

Abstract
Diabetes‐related foot disease (DFD) is imposing an enormous burden on the health system and society due to the rapid growth of diabetes worldwide. Given the paucity of robust data on the disease burden of DFD in Australia, this study aimed to estimate the burden of disease due to DFD. The burden of DFD was estimated using the disability‐adjusted life‐years (DALY) approach. Data of 27 931 individuals aged 45 years and older with diabetes residing in New South Wales (NSW) from the 45 and Up Study survey were used in this study by linking it with the emergency department, hospital admissions and the deaths' registry data. The disease burden of DFD was estimated as 8915 DALY in NSW and 27 164 DALY in Australia in 2011. The burden was prominent among males and people aged 65 years and older. Most of the DALY (87%) was attributed to years of life lost or the fatal burden due to diabetes‐related lower limb amputation (DRLEA). The total monetary values of DALY of DFD for NSW and Australia were estimated at approximately AUD 2 billion and AUD 6 billion annually, respectively. Preventative and curative priorities should be given to DRLEA to reduce this burden and target males, especially those aged 65 years and older.
Keywords: Australia, burden of disease, DALY, diabetic foot, New South Wales, older adults
1. BACKGROUND
Diabetes mellitus is the fastest growing chronic disease in the world. According to the International Diabetes Federation, the estimated number of people with diabetes (18‐99 years) was 451 million in 2017 globally, and it was projected to increase to 693 million by 2045. 1 Approximately, 5 million deaths were associated with diabetes in 2017. 1 The global burden of disease attributable to diabetes was estimated as 67.9 million disability‐adjusted life‐years (DALY) 2 in 2017. People with diabetes are at significantly increased risk of having a range of complications, including cardiovascular, renal, eye and lower‐extremity complications. 3 , 4 The most disabling among these are the lower‐extremity complications of peripheral neuropathy, foot ulceration, infection and amputation. 5 , 6 Diabetes‐related foot disease (DFD) affected 131 million people worldwide in 2016, ranking 11th in global disease burden. 7 At the same time, it ranked higher than ischemic stroke (17th), ischemic heart disease (29th) and chronic kidney disease (52nd) attributed to diabetes. 7
Australia is not immune to this global public health problem. The prevalence of diabetes in Australia has had an upward trend for the last 25 years, and the total number of people with diabetes has tripled during this time. 8 According to the Australian Bureau of Statistics (ABS) 2017‐18 National Health Survey, an estimated 1.2 million Australians (4.9% of the total population) had diabetes. 8 The growing number of people with diabetes due to a higher incidence of obesity, an ageing population and a more sedentary lifestyle can exaggerate the situation in the future. 8
The prevalence of diabetes‐related foot ulcer among diabetes inpatients in Australia was reported as 15.1% in 2016, 9 with DFD being responsible for 5400 lower limb amputations annually. 10 The amputation rate due to diabetes in Australia was reported as one of the highest among developed countries. 10 The high rates have not decreased in a decade despite the country's economic progress. 11 Lower limb amputations and DFD are also associated with considerable morbidity and death. Over 5 years, the death rate after amputation ranged from 39% to 80%, much greater than the mortality rate after many cancers. 12 DFD was responsible for almost 1000 deaths in 2005, the most recent year for which statistics are available, accounting for approximately 8% of all diabetes‐related deaths in Australia. 8
Assessment of disease burden is important for understanding the full impact of the disease. 13 Despite DFD being a major public health concern, the availability of robust data on the disease burden of DFD in Australia and worldwide is very limited. Zhang et al. (2020) were the first to report the global DFD burden in 2016. 7 They reported the global burden estimates of DFD, and therefore, there is a scope of estimating the burden of disease attributed to DFD for Australia and detailing it by age and gender. Most recent Australian Burden of Disease studies (ABDS) (2011 and 2015) reported the burden of disease of diabetes aggregately; no separate estimates were reported for diabetic foot complications. 14 , 15 Besides these reports, there have been some state‐level and disease‐specific analyses of the burden of disease. The study by the Australian Institute of Health and Welfare (AIHW) (2017) was the first study to estimate Australia's disease burden of diabetes‐related lower limb amputation (DRLEA) in 2011 at the national level based on Western Australian linked hospitalisation and death data. 16 In the report, the non‐fatal burden of DRLEA was demonstrated in detail. At the same time, the report also stressed the importance of using linked hospital data at the personal level to estimate the burden more precisely by including other diabetic foot complications and related fatal burden.
