

Abstract
Rationale:
Much of the research linking racism-related stressors to poor health has focused on fairly non-violent forms of racism that directly impact individuals under study. Exposure to particularly extreme and/or violent racist events are increasingly visible via smartphone recordings and social media, with consistent anecdotal reports of the effects of seeing and hearing about these events on sleep among minorities who racially identify with the victims.
Objective:
This study examines whether exposure to direct and vicarious racism-related events (RREs), including more extreme events, are associated with sleep quality. Additionally, we examine effects of less and more violent direct RREs and vicarious RREs witnessed in person and via social media.
Methods:
Among 422 African-American women, we assessed exposure to RREs using a modified version of the Race-Related Events Scale and assessed sleep quality using the Pittsburgh Sleep Quality Index (PSQI). Linear regression analyses were used to model continuous global sleep.
Results:
Direct (β = 0.24 [95% CI: 0.13, 0.35]) RREs were associated with worse continuous global sleep quality scores in analyses adjusted for sociodemographics and risk factors for poor sleep. More violent direct RREs (β = 0.59 [95% CI: 0.30, 0.89]) had stronger associations with poor sleep quality than less violent direct RREs (β = 0.25 [95% CI: 0.11, 0.40]). Vicarious RREs overall (β = 0.04 [95% CI: 0.14, 0.21]) and those witnessed via social media (β = −0.07 [95% CI: 0.29, 0.14]) were not associated with global sleep quality; conversely, vicarious RREs witnessed in person were (β = 0.52 [95% CI: 0.21, 0.83]).
Conclusion:
Extreme, direct experiences of racism, particularly those that are violent in nature, are associated with poor sleep quality. However, extreme vicarious experiences are not– unless witnessed in person.
Keywords: African-americans, racism, sleep, Social determinants of health, Social media, vicarious trauma, women
1. Introduction
A large and growing body of research suggests that experiences of racism are harmful to health. Empirical evidence demonstrates fairly strong associations between self-reported experiences of discrimination and adverse health outcomes among racial/ethnic minorities, beyond the impact of racial/ethnic socioeconomic disparities and other psychosocial stressors (Lewis et al., 2015). Yet, to date, much of the empirical evidence linking self-reported experiences of discrimination with health outcomes focuses on racism-related stressors that directly impact the individual under study, as well as day-to-day, fairly non-violent events. The idea that racism-related events (RREs) that happen to family, friends, and even strangers are a salient source of psychosocial stress that may contribute to racial health inequalities has been long conceived. Nevertheless, research on indirect exposure to racism remains in its infancy (Harrell, 2000; Martz et al., 2019), despite current evidence strongly suggesting that people report discrimination toward their racial group more often than experiences directed towards themselves (Harrell, 2000), that vicarious experiences of discrimination via loved ones are particularly prevalent among African-American children and adults (Mason et al., 2017), and that experiencing discrimination through group or vicarious exposure can be distressing with implications for health similar to those of direct discrimination (Harrell, 2000). Another notable gap in studies of racism and health is the lack of assessment of exposure to more extreme, violent events (Paradies et al., 2015), whether direct or vicarious, despite increasing trends in violent hate crimes (Allam, 2020) as well as increasing coverage and accessibility to information about violent racism-related events via television and social media (i.e., police killings of unarmed African-American people) (Martz et al., 2019).
Vicarious racism is often described as “secondhand” exposure to racial discrimination directed at another individual – more specifically, hearing about or witnessing the unfair treatment of others in your racial group based on their race, including the experiences of family and friends or others (Heard-Garris et al., 2018; Neblett Jr, 2019). In the racism and health literature, the concept of linked lives recognizes the interdependence among people and the idea that events affecting one person can also affect family, friends, and others in one’s social network, supporting the potential for vicarious effects of racism (Gee et al., 2012). Expanding upon the idea of linked lives, which focuses on experiences within one’s network, even when the target of discrimination is an unknown person, vicarious exposures may have an impact. African-Americans tend to strongly identify with their racial group, having feelings of closeness and solidarity with other African-Americans; but this closeness also means that acts of racial terrorism and violence can trigger a collective sense of threat and helplessness, and common feelings of “that could have been me or a loved one,” in other members of the targeted racial group, partially via a sense of linked fate – a concept well-described among African-Americans (Dawson, 1995; Heard-Garris et al., 2018; Monk Jr, 2020). Therefore, even when an African-American person is not the direct target, RREs that happen to loved ones or other African-American people in the general population may still be stressors causing similar cognitive and emotional reactions of a direct exposure, making vicarious racism a stressor with potentially similar effects as direct exposure to racism. Vicarious discrimination may be a particularly salient stressor among African-American women as vicarious discrimination experienced via loved ones has been identified as a particularly prevalent and major form of stress among African-American women (Nuru-Jeter et al., 2009), and a sense of linked fate may be qualitatively different and stronger among African-American women compared to African-American men (Simien, 2005).
Vicarious exposures to racist events that happen to others have become increasingly visible via smartphone recordings and social media, including particularly violent events (Chae et al., 2021), and there have consistently been anecdotal reports of the effects of seeing and hearing about these events on sleep among minorities who racially identify with the victims (Pridgett, 2020). Sleep is an important physiologic activity and health behavior integral to optimal health and quality of life. Poor sleep quality is associated with several adverse chronic health outcomes, including negative mood, impaired cognition, obesity, hypertension, diabetes, stroke, and cardiovascular disease (Johnson et al., 2019; Van Dyke et al., 2016). Compared to other race/gender groups, African-American women experience worse sleep health. For instance, relative to White women, African-American women exhibit poorer sleep on multiple dimensions (Hall et al., 2009; Knutson et al., 2006; Lauderdale et al., 2009). Additionally, compared to African-American men, African-American women report significantly worse sleep quality (Johnson et al., 2016). This pattern in sleep health parallels overall gendered patterns in which women, on average, report more sleep interruptions (Burgard and Ailshire, 2013; Maume et al., 2009) and higher rates of insomnia than men (Zhang and Wing, 2006). These findings highlight the need for more research to better understand factors contributing to the disproportionate burden of poor sleep health among African-American women.
While several studies have examined racism-related stressors as an exposure associated with poor sleep (Johnson et al., 2019; Yip and Cheon, 2020), most studies focus on direct, fairly non-extreme exposure to racism. To our knowledge, no studies have separately explored associations between vicarious racism as its own construct, or more extreme, violent experiences of both direct and vicarious racism with sleep health (Lewis and McKinnon, 2019; Slopen et al., 2016). This addition to the literature may highlight an important pathway through which racism may get under the skin and cause other poor health outcomes among African-American women – through poor sleep, an important risk factor for adverse mental and physical health.
Therefore, the main objective of the current study is to separately examine direct and vicarious RREs and their relationship with sleep quality in a cohort of African-American women in the southeast US. Importantly, when measuring direct and vicarious RREs in this study, we measure not only day-to-day, fairly non-violent events that are often included in studies of racism and health, but include more extreme, violent events (Carter et al., 2013). We hypothesize that both direct and vicarious RREs will be associated with sleep quality. In secondary analyses, we examine whether less violent and more violent direct RREs are associated with sleep quality and whether vicarious RREs witnessed in person, as well as those observed via social media are associated with sleep quality. Moreover, because anecdotal reports of RREs affecting sleep often include various forms of negative affect associated with experiences of racism (David K. Li, 2021; Roth, 2020), particularly depression and intrusive, negative thoughts about the event in the form of rumination – which have both been found to contribute to sleep disturbances (Lewis and McKinnon, 2019; Riemann et al., 2001; Tousignant et al., 2019) – in exploratory analyses, we examine the extent to which these factors attenuate associations between RREs and sleep quality.
