

Abstract
Objective:
Behavioral inhibition (BI) is an infant temperament characterized by heightened reactivity and negative affect in response to novel people and situations. BI is among the earliest and strongest predictors of future anxiety problems. However, not all children with a history of BI will manifest anxiety problems. A growing body of evidence suggests that proactive control skills may help buffer youth with BI from future anxiety difficulties; yet, it remains unclear how temperament may interact with the development of cognitive control to influence anxiety risk. The present study tests whether enhancements in proactive control occurring during adolescence may reduce risk for anxiety among youth with a history of BI.
Method:
Participants included 185 adolescents (56% female) whose temperament was assessed during toddlerhood. In adolescence, participants completed anxiety assessments and an AX Continuous Performance Test (AX-CPT) to assess cognitive control strategy. Both assessments were administered at age 13 years and again at 15 years.
Results:
Latent change score modeling revealed that, on average, participants increasingly used proactive control strategies and experienced worsening anxiety from age 13 to 15 years. Early BI was associated with a smaller anxiety increase from 13 to 15 years, but only among those whose proactive control skills improved at mean or greater rates.
Conclusion:
The present findings suggest that greater proactive control development during adolescence protects youth with high BI youth from age-related increases in anxiety. Results support a framework that highlights cognitive control as a key moderator of anxiety risk among children with a history of high BI.
Keywords: anxiety, development, cognitive control, behavioral inhibition, adolescence
Introduction
Behavioral inhibition (BI) is an infant temperament characterized by heightened distress to and avoidance of novelty1. It is among the earliest and strongest risk markers for future anxiety difficulties2. Nevertheless, only approximately half of all toddlers with high BI develop clinically significant anxiety problems3. Understanding factors that moderate the BI-anxiety relation may help identify youth who are at particularly elevated risk for anxiety and inform prevention efforts.
Across at least four independent samples, children’s cognitive control skills – skills involved in monitoring and adapting behavior in accordance with behavioral goals – have consistently been shown to modulate anxiety risk for children with BI4–7 (for a recent review, see8). The dual-mechanisms of control theory9 differentiates two temporally distinct and complementary modes of cognitive control: proactive and reactive. Proactive control involves early selection and maintenance of goal-relevant information over time, whereas reactive control involves in-the-moment recruitment of resources, often in response to conflict. For example, a child who is about to engage in play with a peer must proactively select and maintain in working memory their goal of playing, which includes information about the selected activity such as the rules of the game to be played. Reactive control, in contrast, may be recruited in response to unexpected events. For example, the sudden appearance of a peer’s angry facial expression may trigger reactive control processes that shift attention away from the game and towards the peer’s expression, thus disrupting proactive goal maintenance and potentially increasing anxiety risk.
An emerging view of BI’s neurophysiological profile recognizes heightened detection of salient stimuli (e.g., threatening faces) as a core feature of the temperament8. According to this view, some children with BI learn to regulate their responses to such cues via improved proactive control skills8,10–13. This increased proactive control likely helps the child resist goal-irrelevant demands on their attention (e.g., ignoring the peer’s potentially threatening facial expression) or, otherwise, more efficiently recover their goal-oriented attention (e.g., quickly refocusing attention back toward the game), thereby reducing risk for anxiety. To date, cross-sectional evidence suggests that typically developing youth gradually transition from greater reliance on reactive control to greater reliance on proactive control from childhood to early adulthood14–21. However, to the authors’ knowledge, no study to date has examined proactive control development longitudinally. Moreover, no known study has examined how proactive development may relate to early temperament or to changes in anxiety over time. Adolescence is a time of markedly elevated neurocognitive development22 and is when the most prevalent anxiety disorders (e.g., social anxiety disorder) typically emerge23. Understanding how developmental changes in cognitive control and anxiety relate to one another may inform the assessment and identification of youth who are at heightened risk of manifesting anxiety difficulties and may also highlight potential target mechanisms for intervention.
One of the few available tasks used to measure proactive control processes is the AX Continuous Performance Test (AX-CPT24). The AX-CPT presents a series of letter pairs dissociable into four trial types (AX, AY, BX, and BY). The task enables measurement of proactive control via contextual cues (e.g., the letters “A” or “B”) that indicate to the participant how they should respond to an upcoming probe (e.g., the letters “X” or “Y”). The task also involves differential probabilities of trials (i.e., some trial types are more common than others), making some trial types relatively expected and others relatively unexpected. Participants are instructed to press a target button only when they see an “A” that is followed by an “X.” As such, accurate performance depends, in part, on proactively attending to the cue identity and maintaining it in working memory until the probe letter appears. Recently, we used the AX-CPT in a longitudinal study examining cognitive control factors in the context of BI-anxiety relations. We found that 13-year-old children with a history of high BI during toddlerhood tended to rely less on proactive control, as indicated by lower d’ context scores computed from their AX-CPT behavioral responses, than children without such history25. d’ context is a behavioral index based on signal detection theory and involves comparing hit rate on AX trials to false alarm rate on BX trials; thus, d’ context reflects the extent to which participants discriminate between target and nontarget trials as a function of the cue identity, with higher scores indicating greater proactive control use24. In addition to the association between BI and less proactive control use, we also found that youth with BI who used less proactive control had greater parent-reported total anxiety than youth with BI who used more proactive control25. In a later follow-up of the same cohort, involving the AX-CPT combined with EEG, BI was associated with elevated anxiety specifically among youth using a cognitive control strategy characterized by the combination of low proactive control and high reactive control as measured via event-related potentials13. Overall, there is emerging evidence based on both behavioral and neural data suggesting that children with BI who engage less in proactive control may be at greater risk for anxiety difficulties.
However, as noted earlier, all known studies to date examining the development of proactive control have been cross-sectional. Cross-sectional analyses using only one time of measurement per participant can usefully generate hypotheses about longitudinal change. However, these approaches often seriously misrepresent developmental processes26. This is largely because cohort effects have nonintuitive and cumulative impacts on group means and standard deviations (for examples illustrated with simulated data, see26). Therefore, making correct developmental inferences requires longitudinal research designs paired with analyses that capture change over time.
