

Abstract
Understanding whether and how the absence of positive relationships may predict longer-term physical health outcomes is central to building a working conceptual model of the interplay of social and physical development across the lifespan. This study sought to examine the extent to which difficulties establishing positive social relationships from adolescence onward serve as long-term predictors of low adult vagal tone, which in turn has been linked to numerous long-term health problems. A diverse community sample of 141 individuals was followed via multiple methods and reporters from age 13 to 29. Across this span, social relationship quality was assessed via close friend and peer reports, observations of romantic interactions, and self-reported romantic relationship satisfaction. A range of potential personality and functional covariates was also considered. Vagal tone while at rest was assessed at age 29. Adult vagal tone was predicted across periods as long as 16 years by: adolescents’ difficulty establishing themselves as desirable companions among peers; early adults’ inability to establish strong close friendships; and lack of warmth in romantic relationships as an adult. Poor early adult friendship quality statistically mediated the link from adolescent peer difficulties to adult vagal tone. A range of potential confounding factors was examined but was not linked to vagal tone. Within the limits of the correlational design of the study, robust connections between adult vagal tone and social relationship quality from adolescence onward suggest at least a possible mechanism by which relationship difficulties may get ‘under the skin’ to influence future physiological functioning.
Keywords: Vagal tone, Social relationships, Romantic relationships, Adolescence, Close friendships, Longitudinal follow-up
Introduction
Struggles to establish positive peer relationships in adolescence and young adulthood have been linked to numerous mental health difficulties (Bagwell et al., 2001; Zimmer-Gembeck et al., 2016), but evidence is growing that these struggles may also have long-term implications for physical health into adulthood (Allen et al., 2015, 2017). Increasing our understanding of whether and how the absence of positive relationships actually gets ‘under the skin’ to predict longer-term physical outcomes is central to building a working conceptual model of the interplay of social and physical development across the lifespan. If long-term links between a lack of positive adolescent social relationships and adult health exist and can be identified, these would suggest both the importance of these (often trivialized) adolescent relationships as well as potential routes for intervention to enhance physical health outcomes across the life course.
One mechanism by which absence of positive social relationships appears likely to potentially influence long-term health is via its impact on the parasympathetic nervous system. This system plays a key role in adaptively downregulating stress responses under conditions of perceived safety. This downregulation capacity, referred to as vagal tone, provides the organism with a reserve to handle stressful situations while also serving to down-regulate key physiological functions ranging from heart rate to blood pressure (Porges, 2007, 2020). Vagal tone is most frequently conceptualized and measured in terms of respiratory sinus arrythmia when at rest—a marker of the extent to which the parasympathetic system controls heart rate via a central respiratory generator (Smith et al., 2020). Dysfunction of this down-regulation process (i.e., low vagal tone), creates the equivalent of a chronic, low-grade state of ‘fight or flight’ preparation which has been linked to a broad range of negative health outcomes, up to and including all-cause mortality (Binkley et al., 1991; Braune & Geisendörfer, 1995; Christensen et al., 1999; Porges, 2007; Schroeder et al., 2003; Thayer & Lane, 2007; Thayer et al., 2010; Ziegler et al., 2001).
Equally importantly, a growing body of evidence suggests that vagal tone is likely to be influenced by the quality of an individual’s social relationships and social experiences. The generalized unsafety theory of stress posits that vagal tone will be reduced under conditions of threat (Brosschot et al., 2017). In the context of actual danger, this reduction in vagal tone is useful in facilitating adaptive stress responses (e.g., fight or flight) (Maier & Watkins, 1998). Several studies, for example, have found short-term links between situational changes in perceptions of threat vs. safety and corresponding short-term changes in vagal tone (Brosschot et al., 2016, 2017; Smith et al., 2020). Social baseline theory suggests that the absence of supportive others violates the default expectations of the brain, and is thus likely to create at least a mild degree of heightened experience of threat (Coan & Sbarra, 2015). A range of studies, from cross-sectional to longitudinal, has linked vagal tone to social relationship qualities. The presence of positive friendships has been linked cross-sectionally to higher resting vagal tone (Holt-Lunstad et al., 2007). Conversely, positive social connections have also been found to predict increased vagal tone in studies following adults over periods ranging from nine weeks to five months (Gouin et al., 2015; Kok & Fredrickson, 2010). Increases in marital satisfaction have been found to predict increases in vagal tone across durations as long as ten years (Donoho et al., 2015).
But why would adult vagal tone be influenced by adolescent experiences? Several lines of reasoning suggest that struggles with peer relationships beginning at least as early as adolescence have the potential to predict problematic long-term outcomes in terms of vagal functioning. The combination of hormonal changes, neural development, and social stressors in adolescence makes this one of the most intensely social, yet also intensely lonely and stressful periods of the lifespan (Albert et al., 2013; Charles et al., 2001; Steinberg & Monahan, 2007). Similarly, the cognitive development occurring during this period is increasing the capacity for self-awareness and for awareness of one’s relative social standing (Blakemore & Mills, 2014). The adolescent is thus exposed to intense social stress at a uniquely impressionable age in ways that may influence perceptions of the likely availability of supportive others going forward. Adolescence also appears to be a period in which the stress response system may be particularly plastic (Romeo, 2010). Given growing brain functional connectivity across this period, adolescence has been posited as a ‘switch point’ for the calibration of stress responsivity (Gee et al., 2013; Goff et al., 2013; McEwen, 2007). Chronic stress exposure may even have the potential to alter metabolic systems and anatomic structures related to stress responding in a relatively permanent way (Ben-Shlomo & Kuh, 2002). Alternatively, adolescent struggles to form positive relationships with peers may predict future health outcomes primarily because they forecast continued struggle to form positive peer and romantic relationships into adulthood (Ben-Shlomo & Kuh, 2002; Oudekerk et al., 2015). A lifespan approach to understanding physical health suggests a need to consider both of these developmental pathways in understanding links between social relationship qualities and life course health outcomes (Uchino, 2009). To date, neither perspective has received significant empirical attention with regard to the long-term implications of a lack of positive peer relationships in adolescence.
This fifteen-year multi-method, prospective study examined lack of positive peer relationships from adolescence onward as a predictor of levels of adult resting vagal tone. A developmental model was assessed in which lack of positive peer relationships in middle adolescence was viewed as predicting low adult vagal tone, both directly but also as mediated via a cascade of future markers of difficulty establishing successful peer and romantic relationships. At each developmental epoch examined, the indicators employed were those considered most salient for the given stage. Hence, in adolescence, desirability as a companion was assessed within the broader peer group, along with peer-reported close friendship quality, as both have been linked to positive social adjustment (Allen et al., 2005a; Narr et al., 2019). In early adulthood, close friendship quality was again assessed, as it is considered the most stage salient marker of social adaptation for this developmental epoch (Furman & Collibee, 2014). Given the gradually increasing salience of romantic relationships during this period (Roisman et al., 2004), however, warmth of romantic partner behavior was also considered for the first time. Later in adulthood, close friendship quality was again assessed, but the primary theoretical focus shifted to warmth expressed by a romantic partner, which has been linked in adulthood, both concurrently and longitudinally to both physical health outcomes and specifically to vagal tone (Donoho et al., 2015; Robles et al., 2014).