2. Methods
2.1. Study participants
Participants in the current analysis are from the Mechanisms Underlying the impact of Stress and Emotions on African-American Women’s Health Study (MUSE). The goal of the MUSE study was to investigate the extent to which psychosocial stressors (e.g., expectations of stress) influence cardiovascular disease risk. The present study used baseline data from this cohort, collected from December 2016 to March 2019. All study procedures were approved by the Emory University Institutional Review Board, and all participants provided written informed consent.
Consumer residential and voter registration lists were utilized to identify potential African-American women representing a wide range of socioeconomic backgrounds in the Atlanta, Georgia metropolitan area. Inclusion criteria were self-identifying as an African-American woman, being between 30 and 45 years old at the time of screening (one participant turned 46 by enrollment), and premenopausal with at least one ovary. Exclusion criteria included a history of clinical cardiovascular disease, being pregnant or lactating, any chronic illness known to influence atherosclerosis (e.g., HIV/AIDS, autoimmune or chronic inflammatory diseases such as lupus/rheumatoid arthritis, renal disease, liver disease), current treatment for psychiatric disorders, current illicit drug use (i.e., marijuana, cocaine), or alcohol abuse. Women who reported working overnight shifts were also excluded because of the known impact of shift-work on several markers of cardiovascular risk, primary outcomes in the study.
Based on these inclusion and exclusion criteria, 831 individuals were eligible to participate in the study. Study staff contacted eligible participants and scheduled an in-person visit. A total of 422 eligible respondents completed the in-person interview. For participants missing variables of interest in this study, we imputed the mean score of completed scale items for participants with at least 80% of the scale complete; participants missing more than 20% of scale items were not given a score. For our primary analyses examining associations between direct and vicarious RREs, we excluded participants missing the global sleep quality score (N = 6), direct or vicarious RRE scores (N = 2), and covariates of interest (N = 6), for an analytic sample of 408 participants for our primary analyses. For our secondary analyses examining associations between direct RREs that are less and more violent, separately, and poor sleep, we used the same analytic sample used in our primary analyses as there were no further exclusions. However, for our secondary analyses examining associations between vicarious RREs witnessed in person or via social media and poor sleep, we further excluded from our primary analytic sample those missing scores for vicarious RREs witnessed in person and via social media (N = 17) for an analytic sample of 391 participants. Exploratory analyses examining attenuating effects of depression and rumination for our primary exposures (direct and vicarious RREs) and our secondary exposures (less violent direct RREs and more violent direct RREs, and vicarious RREs witnessed in person and via social media) excluded those missing depression (N = 2) and rumination scores (N = 35), for an analytic sample of 373 participants when examining our primary exposures or less and more violent direct RREs, and 357 participants when examining our other secondary exposures. The 35 women missing data on both depressive symptoms and rumination differed from women with complete data for our primary analyses in that they were more likely to have a college degree, be married or living with a partner, and earn a higher income, and also experienced better sleep. All interviews were conducted in English by interviewers who identified as African-American women.
2.2. Measures
2.2.1. Outcome: sleep quality
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a 19-item questionnaire that measures components of sleep quality over the preceding month (Buysse et al., 1989). As sleep quality is a complex construct that includes both quantitative and subjective aspects of sleep, PSQI examines seven components of sleep, such as subjective sleep quality, sleep duration, and sleep disturbances. A global sleep quality score is the sum of sleep component scores ranging from 0 to 21. Scores greater than 5 on the PSQI indicate overall poor sleep quality (Buysse et al., 1989). The PSQI has been widely used across study populations with evidence of good validity and high test-retest reliability (Backhaus et al., 2002). The PSQI demonstrated adequate internal consistency in this sample (Cronbach’s α = 0.71).
2.2.2. Exposure: direct and vicarious racism
We assessed exposure to direct and vicarious experiences of RREs using a modified version of the Race-Related Events Scale (RES) (Waelde et al., 2010). This RES is a 22-item scale that assesses lifetime exposure to both direct and vicarious experiences of racism. Sixteen (16) items assess direct experiences of racism, including 8 items assessing less violent experiences of direct racism (e.g., “Treated rudely or coldly because of my race or ethnicity; ” “Treated unfairly by a teacher or boss because of my race or ethnicity; ” “Told to leave a place and not come back because of my race or ethnicity”) and 8 items assessing more violent experiences of direct racism (e.g., “Someone chased me because of my race or ethnicity; ” “Someone beat me or hurt me because of my race or ethnicity; ” “Threatened with a knife, gun or other weapon because of my race or ethnicity”), and 6 items assessing mainly more violent experiences of vicarious racism (e.g., “Someone hurt my family member because of his/her race or ethnicity; ” “Saw someone [who is the same race or ethnicity as me]: … “seriously injured; ” “get killed …” “because of their race or ethnicity”). Participants endorsed whether or not they experienced each direct and vicarious event (Yes/No), for a total RRE score ranging from 0 to 22, a direct racism score ranging from 0 to 16 and a vicarious racism score ranging from 0 to 6. In secondary analyses, scores for less violent direct experiences of racism, as well as more violent direct experiences of racism, ranged from 0 to 8. The RES has demonstrated validity, good internal consistency and high test-retest reliability in other samples (Waelde et al., 2010), as well as good internal consistency in this sample (α = 0.87).
Four vicarious racism items asked about witnessing a racist event: “Saw someone [who is the same race or ethnicity as me]: …”get treated in a racist or prejudiced way; ” “almost get seriously injured or killed; ” “seriously injured; ” “get killed …” “because of their race or ethnicity.” To further explore vicarious racism, we modified the original RES to assess whether these witnessed events were witnessed in person (“Is this something you saw happen in real life?”) or via social media (“Is this something you saw happen to a real person on TV, social media, or the internet?”). Participants endorsed whether they witnessed each event in person or via social media (Yes/No), for a summed score for vicarious events witnessed in person ranging from 0 to 4, and vicarious events witnessed via social media ranging from 0 to 4.
2.2.3. Other covariates
Severity of depression symptoms was self-reported using the Beck Depression Inventory (BDI), a 21-item, validated inventory widely used across populations (Beck et al., 1961). As is standard in studies of stress/discrimination and sleep, we excluded the single item on the BDI related to sleep (Lewis et al., 2013), so possible scores on this 20-item modified BDI ranged from 0 to 60. The BDI demonstrated excellent internal consistency in this sample (α = 0.90).
Stress reactive rumination, or repetitive, passive, negative thoughts about stressful events, was measured using the 9-item version of the Stress Reactive Rumination Scale (SRRS) (Connolly and Alloy, 2017). This scale aims to capture the extent to which participants focus on negative attributions and inferences (i.e., “Think about the causes of the stressor”). Participants rate their degree of focus from 0% (no focus on this at all) to 100% (focus on this to a great extent). Responses were summed and divided by nine, total scores ranging from 0 to 100. This scale has demonstrated good validity, internal consistency, and test-retest reliability in other samples(Robinson and Alloy, 2003), and excellent internal consistency in this sample (α = 0.93).