Additionally, none of the existing cross-sectional studies of proactive development has examined relations with anxiety or examined the role of early temperament. Thus, it remains unclear how early temperament may interact with developmental changes in proactive control to influence anxiety risk. To address this question and the problem of relying on cross-sectional analyses, the present study applied a novel latent change score modeling approach to data from a relatively large longitudinal study examining anxiety risk among adolescents with a history of BI. BI was assessed during toddlerhood and AX-CPT behavior and anxiety measures via multi-informant report were obtained at 13 and again at 15 years of age13,25. This is an especially important age window which captures the mean onset for the most prevalent anxiety disorders (e.g., social anxiety disorder, which has a mean age of onset of 14.3 years23). Understanding developmental factors that relate to increases in anxiety during this key period may help identify youth facing particularly elevated risk for anxiety disorders and may inform prevention and intervention efforts that target these factors. It was hypothesized that youth with a history of high BI who experience higher levels of proactive control development (i.e., greater increases in d’ context) from 13 to 15 years would experience smaller increases in anxiety than youth with a history of high BI who experience lower levels of proactive control development.
Method
Participants
Participants included 189 adolescents (56% female) enrolled as part of a longitudinal study examining relations between infant temperament and the emergence of anxiety who were administered the AX-CPT at either the 13- or 15-year assessments. Four of these were excluded due to not having valid AX-CPT data at either time point, for a final sample size of 185 (see AX-CPT section below for more details). This study’s recruitment strategy and screening methods have been described in detail elsewhere27,28. Briefly, infants (N=779; age 4 months) completed a laboratory temperament screening for emotional and motor reactivity towards novel auditory and visual stimuli. From these, infants with high motor and high positive or high negative reactivity were oversampled to reflect a range of temperamental reactivity that is wider than would be found in a randomly selected community sample. The selected infants (N=291) continued to participate in assessments of cognitive and socio-emotional development throughout childhood and adolescence. Informed consent and assent were obtained at each assessment, and each visit protocol was approved by the institutional review board of the University of Maryland, College Park. Race/ethnicity was rated by parents at the time of infant recruitment and was as follows: 17% African American, 5% Hispanic/Latino, 3% Asian, 72% White, and 3% “Other.” The mean age at the 13-year assessment was 13.2 years (SD = 0.6 years) and the mean age at the 15-year assessment was 15.4 years (SD = 0.6 years). The attrition rate from infancy (N=291) to the adolescent assessments (N=189) was 35.1%. Chi-squared and t-tests revealed no significant differences between those who did versus did not participate in the adolescent assessments in terms of race/ethnicity, sex, BI, or maternal education level (all ps > .30).
Behavioral Inhibition
BI was assessed at ages 24 and 36 months via behavioral coding of laboratory assessments27,28. During laboratory observations, children were presented with an unfamiliar person and various novel toys (i.e., robot, inflatable tunnel) during three episodes. Measures of interest were proximity to mother and latency to vocalize, to approach and touch the toys, and to approach a stranger. Additionally, maternal report of social fear was collected using the Toddler Behavior Assessment Questionnaire29. Each questionnaire and observation measure was Z-scored and then all Z-scores were averaged to create a composite BI score that combined ratings across informants and time points. Results when using a measure of BI that includes only observational scores and excludes maternal report measures are presented in Figure S1 (available online) and were similar to those based on the combined BI measure.
AX Continuous Performance Task
To measure proactive control, participants completed an AX-CPT9,24. The AX-CPT presents a continuous series of letter pairs (i.e., a cue letter followed by a probe letter) dissociated into 4 trial types: AX, AY, BX, and BY. AX trials were the target trials, meaning that when participants saw an “A” cue followed by an “X” probe, they were to press a different button in response to the probe than during the other 3 trial types. Specifically, participants were instructed to press a nontarget button (e.g., “1”) following every cue, and following most probe types; however, if an “A” cue was followed by an “X” probe, participants were to press a target button (e.g., “4”) upon seeing the probe.
At age 13 and consistent with past behavioral studies of the AX-CPT, AX trials were presented 70% of the time and the other trial types (i.e., AY, BX, and BY) were each presented 10% of the time25. Participants completed a total of 150 trials presented in random order. Each trial began with a center fixation cross appearing for 200 ms, followed by the presentation of the cue stimulus appearing for 500 ms. Next, a center fixation cross appeared during a 1,000-ms response window and during a subsequent 3,900-ms delay. The probe stimulus was then presented for 500 ms followed by another 1,000-ms response window with a fixation cross. At age 15, the task was modified to facilitate simultaneous collection of EEG (for EEG results from the 15-year assessment, see13). In line with past EEG studies involving the AX-CPT30,31, the breakdown of trial types was changed to 55%/15%/15%/15% and the total number of trials was increased to 319. To accommodate the larger number of trials, the total delay between cue and probe onset was reduced to an interval randomized to between 1,400 and 1,600 ms. These changes were made to acquire enough trials to achieve adequate EEG signal-to-noise ratio in each condition. Critically, because AX trials were still by far the most frequent and comprised the majority of trials, behavioral predictions remained the same as in the 13-year version of the task.
Letter stimuli were presented in boldface 60-point Courier New font on a black background. To make clear the distinction between cues and probes, cues were presented in cyan and probes were presented in white. Stimuli were presented on a 17-inch LCD monitor using E-Prime 2.0 Professional (Psychology Software Tools, Inc., Sharpsburg, PA). Consistent with past work, individual trials were excluded from analysis if reaction time (RT) was >3 standard deviations above or below each participant’s mean RT on correct trials25, resulting in exclusion of less than 3% of all trials at each assessment. After excluding outlier trials, accuracy and mean reaction times were computed for each trial type. Consistent with other studies with children, participants needed at least 60% accuracy on BY trials for inclusion in analyses13,20,25. This resulted in the exclusion of four participants who did not have valid behavioral data for at least one of the AX-CPT assessments (final N=185). Within-subject trial type comparisons of RT and accuracy at age 13 and 15 years have been reported elsewhere13,25. Briefly, at both assessments, B trials were generally faster and more accurate than A trials. AY trials were consistently the slowest and least accurate by a wide margin. This is in accordance with past studies of the AX-CPT in populations predominantly relying on proactive control24,32,33. Behavior on all four trial types was significantly correlated across time (Accuracy – AX: r = .29; AY: r = .29; BX: r = .43, BY: r = .53; RT – AX: r = .42; AY: r = .39; BX: r = .41; BY: r = .33; all ps < .01).
d’ context, a commonly used behavioral index based on signal detection theory, provides a measure of the ability to discriminate between target and nontarget trials as a function of the cue24. d’ context scores were computed by comparing correct responses on AX trials (hits) relative to incorrect responses on BX trials (false alarms). A correction was applied in cases where there was a hit rate of 1 (hit rate = 2−(1/N), where N = number of target trials) or a false alarm rate of 0 (false alarm rate = 1–2−(1/N), where N = number of nontarget trials). The distribution of d’ context scores (13-year: skewness = −0.52, kurtosis = 0.22; 15-year: skewness = −0.05, kurtosis = 2.57) was inspected and determined to be normal (see Table 1 for descriptive statistics). Consistent with the broader literature involving d’ context, higher scores were interpreted to indicate a more proactive style of cognitive control because the participant used the cue information to inform future responses20,24,25.