To reduce both confounds and biases from self-reports (e.g., low vagal tone leading to more negative self-reports), all constructs were assessed via either peer reports or observational assessment. In addition, because low vagal tone has been associated with poor emotion regulation and social functioning (Beauchaine & Thayer, 2015; Porges, 2007; Sack et al., 2004), we also examined several possible alternative explanations for any associations observed (e.g., low vagal tone causing poor peer relations via problematic emotion regulation). We did not have a measure of vagal tone at baseline, however we were able to assess the potential role of several indicators of emotion regulation difficulties in adolescence and early adulthood, including depressive symptoms, state, trait, and social anxiety, externalizing behavior, social problem-solving competence, and trait neuroticism. In addition, given evidence of potential sex differences and effects of family income (Johnson et al., 2017; Koenig & Thayer, 2016) we also controlled for these.
Using this approach, a diverse community sample was used to assess the following specific predictions regarding links between adult vagal tone and peer relationships from adolescence into adulthood:
Lower resting vagal tone assessed in terms of respiratory sinus arrhythmia at age 29 will be best predicted by lack of desirability as a companion among peers and lower quality friendships at ages 13–17, by lower quality close friendships at ages 23–26, and by lack of observed romantic partner warmth at age 27.
Predictions will remain after accounting for potential confounding factors, including adolescent depressive symptoms, trait and social anxiety, and adult levels of neuroticism.
A mediational model, positing both direct effects from adolescent social experiences to adult vagal tone and effects mediated via early adult friendship and romantic relationship qualities will best account for the findings.
Methods
Participants
This report is drawn from a larger longitudinal investigation of adolescent peer influences on adult development. The final sample of 141 participants who had levels of vagal tone assessed at age 29 was a subsample of 184 participants initially assessed at age 13 (an attrition rate of 1.4% per year across 16 years). The final sample included 57 males and 84 females and was racially/ethnically and socioeconomically diverse and representative of the community from which it was drawn: 82 participants (58%) identified themselves as Caucasian, 42 (30%) as African American, 1 (1%) as Hispanic, 2 (1%) as Asian, 1 (1%) as American Indian, and 13 (9%) as of mixed or other race/ethnicity. Adolescents’ parents reported a median family income in the $40,000—$59,999 range at the initial assessment. Adolescents were recruited from the 7th and 8th grades of a public middle school drawing from suburban and urban populations in the Southeastern United States. Information about the study was provided via an initial mailing to parents with follow-up presentations to students at school lunches. Formal recruitment took place via telephone contact with parents. Students who had already served as close peer informants in the study were not eligible to serve as primary participants. Of students eligible for participation, 63% of adolescents and parents agreed to participation when parents were contacted. Adolescents provided informed assent before each interview session, and parents and adult participants provided informed consent. Interviews took place in private offices within a university academic building.
Assessments in this study were obtained at mean ages 13.3 (SD = 0.64), 14.2 (SD = 0.76), 15.1 (SD = 0.80), and 16.3 (SD = 0.88) for adolescent close friend and sociometric measures; 18.3 (SD = 1.06) and 19.6 (SD = 1.08) for anxiety measures; 23.7 (SD = 0.98), 24.6 (SD = 0.95), 25.6 (SD = 0.99), 26.6 (SD = 1.01) for adult close friend reports; 23.99 (SD = 1.12) and 27.4 (SD = 0.1.44) for observed romantic partner behaviors; and 28.7 (SD = 1.18) for vagal tone assessment. For the close friend reports, participants nominated their closest friend to be included in the study (not necessarily the same friend across ages). Close friends in adolescence reported that they had known participants for an average of 4.3 to 5.7 years (SD = 3.1 to 3.8) across the various assessment periods; close friends in adulthood similarly reported that they knew participants for an average of 10.3 to 11.2 years (SD’s = 6.6 to 7.1). Romantic partner observations were obtained for participants who were in a relationship of at least three months duration and in which the romantic partner was willing to come into our offices for an observational assessment. For sociometric assessments, all 141 participants had data available for at least one point; for close friend reports, 136 participants had data available for at least one point; for age 27 romantic relationship observations, 82 participants had available observational data.
Attrition analyses
Attrition analyses examined missing data for each type of data available at baseline. Females were more likely than males to have completed the age 29 vagal tone assessment (85% continuation rate for females vs. 67% for males, p = 0.005). There were no other attrition effects related to completing vs. not completing this assessment. There were also no attrition effects for presence vs. absence of observational romantic partner data at age 27. To best address any potential biases due to attrition in longitudinal analyses or missing data within waves, full information maximum likelihood (FIML) methods were used with analyses including all variables that were linked to future missing data (i.e., where data were not missing completely at random). Because these procedures have been found to yield the least biased estimates when all available data are used for longitudinal analyses (vs. listwise deletion of missing data) (Arbuckle & Schumaker, 1996), the entire original sample was utilized for these analyses. This full sample thus provides the best possible estimates of variances and covariances in measures of interest and was least likely to be biased by missing data.
Procedure
In the initial introduction and throughout all sessions, confidentiality was assured to all study participants and adolescents/adults were told that no one would be informed of any of the answers they provided. Participants’ data were protected by a Confidentiality Certificate issued by the U.S. Department of Health and Human Services, which protected information from subpoena by federal, state, and local courts. Transportation and childcare were provided if necessary. Adolescent/adult participants and participants’ peer and romantic reporters were all paid for participation. Informed consent was obtained from all participating adults. Adolescents provided informed assent and their parents provided informed consent on their behalf.
Measures
Primary measures
Vagal Tone (Age 29)
Vagal tone was assessed in terms of heart interbeat intervals obtained from an electrocardiogramwhile participants were resting in a comfortable chair, watching a soothing outdoors video for ten minutes (Cacioppo et al., 1995; Kirschbaum et al., 1993). Heart rate was continuously monitored (with sampling at 1 kHz) using a Mindware 2000D module. Five-lead electrodes were placed according to standard ECG placement recommendations (Hoetink et al., 2002) and each waveform was verified or edited prior to analyses. RSA was calculated based on the digitized inter-beat-intervals. Following linear detrending, the heart period time series was band pass filtered from 0.12 to 0.40 Hz (Berntson et al., 1993; Litvack et al., 1995). The power spectrum of the heart period time series was calculated using a Fast Fourier Transform and scaled to ms2/Hz. RSA was calculated as the natural log of the area under the heart period power spectrum within the corner frequencies of the band pass filter (Litvack et al., 1995). RSA was calculated on a minute by minute basis and averaged across the last 3 min to increase measurement reliability (Berntson et al., 1997).
Desirability as a companion (Ages 13–16)
Adolescents’ capacity to establish themselves as desirable social companions with a range of their peers was assessed using a limited nomination sociometric procedure. Each adolescent, their closest friend, and two other target peers were asked to nominate up to 10 peers in their grade with whom they would “most like to spend time on a Saturday night.” When these ratings were combined across the entire sample of participants and their peers, a large cohort of peer nominators was thus obtained. This study used grade-based nominations (e.g., students could nominate anyone in their grade at school) rather than classroom-based nominations due to the age and classroom structure of the school that all participants attended. As a result, instead of friendship nominations being done by 15–30 children in a given classroom, each teen’s nominations were culled from among 72 to 146 teens (depending on the teen’s grade level). These nominators comprised approximately 38% of the entire student population in these grades). All participating students in a given grade were thus potential nominators of all other students in that grade, and an open nomination procedure was used (i.e. students were not presented with a roster of other students in their school, but instead wrote in names of liked and disliked students). Students used this procedure easily, producing an average of 9.1 liking nominations (out of 10). The raw number of ‘like’ nominations each teen received was standardized within grade level as a measure of desirability as a social companion in the broader peer group following the procedure described in Coie et al. (Coie et al., 1982). This approach to assessing social acceptance has been previously found to be relatively stable over time and related to adolescent attachment security, qualities of positive parental and peer interactions, and short-term changes in levels of deviant behavior (Allen et al., 2005a, 2007; McElhaney et al., 2008). Scores for each year were standardized and summed together to produce a score for aggregate desirability across adolescence.