The data on the disease burden of diabetic foot complications are also very limited at the state level, such as New South Wales (NSW). More than one‐third of the Australian population with diabetes live in NSW. 17 The population of NSW state can be a good representation of the whole country due to its diverse geography and demography. 17
Given the paucity of research regarding the burden of disease for DFD in Australia and NSW, our study will address the research gap by estimating fatal and non‐fatal disease burden for different DFDs, using a large cohort study in NSW linked with health services data. The objective of the study is to estimate the burden of DFD among older adults in NSW and Australia. Specifically, this article will examine the disease burden for different age groups and gender. The disease burden of DFD in terms of a comparable measure can help to understand the relative importance of DFD in setting up both preventative and curative priorities in the country. Moreover, it will also help to compare the burden due to DFD with other similar countries and contribute to international literature.
2. METHODS
2.1. Data sources and record linkage
Our study used data from the 45 and Up Study baseline survey and three health administrative data that were linked by a unique identifier. The 45 and Up Study survey participants were individuals aged 45 years and above residing in NSW, Australia. The survey was undertaken and managed by the Sax Institute between 2006 and 2009. 18 A random sample of 267 153 individuals aged 45 years and older from the Medicare Australia (Australia's public health insurance system) database was recruited in the survey. The survey's full details are available elsewhere. 18 Our study utilised data from the 45 and Up Study survey on self‐reported diabetes status, gender and age. 19
The linked health administrative datasets included:
NSW Admitted Patient Data Collection (APDC) that contained hospital utilisation data on admitted patients of public and private hospitals and private day procedure centres in NSW;
NSW Emergency Department Data Collection (EDDC) that consisted of health services data of individuals presented at public hospitals in NSW and
NSW Registry of Births, Deaths and Marriages (RBDM) had causes of deaths recorded as texts, with up to five causes of death.
APDC and EDDC were utilised to identify different diabetic foot complications using International Classification of Disease 10th revision Australian Modification (ICD‐10 am), International Classification of Diseases 9—Clinical Modification (ICD‐9 CM) and the Systematised Nomenclature of Medicine—Clinical Terms (SNOMED‐CT) diagnostic codes. RBDM was used to identify any participants who died in NSW, their date of death and whether causes of death were related to diabetic foot complications. These data sources have been detailed elsewhere. 20
The 45 and Up Study survey respondents' data were linked to other data using the probabilistic matching procedure by the Centre for Health Record Linkage (CHeReL) with a unique person project number deidentifying the data. 21 Hosting and access to the data were provided via Secure Unified Research Environment (SURE), a cloud‐based computing environment.
2.2. Ethics approval
This study was approved by NSW Population and Health Services Research Ethics Committee, Western Sydney University Human Research Ethics Committee and ACT Health Human Research Ethics and Governance. The 45 and Up Study had ethical clearance from the University of New South Wales Human Research Ethics Committee.
2.3. Study population and time period
The study year used in this study was 2011 for all survey and health systems data. The study population from the baseline survey in the 45 and Up Study survey in 2011 was 259 407 who were aged 45 years and over.
2.4. Identification of diabetes, DFD and causes of death
Individuals were identified as having diabetes if the 45 and Up Study survey, hospital (APDC, EDDC) or RBDM data reported participants as having diabetes. Diabetes was identified through the self‐reported diabetes status from the 45 an Up Study survey, ICD‐10 AM diagnostic codes (E10, E11, E13 and E14), ICD‐9 CM codes (249, 250) and SNOMED‐CT from APDC and EDDC. 22 , 23 Additionally, this study utilised analysis of the text of causes of deaths from the RBDM to identify people with diabetes.
DFD was only ascertained if diabetes was identified during or prior to the detection of foot complications. Our study included diabetic foot ulcer (E1x.73), infection (L03.02, L03.11, M86.x7, M86.x6), gangrene (E1x.52, R02x), diabetic peripheral neuropathy (DPNP) (E1x.42) and DRLEA (44370‐00, 44373‐00, 44367‐01, 44367‐02, 44338‐00, 44358‐00, 44361‐00, 44361‐01, 44364‐00, 44364‐01, 90557‐00, Z89.4, Z89.5, Z89.6) as DFD. These foot complications were identified from APDC and EDDC. 24 , 25 , 26
The causes of deaths related to DFD were identified from the RBDM data. Diabetic foot ulcer, infection, gangrene (DFUIG), DPNP and DRLEA‐related texts were retrieved to assign the corresponding cause of death. Furthermore, the cause of death was assumed to be associated with DRLEA if diabetes was recorded as a cause of death, 27 with a further assumption based on experts' opinion that DRLEA occurred at least 5 years before the person was deceased.
