

Key Points
Question
Among critically ill patients receiving mechanical ventilation, what is the effect of selective decontamination of the digestive tract (SDD) on hospital mortality?
Findings
In this randomized clinical trial that included 5982 patients, SDD compared with standard care without SDD did not result in a significant difference in in-hospital mortality (27.0% vs 29.1%, respectively; odds ratio, 0.91).
Meaning
Among critically ill patients receiving mechanical ventilation, SDD did not significantly reduce in-hospital mortality compared with standard care without SDD, although the confidence interval around the effect estimate includes a clinically important benefit.
Abstract
Importance
Whether selective decontamination of the digestive tract (SDD) reduces mortality in critically ill patients remains uncertain.
Objective
To determine whether SDD reduces in-hospital mortality in critically ill adults.
Design, Setting, and Participants
A cluster, crossover, randomized clinical trial that recruited 5982 mechanically ventilated adults from 19 intensive care units (ICUs) in Australia between April 2018 and May 2021 (final follow-up, August 2021). A contemporaneous ecological assessment recruited 8599 patients from participating ICUs between May 2017 and August 2021.
Interventions
ICUs were randomly assigned to adopt or not adopt a SDD strategy for 2 alternating 12-month periods, separated by a 3-month interperiod gap. Patients in the SDD group (n = 2791) received a 6-hourly application of an oral paste and administration of a gastric suspension containing colistin, tobramycin, and nystatin for the duration of mechanical ventilation, plus a 4-day course of an intravenous antibiotic with a suitable antimicrobial spectrum. Patients in the control group (n = 3191) received standard care.
Main Outcomes and Measures
The primary outcome was in-hospital mortality within 90 days. There were 8 secondary outcomes, including the proportion of patients with new positive blood cultures, antibiotic-resistant organisms (AROs), and Clostridioides difficile infections. For the ecological assessment, a noninferiority margin of 2% was prespecified for 3 outcomes including new cultures of AROs.
Results
Of 5982 patients (mean age, 58.3 years; 36.8% women) enrolled from 19 ICUs, all patients completed the trial. There were 753/2791 (27.0%) and 928/3191 (29.1%) in-hospital deaths in the SDD and standard care groups, respectively (mean difference, −1.7% [95% CI, −4.8% to 1.3%]; odds ratio, 0.91 [95% CI, 0.82-1.02]; P = .12). Of 8 prespecified secondary outcomes, 6 showed no significant differences. In the SDD vs standard care groups, 23.1% vs 34.6% had new ARO cultures (absolute difference, −11.0%; 95% CI, −14.7% to −7.3%), 5.6% vs 8.1% had new positive blood cultures (absolute difference, −1.95%; 95% CI, −3.5% to −0.4%), and 0.5% vs 0.9% had new C difficile infections (absolute difference, −0.24%; 95% CI, −0.6% to 0.1%). In 8599 patients enrolled in the ecological assessment, use of SDD was not shown to be noninferior with regard to the change in the proportion of patients who developed new AROs (−3.3% vs −1.59%; mean difference, −1.71% [1-sided 97.5% CI, −∞ to 4.31%] and 0.88% vs 0.55%; mean difference, −0.32% [1-sided 97.5% CI, −∞ to 5.47%]) in the first and second periods, respectively.
Conclusions and Relevance
Among critically ill patients receiving mechanical ventilation, SDD, compared with standard care without SDD, did not significantly reduce in-hospital mortality. However, the confidence interval around the effect estimate includes a clinically important benefit.
Trial Registration
ClinicalTrials.gov Identifier: NCT02389036
This randomized clinical trial assesses the effect of selective decontamination of the digestive tract compared with standard care on in-hospital mortality among critically ill patients receiving mechanical ventilation.
Introduction
Selective decontamination of the digestive tract (SDD) was originally described in immunocompromised patients with hematological disease1 and in patients with trauma2,3 and was extended to critically ill patients treated in intensive care units (ICUs) in the 1980s.4,5
Selective decontamination of the digestive tract is the application of topical nonabsorbable antibiotics and antifungal agents to the upper gastrointestinal tract combined with a short course of intravenous antibiotics in patients receiving mechanical ventilation via an endotracheal tube.6
The principal aim of SDD is to prevent the development of ventilator-associated pneumonia caused by pathogenic gram-negative bacteria and secondary overgrowth with yeasts from the upper gastrointestinal tract. Selective decontamination of the digestive tract usually consists of an oral paste and gastric suspension of 3 nonabsorbed antimicrobial agents combined with a short course of an intravenous antibiotic with an appropriate antimicrobial spectrum.5
Although systematic reviews of published randomized clinical trials have reported that the use of SDD was associated with reductions in interval mortality rates and in the incidence of ventilator-associated pneumonia,7,8,9,10 widespread international use of SDD as standard care remains low.6,11,12 Clinician uncertainty may relate to concerns about the generalizability of the results of previous randomized clinical trials, weak recommendations about the use of SDD in international clinical practice guidelines,13 and that use of SDD may increase the prevalence of antibiotic-resistant organisms.8,14
To address this uncertainty, the Selective Decontamination of the Digestive Tract in the Intensive Care Unit (SuDDICU) trial was designed to test the hypothesis that adding SDD to standard care would decrease hospital mortality in mechanically ventilated adults in the ICU compared with standard care. An observational evaluation of whether SDD was noninferior to standard care in changes in microbiological ecology was conducted simultaneously.
Methods
Consent
Ethical approval was obtained from human research ethics committees and research governance offices at each site.
Because SDD was implemented as an ICU-wide intervention, a waiver of individual patient consent up to hospital discharge was obtained. For patients in the control group and ecological assessment, a waiver of consent was also obtained because no intervention was offered.
Study Design and Oversight
This was a crossover, cluster randomized clinical trial with a concomitant observational ecological assessment (Figure 1). The trial protocol, changes to the trial protocol, and statistical analysis plan are presented in Supplement 1, Supplement 2, and Supplement 3, respectively.15 The trial was originally planned as an international trial that would include sites outside Australia, in Canada and the United Kingdom. Details of the evolution of the Australian trial are presented in eAppendix 1 in Supplement 4. Data were entered into an encrypted database for statistical analyses conducted at The George Institute for Global Health.
Figure 1. Participant Flow in the SuDDICU Trial.