Table 1.
Descriptive Statistics and Pearson Correlations Among Continuous Measures of Interest and Demographics
| Measure | N | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Behavioral Inhibition (Standardized) | 182 | 0.0 | 0.8 | |||||||||||||
| 2. SCARED Total Anxiety Parent Report: 13-year | 159 | 10.3 | 8.8 | .25** | ||||||||||||
| 3. SCARED Total Anxiety Child Report: 13-year | 168 | 17.9 | 11.4 | .04 | .40*** | |||||||||||
| 4. SCARED Total Anxiety Parent Report: 15-year | 171 | 11.1 | 9.7 | .15 | .74*** | .35*** | ||||||||||
| 5. SCARED Total Anxiety Child Report: 15-year | 157 | 20.5 | 12.2 | .07 | .47*** | .47*** | .52*** | |||||||||
| 6. AX-CPT d’ Context: 13-year | 128 | 1.8 | 1.3 | −.07 | −.02 | −.11 | .10 | −.09 | ||||||||
| 7. AX-CPT d’ Context: 15-year | 164 | 3.1 | 0.7 | .02 | −.05 | −.04 | −.02 | .00 | .45*** | |||||||
| 8. AX-CPT BX Probe Interference Effect: 13-year | 129 | .09 | .17 | .15 | .10 | .12 | −.08 | .14 | −.54*** | −.22* | ||||||
| 9. AX-CPT BX Probe Interference Effect: 15-year | 164 | .03 | .06 | −.14 | .05 | .04 | .04 | −.05 | −.16 | −.56*** | .12 | |||||
| 10. Sex (% male) | 185 | 44.3% | - | −.10 | −.20* | −.33*** | −.32*** | −.38*** | −.08 | −.11 | .04 | .03 | ||||
| 11. Pubertal Development Scale: 13-year | 156 | 2.5 | 0.5 | .07 | .19* | .14 | .17* | .18* | .06 | −.05 | −.05 | .00 | −.53*** | |||
| 12. Pubertal Development Scale: 15-year | 130 | 3.1 | 0.5 | .08 | .10 | −.13 | .04 | −.03 | .16 | .12 | .00 | −.09 | −.08 | .25** | ||
| 13. Race/Ethnicity (% White) | 185 | 71.9% | - | −.09 | −.06 | −.08 | .07 | .05 | .17 | .28*** | −.13 | −.03 | −.07 | −.08 | .13 | |
| 14. Maternal Education | 175 | 1.2 | 0.7 | −.01 | −.24** | −.19* | −.18* | −.14 | −.10 | .07 | −.05 | −.07 | .01 | −.05 | −.08 | .22** |
Note: Reported Ns reflect the number of participants with valid scores for the given measure. Sex was dummy coded as female = 0 and male = 1. Maternal education was coded on an ordinal scale where high school diploma = 0, college degree = 1, and post-graduate degree = 2. Lastly, due to small cell sizes for specific racial/ethnic groups, race/ethnicity was collapsed and dummy coded as Non-White = 0 and White = 1. Pubertal stage was assessed via self-report with the Pubertal Development Scale.41 SCARED = Screen for Child Anxiety Related Emotional Disorders. AX-CPT = AX Continuous Performance Test.
p < .05.
p < .01.
p < .001.
Screen for Child Anxiety Related Emotional Disorders (SCARED)
Each participant and their parent separately completed the revised version of the SCARED34 at the 13- and 15-year assessments. The parent and child versions of the SCARED included 41 items presented on a 3-point Likert scale (0 = never/hardly ever true, 1 = sometimes/somewhat true, 2 = very/often true). Total SCARED scores at each time point and from each reporter were included as indicators in latent change score analyses. Internal consistency (Cronbach’s alpha) of the SCARED was high at both time points and for both reporters (13-year parent = .92; 13-year child = .92; 15-year parent = .93; 15-year child = .93).
Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL)
Participants were administered the K-SADS-PL35 at both time points. The K-SADS-PL is a semi-structured diagnostic interview for assessing current and past psychopathology among children and adolescents according to DSM-5 criteria. It was administered by an advanced graduate student or doctoral level clinician, under the close supervision of a board-certified child and adolescent psychiatrist and a licensed clinical psychologist. Of the 124 participants administered the K-SADS-PL at age 13 years, 18 (14.5%) currently met criteria for at least one anxiety disorder. Specific anxiety diagnoses included social anxiety disorder (n=9; 7.3%), generalized anxiety disorder (n=6; 4.8%), specific phobia (n=3; 2.4%), separation anxiety disorder (n=2; 1.6%), and anxiety disorder not otherwise specified (n=1; 0.8%). Of the 140 participants interviewed at age 15 years, 42 (30.0%) met criteria for at least one anxiety disorder. Specific anxiety diagnoses at age 15 included social anxiety disorder (n=22; 15.7%), generalized anxiety disorder (n=18; 12.9%), specific phobia (n=15; 10.7%), separation anxiety disorder (n=1; 0.7%), and panic disorder (n=1; 0.7%).
Data Analytic Strategy
A series of latent change score models was tested to estimate changes in d’ context and anxiety across ages 13 and 15 years (for models including a behavioral measure of reactive control, the BX probe interference effect36, see Figures S2–S3, available online). Latent change score models are a class of structural equation models enabling estimation of the complex relations between variables assessed at multiple time points. Anxiety at each time point was estimated as a latent score with the following indicators: parent-reported SCARED total score, child-reported SCARED total score, and current presence/absence of any anxiety disorder as assessed with the K-SADS-PL (measured as a binary score). Little’s missing completely at random (MCAR) test revealed missing data were likely MCAR, χ2(254) = 278, p = .144. Due to missing data and potential departures from multivariate normality, all models were estimated using a robust maximum likelihood estimator, which provides unbiased estimates when data are missing at random or MCAR37. For visualization of missing data patterns, see Figure S4, available online. Models were tested in R (version 4.0.5) with the package “lavaan” (version 0.6–838) according to the procedures described by Kievit et al.39.
