

ABSTRACT
Although seemingly benign, the presence of a patent foramen ovale (PFO) may play an important role in the pathophysiology of disease, specifically a paradoxical embolism leading to cryptogenic stroke. The European Society of Cardiology recently published guidelines detailing how PFOs are associated with paradoxical embolism and how they are diagnosed and managed. This review guides physicians in the diagnostic and referral process to a multidisciplinary team involved in PFO closure. It reviews the clinical trials comparing device closure with medical therapy and highlights the current NHS England commissioning process on PFO management. Finally, we give an overview of other conditions where PFO device closure may need to be considered.
KEYWORDS: patent foramen ovale, paradoxical embolism, cardiology, cryptogenic stroke, multidisciplinary team
Introduction
The foramen ovale is an open interatrial communication during foetal development that allows oxygenated blood to bypass pulmonary circulation and usually closes shortly after birth. The foramen may remain open in up to 25% of the population, caused by the septum primum and septum secundum failing to completely fuse and is best visualised during transoesophageal echocardiography (TOE; Fig 1).1–3 Most people with a patent foramen ovale (PFO) remain asymptomatic and do not require any treatment. However, there are instances when a PFO can facilitate a paradoxical thrombo-embolus from the venous to the systemic circulation. This usually lodges in a cerebral artery, leading to a stroke.4
Fig 1.
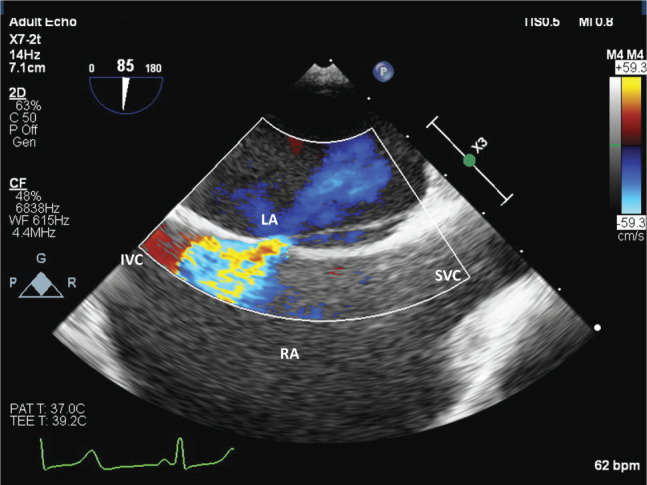
Transoesophageal echocardiography (bi-caval view) showing high-velocity blood flow (red and yellow colour) shunting from the left to the right atrium through the patent foramen ovale. IVC = inferior vena cava; LA = left atrium; RA = right atrium; SVC = superior vena cava.
This review focuses on how PFO is diagnosed following a ‘cryptogenic’ stroke, highlighting the imaging and provocation of a right-to-left shunt through the interatrial septum (IAS; supplementary material S1, Fig S1). It also highlights the indication for percutaneous device closure, reviews other conditions potentially associated with a PFO and makes recommendations on their management.
Cryptogenic stroke
Cryptogenic stroke is a cerebral ischaemia that cannot be definitively attributed to large artery atherosclerosis, small artery disease or a cardio-embolism despite rigorous investigation.5 Cryptogenic stroke most commonly occurs in people aged between 25 to 45 years and PFO prevalence has been reported in up to 40% of such cases, particularly when associated with larger shunts.6,7 An interatrial shunt associated with PFO is a channel-like appearance to blood flow wherein flow normally occurs from the left to the right atrium (Fig 1).8 Supplementary material S1, Fig S1, shows a reversal in direction of blood flow through the PFO, ie, from the right to the left atrium. Atrial septal aneurysms are sometimes associated with PFO and can often result in thrombus formation due to stagnation of blood that increases the risk of stroke.9 There are five types of atrial septal aneurysms that are classified according to the deviation/protrusion of the atrial septum relative to the left or right atrium.9
In contrast, ischaemic strokes, which commonly occur in patients over 60 years of age, are usually attributed to atherosclerosis or cardio-embolic events, particularly in patients with a history of hypertension, diabetes or atrial fibrillation, and often are associated with other cardiovascular risk factors.10
Despite an association between PFO and cryptogenic stroke, confirming that association can be challenging as at least one-third of those discovered are likely to be incidental findings.5 Closure of an incidental PFO would expose the patient to procedural- and device-related risks without reducing the risk of recurrent stroke.5
The benefit from PFO closure is dependent on the probability that the index stroke is attributable to the PFO.5 Imaging of the brain should focus on the location and pattern of cerebral infarction. Thaler et al reported that newly discovered large superficial cortical infarcts were more likely due to paradoxical embolism.11 PFO-mediated strokes are also more prevalent in patients with a risk of paradoxical embolism (RoPE) score >5.10 RoPE is a 10-point combined score used in patients with a history of prior cerebral infarct or transient ischaemic attack (TIA).12 The 10-point score is calculated by subtracting 1 point for each non-age-related factor (diabetes, hypertension, smoking, previous TIA or stroke, or cortical stroke on imaging) and for each completed decade after 20 years of age (up to 5 points) from a total score of 10.10 For example, a 41-year-old man with diabetes and hypertension will score 6 points (–2 points for completing 2 decades over 20 years, –1 for diabetes and –1 for hypertension: 10–2–1–1 = 6).