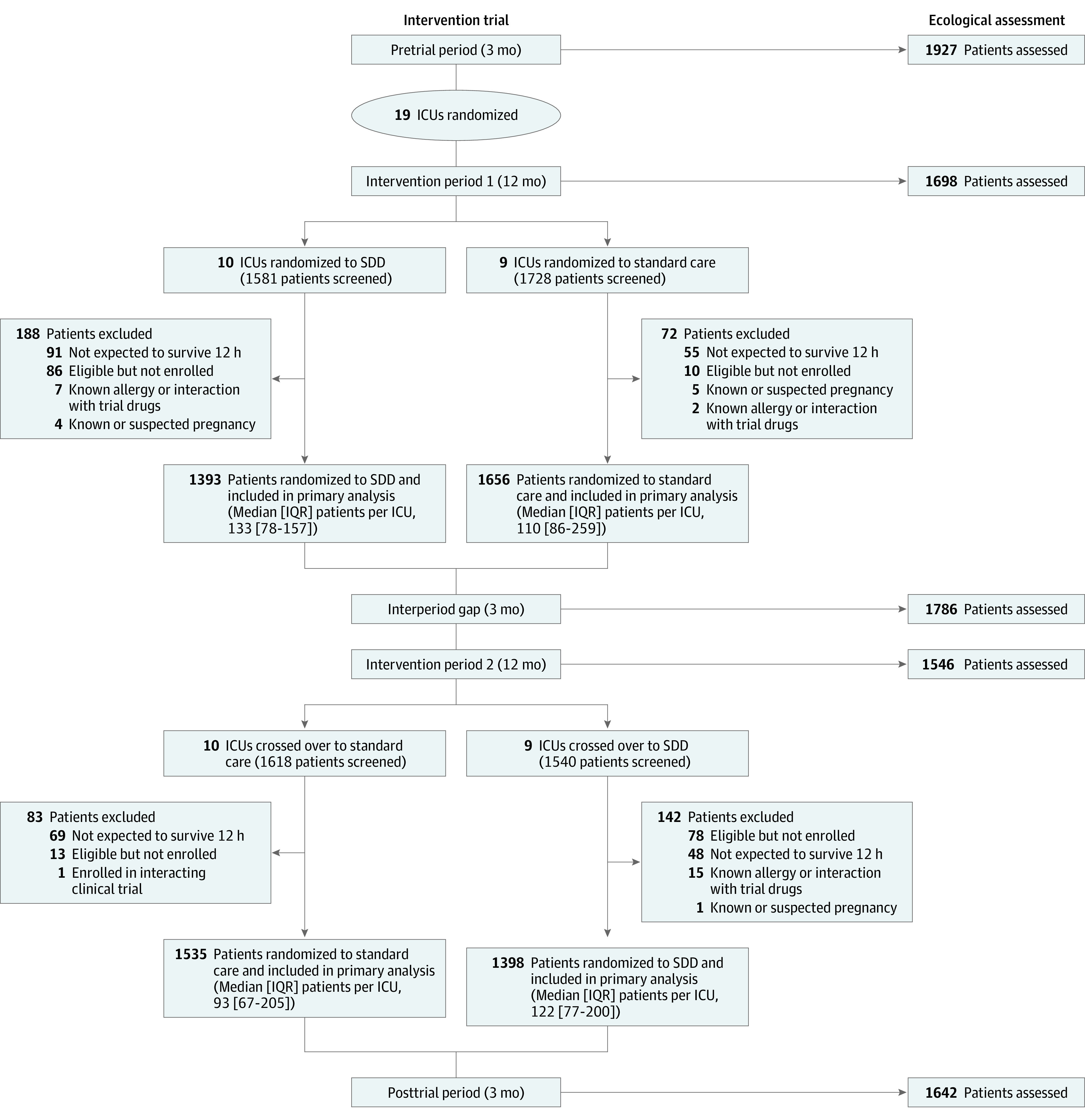
ICU indicates intensive care unit; SDD, selective decontamination of the digestive tract.
The SDD study drug preparations were manufactured by Verita Pharma (Sydney, Australia) under license from The George Institute for Global Health in accordance with the standards for good manufacturing practice approved by the Therapeutic Goods Administration of Australia.
Trial Participants
Eligible ICUs were general medical and surgical facilities in Australia capable of treating mechanically ventilated adults and able to implement the SDD protocol in all eligible patients. Intensive care units were randomly assigned to adopt an SDD strategy or not for 2 alternating 12-month periods, separated by a 3-month interperiod gap.
Eligible patients for the intervention periods were those (1) who were mechanically ventilated via an endotracheal tube on admission to the ICU; (2) who underwent ventilation during that admission; and (3) who were predicted to remain ventilated for at least 48 hours. Patients who were previously predicted not to be mechanically ventilated for more than 48 hours but who subsequently required ongoing ventilation were rescreened for recruitment.
For the ecological assessment that was conducted to determine changes in participating ICU microbiological flora, data were collected for 1 full week of each month during five 3-month ecology collection periods: the pretrial period, interperiod gap, and posttrial period and the final 3 months of each 12-month intervention period. During these periods, all patients admitted to participating ICUs regardless of ventilation status, excluding mechanically ventilated patients who were already enrolled in the intervention groups, were included in the ecology assessment.
Randomization
During the 3-month pretrial period, participating ICUs were stratified by size based on their number of beds and then randomly assigned using a computer-generated program written in SAS (SAS Institute Inc) to deliver either SDD plus standard care (SDD group) or to continue standard care in the first 12-month intervention period. The first intervention period was followed by a 3-month interperiod gap, following which ICUs crossed over to the alternate group for a second 12-month period. This was followed by a 3-month posttrial period (eFigure 1 in Supplement 4).
Interventions
Selective decontamination of the digestive tract comprised (1) a 6-hourly topical application of 0.5 g of oral paste containing 10 mg of colistin, 10 mg of tobramycin, and 125 000 IU of nystatin applied to the buccal mucosa and oropharynx; (2) a 6-hourly administration of 10 mL of gastric suspension containing 100 mg of colistin, 80 mg of tobramycin, and 2 × 106 IU of nystatin to the upper gastrointestinal tract via a gastric or postpyloric tube; and (3) a 4-day course of an intravenous SDD-compliant antibiotic (eg, a third-generation cephalosporin or ciprofloxacin), unless already treated with antibiotics with activity against gram-negative bacteria during the first 4 days after enrollment, in which case additional antibiotics were not administered. Details of the SDD drug preparations are presented in eAppendix 2 (sections O to T) in Supplement 4.
The SDD oral paste and gastric suspension were administered as soon as possible from the time of admission to the ICU, if mechanically ventilated on admission, and/or from the time of endotracheal intubation in the ICU and continued for the duration of mechanical ventilation via an endotracheal tube or until day 90, whichever came first. All other treatments, including the administration of antibiotics for prophylactic or therapeutic indications, were at the discretion of treating clinicians in accordance with respective institutional microbiological prescription polices. A list of SDD-compliant antibiotics is presented in eAppendix 3 (section I) in Supplement 4.
Data and Study Management
Data collected at baseline included demographics, admission diagnosis, the Acute Physiology and Chronic Health Evaluation (APACHE) score (a severity of illness score ranging from 0 to 71 [APACHE II]16 or 0 to 299 [APACHE III],17 with higher scores indicating an increased risk of death), and specific risk factors for infection including prior receipt of oral chlorhexidine and intravenous antibiotics.
