point-of-care testing tools) | 0.8 | 4.2 | 17.5 | 25.4 | 52.1 |
| Availability of hand sanitizers for staff use | 0.4 | 0.8 | 1.7 | 10 | 87.1 |
| Use of face masks and/face shields | 0 | 1.7 | 8.3 | 19.6 | 70.4 |
| Staff washing of hands with soap and water | 0.4 | 2.1 | 4.6 | 25.8 | 67.1 |
| Intentional reduction of the number of workers per day or working in fixed shifts | 11.7 | 8.8 | 14.6 | 20.4 | 44.6 |
| Granting work leave to vulnerable staff (e.g., aged, chronic conditions, acute conditions) | 12.5 | 12.9 | 17.5 | 15.0 | 42.1 |
| Taking precautions while handling or dispensing prescriptions | 0 | 0.4 | 2.9 | 14.6 | 82.1 |
| Limiting the number of customers inside the pharmacy at every point in time | 1.7 | 2.1 | 12.1 | 23.8 | 60.4 |
| Define a specific area for customers having suspected symptoms | 16 | 36 | 56 | 55 | 77 |
| Use of contactless payment options (e.g., point-of-sale/card payment) | 1.3 | 1.3 | 21.3 | 38.8 | 37.5 |
| Ensuring that patients use their face masks before entry and while in the pharmacy | 0.8 | 2.1 | 14.6 | 27.5 | 55.0 |
| Provision of water and soap at the entrance of the pharmacy for client’s/patient’s use | 6.3 | 7.5 | 12.5 | 14.6 | 59.2 |
| Provision of alcohol-based hand sanitizers for customers before entry | 1.7 | 2.5 | 10.0 | 16.3 | 69.6 |
| Provision of signage/banner at the pharmacy entrance displaying information on COVID-19 | 7.9 | 10.8 | 15.8 | 17.1 | 48.3 |
| Carrying out a triage/COVID-19 risk evaluation on clients/patients | 10.8 | 13.8 | 29.2 | 23.8 | 22.5 |
| Installment of counter-top, transparent plastic barrier screens in the Pharmacy | 43.8 | 20.4 | 12.5 | 7.9 | 15.4 |
| Allowing pick-up of medications (refills) on request by patients | 5.0 | 6.7 | 21.7 | 25.8 | 40.8 |
The principal component analysis identified four significant drivers and three significant barriers to providing pharmaceutical services. The identified drivers are; the moral and professional obligation of offering pharmaceutical assistance, professional satisfaction with the contribution to preventing COVID-19, the opportunity to prove to be an inseparable part of health professionals, and measures taken by relevant health institutions [Table 4]. A reduced workforce in the pharmacy, time constraints, and extended working hours was identified as the key barriers to the provision of pharmaceutical services by the community pharmacists [Table 5].
Table 4.
Drivers to provision of pharmaceutical services during the COVID-19 pandemica
| Drivers | Component | ||
|---|---|---|---|
|
| |||
| 1 | 2 | 3 | |
| Moral and professional obligation ofoffering pharmaceutical assistance | 0.835 | ||
| Professional satisfaction with your contributions to preventing COVID-19 | 0.699 | ||
| Opportunity to prove yourselves as being an inseparable part of health professionals | 0.575 | ||
| Measures taken by relevant health institutions | 0.564 | ||
| Better opportunity to use your pharmaceutical skillsand knowledge | 0.800 | ||
| Professional satisfaction with the help you offeredto patients | 0.709 | ||
| Opportunity to elevate your personal, professional image | 0.698 | ||
| Opportunity to elevate the image of the pharmacywhere you work | 0.670 | ||
| Being in line with competition from other pharmacies in the market | 0.780 | ||
| Financial reimbursement you receive during this period | 0.529 | ||
aTen variables were considered and were analyzed individually using PCA. The PCA was carried out based on varimax rotation method. Only factors having eigenvalue above one were considered significant and retained. The eigenvalues indicate that the first component provided the highest value. Items in bold indicate the identified major drivers of pharmacist’s provision of services during the COVID-19 pandemic. PCA=Principal component analysis
Table 5.
