

Abstract
Introduction
Arterial hypertension (AH) and type 2 diabetes (T2D) represent a significant burden for the public health system, with an exceptionally high prevalence in patients aged ≥65 years. This study aims to test the acceptability, clinical effectiveness, and cost-effectiveness of telemonitoring in elderly patients with AH and T2D at the primary care level.
Methods
A m ulti-centre, prospective, randomized, controlled t rial w ill be conducted. Patients a ged ≥ 65 y ears with AH and T2D will be randomized in a 1:1 proportion to a mHealth intervention or standard care group. Patients in the intervention group will measure their blood pressure (BP) twice weekly and blood glucose (BG) once monthly. The readings will be synchronously transmitted via a mobile application to the telemonitoring platform, where they will be reviewed by a general practitioner who will indicate changes in measurement regimen or carry out a teleconsultation. The primary endpoint will be a change in systolic BP (SBP) and glycated haemoglobin (HbA1c) relative to standard care up to 12 months after inclusion. Secondary endpoints will be a change in other observed clinical variables, quality-of-life indexes, and costs.
Expected results
Telemonitoring will be an acceptable method of care associated with significant reductions in SBP and HbA1c levels and an increase in quality-of-life indexes in the intervention group. However, the cost-effectiveness threshold (incremental cost-effectiveness ratio below €25,000/quality-adjusted life year) might not be reached.
Conclusion
This study will provide new evidence for scaling up telemonitoring network at the primary care level and modifying telemonitoring protocols to achieve the best clinical and cost-effective outcomes.
Keywords: mobile health, telemonitoring, blood pressure, blood glucose, HbA1c, aged, primary health care, costs
Izvleček
Uvod
Arterijska hipertenzija (AH) in sladkorna bolezen (SB) tipa 2 predstavljata veliko breme javnozdravstvenemu sistemu. Njuna prevalenca narašča s starostjo in je še posebno visoka v skupini starejših bolnikov. Eno od metod za izboljšanje njune urejenosti predstavlja telemonitoring krvnega tlaka (KT) in krvnega sladkorja (KS). Namen raziskave je oceniti sprejemljivost telemonitoringa, njegovo klinično učinkovitost in učinkovitost glede na stroške v skupini starejših bolnikov z AH in SB tipa 2 na primarni ravni.
Metode
Izvedli bomo multicentrično, prospektivno, randomizirano, kontrolirano raziskavo. Bolnike, stare ≥65 let z AH in SB tipa 2, bomo razvrstili naključno v razmerju 1 : 1 v skupino s telemonitoringom (intervencijska skupina) in standardno oskrbo (kontrolna skupina). Bolniki v intervencijski skupini bodo opravljali meritve KT 2-krat tedensko in meritve KS 1-krat mesečno. Opravljene meritve se bodo preko mobilne aplikacije sinhrono prenesle v telemedicinski portal, kjer jih bo pregledal telemedicinski koordinator. Ta bo indiciral spremembe v protokolu izvajanja meritev ali potrebo po telekonzultaciji z izbranim zdravnikom. Bolniki v kontrolni skupini bodo prejeli zgolj standardno oskrbo. Klinično učinkovitost bomo ocenili z oceno razlike v sistolnem KT (SKT) in vrednostih glikiranega hemoglobina (HbA1c) glede na standardno oskrbo po 12 mesecih spremljanja. Sočasno bomo ocenili tudi razlike v diastolnem KT, vrednostih KS na tešče, lipidnem profilu in indeksu telesne mase glede na standardno oskrbo po 12 mesecih spremljanja. Za oceno sprememb v kakovosti življenja bomo primerjali razlike v vrednostih na lestvici ADS, vprašalniku EQ-5D-5L in lestvici EQ-VAS glede na standardno oskrbo po 12 mesecih spremljanja. Učinkovitost telemonitoringa glede na stroške bomo ocenili z oceno razmerja prirastka stroškov glede na prirastek učinkovitosti (ICER) med obema skupinama po 12 mesecih spremljanja. Stroške bomo ocenili z oceno stroškov dela in materialnih stroškov. Učinkovitost bomo ocenili z oceno prirastka let življenja, uteženih s kakovostjo življenja (QALY), ki jih bomo ocenili s pomočjo vprašalnika EQ-5D-5L in lestvice EQ-VAS. Sprejemljivost intervencije bomo kvalitativno ocenili s pomočjo strukturiranih polodprtih intervjujev.
Pričakovani rezultati
Pričakujemo, da bo telemonitoring med bolniki sprejemljiva metoda oskrbe na daljavo in da bo povezan s pomembnim znižanjem vrednosti SKT ter HbA1c in izboljšanjem indeksov kakovosti življenja v intervencijski skupini. Obstaja verjetnost, da ne bomo uspeli dokazati, da je ICER < 25.000 €/QALY, kar je v Sloveniji trenutno meja za stroškovno učinkovitost intervencije.