Close friendship quality (Ages 13–16)
Each year from age 13 to 17, close friends rated participants on their competence at establishing and maintaining a strong close friendship, using the 4-item friendship competence scale from the Adolescent Self-Perception Profile (Harter, 1988). Although the scale was originally labelled as ‘close friendship competence,’ examination of the items suggests that it is better conceptualized as a measure of the quality and intimacy of the adolescent’s close friendships. Items focused, for example, on extent to which teen had ‘a close friend they share secrets with,’ ‘a friend close enough to share really personal thoughts with,’ and a ‘really close friend to share things with.’ Results were averaged across the four years to produce the final scale. Internal consistency was good (Cronbach’s α’s ranged from 0.70 to 0.86 within years).
Close friendship quality (Ages 23–26, 28–29)
Each year from age 23 to 26 and from 28 to 29, close friendship quality was assessed by asking close friends of participants to complete the three-item overall satisfaction scale from the Network of Relationships Inventory (Furman & Buhrmester, 1985) about their current friendship with the participant. All items are scored on a 5-point Likert scale. Internal consistency was excellent (Cronbach’s α = 0.89 to 0.94 across years). Scores were averaged across ages 23–26 to obtain an early adult aggregate measure and age 28–29 to obtain an adult aggregate measure of the quality of the participant’s closest friendship as rated by that friend.
Romantic partner warmth (Age 24, 27)
Target participants and their romantic partners participated in a revealed differences task at each age in which they discussed an issue in their relationship that they had separately identified as an area of disagreement. The discussion began with target participants playing a recording they had made separately with the interviewer describing the problem and their perspective on it. Typical topics of discussion included money, jealousy, moving, friends, and career issues. These interactions lasted 8 min and were videotaped, transcribed and coded with the Autonomy and Relatedness Coding System for Adolescent-Romantic Partner Interactions (Allen et al., 2005b). Partners’ displayed warmth toward participants was coded in terms of behaviors such as genuine smiles, friendly jokes, and validation of the other person’s statements, using an anchored 0–4 point scale with half point intervals. Interrater reliability was in the excellent range (ICC’s range from = 0.79 to 0.88).
Covariates
Body mass index (BMI, Age 29)
BMI was assessed at the age 29 assessment. Height (in meters) and weight (in kilograms) were assessed with light clothing and BMI was calculated using the standard formula BMI = weight / height2, which was then log-transformed.
Adolescent depressive symptoms
(Ages 13–16) were assessed annwually at ages 13 to 16 with results averaged across ages to yield an overall measure. Participants reported the degree of their depressive symptoms using the Child Depression Inventory (Kovacs & Beck, 1977). This 27-item inventory is based on the Beck Depression Inventory and has been well-validated as a measure of depressive symptomatology linked to poor self-esteem, hopelessness, and negative cognitive attributions (Kazdin, 1990). Internal consistency for this measure was good (Cronbach’s α’s ranged from 0.84 to 0.87).
Social problem-solving competence (Ages 13–16)
A shortened version of the Adolescent Problem Inventory (Freedman et al., 1978) was used to assess adolescents’ social problem-solving competence by examining how effectively participants were able to respond to a variety of socially challenging situations (e.g., confrontations with peers and parents, opportunities to engage in deviant behavior, etc.). In this analogue/test measure, adolescents provided their most likely responses to a series of hypothetical vignettes. Adolescent responses were audio-recorded and then rated by coders unfamiliar with other data from the study on a 0 to 10 scale in terms of competence of the response. Interrater reliability, calculated using the intraclass correlation coefficient, was in what has been labelled the “excellent” range for this statistic (ICC = 0.87) (Cicchetti & Sparrow, 1981). Slightly different items were used for each year of administration and scores were aggregated across the three-years to yield an overall measure of competence.
Early adolescent anxiety symptoms (Age 15, 16)
Anxiety was assessed using the Beck Anxiety Inventory (BAI), which consists of 21 items in which participants were asked to rate their experience over the past week of anxiety symptoms on a four-point scale ranging from 0 to 3: 0 = not at all; 1 = mildly (it did not bother me that much); 2 = moderately (it was very unpleasant, but I could stand it); 3 = severely. Internal consistency was high (Cronbach’s α = 0.90–0.94), and the total anxiety score was aggregated across the two years of assessment to yield the overall measure.
Late adolescent anxiety symptoms (Age 18, 20)
The 20-item trait anxiety scale from the State-trait anxiety inventory (Spielberger et al., 1999) was used to measure stable individual differences in anxiety proneness. Responses used a 4-point Likert scale to which participants indicated their agreement to statements such as “I worry too much over something that doesn’t really matter.” The overall trait anxiety scale has demonstrated strong psychometric properties and external validity (Spielberger et al., 1999), and internal consistency for the scale in this study was high (Cronbach’s α’s = 0.89 and 0.90). Scores were averaged across the two assessment periods.
Late adolescent social anxiety (Age 18, 20)
The Social Anxiety Scale for Adolescents (Greca & Lopez, 1998) is a 22-item scale measuring fear of negative evaluation, social avoidance and distress in new situations, and general social avoidance and distress. The total social anxiety scale was created by summing across these items and had good internal consistency (Cronbach’s α = 0.94 at both ages).
Adolescent externalizing behavior (Age 14, 16, 18)
Reports about target adolescents by mothers and fathers using the Child Behavior Checklist (Achenbach & Edelbrock, 1991; Lizotte et al., 1992). Cronbach’s α for both mothers’ and fathers’ reports ranged from 0.84 to 0.89 across assessment waves. Scores were averaged across parents and across years to yield a summary score for adolescent-era externalizing behavior.
Neuroticism
(Age 24) was assessed using the 10-item neuroticism scale from the International Personality Item Pool (Goldberg et al., 2006), using a 5-point Likert-scale. This measure has previously demonstrated strong internal consistency, retest reliability, convergence with longer Big Five personality measures, and self-peer agreement (Goldberg et al., 2006). For this sample internal consistency for the scale was good (Cronbach’s α = 0.89).
Loneliness
(Ages 24, 27) was assessed via the UCLA Loneliness Scale (Russell et al., 1980). This 20-item measure assesses loneliness using responses on a 4-point Likert-scale. Scores have been related to outcomes ranging from lower life satisfaction to attachment insecurity (Bowlby, 1969; Goswick & Jones, 1982; Kobak & Sceery, 1988; Moore & Schultz, 1983). Internal consistency for this scale was good (Cronbach’s α = 0.97).