The higher the score, the greater the prevalence of a PFO. That is, a person scoring 3 points has a lower prevalence of PFO (23%) compared with a person scoring 9 (73%).10 Therefore, younger patients with superficial cortical strokes and no vascular risk factors score the highest and would potentially benefit more from PFO closure (Fig 2).12,13,18
Fig 2.
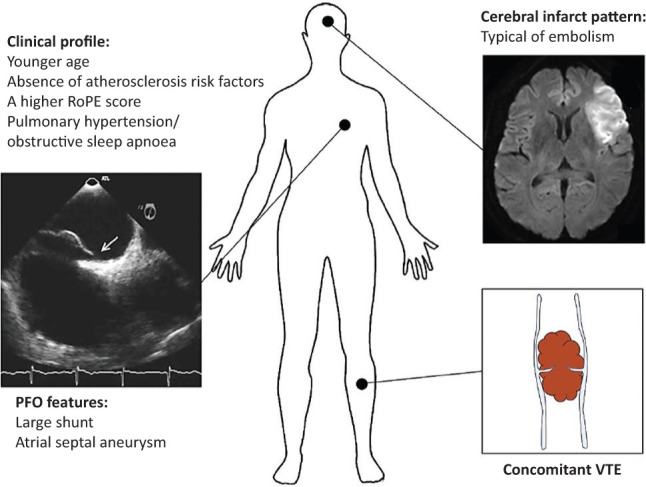
Someone with a higher risk of a patent foramen ovale and would potentially benefit from closure based on a higher RoPE score, concomitant VTE, large superficial cortical infarcts, larger interatrial shunts and associated ASA. ASA = atrial septal aneurysm; PFO = patent foramen ovale; RoPE = risk of paradoxical embolism; VTE = venous thromboembolism. Adapted with permission from Abdelghani M, El-Shedoudy SAO, Nassif M, Bouma BJ, de Winter RJ. Management of patients with patent foramen ovale and cryptogenic stroke: an update. Cardiology 2019;143:62–72 published by S Karger, Basel.
Pooled data from PFO trials comparing device closure versus medical therapy (CLOSURE I, RESPECT and PC trials) assessed RoPE score against risk of recurrent ischaemic strokes.14–16 Patients with a RoPE score >7 (CLOSE trial; 7.4±1.4) had higher estimated attributable fraction of PFO-related cryptogenic stroke rather than PFO as an incidental finding, and these patients benefited more from percutaneous closure.17 The relative importance of age and cardiovascular risk factors in the presence of a PFO was also highlighted with the results of the CLOSURE I trial (PFO device closure versus medical therapy; Table 1), showing no overall benefit from further strokes and TIAs following device closure.10,13,14 Table 1 summarises the effect of cardiovascular risk factors, ischaemic heart disease and atrial fibrillation on the likelihood of suffering a further neurological event despite device implantation in CLOSURE I trial. Assessed independently, a history of diabetes (hazard ratio (HR) 5.54 (95% confidence interval (CI) 2.27–13.57); p=0.0002) and detection of atrial fibrillation (AF; HR 7.29 (95% CI 2.46–21.61); p=0.0003) were associated with increased risk of recurrent ischaemic strokes. A higher index of TIA independently was associated with recurrent TIA (HR 4.71 (95% CI 2.16–10.30); p=0.0001).10,14 Diabetes mellitus, obesity, hypertension and ischaemic heart disease were associated with recurrent neurological events in this study and more common in patients aged >60 years.18
Table 1.