Barriers to provision of pharmaceutical services during the COVID-19 pandemica
| Barriers | Component | ||||
|---|---|---|---|---|---|
|
| |||||
| 1 | 2 | 3 | 4 | 5 | |
| Reduced workforce in the pharmacy | 0.832 | ||||
| Time constraints | 0.721 | ||||
| Pharmacists extended working hours | 0.554 | ||||
| Patient’s pandemics related panic | 0.768 | ||||
| Patients buying unnecessary and excessive products | 0.766 | ||||
| Misinformation around COVID-19 potential treatment options | 0.544 | ||||
| Worrying about getting infected with COVID-19 | - | ||||
| Lack of protective equipment in your pharmacy | 0.768 | ||||
| Lack of your adequate information on COVID-19 | 0.750 | ||||
| Price increase from pharmaceutical wholesalers | 0.792 | ||||
| Price increase of pharmaceutical products in the pharmacy | 0.767 | ||||
| Increased influx of patients to the pharmacy | 0.757 | ||||
| Frequent pharmacy inspections by authorities | 0.728 | ||||
| Inadequate financial compensation during pandemics | - | ||||
Fourteen variables were considered and were analyzed individually using PCA. The PCA was carried out based on varimax rotation method. Only factors having eigenvalue above one were considered significant and retained. The eigenvalues indicate that the first component provided the highest value. Items in bold indicate the identified major barriers to the pharmacist’s provision of services during the COVID-19 pandemic. PCA=Principal component analysis
There was no association between the drivers of pharmaceutical services provision during the COVID-19 pandemic and pharmacists’ sociodemographic factors. However, years of practice experience were significantly associated with the barriers to providing pharmaceutical services during the COVID-19 pandemic at χ2 = 6.506 (P < 0.05).
The most frequently dispensed medications by the community pharmacists for the prevention and treatment of COVID-19 infection are zinc (98.3%), Vitamin C (97.5%), ivermectin (95%), azithromycin (94.6%), and Vitamin D3 (94.2%) tablets [Figure 1].
Figure 1.
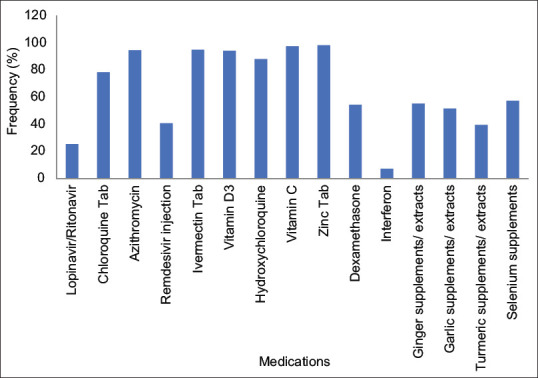
Pharmaceutical prevention and management of COVID-19 infection
DISCUSSION
Our results showed that community pharmacists in Lagos state provide a range of preventive and curative services to their communities in the ongoing pandemic. The most-reported services include counseling, patient education, prescription filling, management of common ailments, and prescription screening for drug interactions. Community pharmacists reported similar services in Ghana[14] and globally.[5,15,16] Common infections such as cold, malaria, and flu are clinically assessed and managed effectively in the community pharmacy. Patient counseling, prescription screening, and filling are the primary roles of a community pharmacist. These roles further come to bear in the heat of the pandemic, with informal reports of patients accumulating medications inappropriately, thus leading to an increase in refill orders received by community pharmacists.[5] The study participants also reported providing expanded or additional services relating to public health responses to help ease the pressure in other health service areas. The most noted of these services is patient education. Patient education has been identified as an effective way community pharmacists can help limit COVID-19 spread.[17,18] Pharmacists apply their extensive knowledge and training in pharmacotherapy and medication use management to provide COVID-19 public health education to the public. By providing accurate and relevant health education to patients, community pharmacists empower them with information to help them prevent the spread of the virus and make the right health choices. Although not identified as a significant service, the pharmacists also engaged with their patients through telepharmacy and telemedicine consulting. Telepharmacy and telemedicine consulting have been used effectively for prescription filling, medication therapy review, adverse drug reaction monitoring, patient counseling, and follow-up.[19] While there has not been any official implementation of telepharmacy in Sub-Saharan Africa, the COVID-19 pandemic has provided an opportunity for the practice to gain ground in some African countries, including Nigeria.[20]
The least reported service was immunization. Despite the willingness to provide this service, low participation of Nigerian pharmacists in immunization services had been reported in earlier studies.[21,22] Quick access and broader COVID-19 vaccine coverage in countries like the US and UK have been attributed to community pharmacists’ involvement in vaccination.[23] There is currently no policy directing the participation of community pharmacists in immunization in Nigeria,[23] which can explain the low report of immunization services during the pandemic. Recently, the Federal Government of Nigeria announced the extension of vaccination centers to select community pharmacies.[24] It is hoped that this policy will be implemented quickly as it would leverage the large workforce of community pharmacists and their easy accessibility to increase immunization coverage.