Zaključek
Raziskava bo zagotovila nove dokaze za širjenje mreže telemonitoringa na primarnem nivoju in spremembo protokolov vodenja kroničnih bolnikov na način, da bodo dosežene čim boljša klinična in stroškovna učinkovitost ter dobra adherenca bolnikov.
Ključne besede: mobilno zdravje, krvni tlak, krvni sladkor, starostniki, primarna raven, stroški
1. Introduction
Arterial hypertension (AH) and type 2 diabetes (T2D) are leading chronic diseases that frequently co-occur, share the same risk factors, and together account for nearly 70% of all-cause deaths (1). The prevalence of their comorbidity increases with age and is particularly high in the elderly group. It is estimated that up to 75% of patients aged ≥65 years have AH, while 25% have T2D (2, 3). Despite the potential for successful treatment, their prevalence is steadily increasing (2, 3). Consequently, these global trends place a significant burden on population health and a financial burden on healthcare systems (2, 3).
One approach to reversing the rising trends, empowering chronic patients, and reducing the incidence of secondary complications from uncontrolled blood pressure (BP) and blood glucose (BG), could be integrated care supported by BP and BG telemonitoring (1, 4, 5, 6). Telemonitoring is a subset of telemedicine and refers to the transmission of physiological data, such as BP and BG values, via automated electronic means or via web-based or telephone data. The data received allows physicians to interpret the data synchronously and make timely decisions about the patient’s treatment (5, 6, 7). Currently, telemonitoring is often combined with teleconsultations, which can be synchronous via videoconferencing devices or asynchronous via email, internet, or mobile phones (57). The combination of frequent BP/BG measurements and timely feedback/consultation from the registered nurse or physician is the main reason why telemonitoring has the potential to significantly improve clinical outcomes (5, 6, 7, 8). In addition, telemonitoring indirectly promotes patient empowerment by increasing their engagement, knowledge, and skills needed to manage their disease (8).
Previous studies have found that BP and BG telemonitoring combined with teleconsultations lasting 12 months or longer had the greatest effect on BP and BG reduction, while isolated interventions lasting 6 months or less were unsuccessful in the long term (1, 5, 7, 9). Meta-analyses of randomized clinical trials examining the clinical effectiveness of BP and BG telemonitoring found a 5-mmHg reduction in SBP and a 0.3% reduction in HbA1c compared with standard care 12 months after study inclusion (1, 5, 7, 9). More complex telehealth interventions may yield even better results, but are associated with higher costs (10).
In Slovenia the healthcare system is based on the Bismarck model, which provides equal and fair access to health care for all patients (4). In 2011, a new working model was introduced in Slovenian family medicine practices. A registered nurse was added to the team consisting of a family physician and a practice nurse. A registered nurse took over the preventive activities and management of patients with stable chronic diseases (including AH and T2D), providing standardized and integrated care at the level of screening, treatment, education, and quality control (11). Patients with AH or T2D are seen by their family physician and registered nurse at least once a year. The physician examines patients, refers them to the laboratory, assesses disease control and the need for titration of therapy, while the registered nurse screens patients for AH/T2D complications, assesses their psychosocial status, educates them about non-pharmacological measures, and refers them to additional health promotion activities within the health education centre, including nutritionists, psychologists or psychotherapists, as appropriate (11, 12). A general problem with previous research is that it has neglected the central role of primary care in the management of chronic diseases, such as AH and T2D. Clinical pathways have generally been designed to be conducted in clinical settings rather than small healthcare centres. Studies were conducted in younger, motivated patients with either AH or T2D, rather than in older, multimorbid patients with little knowledge about the use of modern technologies. The latter have the highest risk of cardiovascular mortality and could benefit significantly from telemonitoring interventions (13). Furthermore, a high threshold for clinical significance in relation to BP and BG reduction calls into question the clinical relevance of telemonitoring. Currently, a 10-mmHg decrease in systolic BP (SBP) and a 0.5% reduction in glycated haemoglobin (HbA1c) are considered clinically relevant (14, 15). Moreover, there is a need for additional evidence on the acceptability of telemonitoring in the elderly group.
From the perspective of the Slovenian healthcare system, there is currently a lack of self-management support for patients with AH and T2D (4, 16). In addition, the challenges of the ageing population and the shortage of primary care physicians require the testing of care models that shift responsibility for their health vertically to patients to a greater extent (16).
