

Introduction
Suicide is the second most common cause of death of adolescents in the United States,[1] and suicidal ideation (SI) is a major risk factor for suicidal behavior.[2] There are, however, no proven pharmacologic treatments for suicidality in youth,[3] and effective interventions for SI are badly needed. Electroconvulsive therapy (ECT) is an effective treatment for affective disorders, and in adults is associated with a reduction in SI.[4] To assess the generalizability of that adult result to adolescents, this study explores the association between ECT and self-reported SI among adolescents.
Methods
This was a single-center retrospective cohort study of adolescent patients who received ECT from May 2011 to Mar 2020 and who self-reported symptoms using the Quick Inventory of Depressive Symptomatology Self-Report 16-item scale (QIDS).[5] QIDS scores were reported by participants at baseline and following treatment #5 and treatment #10. Patients were included in the analysis if they provided baseline QIDS data and at least one post-treatment score (following treatment #5 or treatment #10). Consistent with World Health Organization definitions, adolescence includes individuals through age 19, and so the study cohort includes patients aged 16 to 19. Self-reported SI was assessed based on item 12 of the QIDS, which asks about “thoughts of death or suicide” during the past 7 days on a 4-point scale of: 0 “I do not think of suicide or death”; 1 “I feel that life is empty or wonder if it’s worth living”; 2 “I think of suicide or death several times a week for several minutes”; 3 “I think of suicide or death several times a day in some detail, or I have made specific plans for suicide or have actually tried to take my life.” A score of 0 was defined as the absence of suicidal ideation, and a score of 3 was defined as severe suicidal ideation.
All patients received ECT using a Mecta Spectrum 5000Q (Tualatin, OR), with initial right unilateral electrode placement with individualized seizure threshold determination at time of first treatment, as reported previously.[6,7] Subsequent suprathreshold treatments given at a default schedule of thrice weekly.[8] All patients received succinylcholine muscle relaxant and general anesthesia with methohexital as the default agent although propofol, etomidate, or ketamine could also be used.
For the primary statistical analysis, the difference in the self-reported SI between baseline and following the last reported post-treatment score (treatment #5 or treatment #10) was compared using the Wilcoxon matched-pairs signed rank test using GraphPad Prism (version 9, San Diego, California). The proportion who reported any SI (scores > 0) were compared at baseline and last follow-up using McNemar’s text, as were the proportion reporting severe SI (score of 3). All tests were two-tailed, with results with p < 0.05 considered significant. This study was approved by the Mass General Brigham Institutional Review Board with a waiver of informed consent.
Results
In total, 126 adolescents received ECT during the study period, of whom 108 (64 female; 59.3%) met inclusion criteria by providing at least one follow-up QIDS score, and were included in the analysis (Table S1). Mean age was 18.1±1.0 years, and diagnoses were major depressive disorder (86; 79.6%), bipolar disorder (13; 12.0%), and other (9; 8.3%). Treatments began while inpatient for 51 (47.2%) and outpatient for 55 (50.9%). Demographically, 96 patients (88.9%) self-identified as white, while 9 (8.3%) identified as Asian and 2 (1.9%) as black. Four patients (3.7%) endorsed Latino/Latina ethnicity and 50 (46.3%) did not; ethnicity data were missing for 54 patients (50.0%). At baseline all patients were treated with right unilateral ECT, with 105 (97.2%) receiving ultrabrief pulse treatment (pulse width < 0.5 ms).
In total, 24 patients (22.2%) had a last reported QIDS following treatment #5, and 84 patients (77.8%) reported the QIDS following treatment #10. Treatments #5 and #10 occurred a mean of 12.8±3.9 days and 27.7±6.3 days, respectively, following initial treatment. At the time of last treatment, 7 patients (2.8%) were receiving bilateral ECT and 32 (29.6%) were receiving brief pulse treatments, while 76 (70.4%) received right unilateral ultrabrief treatment.At baseline, 96 patients (88.9%) self-reported SI on the QIDS, with 32 (29.6%) reporting severe SI (Figure 1, top). Following ECT treatment, there was a reduction in the number of patients reporting SI to 62 (57.4%) (McNemar’s test; p < 0.001). There was a corresponding reduction in the number of patients reporting severe SI to 13 (12.0%) (McNemar’s test; p = 0.001). Overall the median reduction in SI over 10 treatments was −1 point on the 5 point scale (p < 0.001; Wilcoxon matched-pairs signed rank test) (Figure 1, bottom). No patients who began ECT without SI reported SI at their last follow-up QIDS assessment. Changes in SI during ECT treatment were correlated with overall change in QIDS (Spearman r = 0.55; 95% CI: 0.40 to 0.68; p < 0.001) (Figure S1). The change in SI was not significantly different among patients with changes in ECT parameters (e.g. from ultrabrief pulse to brief pulse or unilateral to bilateral) compared to those with no parameter changes (Mann-Whitney U; p = 0.882).