For patients treated in ICUs during the SDD intervention period, daily data documenting the delivery of SDD oral paste and gastric suspension were collected for the duration of mechanical ventilation up to 90 days and SDD-compliant antibiotics for 5 days. Adherence in administering the topical components of SDD was reported as the proportion of patients receiving at least 1 eligible SDD dose on a daily basis for the duration of mechanical ventilation.
For all trial participants, doses of all intravenous antibiotics were collected for 28 days. Data recorded daily for 90 days while still in the ICU included the duration of mechanical ventilation, ICU and hospital admission, all new organisms isolated from blood and nonblood cultures, any positive test result for Clostridioides difficile, and antibiotic-resistant organisms from all cultures, as defined in eAppendix 2 (section K) in Supplement 4.
For the ecological assessment, data were collected for 1 full week of each month during five 3-month ecology collection periods, the pretrial period, interperiod gap, and posttrial period and the final 3 months of each 12-month intervention period, for all patients admitted to participating ICUs regardless of mechanical ventilation status, excluding mechanically ventilated patients already enrolled in the intervention periods.
Outcome Measures
The primary outcome was all-cause in-hospital mortality within 90 days of enrollment during the index hospital admission.
Clinical secondary outcomes were ICU mortality and days alive and free of mechanical ventilation, ICU admission, and hospitalization through 90 days.
Microbiological secondary outcomes were the results from all new blood cultures; the incidence of new C difficile infections; the incidence of predefined antibiotic-resistant organisms from all blood, nonblood surveillance, and clinical cultures; and total antibiotic use, defined in daily defined doses.
Ecological assessment outcomes were the same as microbiological secondary outcomes, except that the outcome for total antibiotic use was excluded from the analysis.
Prespecified additional analyses conducted during this trial, but not included in this report, were a nested cohort microbial metagenomic analysis, a health economic analysis from a health care system perspective, and an updated trial-level systematic review with bayesian meta-analysis that included the results of this trial.
Sample Size Calculation
Based on data from a randomized clinical trial conducted in similar populations in Australia and available at the time of trial design,18 a total of about 6000 patients from up to 20 Australian ICUs recruiting 150 patients per treatment period, assuming an intracluster correlation coefficient of 0.01 and an interperiod correlation of 0.005, provided at least 80% power to detect a 4.2-percentage-point reduction in hospital mortality from a baseline mortality rate of 29% at an α = .05. This projected absolute reduction in mortality was considered to fall within a range between 3.5 and 5.0 percentage points, representing a relative risk reduction between 12 and 17 percentage points and a number needed to treat between 20 and 29, consistent with other randomized clinical trials conducted in the Australian context18,19 representing a plausible range for a detectable difference.
For the ecological assessment, the original sample size calculation was based on 40 to 50 sites recruiting 110 to 150 patients per period that would provide 80% power to reject a noninferiority margin of 2%.8 This calculation assumed a base incidence of antibiotic resistance of 10% (as defined in the original study protocol) using an intercluster coefficient of 0.01 and an interperiod coefficient of 0.005 per the mortality analysis. Based on these assumptions, 20 Australian centers had 90% power to reject a noninferiority margin of 3% for antibiotic resistance.
Statistical Analysis
Data were exported to SAS Enterprise Guide version 8.3 for analysis. All patients were analyzed according to their randomization group, regardless of adherence. The primary analysis used all available data with no imputation for missing data.
The primary outcome of death in the hospital within 90 days was analyzed using an individual-level hierarchical logistic regression model, including both a random cluster effect and a random cluster-period effect. The effect of the intervention is presented as the odds ratio for death and the 95% CI, adjusted by the Kenward-Roger correction.20 Prespecified sensitivity analyses were conducted without the Kenward-Roger correction and by fitting a linear regression at the cluster level21 and assessing the potential effect of missing data, using a worst-case and best-case scenario (presented in the statistical analysis plan). Adjusted analyses of the primary outcome were conducted using the logistic regression model after adding age, sex, severity of illness, and operative vs nonoperative diagnosis as fixed covariates. Post hoc analyses included calculation of mean risk differences and 95% CIs for the primary outcome (hospital mortality) and 1 clinical secondary outcome (death within the ICU); secondary analyses included excluding patients who were enrolled less than 1 hour from the time to admission to the ICU; adding prior treatment with oral chlorhexidine and intravenous antibiotics to the model; and presenting the primary outcome for each participating site.
The primary outcome was also examined in 5 prespecified subgroup pairs based on prerandomization age, sex, severity of illness, operative diagnosis, and trauma. Heterogeneity across subgroups was assessed by adding the subgroup variable as well as its interaction with the intervention to the main analysis model.
Analyses of secondary duration outcomes were analyzed as the number of days alive and free of the outcome up to day 90, using a hierarchical linear regression model with the Kenward-Roger correction. Intervention effects were reported as adjusted mean differences and 95% CIs. No adjustments for baseline covariates were made for secondary outcomes. Time to discharge alive from the ICU and the hospital were summarized using cumulative incidence functions treating mortality as a competing risk, censored at day 90. Intervention effects were estimated as hazard ratios and 95% CIs obtained from a cause-specific Cox model, with a fixed effect of treatment and a random site effect. The proportionality assumption was confirmed by visual inspection of the survival curves, given that the test cannot be conducted using a frailty model.
Defined daily doses of antibiotics were defined according to the World Health Organization Collaborating Centre for Drug Statistics Methodology22 and presented as the mean cumulative daily defined dose for all antibiotics and for each antibiotic over the duration of each intervention period up to 28 days. Absolute differences between groups in mean cumulative daily defined doses were tested post hoc using a hierarchical linear mixed model. Microbiological outcomes and adverse events were reported as proportions and compared between treatment groups using an analysis at the cluster-period level.
The statistical significance threshold for the primary outcome was a 2-sided P < .05. For the 4 secondary clinical outcomes, a step-down Holm-Bonferroni approach was prespecified to control the family-wise error rate.23 All other tests were performed using a 2-sided level of .05. Because of the potential for type I error due to multiple comparisons, findings for analyses of secondary end points were considered exploratory.
Ecological data were assessed using a noninferiority comparison and with a noninferiority margin set at 2%, assuming a base incidence of antibiotic resistance of 10%. An increase of 2% is half the increase in tobramycin resistance reported from a previous cluster randomized clinical trial of SDD24 and was considered to represent an increase likely to affect the acceptability of SDD.25,26 Data were analyzed from the 5 study periods using linear regression to model the proportion of events in each cluster and each period, presented as mean proportions and 2-sided 95% CIs (equivalent to a 1-sided 97.5% CI). The main effect of the interventions was estimated as the change, expressed as mean difference and 95% CI (presented as a 1-sided 97.5% CI) in new organisms and antibiotic-resistant organisms isolated from all cultures and new C difficile infections from the pretrial period vs the first intervention period and interperiod gap period combined (first comparison), and from the interperiod gap vs the second intervention period and posttrial period combined (second comparison). A P < .025 from a 1-sided test of noninferiority indicated that the noninferiority margin of 2% was rejected. To declare noninferiority of SDD compared with standard care, the upper bound of the 95% CI around the absolute risk difference between SDD and standard care needed to be lower than 2%. Post hoc, a sensitivity analysis comparing the change in proportions from the pretrial period and each of the 2 intervention periods was conducted.