Finally, there is insufficient evidence on the cost-effectiveness of telemonitoring interventions to drive our research. Previous studies have found telemonitoring to be more cost-effective in patients with T2D, while cost-effectiveness was achieved in a group of patients with AH assuming a lifetime telemonitoring effect (17, 18). This was found with an incremental cost-effectiveness ratio (ICER) of £20,000 per quality-adjusted life year (QALY) (17). Currently, a higher ICER threshold of €25,000/QALY is considered cost-effective in Slovenia (19). A cost-effectiveness analysis in a group of elderly patients with AH and T2D at the primary care level has not yet been published.
This study thus aims to test the acceptability, clinical effectiveness, and cost-effectiveness of telemonitoring in elderly patients with AH and T2D at the primary care level. The specific goals of the study are: (a) to assess the effect of telemonitoring on observed clinical variables and quality of life indexes up to 12 months after inclusion, (b) to compare the difference in costs relative to the difference in QALY between telemonitoring and standard care group 12 months after inclusion, and (c) to assess acceptability of telemonitoring among elderly patients and healthcare workers.
2. Methods
2.1. Study design
A multi-centre, prospective, randomized controlled pilot study will be conducted.
2.2. Study duration
The study will be conducted from March 2021 to June 2023.
2.3. Setting
The study will be conducted in three primary healthcare centres (PHC) in Slovenia. The PHC Ljubljana will reflect the urban population, while two peripheral PHCs (Trebnje, Slovenj Gradec) will reflect the rural population.
2.4. Study population
The population will comprise patients aged ≥65 years with AH and T2D. Demographic characteristics are expected to reflect the general population in this age group, with a mean age of over 70 years and a slightly higher proportion of women than men.
2.5. Inclusion and exclusion criteria
Inclusion criteria will be: (a) ≥65 years of age, (b) confirmed diagnosis of AH with a 7-day mean home BP values ≥135/85 mmHg or with 24-hour blood pressure monitoring mean ≥130/80 mmHg (20), (c) confirmed diagnosis of T2D with fasting BG value ≥7.0 mmol/l or venous plasma glucose ≥11.1 mmol/l 2 hours after glucose tolerance test with 75 g glucose intake or any random opportunity (21), (d) diagnosis of AH and T2D for at least one year, and (e) ability to use telemonitoring equipment.
Exclusion criteria will be: (a) <65 years of age, (b) T2D requiring insulin treatment at inclusion, (c) gestational diabetes or type 1 diabetes, and (d) cognitive impairment, (e) inability to use telemonitoring equipment for any reason.
2.6. Selection of patients
Eligible patients will be invited to participate in the study by their GPs. Patients will receive an explanation of the study’s goals, which will be additionally described on the participant information sheet. Patients who will decide to participate in the study will sign the informed consent form.
2.7. Randomisation
After consenting to participate, patients will be randomized to either the telemonitoring (intervention) group or the standard care (control) group using simple 1:1 randomization (22). The randomization list will be generated by an independent project manager. To avoid randomization bias, patient identification numbers will be used instead of names. The first patient on the list will be randomized to the intervention group, the second patient to the control group, and so on.
2.8. Intervention group
2.8.1. Telemonitoring package and education of patients
At baseline, patients in the intervention group will receive a telemonitoring package that will include an Android smartphone (LG K22®), a validated BP monitor (A&D 651 BLE®), a validated BG monitor (Contour Next One®), and instructions for use. Each patient will receive one hour of training with a nurse on the measurement protocol and how to use the telemonitoring package.
2.8.2. Telemedicine infrastructure
The telemedicine infrastructure will comprise medical sensors (BP and BG monitors), a hub (a smartphone with a mobile application), and a telemedicine platform. First, the results from the medical sensors will be transmitted to the mobile application using Bluetooth wireless technology. The mobile application will serve as a hub from where measurement results will be transferred to the telemedicine cloud platform via a 4G or 5G mobile standard. Patients will communicate with the telemedicine centre coordinator through the application (via messages or video calls). The telemedicine cloud platform will serve as the central data processing point. The platform cloud will be hosted by a third-party provider and will be available to end-users via the internet. The data received will be encrypted and compliant with the General Data Protection Regulation.
2.8.3. Blood pressure measurement
Patients will be instructed to measure their BP twice weekly in the morning and evening in a quiet room after resting for 5 minutes in a seated position with their back and arm supported (Figure 1). Two measurements will be taken, with a programmed 1 minute pause between the first and second measurements. If indicated, patients will perform a 7-day profile of morning and evening BP measurements (20).
Figure 1.
