

Abstract
We present a case of multifocal cutaneous alternariosis in a 69-year-old man with hairy cell leukemia. The patient presented with painful, violaceous nodules of the lower extremities and left forearm. His physical examination was otherwise normal. Biopsy specimens were submitted first for histopathological examination, followed by microbiological testing. Histopathology showed epidermal hyperplasia, intraepidermal abscess formation, and intracellular and extracellular fungal elements. Subsequent microbiological investigations, including fungal culture and polymerase chain reaction (PCR), isolated Alternaria alternata. The patient was treated for cutaneous alternariosis with itraconazole for 12 weeks and demonstrated significant improvement of the lesions. This case highlights the role of dual histopathological and microbiological laboratory investigation in suspected opportunistic cutaneous mycoses.
Keywords: antifungal therapy, fungal infections, immunocompromised host, invasive fungal infections, skin and soft tissue infections
Mots-clés: hôte immunodéprimé, infections fongiques, infections fongiques invasives, infections de la peau et des tissus mous, traitement antifongique
Abstract
Les chercheurs présentent un cas d’alternariose cutanée multifocale chez un homme de 69 ans atteint d’une leucémie à tricholeucocytes. Le patient a consulté à cause de nodules violacés et douloureux sur les extrémités inférieures et l’avant-bras gauche. Son examen physique était autrement normal. Des biopsies ont été d’abord soumises en vue d’un examen histopathologique, puis de tests microbiologiques. L’histopathologie a révélé une hyperplasie épidermique, la formation d’abcès épidermiques et des éléments fongiques intracellulaires et extracellulaires. Les explorations microbiologiques subséquentes, y compris les cultures fongiques et l’amplification en chaîne par polymérase, ont isolé l’Alternaria alternata. Le patient a reçu un traitement de 12 semaines à l’itraconazole pour vaincre une alternariose cutanée, et ses lésions ont considérablement diminué. Ce cas souligne l’intérêt de conjuguer l’exploration histopathologique à l’exploration microbiologique dans les cas présumés de mycose opportuniste.
Case Presentation
A 69-year-old man presented to primary care in Saskatchewan with multiple painful violaceous plaques and nodules on his lower extremities, left forearm, and upper back. He denied any fever or constitutional symptoms. His medical history was significant for hairy cell leukemia, diagnosed 7 years previously. The patient had received his last dose of cladribine 1 month prior to the appearance of the lesions. His hobbies included vegetable gardening and freshwater boating in Saskatchewan. He reported no significant animal or bird contact and denied ingestion of unpasteurized milk products or uncooked meats. The patient had no significant travel history outside of Canada.
Dermatological examination revealed multiple violaceous papules and nodules with an overlying scaly crust on both shins and left forearm (Figure 1). Cardiovascular and respiratory examinations were normal. There was no palpable lymphadenopathy nor hepatosplenomegaly present on examination.
Figure 1:
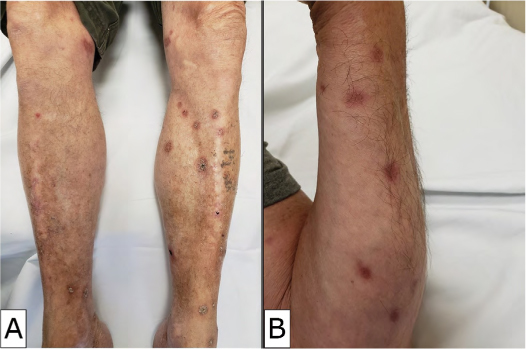
(a) Violaceous plaques and nodules involving bilateral lower extremities of 69-year-old male patient with hairy cell leukemia, and (b) similar lesions involving left forearm
Biochemical and hematological blood tests were performed and demonstrated bicytopenia with hemoglobin of 109 g/L and a platelet count of 118 × 109/L. His leukocyte count was within the reference range (8.0 × 109/L) with mild lymphopenia. Hepatic and renal function tests were normal. Blood cultures were negative for bacterial growth. Serology for HIV was negative, and superficial viral swabs obtained from the nodules for herpes simplex virus and varicella zoster virus polymerase chain reaction (PCR) were negative. His chest X-ray was normal.
A punch biopsy of a pustular lesion on the back was submitted for histopathological examination. Sections showed pseudoepitheliomatous hyperplasia with intraepithelial neutrophils with and without microabscess formation. Within the dermis, there was brisk mixed inflammatory infiltrate consisting of lymphocytes, histiocytes, eosinophils, neutrophils, and occasional multinucleated giant cells. Spherical fungal elements were identified on hematoxylin and eosin (H&E) sections and with periodic acid–Schiff (PAS) stain. These fungal elements were identified within areas of abscess formation and within occasional multinucleated giant cells (Figure 2). A diagnosis of cutaneous mycosis was suspected, with a recommendation to correlate with microbiological culture. PCR for fungal elements was also attempted on the tissue block but failed.