Statistical analyses
For all primary analyses, SAS PROC CALIS (version 9.4, SAS Institute, Cary, NC) was employed using full information maximum likelihood handling of missing data for assessment of key relations in hierarchical regression or path models. Initial analyses were conducted separately for baseline income in adolescents’ family of origin, and current adult body mass index. Follow-up analyses considered the effect of a range of potential covariates/confounding factors, followed by examination of a path model considering the potential mediating role of adult relationship qualities on the link between adolescent peer relationship qualities and adult vagal tone.
Results
Preliminary analyses
Means, standard deviations and intercorrelations for all substantive variables examined are presented in Table 1. Given initial findings suggesting relations of gender and baseline family income to other variables in the study, and similar findings in the existing adult literature (Johnson et al., 2017; Koenig & Thayer, 2016), gender and baseline family income were included as covariates in all analyses. We also examined possible moderating effects of these factors on each of the relationships described in the primary analyses below.
Table 1.
Univariate statistics and intercorrelations among primary constructs
| Mean | SD | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Vagal Tone | 6.18 | 1.25 | 0.30*** | 0.11 | 0.26** | 0.21 | 0.08 | 0.30** | − 0.33*** | − 0.04 | 0.08 |
| 2. Desirability as a peer companion | 0.78 | 1.06 | – | 0.18* | 0.22** | 0.44** | 0.18* | 0.26* | − 0.27*** | − 0.07 | 0.40*** |
| 3. Close friendship quality | 13.4 | 1.78 | – | .16* | −.02 | .11 | −.06 | −.07 | .17* | .03 | |
| 4. Close friendship quality | 12.83 | 1.90 | – | 0.10 | 0.60*** | 0.14 | − 0.04 | 0.09 | 0.04 | ||
| 5. Romantic partner warmth | 1.93 | 0.78 | – | 0.11 | 0.42*** | − 0.26* | − 0.13 | 0.26* | |||
| 6. Close friendship quality | 12.8 | 2.06 | – | 0.10 | 0.03 | 0.21** | 0.03 | ||||
| 7. Romantic partner warmth | 1.67 | 1.06 | – | − 0.13 | 0.03 | 0.29** | |||||
| 8. Body Mass Index | 27.32 | 8.17 | – | 0.13 | − 0.15 | ||||||
| 9. Adolescent gender (1-Male; 2-Female) | – | – | – | − 0.12 | |||||||
| 10. Family income | 6.10 | 1.96 | – |
p < 0.05
p < 0.01
p < 0.001
Moderating effects were assessed by creating interaction terms based on the product of the centered main effect variables. No moderating effects of gender or income were found for any of the analyses reported below.
Given missing data with respect to romantic partner warmth, we also examined whether the presence vs. absence each developmental stage. We first examined two potential indicators of social relationship quality—sociometrically-assessed desirability as a social companion to peers and close friend reported participant close friendship competence—in early and mid-adolescence as predictors of vagal tone at age 29. Models also accounted for adolescent gender, of a romantic partner was linked to adult vagal tone. No such relationship was observed at either the early adult or adult assessment period (p’s > 0.40).
Primary analyses
Hypothesis 1: Lower resting vagal tone at age 29 will be best predicted by lack of desirability as a companion and lower quality close friendships among peers at ages 13–17, by lower quality close friendships at ages 23–26, and by lack of observed romantic partner warmth at age 27.
Results, presented in Model 1 in Table 2, indicate that absence of desirability as a peer companion across ages 13–16 was predictive of lower adult vagal tone at age 29. Next, similar analyses examined effects of close friendship quality and observed warmth in romantic relationships in early adulthood as predictors of future vagal tone. As shown in Model 2 in Table 2, poor close friendship quality was a significant predictor of low vagal tone in this model. Finally, Model 3 in Table 2 shows the effects of concurrent and near concurrent peer and romantic relationship qualities on vagal tone. Specifically, absence of observed partner warmth in romantic relationships was linked to lower vagal tone.
Table 2.
Hierarchical regression models examining vagal tone prediction from relationship qualities in different developmental epochs
| Vagal Tone (age 29) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Model 1—adolescent predictors of vagal tone | Model 2—early adult predictors of vagal tone | Model 3—adulthood predictors of vagal tone | |||||||
| β | ΔR 2 | R 2 | β | ΔR 2 | R 2 | β | ΔR 2 | R 2 | |
| I. Gender (1 = M; 2 = F) | −0.02 | −0.00 | −0.03 | ||||||
| Family Income (Age 13) | −0.05 | 0.00 | −0.05 | ||||||
| Summary Statistics for Step | 0.008 | 0.008 | 0.008 | 0.008 | 0.008 | 0.008 | |||
| II. Body Mass Index (Age 29) | −0.25** | −0.26** | −0.28*** | ||||||
| Summary Statistics for Step | 0.089** | 0.097** | 0.089** | 0.097** | 0.089** | 0.097** | |||
| III. Model 1: adolescent-era predictors | |||||||||
| Desirability as a Peer Companion | 0.24** | ||||||||
| Close friendship quality | 0.07 | ||||||||
| Summary Statistics for Step | 0.058** | 0.155*** | |||||||
| III. Model 2: early adult predictors | |||||||||
| Close Friendship quality | 0.25*** | ||||||||
| Warmth in Romantic Relationship | 0.12 | ||||||||
| Summary Statistics for Step | 0.076** | 0.173*** | |||||||
| III. Model 3: adult predictors | |||||||||
| Close friendship quality | 0.01 | ||||||||
| Warmth in romantic relationship | 0.27** | ||||||||
| Summary statistics for step | 0.074* | 0.166*** | |||||||
β weights are from final models
p < 0.05
p < 0.01
p ≤ 0.001
Hypothesis 2: Predictions will remain after accounting for potential confounding factors, including adolescent-era levels of depression, trait and social anxiety, externalizing behavior, and adult levels of neuroticism.
The next analyses considered the possibility that a number of individual characteristics related to difficulties with emotion regulation (which could have reflected the effects of adolescent-era low vagal tone) would potentially account for the predictions obtained above. Characteristics examined included social problem-solving competence at ages 13 through 16, depressive symptoms at ages 13 through 16, overall levels of anxiety at ages 15 and 16, trait anxiety and social anxiety at ages 18 and 20, externalizing behavior at ages 13, 16 and 18, and trait neuroticism at age 24. Initial analyses revealed that none of these factors was even minimally correlated with adult vagal tone (all r’s < 0.05, all p’s > 0.50); hence these were not analyzed further.
Hypothesis 3: A statistical mediational model, positing both direct effects from adolescent social experiences to adult vagal tone and effects mediated via early adult friendship and romantic relationship qualities will best account for the findings.
A path model was used to examine the extent to which the identified earlier markers of relationship difficulty predicted vagal tone either directly or as statistically mediated by later relationship difficulties. Figure 1 presents a path model including all previously identified predictors with all significant paths and effects depicted. The model fit the data well (χ2(12) = 6.65, p = 0.88; GFI = 0.99, AGFI = 0.93, SRMR = 0.033, CFI = 1.0, RMSEA = 0). Desirability as a peer companion in adolescence was found to predict later close friendship quality which in turn directly predicted vagal tone. Follow-up bootstrap analyses, using the PROCESS macro in SAS (Hayes, 2019) indicated that the full pathway from desirability as a peer companion through to adult vagal tone was significant (Indirect effect = 0.111, 95% CI: 0.007–0.281). Both early adult close friendship quality and age 29 warmth in romantic relationships independently contributed to explaining variance in vagal tone, together accounting for 13.3% of the variance in vagal tone over and above the other factors in the model.
