

Abstract
Background.
During high-resolution anorectal manometry (HR_ARM), the raw data are converted into software-derived summary variables (eg, rectoanal gradient during evacuation) that capture only a snapshot of the data collected during HR_ARM and are less useful than newer indices, which are also derived from the raw data, for diagnosing defecatory disorders (DD). However, it is cumbersome and time consuming to extract raw data from the program and calculate such indices. This study aimed to devise a user-friendly approach to extract anorectal pressures measured with HR_ARM.
Methods.
Anorectal pressures at rest, during anal squeeze, and evacuation were measured with HR_ARM in 180 women, among whom 60 each were healthy, had DD, or fecal incontinence. A reverse-engineering approach extracted pressure values from color images in HR_ARM reports. The summary variables generated by the software and a reverse-engineering approach were compared with Lin’s concordance correlation coefficient (CCC), paired t-tests, and Bland–Altman’s tests.
Results.
Anorectal pressures summarized by the software and a reverse-engineering method were highly concordant for anal resting (CCC [95% CI], 0.98 [0.97, 0.99]) and squeeze pressures (0.99 [0.99, 0.99) and the rectoanal gradient during evacuation with an empty (0.98 [0.97, 0.98]) and a filled balloon (0.99 [0.99, 0.99]). For most variables, the paired t and Bland–Altman comparisons were not significant.
Conclusions.
Anorectal pressures can be accurately determined from pressure topography images in HR_ARM reports. In future, this reverse-engineering approach can be harnessed to compile large HR_ARM datasets across centers and to uncover newer, potentially more useful summary rectoanal pressure variables.
Keywords: chronic constipation, pelvic floor dysfunction, anal weakness, International anorectal physiology working group (IAPWG), diagnostic accuracy
Graphical Abstract
During high-resolution anorectal manometry (HR_ARM), the raw data are converted into software-derived summary variables (eg, rectoanal gradient during evacuation) that capture only a snapshot of the collected data. Computing different, more useful indices from the raw data requires time consuming extraction of raw data from the program. We devised a reverse-engineering method to compute anorectal pressures from pressure topography images in HR_ARM reports. Confirming the accuracy of this method, these pressures were significantly correlated with software-generated values. This method can be harnessed to compile large HR_ARM datasets across centers and to uncover newer, potentially more useful parameters.

BACKGROUND
Anorectal manometry is widely used to diagnose defecatory disorders (DD) and to identify anal weakness in patients with fecal incontinence (FI)1. Differences among HR-ARM systems, including the formulae that are used to summarize pressures at rest, during squeeze and evacuation, hinder the ability to combine data across systems. Besides, the HR-ARM summary variables (e.g., rectoanal gradient during evacuation) only capture a fraction of the rich data recorded during the test. The International Anorectal Physiology Working Group suggested methods for measuring and analyzing anorectal pressures2. Thereafter, modifications that enhance the efficiency of conducting HR_ARM (eg, by measuring anal resting pressure for 20s rather than 60s)3,4 or its diagnostic utility have been recommended5. These studies transferred the raw HR-ARM data to a different program (eg, Microsoft Excel) – and analyzed the data in that program {Sharma, 2020 Jul 01 #6289}. Such analyses are cumbersome and time-consuming. Designed to address these limitations, this study aimed to (1) devise a user-friendly, reverse-engineering approach to extract anorectal pressures measured with HR_ARM and (2) to compare pressures measured with the existing and a reverse-engineering approach.
MATERIALS AND METHODS
Experimental Design
Anorectal pressures were measured with HR_ARM (Medtronic Inc, Minneapolis, MN). Pressures were summarized by the commercial program (ManoView AR v3.0, Medtronic Inc), generating reports in Microsoft Word (Microsoft Inc), which contain color images of pressures. Through a reverse-engineering approach, the pressure values were analyzed from these color images as detailed below.
Participants
Seeking to compare pressures in women who had a spectrum of anorectal disturbances, this study was based on HR_ARM data in 60 women each who were healthy (43 ± 16 y [mean ± SD]), had a DD (39 ± 13 y) or FI (60 ± 10 y). Neither healthy controls nor patients had severe systemic (eg, neurological) diseases nor were they on medications (eg, opioids) that have major effects on gastrointestinal motility. Controls did not have a functional bowel disorder by Rome criteria, obstetric anorectal laceration (grade 3 or 4), or any previous anorectal surgery6,7. In FI women, the severity of FI was also rated8. Some data for anorectal pressures analyzed with the commercial program but not the reverse engineering approach have been published5,9,10.