One prespecified interim analysis was conducted and reviewed by the data and safety monitoring committee after the completion of the first 12-month intervention period, including day 90 follow-up data at all sites.
Results
Study Sites and Patients
From May 2017 to November 2021, 19 ICUs in 17 hospitals in Australia recruited a total of 14 581 participants, of which 5982 participants were enrolled in the intervention study and 8599 were enrolled in the ecological assessment (Figure 1; eTable 1, eFigure 2, and eFigure 3 in Supplement 4).
Intervention Study
For the first intervention period, 3049 patients were recruited, 1393 (45.7%) in ICUs allocated to SDD and 1656 (54.3%) in ICUs allocated to standard care; for the second intervention period, 2933 patients were recruited, 1398 (47.6%) in SDD ICUs and 1535 (52.3%) in standard care ICUs. The primary outcome was available for all patients, 2791 in the SDD group and 3191 in the standard care group.
There were no significant differences in baseline characteristics between the SDD and standard care groups, respectively, other than the median time from ICU admission and enrollment (16.1 [IQR, 3.5-39.7] hours vs 3.7 [IQR, 0.0-20.5] hours) and the number of participants with prior treatment with oral chlorhexidine (778 [27.9%] vs 526 [16.5%]), receipt of preenrollment intravenous antibiotics (2098 [75.2%] vs 2176 [68.2%]), and receipt of intravenous antibiotics for more than 48 hours prior to randomization (689 [32.5%] vs 600 [27.6%]), (Table 1; eTables 2 and 3 in Supplement 4).
Table 1. Baseline Participant Characteristics.
| Characteristics | Selective decontamination of the digestive tract (n = 2791) | Standard care (n = 3191) |
|---|---|---|
| Age, mean (SD), y | 58.2 (17.1) | 58.5 (17.0) |
| Sex, No. (%) | ||
| Female | 1012 (36.3) | 1190 (37.3) |
| Male | 1779 (63.7) | 2001 (62.7) |
| ICU admission source, No. (%) | ||
| Emergency department | 1119 (40.1) | 1170 (36.7) |
| Admitted following emergency surgery | 566 (20.3) | 695 (21.8) |
| Hospital floor (wards) | 517 (18.5) | 575 (18.0) |
| Transfer from another hospital | 236 (8.5) | 314 (9.8) |
| Transfer from another ICU | 189 (6.8) | 209 (6.5) |
| Admitted following elective surgery | 164 (5.9) | 228 (7.1) |
| Time from ICU admission to enrollment, median (IQR), h | 16.1 (3.5-39.7) | 3.7 (0.0-20.5) |
| APACHE diagnostic category: nonoperative, No. (%)a | 2061 (73.8) | 2268 (71.1) |
| Admission diagnosis of trauma, No. (%) | 378 (13.5) | 425 (13.3) |
| Severity of illness score, median (IQR)b | ||
| APACHE II | 20.0 (15.0-26.0) [n = 1479] | 20.0 (15.0-25.0) [n = 2028] |
| APACHE III | 68.0 (49.0-89.0) [n = 1312] | 73.0 (53.0-95.0) [n = 1163] |
| Comorbidities, No. (%) | ||
| Diabetes | 610 (21.9) | 743 (23.3) |
| Systemic steroids | 330 (11.8) | 405 (12.7) |
| Immunosuppression | 231 (8.3) | 279 (8.7) |
| Prior treatments, No. (%) | ||
| Receiving intravenous antibiotics at enrollment | 2098 (75.2) | 2176 (68.2) |
| Receiving intravenous antibiotics for >48 h prior to enrollment | 689 (32.5) | 600 (27.6) |
| Use of oral chlorhexidine | 778 (27.9) | 526 (16.5) |
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit.
The APACHE diagnostic criteria are categorized into nonoperative and operative groups and include prespecified organ system–based criteria with each diagnostic group.
Study Treatments and Process Measures
In the SDD group, the proportion of days of mechanical ventilation during which patients received both the SDD oral paste and gastric suspension was 87.1% (eFigure 4 in Supplement 4). The minimum and total number of eligible doses for the SDD preparations are presented in eTable 4 in Supplement 4.
Over the first 4 days, SDD-compliant intravenous antibiotics were administered to 80.0% patients in the SDD group compared with 53.7% patients in the standard care group (eFigure 5, A and B, in Supplement 4).
Primary Outcome
At hospital discharge, 753 (27.0%) of 2791 patients allocated to SDD and 928 (29.1%) of 3191 patients allocated to standard care had died (mean difference, −1.7% [95% CI, −4.8% to 1.3%]; odds ratio, 0.91 [95% CI, 0.82-1.02]; P = .12). Findings were similar without the Kenward-Roger correction and adjusting for prespecified covariates (Table 2). As all data were available for the primary outcome, sensitivity analyses for missing data did not change the principal analysis (eTable 8 in Supplement 4). Post hoc analyses excluding patients who were enrolled during the first hour after ICU admission (638/2361 [27.0%] vs 577/1889 [30.5%]; odds ratio, 0.85; 95% CI, 0.68-1.06; P = .13) and adjusting for baseline imbalances in chlorhexidine and intravenous antibiotic treatment (odds ratio, 0.91; 95% CI, 0.75-1.11; P = .28) did not significantly alter the analysis (eTable 8 in Supplement 4); hospital mortality at each participating ICU is presented in eTable 9 in Supplement 4.
Table 2. Clinical and Microbiological Outcomes and Adverse Events.