Figure 1:
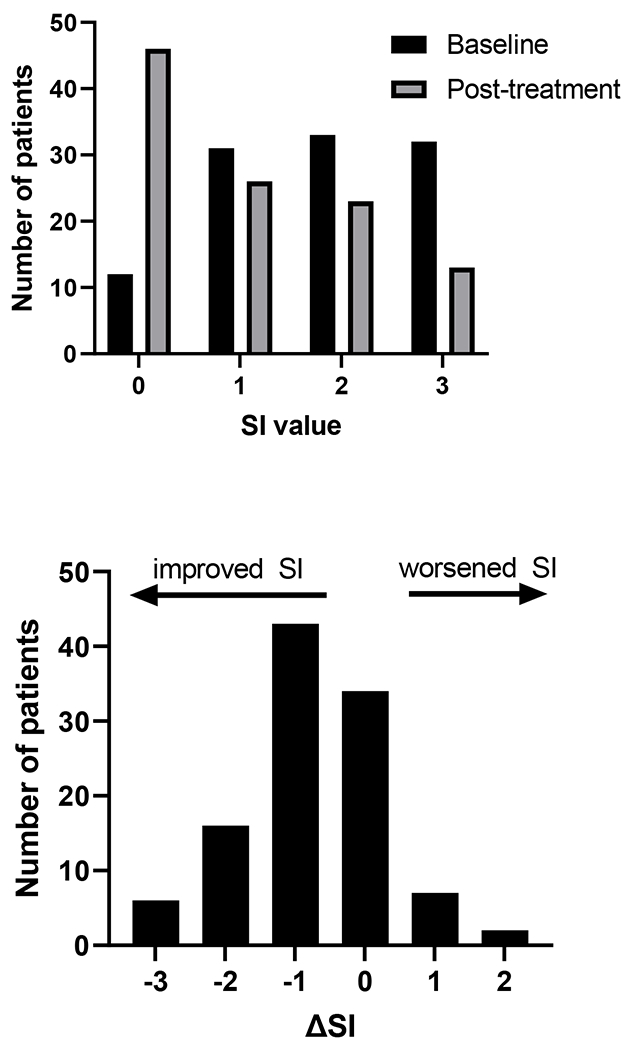
top: distribution self-reported SI at baseline (black) and following ECT treatment (gray). bottom: histogram of change in self-reported SI among individual patients from baseline to following treatment #5 or #10. Negative numbers representing improvement in SI, and positive numbers representing worsening of SI.
Discussion
In this sample of 108 adolescents, 96 of whom reported baseline SI, ECT was associated with a significant reduction in self-reported SI over the course of 5-10 treatments. There was an increase in the proportion of patients not reporting SI by the end of treatment, as well as a reduction in the proportion of patients reporting the most frequent SI symptoms. Improvements in SI were moderately correlated (Spearman r = 0.55) with overall change in QIDS, meaning that while improvements in SI were associated with changes in overall depressive symptoms, some patients had improvement or worsening of suicidality without broader changes in depression symptoms.
At present, there is little evidence for pharmacologic treatments for the treatment of self-harm behaviors[3] or suicidal ideation[9] in adolescents, with only psychotherapeutic techniques showing evidence of efficacy. Prior research has demonstrated the efficacy and tolerability of ECT to be equal in adolescents and young adults,[10] but despite this fewer than 1% of ECT treatments in the US are given to patients younger than 18,[11] and access to the procedure is legally restricted for adolescents in 21 states. These results suggest that such legal restrictions may be hampering access to a promising treatment for acute SI in youth.