Pressure Measurements
Anorectal pressures were measured in the left lateral decubitus position with HR_ARM (Medtronic Inc, Minneapolis, MN). at rest (20s), during contraction of the anal sphincter (3 times, 20s each), and during stimulated evacuation (ie, 2 attempts, 20s each, with a rectal balloon that was either empty or filled with 50 ml of water). Pressures were analyzed with the commercial software (ManoView AR v3.0, Medtronic Inc) that generates reports with color images of pressures. Each pressure reading is assigned a color. An open-source image analysis program (ImageMagick), based on R (R Studio), used the color scale attached to each study to extract pressures (10 Hz) at rest, during squeeze, and evacuation from these images. For most studies, the color scale ranged from 0 to 200 mmHg, which is the default range in the Manoview program. In 74 participants with a pressure greater than 200 mmHg, the color scale was manually adjusted in the Manoview program and ranged from 0to 300 mmHg. The image analysis program identified the rest, squeeze, and evacuation periods by visualizing the boundaries that demarcate these periods. The rectal balloon pressure was obtained from the greater value of two pressures measured by the rectal balloon sensors. Eight anal sensors that span 5.4 cm were used to calculate the anal pressure. Then, also using R, summary variables were calculated from the 10Hz raw data using the same formulae as the commercial software10. The anorectal pressures at rest, during squeeze and simulated evacuation were considered normal or abnormal with respect to the 10th – 90th percentile age-appropriate values in younger (less than 50y) and older (50y and older) healthy women with a normal BET10.
Data and statistical analysis
The Lin’s concordance correlation coefficient (CCC), paired t tests, and Bland–Altman plots were used to compare the summary variables generated with the ManoView software and the reverse engineering approach11. Data are summarized as Mean ± SD.
RESULTS
Clinical features
Among constipated women, 36 had functional constipation, and 24 had constipation-predominant irritable bowel syndrome. Among FI women, the mean FI severity score (10 ± 1) was suggestive of severe FI. Among180 participants, 22 women (1 healthy woman [2%], 7 [12%] with FI, and 14 [23 %] with DD) had a prolonged BET (> 60s).
Anorectal pressures
The anal resting pressure (79 ± 25 mmHg) was greater than the 90th percentile normal value in 30 women (17%) and lower than the 10th percentile normal value in 11 women (6%). During the first squeeze maneuver, the anal pressure (169 ± 69 mmHg) was reduced in 56 women (31%). During simulated evacuation with an empty balloon, the resting anal pressure (74 ± 27 mmHg) was increased in 44 women (24%), the anal relaxation (5 ± 28%) was reduced in 32 women (18%), the rectal pressure (29 ± 19 mmHg) was reduced in 14 women (8%), and the rectoanal gradient (− 45 ± 29 mmHg) was reduced in 40 women (22%). During simulated evacuation with a filled balloon, the anal pressure (66 ± 27 mmHg) was increased in 25 women (14%), the percent anal relaxation (−7 ± 38 mmHg) was reduced in 68 women (38%), the rectal pressure (139 ± 54 mmHg) was reduced in 60 women (33%), and the rectoanal gradient (73 ± 58 mmHg) was reduced in 43 women (24%).
All anorectal pressures computed by the commercial and reverse engineering methods were significantly correlated (Table 1). Anal resting pressure, maximum squeeze pressure during the three maneuvers and the rectoanal gradient during simulated evacuation with an empty balloon in all three cohort of women were slightly lower when measured with the reverse engineering method as compared to ManoView software. For selected variables, some differences were statistically significant; but numerical differences between the methods were small.
Table 1.
Comparison of Anorectal Pressures – ManoView vs Reverse engineering Approach.