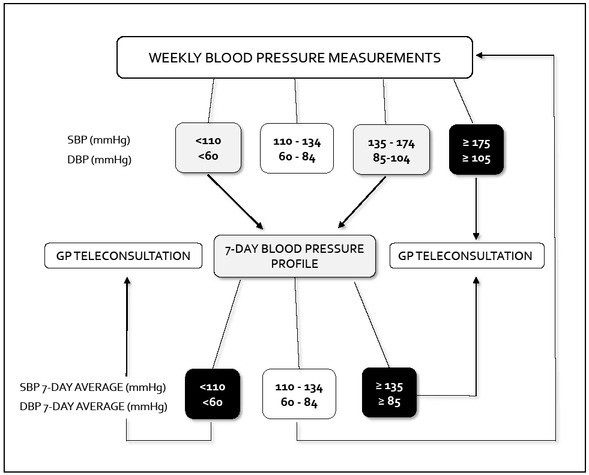
Arterial hypertension telemedicine management algorithm (SBP – systolic blood pressure; DBP – diastolic blood pressure; GP – general practitioner).
2.8.4. Blood glucose measurement
Patients will be instructed to measure their BG value once a month (Figure 2). They will take two measurements: the morning measurement on an empty stomach and the measurement 90 minutes after lunch. If indicated, patients will perform a one-day BG profile (values on an empty stomach, 90 minutes after breakfast, before lunch, 90 minutes after lunch, before dinner, 90 minutes after dinner) (21).
Figure 2.
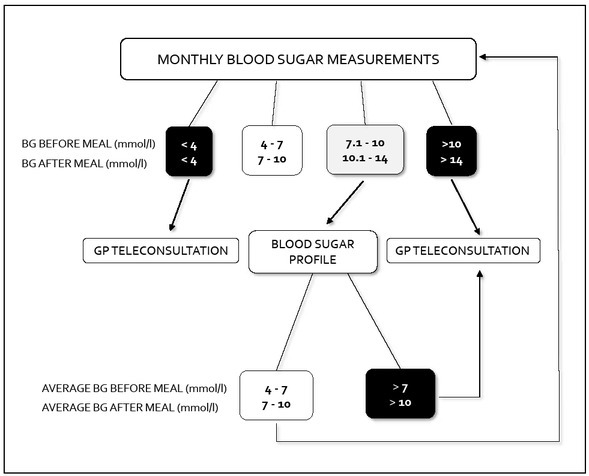
Diabetes mellitus type 2 telemedicine management algorithm (BG – blood glucose; GP – general practitioner).
2.8.5. Management of patients in telemedicine centre
The telemedicine centre will be coordinated by a GP who will review the recorded values and act as a link between other GPs and the included patients. Patients will be treated according to the latest guidelines, which recommend aiming for BP in the home setting <135/85 mmHg, maintaining fasting BG <7 mmol/l and postprandial BG <10 mmol/l (20, 21). However, as the studied population will have T2D and will be ≥65 years old, target home SBP will be 125-135 mmHg and DBP 7079 mmHg (20). Transmitted values will be marked with three colours indicating normal, derailed, or extremely derailed values (Figure 1 and Figure 2). Green (shown as white) will reflect normal values and suggest no changes in monitoring regimen. Yellow (shown as grey) will reflect derailed values and indicate a change in the telemonitoring regimen. Red (shown as black) will reflect extremely derailed values and indicate the need for immediate teleconsultation with a GP, further workup, or a change in the treatment regimen.
2.9. Control group
The control group will receive standard care, described in more detail in the introduction, and will be treated according to the latest guidelines (20, 21).
2.10. Data collection
We will collect various variables from different categories (Table 1). The data sources will be medical records, the telemedicine platform, questionnaires, and interviews conducted at enrolment and at the end of the study.
Table 1.
Study data collection list (AH – arterial hypertension; T2D – type 2 diabetes; CVD – cardiovascular disease; HbA1c – glycated haemoglobin; BG – blood glucose; BMI – body mass index; AUDIT-C – Alcohol Use Disorders Identification Test; ADS – Appraisal of Diabetes Scale; EQ-5D - EuroQol 5-Dimension; QALY – quality adjusted life year).
| CATEGORY | DATA VARIABLE | MEASUREMENT DESCRIPTION |
|---|---|---|
| Demographic data | Age | In full years |
| Gender | Male or female | |
| Education | Primary school, high school graduate, vocational school, bachelor’s degree, master’s degree, doctoral degree | |
|
| ||
| Marital status | Married, divorced, widowed, single | |
| Clinical history | Duration of AH and T2D | In full years |
| Current therapy | Name of drug and dose | |
| Family history of CVD | Yes or no | |
| Associated diseases | Name of disease | |
|
| ||
| Behavioural risk factors | Smoking | Yes or no |
| Daily activity | Adequate or inadequate | |
| Eating habits and behaviours | Healthy or unhealthy | |
| Alcohol use | Score on the AUDIT-C questionnaire | |
|
| ||
| Clinical characteristics | SBP and DBP | 7-day average of morning and evening measurements |
| HbA1c | Laboratory value | |
| Fasting BG | Laboratory value | |
| Lipid profile | Laboratory values | |
| BMI | Measured value | |
|
| ||
| Quality of life | Quantitative | Score on the ADS and EQ-5D scales |
| Qualitative | Semi-structured interviews | |
|
| ||
| Acceptability of intervention | Qualitative | Semi-structured interviews |
|
| ||
| Cost-effectiveness | Costs | Labour costs and material costs per patient |
| Effect | Change in QALY per patient | |
2.10.1. Behavioural risk factors
We will assess daily activity by weekly high- or moderate-intensity physical activity duration. More than 150 minutes of moderate-intensity or more than 75 minutes of high-intensity physical activity per week will be considered adequate (23).