Measurement models including only anxiety (i.e., without d’ context) were tested for measurement invariance across time. There were no significant differences in model fit statistics when anxiety factor loadings were constrained to be equal across the two time points versus when they were unconstrained (χ2diff(2) = 0.09, p = .957), indicating that the factor loadings were invariant across time. Additionally, the constrained model had good fit, χ2robust(7) = 10.14, p = .181, root mean square error of approximation (RMSEA) = .053 [90% CI: .000 .120], standardized root mean squared residual (SRMR) = .039, comparative fit index (CFI) = .986, Yuan-Bentler scaling factor = 1.180. Thus, in all subsequent models involving anxiety, anxiety factor loadings were constrained to be equal across both time points39.
In the next step, separate latent change score models for anxiety and cognitive control strategy were tested to estimate mean levels of change in the absence of any covariates. These models were then combined into a bivariate latent change score model (BLCS; Figure 1) to estimate relations between the two sets of measures39. Lastly, to test for a possible interaction between BI and the change in d’ context in predicting anxiety change, the latent change scores obtained from the BLCS model were extracted and included in a new path model that was also implemented in lavaan (see Figure 2). The interaction test between BI and cognitive control change score was conducted in a separate model to reduce model complexity and improve interpretability of main effects. All predictors were mean-centered prior to computation of the interaction term. Anxiety and d’ context at age 13 years were included as covariates. The interaction was probed with the R package “semTools” (version 0.5–440).
Figure 1. Bivariate Latent Change Score Model Including Anxiety and Proactive Control.
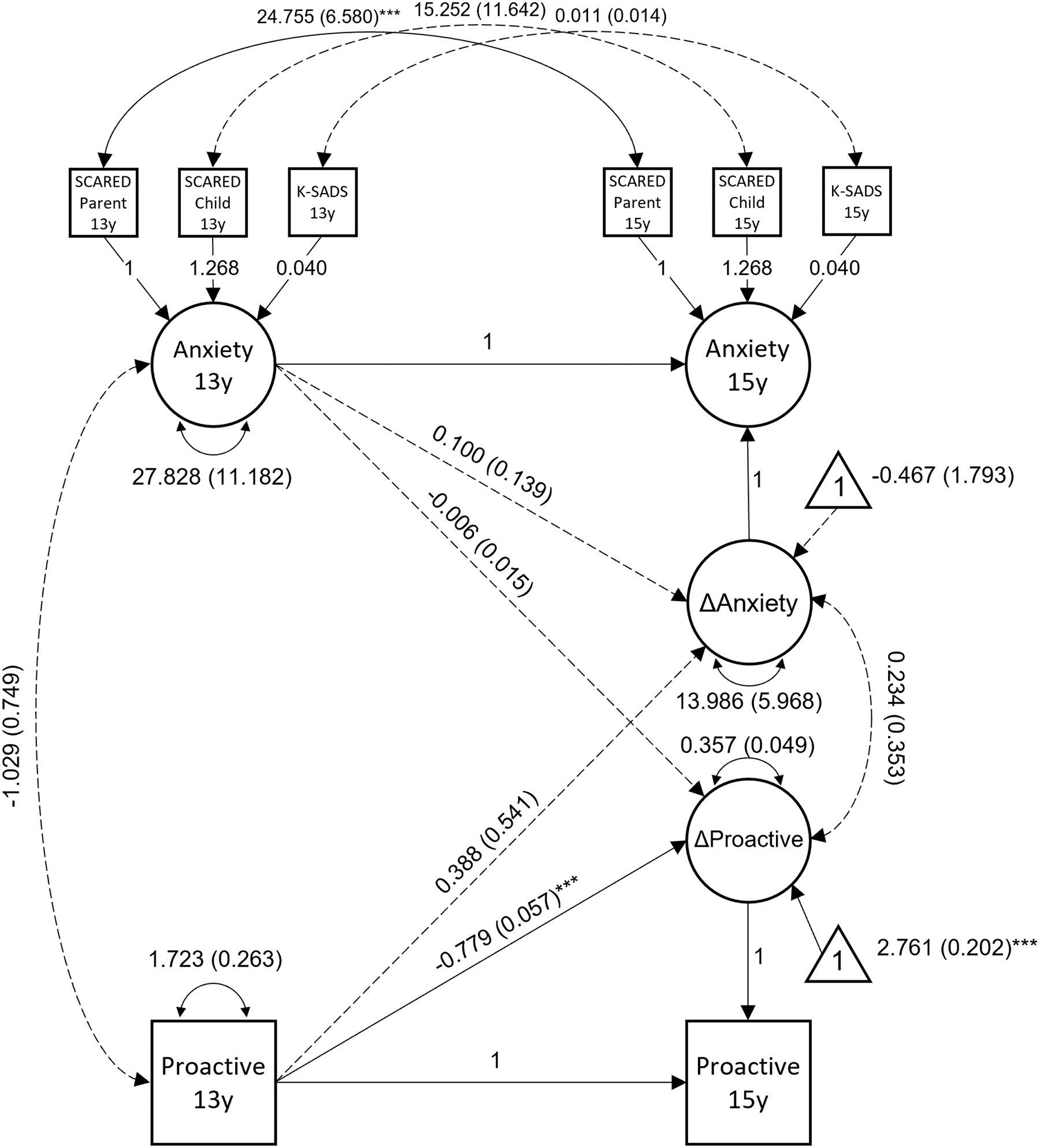
Note: Parameter estimates are shown with standard error in parentheses. 13y = Measured 13-year assessment. 15y = Measured at 15-year assessment. ANX = anxiety latent score. ΔANX = anxiety latent change score. ΔD’ Context = d’ context latent change score. K-SADS = Schedule for Affective Disorders and Schizophrenia for School-Age Children. SCARED = Screen for Child Anxiety Related Emotional Disorders.
***p < .001.
Figure 2. Behavioral Inhibition (BI) Interaction Model and Simple Slopes.