Figure 2:
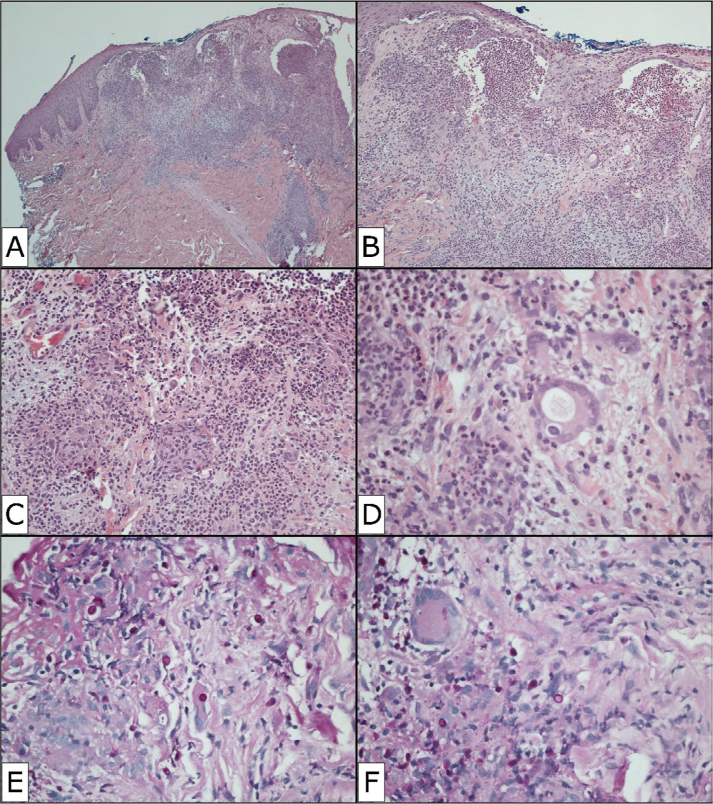
(a) Low power view of skin biopsy from back, demonstrating pseudoepitheliomatous hyperplasia, intraepidermal abscess formation, and dermal inflammation (H&E, 40x magnification); (b) higher magnification of areas of abscess formation with scattered multinucleated giant cells (H&E, 100x magnification); (c) section showing mixed dermal inflammation, granulomas, and intracellular fungal elements (arrow) (H&E, 200x magnification); (d) high power view of intracellular fungal elements (arrow), showing refractile wall and red pigmentation (H&E, 400x magnification); PAS stain highlighting (e) extracellular; and (f) intracellular fungal organisms (PAS stain, 400x magnification)
H&E = Hematoxylin and eosin; PAS = Periodic acid–Schiff
The patient was then referred to Infectious Diseases, who advised to perform a second skin punch biopsy and submit for fungal culture. Additional investigations revealed a negative serum cryptococcal antigen and negative urine Histoplasma antigen. Initial microscopic examination from his second biopsy demonstrated fungal elements with calcofluor stain. The tissue was plated to selective fungal agars (IMA = inhibitory mold agar; CGC = cycloheximide, gentamicin, chloramphenicol; CG = chloramphenicol, gentamicin; SP = sodium pyruvate), and growth was identified after 4 days of incubation at 30°C, consisting of white cotton-like colonies with surface central green colouration and black to brown reverse pigmentation. Lactophenol blue transparent adhesive tape preparation showed septate hyphae and long chains of brown, rounded conidia with beaked apices and both transverse and oblique septae (Figure 3), subsequently identified as Alternaria spp.
Figure 3:

(a) Fungal culture demonstrating cotton-like surface with green to grey pigmentation (Sabouraoud dextrose agar); (b) and (c) lactophenol blue preparations demonstrating septate hyphae and long chains of brown, rounded conidia with beaked apices and both transverse and oblique septae (lactophenol blue preparation, oil immersion, 500x magnification)
Fungal PCR using ribosomal primers designed to amplify the ITS2 region was performed on both the initial skin biopsy (formalin-fixed paraffin-embedded [FFPE]) and the follow-up fresh tissue submitted for microbiology. The FFPE tissue yielded a PCR product. However, sequencing gave indeterminate results. The cultured organism was also submitted for PCR and sequencing, resulting in the identification of Alternaria alternata/A. tenuissima with 98% homology (GenBank database).
The patient was diagnosed with multifocal cutaneous alternariosis and was treated with itraconazole 200 mg once daily for 12 weeks with adjunctive cryotherapy. Following treatment, the nodules had significantly improved with minimal residual skin hyperpigmentation and no ongoing pain (Figure 4). There were no signs of relapse when the patient was seen 6 months later in follow-up.