2.5. Calculation of DALY
The burden of disease was calculated using DALY approach. 28 DALY has two components: years of life lived with disability (YLD) and the years of life lost due to premature death (YLL). Our study adopted the hybrid perspective for calculating DALY, consistent with the ABDS 2011 and recent global studies. 14 , 29 YLL was calculated using the incidence‐based approach, whereas YLD was calculated from the prevalence perspective. There were few advantages of the prevalence‐based of calculating YLD compared to the incidence‐based approach. The duration of the disease was not required to calculate the YLD. As recommended by the ABDS 2011, the time discounting and age‐weighting were not applied to our estimates, consistent with the current international practice. 14 , 15 Age‐standardised rates (ASR) of different DALY components were calculated using the 2001 Australian population as the standard population per ABS and AIHW standards. 14 The life expectancy at the age of death was chosen according to the ABDS 2011. 14
YLD and YLL are summed up to calculate the DALY as follows:
2.5.1. Years lived with disability
The formula for estimating YLD based on prevalence approach follows as:
where: , sum over all age‐sex groups and diabetic foot complications; , point prevalence of diabetic foot complication i of j age‐sex group; , disability weight of diabetic foot complication i.
Aggregate YLD is calculated for DFUIG, whereas YLD for diabetic neuropathy and DRLEA were calculated separately. Both crude and ASR of YLD per 100 000 people were estimated. Total YLD was calculated by summing up YLDs across all DFD.
2.5.2. Years of life lost
YLL measures the fatal component of the burden of disease. The formula for calculating YLL follows as:
, sum over all ages and diabetic foot complications; , number of deaths due to diabetic foot complication i at age a; life expectancy at age a.
Similar to the approach adopted to estimate YLD, aggregate YLL was calculated for DFUIG, whereas YLL for DRLEA was calculated separately.
2.5.3. Disability weights
The disability weights of DFD and DRLEA were chosen according to the Global Burden of Disease Study 2013 (GBD 2013) following ABDS 2011. 14 , 29 The GBD 2013 reported disability weights for diabetic neuropathy, diabetic foot ulcer and toe and leg amputation. Our study made further assumptions to utilise these disability weights. The disability weight of diabetic foot ulcer (0.02) was assigned to diabetic foot ulcer, diabetic foot infection and gangrene, and the disability weight of diabetic neuropathy (0.133) was used for DPNP in our study. In the absence of information related to the prosthesis in the current study, we used the average disability weight of amputation with a prosthesis (0.039) and amputation without a prosthesis (0.173). Again, the disability weight of toe amputation (0.006) was used for toe or foot amputation.
2.5.4. DALY monetary value
After summing up YLD and YLL to calculate DALY, the estimates were also converted to a monetary value by multiplying them with the value of statistical life year. The value of AUD 222 000 measured in 2021 dollars was used in this study, recommended by the Department of the Prime Minister and Cabinet of Australian Government. 30
3. RESULTS
Out of 259 407 participants of the survey, 27 931 individuals were identified to have diabetes, with 755 having DFUIG, 487 having DPNP and 327 having DRLEA in 2011. The frequency and percentage distribution of cases and deaths due to DFD and DRLEA among the survey participants in 2011 are presented in Table 1. All types of DFD and DRLEA cases were prominent (more than 60%) among male participants. Deaths due to these conditions were even more dominant among males. About three‐quarters of deaths were due to DFUIG among males, whereas about 90% of the deaths due to DRLEA was observed among males in the study period. People aged 65 years and older consisted of more than 70% cases for all DFD and DRLEA. This age group was also reported to have most percentage of deaths (over 80%) due to all types of diabetic foot complications.
TABLE 1.
Diabetes‐related foot disease and lower‐limb amputation among study participants in 2011
| Number of cases | Number of cases per 100 000 people a , b | Number of deaths | Number of deaths per 100 000 people a , b | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male (N = 119 081) | Female (N = 140 325) | 45 to 64 y (N = 133 611) | ≥65 y (N = 125 784) | Male (N = 119 081) | Female (N = 140 325) | 45 to 64 y (N = 133 611) | ≥65 y (N = 125 784) | |||
| Diabetic foot ulcer, infection, gangrene (yes) (n = 755, m = 18) | 457 (61%) | 298 (39%) | 132 (17%) | 623 (83%) | 291 | >13 c | <5 c | <5 c | >13 c | 7 |
| Diabetic peripheral neuropathy (yes) d (n = 487, m = 0) | 291 (60%) | 196 (40%) | 128 (26%) | 359 (74%) | 188 | 0 | 0 | 0 | 0 | 0 |
| Diabetes‐related lower limb amputation (yes) (n = 327, m = 40) | 235 (72%) | 92 (28%) | 78 (24%) | 249 (76%) | 126 | >35 c | <5 c | 5 | 35 | 15 |
| Toe or foot d (n = 205, m = 0) | 141 (69%) | 64 (31%) | 56 (27%) | 149 (73%) | 79 | 0 | 0 | 0 | 0 | 0 |
| Below or above knee (n = 122, m = 40) | 94 (77%) | 28 (23%) | 22 (18%) | 100 (82%) | 47 | >35 c | <5 c | 5 | 35 | 15 |
Note: Percentage is reported in parentheses only for the number of cases with diabetic foot complications.