Eating habits and behaviours will be assessed using a structured questionnaire regularly used in Slovenian model practices. We will determine four components of healthy eating habits and behaviours: the daily number of meals, frequency of vegetable consumption, salting food at the table, and type of fat intake. Eating fewer than 3 meals per day, consuming less than one serving of vegetables per day, salting food at the table, and using margarine, butter, cream, and pork fat will be considered unhealthy (24).
We will assess alcohol use with the Alcohol Use Disorders Identification Test (AUDIT-C). We will use the Slovenian validated version, which suggests 6 points for men and 5 points for women as cut-offs for identifying hazardous or harmful drinkers (25).
2.10.2. Systolic and diastolic blood pressure values
SBP and DBP values will be checked at baseline, after 6 months, and after 12 months using validated BP monitors. SBP and DBP values will be defined as 7-day averages of morning and evening measurements, as recommended by the European Society of Cardiology (20).
2.10.3. Glycaemic control and lipid profile
HbA1c level, fasting BG value, and lipid profile values will be determined from peripheral venous blood sampling at baseline and after 12 months. Additionally, fasting BG value will be checked after 6 months using a validated finger-stick BG monitor.
2.10.4. Quality of life
A change in quality of life from baseline up to 12 months will be assessed with two scales. First, the patient’s adjustment to diabetes, psychological burden of self-management, and behaviour modifications will be assessed using the Appraisal of Diabetes Scale (ADS) (26). ADS is a 7-item self-report scale in which respondents rate each statement on a 5-point Likert scale. The smaller the total score, the more positive the appraisal strategy. The related questionnaire will be validated independently of this study.
Second, for the purpose of cost-effectiveness analysis we will assess changes in QALY using the EQ-5D-5L (EuroQol 5-Dimension 5-Level) and EQ VAS (EuroQol Visual Analogue Scale) instruments, which are a standardized, valid, and reliable tools for measuring patients’ health-related quality of life. To calculate the utilities, the value set for Slovenia will be used (27).
2.10.5. Acceptability of intervention
Acceptability of the intervention will be qualitatively assessed through semi-structured interviews with patients, nurse practitioners, and GPs. The initial standardized interview guide will be based on previous evidence and principles of the latest theoretical framework of acceptability (TFA) (28). The TFA describes acceptability as a construct with seven domains, including affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness, and self-efficacy (28). Furthermore, interview guides will cover the health context, recruitment process, coping with technology, telemonitoring routine, change in self-management skills, impact on mental health, and change in patient-doctor relationship. Initial guides might be modified after piloting the first 10 interviews.
2.10.6. Costs
To measure costs, a human capital approach will be used. The costs will include material and labour costs. Material costs will be determined by depreciation of the equipment. Labour costs will be determined by the following factors: time spent by the telemedicine centre coordinator reviewing data and communicating with patients and their GPs, time spent training patients to use the telemonitoring package, frequency of additional patient teleconsultations with GPs, frequency of additional outpatient visits and time spent by patient on the additional tasks needed. As the study period will be 1 year, no discounting will be applied.
2.11. Endpoints
The primary endpoint will be a change in SBP and HbA1c relative to the standard care up to 12 months after inclusion.
Secondary endpoints will be a change in diastolic BP (DBP), fasting BG, lipid profile, body mass index, ADS score, EQ-5D-5L score, and EQ VAS score relative to the standard care up to 12 months after inclusion.
2.12. Sample size and power of the research
Because of limited telemonitoring equipment, our sample size is limited to 60 patients in the intervention group, altogether 120 patients with the control group included. Therefore, instead of calculating the sample size to demonstrate a 10-mmHg reduction in SBP and a 0.5% reduction in HbA1c, we calculated the expected minimum detectable difference between groups with the planned sample size. We considered multiple studies to estimate the expected standard deviation (SD) of a change in SBP and HbA1c in the intervention and control groups 12 months after inclusion (29, 30, 31, 32). Power calculations were performed using a two-tailed independent equal-variance t test in PASS 14 power analysis software.