Strengths of this study include its large sample size, with broad inclusion criteria making the sample more likely to be representative of typical clinical practice. Limitations of this study include its retrospective observational nature without control group, which prevents determination of causality. We are unable to control for the effects of concomitant pharmacologic or psychotherapeutic treatments occurring during ECT treatment, which may confound the influence of ECT on self-reported SI. Moreover, 18 adolescents who began ECT did not report a follow-up suicide assessment and were not analyzed, and we are unable to analyze potential effects of ECT on suicidality among these patients. Additionally, while our study records self-reported suicidal ideation, we do not have data regarding suicidal behaviors or suicide attempts among patients, which limits the generalizability of findings. Finally, we are unable to assess changes in SI following discontinuation of ECT, and so the durability of these improvements is unknown.
Supplementary Material
Funding
This work was supported by the National Institute of Mental Health (T32MH112485, JL; R01MH120991, THM; 5R01MH112737-03, MEH) The sponsors had no role in study design, writing of the report, or data collection, analysis, or interpretation.
Conflicts of Interest
THM receives research funding from the Stanley Center at the Broad Institute, the Brain and Behavior Research Foundation, National Institute of Mental Health, National Human Genome Research Institute Home, and Telefonica Alfa. The remaining authors have no disclosures to report.
Bibliography
- [1].Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. 2019. [Google Scholar]
- [2].Glenn CR, Nock MK. Improving the Prediction of Suicidal Behavior in Youth. Int J Behav Consult Ther 2014;9:7–10. [PMC free article] [PubMed] [Google Scholar]
- [3].Witt KG, Hetrick SE, Rajaram G, Hazell P, Taylor Salisbury TL, Townsend E, et al. Interventions for self-harm in children and adolescents. Cochrane Database Syst Rev 2021;3:CD013667. 10.1002/14651858.CD013667.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Fink M, Kellner CH, McCall WV. The Role of ECT in Suicide Prevention. The Journal of ECT 2014;30:5–9. 10.1097/YCT.0b013e3182a6ad0d. [DOI] [PubMed] [Google Scholar]
- [5].Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry 2003;54:573–83. 10.1016/s0006-3223(02)01866-8. [DOI] [PubMed] [Google Scholar]
- [6].Luccarelli J, McCoy THJ, Seiner SJ, Henry ME. Total Charge Required to Induce a Seizure in a Retrospective Cohort of Patients Undergoing Dose Titration of Right Unilateral Ultrabrief Pulse Electroconvulsive Therapy. The Journal of ECT 2021;37:40–5. 10.1097/YCT.0000000000000714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Luccarelli J, McCoy TH, Seiner SJ, Henry ME. Charge required to induce a seizure during initial dose titration using right unilateral brief pulse electroconvulsive therapy. Brain Stimulation: Basic, Translational, and Clinical Research in Neuromodulation 2020;13:1504–6. 10.1016/j.brs.2020.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Luccarelli J, McCoy TH, Shannon AP, Forester BP, Seiner SJ, Henry ME. Rate of continuing acute course treatment using right unilateral ultrabrief pulse electroconvulsive therapy at a large academic medical center. Eur Arch Psychiatry Clin Neurosci 2021;271:191–7. 10.1007/s00406-020-01202-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Kothgassner OD, Robinson K, Goreis A, Ougrin D, Plener PL. Does treatment method matter? A meta-analysis of the past 20 years of research on therapeutic interventions for self-harm and suicidal ideation in adolescents. Borderline Personality Disorder and Emotion Dysregulation 2020;7:9. 10.1186/s40479-020-00123-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Luccarelli J, McCoy TH, Uchida M, Green A, Seiner SJ, Henry ME. The Efficacy and Cognitive Effects of Acute Course Electroconvulsive Therapy Are Equal in Adolescents, Transitional Age Youth, and Young Adults. J Child Adolesc Psychopharmacol 2021;31:538–44. 10.1089/cap.2021.0064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Luccarelli J, Henry ME, McCoy TH. Demographics of Patients Receiving Electroconvulsive Therapy Based on State-Mandated Reporting Data. J ECT 2020;36:229–33. 10.1097/YCT.0000000000000692. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.