Total sample size = 259 407.
Gender variable had 1 missing value, and age variable had 12 missing values.
True numbers are not reported due to the confidentiality requirement of the Sax Institute's 45 and Up Study.
Neither diabetic peripheral neuropathy nor diabetes‐related foot/toe amputation was found as a cause of death in the RBDM data in 2011, n = number of total cases, m = number of total deaths.
In Figure 1, a comparison of YLD for males and females is shown by different age groups. For every age group, the non‐fatal burden of all types of DFD and DRLEA was mostly borne by males. Among all foot complications, DRLEA had widest the gap between male YLD and female YLD. For instance, for the age group 80 to 85 years, males had five times more YLD due to DRLEA than females. However, the difference between YLD of males and females due to DPNP and DFUIG narrowed for 75 years and above. The figure also clearly depicts that the YLD increased with age. The relevant data of Figure 1 are presented in Table S1.
FIGURE 1.
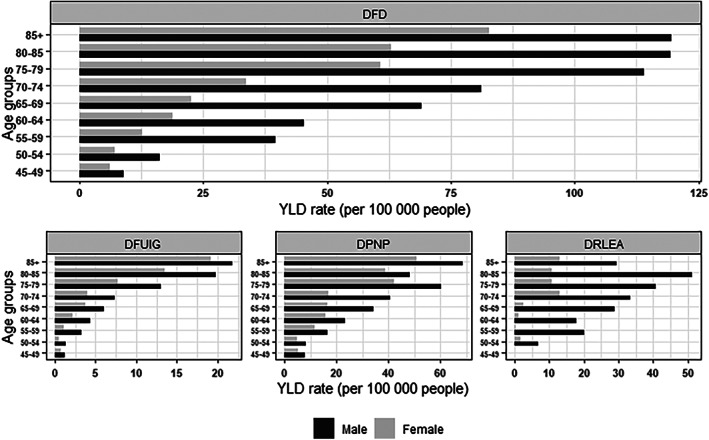
Age‐standardised years of life lived with disability (YLD) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender
In Figure 2, a comparison of YLLs for males and females is shown by different age groups. Due to the low number of deaths, the comparison was presented in two age groups: 45 to 64 years and 65 years and older. As no death was associated with DPNP, there was no YLL associated with this complication. Similar to YLD burden, YLL is significantly prominent among males. About 90% of the YLL burden due to DFUIG and DRLEA was borne by males. The major proportion of the total disease burden for males was attributed to DRLEA. Therefore, as expected, it can be seen from Figure 3 that DALY experienced by males was highly prominent (about 80% of the burden). The relevant data of Figures 2 and 3 are presented in Tables S2 and S3, respectively.
FIGURE 2.
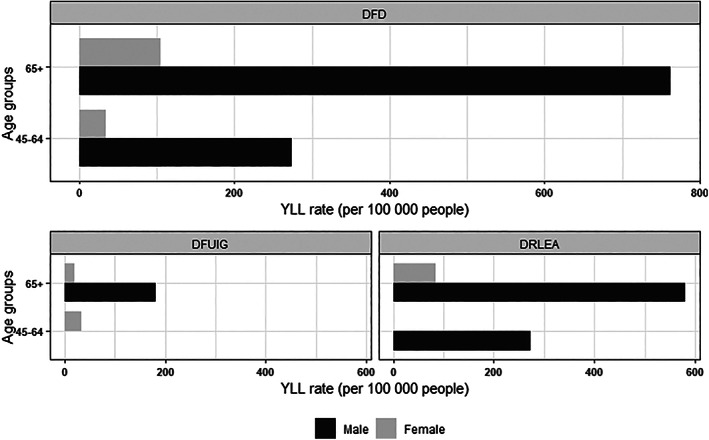
Age‐standardised years of life lost (YLL) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender
FIGURE 3.