Risk of recurrent ischaemic stroke in patients with comorbidities
| Univariable hazard ratio (95% confidence interval) | p-value | Multivariable hazard ratio (95% confidence interval) | p-value | |
|---|---|---|---|---|
| Diabetes mellitus | 2.88 (1.45–5.74) | 0.0027 | 3.39 (1.69–6.84) | 0.0007 |
| Body mass index >30 kg/m2 | 1.05 (1.00–1.09) | 0.033 | N/A | N/A |
| Hypertension | 1.92 (1.11–3.31) | 0.019 | N/A | N/A |
| Ischaemic heart disease | 4.38 (1.07–18.01) | 0.04 | N/A | N/A |
| Index transient ischaemic stroke vs stroke | 1.98 (1.14–3.43) | 0.015 | 2.13 (1.20–3.80) | 0.010 |
| Detection of atrial fibrillation | 4.94 (2.23–10.96) | <0.0001 | 4.85 (2.05–11.47) | 0.0003 |
The multidisciplinary team process
Multidisciplinary team (MDT) discussion involving an interventional cardiologist, imaging cardiologist and stroke physicians (supported by haematology and neurology, as appropriate) is required.18 Selected patients are usually aged less than 60 years and who have made a good functional recovery following stroke (modified Rankin scale <3). The importance of good clinical history taking prior to referral cannot be overemphasised as these patients can have a history of recent deep venous thromboembolism, migraine, recent travel, sleep apnoea and sometimes a history of a Valsalva manoeuvre (toilet straining, for example) preceding the stroke.19
The clinical diagnosis of ischaemic brain infarction must be supported by magnetic resonance imaging (MRI) and/or computed tomography (CT), remembering to prior exclude other potential causes including cardioembolic episodes, large-vessel atherosclerosis and lacunar (small-artery) ischaemia.1 Patients with a clinical suspicion of stroke and a normal brain scan, and those with a TIA are not usually considered for a PFO closure.1
Ambulatory electrocardiography (ECG) monitoring (usually for minimum of 72 hours or a 2-week ‘patch recording’) is required to exclude atrial arrhythmias (specifically AF) and some cardiologists recommend an implantable loop recorder. Early detection of atrial fibrillation by long-term monitoring using an insertable cardiac monitor has shown clinical benefit (CRYSTAL-AF trial).10,13,20 Carotid Doppler tests are used to rule out sub-stenotic lesions, vessel dissection or aneurysm formation. A prior thrombophilia screen (Table 2) is required to exclude hypercoagulability causes of vascular thrombosis.1,2,22 The presence of thrombophilia is also associated with an increased risk of stroke recurrence in patients with PFO, which would require antithrombotic therapy even if device closure is being considered.21
Table 2.
Laboratory diagnostics in thrombophilia
| Condition predisposing to thrombophilia | Investigations |
|---|---|
| Factor V Leiden | Direct DNA genotyping. |
| Prothrombin G20210A | Direct DNA genotyping. |
| Antithrombin, protein C and protein S deficiencies (natural coagulation inhibitors) | Immunologic antigen assays and chromogenic or clot-based activity assays. Potential conditions such as concomitant liver disease, pregnancy and anticoagulation therapy must be considered and excluded before the diagnosis of an inhibitor deficiency can be made. |
| Antiphospholipid syndrome (APS) | Testing for lupus anticoagulants (LAs), the presence of immunoglobulin (Ig) G or IgM antibodies directed against phospholipids and phospholipid-binding proteins such as beta-2-glycoprotein-I. A combination of clot-based assays has been recommended to demonstrate LA activity, whereas solid-phase immunoassays allow the detection of anti-cardiolipin and anti-beta-2-glycoprotein-I antibodies. The diagnosis of APS requires the persistence of antiphospholipid antibodies for at least 12 weeks together with thrombotic and/or obstetric features of APS including recurrent early miscarriages, fetal death at or beyond 10 weeks of gestation, and early delivery for severe preeclampsia or placental insufficiency. |
The transthoracic echocardiography (TTE) with bubble contrast (conducted by injecting agitated saline solution into the left cubital vein) is required for the MDT (supplementary material S1, Figs S1, S2 and S3). The magnitude of bubbles crossing the interatrial septum into the left heart chambers within three cardiac cycles (at rest or following a provocation manoeuvre, such as Valsalva) are reviewed. There is currently no standard accepted grading for shunt size but the number of bubbles within three cardiac cycles can be graded as small (<5), medium (5–25) and large (>25) in accordance with a study conducted in 2010.7 Transcranial Doppler is an alternative investigation to assess the magnitude of right-to-left shunt and has a higher sensitivity compared with TTE but is not readily available in many hospitals.23
A TOE may be required after MDT discussion and will provide additional information by assessing the size and location of the PFO tunnel and the interatrial shunt can be further evaluated (Fig 1). Interatrial septum (IAS) hypermobility aneurysm (ASA) formation and large interatrial shunt size are ‘high-risk’ features favouring device closure.5,17,24,25 ASA may facilitate a thrombus moving from the right atrium into the PFO or causing thrombosis in the PFO tunnel itself by inducing flow turbulence or stagnation.18 A visible thrombus may necessitate a period of oral anticoagulation prior to device closure.2 TOE can also be useful in excluding an arterio-venous (A-V) malformation (an alternative cause of paradoxical embolism) by a later detection (3–5 cardiac cycles) of bubble echocardiography contrast into the left atrium from the pulmonary veins rather than across the IAS.