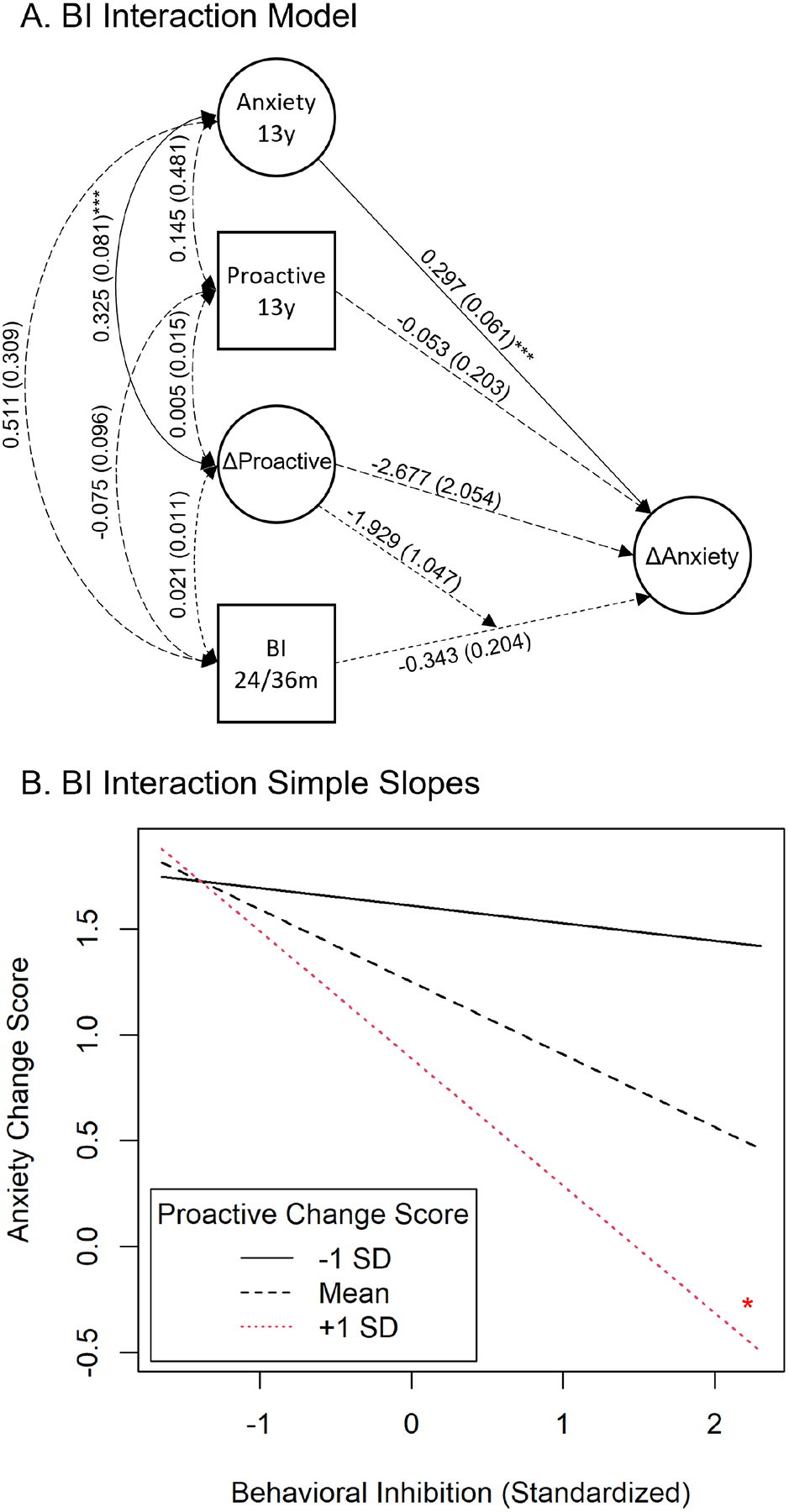
Note: A) Model testing interaction between proactive control latent change score and BI, controlling for 13-year anxiety and 13-year proactive control. Parameter estimates are shown with standard error in parentheses. 13y = measured at 13-year assessment. BI 24/36m = behavioral inhibition averaged across 24 and 36 months of age. B) Simple slopes from the BI X d’ context latent change score interaction. BI was associated with a smaller 13- to 15-year anxiety increase specifically among participants with proactive control change scores that were at least 1 SD above the mean.
*p < .05. **p < .01. ***p < .001.
Results
The univariate latent change score model for anxiety had good model fit: χ2robust(7) = 10.14, p = .181, RMSEA = .053 [90% CI: .000 .120], SRMR = .039, CFI = .986, Yuan-Bentler scaling factor = 1.180. The anxiety latent change score was significantly greater than zero (Estimate = 1.23, SE = 0.56, p = .028), indicating that, on average, anxiety increased from 13 to 15 years. Similarly, the d’ context latent change score was significantly greater than zero (Estimate = 1.31, SE = 0.11, p < .001), suggesting youth used more proactive strategies at age 15 than at age 13 years. There are no model fit statistics to report for the d’ context model because this model had no free parameters (i.e., the model was “identified”).
BLCS model fit was good: χ2robust(15) = 24.07, p = .064, RMSEA = .057 [90% CI: .000 .098], SRMR = .046, CFI = .963, Yuan-Bentler scaling factor = 1.009 (Figure 1). Inspection of key parameters revealed that greater d’ context at 13 years was associated with a smaller d’ context change from 13 to 15 years (p < .001). There was no significant association between 13-year anxiety and anxiety change (p = .470), between anxiety and d’ context 13-year scores (p = .169), or between anxiety and d’ context change scores (p = .507).
The BI interaction model predicting 13- to 15-year anxiety change scores revealed a main effect of 13-year anxiety (Figure 2, top panel). Greater anxiety at age 13 was associated with a larger anxiety increase from 13 to 15 years (p < .001). The hypothesized interaction between d’ context change score and BI was not significant – albeit it was a non-significant trend (p = .065); however, this interaction did reach significance when using a measure of BI that excludes maternal report (Figure S1, available online), when controlling for potential interactions with sex (Figure S5, available online), or when using change scores obtained from a model that included reactive control (Figures S2–S3, available online). Planned follow-up of this interaction revealed that BI was associated with a smaller 13- to 15-year anxiety increase specifically among participants with levels of d’ context change that were at least 1 SD above the mean (p = .015; Figure 2, bottom panel). The same pattern of results was also found when controlling for sex, race/ethnicity, maternal education level, and pubertal stage (Figure S6, available online). Supplemental analyses including the behavioral measure of reactive control revealed that the proactive and reactive control measures were strongly negatively correlated, as were their two change scores (Figure S2, available online). The interactions between BI and proactive and reactive control change were both significant and in opposite directions (Figure S3, available online). That is, BI was associated with a smaller anxiety increase among participants with larger proactive control increases or those with smaller reactive control increases.