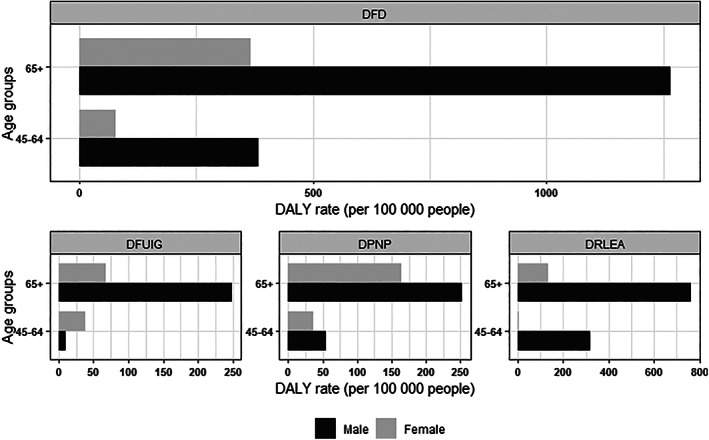
Age‐standardised disability‐adjusted life‐years (DALY) rate (per 100 000 people) due to due to different types of diabetes‐related foot disease (DFD) by age and gender
In Table 2, crude and ASR of all components of burden of disease due to DFD and DRLEA are presented. The ASR of DALY due to DRLEA (200.1) was about 10 times higher than the DALY imposed by DPNP (20.0) and nearly 4 times higher than DFUIG (52.6). However, the ASR of YLD for the DPNP (20.0) was the highest (62% of ASR of YLD) among all foot complications. Overall, about 80% and 73% of ASR of YLL and DALY were due to DRLEA.
TABLE 2.
Crude and age‐standardised years of life lived with disability (YLD), years of life lost (YLL) and disability‐adjusted life‐years (DALY) for people (45 years and above) with diabetes‐related foot disease (DFD) in New South Wales (NSW) in 2011
| YLD | YLL | DALY | ||||
|---|---|---|---|---|---|---|
| Crude rate | Age‐standardised rate | Crude rate | Age‐standardised rate | Crude rate | Age‐standardised rate | |
| Diabetic foot ulcer, infection and gangrene | ||||||
| Male | 7.7 | 5.5 | 95.7 | 64.1 | 103.4 | 69.6 |
| Female | 4.3 | 3.4 | 27.6 | 28.8 | 31.8 | 32.2 |
| Person | 5.8 | 4.4 | 58.9 | 48.2 | 64.7 | 52.6 |
| Diabetic peripheral neuropathy | ||||||
| Male | 32.6 | 24.8 | 0.0 | 0.0 | 32.6 | 24.8 |
| Female | 18.6 | 15.6 | 0.0 | 0.0 | 18.6 | 15.6 |
| Person | 25.0 | 20.0 | 0.0 | 0.0 | 25.0 | 20.0 |
| Diabetes‐related lower limb amputation | ||||||
| Male | 17.5 | 18.8 | 435.9 | 382.6 | 453.4 | 401.4 |
| Female | 4.5 | 3.7 | 37.8 | 29.9 | 42.3 | 33.6 |
| Person | 10.4 | 7.9 | 220.7 | 192.2 | 231.1 | 200.1 |
| All DFD and diabetes‐related lower limb amputation | ||||||
| Male | 57.7 | 49.2 | 531.7 | 446.7 | 589.4 | 495.9 |
| Female | 27.4 | 22.7 | 65.4 | 58.7 | 92.8 | 81.4 |
| Person | 41.3 | 32.4 | 279.5 | 240.4 | 320.8 | 272.7 |
Table 3 illustrated total YLD, YLL and DALY due to diabetic foot complications and converted monetary values for NSW and Australia. We calculated the estimates for Australia assuming the same prevalence of diabetic foot complications and incidence of mortality. Total DALY due to DFD and DRLEA in NSW in 2011 was estimated as 8915, with more than 70% coming from DRLEA. Out of this 8915 DALY, YLL contributed to 7767 (87%) DALY. The monetary values of DALY of NSW and Australia were estimated as AUD 1979 million and AUD 6030 million, respectively.
TABLE 3.
Burden of disease due to different types of diabetes‐related foot disease (DFD) among people aged 45 years and older in New South Wales (NSW) a and Australia b in 2011
| Total YLD in NSW | Total YLD in Australia | Total YLL in NSW | Total YLL in Australia | Total DALY in NSW | Total DALY in Australia | Monetary value c of DALY (NSW) | Monetary value c of DALY (Australia) | |
|---|---|---|---|---|---|---|---|---|
| Diabetic foot ulcer, infection and gangrene | 162 | 494 | 1636 | 4984 | 1798 | 5478 | 399 | 1216 |
| Diabetic peripheral neuropathy | 695 | 2118 | — | — | 695 | 2118 | 154 | 470 |
| Diabetes‐related lower limb amputation | 290 | 885 | 6132 | 18 683 | 6422 | 19 568 | 1426 | 4344 |
| All DFD and DRLEA | 1148 | 3497 | 7767 | 23 667 | 8915 | 27 164 | 1979 | 6030 |
Abbreviations: DALY, disability‐adjusted life‐years; DRLEA, diabetes‐related lower limb amputation; YLD, years of life lived with disability; YLL, years of life lost.