Fig. 1.
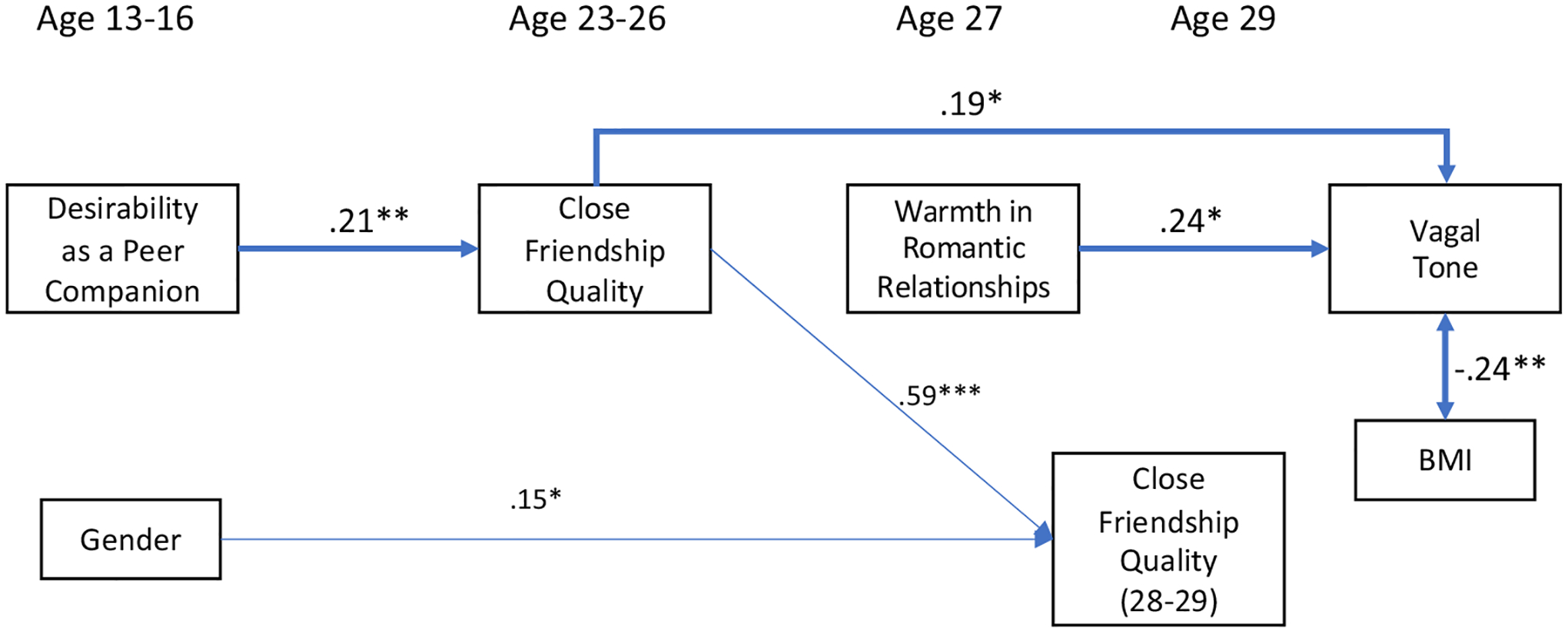
Direct and mediated prediction of adult vagal tone. Only significant paths are illustrated with arrows. Variables entered but with no relation to other variables in model (not depicted): close friendship quality (ages 13–16), warmth in romantic relationships (age 24), baseline family income. Vagal Tone Total R2 = 0.258, p < 0.001. Indirect effect from Desirability as a Companion to Vagal Tone via Close Friendship Quality was significant in Bootstrap analyses at p < 0.05
Post-hoc analyses
Although this study relied upon non-self-report data regarding relationship qualities so as to eliminate the possibility that (unmeasured) adolescent vagal tone was driving subsequent self-reports, post-hoc analysis considered whether self-reported loneliness in adulthood (ages 24 and 27) could have acted as a mediator for observed predictions from adolescence. Neither measure of loneliness was predictive of vagal tone either in simple correlations or when added to regression models as described in Table 2.
Discussion
This study found that, beginning as early as age 13, difficulty establishing positive relationships with peers was linked to lower vagal tone, assessed in terms of respiratory sinus arrhythmia in adulthood across periods spanning as long as 16 years. Linkages were established across multiple measures of relationship functioning, all of which were obtained by other than self-report, and several of which were aggregated over a multi-year period. Given that low vagal tone has been repeatedly identified as a risk factor for an array of long-term health problems up to and including early mortality (Binkley et al., 1991; Thayer & Lane, 2007; Thayer et al., 2010), these findings suggest both the potential importance of early relationship experiences for life course physical health risks, and a specific route by which these experiences might translate into physical problems.
The results of this study expand our understanding of the potential long-term duration of the effects of social isolation by linking low vagal tone to peer struggles at far earlier points in the lifespan and over a far longer span of time than has been previously examined. The long duration between observations of exposure to relative isolation and vagal tone assessments is perhaps the most intriguing and disturbing aspect of the current findings. These long-term linkages were only partially mediated via more recent relationship difficulties, and were not linked to adult personality traits, even though both of these potential mediators were assessed more proximately to the vagal tone assessment.
The earliest predictors of adult vagal tone were identified in early to mid-adolescence, with teens who were less likely to be rated as a desirable companion within their broader peer group from ages 13 to 16 having lower vagal tone at age 29. Similarly, participants whose closest friends rated the friendship as less satisfying at ages 23–26 also had lower vagal tone at age 29. Finally, lower vagal tone was predicted by lack of observed warmth from a romantic partner in a videorecorded interaction task at age 27. These findings are consistent with both attachment and social baseline theories, which highlight the role of important social relationships in providing an experience of safety and security that has been linked to greater parasympathetic activity (Bowlby, 1980; Coan & Sbarra, 2015). One explanation for these findings is that the observed relationship difficulties create a chronic, perhaps low-grade absence of experiences of security and safety. Primate research has suggested that separation from the larger ‘pack’ creates significant stressors, both physiological and emotional, for non-human primates, which likely generalize to humans as well (Sapolsky, 2004). In this context, the link to low vagal tone suggests that a relative lack of acceptance by others makes the ‘relax’ response handled by the parasympathetic nervous system less likely to fully activate even under otherwise restful conditions. Numerous studies have shown that social relationship difficulties and social isolation have substantial deleterious effects on long-term health; this study not only suggests that this pattern of difficulty connecting meaningfully with others may be identifiable as early as age 13, it also suggests one mechanism by which the chronic low-grade lack of security implied by this isolation may get under the skin to affect health outcomes.
The results of this study supported an interpretation in which adolescent experiences have their link to vagal tone mediated by experiences in adulthood, with some evidence consistent with a potential developmental cascade of social difficulties (Oudekerk et al., 2015): Lack of acceptance by peers in adolescence was predictive of future vagal tone, but this prediction appeared to be mediated by the link to poor quality early adult close friendships. Within adulthood poor early adult friendship quality remained a direct predictor of adult vagal tone even after accounting for both warmth in romantic relationships and later adult friendship quality, with both factors contributing uniquely to explaining variance in adult vagal tone. One explanation for these findings is that the experience of insecurity that comes from lacking close connections to others in early adulthood persists over time, even as actual relationship qualities evolve. Whether this persistence is a result of psychological factors (e.g., lack of felt security) or physiological factors (e.g., attunement of the nervous system to a slightly higher level of stress), would be important for future research to consider.