Demographic information included self-reported age, educational attainment, income, employment status and partner status. Educational attainment was assessed as years of education and categorized in analyses as high school or less, some college, and college or more. Household income was assessed with the following categories: <$35K, $35-<$50K, $50-<$75K, ≥$75K. Employment status was categorized as full-time, part-time, or unemployed, and partner status dichotomized as married/living with a partner or not. Additional covariates included health-relevant factors known to impact sleep, including body mass index (BMI) calculated as measured weight divided by the square of measured height (kg/m2), and current smoking status (dichotomized: current smoker or not).
2.3. Statistical analyses
We calculated descriptive statistics to characterize the sample. To examine our main outcome of interest, global sleep quality score, we first depicted unadjusted associations between direct and vicarious RREs and poor sleep with graphs comparing the average global sleep quality score across tertiles of total RRE scores (the sum of direct and vicarious), direct RRE scores and vicarious RRE scores. We also created these graphs of average global sleep quality scores across tertiles of scores for less and more violent direct RREs and vicarious RREs witnessed in person and via social media.
We fit linear regression models to further examine the relationships between exposure to direct and vicarious RREs (continuous scores), together and separately, and continuous global sleep quality score. Model 1 was unadjusted. Further models were adjusted for sociodemographic factors including age, educational attainment, income, employment status, and partner status (Model 2), and health-relevant factors that affect sleep including BMI and current smoking status (Model 3).
Secondary analyses were conducted further examining associations for direct RREs by separately examining direct RREs that were less violent and those that were more violent, as well as further examining associations for mainly violent vicarious RREs by separately examining vicarious RREs that were witnessed in person and those witnessed via social media. Moreover, as depression and rumination are psychological risk factors for poor sleep that are potential downstream mediators of the relationship between RREs and sleep, in further exploratory analyses we sought to examine the extent to which adjusting for depression and rumination attenuated the effects of RREs on sleep quality. Therefore, we adjust for depression symptom severity (Model 4), stress reactive rumination (Model 5), and both factors together (Model 6) in additional analyses and calculate the percent attenuation of the association coefficient in Model 3 after adjustment in Models 4–6 (e.g., ). We also fit logistic regression models (Models 1–6) in order to examine these relationships between RREs and the global sleep quality score modeled as a dichotomous outcome (poor sleep quality is global score >5 and the comparison group is ≤ 5) in supplemental analyses. All statistical analyses were conducted using SAS version 9.4.
3. Results
3.1. Participant characteristics
Table 1 shows descriptive statistics of the sample, though descriptive statistics for exposures and outcomes are not shown. Sample participants endorsed on average approximately 7 out of the 22 total RREs (direct and vicarious). Though there were fewer vicarious events included in the RES, participants on average experienced a greater proportion of vicarious RREs compared to direct RREs – approximately 4 of the 16 direct events (~25%) and 3 out of the 6 vicarious events (~50%). On average, participants experienced less violent direct events (mean = 3.3, SD = 2.4) more often than more violent direct events (mean = 0.4, SD = 1.1), about 84% (N = 344) of the sample experiencing at least 1 less violent direct RRE and 19% of the sample (N = 77) experiencing at least 1 more violent direct RRE. Participants reported witnessing more vicarious RREs via social media (approximately 2 out of 4) compared to in person (approximately 1 out of 4).
Table 1.
Descriptive characteristics of analytic sample (N = 408) in the Mechanisms Underlying the impact of Stress and Emotions (MUSE) on African-American Women’s Health study, 2016–2019.
| Age, years, mean (SD) | 38.0 (4.3) |
|---|---|
| Educational attainment, N (%) | |
| High School or Less | 128 (31) |
| Some College | 86 (21) |
| College or Higher | 194 (48) |
| Married/Partnered, N (%) | 150 (37) |
| Employment Status, N (%) | |
| Unemployed | 56 (14) |
| Part-time | 79 (19) |
| Full-time | 264 (65) |
| Income, N (%) | |
| <$35K | 100 (25) |
| $35 – <$50K | 85 (21) |
| $50 – <$75K | 91 (22) |
| ≥$75K | 125 (31) |
| Current Smoker, N (%) | 39 (10) |
| Body Mass Index, mean (SD) | 32.8 (8.4) |
| Beck Depression Inventory (missing sleep), mean (SD) | 5.4 (6.6) |
| Stress Reactive Rumination Scale (average), mean (SD) | 51.1 (24.9) |
The average global sleep quality score as measured via the PSQI was 6.7 (SD = 3.6; possible range = 0–21). The majority of participants (57%) had PSQI scores greater than 5, a common cutoff used to determine overall poor sleep quality (Buysse et al., 1989). Participants had an average BDI score of 5.4 (SD = 6.6; possible range = 0–60), and an average SRRS score of 51.1 (SD = 24.9; possible range = 0–100).
There were weak to moderate correlations between covariates adjusted for in primary analyses (age, educational attainment, employment status, income, partner status, BMI, current smoking status) and RRE and global sleep quality scores. We include a table of variable correlations in the Supplement (Supplementary Table 1).
3.2. Primary analyses
Fig. 1 depicts unadjusted levels of average global sleep score separately across tertiles of total, direct, and vicarious RREs. As total RRE score increased, the average global sleep quality score was greater, denoting worse sleep. As direct RRE score increased, there was an even more pronounced greater average global sleep quality score compared to the total RRE score. On the other hand, this positive trend was not observed for vicarious RRE score and average global sleep quality score. Fig. 2 depicts unadjusted levels of average global sleep score across tertiles of direct RREs that were less violent (Panel A) and those that were more violent (Panel B), as well as vicarious RREs witnessed separately in person (Panel C) and via social media (Panel D). Whether less or more violent, as the direct RRE score increased, the average global sleep quality score was greater, though this association was more pronounced with more violent direct RREs. There was a notably higher global PSQI score as vicarious RREs witnessed in person score increased; however, this trend was not observed for vicarious events witnessed via social media.
Fig. 1.
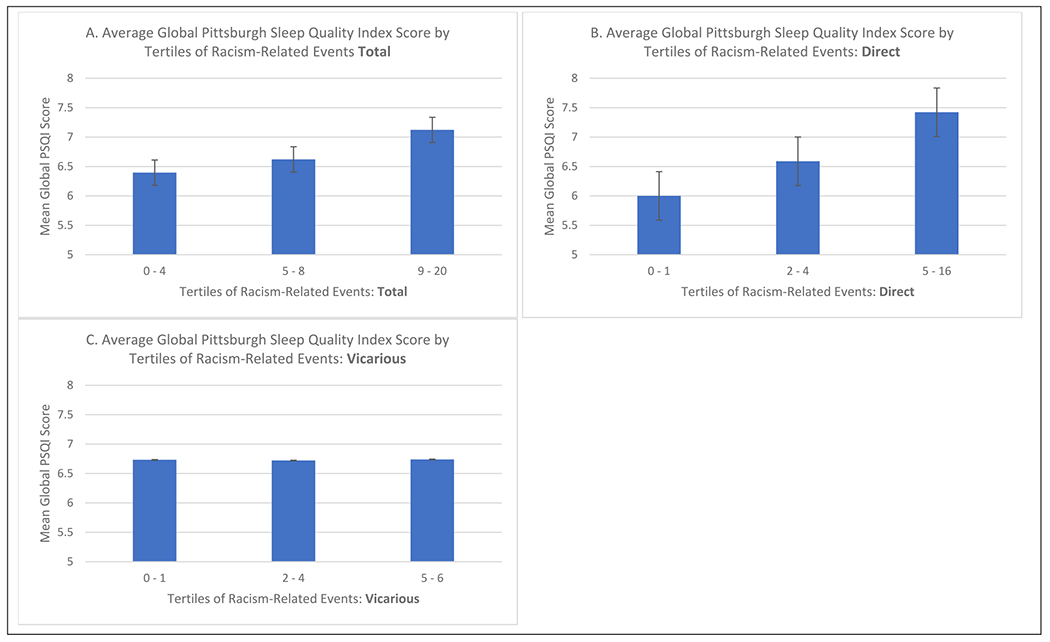
Mean global Pittsburgh sleep quality index score by tertiles of total (panel A), direct (panel B), and vicarious (panel C) racism-related events.