In line with the FIP recommended guidelines at the workplace for pharmacists and pharmacy staff, our study participants carried out COVID-19 IPC practices that pertained to the pharmacy premise and staff and the clients visiting the premise. Providing hand sanitizers and cleaning floors with soap and water was the most reported IPC practice within the pharmacy premise. A similar study in Australia also reported a high implementation of IPC through regular cleaning with detergent and disinfection of commonly touched surfaces.[25] The installation and use of counter-top transparent plastic barrier screens was the least reported IPC measure within the pharmacy premise. The installation costs and the likely changes these structures will make to the pharmacies are possible explanations for the low implementation of this measure. Similar to Hoti et al.'s findings, the community pharmacists did not provide a defined area for clients/patients having suspected symptoms of COVID.[10] This could be due to concerns about the pharmacists contracting the virus due to potential close contact with the clients.
Regarding IPC measures concerning the clients and patients, the community pharmacists mostly implemented the provision of hand sanitizer at the pharmacy entrance, thereby complying with the CDC's directive of frequent hand hygiene as one of the steps to help prevent illness during the COVID-19 pandemic. For the general public, the recommendation is to use soap and water and, if water is unavailable, a hand sanitizer containing at least 60% alcohol.[26] Triage and COVID-19 risk evaluation of patients was the least implemented IPC measure, probably due to a lack of training and expertise to carry out such risk evaluation. Evaluating patients for the risk of COVID-19 infection could help protect vulnerable patients from contracting the virus within the pharmacy premises.
The drivers to providing pharmaceutical services identified in this study are similar to those reported by Hoti et al.[10] Pharmacists are ethically required to prioritize patients’ health and well-being. Interestingly, most community pharmacists report their moral and professional obligation to offer pharmaceutical assistance as a driver for providing pharmaceutical services during the pandemic. The identified significant barriers from this study contrast with a similar study in Kosovo, which reported price increases by pharmaceutical wholesalers, patient pandemic-related panic, and patients’ purchase of unnecessary products as critical barriers to providing community pharmacy services during the pandemic.[10] The reduced workforce reported by our participants could be attributed to fear of contracting COVID-19, intentional hold-off of duties by staff at risk, and an attempt to reduce over-crowding of the pharmacy premise. A reduced workforce invariably implies more responsibilities for available staff, extended working hours, and a stressful work environment. Such working conditions can also impact the productivity and quality of services provided by pharmacists.
Zinc, Vitamin C, ivermectin, azithromycin, and Vitamin D3 tablets were mainly used for COVID-19 prevention and treatment. Interestingly, these medicines have been suggested to play a role in mitigating COVID-19 infection, which could explain their frequency or high use during the pandemic. Previous studies have reported that zinc can reduce the risk of COVID-19 infection and reduce the duration and severity of COVID-19 illness.[27] Vitamin C's wide range of pharmacological activities makes it an excellent adjunct therapeutic option for preventing and managing COVID-19 infection. Vitamin D3 supplementation is quite popular in COVID-19 management despite several debates on its actual benefits for the disease. Current evidence is insufficient to conclude that Vitamin D supplementation provides tangible benefits in COVID-19 management.[28] Azithromycin and ivermectin are part of the medications repurposed for use in COVID-19 management. While there is no direct evidence of the effectiveness of azithromycin in COVID-19, some researchers have suggested that its antimicrobial activity remains helpful in the empirical treatment of community-acquired pneumonia occurring in COVID-19 patients.[29] The far-reaching consequence of community pharmacists increasingly dispensing this medication is the increasing risk of antimicrobial resistance, which is already a public health concern in Africa.[30] It is thus vital for community pharmacists to encourage the rational use of this antibiotic by dispensing it strictly on medical prescription.
Our study has broad coverage of the community pharmacy populace in Lagos state. However, community pharmacists who are not active on the social media platform (WhatsApp) used for the study may not have been reached. Also, the results of this study should be interpreted bearing in mind that the pandemic keeps evolving. The primary services provided and the medicines mostly used to manage COVID-19 infection might have changed over time.