Figure 4:

(a) Cutaneous lesions on legs at presentation. Lesion after (b) 8 weeks and (c) 12 weeks of systemic itraconazole treatment
Discussion
Alternaria spp are dematiaceous molds known to infrequently cause opportunistic phaeohyphomycoses in humans. The genus is large and complex, with only a few species consistently reported to be human pathogens (1,2). They are ubiquitous within the environment, commonly found as saprophytes in soil, and have a worldwide geographic distribution. Alternaria spp are common plant pathogens in Saskatchewan and across Canada, found in crops and cultivated and wild vegetation (3).
While Alternaria spp infrequently cause human infection in immunocompetent hosts, the number of cases of alternariosis in immunocompromised patients is increasing. The most common risk factors are solid organ and hematopoietic stem cell transplantation; receipt of immunosuppressive medications including corticosteroids; hematological disease; diabetes; HIV; and Cushing syndrome (1,2,4,5). Infection is acquired via traumatic inoculation or respiratory inhalation through contact with contaminated soil or vegetation (4). While dermatological manifestations involving cutaneous and subcutaneous tissue are most common, other manifestations of alternariosis, including rhinosinusitis, ocular infections, and onychomycosis with invasive disseminated disease are reported infrequently (1,2).
Cutaneous alternariosis usually presents as erythematous papules and nodules on the extremities that are sometimes associated with pain. The lesions can develop an erosion and ulcerate over time and with corticosteroid treatment (1,4–6). In immunocompromised patients, multiple lesions are often identified, and investigation for disseminated disease is warranted (7). Tissue biopsy is often required to establish the diagnosis of cutaneous alternariosis with evidence of fungal tissue invasion; molecular techniques can also be useful to identify Alternaria spp. As Alternaria spp are ubiquitous in the environment, positive fungal cultures and visualization of fungal elements within histopathology sections are necessary to distinguish infection from contamination (2,5).
Infection with Alternaria spp can demonstrate a spectrum of histologic findings, ranging from dermal inflammation with fungal elements to epidermal hyperplasia with intraepidermal abscesses and suppurative granulomas. Of note, as the lesions age, the granulomatous component can become more prominent and may be replaced by fibrosis (7). In our case, sections showed pseudoepitheliomatous hyperplasia with superficial, almost intraepidermal, abscess formation with brisk mixed dermal inflammatory cells, including abundant histiocytes and scattered multinucleated giant cells; these are classically described histologic features associated with Alternaria spp infection. The walls of the spore-like elements show brown to red pigmentation, making identification on H&E stains possible (5,7). In our case, both septate hyphae and round spore-like elements were identified on routine H&E stain and PAS histochemical stain. Microscopic examination of the culture shows characteristic conidia with beaked apices. Morphological differences, such as the degree of branching in the conidia chains and orientation of septa, have been suggested to differentiate between species (1). However, a combination of morphology and molecular evaluation is reported to be more reliable for speciation of Alternaria (8,9).
Various molecular methods are available for the identification of fungal organisms, including both pan-fungal and genus or species-specific methods. Most methods have been validated to be used on unprocessed fresh samples, culture specimens, and FFPE tissue (10,11,12). The most widely used is internal transcribed spacer (ITS) sequencing, as the target region contains conserved sequences in the majority of fungi and the species resolution using this method is high (10,11). Comparison of the obtained sequence to a reliable reference sequence in a database with strict quality control (for example, The National Centre for Biotechnology Information Basic Local Alignment Search Tool [NCBI BLAST]) is essential to accurate speciation of the fungus (1,10). In our case, the FFPE specimen gave indeterminate sequencing results, although PCR product was identified. Various reasons for reduced sensitivity of PCR on FFPE tissue have been reported, including low organism burden, DNA fragmentation and cross-linking secondary to formalin fixation, and non-specific amplification of background human DNA (11,12). In our histology specimen, the organism count was low and may explain the failure of the FFPE tissue sequencing. The sequence obtained from our fungal culture was consistent with previous reports of molecular taxonomy of Alternaria spp, in which A. tenuissima cannot be distinguished from A. alternata by molecular methods (1). Microscopic characteristics help identify Alternaria to the genus level but may be insufficient to differentiate to the species level.
Currently, there are no randomized controlled trials that have evaluated treatment strategies for alternariosis, nor are there standardized treatment recommendations. Itraconazole is the most commonly used antimicrobial described in treating alternariosis. Other agents, including voriconazole, posaconazole, and amphotericin B, have been reported to be successful in treating cutaneous alternariosis. In some cases, adjunctive surgical debridement or cryotherapy can be employed to optimize clinical cure (13,14).