Discussion
The present study tested whether the relations between early BI and changes in anxiety vary as a function of proactive control development during adolescence. This study benefitted from several strengths, including a relatively large longitudinal sample beginning in infancy and the application of a novel structural equation modeling approach combining multi-informant assessments of psychopathology. The analytic approach was robust to data missingness typical of long-term longitudinal designs. It was hypothesized that youth with a history of high BI would be relatively protected against anxiety if they had higher levels of proactive control development, compared to those with a history of high BI with lower levels of proactive control development8,13,25. On average, youth experienced worsening anxiety from age 13 to 15 years. However, youth with early BI were protected from this anxiety increase if their proactive control skills developed at a relatively faster rate. Youth at the highest levels of both BI and proactive control development even experienced somewhat decreased anxiety from 13 to 15 years. Because all models controlled for 13-year scores, this effect was not explained by potential individual differences in 13-year anxiety or proactive control. Age-related change in proactive control did not predict age-related change in anxiety among youth low in BI. Due to the observed main effect of 13-year anxiety on the increase in symptoms from 13 to 15, adolescents with high anxiety at age 13 faced elevated risk for even higher levels of anxiety by age 15. This pattern held for participants low in BI and/or with stable levels of proactive control. However, this was not the case for the unique subset of highly anxious 13-year-old adolescents who also had a history of behavioral inhibition and showed an increase in proactive control between the ages of 13 and 15. For this unique subset of highly anxious 13-year-old adolescents, anxiety either did not change or decreased. According to an emerging framework, some children with BI learn to downregulate their responses to potentially threatening stimuli via increased proactive control8. In line with the present results, an increase in the deployment of proactive control may help ameliorate BI-related risk for anxiety during adolescence.
The current findings have implications for understanding the development of cognitive control. First, youth tended to use increasingly proactive strategies between the ages of 13 and 15 years. Second, 13-year anxiety was associated with greater proactive control development from 13 to 15, suggesting that proactive control development may be, in part, a response to early anxiety. Third, youth who were already utilizing predominantly proactive strategies by age 13 tended to exhibit less of a proactive control shift from age 13 to 15, indicating that some youth may have experienced their shift toward greater proactive control earlier in development. To address these last two possibilities, assessments of proactive control beginning prior to adolescence will be needed. An important caveat to these developmental findings is that the AX-CPT administered at age 15 had shorter delays between the cue and probe than the 13-year version (1,400 – 1,600 ms vs. 4,900 ms). This may have made it easier to use proactive strategies at age 15 because the cue identity did not have to be maintained in working memory for as long as in the 13-year version. Furthermore, the 15-year task was administered with EEG. Thus, a portion of the observed proactive control increase from age 13 to 15 may have been due to these differences in the task and context, in addition to potential practice effects. Nevertheless, although previous work has found cross-sectional differences in proactive control use across child, adolescent, and adult age groups14–21, the present study is the first to our knowledge to examine longitudinal increases in proactive control use. Though the changes in task parameters from age 13 to 15 years allow for only cautious interpretations of group-level development of proactive control, the fact that all youth experienced the same task changes permits confident interpretations of betweensubject differences in proactive control development, which were the focus of the present study. Future work investigating the development of proactive control would benefit from a larger number of repeated assessments beginning earlier in childhood and, if possible, employing identical tasks across those assessments. Together, this would help provide greater temporal separation and inform a more comprehensive understanding of these processes across development, thus, helping to distinguish between potential causes versus consequences of anxiety.
Because proactive control development from age 13 to 15 years protected youth with BI from increased anxiety, the present findings may inform anxiety prevention and intervention efforts. Assessments of cognitive control strategy may eventually help identify children or adolescents with BI facing particularly elevated anxiety risk. These youth may benefit from existing psychosocial interventions designed for children with BI42,43, from cognitive control training programs targeting proactive control directly33,44–46, or a combination of the two. A key limitation, however, is that temporal precedence of proactive control development over anxiety onset has yet to be established, further underscoring the need for more longitudinal work in this area. Nevertheless, it is encouraging that anxiety risk among youth with BI has consistently been shown to be modulated by cognitive control processes5,6,13,25,30,47–50.
In summary, the present findings indicate that, among youth with a history of BI, a shift toward greater proactive control use during early adolescence may be associated with smaller increases in anxiety (and, in some cases, even decreased anxiety) during this key period for the emergence of anxiety disorders23. The present study contributes to an emerging understanding of how cognitive control factors may buffer anxiety risk that is otherwise associated with fearful temperament8 and, more generally, of plasticity in cognitive and emotional functioning during adolescence. Further longitudinal studies beginning earlier in childhood are needed to better understand the relations between proactive control skills and anxiety risk across development.
Supplementary Material
Acknowledgments
The authors would like to thank all the participants who have continued to dedicate their time to this research starting from infancy all the way to young adulthood. They also thank the many research assistants who helped with data collection as part of this longitudinal study.
Disclosure:
Dr. Troller-Renfree has received grant support from NIMH and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Dr. Henderson has received grant support from the Social Sciences and Humanities Research Council of Canada and the Canada Foundation for Innovation. Dr. Chronis-Tuscano has received funding from the National Institutes of Health, royalties from Oxford University Press, and honoraria for lectures to professional audiences. Dr. Fox has received grant support from NIMH, NICHD, the National Science Foundation, the National Institutes of Health Environmental Influences on Child Health Outcomes Consortium, the Russell Sage Foundation, and the Lumos Foundation. He has received royalties from Guilford Press and Harvard University Press and honoraria for lectures to professional audiences. Drs. Valadez, Morales, Buzzell, and Pine have reported no biomedical financial interests or potential conflicts of interest.
This research was supported by the National Institute of Mental Health (NIMH), Grand/Award Number: U01MH093349 (to N.A.F.) and Intramural Research Project ZIAMH002782 (to D.S.P.).
De-identified data supporting this manuscript will be available from NIMH Data Archive (NDA; see https://nda.nih.gov/edit_collection.html?id=2538).
The research was performed with permission from the University of Maryland, College Park’s Institutional Review Board.
Consent has been provided for descriptions of specific patient information.