In conclusion, community pharmacists in Lagos state, Nigeria, provide various services to their communities during the COVID-19 pandemic. They are also implementing the recommended IPC practices to curb the infection spread within their premises and visiting patients. Efforts should be intensified toward the sparsely provided services such as immunization. While encouraging the drivers to provide pharmacy services, action should be taken individually and collectively at the ACPN level to combat the identified barriers to providing pharmaceutical services.
AUTHORS’ CONTRIBUTION
O Amaeze conceived the study. A. Akinola and A. Aiyeolemi designed the study instrument and Google form for data collection. O Ijomone and F Lawal coordinated the data collection. U Mbata and O Amaeze carried out the data analysis. All authors contributed to writing the manuscript and approved the final version of the manuscript.
Financial support and sponsorship
Ladipo Mobolaji Abisogun-Afodu Research Grant in Pharmacy 2020.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19. 2020. [Last accessed on 2021 Dec 23]. Avaialble from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefingon-covid-19---11-march-2020 .
- 2.Parreiras Martins MA, Fonseca de Medeiros A, Dias Carneiro de Almeida C, Moreira Reis AM. Preparedness of pharmacists to respond to the emergency of the COVID-19 pandemic in Brazil: A comprehensive overview. Drugs Ther Perspect. 2020;36:455–62. doi: 10.1007/s40267-020-00761-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nigeria Center for Disease Control. First Case of Coronavirus Disease Confirmed in Nigeria. 2020. [Last accessed on 2022 Jan 14]. Avaialble from: https://ncdc.gov.ng/news/227/first-case-of-corona-virus-disease-confirmed-innigeria .
- 4.Nigeria Centre for Disease Control. Covid-19 Nigeria. 2022. [Last accessed on 2022 Jan 14]. Avaialble from: https://covid19.ncdc.gov.ng/
- 5.Cadogan CA, Hughes CM. On the frontline against COVID-19: Community pharmacists’ contribution during a public health crisis. Res Social Adm Pharm. 2021;17:2032–5. doi: 10.1016/j.sapharm.2020.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Goff DA, Ashiru-Oredope D, Cairns KA, Eljaaly K, Langford BJ, Messina AP, et al. Global contributions of pharmacists during the COVID -19 pandemic. J Am Coll Clin Pharm. 2020;3:1480–92. doi: 10.1002/jac5.1329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.International Pharmaceutical Federation. COVID-19: Guidelines for Pharmacists and the Pharmacy Workforce. 2020. [Last accessed on 2022 Dec 23]. Avaialble from: https://www.fip.org//publications?publicationCategory=97&publicationYear=2020&publicationKeyword=
- 8.Ahmed N, Saeed A. Pharmacists knowledge and contribution during coronavirus disease-2019 pandemic in Sudan, 2020. Matrix Sci Med. 2021;5:31. [Google Scholar]
- 9.Atif M, Malik I. COVID-19 and community pharmacy services in Pakistan: Challenges, barriers and solution for progress. J Pharm Policy Pract. 2020;13:33. doi: 10.1186/s40545-020-00240-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hoti K, Jakupi A, Hetemi D, Raka D, Hughes J, Desselle S. Provision of community pharmacy services during COVID-19 pandemic: A cross sectional study of community pharmacists’ experiences with preventative measures and sources of information. Int J Clin Pharm. 2020;42:1197–206. doi: 10.1007/s11096-020-01078-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.World Population Review. Lagos Population 2021 (Demographics, Maps, Graphs) 2021. [Last accessed on 2022 Jan 14]. Avaialble from: https://worldpopulationreview.com/world-cities/lagos-population .