Notably, although several relationship constructs were examined at each developmental stage, the specific constructs found to be predictive at a given stage were arguably those that were most developmentally salient at that stage. In early/mid-adolescence, achieving status within the broad peer group is a primary goal, linked to numerous markers of adaptive development (Allen et al., 2005a; Bukowski et al., 1993). It may be that during this developmental stage it is actually status within the broader peer group that provides the social resources (i.e., safety in numbers) that reduce any potential sense of threat vis a vis peers. In early adulthood, close friendship competence predicted future vagal tone whereas current warmth in romantic relationships did not. Close friendships are likely to be the most stable available peer relationship during this phase, even if they are ultimately supplanted in importance by romantic relationships later in adulthood (Allen et al., 2020). By later in adulthood, however, this balance flips, such that long-term romantic pair bonds are most central, and it was the quality of these bonds that was linked to vagal tone. Together, these findings indicate the importance of taking on a developmental perspective when considering the role of social relationships and functioning at different points in the lifespan.
This study also sought to address the concern that observed effects reflected in the data could be an artifact of stable low vagal tone across the span studied giving rise to the relationship difficulties observed. Low vagal tone has been previously associated with both difficulties in affect regulation and with major depression (Beauchaine & Thayer, 2015; Sack et al., 2004), either of which could potentially have reduced the quality of peer relationships. We partly addressed this concern by using measures that did not depend on participant self-assessment and thus that did not simply reflect participants’ internal states. We also examined a range of the factors that would have likely mediated a reverse causal process if one existed, including depressive symptoms, externalizing behavior, social anxiety, social problem-solving competence, and trait neuroticism. None of these factors were linked to adult vagal tone. The contrast between the predictions from relationship qualities and the lack of predictions from mental health related factors suggests that ongoing relationships may have a unique status with respect to predicting future autonomic system outcomes over and above their relation to mental health symptoms. Nonetheless, other factors which we did not measure, for example baseline BMI, could still potentially have influenced both future vagal tone and peer relationship qualities.
Although this study focused upon measures of relationship quality independent of the participant’s perception, it is noteworthy that post-hoc analyses found no evidence that loneliness—one measure of the perceived absence of relationships—was linked to vagal tone. Of course, loneliness reflects simply that relationship quality is not as great as desired, and depending upon levels of desired relationships, may not even reflect low relationship quality. Nevertheless, given that measures of reported anxiety in early adulthood were also unrelated to vagal tone, it may also be that conscious perceptions regarding relationship anxiety and its effects are less important than non-conscious physiological experiences resulting from relationship absence.
Several limitations of this study also warrant consideration in addition to the absence of baseline vagal tone data noted above. Although results are consistent with findings from research in adulthood and extend these to a far earlier stage of the lifespan, direct causal inferences cannot be supported by these data. An additional limitation is that the observational and other-report assessment procedures used permitted only snapshots of difficulties with relationships at various points in adolescence and early adulthood. Given that it is an enduring pattern of exposure to these struggles that is the underlying construct of interest, it is quite likely that these findings would underestimate the true extent of the relations observed. Relatedly, this study focused only on the absence of positive relationships (as opposed to other types of relationship stressors). Also, this study did not have data from pre-adolescent periods. Thus, these findings raise, but cannot answer, questions as to whether adolescent relational stressors might mediate some of the effects of earlier stressors such as harsh parenting that are known to be linked to later relational difficulties. Finally, vagal tone was assessed in a laboratory setting, and although efforts were made to have participants as relaxed as possible (e.g., assessing vagal tone only at the end of a period watching a relaxing video), the resulting measurement may not fully accurately reflect true resting vagal tone.
Given these limitations, these data are nonetheless the first to link the absence of positive relationships in adolescence to autonomic functioning in adulthood, suggesting another important route by which relationship experiences might have implications for lifespan health outcomes. Prior research has found that conflict in relationships (but not lack of connection) was predictive of markers of inflammation across similar developmental spans (Allen et al., 2017). The present study, in contrast, identifies a different biological system that displays long-term links to the absence of satisfying relationships. Taken together, these findings begin to flesh out results of prior research which has established links of adolescent peer relationship qualities to self-reported health in early adulthood (Allen et al., 2015).
From a risk and prevention perspective, the absence of positive peer relationships beginning in adolescence may now be considered as a potential marker of risk for long-term health difficulties. Currently, national recommendations from the primary government agencies tasked with the prevention of age-related disease fail to consider any social relationship factors in adolescence or early adulthood (Centers for Disease Control & Prevention, 2017; Holt-Lunstad et al., 2017; Institute of Medicine, 2012). Yet, relational factors linked to autonomic functioning may be at least as modifiable as other identified risks in adolescence (e.g., smoking and obesity) (Schreier et al., 2013). The results of this study, if confirmed, suggest a range of potential entry points for intervention to improve life course health—ranging from modifications to social characteristics of secondary schools to interventions that directly target adolescents and young adults at-risk for relationship dysfunction (Allen et al., 2021).
Acknowledgements
This study was supported by grants from the National Institute of Child Health and Human Development and the National Institute of Mental Health (R37HD058305 & R01-MH58066).
Funding
The funding was provided by Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant Nos. R37HD058305, R01HD058305), National Institute of Mental Health (Grant No. R01-MH58066).
Footnotes
Conflict of interest The authors declare that they have no conflict of interest.
Human and animal rights Human subject protections were followed along with IRB review.
Informed consent All participants or their parents provided informed consent.