Fig. 2.
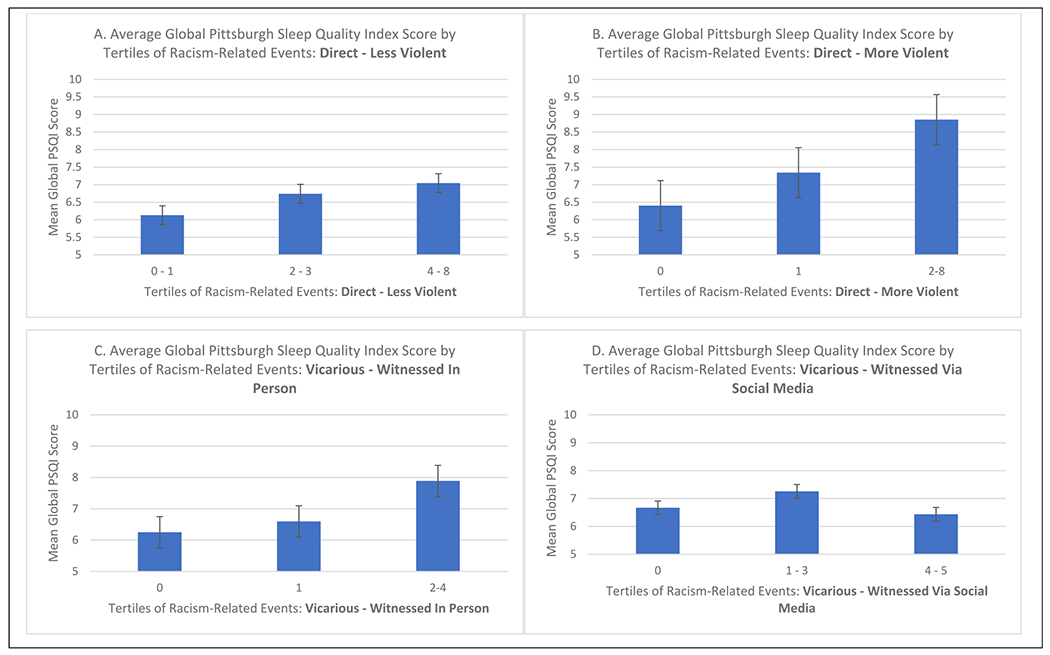
Mean global Pittsburgh sleep quality index score by tertiles of less violent (panel A) and more violent (panel B) direct racism-related events and vicarious racism-related events witnessed in person (panel C) and witnessed via social media (panel D).
Table 2 shows results from unadjusted and adjusted multivariable linear regression models examining associations between continuous RRE scores (total, direct and vicarious) and the continuous global sleep quality score. In Model 1 (unadjusted), total RREs (the sum of direct and vicarious; first column) were associated with global sleep quality score. As the number of RREs endorsed increased, the global PSQI score was greater by approximately 0.12 points (95% CI: 0.04, 0.20). Each additional direct RRE (second column) was associated with a 0.24 (95% CI: 0.13, 0.35) point greater global sleep quality score in the unadjusted model. On the other hand, vicarious RREs (third column) were not associated with global sleep quality score (β = 0.04; 95% CI: 0.14, 0.21). Associations adjusted for sociodemographics (Model 2) as well as risk factors for poor sleep (Model 3) were comparable to unadjusted models.
Table 2.
Adjusted Association between Direct and Vicarious Racism-Related Events (per 1-Point Score Increment) and Global Sleep Quality Index Score in the Mechanisms Underlying the impact of Stress and Emotions (MUSE) study, 2016–2019.
| Model | Racism-Related Events: Total (Direct + Vicarious; N = 408) | Racism-Related Events: Direct (N = 408) | Racism-Related Events: Vicarious (N = 408) |
|---|---|---|---|
|
|
|
|
|
| Model 1. Unadjusted | 0.12 (0.04, 0.20)* | 0.24 (0.13, 0.35)* | 0.04 (−0.14, 0.21) |
| Model 2. Adjusted for sociodemographic factorsa | 0.14 (0.06, 0.22)* | 0.26 (0.14, 0.37)* | 0.07 (−0.10, 0.2) |
| Model 3. Model 2 + risk factors for poor sleepb | 0.14 (0.06, 0.22)* | 0.26 (0.15, 0.36)* | 0.09 (−0.08, 0.26) |
| Exploratory Analyses (Attenuation by Potential Mediators) | |||
| Model 4. Model 3 + symptoms of depression severityc | 0.11 (0.04, 0.19)* | 0.19 (0.08, 0.30)* | 0.10 (−0.07, 0.27) |
| Model 5. Model 3 + stress reactive ruminationd | 0.12 (0.04, 0.20)* | 0.21 (0.10, 0.33)* | 0.10 (−0.07, 0.28) |
| Model 6. Model 4 + stress reactive ruminationd | 0.10 (0.02, 0.18)* | 0.17 (0.06, 0.29)* | 0.09 (−0.08, 0.25) |
p-value <0.05.
Age, educational attainment, employment status, income, and partner status.
BMI and smoking status.
Beck Depression Inventory score.
Stress Reactive Rumination Scale.
3.3. Secondary analyses
Table 3 shows results for secondary analyses examining types of direct RREs (less violent and more violent), as well as types of vicarious RREs (witnessed in person and witnessed via social media). In unadjusted analyses, each additional direct RRE that was less violent (first column) was associated with a 0.25 point (95% CI: 0.11, 0.40) greater global sleep quality score in the unadjusted model, while each additional direct RRE that was more violent (second column) was associated with a 0.59 point (95% CI: 0.30, 0.89) greater global sleep quality score. Witnessing vicarious events in person (third column) was associated with a 0.52 point (95% CI: 0.21, 0.83) greater global sleep quality score, while witnessing vicarious events via social media (fourth column) was not associated with global sleep quality score (β = −0.07; 95% CI: 0.29, 0.14). Associations adjusted for sociodemographics and risk factors for poor sleep were comparable to unadjusted models.
Table 3.