Based on NSW population (45 years and older) of 2.78 million in 2011.
Based on Australian population (45 years and older) of 8.47 million in 2011.
Monetary value is expressed in 2021 AUD (in million) and rounded to zero decimal place.
4. DISCUSSION
The current study set out to estimate the fatal and non‐fatal burden of disease of DFD and DRLEA among people aged 45 years and older in NSW and Australia in 2011. Total DALY was calculated as 8915 in 2011. Extrapolated to Australians aged 45 years and above, the total DALY was estimated as 27 164. Results showed that the burden was prominent among males and people aged 65 years and over. About 87% of DALY was attributed to YLL. Among different diabetic foot complications, DRLEA contributed to most of the YLL and DALY, with DPNP being the most contributor to YLD.
The ABDS 2011 on lower limb amputation found that age‐standardised YLD rate of 1.8 per 100 000 people in Australia in 2011 due to DRLEA. 16 The estimate was lower compared to our estimate of 7.9. The prevalence and other inputs used in the ABDS 2011 were based on the National Hospital Morbidity Database and Western Australian linked hospitalisation and death data. Our study data were based on NSW. The difference in estimates might be attributed to the prevalence of DRLEA in two regions in 2011.
Our study found that most of the burden of DFD was concentrated among males and the older population. The findings are similar to the ABDS 2011 on lower limb amputation, where it was found that 73% of the YLD burden due to DRLEA was borne by males. 16 They also found that the burden peaked at ages 85 years and over, whereas our estimates were the highest for the 80 to 84 years age group. Our finding is also corroborated by the study by Zhang et al. (2020), where they reported that the burden disproportionately affected males and the older aged population globally. 7 Although females in Australia have a higher life expectancy, the higher YLD burden could be due to the higher prevalence of diabetic foot complications among males for most age groups, as documented by several studies. 23 , 31 , 32 , 33 , 34
Our study found that the number of deaths due to DFUIG was 7 per 100 000 people in 2011 among individuals aged 45 years and older. At this rate, the total number of deaths due would equate to 587 deaths due to DFUIG in Australia. The most recent data on mortality due to diabetic foot complications dates to 2005, which was reported in the study by the AIHW (2020). 8 They reported over 1000 deaths due to diabetic foot ulcer. There might be an indication that the number of deaths to diabetic foot ulcers decreased over the 6 years from 2005 to 2011. However, the burden attributed to mortality was still the dominant contributor to the disease in our study. We could not compare our results on the fatal burden of DFD and DRLEA in the Australian setting due to the unavailability of estimates in this regard in the existing literature. However, our finding was contrary to an international study based in Brazil, where they found that non‐fatal burden comprised the majority proportion of the total DALY burden. 27 The reasons for the lower contribution of YLD in the case of Australia might be that the years lived with a disability after major amputation could be low as the incidence of amputation occurred at a comparatively older age with a lower survival rate in the Australian population.
While our study found DRLEA to be the most contributor (80%) of the fatal burden, DPNP had a higher non‐fatal burden than any other diabetic foot complications in this study (62%). The finding is consistent with the most recent global study, which reported that neuropathy had the largest share (76%) of the YLD burden. 7 DPNP was associated with a high disability weight, which could contribute to this burden along with the fact it is a permanent condition, unlike diabetic foot ulcer or infection. It could be possible that DPNP‐attributed YLD was an overestimation because DPNP may occur other than lower extremity. In the absence of etiological information in ICD‐10 AM, we could not separate DPNP by its location. However, DPNP is more likely to affect the lower extremity, minimising the overestimation. 35
Our study could provide new insights when findings were compared with the ABDS 2011. In the ABDS 2011, it was reported that a total of 106 097 DALY was due to endocrine disorders. 14 Our study found that DFD contributed 27 164 DALY in Australia in 2011, about 25% of the total endocrine burden. At the same time, the burden share of DFD was about 0.6% of total DALY due to all causes in Australia, which ranks below the reproductive/maternal‐related health problem. Even with a separate cause and an estimation for a sub‐population, DALY due to DFD would be ranked within 20 in the ABDS 2011.