Dr. Morales served as the statistical expert for this research.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Kagan J, Reznick JS, Clarke C, Snidman N, Garcia-Coll C. Behavioral inhibition to the unfamiliar. Child Development. 1984;55(6):2212–2225. doi: 10.2307/1129793 [DOI] [Google Scholar]
- 2.Chronis-Tuscano A, Degnan KA, Pine DS, et al. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. Journal of the American Academy of Child & Adolescent Psychiatry. 2009;48(9):928–935. doi: 10.1097/CHI.0b013e3181ae09df [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Clauss JA, Blackford JU. Behavioral Inhibition and Risk for Developing Social Anxiety Disorder: A Meta-Analytic Study. J Am Acad Child Adolesc Psychiatry. 2012;51(10):1066–1075.e1. doi: 10.1016/j.jaac.2012.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Buzzell GA, Morales S, Bowers ME, et al. Inhibitory control and set shifting describe different pathways from behavioral inhibition to socially anxious behavior. Dev Sci. 2021;24(1):e13040. doi: 10.1111/desc.13040 [DOI] [PubMed] [Google Scholar]
- 5.Henderson HA. Electrophysiological correlates of cognitive control and the regulation of shyness in children. Developmental Neuropsychology. 2010;35(2):177–193. doi: 10.1080/87565640903526538 [DOI] [PubMed] [Google Scholar]
- 6.Thai N, Taber-Thomas BC, Pérez-Edgar KE. Neural correlates of attention biases, behavioral inhibition, and social anxiety in children: An ERP study. Developmental Cognitive Neuroscience. 2016;19:200–210. doi: 10.1016/j.dcn.2016.03.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Thorell L, Bohlin G, Rydell AM. Two types of inhibitory control: Predictive relations to social functioning. International Journal of Behavioral Development. 2004;28(3):193–203. doi: 10.1080/01650250344000389 [DOI] [Google Scholar]
- 8.Fox NA, Buzzell GA, Morales S, Valadez EA, Wilson M, Henderson HA. Understanding the Emergence of Social Anxiety in Children With Behavioral Inhibition. Biological Psychiatry. Published online October 10, 2020. doi: 10.1016/j.biopsych.2020.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Braver TS. The variable nature of cognitive control: A dual mechanisms framework. Trends in Cognitive Sciences. 2012;16(2):106–113. doi: 10.1016/j.tics.2011.12.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Buzzell GA, Troller-Renfree SV, Morales S, Fox NA. Relations between behavioral inhibition, cognitive control, and anxiety: Novel insights provided by parsing subdomains of cognitive control. In: Pérez-Edgar K, Fox NA, eds. Behavioral Inhibition: Integrating Theory, Research, and Clinical Perspectives. Springer International Publishing; 2018:213–235. doi: 10.1007/978-3-319-98077-5_10 [DOI] [Google Scholar]
- 11.Henderson HA, Pine DS, Fox NA. Behavioral inhibition and developmental risk: A dual-processing perspective. Neuropsychopharmacology. 2015;40(1):207–224. doi: 10.1038/npp.2014.189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Henderson HA, Wilson MJG. Attention processes underlying risk and resilience in behaviorally inhibited children. Curr Behav Neurosci Rep. 2017;4(2):99–106. doi: 10.1007/s40473-017-0111-z [DOI] [Google Scholar]
- 13.Valadez EA, Troller-Renfree SV, Buzzell GA, et al. Behavioral Inhibition and Dual Mechanisms of Anxiety Risk: Disentangling Neural Correlates of Proactive and Reactive Control. JCPP Advances. 2021;1(2):e12022. doi: 10.1002/jcv2.12022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andrews-Hanna JR, Seghete KLM, Claus ED, Burgess GC, Ruzic L, Banich MT. Cognitive Control in Adolescence: Neural Underpinnings and Relation to Self-Report Behaviors. PLOS ONE. 2011;6(6):e21598. doi: 10.1371/journal.pone.0021598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chatham CH, Frank MJ, Munakata Y. Pupillometric and behavioral markers of a developmental shift in the temporal dynamics of cognitive control. Proc Natl Acad Sci USA. 2009;106(14):5529. doi: 10.1073/pnas.0810002106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chevalier N, James TD, Wiebe SA, Nelson JM, Espy KA. Contribution of reactive and proactive control to children’s working memory performance: Insight from item recall durations in response sequence planning. Developmental Psychology. 2014;50(7):1999–2008. doi: 10.1037/a0036644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chevalier N, Martis SB, Curran T, Munakata Y. Metacognitive processes in executive control development: The case of reactive and proactive control. Journal of Cognitive Neuroscience. 2015;27(6):1125–1136. doi: 10.1162/jocn_a_00782 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lorsbach TC, Reimer JF. Developmental Differences in Cognitive Control: Goal Representation and Maintenance During a Continuous Performance Task. Journal of Cognition and Development. 2010;11(2):185–216. doi: 10.1080/15248371003699936 [DOI] [Google Scholar]
- 19.Lucenet J, Blaye A. Age-related changes in the temporal dynamics of executive control: A study in 5- and 6-year-old children. Frontiers in Psychology. 2014;5:831. doi: 10.3389/fpsyg.2014.00831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Troller-Renfree SV, Buzzell G, Fox NA. Changes in working memory influence the transition from reactive to proactive cognitive control during childhood. Developmental Science. Published online 2020. doi: 10.1111/desc.12959 [DOI] [PubMed] [Google Scholar]
- 21.Unger K, Ackerman L, Chatham CH, Amso D, Badre D. Working memory gating mechanisms explain developmental change in rule-guided behavior. Cognition. 2016;155:8–22. doi: 10.1016/j.cognition.2016.05.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Fuhrmann D, Knoll LJ, Blakemore SJ. Adolescence as a Sensitive Period of Brain Development. Trends in Cognitive Sciences. 2015;19(10):558–566. doi: 10.1016/j.tics.2015.07.008 [DOI] [PubMed] [Google Scholar]
- 23.de Lijster JM, Dierckx B, Utens EMWJ, et al. The Age of Onset of Anxiety Disorders. Can J Psychiatry. 2017;62(4):237–246. doi: 10.1177/0706743716640757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cohen JD, Barch DM, Carter C, Servan-Schreiber D. Context-processing deficits in schizophrenia: Converging evidence from three theoretically motivated cognitive tasks. J Abnorm Psychol. 1999;108(1):120–133. doi: 10.1037//0021-843x.108.1.120 [DOI] [PubMed] [Google Scholar]