| Controls | DD | FI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter (mmHg) | ManoView, Mean (SD) | Reverse engineering, Mean (SD) | CCC (95% CI) | ManoView Mean (SD) | Reverse engineering,Mean (SD) | CCC (95% CI) | ManoView Mean (SD) | Reverse engineering,Mean (SD) | CCC (95% CI) |
| Rest | |||||||||
| Mean resting pressure | 79 (24) | 78 (25) | 0.98 (0.96, 0.99) |
91 (20) | 88 (18)3 | 0.96 (0.93, 0.97) |
69 (28) | 66 (27)1 | 0.99 (0.98, 0.99) |
| Squeeze 1 | |||||||||
| Maximum squeeze pressure | 193 (62) | 188 (59)1 | 0.99 (0.98, 0.99) |
194 (61) | 189 (56)1 | 0.99 (0.98, 0.99) |
122 (60) | 120 (57)5 | 0.99 (0.99, 0.99) |
| Squeeze 2 | |||||||||
| Maximum squeeze pressure | 183 (59) | 181 (58)2 | 0.99 (0.98, 0.99) |
188 (63) | 183 (61)1 | 0.99 (0.99, 0.99) |
125 (57) | 125 (53) | 0.99 (0.99, 0.99) |
| Squeeze 3 | |||||||||
| Maximum squeeze pressure | 184(60) | 182 (59) | 0.99 (0.98, 0.99) |
179 (60) | 175 (57)1 | 0.99 (0.99, 0.99) |
120 (55) | 119 (54)4 | 0.97 (0.96, 0.98) |
| Simulated evacuation without rectal distention | |||||||||
| Rectal pressure | 27 (18) | 25 (19)2 | 0.93 (0.89, 0.96) |
25 (15) | 24 (15)4 | 0.97 (0.94, 0.98) |
34 (21) | 31 (21)1 | 0.97 (0.96, 0.98) |
| Anal pressure | 63 (19) | 62 (19) | 0.98 (0.97, 0.99) |
87 (24) | 86 (23)2 | 0.98 (0.97, 0.99) |
70 (32) | 69 (32)6 | 0.99 (0.99, 0.99) |
| Rectoanal gradient | −36 (24) | −38 (25) | 0.95 (0.92, 0.97) |
−62 (25) | −62 (23) | 0.98 (0.97, 0.99) |
−37 (30) | −38 (30)7 | 0.99 (0.98, 0.99) |
| Simulated evacuation with rectal distention | |||||||||
| Rectal pressure | 165 (37) | 164 (38) | 0.99 (0.98, 0.99) |
99 (49) | 99 (49 | 0.99 (0.99, 0.99) |
153 (52) | 154 (52) | 0.99 (0.99, 0.99) |
| Anal pressure | 65 (22) | 64 (21) | 0.98 (0.96, 0.98) |
75 (29) | 74 (28) | 0.98 (0.97, 0.99) |
58 (27) | 59 (28) | 0.98 (0.96, 0.99) |
| Rectoanal gradient | 100 (41) | 100 (41) | 0.99 (0.98, 0.99) |
28 (53) | 24 (49) | 0.99 (0.99, 0.99) |
95 (52) | 94 (52) | 0.99 (0.99, 0.99) |
Values are Mean (SD)
1 P = .0001, 2 P = .03, 3 P = .002, 4 P = .05, 5 P = .003, 6 P = .005, 7 P = .01 vs corresponding ManoView value
For the maximum anal squeeze pressure, the Bland Altman test was significant (P = .01), which indicates that the differences between measurements was related to the mean value (Figure 1). The Bland-Altman plots (Figure 1) demonstrate that on average, the new approach overestimated the resting anal pressure by 1.7 ([−11 – 8] mmHg, mean [95% CI]) vs the software-derived value. For anal squeeze pressure, the new approach underestimated the corresponding software value by 3.7 (−9.7 – 17) mmHg vs the software-derived value. For the rectoanal gradient during evacuation without and with rectal distension, the new approach underestimated the corresponding software value by 1 (−9.9 – 12) mmHg and 0.4 (−11 – 12) mmHg. For the mean anal resting pressure, rectoanal gradient during evacuation with an empty and a filled balloon, corresponding values were not significant (Figure 1).
Figure 1. Comparison of anorectal pressures analyzed with the existing (ManoView) and new methods.