For a change in SBP, the planned sample size of 120 achieves a power of 80% to reject the null hypothesis of equal means with a significance level of 0.05 when the population mean difference between groups is at least 6.2 mmHg (if SD is equal to 12 for both groups) or 10.8 mmHg (if SD is 21). For the change in HbA1c, this is possible when the population mean difference between groups is at least 0.7% (if SD is equal to 1.3 for both groups) or 1.2% (if SD is 2.4).
2.13. Statistical analysis
Data will be analysed using the R statistical software. Numeric variables will be summarized with means and standard deviations or medians and interquartile ranges. Categorical variables will be presented with absolute and relative frequencies. Differences between groups in numeric variables will be tested using a two-tailed independent samples t-test or the Mann-Whitney U-test. Differences between groups in categorical variables will be tested using the chi-squared test or Fisher’s exact test. In the case of significant differences between groups at baseline, regression methods will be used. We will consider a p-value of <0.05 as statistically significant.
2.14. Qualitative analysis
Qualitative analysis will be conducted using an inductive thematic analysis approach (33). The semi-structured interviews will be recorded, transcribed verbatim and transcriptions will later be checked for accuracy. Two independent researchers will analyse data in three steps: open coding, formation of subthemes and themes, abstraction. Sample size will be determined by inductive thematic saturation. After independent coding, the final thematic analysis will be compiled through a triangulation process among coders. If consensus between two coders on the grouping of codes will not be achieved, an experienced supervisor will be consulted (33).
2.15. Cost-effectiveness analysis
Cost-effectiveness will be expressed as an ICER, in which the difference in costs between the two approaches (telemonitoring vs. standard care) and the difference in QALYs will be compared. Difference in QALYs will be measured using the EQ-5D-5L and EQ VAS instruments, difference in costs will be estimated from calculated material and labour costs (27). Currently, an ICER in Slovenia is set to €25,000/QALY (19). This threshold will be considered to determine whether the intervention is cost-effective.
3. Discussion
This is the first study to investigate the feasibility, clinical effectiveness, and cost-effectiveness of BP and BG telemonitoring in elderly patients with comorbid AH and T2D at the primary care level.
In previous studies, older multimorbid patients were often excluded because they could not use modern technologies, were not motivated to participate in the study, or needed additional support from family members (1, 5, 7). According to recent projections, the global population of people over 65 years of age will more than double by 2050, while the proportion of elderly people in the global population will increase from 9% to 16% (34). Therefore, exploring novel approaches such as telemonitoring to promote patient-centred care focused on quality of life and self-management support is essential.
The reason for the slow integration of telemonitoring into daily practice could be its unconvincing clinical and cost-effectiveness (5, 7, 17, 18). From the healthcare workers’ perspective, the main barriers are the lack of adaptation to workflows within practices, concerns about creating anxiety and dependency, and fear of additional workload (35). All these concerns should be taken into account when developing future models of care.
The strength of this pilot study lies in the sufficient follow-up time, the multi-centre randomized controlled nature, the complexity of the observed outcomes, and the originality of the population observed. Moreover, we designed the inclusion criteria to include not only patients with derailed BP (>150/100 mmHg) and HbA1c (>7.5%) values, but also those with relatively well-controlled parameters. This was done to capture the population that would otherwise be treated at the primary care level. This could result in lower observed differences, but will give us diversity in the observed population, which will also be reflected in the results of the qualitative content analysis. Due to multimorbidity, intensive BP measurement regimen, and difficulty in completing regular check-ups with their GPs and specialists in the control group during the COVID-19 pandemic, we expect to observe larger differences between groups compared to previous studies (1, 5, 7). In terms of cost-effectiveness, we expect an increase in EQ-5D-5L and EQ VAS index scores. However, based on previous evidence, the threshold for cost-effectiveness may not be reached (17, 18).
Finally, there might be limitations in our study design. Due to the pilot nature of the study and the relatively small sample size, the power of the study will be low. In addition, we defined SBP and DBP values at baseline and follow-up as 7-day BP averages of morning and evening readings, although the gold standard is still the 24-hour average of BP monitoring (20). This was done for practical reasons, and is more reliable than in previous studies where the mean of the second and third ambulance readings was used as the primary outcome (29). Furthermore, there are some common risks of randomized controlled trials, such as loss to follow-up, the risk that randomized patients are not representative of the population studied, and imbalance between groups in baseline variables, which may affect the results.
4. Conclusion
This study will provide new evidence for scaling up a telemonitoring network at the primary care level and modifying telemonitoring protocols to achieve the best clinical and cost-effective outcomes, and good patient adherence. Further studies should examine a larger population and follow patients for at least 5 years to assess long-term outcomes. However, without recognition of telemonitoring as an essential component of chronic patient care by policymakers, further large-scale and long-term expansion is questionable.
Funding Statement
The study is funded from the SCUBY project. SCUBY is an international research project co-funded by the EU under the H2020 – Health programme (H2020-SC1) with contract number 825432 - SCUBY.