References
- Achenbach TM, & Edelbrock CS (1991). Manual for the child behavior checklist/4–18 and 1991 profile. University of Vermont Department of Psychiatry [Google Scholar]
- Albert D, Chein J, & Steinberg L (2013). The teenage brain peer influences on adolescent decision making. Current Directions in Psychological Science, 22, 114–120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Porter MR, McFarland CF, Marsh PA, & McElhaney KB (2005a). The two faces of adolescents’ success with peers: Adolescent popularity, social adaptation, and deviant behavior. Child Development, 76, 747–760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Porter MR, McFarland FC, Hare A, Miga E, & Schad M (2005b). Autonomy and relatedness coding manual for adolescent-romantic partner dyads. University of Virginia [Google Scholar]
- Allen JP, Porter MR, McFarland FC, McElhaney KB, & Marsh PA (2007). The relation of attachment security to adolescents’ paternal and peer relationships, depression, and externalizing behavior. Child Development, 78, 1222–1239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Uchino BN, & Hafen CA (2015). Running with the pack: Teen peer-relationship qualities as predictors of adult physical health. Psychological Science, 26, 1574–1583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Loeb EL, Tan JS, Narr RK, & Uchino BN (2017). The body remembers: Adolescent conflict struggles predict adult interleukin-6 levels. Development and Psychopathology (Online Version) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Narr RK, Kansky J, & Szwedo DE (2020). Adolescent peer relationship qualities as predictors of long-term romantic life satisfaction. Child Development, 91, 327–340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Narr RK, Nagel AG, Costello MA, & Guskin K (2021). The connection project: Changing the peer environment to improve outcomes for marginalized adolescents. Development & Psychopathology, 33, 647–657 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbuckle JL (1996). Full information estimation in the presence of incomplete data. In M. GA Schumaker RE (Ed.), Advanced structural modeling: Issues and Techniques (pp. 243–277). Erlbaum [Google Scholar]
- Bagwell CL, Schmidt ME, Newcomb AF, & Bukowski WM (2001). Friendship and peer rejection as predictors of adult adjustment. In Nangle DW & Erdley CA (Eds.), New directions in child development: The role of friendship in psychological adjustment (pp. 25–49). Jossey-Bass. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, & Thayer JF (2015). Heart rate variability as a transdiagnostic biomarker of psychopathology. International Journal of Psychophysiology, 98, 338–350. [DOI] [PubMed] [Google Scholar]
- Ben-Shlomo Y, & Kuh D (2002). A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. International Journal of Epidemiology, 31, 285–293. [PubMed] [Google Scholar]
- Berntson GG, Cacioppo JT, & Quigley KS (1993). Cardiac psychophysiology and autonomic space in humans: Empirical perspectives and conceptual implications. Psychological Bulletin, 114, 296. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Thomas Bigger J Jr, Eckberg DL, Grossman P, Kaufmann PG, Malik M, Nagaraja HN, Porges SW, Saul JP, Stone PH, & Van Der Molen MW (1997). Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology, 34, 623–648 [DOI] [PubMed] [Google Scholar]
- Binkley PF, Nunziata E, Haas GJ, Nelson SD, & Cody RJ (1991). Parasympathetic withdrawal is an integral component of autonomic imbalance in congestive heart failure: Demonstration in human subjects and verification in a paced canine model of ventricular failure. Journal of the American College of Cardiology, 18, 464–472. [DOI] [PubMed] [Google Scholar]
- Blakemore S-J, & Mills KL (2014). Is adolescence a sensitive period for sociocultural processing? Annual Review of Psychology, 65, 187–207. [DOI] [PubMed] [Google Scholar]
- Bowlby J (1969/1982). Attachment and loss (Vol. 1). Basic Books [Google Scholar]
- Bowlby J (1980) Attachment and loss: Vol. 3: Loss, sadness and depression. Basic Books [Google Scholar]
- Braune H-J, & Geisendörfer U (1995). Measurement of heart rate variations: Influencing factors, normal values and diagnostic impact on diabetic autonomic neuropathy. Diabetes Research and Clinical Practice, 29, 179–187. [DOI] [PubMed] [Google Scholar]
- Brosschot JF, Verkuil B, & Thayer JF (2016). The default response to uncertainty and the importance of perceived safety in anxiety and stress: An evolution-theoretical perspective. Journal of Anxiety Disorders, 41, 22–34. [DOI] [PubMed] [Google Scholar]
- Brosschot JF, Verkuil B, & Thayer JF (2017). Exposed to events that never happen: Generalized unsafety, the default stress response, and prolonged autonomic activity. Neuroscience & Biobehavioral Reviews, 74, 287–296. [DOI] [PubMed] [Google Scholar]
- Bukowski WM, Hoza B, & Boivin M (1993). Popularity, friendship, and emotional adjustment during early adolescence. New Directions for Child and Adolescent Development, 1993, 23–37. [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, Malarkey WB, Kiecolt-Glaser JK, Uchino BN, Sgoutas-Emch SA, Sheridan JF, Berntson GG, & Glaser R (1995). Heterogeneity in neuroendocrine and immune responses to brief psychologicalstressors as a function of autonomic cardiac activation. Psychosomatic Medicine, 57, 154–164. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2017). Four domains of chronic disease prevention. Author. [Google Scholar]
- Charles ST, Reynolds CA, & Gatz M (2001). Age-related differences and change in positive and negative affect over 23 years. Journal of Personality and Social Psychology, 80, 136. [PubMed] [Google Scholar]
- Christensen JH, Toft E, Christensen MS, & Schmidt EB (1999). Heart rate variability and plasma lipids in men with and without ischaemic heart disease. Atherosclerosis, 145, 181–186. [DOI] [PubMed] [Google Scholar]
- Cicchetti DV, & Sparrow SA (1981). Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. American Journal of Mental Deficiency, 86, 127–137. [PubMed] [Google Scholar]
- Coan JA, & Sbarra DA (2015). Social baseline theory: The social regulation of risk and effort. Current Opinion in Psychology, 1, 87–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coie JD, Dodge KA, & Coppotelli H (1982). Dimensions and types of social status: A cross age perspective. Developmental Psychology, 18, 121–132. [Google Scholar]
- Donoho CJ, Seeman TE, Sloan RP, & Crimmins EM (2015). Marital status, marital quality, and heart rate variability in the MIDUS cohort. Journal of Family Psychology, 29, 290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman BJ, Rosenthal L, Donahoe CP, Schlundt DG, & McFall RM (1978). A social-behavioral analysis of skill deficits in delinquent and nondelinquent adolescent boys. Journal of Consulting & Clinical Psychology, 46, 1448–1462. [DOI] [PubMed] [Google Scholar]
- Furman W, & Buhrmester D (1985). Childrens’ perceptions of the personal relationships in their social networks. Developmental Psychology, 21, 1016–1024. [Google Scholar]
- Furman W, & Collibee C (2014). A matter of timing: Developmental theories of romantic involvement and psychosocial adjustment. Development and Psychopathology, 26, 1149–1160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gee DG, Humphreys KL, Flannery J, Goff B, Telzer EH, Shapiro M, Hare TA, Bookheimer SY, & Tottenham N (2013). A developmental shift from positive to negative connectivity in human amygdala-prefrontal circuitry. Journal of Neuroscience, 33, 4584–4593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goff B, Gee DG, Telzer EH, Humphreys KL, Gabard-Durnam L, Flannery J, & Tottenham N (2013). Reduced nucleus accumbens reactivity and adolescent depression following early-life stress. Neuroscience, 249, 129–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg LR, Johnson JA, Eber HW, Hogan R, Ashton MC, Cloninger CR, & Gough HG (2006). The international personality item pool and the future of public-domain personality measures. Journal of Research in Personality, 40, 84–96. [Google Scholar]
- Goswick RA, & Jones WH (1982). Components of loneliness during adolescence. Journal of Youth and Adolescence, 11, 373. [DOI] [PubMed] [Google Scholar]