Adjusted Association between Subtypes of Direct (More Versus Less Violent) and Subtypes of Vicarious (In Person Versus Social Media) Racism-Related Events (per 1-Point Score Increment) and Global Sleep Quality Index Score in the Mechanisms Underlying the impact of Stress and Emotions (MUSE) study, 2016–2019.
| Model | Types of Direct Racism |
Types of Vicarious Racism |
||
|---|---|---|---|---|
| N = 408 |
N = 408 |
N = 391 |
N = 391 |
|
| Racism-Related Events: Direct – Less Violent | Racism-Related Events: Direct – More Violent | Racism-Related Events: Vicarious – Witnessed In Person | Racism-Related Events: Vicarious - Witnessed Via Social Media | |
| Model 1. Unadjusted | 0.25 (0.11, 0.40)* | 0.59 (0.30, 0.89)* | 0.52 (0.21, 0.83)* | −0.07 (−0.29, 0.14) |
| Model 2. Adjusted for sociodemographic Factorsa | 0.29 (0.15, 0.44)* | 0.56 (0.27, 0.86)* | 0.49 (0.18, 0.80)* | −0.03 (−0.24, 0.18) |
| Model 3. Model 2 + risk factors for poor sleepb | 0.29 (0.15, 0.44)* | 0.55 (0.26, 0.84)* | 0.50 (0.19, 0.81)* | 0.003 (−0.21, 0.21) |
| Exploratory Analyses (Attenuation by Potential Mediators) | ||||
| Model 4. Model 3 + symptoms of depression severityc | 0.20 (0.06, 0.35)* | 0.44 (0.16, 0.72)* | 0.42 (0.11, 0.72)* | 0.04 (−0.17, 0.24) |
| Model 5. Model 3 + stress reactive ruminationd | 0.24 (0.09, 0.39)* | 0.47 (0.17, 0.76)* | 0.44 (0.13, 0.76)* | 0.03 (−0.19, 0.24) |
| Model 6. Model 4 + stress reactive ruminationd | 0.18 (0.04, 0.33)* | 0.42 (0.13, 0.70)* | 0.40 (0.09, 0.70)* | 0.03 (−0.18, 0.23) |
p-value < 0.05.
Age, educational attainment, employment status, income, and partner status.
BMI and smoking status.
Beck Depression Inventory score.
Stress Reactive Rumination Scale.
3.4. Exploratory analyses
In our examination of associations between RREs and the global sleep quality score, in further exploratory analyses we adjust for depression symptom severity and stress reactive rumination in Models 4–6, also included in Tables 2 and 3 Compared to models adjusted for sociodemographics and risk factors for poor sleep (Model 3), adjusting for depression symptom severity in Model 4 attenuated the coefficient for positive associations found for total, direct (less and more violent combined), less violent direct, more violent direct, and vicarious RREs witnessed in person by 21%, 27%, 31%, 20%, and 16%, respectively, while adjusting for stress reactive rumination in Model 5 attenuated these associations by 14%, 19%, 17%, 54%, and 12%. Adjusting for depression symptom severity and stress reactive rumination together in Model 6 attenuated these associations for total, direct and vicarious RREs witnessed in person by 29%, 35%, 38%, 24%, and 20%, respectively. Associations between vicarious RREs (Table 2) and vicarious RREs witnessed via social media (Table 3) with global sleep quality scores were near null, and adjusting for depression symptom severity and/or stress reactive rumination did not attenuate these associations.
3.5. Supplemental analyses
Tables for analyses examining associations between RREs and the global sleep quality score modeled as a dichotomous outcome (poor sleep quality is global score >5 and the comparison group is ≤ 5) are included in the Supplement (Supplementary Tables 2 and 3). Patterns of associations matched those observed for the continuous sleep score, though total RREs were not associated with the odds of having poor sleep quality (OR = 1.03; 95% CI: 0.99, 1.08). In Model 1 (unadjusted), the odds of having poor sleep was higher by 10% (OR = 1.10; 95% CI: 1.03, 1.18) for each additional direct RRE, by 14% for each additional direct RRE that was less violent (OR = 1.14; 95% CI: 1.02, 1.21), by 26% for each additional direct RRE that was more violent (OR = 1.26; 95% CI: 1.02, 1.55), and by 28% (OR = 1.28; 95% CI: 1.06, 1.55) for each additional vicarious RRE witnessed in person. Vicarious RREs overall and those witnessed via social media were again not associated with higher odds of having poor sleep quality. Compared to models adjusted for sociodemographics and risk factors for poor sleep (Model 3), adjusting for depression symptom severity in Model 4 attenuated associations for direct (overall), less violent direct, more violent direct, and vicarious RREs witnessed in person by 27%, 38%, 33%, and 22%, respectively, and adjusting for stress reactive rumination in Model 5 attenuated associations by 27%, 38%, 29%, and 26%, while adjusting for both factors in Model 6 attenuated these associations by 45%, 54%, 48%, and 30%.
4. Discussion
In this cohort of African-American women in the southeast US, we sought to examine associations between racist events and poor sleep, moving beyond examination of direct, fairly non-extreme experiences of racism alone to include vicarious experiences of racism as well as more extreme and violent direct and vicarious experiences. In accordance with prevailing hypotheses, we found total experiences of racism were associated with worse overall global sleep quality; and, this was driven by strong associations between direct experiences of racism and worse global sleep quality. Contrary to our hypotheses, we did not find associations between overall vicarious experiences of racism and poor sleep. These results were found in analyses modeling global sleep quality both continuously and dichotomously using scores greater than 5 as a standard cutoff for overall poor sleep (compared to scores ≤5).
Another innovative aspect of this study was using a measure of racism that included the everyday, less violent experiences of racism often used in studies, as well as more extreme, violent experiences of racism. As measures of direct RREs included a number of less and more violent events, in secondary analyses we separately examined less violent and more violent direct RREs. Aligned with our hypotheses, we found both less and more violent direct RREs were associated with poor sleep quality, though stronger associations were found for more violent direct RREs. We also explored mainly violent vicarious RREs more closely in secondary analyses, and despite null associations between vicarious RREs overall and poor sleep quality, we found large, positive associations between vicarious RREs witnessed in person and global sleep quality score, with effect sizes twice as large as those for direct RREs overall, and similar to effect sizes observed for more violent direct RREs. No associations were observed for vicarious RREs witnessed via social media.
To our knowledge, no other study has examined how both direct and vicarious forms of racism influence African-American women’s sleep quality. In a 2019 review of the discrimination and sleep literature, Lewis and McKinnon (2019) explicitly noted the dearth of studies examining vicarious racism and poor sleep, finding only two studies (Thomas et al., 2006; Tomfohr et al., 2012) using a validated scale measuring vicarious exposure to racism. Unlike our study, both studies found associations between vicarious racism and objective measures of poor sleep. Both studies used the Perceived Discrimination subscale of the Scale of Ethnic Experiences, a 9-item scale that includes two items assessing direct exposure to discrimination (“In my life I have experienced prejudice because of my ethnicity” and “I have not felt discriminated against in American society because of my ethnic background”) and seven items assessing perceptions of how one’s ethnic group has been treated in the US (i.e., “My ethnic group has been treated well in American society” and “My ethnic group does not have the same opportunities as other ethnic groups”) (Malcarne et al., 2006). In cohorts of African-American and White Americans, these studies found ethnic discrimination was a mediator of ethnic differences in polysomnography-assessed sleep architecture, such that those reporting more ethnic discrimination experienced less deep, slow wave sleep and more light, Stage 2 sleep, as well as more physical fatigue (Thomas et al., 2006; Tomfohr et al., 2012). However, the Perceived Discrimination subscale of the Scale of Ethnic Experiences does not include items on conceptual aspects of vicarious discrimination that we include in this study. For example, the RES includes items that assess hearing about and witnessing specific racist events experienced by family or others, rather than asking about perceptions of the existence of discrimination towards one’s racial group overall as is assessed in the Perceived Discrimination subscale. Also, the Perceived Discrimination subscale includes items assessing direct as well as vicarious experiences of racism without disentangling the separate effects of these forms of racism (Malcarne et al., 2006).