Conclusion
Cutaneous infection with Alternaria spp is a relatively uncommon complication that has been described in patients who are immunocompromised. Our case demonstrates the importance of histopathology and microbiology investigations in patients with suspected opportunistic cutaneous mycoses. Furthermore, this case emphasizes the value of collaboration between infectious diseases, microbiology, and pathology.
Ethics approval:
N/A
Informed consent:
Informed consent was obtained from the patient.
Funding:
No funding was received for this article.
Disclosures:
The authors have nothing to disclose.
Peer review:
This manuscript has been peer reviewed.
References
- 1.Pastor FJ, Guarro J. Alternaria infections: laboratory diagnosis and relevant clinical features. Clin Microbiol Infect. 2008;14(8):734–46. 10.1111/j.1469-0691.2008.02024.x. Medline: [DOI] [PubMed] [Google Scholar]
- 2.Hsu CC, Chang SS, Lee PC, Chao SC. Cutaneous alternariosis in a renal transplant recipient: a case report and literature review. Asian J Surg. 2015;38(1):47–57. 10.1016/j.asjsur.2012.08.010. Medline: [DOI] [PubMed] [Google Scholar]
- 3.Elmhirst J, editor. The Canadian Phytopathological Society Canadian plant disease survey: disease highlights 2019. Can J Plant Pathol. 2019;41(sup1):1–197. 10.1080/07060661.2019.1619270. [DOI] [Google Scholar]
- 4.Ioannidou D, Maraki S, Krüger Krasagakis, S et al. Cutaneous alternariosis revealing acute myeloid leukemia in an adult patient. Mycoses. 2004;47(5-6):227–30. 10.1111/j.1439-0507.2004.00954.x. Medline: [DOI] [PubMed] [Google Scholar]
- 5.Caviedes MP, Torre AC, Eliceche ML, Valdivia Monteros DC, Volonteri VI, Galimberti RL. Cutaneous phaeohyphomycosis. Int J Dermatol. 2017;56(4):415–20. 10.1111/ijd.13590. Medline: [DOI] [PubMed] [Google Scholar]
- 6.Hu W, Ran Y, Zhuang K, Lama J, Zhang C. Alternaria arborescens infection in a healthy individual and literature review of cutaneous alternariosis. Mycopathologia. 2015;179(1-2):147–52. 10.1007/s11046-014-9822-9. Medline: [DOI] [PubMed] [Google Scholar]
- 7.Ferrándiz-Pulido C, Martin-Gomez MT, Repiso T, et al. Cutaneous infections by dematiaceous opportunistic fungi: diagnosis and management in 11 solid organ transplant recipients. Mycoses. 2019;62(2):121–7. 10.1111/myc.12853. Medline: [DOI] [PubMed] [Google Scholar]
- 8.Brás S, Sabino R, Laureano A, et al. Cutaneous infection by different Alternaria species in a liver transplant recipient. Med Mycol Case Rep. 2015;8:1–4. 10.1016/j.mmcr.2015.01.004. Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Albataineh MT, Sutton DA, Fothergill AW, Wiederhold NP. Update from the laboratory: clinical identification and susceptibility testing of fungi and trends in antifungal resistance. Infect Dis Clin North Am. 2016;30(1):13–35. 10.1016/j.idc.2015.10.014. Medline: [DOI] [PubMed] [Google Scholar]
- 10.Schuermans W, Hoet K, Stessens L, et al. Molecular identification of cutaneous alternariosis in a renal transplant patient. Mycopathologia. 2017;182(9-10):873–7. 10.1007/s11046-017-0166-0. Medline: [DOI] [PubMed] [Google Scholar]
- 11.Rickerts V. Identification of fungal pathogens in formalin-fixed, paraffin-embedded tissue samples by molecular methods. Fungal Biol. 2016;120(2):279–87. 10.1016/j.funbio.2015.07.002. Medline: [DOI] [PubMed] [Google Scholar]
- 12.Sunderkötter C, Becker K, Kutzner H, et al. Molecular diagnosis of skin infections using paraffin-embedded tissue—review and interdisciplinary consensus. J Dtsch Dermatol Ges. 2018;16(2):139–47. 10.1111/ddg.13438. Medline: [DOI] [PubMed] [Google Scholar]
- 13.Bajwa R, Wojciechowski AL, Hsiao C. Cutaneous alternariosis in a renal transplant patient successfully treated with posaconazole: case report and literature review. Med Mycol Case Rep. 2017;15:16–20. 10.1016/j.mmcr.2017.01.003. Medline: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chowdhary A, Meis JF, Guarro J, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: diseases caused by black fungi. Clin Microbiol Infect. 2014;20(Suppl 3):47–75. 10.1111/1469-0691.12515. Medline: [DOI] [PubMed] [Google Scholar]