| Outcomes and adverse events | Selective decontamination of the digestive tract (n = 2791) | Standard care (n = 3191) | Difference, % (95% CI) | Odds ratio (95% CI) | P value |
|---|---|---|---|---|---|
| Primary outcome: in-hospital death within 90 d, No. (%)a,b | |||||
| Primary analysisc | 753 (27.0) | 928 (29.1) | MD, −1.7 (−4.38 to 1.3) | 0.91 (0.82-1.02) | .12 |
| Adjusted analysisd | 0.92 (0.75-1.11) | .35 | |||
| Clinical secondary outcomesb,e | |||||
| Death in the ICU, No. (%) | 591 (21.2) | 727 (22.8) | MD, −1.4 (−3.5 to 0.7) | 0.92 (0.79-1.08) | |
| Days alive and free of mechanical ventilation | |||||
| Mean (SD) | 61.9 (36.1) | 59.7 (37.1) | MD, 2.09 (−0.35 to 4.53) | ||
| Median (IQR) | 83 (18-87) | 83 (7-87) | |||
| Days alive and free of ICU admission | |||||
| Mean (SD) | 58.4 (35.7) | 56.4 (36.4) | MD, 1.75 (−0.62 to 4.12) | ||
| Median (IQR) | 79 (6-85) | 78 (2-85) | |||
| Days alive and free of hospital admissionf | |||||
| Mean (SD) | 45.3 (33.4) | 44.0 (34.4) | MD, 1.34 (−0.89 to 3.58) | ||
| Median (IQR) | 59 (0-76) | 57 (0-76) | |||
| Microbiological secondary outcomesb | |||||
| Any antibiotic-resistant organism found, No. (%) | 583 (20.9) | 1036 (32.5) | AD, −11.0 (−14.7 to −7.3) | ||
| Any blood organism found, No. (%) | 156 (5.6) | 259 (8.1) | AD, −1.95 (−3.47 to −0.43) | ||
| Positive for Clostridioides difficile, No. (%) | 14 (0.5) | 29 (0.9) | AD, −0.24 (−0.59 to 0.10) | ||
| Defined daily dose of antibiotics over 28 d, mean (95% CI)g | 0.81 (0.75-0.88) | 0.85 (0.78-0.91) | MD, −0.035 (−0.13 to 0.06) | ||
| Adverse events | |||||
| Adverse medication reactions | 0 | 0 | |||
| Serious adverse medication reactions | 0 | 0 | |||
| Suspected unexpected serious adverse reactions | 0 | 0 | |||
| Serious adverse events | |||||
| Any event | 29 (1.0) | 29 (0.9) | |||
| Blocked gastric tube | 7 (0.3) | 0 | |||
| Otherh | 7 (0.3) | 0 |
Abbreviations: AD, absolute difference; ICU, intensive care unit; MD, mean difference.
Intercluster coefficient for primary outcome is 0.007. There was no significant interaction between treatment and period when analyzing the primary outcome (P = .76). No sensitivity analyses for missing data for the primary outcome was performed because there was 100% data available for analyses. Post hoc determination of the intracluster coefficient and interperiod correlation is presented in eTable 7 in Supplement 4. Post hoc sensitivity analyses adjusting the primary outcome for baseline imbalances for prior use of chlorhexidine and intravenous antibiotics are presented in eTable 8 in Supplement 4.
Data were censored at day 90 after enrollment.
Hierarchical model with Kenward-Roger correction.
Analysis adjusted for age, sex, severity of illness, and operative vs nonoperative diagnosis.
Given than none of the differences were significant at the .05 level for the 4 clinical secondary outcomes, the prespecified Holm-Bonferroni multiplicity correction was not applied.
The median time to hospital discharge was 16 days in the selective decontamination of the digestive tract group and 15 days in the standard care group.
Defined daily doses of antibiotics were defined as the assumed mean maintenance dose per day for a drug used for its main indication in adults according to the World Health Organization Collaborating Centre for Drug Statistics Methodology.22
Other serious adverse events were 1 case each of change in kidney function, persistent diarrhea, toxic epidermal necrolysis, persist fever, and elevated creatinine kinase, and 2 skin rashes.
Clinical Secondary Outcomes
There were no significant between-group differences in ICU mortality (mean difference, −1.4% [95% CI, −3.5% to 0.7%]; odds ratio, 0.92 [95% CI, 0.79-1.08]), the number of days alive and free of mechanical ventilation (mean difference, 2.09 days; 95% CI, −0.35 to 4.53 days), ICU admission (mean difference, 1.75 days; 95% CI, −0.62 to 4.12 days), and hospital admission (mean difference, 1.34 days; 95% CI, −0.89 to 3.58 days) (Table 2). Given that none of the differences were significant at the .05 level, the prespecified Holm-Bonferroni multiplicity correction was not applied. Proximate and underlying causes of death are presented in eTable 10 in Supplement 4. There were no significant between-group differences in the time to death (hazard ratio, 0.93; 95% CI, 0.84-1.02), time to ICU discharge (hazard ratio, 1.05; 95% CI, 0.99-1.11), or time to hospital discharge (hazard ratio, 1.01; 95% CI, 0.95-1.08) (Figure 2A; eFigures 8 and 9 in Supplement 4). There was no significant heterogeneity in the effect of intervention assignment on hospital mortality in any of the 5 predefined subgroup pairs (Figure 2B).
Figure 2. In-Hospital Mortality in the Selective Decontamination of the Digestive Tract and Standard Care Groups.

SDD indicates selective decontamination of the digestive tract. Severity of illness was determined by the Acute Physiology and Chronic Health Evaluation (APACHE) scores, ranging from 0 to 71 (APACHE II)16 or 0 to 299 (APACHE III),17 with higher scores indicating an increased risk of death. The median APACHE II and APACHE III scores were 20 and 70, respectively. P values are from the likelihood ratio test of the interaction term between the subgroup variable and the intervention.
Microbiological Secondary Outcomes
During the intervention period, in the SDD and standard care groups, the number of patients with blood cultures collected was 1664 (59.6%) vs 2163 (67.8%), and the number of patients with nonblood cultures collected was 583 (20.9%) vs 1036 (32.5%), respectively (eTables 5 and 6 in Supplement 4). There was a statistically significant reduction in the proportion of patients from whom antibiotic-resistant organisms were cultured (23.1% vs 34.6%; absolute difference, −11.0%; 95% CI, −14.7% to −7.3%) and who had new positive blood cultures (5.6% vs 8.1%; absolute difference, −1.95%; 95% CI, −3.5% to −0.4%) in the SDD group compared with the standard care group. There was no significant difference in the incidence of new C difficile infection (0.5% vs 0.9%; absolute difference, 0.24%; 95% CI, −0.6% to 0.1%) between the 2 groups (Table 2).
There was no significant difference in mean cumulative daily defined dose of all intravenous antibiotics administered over the first 28 days (0.81 doses [95% CI, 0.75-0.88] vs 0.85 [95% CI, 0.78-0.91]; mean difference, −0.035; 95% CI, −0.13 to 0.06) (Table 2) and in the overall total daily defined dose (eFigure 6 in Supplement 4) or for each antibiotic class (eFigure 7 in Supplement 4) between the SDD and standard care groups.