Footnotes
Conflicts of interest
The authors declare that no conflicts of interest exist.
Ethical approval and registration
The study was approved by the National Medical Ethics Committee (reference number 0120-219/2019/4) and is registered in the ISRCTN registry (https://doi.org/10.1186/ISRCTN31471852)
References
- 1.Zhang W, Cheng B, Zhu W, Huang X, Shen C. Effect of telemedicine on quality of care in patients with coexisting hypertension and diabetes: a systematic review and meta-analysis. Telemed J E Health. 2021;27(6):603–14. doi: 10.1089/tmj.2020.0122. [DOI] [PubMed] [Google Scholar]
- 2.Zhou B, Carrillo-Larco RM, Danaei G, Riley LM, Paciorek CJ, Stevens GA. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–80. doi: 10.1016/S0140-6736(21)01330-1. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi: 10.1016/j.diabres.2019.107843. et al. [DOI] [PubMed] [Google Scholar]
- 4.Klemenc-Ketiš Z, Stojnić N, Zavrnik Č, Gorenjec NR, Danhieux K, Lukančič MM. Implementation of integrated primary care for patients with diabetes and hypertension: a case from Slovenia. Int J Integr Care. 2021;21(3):15. doi: 10.5334/ijic.5637. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Omboni S, McManus Richard J, Bosworth Hayden B, Chappell Lucy C, Green Beverly B, Kario K. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension. Hypertension. 2020;76(5):1368–83. doi: 10.1161/HYPERTENSIONAHA.120.15873. et al. [DOI] [PubMed] [Google Scholar]
- 6.Vodička S, Naji HF, Zelko E. The role of telecardiology in dealing with patients with cardiac rhythm disorders in family medicine: systematic review. Zdr Varst. 2020;59(2):108–16. doi: 10.2478/sjph-2020-0014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Timpel P, Oswald S, Schwarz PEH, Harst L. Mapping the evidence on the effectiveness of telemedicine interventions in diabetes, dyslipidemia, and hypertension: an umbrella review of systematic reviews and meta-analyses. J Med Internet Res. 2020;22(3):e16791. doi: 10.2196/16791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McGloin H, O’Connell D, Glacken M, Mc Sharry P, Healy D, Winters-O’Donnell L. Patient empowerment using electronic telemonitoring with telephone support in the transition to insulin therapy in adults with type 2 diabetes: observational, pre-post, mixed methods study. J Med Internet Res. 2020;22(5):e16161. doi: 10.2196/16161. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Robson N, Hosseinzadeh H. Impact of telehealth care among adults living with type 2 diabetes in primary care: a systematic review and meta-analysis of randomised controlled trials. Int J Environ Res Public Health. 2021;18(22):12171. doi: 10.3390/ijerph182212171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Crowley MJ, Tarkington PE, Bosworth HB, Jeffreys AS, Coffman CJ, Maciejewski ML. Effect of a comprehensive telehealth intervention vs telemonitoring and care coordination in patients with persistently poor type 2 diabetes control: a randomized clinical trial. JAMA Intern Med. 2022. p. e222947. et al. [DOI] [PMC free article] [PubMed]
- 11.Poplas Susič A, Švab I, Klemenc-Ketiš Z. Upgrading the model of care in family medicine: a Slovenian example. Public Health Panorama. 2018;4(3):550–5. [Google Scholar]
- 12.Vodopivec Jamšek V. The protocol of chronic patient management in a family medicine practice. Zdrav Vestn. 2013;82:711–7. [Google Scholar]
- 13.Rodgers JL, Jones J, Bolleddu SI, Vanthenapalli S, Rodgers LE, Shah K. Cardiovascular risks associated with gender and aging. J Cardiovasc Dev Dis. 2019;6(2):19. doi: 10.3390/jcdd6020019. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–67. doi: 10.1016/S0140-6736(15)01225-8. et al. [DOI] [PubMed] [Google Scholar]
- 15.Little RR, Rohlfing CL, Sacks DB. Status of hemoglobin A1c measurement and goals for improvement: from chaos to order for improving diabetes care. Clin Chem. 2011;57(2):205–14. doi: 10.1373/clinchem.2010.148841. [DOI] [PubMed] [Google Scholar]
- 16.Švab I, Klemenc-Ketiš Z, Poplas Susič T, Rotar Pavlič D, Petek Šter M, Cedilnik Gorup E. Family medicine in Slovenia: overview of the state of affairs and suggestions for improvement. Zdrav Vestn. 2021;90(1–2):112–25. doi: 10.6016/ZdravVestn.3010. et al. [DOI] [Google Scholar]
- 17.Monahan M, Jowett S, Nickless A, Franssen M, Grant S, Greenfield S. Cost-effectiveness of telemonitoring and self-monitoring of blood pressure for antihypertensive titration in primary care (TASMINH4) Hypertension. 2019;73(6):1231–9. doi: 10.1161/HYPERTENSIONAHA.118.12415. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Warren R, Carlisle K, Mihala G, Scuffham PA. Effects of telemonitoring on glycaemic control and healthcare costs in type 2 diabetes: a randomised controlled trial. J Telemed Telecare. 2018;24(9):586–95. doi: 10.1177/1357633X17723943. [DOI] [PubMed] [Google Scholar]
- 19.Decision on setting cost-effectiveness ratio in Slovenia. 2022. https://api.zzzs.si/zzzs/info/egradiva.nsf/0/de161d25a238859cc1257c1d0026d7f9/$FILE/Podpisan%20sklep%20ICER.pdf Acessed February 26th. at.