- 12.Khan Z, Muhammad K, Ahmed A, Rahman H. Coronavirus outbreaks: prevention and management recommendations. Drug Ther Perspect. 2020;36((5)):215–217. doi: 10.1007/s40267-020-00717-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zheng SQ, Yang L, Zhou PX, Li HB, Liu F, Zhao RS. Recommendations and guidance for providing pharmaceutical care services during COVID-19 pandemic: A China perspective. Res Social Adm Pharm. 2021;17:1819–24. doi: 10.1016/j.sapharm.2020.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Basheti IA, Nassar R, Barakat M, Alqudah R, Farha RA, Muqatash T, et al. Pharmacists’ perceived barriers towards delivering their emergency roles during the COVID-19 pandemic and perceived policymakers’ responsibilities. J Pharm Policy Pract. 2020;13:62. doi: 10.1186/s40545-020-00254-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ung CO. Community pharmacist in public health emergencies: Quick to action against the coronavirus 2019-nCoV outbreak. Res Social Adm Pharm. 2020;16:583–6. doi: 10.1016/j.sapharm.2020.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Visacri MB, Figueiredo IV, Lima TM. Role of pharmacist during the COVID-19 pandemic: A scoping review. Res Social Adm Pharm. 2021;17:1799–806. doi: 10.1016/j.sapharm.2020.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Joda AE, Olugbake OA, Oyetunde OO, Awofisayo O, Ibrahim M, Williams FE, et al. Pharmacists’ perception of their roles and involvement in coronavirus disease 2019 (COVID-19) J Basic Soc Pharm Res. 2020;1:68–82. [Google Scholar]
- 18.Al-Quteimat OM, Amer AM. SARS-CoV-2 outbreak: How can pharmacists help? Res Social Adm Pharm. 2021;17:480–2. doi: 10.1016/j.sapharm.2020.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liao Y, Ma C, Lau AH, Zhong M. Role of pharmacists during the COVID-19 pandemic in China – Shanghai Experiences. J Am Coll Clin Pharm. 2020;3((5)):997–1002. doi: 10.1002/jac5.1288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hedima EW, Okoro RN. Telepharmacy: An opportunity for community pharmacists during the COVID-19 pandemic in Sub Saharan Africa. Health Policy Technol. 2021;10:23–4. doi: 10.1016/j.hlpt.2020.10.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Olumide IS, Oladipo OH. Knowledge, attitudes and participation of community pharmacists in Lagos State, Nigeria towards primary health care (PHC) J Public Health Epidemiol. 2015;7:15–9. [Google Scholar]
- 22.Aderemi-Williams RI, Igwilo CI. Community pharmacies as possible centres for routine immunization. Nig Q J Hosp Med. 2007;17:131–3. doi: 10.4314/nqjhm.v17i4.12692. [DOI] [PubMed] [Google Scholar]
- 23.Wada YH, Musa MK, Ekpenyong A, Adebisi YA, Musa MB, Khalid GM. Increasing coverage of vaccination by Pharmacists in Nigeria; an urgent need. Public Health Pract. 2021;2:100148. doi: 10.1016/j.puhip.2021.100148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ojerinde D. PSN, ACPN Commend FG for Choosing Pharmacies as Vaccination Centres. Punch Newspaper. 2021. [Last accessed on 2021 Dec 23]. Avaialble from: https://www.sunnewsonline.com/psn-acpn-commend-fg-for-choosing-pharmacies-as-vaccinationcentres/
- 25.Sum ZZ, Ow CJ. Community pharmacy response to infection control during COVID-19. A cross-sectional survey. Res Social Adm Pharm. 2021;17:1845–52. doi: 10.1016/j.sapharm.2020.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Centre for Disease Control. Guideline for Hand Hygiene in Healthcare Settings. 2019. [Last accessed on 2021 Dec 23]. Avaialble from: https://www.cdc.gov/infectioncontrol/guidelines/hand-hygiene/index.html .
- 27.Hunter J, Arentz S, Goldenberg J, Yang G, Beardsley J, Mertz D, et al. Rapid review protocol: Zinc for the prevention or treatment of COVID-19 and other coronavirus-related respiratory tract infections. Integr Med Res. 2020;9:100457. doi: 10.1016/j.imr.2020.100457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sindhusen P. Vitamin D and COVID-19: A physiological perspective. Biomed Res Ther. 2021;8:4358–66. [Google Scholar]
- 29.Sultana J, Cutroneo PM, Crisafulli S, Puglisi G, Caramori G, Trifirò G. Azithromycin in COVID-19 patients: Pharmacological mechanism, clinical evidence and prescribing guidelines. Drug Saf. 2020;43:691–8. doi: 10.1007/s40264-020-00976-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sefah IA, Ogunleye OO, Essah DO, Opanga SA, Butt N, Wamaitha A, et al. Rapid assessment of the potential paucity and price increases for suggested medicines and protection equipment for COVID-19 across developing countries with a particular focus on Africa and the implications. Front Pharmacol. 2020;11:588106. doi: 10.3389/fphar.2020.588106. [DOI] [PMC free article] [PubMed] [Google Scholar]