Ecological Assessment
Among 8599 patients recruited into the ecological assessment, there were no significant between-group differences in demographics, severity of illness scores, hospital mortality, and microbiological cultures over the five 3-month assessment periods (eTable 11 in Supplement 4). The proportions of participants with development of antibiotic-resistant organisms, new positive blood cultures, and C difficile infections over the five 3-month assessment periods are presented in Table 3. For the pretrial period vs the first intervention period and interperiod gap period combined (first comparison) and from the interperiod gap vs the second intervention period and posttrial period combined (second comparison), SDD was noninferior to standard care for the change in the proportion of new positive blood cultures (first comparison: −0.75% vs 0.30%; mean difference, −1.05% [1-sided 97.5% CI, −∞ to 0.47%]; noninferiority P < .001; second comparison: −0.90% vs −0.86%; mean difference, 0.04% [1-sided 97.5% CI, −∞ to 1.67%]; noninferiority P = .008) and for C difficile infections (first comparison: −0.19% vs 0.05%; mean difference, −0.24% [1-sided 97.5% CI, −∞ to 0.18%]; noninferiority P < .001; second comparison: 0.03% vs −0.03%; mean difference, −0.05% [1-sided 97.5% CI, −∞ to 0.37%]; noninferiority P < .001), but not for the change in proportions with positive cultures for antibiotic-resistant organisms (first comparison: −3.3% vs −1.59%; mean difference, −1.71% [1-sided 97.5% CI, −∞ to 4.31%]; noninferiority P = .11; second comparison: 0.88% vs 0.55%; mean difference, −0.32% [1-sided 97.5% CI, −∞ to 5.47%]; noninferiority P = .21) (Figure 3). A post hoc sensitivity analysis comparing the pretrial period with each postintervention period did not meaningfully alter the results (eTable 12 and eFigure 10 in Supplement 4).
Table 3. Ecological Assessment Outcomes.
| Pretrial period, No./total (%) | Period 1 and interperiod gap, No./total (%) | Intervention crossover | Interperiod gap, No./total (%) | Period 2 and posttrial period, No./total (%) | |
|---|---|---|---|---|---|
| New infections with antibiotic-resistant organisms from all blood and nonblood cultures a , b | |||||
| SDD | 108/915 (11.8) | 184/1719 (10.7) | Standard care | 100/874 (11.4) | 159/1589 (10.0) |
| Standard care | 94/1012 (9.3) | 149/1765 (8.4) | SDD | 79/912 (8.7) | 136/1599 (8.5) |
| New positive blood culturesa | |||||
| SDD | 26/915 (2.8) | 40/1719 (2.3) | Standard care | 26/874 (3.0) | 35/1589 (2.2) |
| Standard care | 20/1012 (2.0) | 43/1765 (2.4) | SDD | 29/912 (3.2) | 26/1599 (1.6) |
| New infections with Clostridioides difficilea | |||||
| SDD | 6/915 (0.7) | 5/1719 (0.3) | Standard care | 2/874 (0.2) | 5/1589 (0.3) |
| Standard care | 2/1012 (0.2) | 2/1765 (0.1) | SDD | 2/912 (0.2) | 4/1599 (0.3) |
Abbreviation: SDD, selective decontamination of the digestive tract.
Three microbiological outcomes are presented for sites randomized to each intervention period. Proportions of patients were obtained using linear regression to model the proportion of microbiological outcomes in each cluster and each period during the 2 comparative trial periods: pretrial period vs intervention period 1 and interperiod gap combined and interperiod gap vs intervention period 2 and posttrial period combined.
Antibiotic-resistant organisms were defined according to a modification of the Dutch Nosocomial Infection Guidelines (eAppendix 2 [Section G] in Supplement 4).
Figure 3. Ecological Assessment Outcomes.

The change in mean proportions of microbiological outcomes between selective decontamination of the digestive tract (SDD) and standard care are presented from the pretrial period vs intervention period 1 and the interperiod gap combined (first intervention) and from the interperiod gap vs intervention period 2 and the posttrial period combined (second intervention). The predefined noninferiority margin of 2% is presented as the red line. The noninferiority margin was rejected for new organisms isolated and Clostridioides difficile infection, but not for cultures of antibiotic-resistant organisms, presented by the noninferiority P value.
Adverse Events and Protocol Deviations
Adverse and serious adverse reactions were not notably different between the SDD and standard care groups (Table 2; eTable 13 in Supplement 4). Protocol deviations and valid reasons for not administering SDD interventions are presented in eTables 14 and 15 in Supplement 4.
Discussion
In this crossover, cluster randomized clinical trial, the use of SDD in mechanically ventilated critically ill adults did not significantly reduce in-hospital mortality compared with standard care without SDD, although the confidence interval around the effect estimate includes a clinically important benefit.
The use of SDD did not significantly reduce ICU mortality, the duration of mechanical ventilation, or the duration of ICU and hospital admission. There was a significant reduction in positive blood cultures and cultures of antibiotic-resistant organisms and no significant increase in new C difficile infections in patients who received SDD. Overall antibiotic use was not increased in patients receiving SDD. In the ecology assessment, the use of SDD was noninferior to standard care for the development of new positive blood cultures and C difficile infections, but not for cultures of new antibiotic-resistant organisms. The use of SDD was not associated with an increased incidence of adverse events.
This pragmatic randomized clinical trial has a number of strengths that include a large study population recruited from multiple ICUs under routine clinical care conditions that assessed the effect of SDD on a robust patient-centered outcome. Second, to our knowledge, the trial used the first mass-produced, commercially manufactured good manufacturing practice–compliant SDD preparation that comprised the antimicrobial components previously identified to reduce the incidence of ventilator-associated pneumonia. Third, the trial was conducted according to a prepublished protocol and statistical analysis plan that included a hierarchical logistic regression model to adjust for the cluster size and a robust assessment of treatment adherence. Fourth, the trial had no loss to follow-up. Fifth, the observed baseline mortality rate of 29% confirms the high acuity of illness severity in the study population. Sixth, microbiological surveillance and antibiotic prescription were conducted in accordance with international practice standards within the context of a pragmatic trial. Seventh, the concurrent observational ecological assessment to evaluate changes in ICU microbiology; specifically, antibiotic resistance over the trial period provides new contextual information about the effect of SDD on unit ecology.
A nonsystematic analysis of patient-level data from selected randomized clinical trials conducted between 2000 and 201710 and the current Cochrane Library systematic review27 reported that SDD was associated with a statistically significant reduction in hospital mortality compared with standard care, with an absolute risk reduction in mortality that is similar to the point estimate from this trial.
Consistent with the results of this trial, previous randomized clinical trials conducted in environments of low endemic resistance did not report an increase in antibiotic resistance associated with the use of SDD.5,10,28 A randomized clinical trial conducted in ICUs between 2013 and 2017 with moderate to high baseline rates of antibiotic resistance reported no statistically significant difference in the incidence of new bloodstream infections with multiresistant gram-negative bacteria (the primary outcome) and no significant differences in new highly resistant microorganisms or 28-day mortality between SDD and baseline standard care.29
While clinicians will need to consider the primacy of the effectiveness of SDD in improving patient-centered outcomes over the effect on microbiological outcomes, the use of SDD may confer benefits in specific patient populations such as those with trauma,3 and further trials are needed to confirm benefits in these patients, particularly in environments with high endemic antibiotic resistance.