While limited, studies examining other health outcomes also provide evidence for the negative health consequences of vicarious exposure to racism-related stress, including vicarious effects of parental exposure to racism on child health (Heard-Garris et al., 2018), vicarious effects of police killings of unarmed African-American Americans and other highly publicized anti-African-American violence on the mental health of African-American adults in the general population (Bor et al., 2018; Curtis et al., 2021), and vicarious effects of racism on disease activity among African-American women with lupus (Martz et al., 2019). In contrast, in our study we found that overall vicarious racism – measured as hearing about or witnessing family or someone (who is the same race or ethnicity as me) getting treated in a prejudiced way, almost get seriously injured or killed, or get seriously injured or killed because of their race or ethnicity – was not associated with poor sleep quality. However, witnessing these events in person was associated with worse global sleep quality, while witnessing events via social media was not. Qualitative studies exist that describe exposure to witnessing violent acts related to racism via social media and effects on mental and emotional health, particularly among adolescents who tend to be the biggest consumers of social media; however, we have yet to find quantitative, empirical studies examining the effects of vicarious racism specific to social media on any health outcomes. Though adolescents have high rates of social media usage, adults between 30 and 49 years old, the approximate age range of this cohort, have similar usage rates (Sheet, 2018). Therefore, while we might expect based on qualitative literature that exposure to vicarious racism via social media would have effects on health that might include sleep, our quantitative analysis suggests otherwise.
In keeping with our emphasis on extreme RREs, our findings are slightly stronger than those observed in prior studies. For example, a study by Francis et al. (2017) measuring direct exposure to racism using the Everyday Discrimination Scale, which includes day-to-day, fairly non-violent racism-related events, found experiences of direct racism to be associated with a 0.05 increase in global sleep quality score as measured via PSQI among pregnant African-American women (Francis et al., 2017). We found stronger effect sizes using our measure of direct racism (0.12 increase in global sleep quality score), likely due to inclusion of more extreme, violent events in the RES. When we separated less violent from more violent direct RREs in secondary analyses, while both forms of direct racism were associated with poor sleep, more violent direct events had stronger effects on worse sleep. Effect sizes for more violent direct RREs on poor sleep were similar to those found for vicarious RREs witnessed in person. Similarities in effect sizes between more violent direct RREs and vicarious RREs witnessed in person is likely attributable to the fact that the vicarious RREs included in the measure were mainly violent events (e.g., seeing people hurt, injured or killed).
Violent images of racism are often prevalent on television and social media – racism-related violence against African-Americans in America often being retold via media (i.e., slavery, lynchings, killings of unarmed African-American people), eliciting studies demonstrating the effects of exposure to high-profile racist events, particularly on mental health outcomes (Curtis et al., 2021). However, as evidenced in this study, witnessing violent events in person may be comparatively more traumatic and cause distress, sense of threat, and psychological and physiological arousal that is more severe than witnessing these events on a screen, and perhaps is experientially closer to having a direct experience. This kind of in-person proximity to violence is often studied when examining trauma in research, including sleep research that includes mechanistic models of trauma-induced insomnia (Sinha, 2016). Additionally, it may be that RREs witnessed in person are more likely to be experienced by someone much closer to the person reporting the vicarious experience, or perhaps happen closer to one’s neighborhood and home. If RREs are happening to those in one’s social network or in spaces one occupies, that may elicit a stronger psychological and physiological response than RREs happening to strangers far away from home, as is more likely with RREs witnessed via social media.
Additional exploratory analyses examined hypotheses that depression and rumination would attenuate effects of discrimination on poor sleep, as these factors have been identified as potential downstream mediators between discrimination and poor sleep. While we were unable to conduct formal mediation analyses in this cross-sectional study, we found that depression symptom severity and stress reactive rumination and depression symptom severity attenuated associations found between direct and vicarious RREs witnessed in person and poor sleep. Previous studies have provided evidence that negative affect resulting from experiences of racism can contribute to sleep disturbances and autonomic arousal, resulting in poor sleep (Lewis and McKinnon, 2019). For example, prospective studies show experiences of discrimination result in the development and exacerbation of depressive symptoms (Saelee et al., 2019), and more than 90% of patients with depression report impaired sleep quality, with polysomnographic studies showing depression linked to more disturbances of sleep continuity and reduction of deep, slow wave sleep (Riemann et al., 2001). Sleep disturbances are also a core symptom of depression. Several theoretical models having been developed to explain this link, making depression an important psychological risk factor to consider in an examination of discrimination and poor sleep (Lewis et al., 2015; Riemann et al., 2001). Moreover, people who experience RREs can also experience intrusive, negative thoughts about the event in the form of rumination, exacerbating the stress process by prolonging psychological and physiological responses to racism-related stressors; this theory is known as the perseverative cognition hypothesis (Brosschot et al., 2006). There is strong evidence for negative effects of rumination on sleep outcomes, and studies have found rumination mediates relationships between stressors and sleep outcomes (Hoggard and Hill, 2018; Tousignant et al., 2019). Again, these studies exploring and demonstrating the mediating effects of depression and rumination on poor sleep have focused on direct, less extreme forms of racism, and this is the first study to our knowledge to examine and demonstrate the attenuating effects of these factors on associations between vicarious racism (more specifically those events witnessed in person) and more extreme, violent experiences of racism and poor sleep.
While both depression and rumination attenuated associations between RREs and poor sleep both separately and more so together, part of the effect of direct RREs and vicarious RREs witnessed in person persisted after adjustment for depression and rumination. This suggests that other mechanisms may be at play and should be explored to highlight or potentially intervene in how experiences of racism contribute to poor sleep. Future studies should continue to explore relatively understudied mechanisms relating discrimination to poor sleep among African-American women that may be particularly relevant for more violent experiences of racism, including further elucidating factors related to autonomic arousal, such as vigilance (Hicken et al., 2013; Lewis and McKinnon, 2019).
Overall, in this study, patterns of associations between RREs and poor sleep were consistent whether measuring sleep continuously or dichotomously using a threshold to define poor sleep (poor sleep is continuous global sleep quality score >5 and the comparison group is ≤5). However, while similar patterns of attenuation by depression and/or rumination were found when sleep was measured continuously or dichotomously, attenuations were stronger for the dichotomous sleep outcome, resulting in the lower end of the confidence interval for direct and vicarious RRE associations with the dichotomous sleep outcome to be at or below the null. These results may suggest that the attenuations we witnessed for associations between RREs and the continuous global sleep quality score after adjusting for depression and rumination were enough to lower risk for reaching the threshold for poor sleep. Additionally, depression and rumination may be important factors on the pathway between racism and poor sleep quality as indicated by the cut point for poor sleep, but to a lesser degree explain poor sleep severity beyond this threshold. However, these results may also reflect a loss of statistical power after categorizing our continuous measure. Future studies should conduct formal mediation analyses with larger samples to further shed light on mechanisms through which discrimination affects sleep among African-American women, including associations with risk for reaching poor sleep thresholds.