Treatment options for PFO following a cryptogenic stroke
Medical therapy
Ischaemic stroke is usually treated with antiplatelet agents (such as clopidogrel or aspirin) or with oral anticoagulants (OACs) in the presence of concurrent AF.26 In patients with cryptogenic stroke associated with PFO, OACs have been compared against antiplatelet medication in both the CLOSE and CLOSURE I trials (underpowered when designed to compare PFO device closure with anti-platelet or OAC therapy).14,17 The reduction in stroke with OACs compared with anti-platelet therapy was not significantly different and there was a higher risk of major bleeding with OACs.14,17
The NAVIGATE ESUS trial comparing rivaroxaban (factor Xa inhibitor) with aspirin did not demonstrate a statistically significant difference in the rate of stroke recurrence in the rivaroxaban group (HR 1.32 (95% CI 0.43–4.03); p=0.63) but the risk of bleeding with rivaroxaban was significantly higher.17,27 The use of OACs does not appear superior to anti-platelet therapy for secondary prevention of PFO-related stroke and is associated with increased haemorrhagic risk.14,17,27
PFO device closure
A meta-analysis of six trials have shown that PFO device closure plus medical therapy is superior to anti-platelet therapy alone in reducing the risk of recurrence following a cryptogenic stroke.14–17,24–26 Procedural success from device closure occurred in 89.12% of patients.25 There was no clear superiority of PFO closure in two of these trials (CLOSURE I and PC) but they were underpowered to assess the clinical endpoints.14,16 PFO closure was associated with femoral vascular access site complications and new onset AF (risk range 3.9%–6% across the six trials).14–17,24,26 Most cases of atrial fibrillation were periprocedural, being detected within a month after closure.14,15,25
Another reported adverse event was deep venous thrombosis (DVT; device closure group 0.2%) and pulmonary embolism (PE; device closure group 0.4%), presumably related to complications from femoral venous access.15 Currently, ultrasound-guided venous puncture is used to reduce vascular complications by reducing the frequency of puncture and, hence, blood stagnation, while monitoring a whole blood activated clotting time (ACT; >250 seconds) measures the therapeutic effect of heparin. In the unlikely event that DVT/PE is still provoked, oral anticoagulation is indicated, usually for 3–6 months after the procedure. Periprocedural AF warrants lifelong oral anticoagulation.15
Other complications reported by the trials include cardiac tamponade (0.4%), device migration/embolisation (0.5%), infective endocarditis (0.2%), stroke (0.4%) and death (0.5%).14,15,24 These potential complications are rare, but all should be mentioned in the patient consent process for device closure.
Interatrial shunt size and the presence of ASA have been evaluated in several trials assessing recurrence of stroke and stroke risk reduction with PFO closure.14–16,25,28 A greater decrease in recurrence is seen in PFO patients with larger interatrial shunts and ASA.5,17,25 The greater benefit of device closure in reducing recurrent stroke in patients with a substantial shunt was also highlighted in the meta-analysis by Abdelaziz et al (supplementary material S1, Fig S4).29
Recent trials, including CLOSE and REDUCE, compared with RESPECT and PC trials were found to significantly reduce the risk of stroke recurrences; however, device closure was significantly associated with adverse events (mainly AF) resulting in a higher number needed to treat (NNT).15–17,24,30 The NNT to avoid one stroke in 5 years in the RESPECT trial was 42, in the CLOSE trial it was even lower with 20.15,17 In the REDUCE trial, the NNT was 28 at 2 years.24 This can be reduced by longer follow-up (eg at 10 years the NNT is 18).30 As a result, PFO closure can be an effective treatment, but should be only performed in selected patients with certain indications as highlighted earlier by Abdelghani et al.18
PFO shunt closure following device implantation can take up to 5 years (the process of complete endothelialisation) and aspirin is usually the mainstay of treatment over this time.17 The REDUCE PFO device closure trial compared three different antiplatelet regimens and showed better outcomes using aspirin relative to clopidogrel (1.4 and 3.6 stroke recurrences per 100 person-years, respectively).24 Adjunct antiplatelet agents or oral anticoagulation following device closure were also compared in the RESPECT trial.15 Both treatment groups were associated with an overall reduction of stroke recurrence (HR 0.38 (95% CI 0.18–0.79); p=0.007). Antiplatelet therapy was more commonly used and was more effective in reducing the rate of recurrent stroke. The prescribing and duration of single or dual antiplatelet therapy after device closure has been variable among physicians and the European joint taskforce position paper recommends dual anti-platelet therapy for 1–6 months and single anti-platelet therapy (usually aspirin) for at least 5 years.31,32
Assessing residual shunts after PFO closure (especially in asymptomatic patients) is also variable and many cardiologists do not routinely use repeat contrast bubble echocardiography.33 A second device implantation is occasionally required for persistent right-to-left shunts, specifically, when there are further cerebrovascular events.33 Dual antiplatelet therapy is usually recommended for up to 6 months after a second device, and single antiplatelet therapy thereafter, probably for life.33
The Amplatzer PFO Occluder (Fig 3) is the most effective device in reducing the rate of cryptogenic stroke by achieving complete closure in most patients and is also associated with better clinical outcomes compared with the other PFO devices (including HELEX and CardioSEAL-STARflex).34 This device is rarely associated with thrombus formation or device embolisation.33
Fig 3.