Limitations
This study had several limitations. First, due its nature, the intervention was unblinded, although this was mitigated by the objective primary outcome and the adoption of SDD as standard care administered to all eligible patients during the intervention period. Second, while more patients were recruited into the standard care group compared with the SDD group, this imbalance is likely due to greater reluctance to recruit patients to the intervention group vs control group when doubt about their duration of ventilation or likelihood of surviving greater than 12 hours existed. Third, while protocol adherence for the use of SDD approached 90% over the duration of the inception period and more than 130 000 doses of SDD were administered, prolonged use of SDD in long-term ventilated patients declined over time due to nonpalatability of the oral paste and reduced access to the upper gastrointestinal tract for the gastric suspension. Fourth, reductions in antibiotic resistance and new blood cultures associated with SDD in the intervention trial may not represent the efficiency of SDD at an individual or institutional level within the context of an effectiveness trial. Fifth, due to the overall low rate of antimicrobial resistance and relatively short period of observation, the ecological assessment had limited power to confirm or refute noninferiority of SDD compared with standard care and did not assess changes in microbiological outcomes at a hospital level or changes in ecology that might be associated with longer-term use of SDD.
Conclusions
Among critically ill patients receiving mechanical ventilation, SDD, compared with standard care without SDD, did not significantly reduce in-hospital mortality. However, the confidence interval around the effect estimate includes a clinically important benefit.
Section Editor: Christopher Seymour, MD, Associate Editor, JAMA (christopher.seymour@jamanetwork.org).
Trial Protocol
Changes to the Trial Protocol
Statistical Analysis Plan
eAppendix 1. Trial Management, Sponsor, Collaborating Centres and Committees, Funding Bodies and Endorsement, and SuDDICU Australia Trial Investigators
eAppendix 2. Supplementary Methods
eTable 1. Representativeness of Trial Participants
eTable 2. APACHE-III Diagnostic Categories
eTable 3. Inclusion Criteria by Category
eTable 4. Minimum and Total Doses of SDD Oral Paste and Gastric Suspension
eTable 5. Organisms Isolated in the Intervention Periods
eTable 6. Specimens Collected for Non-Blood Antibiotic Resistant Organism (ARO) Evaluation
eTable 7. Primary Outcome: Post Hoc Determination of Intra-Cluster Correlation Coefficient and Inter-Period Correlation
eTable 8. Primary Outcome: Adjusted and Post Hoc Sensitivity Analyses
eTable 9. Primary Outcome by Site
eTable 10. Cause of Death
eTable 11. Ecological Assessment Characteristics
eTable 12. Ecological Assessment Microbiological Outcomes: Sensitivity Analysis
eTable 13. Adverse Events
eTable 14. Protocol Deviations
eTable 15. Valid Reasons for Not Administering SDD Interventions
eFigure 1. Trial Design Diagram
eFigure 2. Individual Site Timelines
eFigure 3. Enrolled Patients by Site
eFigure 4. SDD Intervention Compliance
eFigure 5A. Proportion of Patients in the Selective Decontamination of the Digestive Tract Group Receiving SDD-Compliant Antibiotics
eFigure 5B. Proportion of patients in the Standard Care group receiving SDD-compliant antibiotics
eFigure 6. Overall Antibiotic Use in Mean Daily Defined Doses (Days 1-28)
eFigure 7. Cumulative Mean Number of Daily Defined Doses of Antibiotics by Class
eFigure 8. Cumulative Incidence Function to Time to ICU Discharge
eFigure 9. Cumulative Incidence Function to Time of Hospital Discharge
eFigure 10. Ecological Assessment Outcomes: Sensitivity Analysis
eReferences
Nonauthor Collaborators. SuDDICU Investigators for the Australian and New Zealand Intensive Care Society Clinical Trials Group
Data Sharing Statement
References
- 1.Schimpff SC. Infection prevention during profound granulocytopenia: new approaches to alimentary canal microbial suppression. Ann Intern Med. 1980;93(2):358-361. doi: 10.7326/0003-4819-93-2-358 [DOI] [PubMed] [Google Scholar]
- 2.Stoutenbeek CP, van Saene HK, Miranda DR, Zandstra DF. The effect of selective decontamination of the digestive tract on colonisation and infection rate in multiple trauma patients. Intensive Care Med. 1984;10(4):185-192. doi: 10.1007/BF00259435 [DOI] [PubMed] [Google Scholar]
- 3.Stoutenbeek CP, van Saene HK, Little RA, Whitehead A; Working Group on Selective Decontamination of the Digestive Tract . The effect of selective decontamination of the digestive tract on mortality in multiple trauma patients: a multicenter randomized controlled trial. Intensive Care Med. 2007;33(2):261-270. doi: 10.1007/s00134-006-0455-4 [DOI] [PubMed] [Google Scholar]
- 4.van Saene HK, Stoutenbeek CP, Hart CA. Selective decontamination of the digestive tract (SDD) in intensive care patients: a critical evaluation of the clinical, bacteriological and epidemiological benefits. J Hosp Infect. 1991;18(4):261-277. doi: 10.1016/0195-6701(91)90184-A [DOI] [PubMed] [Google Scholar]
- 5.de Smet AM, Kluytmans JA, Cooper BS, et al. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med. 2009;360(1):20-31. doi: 10.1056/NEJMoa0800394 [DOI] [PubMed] [Google Scholar]
- 6.Wittekamp BHJ, Oostdijk EAN, Cuthbertson BH, et al. Selective decontamination of the digestive tract (SDD) in critically ill patients: a narrative review. Intensive Care Med. 2020;46(2):343-349. doi: 10.1007/s00134-019-05883-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Silvestri L, van Saene HK, Zandstra DF, et al. Impact of selective decontamination of the digestive tract on multiple organ dysfunction syndrome: systematic review of randomized controlled trials. Crit Care Med. 2010;38(5):1370-1376. doi: 10.1097/CCM.0b013e3181d9db8c [DOI] [PubMed] [Google Scholar]
- 8.Daneman N, Sarwar S, Fowler RA, Cuthbertson BH; SuDDICU Canadian Study Group . Effect of selective decontamination on antimicrobial resistance in intensive care units: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(4):328-341. doi: 10.1016/S1473-3099(12)70322-5 [DOI] [PubMed] [Google Scholar]
- 9.Roquilly A, Marret E, Abraham E, Asehnoune K. Pneumonia prevention to decrease mortality in intensive care unit: a systematic review and meta-analysis. Clin Infect Dis. 2015;60(1):64-75. doi: 10.1093/cid/ciu740 [DOI] [PubMed] [Google Scholar]