The key strength of our study is that it included an in‐depth analysis of the burden of diabetic foot complications in terms of both morbidity and mortality of the disease in NSW and Australia. Another strength is the inclusion of different diabetic foot complications such as diabetic foot infection, gangrene and minor amputation, which were not included in existing Australian and global studies. However, the findings of this study should be interpreted in light of a few limitations. First, similar to the GBD studies, our study assumed that the morbidity and death were attributed to DFD and DRLEA, although the individual could have morbidity and mortality from multiple causes. Second, the DALY calculated for Australia might be a conservative estimate because the prevalence of diabetes in other states of Australia could be higher than NSW. However, the findings in terms of YLD and YLL, which were not previously available in detail, could add valuable insights to our understanding. Finally, the study findings are not for the most recent year. However, to our knowledge, our study estimates are the most recent available information for NSW and Australia.
5. CONCLUSION
This study sought to fill the gap in the existing literature about the burden of disease attributed to DFD and DRLEA, and as such, provided comparable estimates in terms of gender and age. The study found that males and very old individuals disproportionately suffered from the burden. It was also found that the mortality burden comprised much of this burden, which was due to preventable DRLEA. Our research can help understand the relative importance of diabetic foot complications in setting up both preventative and curative priorities. It can also help decision‐makers to allocate resources for health services research. At the same time, this study can help identify the disadvantaged groups and target health interventions. Future research incorporating all diabetic foot complications and most recent data can be considered to understand the trend and depth of the burden of this major health problem more precisely. We also recommend diabetic foot complications to be treated as a separate cause in future ABDS.
Supporting information
Table S1. Age‐standardised years of life lived with disability (YLD) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Table S2. Age‐standardised years of life lost (YLL) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Table S3. Age‐standardised disability‐adjusted life‐years (DALY) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Ahmed MU, Tannous WK, Agho KE, Henshaw F, Turner D, Simmons D. The burden of diabetes‐related foot disease among older adults in Australia. Int Wound J. 2022;19(7):1758‐1768. doi: 10.1111/iwj.13781
Funding information South Western Sydney Local Health District, Grant/Award Number: P00025334
DATA AVAILABILITY STATEMENT
Due to privacy concerns, data from the 45 and Up Study cohort and other linked sources cannot be made publicly accessible. Rules and procedures to access data are available at https://www.saxinstitute.org.au.
REFERENCES
- 1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271‐281. [DOI] [PubMed] [Google Scholar]
- 2. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Gregg EW, Sattar N, Ali MK. The changing face of diabetes complications. Lancet Diabetes Endocrinol. 2016;4(6):537‐547. [DOI] [PubMed] [Google Scholar]
- 4. Harding JL, Pavkov ME, Magliano DJ, Shaw JE, Gregg EW. Global trends in diabetes complications: a review of current evidence. Diabetologia. 2019;62(1):3‐16. [DOI] [PubMed] [Google Scholar]
- 5. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367‐2375. [DOI] [PubMed] [Google Scholar]
- 6. Boulton AJM, Vileikyte L, Ragnarson‐Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;366(9498):1719‐1724. [DOI] [PubMed] [Google Scholar]
- 7. Zhang Y, Lazzarini PA, Mcphail SM, Van Netten JJ, Armstrong DG, Pacella RE. Global disability burdens of diabetes‐related lower‐extremity complications in 1990 and 2016. Diabetes Care. 2020;43(5):964‐974. [DOI] [PubMed] [Google Scholar]
- 8. Australian Institute of Health and Welfare. Diabetes. 2020. https://www.aihw.gov.au/reports/diabetes/diabetes
- 9. Lazzarini PA, Hurn SE, Kuys SS, et al. Direct inpatient burden caused by foot‐related conditions: a multisite point‐prevalence study. BMJ Open. 2016;6(6):e010811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Australian Institute of Health and Welfare . Indicators for the Australian National Diabetes Strategy 2016–2020: Data Update; 2020. https://www.aihw.gov.au/reports/diabetes/diabetes-indicators-strategy-2016-2020.
- 11. Lazzarini PA, Gurr JM, Rogers JR, Schox A, Bergin SM. Diabetes foot disease: the Cinderella of Australian diabetes management? J Foot Ankle Res. 2012;5(1):24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217‐228. [DOI] [PubMed] [Google Scholar]
- 13. Australian Institute of Health and Welfare . Burden of Disease. https://www.aihw.gov.au/reports/australias-health/burden-of-disease.
- 14. Australian Institute of Health and Welfare . Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2011; 2016. https://www.aihw.gov.au/reports/burden-of-disease/abds-impact-and-causes-of-illness-death-2011/contents/highlights.
- 15. Australian Institute of Health and Welfare . Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2015 2019. https://www.aihw.gov.au/reports/burden-of-disease/burden-disease-study-illness-death-2015/summary.