4.1. Limitations
There are important limitations of this study that should be noted. Sleep is a self-reported measure in this study, and objective measures are considered the gold standard for measuring sleep. However, PSQI is a widely-used, validated self-report measure of sleep and provides unique participant-centered aspects of sleep (Buysse, 2014). Also, while we examine forms of direct and vicarious racism, a novel aspect of this study, the subscales and modified RES measures used to capture this information have yet to be validated. Furthermore, the cross-sectional nature of these data does not allow us to make assumptions on temporality or causality in the associations between RREs and poor sleep. However, the RES measures whether discrimination has ever occurred whereas the PSQI measures sleep quality in the past month, so it is likely that experiences of discrimination reported in the RES preceded sleep quality reported in the PSQI. Other studies have found associations between racism and sleep using measures that assess discrimination ever in one’s life as well as more proximal to the timing of poor sleep, and in this study, we find that ever having experiences of discrimination is associated with poor sleep. These results would suggest the effects of discrimination on sleep are not time-dependent, or that experiences of discrimination can have long-term effects on sleep, perhaps through persistent effects of discrimination on depression and rumination. However, future studies should continue to explore the potential for the effects of discrimination on sleep to be moderated by timing of discriminatory events. Additionally, results of this study may not be generalizable to all African-American women as nearly half of participants in the study are college educated and two-thirds are employed full-time (higher than national rates), and all are from the Atlanta metropolitan area. However, previous studies have demonstrated that higher socioeconomic status (SES) African-American women report more discrimination than lower SES African-American women (Lewis and Van Dyke, 2018), and experience worse sleep than lower SES African-American women (Petrov et al., 2020) – disparities in sleep between African-Americans and Whites are greatest among those who hold professional occupations with more responsibilities (Jackson et al., 2013). Therefore, higher SES is neither protective against poor sleep nor experiences of discrimination, making this sample that includes many highly educated African-American women appropriate for examining our associations of interest. Also, participants were excluded if they had a history of major cardiovascular disease events and chronic conditions, which may affect generalizability of these findings to other populations without these restrictions; however, the specific conditions that we excluded (heart attack, stroke, etc.) are uncommon among Black women under the age of 45 (Virani et al., 2021), and we did not exclude other more common conditions in this age group (i.e., hypertension, obesity, diabetes) (Vatsa et al., 2021). Shift workers were also excluded because of the known impact of shift-work on several markers of cardiovascular risk, a primary outcome in the MUSE study, however shift-workers may also have more disrupted sleep than those who are not shift workers, so there was potentially selection bias into the study related to our outcome as selection into the study may have differed by sleep quality. Moreover, the 35 women excluded from our exploratory analyses with rumination and depressive symptoms actually had better sleep than included women. Thus, our observed associations in those analyses may be biased away from the null, with attenuations weaker if these participants were included.
5. Conclusions
In conclusion, in this cohort of African-American women in the southeast US, direct experiences of racism, particularly those that were more violent, were associated with poor sleep, while mainly violent vicarious experiences were not – unless witnessed in person. This study sheds light on aspects of racism and health that are relatively under-studied in this literature – the effects of vicarious forms (witnessed in person or via social media) of racism and particularly violent exposures to racism – providing a fuller understanding of how racism in its different forms in society may affect sleep health. This study also implies that some forms of racism, including direct experiences and witnessing experiences among same race others in person, in particular may require intervention to buffer the effects of these exposures; perhaps through addressing depression and rumination which may explain part of the effects of these exposures on sleep.
Supplementary Material
Funding
The author would like to acknowledge the following grants funding this work: T32 HL130025; R01 HL130471; K24 163696; R01 158141.
Footnotes
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.socscimed.2022.115269.
Data availability
Data will be made available on request.
References
- Allam H, 2020. FBI report: bias-Motivated killings at Record high amid Nationwide Rise in hate crime. NPR: NPR. https://www.wbur.org/npr/935439777/fbi-report-bias-motivated-killings-at-record-high-amid-nationwide-rise-in-hate-c. [Google Scholar]
- Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F, 2002. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res 53, 737–740. [DOI] [PubMed] [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J, 1961. An inventory for measuring depression. Arch Gen Psychiatry 4, 561–571. [DOI] [PubMed] [Google Scholar]
- Bor J, Venkataramani AS, Williams DR, Tsai AC, 2018. Police killings and their spillover effects on the mental health of black Americans: a population-based, quasi-experimental study. Lancet 392, 302–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brosschot JF, Gerin W, Thayer JF, 2006. The perseverative cognition hypothesis: a review of worry, prolonged stress-related physiological activation, and health. J. Psychosom. Res 60, 113–124. [DOI] [PubMed] [Google Scholar]
- Burgard SA, Ailshire JA, 2013. Gender and time for sleep among US adults. Am. Socio. Rev 78, 51–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buysse DJ, 2014. Sleep health: can we define it? Does it matter? Sleep 37, 9–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ, 1989. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatr. Res 28, 193–213. [DOI] [PubMed] [Google Scholar]
- Carter RT, Mazzula S, Victoria R, Vazquez R, Hall S, Smith S, et al. , 2013. Initial development of the race-based traumatic stress symptom scale: assessing the emotional impact of racism. Psychological Trauma: Theory, Research, Practice, and Policy 5, 1. [Google Scholar]
- Chae DH, Yip T, Martz CD, Chung K, Richeson JA, Hajat A, et al. , 2021. Vicarious Racism and Vigilance during the CoViD-19 Pandemic: Mental Health Implications Among Asian and Black Americans. Public Health Reports, 00333549211018675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connolly SL, Alloy LB, 2017. Rumination interacts with life stress to predict depressive symptoms: an ecological momentary assessment study. Behav. Res. Ther 97, 86–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis DS, Washburn T, Lee H, Smith KR, Kim J, Martz CD, et al. , 2021. Highly public anti-Black violence is associated with poor mental health days for Black Americans. Proc. Natl. Acad. Sci. USA 118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- David K, Li JG, 2021. Tearful Witness Regrets Not Doing More to Possibly Save George Floyd’s Life. NBC News: NBC News. [Google Scholar]
- Dawson MC, 1995. Behind the Mule: Race and Class in African-American Politics. Princeton University Press. [Google Scholar]
- Francis B, Klebanoff M, Oza-Frank R, 2017. Racial discrimination and perinatal sleep quality. Sleep Health 3, 300–305. [DOI] [PubMed] [Google Scholar]
- Gee GC, Walsemann KM, Brondolo E, 2012. A life course perspective on how racism may be related to health inequities. American journal of public health 102, 967–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall MH, Matthews KA, Kravitz HM, Gold EB, Buysse DJ, Bromberger JT, et al. , 2009. Race and financial strain are independent correlates of sleep in midlife women: the SWAN sleep study. Sleep 32, 73–82. [PMC free article] [PubMed] [Google Scholar]