Transoesophageal echocardiography during patent foramen ovale closure. The device discs (Amplatzer PFO Occluder; yellow arrow) are correctly positioned on the left and right side of the interatrial septum. IVC = inferior vena cava; LA = left atrium; SVC = superior vena cava.
The NHS England commissioning policy (Box 1) guides physicians in the selection of suitable candidates for device closure with an aim to prevent exposing patients to potential procedural and device-related risks unless there is clear benefit from percutaneous closure.34,35 While the current NHS commissioning criteria permit device closure of PFO for secondary prevention of cryptogenic stroke, they do not presently consider PFO closure for primary prevention of stroke or for other pathological conditions.
Box 1.
NHS England commissioning guidelines for patent foramen ovale closure in the UK
|
Potential indications for device closure
Systemic embolism
Not all paradoxical emboli get lodged in the cerebral circulation. PFO may be associated with arterial embolisation to the gastrointestinal system, upper or lower limbs, or the coronary circulation (presenting as acute myocardial infarction), to name a few.36–38 Selected cases of a paradoxical systemic embolus in younger patients with an absence for risk factors of atherosclerosis may be potential indications for PFO closure and should be referred to the MDT, if no other source of embolisation can be elucidated.
Decompression sickness
Decompression sickness (DCS) is caused by the formation of gas bubbles that occur from exposure to low barometric pressures by causing inert gases (mainly nitrogen), that are normally dissolved in body fluids and tissues, to come out of physical solution and form bubbles. It can occur during scuba diving, in commercial divers who breathe ‘heliox’ (a special mixture of oxygen and helium), and in astronauts and aviators who experience rapid changes in pressure from sea level. In patients with a right-to-left shunt through a PFO, the nitrogen bubbles bypass the pulmonary circulation increasing the risk of arterial occlusion by coalescence, thus causing DCS (also known as the ‘bends’; DCS I is musculocutaneous; DCS II is neurologic).2,39 A large PFO shunt size increases this risk.39
Case-controlled studies (Table 3) suggest that PFO device closure reduces the incidence of DCS at diving depths greater than 18 metres and could be recommended for professional divers who have experienced DCS II, otherwise they need to refrain from the precipitating activity.39,41 Owing to the discrepancy between PFO prevalence and DCS, routine screening for PFO is not recommended.1,39,40
Table 3.
Studies supporting potential indications for patent foramen ovale closure that are not currently commissioned in the UK
| Indications | Study | Findings |
|---|---|---|
| Decompression sickness | Pristipino et al39 | Presence of a right-to-left shunt is associated with a higher risk of incidence of decompression sickness. Odds ratio 5.63 (95% confidence interval 3.14–10.09) |
| Honek et al41 | 34% in PFO group and 0% in closure group (p=0.02) for 18 metre dive; 88% in the PFO group and 0% in the closure group (p<0.01) for 50 metre dive | |
| Migraine with aura | Mattle et al44 | Although a greater reduction in number of migraine days (–2.9 vs –1.7 days; p=0.17) and frequency of attacks (–2.1 vs –1.3; p=0.097) was noted in the closure group vs non-closure group, respectively, the results of the study were not significant and, hence, it cannot be concluded that PFO closure may be appropriate for migraine with aura. |
| Platypnoea-orthodeoxia syndrome | Blanche et al45 | PFO closure is associated with improvement in oxygen saturation (from 83% ±3% to 93% ±2%) |
| Liver transplantation | Flocco et al47 | Reduction in cardiopulmonary complications in patients with PFO closure vs without closure (73% vs 51%, respectively; p=0.02). |
PFO = patent foramen ovale.
Migraine with aura
A higher prevalence of PFO has been reported in migraine patients with aura than in the general population.42 It has been hypothesised that right-to-left shunt in patients with a PFO allows the vasoactive substances to bypass the pulmonary–capillary filter and reach the cerebral arterial circulation, thereby triggering a migraine attack.2 Patients with a large PFO have increased frequency of migraine attacks on exertion.43,44 Migraine with aura is also an independent risk factor for ischaemic stroke in patients aged under 45 years (6–8-fold higher risk) and those with a PFO may be at compounded risk.43,44 Some studies (Table 3) have suggested a potential benefit of PFO closure in these patients.42 However, further research is required and PFO device closure is presently not commissioned for migraine with aura. MDT referral is therefore not recommended.
Platypnoea-orthodeoxia syndrome
Platypnoea-orthodeoxia syndrome (POS) is a rare but under-diagnosed condition characterised by dyspnoea and deoxygenation when changing from a recumbent to an upright position. It is usually caused by increased right-to-left shunting of blood in the upright position and is associated with PFO in the presence of raised right atrial pressure and change of the atrial septal architecture. There are several other potential causes to consider in the differential diagnosis of POS, including causes of intrapulmonary shunting (for example, multiple pulmonary emboli or arterio-venous malformations).45,46 Studies suggest that PFO closure results in an improvement in oxygen saturation with resolution of symptoms.45,46 Patients with this condition and who have a significant PFO should be assessed by the MDT, but device closure is presently not commissioned by NHS England.