- 10.Plantinga NL, de Smet AMGA, Oostdijk EAN, et al. Selective digestive and oropharyngeal decontamination in medical and surgical ICU patients: individual patient data meta-analysis. Clin Microbiol Infect. 2018;24(5):505-513. doi: 10.1016/j.cmi.2017.08.019 [DOI] [PubMed] [Google Scholar]
- 11.Canter RR, Harvey SE, Harrison DA, et al. ; SuDDICU Investigators . Observational study of current use of selective decontamination of the digestive tract in UK critical care units. Br J Anaesth. 2014;113(4):610-617. doi: 10.1093/bja/aeu108 [DOI] [PubMed] [Google Scholar]
- 12.Cuthbertson BH, Campbell MK, MacLennan G, et al. Clinical stakeholders’ opinions on the use of selective decontamination of the digestive tract in critically ill patients in intensive care units. Crit Care. 2013;17(6):R266. doi: 10.1186/cc13096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. doi: 10.1007/s00134-021-06506-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Oostdijk EAN, Kesecioglu J, Schultz MJ, et al. Effects of decontamination of the oropharynx and intestinal tract on antibiotic resistance in ICUs: a randomized clinical trial. JAMA. 2014;312(14):1429-1437. doi: 10.1001/jama.2014.7247 [DOI] [PubMed] [Google Scholar]
- 15.SuDDICU Investigators . Protocol summary and statistical analysis plan for the Selective Decontamination of the Digestive Tract in Intensive Care Patients (SuDDICU) crossover, cluster randomised controlled trial. Crit Care Resusc. 2021;23:183-193. doi: 10.51893/2021.2.oa5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818-829. doi: 10.1097/00003246-198510000-00009 [DOI] [PubMed] [Google Scholar]
- 17.Knaus WA, Wagner DP, Draper EA, et al. The APACHE III prognostic system: risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100(6):1619-1636. doi: 10.1378/chest.100.6.1619 [DOI] [PubMed] [Google Scholar]
- 18.Finfer S, Chittock DR, Su SY, et al. ; NICE-SUGAR Study Investigators . Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-1297. doi: 10.1056/NEJMoa0810625 [DOI] [PubMed] [Google Scholar]
- 19.Venkatesh B, Finfer S, Cohen J, et al. ; ADRENAL Trial Investigators and Australian–New Zealand Intensive Care Society Clinical Trials Group . Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378(9):797-808. doi: 10.1056/NEJMoa1705835 [DOI] [PubMed] [Google Scholar]
- 20.Kenward MG, Roger JH. An improved approximation to the precision of fixed effects from restricted maximum likelihood. Comput Stat Data Anal. 2009;53(7):2583-2595. doi: 10.1016/j.csda.2008.12.013 [DOI] [Google Scholar]
- 21.Morgan KE, Forbes AB, Keogh RH, et al. Choosing appropriate analysis methods for cluster randomised cross-over trials with a binary outcome. Stat Med. 2017;36(2):318-333. doi: 10.1002/sim.7137 [DOI] [PubMed] [Google Scholar]
- 22.World Health Organization . Defined daily dose (DDD). Accessed September 7, 2016. https://www.who.int/tools/atc-ddd-toolkit/about-ddd
- 23.Holm S. Simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6:65-70. [Google Scholar]
- 24.Oostdijk EA, de Smet AM, Blok HE, et al. Ecological effects of selective decontamination on resistant gram-negative bacterial colonization. Am J Respir Crit Care Med. 2010;181(5):452-457. doi: 10.1164/rccm.200908-1210OC [DOI] [PubMed] [Google Scholar]
- 25.Duncan EM, Cuthbertson BH, Prior ME, et al. ; SuDDICU International Study Group . The views of health care professionals about selective decontamination of the digestive tract: an international, theoretically informed interview study. J Crit Care. 2014;29(4):634-640. doi: 10.1016/j.jcrc.2014.03.013 [DOI] [PubMed] [Google Scholar]
- 26.Wunderink RG. Welkommen to our world: emergence of antibiotic resistance with selective decontamination of the digestive tract. Am J Respir Crit Care Med. 2010;181(5):426-427. doi: 10.1164/rccm.200912-1821ED [DOI] [PubMed] [Google Scholar]
- 27.Minozzi S, Pifferi S, Brazzi L, et al. Topical antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving mechanical ventilation. Cochrane Database Syst Rev. 2021;1:CD000022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.de Jonge E, Schultz MJ, Spanjaard L, et al. Effects of selective decontamination of digestive tract on mortality and acquisition of resistant bacteria in intensive care: a randomised controlled trial. Lancet. 2003;362(9389):1011-1016. doi: 10.1016/S0140-6736(03)14409-1 [DOI] [PubMed] [Google Scholar]
- 29.Wittekamp BH, Plantinga NL, Cooper BS, et al. Decontamination strategies and bloodstream infections with antibiotic-resistant microorganisms in ventilated patients: a randomized clinical trial. JAMA. 2018;320(20):2087-2098. doi: 10.1001/jama.2018.13765 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
Changes to the Trial Protocol
Statistical Analysis Plan
eAppendix 1. Trial Management, Sponsor, Collaborating Centres and Committees, Funding Bodies and Endorsement, and SuDDICU Australia Trial Investigators
eAppendix 2. Supplementary Methods
eTable 1. Representativeness of Trial Participants
eTable 2. APACHE-III Diagnostic Categories
eTable 3. Inclusion Criteria by Category
eTable 4. Minimum and Total Doses of SDD Oral Paste and Gastric Suspension
eTable 5. Organisms Isolated in the Intervention Periods
eTable 6. Specimens Collected for Non-Blood Antibiotic Resistant Organism (ARO) Evaluation
eTable 7. Primary Outcome: Post Hoc Determination of Intra-Cluster Correlation Coefficient and Inter-Period Correlation
eTable 8. Primary Outcome: Adjusted and Post Hoc Sensitivity Analyses
eTable 9. Primary Outcome by Site
eTable 10. Cause of Death
eTable 11. Ecological Assessment Characteristics
eTable 12. Ecological Assessment Microbiological Outcomes: Sensitivity Analysis
eTable 13. Adverse Events
eTable 14. Protocol Deviations
eTable 15. Valid Reasons for Not Administering SDD Interventions
eFigure 1. Trial Design Diagram
eFigure 2. Individual Site Timelines
eFigure 3. Enrolled Patients by Site
eFigure 4. SDD Intervention Compliance
eFigure 5A. Proportion of Patients in the Selective Decontamination of the Digestive Tract Group Receiving SDD-Compliant Antibiotics
eFigure 5B. Proportion of patients in the Standard Care group receiving SDD-compliant antibiotics
eFigure 6. Overall Antibiotic Use in Mean Daily Defined Doses (Days 1-28)
eFigure 7. Cumulative Mean Number of Daily Defined Doses of Antibiotics by Class
eFigure 8. Cumulative Incidence Function to Time to ICU Discharge
eFigure 9. Cumulative Incidence Function to Time of Hospital Discharge
eFigure 10. Ecological Assessment Outcomes: Sensitivity Analysis
eReferences
Nonauthor Collaborators. SuDDICU Investigators for the Australian and New Zealand Intensive Care Society Clinical Trials Group
Data Sharing Statement