- Harrell SP, 2000. A multidimensional conceptualization of racism-related stress: implications for the well-being of people of color. Am. J. Orthopsychiatry 70, 42–57. [DOI] [PubMed] [Google Scholar]
- Heard-Garris NJ, Cale M, Camaj L, Hamati MC, Dominguez TP, 2018. Transmitting trauma: a systematic review of vicarious racism and child health. Soc. Sci. Med 199, 230–240. [DOI] [PubMed] [Google Scholar]
- Hicken MT, Lee H, Ailshire J, Burgard SA, Williams DR, 2013. Every shut eye, ain’t sleep”: the role of racism-related vigilance in racial/ethnic disparities in sleep difficulty. Race and social problems 5, 100–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoggard LS, Hill LK, 2018. Examining how racial discrimination impacts sleep quality in African Americans: is perseveration the answer? Behav. Sleep Med 16, 471–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson CL, Redline S, Kawachi I, Williams MA, Hu FB, 2013. Racial disparities in short sleep duration by occupation and industry. American journal of epidemiology 178, 1442–1451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson DA, Jackson CL, Williams NJ, Alcántara C, 2019. Are sleep patterns influenced by race/ethnicity–a marker of relative advantage or disadvantage? Evidence to date. Nat. Sci. Sleep 11, 79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson DA, Lisabeth L, Lewis TT, Sims M, Hickson DA, Samdarshi T, et al. , 2016. The contribution of psychosocial stressors to sleep among African Americans in the Jackson Heart Study. Sleep 39, 1411–1419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knutson KL, Rathouz PJ, Yan LL, Liu K, Lauderdale DS, 2006. Stability of the Pittsburgh sleep quality index and the Epworth Sleepiness questionnaires over 1 year in early middle-aged adults: the CARDIA study. Sleep 29, 1503–1506. [DOI] [PubMed] [Google Scholar]
- Lauderdale DS, Knutson KL, Rathouz PJ, Yan LL, Hulley SB, Liu K, 2009. Cross-sectional and longitudinal associations between objectively measured sleep duration and body mass index: the CARDIA Sleep Study. American journal of epidemiology 170, 805–813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis TT, Cogburn CD, Williams DR, 2015. Self-reported experiences of discrimination and health: scientific advances, ongoing controversies, and emerging issues. Annu. Rev. Clin. Psychol 11, 407–440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis TT, McKinnon II, 2019. Exposure to Discrimination and Sleep, vol. 257. The Social Epidemiology of Sleep. [Google Scholar]
- Lewis TT, Troxel WM, Kravitz HM, Bromberger JT, Matthews KA, Hall MH, 2013. Chronic exposure to everyday discrimination and sleep in a multiethnic sample of middle-aged women. Health Psychol. 32, 810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis TT, Van Dyke ME, 2018. Discrimination and the health of African Americans: the potential importance of intersectionalities. Curr. Dir. Psychol. Sci 27, 176–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malcarne VL, Chavira DA, Fernandez S, Liu P-J, 2006. The scale of ethnic experience: development and psychometric properties. J. Pers. Assess 86, 150–161. [DOI] [PubMed] [Google Scholar]
- Martz CD, Allen AM, Fuller-Rowell TE, Spears EC, Lim SS, Drenkard C, et al. , 2019. Vicarious racism stress and disease activity: the Black women’s experiences living with lupus (BeWELL) study. Journal of racial and ethnic health disparities 6, 1044–1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason TB, Maduro RS, Derlega VJ, Hacker DS, Winstead BA, Haywood JE, 2017. Individual differences in the impact of vicarious racism: African American students react to the George Zimmerman trial. Cult. Divers Ethnic Minor. Psychol 23, 174. [DOI] [PubMed] [Google Scholar]
- Maume DJ, Sebastian RA, Bardo AR, 2009. Gender differences in sleep disruption among retail food workers. Am. Socio. Rev 74, 989–1007. [Google Scholar]
- Monk EP Jr., 2020. Linked fate and mental health among African Americans. Soc. Sci. Med 266, 113340. [DOI] [PubMed] [Google Scholar]
- Neblett EW Jr., 2019. Racism and health: Challenges and future directions in behavioral and psychological research. Cult. Divers Ethnic Minor. Psychol 25, 12. [DOI] [PubMed] [Google Scholar]
- Nuru-Jeter A, Dominguez TP, Hammond WP, Leu J, Skaff M, Egerter S, et al. , 2009. It’s the skin you’re in”: African-American women talk about their experiences of racism. An exploratory study to develop measures of racism for birth outcome studies. Matern. Child Health J 13, 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paradies Y, Ben J, Denson N, Elias A, Priest N, Pieterse A, et al. , 2015. Racism as a determinant of health: a systematic review and meta-analysis. PLoS One 10, e0138511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrov ME, Long DL, Grandner MA, MacDonald LA, Cribbet MR, Robbins R, et al. , 2020. Racial differences in sleep duration intersect with sex, socioeconomic status, and US geographic region: the REGARDS study. Sleep Health 6, 442–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pridgett T, 2020. A Public-Health Expert Explains How Racism and White Supremacy Negatively Affect Black People’s Sleep. Popsugar: Popsugar. [Google Scholar]
- Riemann D, Berger M, Voderholzer U, 2001. Sleep and depression—results from psychobiological studies: an overview. Biol. Psychol 57, 67–103. [DOI] [PubMed] [Google Scholar]
- Robinson MS, Alloy LB, 2003. Negative cognitive styles and stress-reactive rumination interact to predict depression: a prospective study. Cognit. Ther. Res 27, 275–291. [Google Scholar]
- Roth A, 2020. ‘She saw me in George Floyd’: The trauma of watching another black person die. MPR News: MPR News. [Google Scholar]
- Saelee R, Vaccarino V, Sullivan S, Hammadah M, Shah A, Wilmot K, et al. , 2019. Longitudinal associations between self-reported experiences of discrimination and depressive symptoms in young women and men post- myocardial infarction. J. Psychosom. Res 124, 109782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheet F, 2018. Social Media Fact Sheet. Pew Research Center. [Google Scholar]
- Simien EM, 2005. Race, gender, and linked fate. J. Black Stud 35, 529–550. [Google Scholar]
- Sinha SS, 2016. Trauma-induced insomnia: a novel model for trauma and sleep research. Sleep Med. Rev 25, 74–83. [DOI] [PubMed] [Google Scholar]
- Slopen N, Lewis TT, Williams DR, 2016. Discrimination and sleep: a systematic review. Sleep Med. 18, 88–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas KS, Bardwell WA, Ancoli-Israel S, Dimsdale JE, 2006. The toll of ethnic discrimination on sleep architecture and fatigue. Health Psychol. 25, 635. [DOI] [PubMed] [Google Scholar]
- Tomfohr L, Pung MA, Edwards KM, Dimsdale JE, 2012. Racial differences in sleep architecture: the role of ethnic discrimination. Biol. Psychol 89, 34–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tousignant OH, Taylor ND, Suvak MK, Fireman GD, 2019. Effects of rumination and worry on sleep. Behav. Ther 50, 558–570. [DOI] [PubMed] [Google Scholar]
- Van Dyke ME, Vaccarino V, Quyyumi AA, Lewis TT, 2016. Socioeconomic status discrimination is associated with poor sleep in African-Americans, but not Whites. Soc. Sci. Med 153, 141–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vatsa N, Thobani A, Buendia L, Murphy K, Asier S, Chen Z, et al. , 2021. Cardiovascular risk factors in Younger black women: results from the 10,000 women Community screening Project. Am. Heart J.: Cardiol. Res. Pract 8, 100037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. , 2021. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation 143, e254–e743. [DOI] [PubMed] [Google Scholar]
- Waelde LC, Pennington D, Mahan C, Mahan R, Kabour M, Marquett R, 2010. Psychometric properties of the race-related events scale. Psychological Trauma: Theory, Research, Practice, and Policy 2, 4. [Google Scholar]
- Yip T, Cheon YM, 2020. Sleep, psychopathology and cultural diversity. Current opinion in psychology 34, 123–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang B, Wing Y-K, 2006. Sex differences in insomnia: a meta-analysis. Sleep 29, 85–93. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data will be made available on request.