Liver transplantation
PFO may permit the passage of an air embolus from the central placement lines, caval clamping or inadequate flushing of the transplanted liver, thereby increasing the risk of paradoxical embolism.3 One study suggests that cardiopulmonary complications in liver transplant patients with a large PFO may benefit from device closure but the lack of randomised controlled trials makes it difficult to draw firm conclusions and highlights the need for future research.47 Such cases should be discussed through the MDT, but device closure cannot presently be recommended.
Right-sided cardio-pulmonary disease
Elevated right heart pressures (pulmonary hypertension and large pulmonary embolism) are associated with an increased risk of right-to-left shunting in patients with a PFO, thereby increasing the risk of cerebrovascular events and exacerbating cyanosis.40 Such patients often receive oral anticoagulants and there is a lack of clinical trials evaluating whether PFO closure provides additional clinical benefit. In general, PFO closure in a patient with pulmonary hypertension is considered unsafe and could lead to right ventricular failure.
PFO with right-to-left shunt has also been suggested as a potential cause of worsening hypoxaemia in patients with chronic obstructive pulmonary disease, although it is often difficult to distinguish the relative contributions of the right-to-left shunt versus the underlying pulmonary disease to the patient's hypoxaemia.40 There is a lack of clinical trials evaluating whether PFO closure provides any clinical benefit.
Conclusion
PFO device closure plus anti-platelet therapy lowers the risk of recurrent cryptogenic stroke compared with antiplatelet therapy alone. Further research is needed to evaluate the effectiveness of PFO device closure in patients presenting with DCS, migraine with aura and platypnoea-orthodeoxia syndrome, among others.
Key points
Confirming that a cryptogenic stroke is secondary to a PFO requires extensive investigation. The diagnostic pathway is summarised in Fig 4.1
MDT discussion involving both interventional and imaging cardiologists supported by stroke physicians is necessary to identify patients who are suitable for PFO device closure.
Device closure in conjunction with antiplatelet therapy is associated with reduced incidence of a recurrent stroke when compared with antiplatelet monotherapy.
Antiplatelet therapy is still used after PFO device closure, but the duration is based on the discretion of the treating clinician.
PFO closure is associated with a low complication rate, but new onset atrial fibrillation and associated thromboembolism can occur.
NHS England commissions device closure of PFO for the secondary prevention of a cryptogenic stroke in approved centres.
Other potential indications for device closure include decompression sickness, migraine with aura and platypnoea-orthodeoxia syndrome but fall outside the present commissioning process in UK.
Fig 4.

The diagnosis of a patent foramen ovale in patients with cryptogenic stroke. CT = computed tomography; CTA = computed tomography angiography; ECG = electrocardiography; HbA1c = glycated haemoglobin; INR = international normalised ratio; MRA = magnetic resonance angiography; MRI = magnetic resonance imaging; PFO = patent foramen ovale; U&Es = urea and electrolytes.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Additional figures.
Acknowledgements
We would like to thank Mr Christopher Hesketh, chief physiological measurement technician, Blackpool Teaching Hospitals NHS Foundation Trust, for providing echocardiography images.
References
- 1.American Stroke Association . Understanding diagnosis and treatment of cryptogenic stroke. American Stroke Association, 2021. www.stroke.org/-/media/Stroke-Files/Cryptogenic-Professional-Resource-Files/Cryptogenic-Professional-Guide-ucm-477051.pdf [Accessed 20 March 2021]. [Google Scholar]
- 2.Giblett JP, Abdul-Samad O, Shapiro LM, Rana BS, Calvert PA. Patent foramen ovale closure in 2019. Interv Cardiol 2019;14:34–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Collado FMS, Poulin MF, Murphy JJ, Jneid H, Kavinsky CJ. Patent foramen ovale closure for stroke prevention and other disorders. J Am Heart Assoc 2018;7:e007146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gomperts N, Fowler R, Horlick E, McLaughlin P. A broken heart: right-to-left shunt in the setting of normal cardiac pressures. Can J Cardiol 2008;24:227–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alsheikh-Ali AA, Thaler DE, Kent DM. Patent foramen ovale in cryptogenic stroke: incidental or pathogenic? Stroke 2009;40:2349–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ali Ebrahimi H, Hamzeaie Moghadam A, Aredestani E. Evaluation of patent foramen ovale in young adults with cryptogenic stroke. ARYA Atheroscler 2011;7:74–7. [PMC free article] [PubMed] [Google Scholar]