- 20.Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–104. doi: 10.1093/eurheartj/ehy339. et al. [DOI] [PubMed] [Google Scholar]
- 21.Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2019;41(2):255–323. doi: 10.1093/eurheartj/ehz486. et al. [DOI] [PubMed] [Google Scholar]
- 22.Kim J, Shin W. How to do random allocation (randomization) Clin Orthop Surg. 2014;6(1):103–9. doi: 10.4055/cios.2014.6.1.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gelius P, Tcymbal A, Abu-Omar K, Mendes R, Tribuzi Morais S, Whiting S. Status and contents of physical activity recommendations in European Union countries: a systematic comparative analysis. BMJ Open. 2020;10(2):e034045. doi: 10.1136/bmjopen-2019-034045. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Herforth A, Arimond M, Álvarez-Sánchez C, Coates J, Christianson K, Muehlhoff E. A global review of food-based dietary guidelines. Adv Nutr. 2019;10(4):590–605. doi: 10.1093/advances/nmy130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kolšek M, Poplas Susič T, Kersnik J. Slovenian adaptation of the original AUDIT-C questionnaire. Subst Use Misuse. 2013;48(8):581–9. doi: 10.3109/10826084.2013.793354. [DOI] [PubMed] [Google Scholar]
- 26.Carey MP, Jorgensen RS, Weinstock RS, Sprafkin RP, Lantinga LJ, Carnrike CL. Reliability and validity of the appraisal of diabetes scale. J Behav Med. 1991;14(1):43–51. doi: 10.1007/BF00844767. Jr, et al. [DOI] [PubMed] [Google Scholar]
- 27.Prevolnik Rupel V, Ogorevc M. Crosswalk EQ-5D-5L value set for Slovenia. Zdr Varst. 2020;59(3):189–94. doi: 10.2478/sjph-2020-0024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):88. doi: 10.1186/s12913-017-2031-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McManus RJ, Mant J, Franssen M, Nickless A, Schwartz C, Hodgkinson J. Efficacy of self-monitored blood pressure, with or without telemonitoring, for titration of antihypertensive medication (TASMINH4): an unmasked randomised controlled trial. Lancet. 2018;391(10124):949–59. doi: 10.1016/S0140-6736(18)30309-X. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shea S, Weinstock RS, Teresi JA, Palmas W, Starren J, Cimino JJ. A randomized trial comparing telemedicine case management with usual care in older, ethnically diverse, medically underserved patients with diabetes mellitus: 5 year results of the IDEATel study. J Am Med Inform Assoc. 2009;16(4):446–56. doi: 10.1197/jamia.M3157. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Steventon A, Bardsley M, Doll H, Tuckey E, Newman SP. Effect of telehealth on glycaemic control: analysis of patients with type 2 diabetes in the Whole Systems Demonstrator cluster randomised trial. BMC Health Serv Res. 2014;14:334. doi: 10.1186/1472-6963-14-334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Karhula T, Vuorinen AL, Rääpysjärvi K, Pakanen M, Itkonen P, Tepponen M. Telemonitoring and mobile phone-based health coaching among Finnish diabetic and heart disease patients: randomized controlled trial. J Med Internet Res. 2015;17(6):e153. doi: 10.2196/jmir.4059. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020;42(8):846–54. doi: 10.1080/0142159X.2020.1755030. [DOI] [PubMed] [Google Scholar]
- 34.Marois G, Aktas A. Projecting health-ageing trajectories in Europe using a dynamic microsimulation model. Sci Rep. 2021;11(1):1785. doi: 10.1038/s41598-021-81092-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hanley J, Pinnock H, Paterson M, Mckinstry B. Implementing telemonitoring in primary care: learning from a large qualitative dataset gathered during a series of studies. BMC Fam Pract. 2018;19(1):118. doi: 10.1186/s12875-018-0814-6. [DOI] [PMC free article] [PubMed] [Google Scholar]