- 25.Troller-Renfree SV, Buzzell GA, Pine DS, Henderson HA, Fox NA. Consequences of not planning ahead: Reduced proactive control moderates longitudinal relations between behavioral inhibition and anxiety. Journal of the American Academy of Child & Adolescent Psychiatry. 2019;58(8):768775.e1. doi: 10.1016/j.jaac.2018.06.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kraemer HC, Yesavage JA, Taylor JL, Kupfer D. How Can We Learn About Developmental Processes From Cross-Sectional Studies, or Can We? AJP. 2000;157(2):163–171. doi: 10.1176/appi.ajp.157.2.163 [DOI] [PubMed] [Google Scholar]
- 27.Calkins SD, Fox NA, Marshall TR. Behavioral and physiological antecedents of inhibited and uninhibited behavior. Child Dev. 1996;67(2):523–540. [PubMed] [Google Scholar]
- 28.Fox NA, Henderson HA, Rubin KH, Calkins SD, Schmidt LA. Continuity and discontinuity of behavioral inhibition and exuberance: Psychophysiological and behavioral influences across the first four years of life. Child Dev. 2001;72(1):1–21. doi: 10.1111/1467-8624.00262 [DOI] [PubMed] [Google Scholar]
- 29.Goldsmith HH. Studying Temperament via Construction of the Toddler Behavior Assessment Questionnaire. Child Development. 1996;67(1):218–235. doi: 10.1111/j.1467-8624.1996.tb01730.x [DOI] [PubMed] [Google Scholar]
- 30.Lamm C, Pine DS, Fox NA. Impact of negative affectively charged stimuli and response style on cognitive-control-related neural activation: An ERP study. Brain and Cognition. 2013;83(2):234243. doi: 10.1016/j.bandc.2013.07.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Troller-Renfree SV. The development of cognitive control during childhood: A neurocognitive perspective. Published online 2018. 10.13016/M2ZC7RX9B [DOI] [Google Scholar]
- 32.Braver TS, Paxton JL, Locke HS, Barch DM. Flexible neural mechanisms of cognitive control within human prefrontal cortex. Proceedings of the National Academy of Sciences. 2009;106(18):73517356. doi: 10.1073/pnas.0808187106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gonthier C, Macnamara BN, Chow M, Conway ARA, Braver TS. Inducing Proactive Control Shifts in the AX-CPT. Front Psychol. 2016;7. doi: 10.3389/fpsyg.2016.01822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Birmaher B, Khetarpal S, Brent D, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale Construction and Psychometric Characteristics. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36(4):545–553. doi: 10.1097/00004583-199704000-00018 [DOI] [PubMed] [Google Scholar]
- 35.Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial Reliability and Validity Data. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36(7):980–988. doi: 10.1097/00004583-199707000-00021 [DOI] [PubMed] [Google Scholar]
- 36.Tang R, Etzel JA, Kizhner A, Braver TS. Frontoparietal pattern similarity analyses of cognitive control in monozygotic twins. NeuroImage. 2021;241:118415. doi: 10.1016/j.neuroimage.2021.118415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yuan KH, Bentler PM. Robust mean and covariance structure analysis through iteratively reweighted least squares. Psychometrika. 2000;65(1):43–58. doi: 10.1007/BF02294185 [DOI] [Google Scholar]
- 38.Rosseel Y lavaan: An R Package for Structural Equation Modeling. Journal of Statistical Software. 2012;48(1):1–36. doi: 10.18637/jss.v048.i02 [DOI] [Google Scholar]
- 39.Kievit RA, Brandmaier AM, Ziegler G, et al. Developmental cognitive neuroscience using latent change score models: A tutorial and applications. Developmental Cognitive Neuroscience. 2018;33:99–117. doi: 10.1016/j.dcn.2017.11.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Jorgensen TD, Pornprasertmanit S, Schoemann AM, et al. SemTools: Useful Tools for Structural Equation Modeling; 2021. Accessed April 15, 2021. https://CRAN.R-project.org/package=semTools
- 41.Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: Reliability, validity, and initial norms. J Youth Adolescence. 1988;17(2):117–133. doi: 10.1007/BF01537962 [DOI] [PubMed] [Google Scholar]
- 42.Chronis-Tuscano A, Rubin KH, O’Brien KA, et al. Preliminary Evaluation of a Multi-Modal Early Intervention Program for Behaviorally Inhibited Preschoolers. J Consult Clin Psychol. 2015;83(3):534–540. doi: 10.1037/a0039043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Rapee RM, Kennedy S, Ingram M, Edwards S, Sweeney L. Prevention and early intervention of anxiety disorders in inhibited preschool children. J Consult Clin Psychol. 2005;73(3):488–497. doi: 10.1037/0022-006X.73.3.488 [DOI] [PubMed] [Google Scholar]
- 44.Beloe P, Derakshan N. Adaptive working memory training can reduce anxiety and depression vulnerability in adolescents. Developmental Science. 2020;23(4):e12831. doi: 10.1111/desc.12831 [DOI] [PubMed] [Google Scholar]
- 45.Li Y, Liu F, Zhang Q, Liu X, Wei P. The Effect of Mindfulness Training on Proactive and Reactive Cognitive Control. Front Psychol. 2018;9. doi: 10.3389/fpsyg.2018.01002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Pan D ni, Hoid D, Wang X bo, Jia Z, Li X. When expanding training from working memory to emotional working memory: not only improving explicit emotion regulation but also implicit negative control for anxious individuals. Psychological Medicine. Published online 2020:1–10. doi: 10.1017/S0033291720002275 [DOI] [PubMed] [Google Scholar]
- 47.Lahat A, Lamm C, Chronis-Tuscano A, Pine D, Henderson H, Fox NA. Early behavioral inhibition and increased error monitoring predict later social phobia symptoms in childhood. Journal of the American Academy of Child and Adolescent Psychiatry. 2014;53(4):447–455. doi: 10.1016/j.jaac.2013.12.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.McDermott JM, Perez-Edgar K, Henderson HA, Chronis-Tuscano A, Pine DS, Fox NA. A history of childhood behavioral inhibition and enhanced response monitoring in adolescence are linked to clinical anxiety. Biol Psychiatry. 2009;65(5):445–448. doi: 10.1016/j.biopsych.2008.10.043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Reeb-Sutherland BC, Vanderwert RE, Degnan KA, et al. Attention to novelty in behaviorally inhibited adolescents moderates risk for anxiety. Journal of Child Psychology and Psychiatry. 2009;50(11):1365–1372. doi: 10.1111/j.1469-7610.2009.02170.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.White LK, McDermott JM, Degnan KA, Henderson HA, Fox NA. Behavioral inhibition and anxiety: The moderating roles of inhibitory control and attention shifting. J Abnorm Child Psychol. 2011;39(5):735–747. doi: 10.1007/s10802-011-9490-x [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.