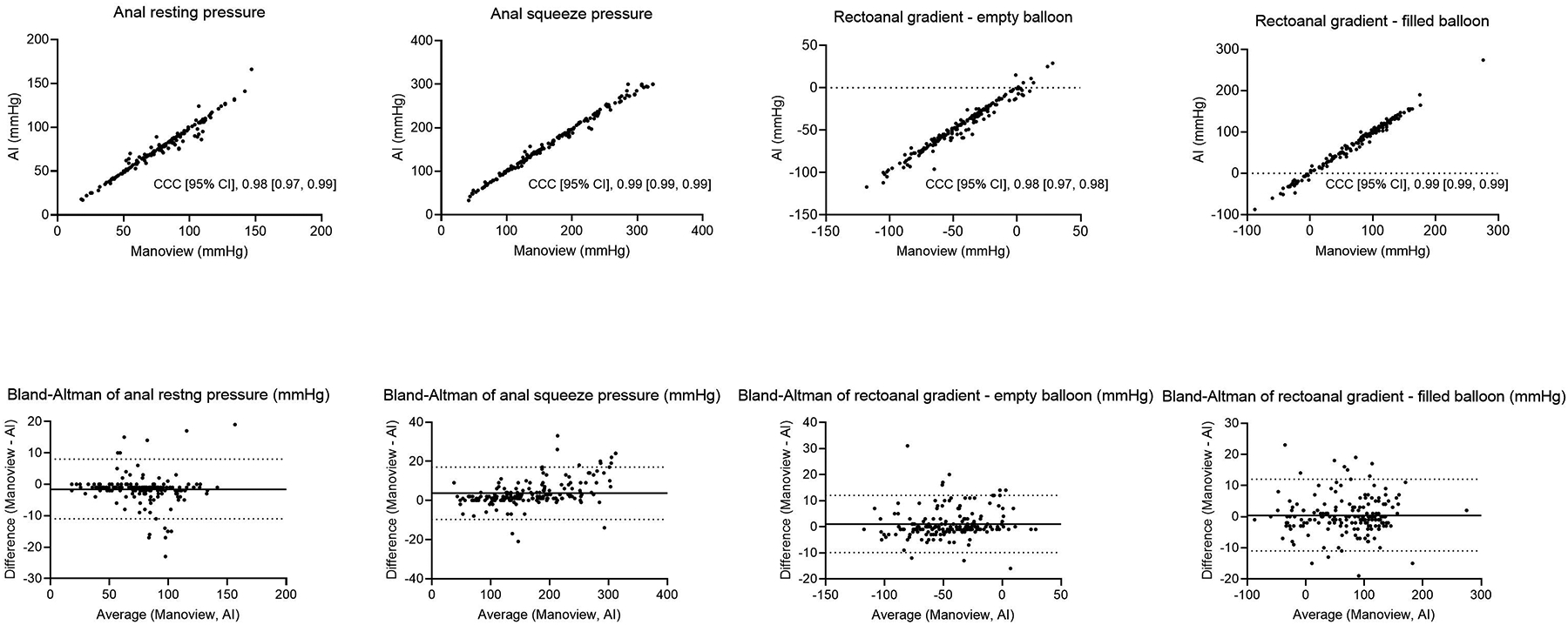
Upper panel displays mean anal resting pressure, maximum anal squeeze pressure, and the rectoanal gradient during evacuation with an empty and a filled balloon. Observe the excellent agreement between pressures measured with the ManoView software and the reverse engineering technique. In the Bland-Altman plots (lower panel), the black dotted lines show the upper and lower limits of agreement for 11.96*standard deviation and the black solid lines show the mean difference. Except for the anal squeeze pressure, the Bland Altman test was not significant. CCC = Concordance Correlation Coefficient
DISCUSSION
These findings demonstrate that anorectal pressures at rest, during squeeze, and simulated evacuation extracted from the color images of pressures in anorectal manometry reports closely approximate the summary variables provided by the commercial software reports. On average, the program takes approximately 10 seconds to extract the data from a single study. Thus, anorectal pressures can be accurately extracted and summarized from images in Word reports.
Because we sought to compare the accuracy of pressures measured by the reverse engineering approach vs the values provided by the program, the same formulae were used to compute the summary pressures (eg, anal mean resting pressure) with both approaches. In future, this reverse engineering approach should facilitate the rapid discovery of newer, potentially more useful, summary HR_ARM variables. For example, consider a study designed to compare the diagnostic utility of anal resting pressures averaged over 10, 20, 30, or 60s for distinguishing between healthy controls and FI patients. If the commercial software were used for this analysis, the observer must analyze each HR_ARM study four times and use the interface to demarcate frames that are 10, 20, 30, or 60s in duration around the resting measurement. Alternatively, the raw data can be transferred to and analyzed in Microsoft Excel. By contrast, with the reverse engineering approach, data for the entire study can be efficiently extracted from reports in 10s, then summarized as necessary.
Most HR-ARM publications emanate from relatively small, single-center studies. The existing reverse engineering approach can be used to combine the data from patients who were studied with the same anorectal probe. With relatively minor software adjustments, it should be possible to combine data acquired with different probes or even esophageal manometry.
This approach has some limitations. When the pressure values are erroneous (eg, due to inaccurate thermal compensation13), the pressures extracted by the reverse engineering program will approximate to the values generated by the software but are nonetheless inaccurate. If the color scale is not manually adjusted to encompass the range of pressures recorded in the study when that is necessary, the program will misinterpret pressures. In some studies, the reverse engineering approach can also identify sensory thresholds during rectal distention (data not shown). However, extracting sensory thresholds is more challenging because the reverse engineering approach relies on using optical character recognition (OCR) to read the balloon volume numbers indicated on the image. If the pixel resolution of the Manoview-generated image is too low, the small font size precludes reliable OCR.