- 16. Australian Institute of Health Welfare . Burden of Lower Limb Amputations Due to Diabetes in Australia: Australian Burden of Disease Study 2011; 2017. https://www.aihw.gov.au/reports/burden-of-disease/lower-limb-amputations-due-to-diabetes.
- 17. Australian Bureau of Statistics . National Health Survey: First Results, Australia 2014–15; 2015. https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4364.0.55.0012014-15?OpenDocument.
- 18. 45 and Up Study Collaborators. Cohort Profile: The 45 and Up Study. Int J Epidemiol. 2008;37(5):941‐947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. The Sax Institute . Data and Technical Information. https://www.saxinstitute.org.au/our-work/45-up-study/data-book/.
- 20. Centre for Health Record Linkage (CheReL) . Data Dictionaries. https://www.cherel.org.au/data-dictionaries.
- 21. Centre for Health Record Linkage (CHeReL) . How Record Linkage Works. http://www.cherel.org.au/how-record-linkage-works.
- 22. Comino EJ, Tran DT, Haas M, et al. Validating self‐report of diabetes use by participants in the 45 and Up Study: a record linkage study. BMC Health Serv Res. 2013;13(1):481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ahmed MU, Tannous WK, Agho KE, Henshaw F, Turner D, Simmons D. Prevalence and burden of diabetes‐related foot disease in New South Wales, Australia: evidence from the 45 and Up Study survey data linked with health services data. Int J Environ Res Public Health. 2021;18(21):11528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Commons RJ, Robinson CH, Gawler D, Davis JS, Price RN. High burden of diabetic foot infections in the top end of Australia: an emerging health crisis (DEFINE study). Diabetes Res Clin Pract. 2015;110(2):147‐157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Lipsky BA, Peters EJG, Senneville E, et al. Expert opinion on the management of infections in the diabetic foot. Diabetes Metab Res Rev. 2012;28(S1):163‐178. [DOI] [PubMed] [Google Scholar]
- 26. van Netten JJ, Bus SA, Apelqvist J, et al. Definitions and criteria for diabetic foot disease. Diabetes Metab Res Rev. 2020;36(S1):e3268. [DOI] [PubMed] [Google Scholar]
- 27. Santos KP, Luz SC, Mochizuki L, d'Orsi E. Burden of disease from lower limb amputations attributable to diabetes mellitus in Santa Catarina state, Brazil, 2008‐2013. Cad Saude Publica. 2018;34(1):e00013116. [DOI] [PubMed] [Google Scholar]
- 28. Murray CJ. Quantifying the burden of disease: the technical basis for disability‐adjusted life years. Bull World Health Organ. 1994;72(3):429‐445. [PMC free article] [PubMed] [Google Scholar]
- 29. Salomon JA, Haagsma JA, Davis A, et al. Disability weights for the global burden of disease 2013 study. Lancet Global Health. 2015;3(11):e712‐e723. [DOI] [PubMed] [Google Scholar]
- 30. The Office of Best Practice Regulation, Australian Government . Best Practice Regulation Guidance Note Value of statistical life; 2021. https://obpr.pmc.gov.au/sites/default/files/2021-09/value-of-statistical-life-guidance-note-2020-08.pdf.
- 31. Parisi MCR, Moura Neto A, Menezes FH, et al. Baseline characteristics and risk factors for ulcer, amputation and severe neuropathy in diabetic foot at risk: the BRAZUPA study. Diabetol Metab Syndr. 2016;8(1):25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Tapp RJ, Shaw JE, De Courten MP, Dunstan DW, Welborn TA, Zimmet PZ. Foot complications in type 2 diabetes: an Australian population‐based study. Diabet Med. 2003;20(2):105‐113. [DOI] [PubMed] [Google Scholar]
- 33. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta‐analysis. Ann Med. 2017;49(2):106‐116. [DOI] [PubMed] [Google Scholar]
- 34. Ahmed MU, Tannous WK, Agho KE, Henshaw F, Turner D, Simmons D. Social determinants of diabetes‐related foot disease among older adults in New South Wales, Australia: evidence from a population‐based study. J Foot Ankle Res. 2021;14(1):65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Pop‐Busui R, Boulton AJM, Feldman EL, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Age‐standardised years of life lived with disability (YLD) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Table S2. Age‐standardised years of life lost (YLL) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Table S3. Age‐standardised disability‐adjusted life‐years (DALY) rate (per 100 000 people) due to different types of diabetes‐related foot disease (DFD) by age and gender.
Data Availability Statement
Due to privacy concerns, data from the 45 and Up Study cohort and other linked sources cannot be made publicly accessible. Rules and procedures to access data are available at https://www.saxinstitute.org.au.