- 7.Yuan K, Kasner SE. Patent foramen ovale and cryptogenic stroke: diagnosis and updates in secondary stroke prevention. Stroke Vasc Neurol 2018;3:84–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rana BS, Thomas MR, Calvert PA, Monaghan MJ, Hildick-Smith D. Echocardiographic evaluation of patent foramen ovale prior to device closure. JACC Cardiovasc Imaging 2010;3:749–60. [DOI] [PubMed] [Google Scholar]
- 9.Jatav RK, Kumbhare MB, Surender T, Rachan C, Krishna TVV. Atrial septal aneurysm in adult patients: spectrum of clinical, echocardiographic presentation and to propose a new classification on the basis of trans-thoracic-two-dimensional echocardiography. Int J Res Med Sci 2014;2:708–17. [Google Scholar]
- 10.Elmariah S, Furlan AJ, Reisman M, et al. Predictors of recurrent events in patients with cryptogenic stroke and patent foramen ovale within the CLOSURE I (Evaluation of the STARFlex Septal Closure System in Patients with a Stroke and/or Transient Ischemic Attack Due to Presumed Paradoxical Embolism Through a Patent Foramen Ovale) trial. JACC Cardiovasc Interv 2014;7:913–20. [DOI] [PubMed] [Google Scholar]
- 11.Thaler DE, Ruthazer R, Di Angelantonio E, et al. Neuroimaging findings in cryptogenic stroke patients with and without patent foramen ovale. Stroke 2013;44:675–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kent DM, Saver JL, Ruthazer R, et al. Risk of paradoxical embolism (RoPE)-estimated attributable fraction correlates with the benefit of patent foramen ovale closure: an analysis of 3 trials. Stroke 2020;51:3119–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kent DM, Ruthazer R, Weimar C, et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke. Neurology 2013;81:619–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Furlan AJ, Reisman M, Massaro J, et al. Closure or medical therapy for cryptogenic stroke with patent foramen ovale. N Engl J Med 2012;366:991–9. [DOI] [PubMed] [Google Scholar]
- 15.Saver JL, Carroll JD, Thaler DE, et al. Long-term outcomes of patent foramen ovale closure or medical therapy after stroke. N Engl J Med 2017;377:1022–32. [DOI] [PubMed] [Google Scholar]
- 16.Meier B, Kalesan B, Mattle HP, et al. Percutaneous closure of patent foramen ovale in cryptogenic embolism. N Engl J Med 2013;368:1083–91. [DOI] [PubMed] [Google Scholar]
- 17.Mas JL, Derumeaux G, Guillon B, et al. Patent foramen ovale closure or anticoagulation vs. antiplatelets after stroke. N Engl J Med 2017;377:1011–21. [DOI] [PubMed] [Google Scholar]
- 18.Abdelghani M, El-Shedoudy SAO, Nassif M, Bouma BJ, de Winter RJ. Management of patients with patent foramen ovale and cryptogenic stroke: an update. Cardiology 2019;143:62–72. [DOI] [PubMed] [Google Scholar]
- 19.Ozdemir AO, Tamayo A, Munoz C, Dias B, Spence JD. Cryptogenic stroke and patent foramen ovale: clinical clues to paradoxical embolism. J Neurol Sci 2008;275:121–7. [DOI] [PubMed] [Google Scholar]
- 20.Sanna T, Diener HC, Passman RS, et al. Cryptogenic stroke and underlying atrial fibrillation. N Engl J Med 2014;370:2478–86. [DOI] [PubMed] [Google Scholar]
- 21.Hviid CVB, Simonsen CZ, Hvas AM. Recurrence risk in patients with cryptogenic stroke, patent foramen ovale, and thrombophilia: a systematic review and meta-analysis. Thromb Haemost 2019;119:1839–48. [DOI] [PubMed] [Google Scholar]
- 22.Linnemann B, Hart C. Laboratory diagnostics in thrombophilia. Hamostaseologie 2019;39:49–61. [DOI] [PubMed] [Google Scholar]
- 23.Katsanos AH, Psaltopoulou T, Sergentanis TN, et al. Transcranial Doppler versus transthoracic echocardiography for the detection of patent foramen ovale in patients with cryptogenic cerebral ischemia: A systematic review and diagnostic test accuracy meta-analysis. Ann Neurol 2016;79:625–35. [DOI] [PubMed] [Google Scholar]
- 24.Søndergaard L, Kasner SE, Rhodes JF, et al. Patent foramen ovale closure or antiplatelet therapy for cryptogenic stroke. N Engl J Med 2017;377:1033–42. [DOI] [PubMed] [Google Scholar]
- 25.Nasir UB, Qureshi WT, Jogu H, et al. Updated meta-analysis of closure of patent foramen ovale versus medical therapy after cryptogenic stroke. Cardiovasc Revasc Med 2019;20:187–93. [DOI] [PubMed] [Google Scholar]