In summary, we have devised a reverse engineering approach to extract pressures accurately and efficiently from color images in anorectal manometry reports and to summarize the pressures obtained thereof.
KEY MESSAGES.
Using a reverse engineering approach, anorectal pressures measured with high resolution manometry were determined by analyzing the color images in these reports.
The summary pressures generated by this reverse engineering approach and commercial software programs were strongly correlated, which demonstrates that the pressures extracted from the reports with the reverse engineering approach are accurate.
This approach can be used to compile HR_ARM datasets across centers and to uncover newer, potentially more useful summary parameters for rectoanal pressure topography.
Funding:
This study was supported by National Institute of Diabetes and Digestive and Kidney Diseases Grant R01 DK78924
ABBREVIATIONS
- BET
balloon expulsion time
- HR_ARM
high resolution anorectal manometry
- ARM
anorectal manometry
- CI
confidence interval
- CCC
concordance correlation coefficient
- DD
defecatory disorder
- FI
fecal incontinence
- SD
standard deviation
Footnotes
Disclosure: Dr. Bharucha jointly holds patents for an anorectal catheter fixation device, anorectal manometry probe, and an anorectal device for fecal incontinence respectively with Medtronic Inc, Medspira Inc, and Minnesota Medical Technologies, receives royalties from Medspira Inc, and an honorarium from GI Supply Inc
REFERENCES
- 1.Bharucha AE, Basilisco G, Malcolm A, et al. A Review of the Indications, Methods, and Clinical Utility of Anorectal Manometry. Neurogastroenterology and Motility. 2022. Feb 27:e14335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Carrington EV, Heinrich H, Knowles CH, et al. The international anorectal physiology working group (IAPWG) recommendations: Standardized testing protocol and the London classification for disorders of anorectal function. Neurogastroenterology and Motility. 2020;32(1):e13679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ang D, Vollebregt P, Carrington EV, Knowles CH, Scott SM. Redundancy in the International Anorectal Physiology Working Group Manometry Protocol: A Diagnostic Accuracy Study in Fecal Incontinence. Dig Dis Sci. 2021;03:03. [DOI] [PubMed] [Google Scholar]
- 4.Oblizajek NR, Deb B, Kathavarayan Ramu S, et al. Optimizing Techniques for Measuring Anal Resting and Squeeze Pressures with High Resolution Manometry Neurogastroenterology and Motility. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sharma M, Muthyala A, Feuerhak K, Narayanan SP, Bailey KR, Bharucha AE. Improving the Utility of High Resolution Manometry for the Diagnosis of Defecatory Disorders in Women with Chronic Constipation. Neurogastroenterology and Motility. 2020. Jul 01:e13910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–1491. [DOI] [PubMed] [Google Scholar]
- 7.Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal disorders. Gastroenterology. 2006;130(5):1510–1518. [DOI] [PubMed] [Google Scholar]
- 8.Noelting J, Zinsmeister AR, Bharucha AE. Validating endpoints for therapeutic trials in fecal incontinence. Neurogastroenterology and Motility. 2016;28(8):1148–1156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chakraborty S, Feuerhak K, Muthyala A, Harmsen WS, Bailey KR, Bharucha AE. Effects of Alfuzosin, an alpha1-Adrenergic Antagonist, on Anal Pressures and Bowel Habits in Women With and Without Defecatory Disorders. Clin Gastroenterol Hepatol. 2019;17:1138–1147, e1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Oblizajek NR, Gandhi S, Sharma M, et al. Anorectal pressures measured with high-resolution manometry in healthy people—Normal values and asymptomatic pelvic floor dysfunction. Neurogastroenterology and Motility : the official journal of the European Gastrointestinal Motility Society. 2019:e13597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Carrasco JL, Jover L. Estimating the generalized concordance correlation coefficient through variance components. Biometrics. 2003;59(4):849–858. [DOI] [PubMed] [Google Scholar]
- 12.Carrington EV, Knowles CH, Grossi U, Scott SM. High-resolution Anorectal Manometry Measures Are More Accurate Than Conventional Measures in Detecting Anal Hypocontractility in Women With Fecal Incontinence. Clinical Gastroenterology & Hepatology. 2019;17(3):477–485.e479. [DOI] [PubMed] [Google Scholar]
- 13.Parthasarathy G, McMaster J, Feuerhak K, Zinsmeister AR, Bharucha AE. Determinants and clinical impact of pressure drift in manoscan anorectal high resolution manometry system. Neurogastroenterology and Motility. 2016;28(9):1433–1437. [DOI] [PMC free article] [PubMed] [Google Scholar]