- Gouin J-P, Zhou B, & Fitzpatrick S (2015). Social integration prospectively predicts changes in heart rate variability among individuals undergoing migration stress. Annals of Behavioral Medicine, 49, 230–238. [DOI] [PubMed] [Google Scholar]
- Harter S (1988). Manual for the self-perception profile for adolescents. University of Denver. [Google Scholar]
- Hayes AF (2019). Introduction to mediation, moderation, and conditional process analysis, second edition: A regression-based approach. ProQuest Ebook Central. http://ebookcentral.proquest.com/lib/uva/detail.action?docID=5109647). Guilford [Google Scholar]
- Hoetink AE, Faes TJ, Schuur EH, Gorkink R, Goovaerts HG, Meijer JH, & Heethaar RM (2002). Comparing spot electrode arrangements for electric impedance cardiography. Physiological Measurement, 23, 457. [DOI] [PubMed] [Google Scholar]
- Holt-Lunstad J, Uchino BN, Smith TW, & Hicks A (2007). On the importance of relationship quality: The impact of ambivalence in friendships on cardiovascular functioning. Annals of Behavioral Medicine, 33, 278–290. [DOI] [PubMed] [Google Scholar]
- Holt-Lunstad J, Robles TF, & Sbarra DA (2017). Advancing social connection as a public health priority in the United States. American Psychologist, 72, 517–530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute of Medicine. (2012). Accelerating progress in obesity prevention: Solving the weight of the nation. Author. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson M, Deardorff J, Davis EL, Martinez W, Eskenazi B, & Alkon A (2017). The relationship between maternal responsivity, socioeconomic status, and resting autonomic nervous system functioning in Mexican American children. International Journal of Psychophysiology, 116, 45–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kazdin AE (1990). Childhood depression. Journal of Child Psychology & Psychiatry & Allied Disciplines, 31, 121–160. [DOI] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke K-M, & Hellhammer DH (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28, 76–81. [DOI] [PubMed] [Google Scholar]
- Kobak RR, & Sceery A (1988). Attachment in late adolescence: Working models, affect regulation and representations of self and others. Child Development, 59, 135–146. [DOI] [PubMed] [Google Scholar]
- Koenig J, & Thayer JF (2016). Sex differences in healthy human heart rate variability: A meta-analysis. Neuroscience & Biobehavioral Reviews, 64, 288–310. [DOI] [PubMed] [Google Scholar]
- Kok BE, & Fredrickson BL (2010). Upward spirals of the heart: Autonomic flexibility, as indexed by vagal tone, reciprocally and prospectively predicts positive emotions and social connectedness. Biological Psychology, 85, 432–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kovacs M, & Beck AT (1977). An empirical clinical approach toward a definition of childhood depression. Raven Press. [Google Scholar]
- La Greca AM, & Lopez N (1998). Social anxiety among adolescents: Linkages with peer relations and friendships. Journal of Abnormal Child Psychology, 26, 83–94. [DOI] [PubMed] [Google Scholar]
- Litvack DA, Oberlander TF, Carney LH, & Saul JP (1995). Time and frequency domain methods for heart rate variability analysis: A methodological comparison. Psychophysiology, 32, 492–504. [DOI] [PubMed] [Google Scholar]
- Lizotte AJ, Chard-Wierschem DJ, Loeber R, & Stern SB (1992). A shortened Child Behavior Checklist for delinquency studies. Jour nal of Quantitative Criminology, 8, 233–245. [Google Scholar]
- Maier SF, & Watkins LR (1998). Cytokines for psychologists: Implications of bidirectional immune-to-brain communication for understanding behavior, mood, and cognition. Psychological Review, 105, 83. [DOI] [PubMed] [Google Scholar]
- McElhaney KB, Antonishak J, & Allen JP (2008). They like me, they like me not: Popularity and adolescents’ perceptions of acceptance predicting changing social functioning over time. Child Development, 79, 720–731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen BS (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiology Review, 87, 873–904. [DOI] [PubMed] [Google Scholar]
- Moore D, & Schultz NR (1983). Loneliness at adolescence: Correlates, attributions, and coping. Journal of Youth and Adolescence, 12, 95. [DOI] [PubMed] [Google Scholar]
- Narr RK, Allen JP, Tan JS, & Loeb EL (2019). Close friendship strength and broader peer group desirability as differential predictors of adult mental health. Child Development, 90, 298–313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oudekerk BA, Allen JP, Hessel ET, & Molloy LE (2015). The cascading development of autonomy and relatedness from adolescence to adulthood. Child Development, 86, 472–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porges SW (2007). The polyvagal perspective. Biological Psychology, 74, 116–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, & McGinn MM (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140, 140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roisman GI, Masten AS, Coatsworth JD, & Tellegen A (2004). Salient and emerging developmental tasks in the transition to adulthood. Child Development, 75, 123–133. [DOI] [PubMed] [Google Scholar]
- Romeo RD (2010). Adolescence: A central event in shaping stress reactivity. Developmental Psychobiology, 52, 244–253. [DOI] [PubMed] [Google Scholar]
- Russell D, Peplau LA, & Cutrona CE (1980). The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. Journal of Personality and Social Psychology, 39, 472–480. [DOI] [PubMed] [Google Scholar]
- Sack M, Hopper JW, & Lamprecht F (2004). Low respiratory sinus arrhythmia and prolonged psychophysiological arousal in posttraumatic stress disorder: Heart rate dynamics and individual differences in arousal regulation. Biological Psychiatry, 55, 284–290. [DOI] [PubMed] [Google Scholar]
- Sapolsky RM (2004). Why zebras don’t get ulcers: The acclaimed guide to stress, stress-related diseases, and coping-now revised and updated. Macmillan [Google Scholar]
- Schreier HM, Schonert-Reichl KA, & Chen E (2013). Effect of volunteering on risk factors for cardiovascular disease in adolescents: A randomized controlled trial. Journal of the American Medical Association: Pediatrics, 167, 1–6. [DOI] [PubMed] [Google Scholar]
- Schroeder EB, Liao D, Chambless LE, Prineas RJ, Evans GW, & Heiss G (2003). Hypertension, blood pressure, and heart rate variability: The atherosclerosis risk in communities (ARIC) study. Hypertension, 42, 1106–1111. [DOI] [PubMed] [Google Scholar]
- Smith TW, Deits-Lebehn C, Williams PG, Baucom BR, & Uchino BN (2020). Toward a social psychophysiology of vagally mediated heart rate variability: Concepts and methods in self-regulation, emotion, and interpersonal processes. Social and Personality Psychology Compass, 2020, e12516. [Google Scholar]
- Spielberger CD, Sydeman SJ, Owen AE, & Marsh BJ (1999). Measuring anxiety and anger with the State-Trait Anxiety Inventory (STAI) and the State-Trait Anger Expression Inventory (STAXI). In Maruish ME (Ed.), The use of psychological testing for treatment planning and outcomes assessment (pp. 993–1021). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Steinberg L, & Monahan KC (2007). Age differences in resistance to peer influence. Developmental Psychology, 43, 1531–1543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thayer JF, & Lane RD (2007). The role of vagal function in the risk for cardiovascular disease and mortality. Biological Psychology, 74, 224–242. [DOI] [PubMed] [Google Scholar]
- Thayer JF, Yamamoto SS, & Brosschot JF (2010). The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. International Journal of Cardiology, 141, 122–131. [DOI] [PubMed] [Google Scholar]
- Uchino BN (2009). What a lifespan approach might tell us about why distinct measures of social support have differential links to physical health. Journal of Social and Personal Relationships, 26, 53–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziegler D, Laude D, Akila F, & Elghozi J-L (2001). Time-and frequency-domain estimation of early diabetic cardiovascular autonomic neuropathy. Clinical Autonomic Research, 11, 369–376 [DOI] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, Nesdale D, Webb HJ, Khatibi M, & Downey G (2016). A longitudinal rejection sensitivity model of depression and aggression: Unique roles of anxiety, anger, blame, withdrawal and retribution. Journal of Abnormal Child Psychology, 44, 1291–1307 [DOI] [PubMed] [Google Scholar]