- 26.Lee PH, Song JK, Kim JS, et al. Cryptogenic stroke and high-risk patent foramen ovale: The DEFENSE-PFO Trial. J Am Coll Cardiol 2018;71:2335–42. [DOI] [PubMed] [Google Scholar]
- 27.Kasner SE, Swaminathan B, Lavados P, et al. Rivaroxaban or aspirin for patent foramen ovale and embolic stroke of undetermined source: a prespecified subgroup analysis from the NAVIGATE ESUS trial. Lancet Neurol 2018;17:1053–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mas JL, Arquizan C, Lamy C, et al. Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N Engl J Med 2001;345:1740–6. [DOI] [PubMed] [Google Scholar]
- 29.Abdelaziz HK, Saad M, Abuomara HZ, et al. Long-term outcomes of patent foramen ovale closure or medical therapy after cryptogenic stroke: A meta-analysis of randomized trials. Catheter Cardiovasc Interv 2018;92:176–18. [DOI] [PubMed] [Google Scholar]
- 30.Maloku A, Hamadanchi A, Franz M, et al. [Patent foramen ovale-When to close and how?] Herz 2021;46:445–51. [DOI] [PubMed] [Google Scholar]
- 31.Kosehan D, Akin K, Koktener A, et al. Interatrial shunt: diagnosis of patent foramen ovale and atrial septal defect with 64-row coronary computed tomography angiography. Jpn J Radiol 2011;29:576–82. [DOI] [PubMed] [Google Scholar]
- 32.Pristipino C, Sievert H, D'Ascenzo F, et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur Heart J 2018;40:3182–3. [DOI] [PubMed] [Google Scholar]
- 33.Hornung M, Bertog SC, Franke J, et al. Long-term results of a randomized trial comparing three different devices for percutaneous closure of a patent foramen ovale. Eur Heart J 2013;34:3362–9. [DOI] [PubMed] [Google Scholar]
- 34.NHS England . Percutaneous patent foraman ovale closure for the prevention of recurrent cerebral embolic stroke in adults (around age 60 years and under). NHS, 2019. [Google Scholar]
- 35.National Institute for Health and Care Excellence . Percutaneous closure of patent foramen ovale to prevent recurrent cerebral embolic events: Interventional procedures guidance [IPG472]. NICE, 2013. www.nice.org.uk/guidance/ipg472 [Google Scholar]
- 36.Caretta G, Robba D, Bonadei I, et al. Multiorgan paradoxical embolism consequent to acute pulmonary thromboembolism with patent foramen ovale: a case report. Cases Journal 2009;2:8358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ahmed S, Siddiqui AK, Mattana J, Sadiq A, Borgen E. Paradoxical arterial emboli causing acute limb ischemia in a patient with essential thrombocytosis. Am J Med Sci 2003;326:156–8. [DOI] [PubMed] [Google Scholar]
- 38.Dao CN, Tobis JM. PFO and paradoxical embolism producing events other than stroke. Catheter Cardiovasc Interv 2011;77:903–9. [DOI] [PubMed] [Google Scholar]
- 39.Pristipino C, Germonpré P, Toni D, et al. European position paper on the management of patients with patent foramen ovale. Part II - Decompression sickness, migraine, arterial deoxygenation syndromes and select high-risk clinical conditions. Eur Heart J 2021;42:1545–53. [DOI] [PubMed] [Google Scholar]
- 40.Landzberg MJ, Khairy P. Indications for the closure of patent foramen ovale. Heart 2004;90:219–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Honěk J, Šrámek M, Šefc L, et al. Effect of catheter-based patent foramen ovale closure on the occurrence of arterial bubbles in scuba divers. J Am Coll Cardiol Intv 2014;7:403–8. [DOI] [PubMed] [Google Scholar]
- 42.Schwedt TJ, Demaerschalk BM, Dodick DW. Patent Foramen ovale and migraine: a quantitative systematic review. Cephalalgia 2008;28:531–40. [DOI] [PubMed] [Google Scholar]
- 43.Finocchi C, Del Sette M. Migraine with aura and patent foramen ovale: myth or reality? Neurological Sciences 2015;36:61–6. [DOI] [PubMed] [Google Scholar]
- 44.Mattle HP, Evers S, Hildick-Smith D, et al. Percutaneous closure of patent foramen ovale in migraine with aura, a randomized controlled trial. Eur Heart J 2016;37:2029–36. [DOI] [PubMed] [Google Scholar]
- 45.Blanche C, Noble S, Roffi M, et al. Platypnea-orthodeoxia syndrome in the elderly treated by percutaneous patent foramen ovale closure: a case series and literature review. Eur J Intern Med 2013;24:813–7. [DOI] [PubMed] [Google Scholar]
- 46.Shah Ashish H, Osten M, Leventhal A, et al. Percutaneous intervention to treat platypnea–orthodeoxia syndrome. J Am Coll Cardiol Intv 2016;9:1928–38. [DOI] [PubMed] [Google Scholar]
- 47.Flocco G, Crespo HJ, Matute CM, Lindenmeyer C, Cubeddu RJ. Implications of patent foramen ovale in patients undergoing liver transplantation. American Journal of Gastroenterology 2018;113:S477–9. [Google Scholar]